

ABSTRACT
Background
Correct working length determination is one of the main factors leading to success in root canal treatment. The digital tactile sense technique and conventional radiography (CR) are common techniques for working length determination but both techniques have some limitations. A newer method of working length estimation involves use of the apex locator. The current study was carried out to compare the accuracy of the apex locator with a tactile and conventional radiographic method for working length determination in primary and permanent teeth.
Materials and methods
The study was conducted on 60 children selected randomly from the outpatient department of the Department of Pediatric and Preventive Dentistry. The patients were divided into two groups: primary and permanent. An informed consent was obtained. After radiographic confirmation of the presence of more than two-third root length access, opening was done in all the teeth. The pulp was extirpated completely from the chamber and canals. Canals were dried completely using paper points. Working length was determined by all the three methods, i.e., digital tactile method, apex locator, and conventional intraoral periapical radiographic method in both primary and permanent teeth.
Results
The data were coded and entered into the Microsoft Excel spreadsheet. The analysis was done using the SPSS version 20 (IBM SPSS Statistics Inc., Chicago, Illinois, USA) Windows software program. The variables were assessed for normality using the one-way ANOVA test. Within the limitations of this study, working lengths obtained by the tactile method, the apex locator, and the radiographic method were comparable. There was no statistically significant difference among the three methods except in mesiolingual and distobuccal canals of permanent teeth.
Conclusion
The apex locator can serve as a useful guide to determine the working length in permanent as well as primary teeth.
How to cite this article
Rathore K, Tandon S, Sharma M, et al. Comparison of Accuracy of Apex Locator with Tactile and Conventional Radiographic Method for Working Length Determination in Primary and Permanent Teeth. Int J Clin Pediatr Dent 2020;13(3):235–239.
Keywords: Permanent teeth, Primary teeth, Root canal treatment, Working length
BACKGROUND
“It is of great use to the sailor to know the length of his line, though he cannot with it fathom all the depths of the ocean.”—John Locke
Working length determination forms one of the critical steps in endodontic treatment. Accurate determination of apical stop aids in limiting instrumentation within the confines of the root canal. It minimizes the damage to the developing tooth bud in primary teeth. Estimation of working length is difficult in primary teeth because of the irregular oblique resorption pattern in deciduous root canals, making it difficult to determine the apical foramen accurately.1
The digital tactile sense technique and conventional radiography (CR) are common techniques of working length determination but both techniques have some limitations. The digital tactile sense technique requires that the clinician be trained and have experience.2 This technique is mostly obsolete these days and there are very few studies published justifying its use in determination of working length. Radiography is traditionally used to obtain information about root canal anatomy, working length, and the surrounding apical tissues. However, the accurate determination of root canal length radiographically is compromised because of the anatomical variations or projection errors. In addition, there is radiation hazard both to the patient and dental personnel. The observers’ bias in radiographic interpretation may lead to errors. Moreover, it is often difficult to obtain a diagnostic radiograph in children because of poor cooperation and limited access to the mouth leading to difficulty in film placement.1,3
In primary teeth, electronic devices (apex locators) have been proposed to determine root canal working lengths. Reduction in radiation dosage and procedure time is the advantage of these devices, which aid in patient cooperation. Apex locators also accurately measures the foramen or more precisely an area between the minor and major diameter.1
Many reports have been published on the accuracy of apex locators in permanent teeth but the information on primary teeth is limited.4 So, the current study was carried out to compare the accuracy of the apex locator with the tactile and conventional radiographic method for working length determination in primary and permanent teeth.
MATERIALS AND METHODS
Type of Study
This study was a randomized control trial. The study was approved by the institutional ethical committee. The procedure was fully explained to the parents of the children involved and their written consent was obtained prior to the procedure.
Details of Study Subjects
The study was conducted on 60 children selected randomly from the outpatient department of the Department of Pediatric and Preventive Dentistry. The patients were divided into two groups: primary and permanent.
Inclusion Criteria
Patient Selection
Cooperative children in the age group of 5–12 years.
Patients with no history of systemic illness/disease or recent hospitalization.
Tooth Selection
Primary molars indicated for pulpectomy with minimum of two-third of root length present.
Permanent molars indicated for root canal treatment with closed apex.
Exclusion Criteria
Uncooperative patients
Permanent teeth with incompletely formed root
Teeth with excessive root resorption or evident root fracture.
Study Groups
The subjects were divided into two groups:
Group I: Children requiring pulpectomy for their primary molars (30).
