

Summary:
Implant-based breast reconstruction is a safe and effective option associated with high patient satisfaction. Techniques have evolved significantly over the past several decades, characterized mostly by a reduction in the number of stages and time required to complete reconstruction, with maximal preservation of native breast elements. Nevertheless, both old and new techniques of implant-based breast reconstruction have a role depending on the specific clinical scenario, and thus plastic surgeons should be well versed in the full spectrum of options. This article reviews the key considerations underlying decision-making in implant-based breast reconstruction and the most effective techniques, with a focus on optimizing safety and efficiency.
INTRODUCTION
Implant-based breast reconstruction remains a safe, effective, and popular option for postmastectomy patients. Compared with autologous breast reconstruction, implant-based techniques entail more expedient surgery and recovery without the need for a donor site. Alloplastic breast reconstruction is associated with high degrees of patient satisfaction and health-related quality of life.1 In the United States, there has been a trend toward greater use of implants for breast reconstruction.2
The techniques of implant-based breast reconstruction have advanced significantly over the past several decades. This evolution has been mostly characterized by a reduction in the number of stages and time required to complete reconstruction, with maximal preservation of native breast elements. To this end, technological innovations have been instrumental, particularly the use of acellular dermal matrix (ADM). Nevertheless, both old and new techniques of implant-based breast reconstruction have a role depending on the specific clinical scenario, and thus plastic surgeons should be well versed in the full spectrum of options.
GOALS OF THE PROCEDURE
The objectives of implant-based breast reconstruction are to (1) create a natural and aesthetically pleasing breast; (2) attain symmetry; (3) complete the reconstructive process in the fewest number of procedures and least amount of time; and (4) minimize complications. To accomplish these goals, a number of variables need to be considered, as described next in this section. While this article will later describe 3 of the most effective techniques for implant-based breast reconstruction, it is important to emphasize that a multitude of combinations of these variables is possible, and that an individualized plan should be developed for each patient that considers all factors.
Mastectomy Type and Incisional Design
Preoperatively, the plastic surgeon should confer with the surgical oncologist about the type of mastectomy (traditional, skin-sparing, nipple-sparing), and to design the incision jointly to meet both reconstructive and oncologic needs. Preservation of as much of the native breast skin envelope as possible is preferable over tissue-expanded skin to maximize breast aesthetics. In patients with large breasts and significant ptosis, skin reduction techniques such as Wise pattern are useful.
Nipple-sparing mastectomy (NSM) is an oncologically safe option for many patients that can confer a good aesthetic result while obviating the need for nipple reconstruction.3 Contraindications to NSM include tumor involvement with the nipple or subareolar tissues, and nipple discharge associated with malignancy.4 Risk factors for complications with NSM include obesity, smoking, and a history of radiation therapy.5 In patients at increased risk for complications, surgical delay of the nipple can be beneficial.6,7 While many different types of incisions have been used in NSM, the inframammary incision is associated with lower rates of complications, including nipple necrosis.8,9
Number of Stages
One-stage techniques have the clear advantage of completing the breast reconstruction in a single operation. Optimal candidates for direct-to-implant breast reconstruction are patients with relatively smaller breasts (A-B cup) who wish to achieve a similarly sized reconstructed breast.10 However, single-stage direct-to-implant breast reconstruction may not always be the most appropriate option. Situations where this might be the case include patients in whom perfusion of the mastectomy flaps is a concern, such as due to patient (eg, smoking) or surgical (eg, mastectomy) factors. In these cases, a 2-stage approach utilizing a tissue expander at the initial operation may be advisable to minimize pressure on the flaps by the implant.
Implant Plane
There are 3 possible tissue planes for implant placement: subpectoral, dual-plane (ie, subpectoral and sub-ADM), and prepectoral. Dual-plane and prepectoral techniques both allow for partial intraoperative filling of the expander or immediate insertion of the implant, and thus greater preservation of the native breast skin envelope. The dual-plane approach affords greater soft tissue coverage of the device and may reduce implant rippling and palpability. Prepectoral positioning avoids the possibility of a postoperative animation deformity and may reduce pain and spasm from muscle dissection.11 Subpectoral placement allows for total muscle coverage of a tissue expander without ADM, and may be useful in patients in whom there may be concerns about healing capacity and tissue perfusion.
DESCRIPTION OF MOST-EFFECTIVE PROCEDURES
Total Submuscular Reconstruction
Although one of the earliest and most basic of implant-based techniques, 2-stage total submuscular reconstruction remains an important option in contemporary breast reconstruction. In particular, this approach may be considered in patients at high risk for healing complications. The ability to minimize pressure on the mastectomy flaps and avoid the use of ADM as an additional foreign body may be prudent in patients with diabetes, smokers, or tenuous mastectomy flaps. This is also the approach that is necessary in most cases of delayed reconstruction cases, where the preoperative chest wall contour is flat.
In the first-stage, the tissue expander is placed beneath 3 musculofascial structures (Fig. 1). Typically, the subpectoral plane is developed first, and then this dissection is continued inferiorly in a submuscular plane beneath the anterior rectus sheath to the level of the inframammary fold as one contiguous plane. In some cases, individual patient anatomy may preclude continuing the subpectoral plane inferiorly contiguous with the anterior rectus sheath, in which case a dual-plane approach (described below) may be necessary. Laterally, the serratus anterior muscle or fascia is then elevated to complete creation of the expander pocket. After irrigation and hemostasis, the tissue expander is inserted, and the pectoralis major and serratus anterior muscle/fascia are approximated to achieve total submuscular coverage of the device (Fig. 2). Intraoperative expansion is then performed while directly assessing the tension on the muscle closure and skin flaps. Approximately 10–14 days later, postoperative expansion is resumed.
Fig. 1.
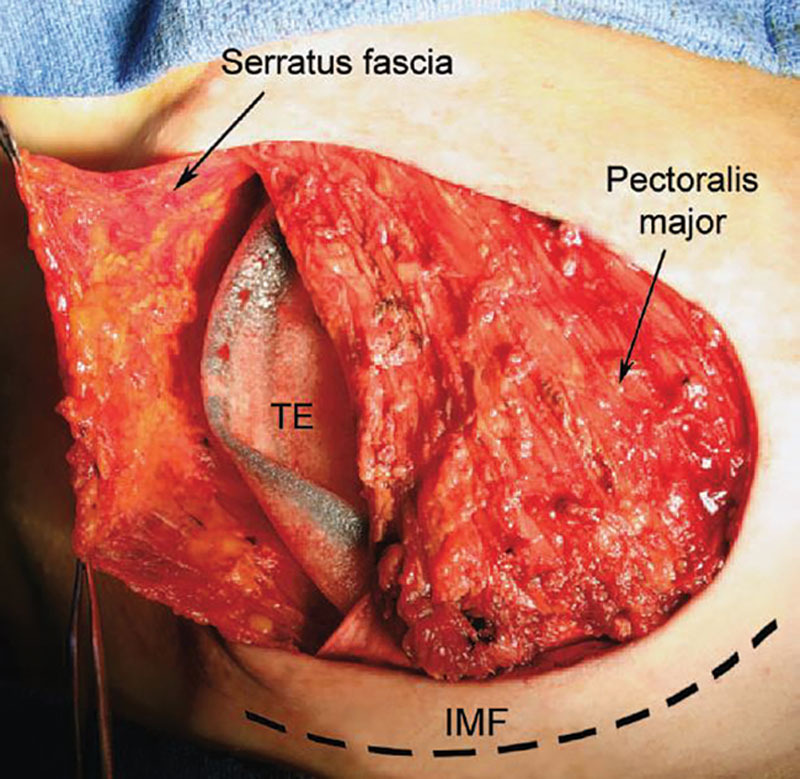
Intraoperative photograph demonstrating tissue expander placement beneath the pectoralis major muscle and the serratus anterior fascia. IMF, inframammary fold; TE, tissue expander. Adapted with permission from Plast Reconstr Surg. 2010;125:1057–1064.
Fig. 2.
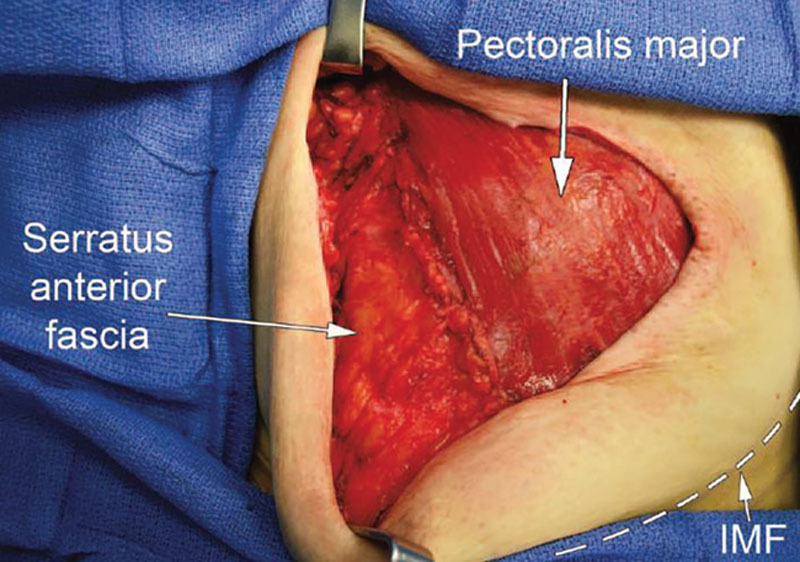
Intraoperative photograph demonstrating inset of the anterior border of the serratus anterior fascia to the lateral border of the pectoralis major muscle to achieve total coverage of the tissue expander. IMF, inframammary fold. Adapted with permission from Plast Reconstr Surg. 2010;125:1057–1064.