Group II: Children requiring root canal treatment for their permanent molars (30).
Steps of Study
An informed consent was obtained from guardian/parent accompanying the pediatric patient under study approved by the ethical committee.
Isolation of tooth was obtained using a rubber dam.
After radiographic confirmation of the presence of more than two-third root length access, opening was done in all the teeth.
The pulp was extirpated completely from the chamber and canals.
Canals were dried completely using paper points.
Working length was determined by all the three methods, i.e., digital tactile method, apex locator, and conventional intraoral periapical radiographic method in both primary and permanent teeth.
Tactile Method
A flat reference point was prepared and marked on the occlusal surface of the teeth to allow for precise positioning of the k-file for working length determination. The size of the k-file used was such that passive binding occurred as the file approached the estimated length. Tentative working length was recorded at this point using a ruler.
Apex Locator
In each tooth, electronic root length was measured by the Root zx apex locator following the manufacturer's instructions. If the reading were stable for at least 5 seconds, the electronic root canal length was measured using the 0.5-mm precision endodontic ruler considering the actual root length5 (Fig. 1).
Fig. 1.
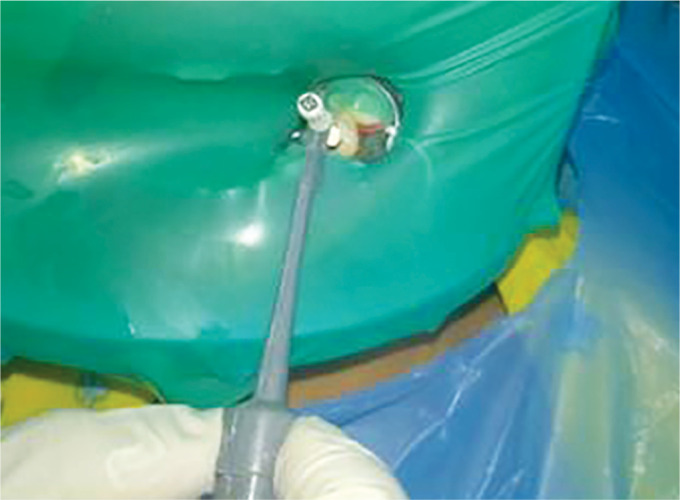
Determination of working Length by apex locator
Conventional Radiographic Method
Exact working length of the teeth was determined using the Grossman's method6 (Figs 2 and 3).
Fig. 2.
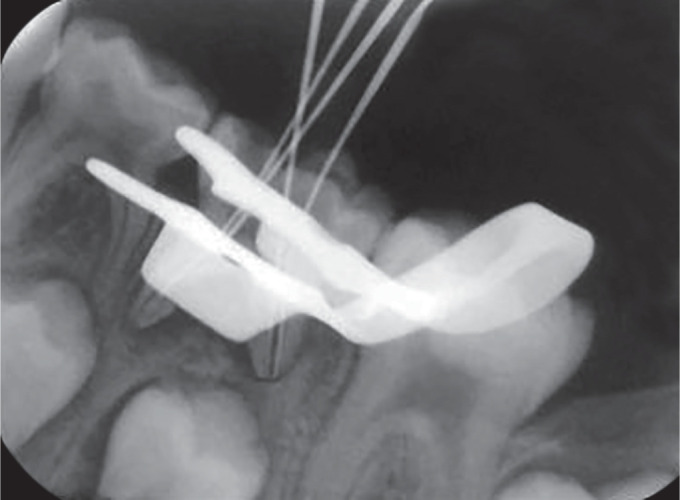
Determination of working length by radiograph in primary tooth
Fig. 3.
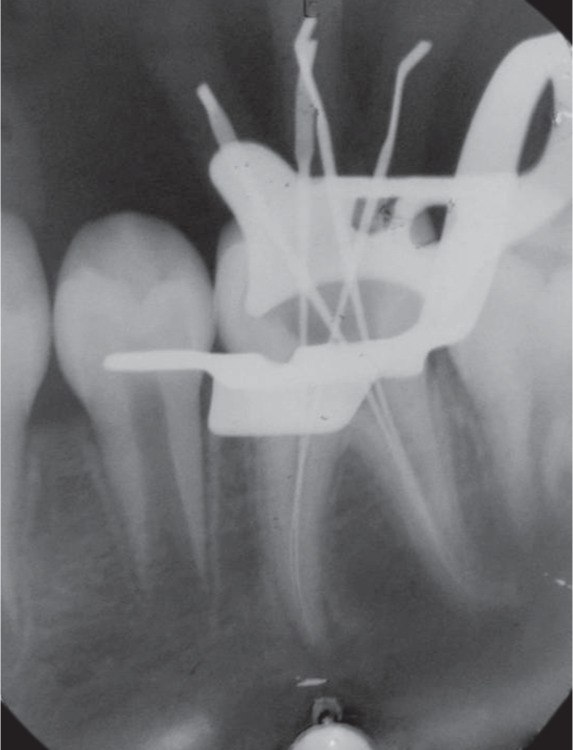
Determination of working length by radiograph in permanent tooth
OBSERVATIONS AND RESULTS
Statistical Analysis
Out of the 30 primary lower molars included in the study, 5 had three canals and 25 had four canals. Out of the 30 permanent lower molars, 7 teeth had three canals and 23 had four canals. In order to reduce bias in the study, only teeth with four canals were included in the study.
The data were coded and entered into the Microsoft Excel spreadsheet. The analysis was done using the SPSS version 20 (IBM SPSS Statistics Inc., Chicago, Illinois, USA) Windows software program. The variables were assessed for normality using the one-way ANOVA test. After that, comparison among the methods was also performed using one-way ANOVA. The level of significance was set at p = 0.05 (p ≤ 0.05—significant, p ≤ 0.01—highly significant, p ≤ 0.0001—very highly significant). From the present in vivo study, following results were obtained.
Table 1 shows that with the tactile method the mesiobuccal, mesiolingual, distobuccal, and distolingual canals of primary teeth showed the mean value of working length to be 11.73 ± 1.48, 11.13 ± 1.63, 11.70 ± 1.48, and 10.28 ± 1.64, respectively. For the apex locator, it is 11.75 ± 0.85, 11.03 ± 1.14, 12.01 ± 1.68, and 10.09 ± 1.60, respectively. The conventional radiograph showed 11.350 ± 0.99, 10.58 ± 1.28, 11.80 ± 1.50, and 11.68 ± 1.60, respectively. The p values for these three methods in mesiobuccal, mesiolingual, distobuccal, and distolingual canals are shown in Table 2. It was found to be statistically insignificant.
Table 1.
Comparisons of root canal measurement by tactile, conventional radiograph, and apex locator methods in primary teeth. Working length (mean ± SD)
| Variable | Mesiobuccal canal | Mesiolingual canal | Distobuccal canal | Distolingual canal |
|---|---|---|---|---|
| Tactile method | 11.73 ± 1.48 | 11.13 ± 1.63 | 11.70 ± 1.48 | 10.28 ± 1.64 |
| Apex locator | 11.75 ± 0.85 | 11.03 ± 1.14 | 12.01 ± 1.68 | 10.09 ± 1.60 |
| Conventional radiograph | 11.350 ± 0.99 | 10.58 ± 1.28 | 11.80 ± 1.50 | 11.68 ± 1.60 |
Statistically significant difference at p = 0.05. Test of significance—one-way ANOVA test; SD, standard deviation
Table 2.
Intergroup comparisons of root canal measurement by tactile, apex locator, and conventional radiograph methods in primary teeth (p value)
| Mesiobuccal canal | Mesiolingual canal | Distobuccal canal | Distolingual canal | ||
|---|---|---|---|---|---|
| Tactile method | Conventional radiograph | 0.59 | 0.37 | 1.000 | 1.000 |
| Apex locator | 1.000 | 1.000 | 1.000 | 0.53 | |
| Apex locator | Tactile method | 1.000 | 1.000 | 1.000 | 0.53 |
| Conventional radiograph | 0.53 | 0.62 | 1.000 | 1.000 | |
| Conventional radiograph | Tactile method | 0.59 | 0.37 | 1.000 | 1.000 |
| Apex locator | 0.53 | 0.62 | 1.000 | 1.000 |
Table 2 shows intergroup comparisons of root canal measurement by tactile, apex locator, and conventional radiograph methods in primary teeth (Fig. 4).
Fig. 4.

Comparison of root canal measurement in primary teeth
Table 3 shows that with the tactile method the mesiobuccal, mesiolingual, distobuccal, and distolingual canals of permanent teeth showed the mean values of working length to be 18.83 ± 1.05, 18.33 ± 1.49, 19.96 ± 0.99, and 19.65 ± 1.07, respectively. For the apex locator, it is 19.41 ± 0.87, 19.02 ± 0.65, 19.9 ± 0.75, and 19.52 ± 0.85, respectively. The conventional radiograph showed 19.3 ± 0.83, 19.15 ± 0.69, 19.83 ± 0.86, and 19.34 ± 0.66, respectively. The p values for these three methods in mesiobuccal and mesiolingual canals were 0.04*, 0.002*, which is statistically significant, and 0.84 and 0.48 in distobuccal and distolingual canals, which is statistically insignificant.