At the second stage, the tissue expander is exchanged for the permanent prosthesis. During this operation, capsule work is often performed to adjust breast shape and position. Capsulotomies are generally performed in locations where one desires proportionately a greater implant volume. For example, if performed along the inferior pole, there will be descent of the implant and greater ptosis. Capsulotomies can be performed both radially and longitudinally depending on the desired effect, taking into account that additional tissue stretching will occur postoperatively. In some cases, partial or total capsulectomy may be necessary. For example, capsule modifications performed inferiorly can help increase ptosis. The use of implant sizers is helpful to select the most appropriate implant and the adequacy of capsule modifications. Both saline and silicone implants are safe and effective, although silicone implants are associated with higher patient satisfaction.1,12 In unilateral cases, symmetry procedures on the contralateral breast are usually performed at this time. When assessing the result intraoperatively, it is essential to sit the patient up and adduct the arms before making final decisions about implant selection and inset. Fat grafting can be a useful adjunct to optimize the aesthetic outcome to address contour deformities. However, since fat grafts require a well-vascularized recipient site, they generally should not be placed at the time of the mastectomy or concurrent with capsule work.
Dual-plane Direct-to-implant Reconstruction
Dual-plane direct-to-implant reconstruction (DP-DTI) entails placement of the implant within a combined subpectoral and sub-ADM pocket. A strength of this approach is the ability to complete the reconstruction in a single-stage, while maintaining similar rates of revision and complications as well as patient-reported outcomes compared with tissue expander/implant reconstruction.13,14 Optimal candidates for DP-DTI reconstruction are patients with relatively smaller breasts who wish to maintain the same size.10,15 In addition, it is best performed in patients who demonstrate well-perfused mastectomy flaps because ADM is fundamentally a graft that relies on revascularization by the overlying tissues. Thus, patients who are diabetic, smoke, or who have a history of radiation therapy are generally not suitable candidates.
Elevation in a subpectoral plane is initiated with disinsertion of the muscle inferiorly. ADM is then shaped to bridge the inferior border of the pectoralis muscle with the inframammary fold inferiorly, and the lateral border of the pectoralis muscle with the outer curvature of the breast laterally (Fig. 3). The vertical and horizontal dimensions of the ADM should be designed to take into account the overlying skin envelope and desired amount of ptosis. Achieving a smooth contour to the ADM, meshing or use of a perforated variety of ADM, and drain placement are important measures to facilitate graft take. Partial inset of the ADM to the chest wall is then performed, most commonly along its inferior and lateral aspects to provide ready access to the pocket centrally for subsequent implant placement. At this point, sizers and mastectomy specimen weight are used to help select the implant. After irrigation and hemostasis, the implant is inserted and the superior aspect of the ADM is approximated to the inferior and lateral borders of the pectoralis muscle to close the implant pocket. In unilateral cases, symmetry procedures on the contralateral breast are usually performed at this time. If necessary, DP-DTI can be converted intraoperatively to a 2-stage reconstruction using a tissue expander, which is then managed postoperatively similar to total submuscular reconstruction. Doing so can relieve pressure on the mastectomy flaps, although this may not necessarily accelerate the rate of expansion compared with total submuscular tissue expander placement.16
Fig. 3.
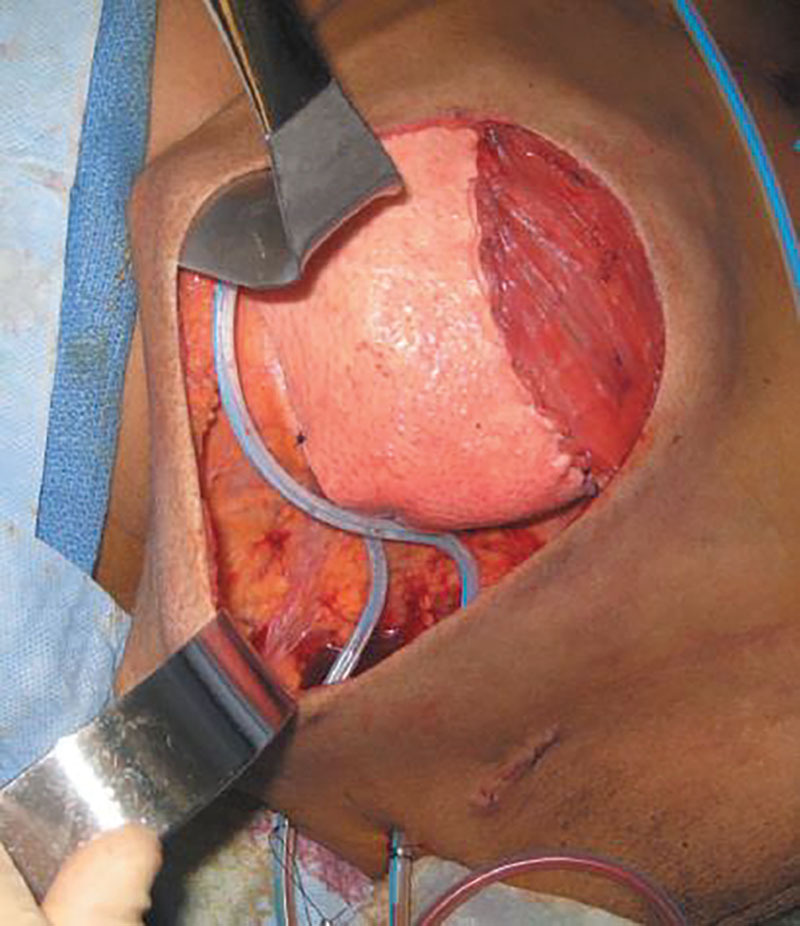
Intraoperative photograph demonstrating dual-plane implant placement beneath the pectoralis major muscle and ADM. Adapted with permission from Plast Reconstr Surg. 2012;130:44S–53S.
Two-stage Prepectoral Reconstruction
The modern-day technique of prepectoral breast reconstruction involves placement of the device entirely beneath a sub-ADM plane, which in turn is located subcutaneously. The use of ADM is advisable to provide support, control position, and to potentially reduce the risk of capsular contracture.17 This approach has gained popularity relatively recently over the past few years.18,19 While recent reports of prepectoral direct-to-implant reconstruction are promising, a 2-stage approach affords greater control over implant position and mastectomy flap perfusion.20,21 Optimal candidates for prepectoral reconstruction have well perfused and suitably thick mastectomy flaps, which can help minimize rippling and palpability.
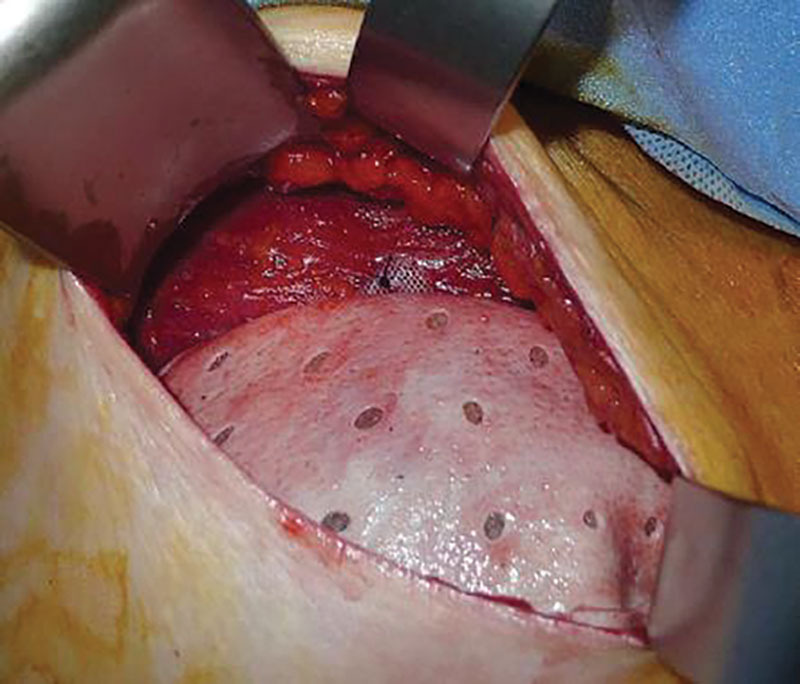
The key initial step in prepectoral reconstruction is creation of a subcutaneous implant pocket that has a hand-in-glove fit. This is critical to optimize the aesthetic outcome, including a smooth contour to the breast, as well as to maximize contact between the mastectomy flaps and the ADM. In this regard, anatomic landmarks such as the inframammary fold should be reconstructed, redundant mastectomy flaps revised, and a prosthesis with appropriate dimensions selected. Next, ADM is shaped to envelop the anterior surface of the tissue expander or implant (Fig. 4). Like with DP-DTI, achieving a smooth contour to the ADM, meshing or use of a perforated variety of ADM, and drain placement are important measures to facilitate graft take. After irrigation and hemostasis, the tissue expander (preferably a tabbed variety that can be positionally secured) or implant is inserted. The previously prepared ADM is then inset circumferentially around the device to the chest wall to help control its subcutaneous position (Fig. 5). In direct-to-implant cases, some authors have sutured the ADM to itself along the posterior aspect of the implant, and then inserted the ADM and implant as a single apparatus. This approach facilitates device placement, but entails greater reliance on the pocket to control position.22 When a 2-stage approach is taken, postoperative expansion and eventual implant exchange are performed as described for total submuscular reconstruction.