Table 3.
Comparisons of root canal measurement by tactile, apex locator, and conventional radiograph methods in permanent teeth
| Variable | Mesiobuccal canal | Mesiolingual canal | Distobuccal canal | Distolingual canal |
|---|---|---|---|---|
| Tactile method | 18.83 ± 1.05 | 18.33 ± 1.49 | 19.96 ± 0.99 | 19.65 ± 1.07 |
| Apex locator | 19.41 ± 0.87 | 19.02 ± 0.65 | 19.90 ± 0.75 | 19.52 ± 0.85 |
| Conventional radiograph | 19.30 ± 0.83 | 19.15 ± 0.69 | 19.83 ± 0.86 | 19.34 ± 0.66 |
Statistically significant difference at p = 0.05. Test of significance—one-way ANOVA test; SD, standard deviation
Table 4 shows intergroup comparisons of root canals by tactile, apex locator, and conventional radiograph methods in permanent teeth. The apex locator showed a p value of 1.000 with the tactile method in the distobuccal canal and distolingual canal and with the conventional radiograph method in all four canals. The tactile method showed a value of 0.16 with conventional radiograph in the mesiobuccal canal, 0.008* in the mesiolingual canal, and 0.70 in the distolingual canal. With the apex locator it showed a value of 0.05* in the mesiobuccal canal and 0.004* in the mesiolingual canal (Fig. 5).
Table 4.
Intergroup comparisons of root canal measurement by tactile, apex locator and conventional radiograph methods in permanent teeth (mesiobuccal) canal
| Mesiobuccal canal | Mesiolingual canal | Distobuccal canal | Distolingual canal | ||
|---|---|---|---|---|---|
| Tactile method | Conventional radiograph | 0.16 | 0.008* | 1.000 | 0.70 |
| Apex locator | 0.05* | 0.004* | 1.000 | 1.000 | |
| Apex locator | Tactile method | 0.05* | 0.004* | 1.000 | 1.000 |
| Conventional radiograph | 1.000 | 1.000 | 1.000 | 1.000 | |
| Conventional radiograph | Tactile method | 0.16 | 0.008* | 1.000 | 0.70 |
| Apex locator | 1.000 | 1.000 | 1.000 | 1.000 |
Statistically significant finding
Fig. 5.

Comparison of root canal measurement in permanent teeth
DISCUSSION
In the present study, the radiographic method of root canal determination has been compared with the tactile method and the apex locator as these are the most commonly used methods.
A sample size of 60 subjects has been taken for the study, which is much larger than the previous studies conducted by Mello-Moura et al.,3 Mente et al.,7 Odabaş,8 and Parekh.9
Most of the studies have been conducted on single rooted teeth.3,7,9–13 In the current study, only multirooted teeth have been selected similar to the studies conducted by Odabaş et al.,8 Angwaravong,14 and Soruri.15 In the all previous studies conducted on multirooted teeth, only number of canal as a whole has been taken into consideration. In the present study, all the four canals (mesiobuccal, mesiolingual, distobuccal, and distolingual) have been compared individually for working length estimation by all the three methods.
Most of the studies on working length determination are either in vitro or had been conducted on teeth indicated for extraction.9,10,12 The present study is an in vivo study and the teeth selected for working length estimation were not extracted.
The digital tactile sense method is still most common method of working length determination. But previous studies conducted by Mello-Moura et al., Mohammed, and Shanmugaraj have shown tactile sense is a less accurate method for root canal working length determination.3,16,17 However, in the current study the working length estimation by the tactile method has been found to be comparable to the apex locator and the conventional radiographic method except in mesiobuccal and mesiolingual canals of permanent teeth (p < 0.5). This was in consistence with a study conducted by Dohaithem et al., which concluded that tactile working length determination in basic root canal treatment results in comparable treatment outcomes in radiographic and clinical aspects compared with standard endodontic treatment with radiographic working length determination.18
Conventional radiographs are needed before, during, and immediately after endodontic treatment and then periodically to evaluate the success or failure of the therapy. Therefore, repeated exposure to dosage of radiations is required. The Root zx apex locator has been used in the present study as it is the most studied apex locator. Various studies have found it to be a reliable method of root canal working length estimation.2,12,16,19,20
In the present study, working length estimation by the Root zx apex locator in all the four canals of primary molars was comparable to tactile and radiographic method and the one-way ANOVA test showed statistically insignificant difference.