Fig. 4.
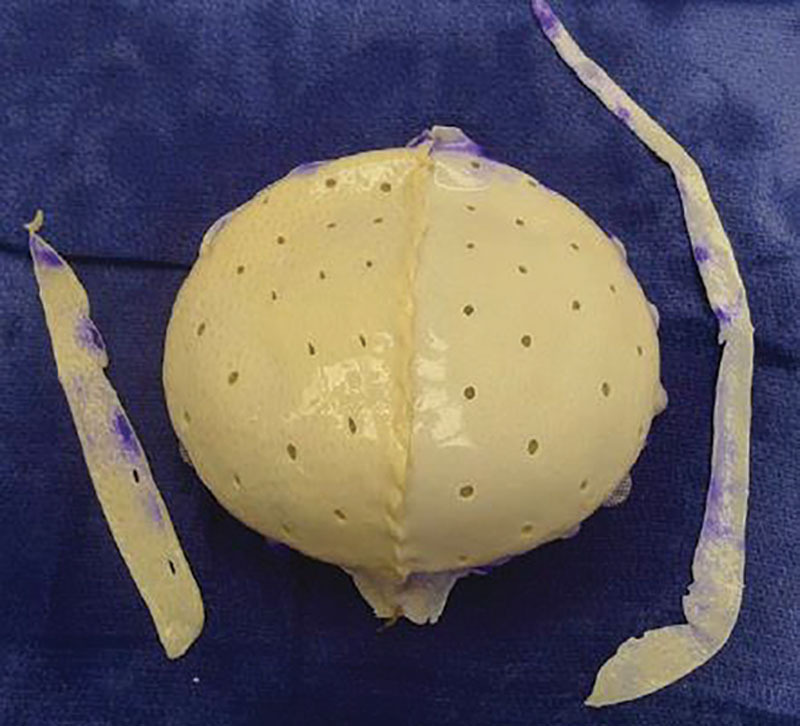
Two sheets of ADM are draped over the tissue expander to achieve a smooth contour. Adapted with permission from Plast Reconstr Surg. 2017;140:51S–59S.
Fig. 5.
The tissue expander position is secured by utilizing its suture tabs to the underlying pectoralis major muscle. Adapted with permission from Plast Reconstr Surg. 2017;140:51S–59S.
AVOIDING AND MANAGING MOST-DANGEROUS COMPLICATIONS
Infection
One of the most potentially impactful complications in implant-based breast reconstruction is infection. Since salvage is not always possible, infection can be a source of overall reconstructive failure. A key component of infection prevention is proper preparation of the surgical field and pocket before tissue expander and implant placement. Before insertion of the device, the pocket should be thoroughly irrigated, the skin cleansed with povidone-iodine solution, and new surgical gloves donned. The device should be minimally handled during placement, and at that juncture it is advisable to use only surgical instruments not used earlier in the case. Standardized protocols that incorporate these elements have been described and found to reduce the risk of infection.23 Judicious drain placement is also recommended to prevent fluid collections that can serve as a nidus for infection. Existing evidence does not support the routine use of postoperative prophylactic antibiotics.24,25
Salvage of an infected prosthesis is possible in some cases. A multitude of management approaches have been described that include varying combinations of antibiotic therapy, radiologic drain placement, capsule curettage, capsulectomy, device exchange, and continuous antibiotic irrigation.26 However, it is debated as to which of these interventions should be performed and precisely when to maximize the likelihood of successful salvage. Nevertheless, there are general principles that should be followed. First, the earlier infection is identified and addressed, the higher the likelihood of salvage. In this regard, it is important to educate patients on the signs and symptoms of infection. Second, initial management should consist of broad spectrum antibiotic therapy that covers the most common causative organisms, namely Staphylococcus epidermidis, S. aureus, Escherichia coli, Pseudomonas aeruginosa, Propionibacterium, and Corynebacterium.27 Institutional antibiograms can aid antibiotic selection based on sensitivities of local microbiomes.28 Patients should be followed closely to assess the response to antibiotic therapy, and if inadequate then surgical intervention is undertaken. Third, thorough evaluation (including intraoperative gram stain), irrigation, and debridement of involved tissues should be performed before making a decision about whether to attempt salvage of the reconstruction with device exchange. In patients who ultimately require tissue expander explantation, a second attempt at implant-based reconstruction is usually successful (79%).29
Exposure
Another potential source of reconstructive failure is device exposure. Like with infection, prevention is critical because once a prosthesis is exposed it is often unsalvageable. Exposure can occur both through sites of mastectomy flap necrosis or the incision itself. At the time of the breast reconstruction procedure, a thorough assessment of the thickness and perfusion of the flaps should be performed. Use of a tissue expander filled conservatively with air, or not at all, can help reduce pressure on the incision and mastectomy flaps when they may be marginal. If air is used, saline exchange is subsequently performed in the clinic at an appropriate time based on clinical assessment. Total submuscular reconstruction or delayed reconstruction should be considered when there are greater concerns about soft tissue coverage.
Breast Implant-associated Anaplastic Large Cell Lymphoma
Breast-implant–associated anaplastic large cell lymphoma (BIA-ALCL) is a form of lymphoma that can occur secondary to textured breast implants. The lifetime risk of developing BIA-ALCL is estimated to be approximately 1 in 2200 to 86,000.30 Although rare, it is a potentially fatal condition, but readily treatable if identified and managed appropriately. Patients with BIA-ALCL most often present with breast asymmetry, mass, pain, or skin changes more than 1 year after placement of the implant. Patients with these signs and symptoms should be initially evaluated with ultrasound of the breast and regional lymph node basins.31 If an effusion or mass is seen, fluid or tissue sampling should be performed, with cytology, histology, flow cytometry, and CD30 immunohistochemistry. A confirmed diagnosis of BIA-ALCL is most appropriately managed through a multidisciplinary approach. The surgical component of treatment generally consists of explantation and total capsulectomy. Immediate reconstruction should only be considered for disease that is confined to the capsule on preoperative positive emission tomography/computed tomography scan.32
There is currently no evidence that a difference in aesthetic outcome exists between textured anatomic implants and smooth round implants in breast reconstruction.33,34 In this regard, and since a variety of cohesivity levels are widely available with smooth devices, it may be prudent for plastic surgeons to utilize implants with smooth shells, which can produce excellent aesthetic results while eliminating the potential risk for BIA-ALCL.
PEARLS AND PITFALLS
Thorough assessment of the mastectomy flaps intraoperatively should be performed before committing to a particular technique. Preoperatively, patients should be counseled on the possibility of a change in plan as to the specific type of implant-based reconstruction that is ultimately performed. Fluorescent angiography performed both before and after implant sizer placement can aid in decision-making. When limited areas of the mastectomy flaps appear compromised, preemptive excision and closure within the controlled setting conferred by the operating room can be helpful.
Radiation therapy can adversely affect the outcomes of implant-based breast reconstruction, which can result in fibrosis, diminished vascularity and healing capacity, capsular contracture, and even reconstructive failure. These effects can be mitigated through careful planning. In patients undergoing tissue expander/implant reconstruction who will receive adjuvant radiation therapy, there are 2 reconstructive timelines to consider: implant exchange before radiation therapy versus subsequent to radiation therapy. Performing implant exchange before radiation therapy is generally feasible only if the patient will also be receiving adjuvant chemotherapy during which the expansion process can be completed. In this scenario, implant exchange is performed approximately 4 weeks after chemotherapy and 4 weeks before radiation therapy. This approach is associated with a lower risk of reconstructive failure (16% risk of explantation) but a higher incidence of capsular contracture compared with implant exchange after radiation therapy (32% risk of explantation).35 When implant exchange is performed after radiation therapy, it is advisable to wait at least 6 months to allow radiation effects to subside. In these cases, conservative implant sizing and capsule work may be prudent. Both timing strategies are associated with similar patient-reported outcomes.
WHAT PATIENTS SHOULD KNOW BEFORE HAVING THIS PROCEDURE
Implant-based breast reconstruction is a safe and effective procedure that is associated with high patient satisfaction. Although a 1-stage approach may be preferable, this may not always be feasible, including because of findings that only become evident during the surgery itself. Multiple surgical procedures, including to revise an existing reconstruction, may be necessary to achieve the best result. In addition, breast implants may not remain intact for the entirety of a patient’s lifetime. While implants can generally be expected to maintain their integrity for over a decade, additional surgery may be indicated in the distant future to replace a ruptured implant.36 Lastly, adjuvant therapies, specifically radiation therapy, can adversely affect the outcomes of implant-based breast reconstruction and increase the likelihood of loss of the implant.37–39
Footnotes
Published online 24 September 2020.
Disclosure: The author has no financial interest to declare in relation to the content of this article.
REFERENCES
- 1.Macadam SA, Ho AL, Cook EF, Jr, et al. Patient satisfaction and health-related quality of life following breast reconstruction: patient-reported outcomes among saline and silicone implant recipients. Plast Reconstr Surg. 2010;125:761. [DOI] [PubMed] [Google Scholar]
- 2.Albornoz CR, Bach PB, Mehrara BJ, et al. A paradigm shift in U.S. Breast reconstruction: increasing implant rates. Plast Reconstr Surg. 2013;131:15–23. [DOI] [PubMed] [Google Scholar]
- 3.Margenthaler JA, Gan C, Yan Y, et al. Oncologic safety and outcomes in patients undergoing nipple-sparing mastectomy. J Am Coll Surg. 2020;230:535–541. [DOI] [PubMed] [Google Scholar]
- 4.National Comprehensive Cancer Network (NCCN). NCCN clinical practice guidelines in oncology: breast cancer. Available at https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf. Accessed June 29, 2020.