The mean of working length of the primary molar mesiobuccal canal obtained with the apex locator was 11.75 mm, which was closer to working length measured by the tactile method (11.73 mm). Working length obtained with the conventional radiograph was 11.35 mm. The standard deviation was more in case of working length estimation by the tactile method (1.48). Intergroup comparison with one-way ANOVA with the Bonferroni test revealed the p value was 1.000 when the tactile method was compared with the apex locator. It was almost similar when comparison was made between the tactile method and the radiographic method and between the apex locator and the radiographic method (0.59 and 0.53, respectively). Thus, the apex locator and the radiographic method were found to be more reliable. Similar results were obtained in other three canals of the teeth.
The mean of working length of the permanent molar mesiobuccal canal obtained with the apex locator was 19.41 mm, which was closer to working length measured by the conventional radiographic method (19.30 mm). Working length obtained with the tactile method was 18.83 mm. The standard deviation was more in case of working length estimation by the tactile method (1.05). Intergroup comparison with one-way ANOVA with the Bonferroni test revealed the p value was 0.05 when the tactile method was compared with the apex locator, which was statistically insignificant. It was 0.16 and 1.000, respectively, when comparison was made between the tactile method and the radiographic method and between the apex locator and the radiographic method. Thus, it can be concluded that the apex locator and radiographs give similar results and the tactile method shows more variation in working length estimation.
In a previous study conducted by Lumnije Kqiku et al., Euiseong Kim et al., KM Nanda Kishor, and Smadino, significant difference was found between the radiographic and electronic root canal working length determination. Studies done by Muthu Shanmugaraj et al., Don H. Pratten et al., and Chougule showed the electronic apex locator was a superior method of working length estimation.
In the present study, the radiographic method of working length determination has been used as standard to compare the other two methods. The results showed that there was no statistically significant difference in the three methods of working length determination. Radiographic verification was considered sufficient to accurately reflect the working length. It is, however, recommended for future investigation to include tooth extraction and sectioning or clearing, with microscopic inspection, to accurately determine the exact relationship between the determined length and the apical constriction. Martínez-Lozano et al. stated that the histological method is the best approach to establish actual working length, i.e., by removing cementum and dentin.
CONCLUSION
Within the limitations of this study, working lengths obtained by the tactile method, the apex locator and the radiographic method were comparable. There was no statistically significant difference among the three methods except in mesiolingual and distobuccal canals of permanent teeth.
Under clinical settings in order to reduce radiation exposure and establish the most accurate working length, it is recommended to establish a tentative working length based on the preoperative radiograph and tactile perception followed by working length estimation by the apex locator, which then should be confirmed by radiograph. If the radiographic method alone is used to establish working length, more than one radiograph may be required to measure the length accurately. The apex locator thus gives an idea of exact working length and reduces the number of radiographs.
Footnotes
Source of support: Nil
Conflict of interest: None
REFERENCES
- 1.Sivadas G, Sudha P, Shenoy R, et al. Accuracy of apex locator for root canal length determination of deciduous molars compared to conventional radiograph. J Interdiscip Dent. 2013;3(3):163–166. doi: 10.4103/2229-5194.131209. DOI: [DOI] [Google Scholar]
- 2.Marín PN, Alonso ZNV, Castañón MGA, et al. Clinical evaluation of the accuracy of conventional radiography and apex locators in primary teeth. Pediatr Dent. 2011;33(1):19–22. [PubMed] [Google Scholar]
- 3.Mello-Moura ACV, Moura-Netto C, Araki AT, et al. Ex vivo performance of five methods for root canal length determination in primary anterior teeth. Int Endod J. 2010;43(2):142–147. doi: 10.1111/j.1365-2591.2009.01667.x. DOI: [DOI] [PubMed] [Google Scholar]
- 4.AAE Glossary of Endodontic Terms. 9th ed.