- 5.Colwell AS, Tessler O, Lin AM, et al. Breast reconstruction following nipple-sparing mastectomy: predictors of complications, reconstruction outcomes, and 5-year trends. Plast Reconstr Surg. 2014;133:496–506. [DOI] [PubMed] [Google Scholar]
- 6.Karian LS, Therattil PJ, Wey PD, et al. Delay techniques for nipple-sparing mastectomy: a systematic review. J Plast Reconstr Aesthet Surg. 2017;70:236–242. [DOI] [PubMed] [Google Scholar]
- 7.Bertoni DM, Nguyen D, Rochlin D, et al. Protecting nipple perfusion by devascularization and surgical delay in patients at risk for ischemic complications during nipple-sparing mastectomies. Ann Surg Oncol. 2016;23:2665–2672. [DOI] [PubMed] [Google Scholar]
- 8.Daar DA, Abdou SA, Rosario L, et al. Is there a preferred incision location for nipple-sparing mastectomy? A systematic review and meta-analysis. Plast Reconstr Surg. 2019;143:906e–919e. [DOI] [PubMed] [Google Scholar]
- 9.Frey JD, Salibian AA, Levine JP, et al. Incision choices in nipple-sparing mastectomy: a comparative analysis of outcomes and evolution of a clinical algorithm. Plast Reconstr Surg. 2018;142:826e–835e. [DOI] [PubMed] [Google Scholar]
- 10.Gdalevitch P, Ho A, Genoway K, et al. Direct-to-implant single-stage immediate breast reconstruction with acellular dermal matrix: predictors of failure. Plast Reconstr Surg. 2014;133:738e–747e. [DOI] [PubMed] [Google Scholar]
- 11.Nahabedian MY.Current approaches to prepectoral breast reconstruction. Plast Reconstr Surg. 2018;142:871–880. [DOI] [PubMed] [Google Scholar]
- 12.McCarthy CM, Klassen AF, Cano SJ, et al. Patient satisfaction with postmastectomy breast reconstruction: a comparison of saline and silicone implants. Cancer. 2010;116:5584–5591. [DOI] [PubMed] [Google Scholar]
- 13.Clarke-Pearson EM, Lin AM, Hertl C, et al. Revisions in implant-based breast reconstruction: how does direct-to-implant measure up? Plast Reconstr Surg. 2016;137:1690–1699. [DOI] [PubMed] [Google Scholar]
- 14.Srinivasa DR, Garvey PB, Qi J, et al. Direct-to-implant versus two-stage tissue expander/implant reconstruction: 2-year risks and patient-reported outcomes from a prospective, multicenter study. Plast Reconstr Surg. 2017;140:869–877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Basta MN, Gerety PA, Serletti JM, et al. A systematic review and head-to-head meta-analysis of outcomes following direct-to-implant versus conventional two-stage implant reconstruction. Plast Reconstr Surg. 2015;136:1135–1144. [DOI] [PubMed] [Google Scholar]
- 16.McCarthy CM, Lee CN, Halvorson EG, et al. The use of acellular dermal matrices in two-stage expander/implant reconstruction: a multicenter, blinded, randomized controlled trial. Plast Reconstr Surg. 2012;1305 suppl 257S–66S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Basu CB, Jeffers L.The role of acellular dermal matrices in capsular contracture: a review of the evidence. Plast Reconstr Surg. 2012;1305 suppl 2118S–124S. [DOI] [PubMed] [Google Scholar]
- 18.Sigalove S, Maxwell GP, Sigalove NM, et al. Prepectoral implant-based breast reconstruction: rationale, indications, and preliminary results. Plast Reconstr Surg. 2017;139:287–294. [DOI] [PubMed] [Google Scholar]
- 19.Ter Louw RP, Nahabedian MY.Prepectoral breast reconstruction. Plast Reconstr Surg. 2017;1405S Advances in Breast Reconstruction51S–59S. [DOI] [PubMed] [Google Scholar]
- 20.Nahabedian MY, Cocilovo C.Two-stage prosthetic breast reconstruction: a comparison between prepectoral and partial subpectoral techniques. Plast Reconstr Surg. 2017;1406S Prepectoral Breast Reconstruction22S–30S. [DOI] [PubMed] [Google Scholar]
- 21.Nealon KP, Weitzman RE, Sobti N, et al. Prepectoral direct-to-implant breast reconstruction: safety outcome endpoints and delineation of risk factors. Plast Reconstr Surg. 2020;145:898e–908e. [DOI] [PubMed] [Google Scholar]
- 22.Safran T, Al-Halabi B, Viezel-Mathieu A, et al. Direct-to-implant, prepectoral breast reconstruction: a single-surgeon experience with 201 consecutive patients. Plast Reconstr Surg. 2020;145:686e–696e. [DOI] [PubMed] [Google Scholar]