- 5.Poornima P, Ramchandani G, Neena IE, et al. Accuracy of root ZX apex locator in primary teeth with different root canal irrigants: an in vivo study. Niger J Experimen Clin Biosci. 2015;3(1):24–28. doi: 10.4103/2348-0149.158161. DOI: [DOI] [Google Scholar]
- 6.Nanda Kishor KM. Comparison of working length determination using apex locator, conventional radiography and radiovisiography: an in vitro study. J Contemp Dent Pract. 2012;13(4):550–553. doi: 10.5005/jp-journals-10024-1184. DOI: [DOI] [PubMed] [Google Scholar]
- 7.Mente J, Seidel J, Buchalla W, et al. Electronic determination of root canal length in primary teeth with and without root resorption. Int Endod J. 2002;35(5):447–452. doi: 10.1046/j.1365-2591.2002.00500.x. DOI: [DOI] [PubMed] [Google Scholar]
- 8.Odabaş ME, Bodur H, Tulunoğlu O, et al. Accuracy of an electronic apex locator: a clinical evaluation in primary molars with and without resorption. J Clin Pediatr Dent. 2011;35(3):255–258. doi: 10.17796/jcpd.35.3.7w71656740286960. DOI: [DOI] [PubMed] [Google Scholar]
- 9.Parekh V, Taluja C. Comparative study of periapical radiographic techniques with apex locator for endodontic working length estimation: an ex vivo study. J Contemp Dent Pract. 2011;12(2):131–134. doi: 10.5005/jp-journals-10024-1022. DOI: [DOI] [PubMed] [Google Scholar]
- 10.Fouad AF, Rivera EM, Krell KV. Accuracy of the Endex with variations in canal irrigants and foramen size. J Endod. 1993;19(2):63–67. doi: 10.1016/s0099-2399(06)81196-9. DOI: [DOI] [PubMed] [Google Scholar]
- 11.Leonardo MR, Silva LA, Nelson-Filho P, et al. Ex vivo evaluation of the accuracy of two electronic apex locators during root canal length determination in primary teeth. Int Endod J. 2008;41(4):317–321. doi: 10.1111/j.1365-2591.2007.01366.x. DOI: [DOI] [PubMed] [Google Scholar]
- 12.Ghaemmaghami S, Eberle J, Duperon D. Evaluation of the root ZX apex locator in primary teeth. Pediatr Dent. 2008;30(6):496–498. [PubMed] [Google Scholar]
- 13.Saritha S, Uloopi KS, Vinay C, et al. Clinical evaluation of root ZX II electronic apex locator in primary teeth. Eur Arch Paediatr Dent. 2012;13(1):32–35. doi: 10.1007/BF03262838. DOI: [DOI] [PubMed] [Google Scholar]
- 14.Angwaravong O, Panitvisai P. Accuracy of an electronic apex locator in primary teeth with root resorption. Int Endod J. 2009;42(2):115–121. doi: 10.1111/j.1365-2591.2008.01476.x. DOI: [DOI] [PubMed] [Google Scholar]
- 15.Soruri M, Moeini M, Rekabi S, et al. A clinical comparison of the accuracy of an electronic apex locator (EAL) and radiography in determination of root canal length in primary molars. Am J Res Communi. 2013;1(2):121–128. [Google Scholar]
- 16.Mohammed AG. An in vitro comparison of root canal length measurements in primary teeth. Rafidain Dent J. 2009;9(1):77–82. doi: 10.33899/rden.2009.45385. DOI: [DOI] [Google Scholar]
- 17.Shanmugaraj M, Nivedha R, Mathan R, et al. Evaluation of working length determination methods: an in vivo/ex vivo study. Indian J Dent Res. 2007;18(2):60–62. doi: 10.4103/0970-9290.32421. DOI: [DOI] [PubMed] [Google Scholar]
- 18.Dohaithem AJ, Bakarman EO, Veitz-Keenan A. Tactile working length determination for root canal therapy in underserved settings. Evid Based Dent. 2014;15(2):56–57. doi: 10.1038/sj.ebd.6401029. DOI: [DOI] [PubMed] [Google Scholar]
- 19.Plotino G, Grande NM, Brigante L, et al. Ex vivo accuracy of three electronic apex locators: root ZX, elements diagnostic unit and apex locator and ProPex. Int Endod J. 2006;39(5):408–414. doi: 10.1111/j.1365-2591.2006.01095.x. DOI: [DOI] [PubMed] [Google Scholar]
- 20.Hassanien E, Hashem A, Chalfin H. Histomorphometric study of the root apex of mandibular premolar teeth: an attempt to correlate working length measured with electronic and radiograph methods to various anatomic positions in the apical portion of the canal. J Endod. 2008;34(4):408–412. doi: 10.1016/j.joen.2007.12.013. DOI: [DOI] [PubMed] [Google Scholar]