- 23.Khansa I, Hendrick RG, Jr, Shore A, et al. Breast reconstruction with tissue expanders: implementation of a standardized best-practices protocol to reduce infection rates. Plast Reconstr Surg. 2014;134:11–18. [DOI] [PubMed] [Google Scholar]
- 24.Ranganathan K, Sears ED, Zhong L, et al. Antibiotic prophylaxis after immediate breast reconstruction: the reality of its efficacy. Plast Reconstr Surg. 2018;141:865–877. [DOI] [PubMed] [Google Scholar]
- 25.Wang F, Chin R, Piper M, et al. Do prolonged prophylactic antibiotics reduce the incidence of surgical-site infections in immediate prosthetic breast reconstruction? Plast Reconstr Surg. 2016;138:1141–1149. [DOI] [PubMed] [Google Scholar]
- 26.Reish RG, Damjanovic B, Austen WG, Jr, et al. Infection following implant-based reconstruction in 1952 consecutive breast reconstructions: salvage rates and predictors of success. Plast Reconstr Surg. 2013;131:1223–1230. [DOI] [PubMed] [Google Scholar]
- 27.Ahn CY, Ko CY, Wagar EA, et al. Microbial evaluation: 139 implants removed from symptomatic patients. Plast Reconstr Surg. 1996;98:1225–1229. [DOI] [PubMed] [Google Scholar]
- 28.Cohen JB, Carroll C, Tenenbaum MM, et al. Breast implant-associated infections: the role of the national surgical quality improvement program and the local microbiome. Plast Reconstr Surg. 2015;136:921–929. [DOI] [PubMed] [Google Scholar]
- 29.Poppler LH, Mundschenk MB, Linkugel A, et al. Tissue expander complications do not preclude a second successful implant-based breast reconstruction. Plast Reconstr Surg. 2019;143:24–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.American Society of Plastic Surgeons. Breast implant associated anaplastic large cell lymphoma (BIA-ALCL). Available at https://www.plasticsurgery.org/patient-safety/breast-implant-safety/bia-alcl-summary. Accessed May 31, 2020.
- 31.Clemens MW, Brody GS, Mahabir RC, et al. How to diagnose and treat breast implant-associated anaplastic large cell lymphoma. Plast Reconstr Surg. 2018;141:586e–599e. [DOI] [PubMed] [Google Scholar]
- 32.Lamaris GA, Butler CE, Deva AK, et al. Breast reconstruction following breast implant-associated anaplastic large cell lymphoma. Plast Reconstr Surg. 2019;1433S A Review of Breast Implant-Associated Anaplastic Large Cell Lymphoma51S–58S. [DOI] [PubMed] [Google Scholar]
- 33.Agochukwu-Nwubah N, Boustany A, Wetzel M, et al. Anatomic implants in breast reconstruction: a comparison of outcomes and aesthetic results compared to smooth round silicone implants. Aesthet Surg J. 2019;39:NP322–NP330. [DOI] [PubMed] [Google Scholar]
- 34.Unger JG, Keller PR.Tradeoffs in implant selection for reconstructive surgery and adjuncts utilized to maximize aesthetic outcomes. Plast Reconstr Surg. 2019;1441S Utilizing a Spectrum of Cohesive Implants in Aesthetic and Reconstructive Breast Surgery51S–59S. [DOI] [PubMed] [Google Scholar]
- 35.Cordeiro PG, Albornoz CR, McCormick B, et al. What is the optimum timing of postmastectomy radiotherapy in two-stage prosthetic reconstruction: radiation to the tissue expander or permanent implant? Plast Reconstr Surg. 2015;135:1509–1517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.American Society of Plastic Surgeons. What is the lifespan of breast implants? Available at https://www.plasticsurgery.org/news/blog/what-is-the-lifespan-of-breast-implants. Accessed June 29, 2020.
- 37.Alderman A, Gutowski K, Ahuja A, et al. Postmastectomy Expander Implant Breast Reconstruction Guideline Work Group. ASPS clinical practice guideline summary on breast reconstruction with expanders and implants. Plast Reconstr Surg. 2014;134:648e–655e. [DOI] [PubMed] [Google Scholar]
- 38.Lam TC, Borotkanics R, Hsieh F, et al. Immediate two-stage prosthetic breast reconstruction failure: radiation is not the only culprit. Plast Reconstr Surg. 2018;141:1315–1324. [DOI] [PubMed] [Google Scholar]
- 39.Schneider LF, Mehrara BJ.De-mythifying breast reconstruction: a review of common misconceptions about breast reconstruction. J Am Coll Surg. 2015;220:353–361. [DOI] [PubMed] [Google Scholar]