

Abstract
Radical cystectomy is considered the standard treatment for patients with muscle-invasive bladder tumors and has high postoperative complication rates among urological surgeries. High-risk patients, defined as those ≥45 years of age with history of coronary artery disease, stroke, or peripheral artery disease or those ≥65 years of age, can have a higher incidence of cardiac complications. Therefore, we evaluated the incidence, risk factors, and outcomes of myocardial injury after non-cardiac surgery (MINS) in high-risk patients who underwent radical cystectomy.
This retrospective observational study analyzed 248 high-risk patients who underwent radical cystectomy. MINS was defined as serum troponin I concentration ≥0.04 mg/L within postoperative 3 days. The risk factors for MINS were evaluated by multivariate logistic regression analysis. Postoperative outcomes were evaluated. The 1-year survival after radical cystectomy was also compared between patients who developed MINS (MINS group) and those who did not (non-MINS group) by Kaplan–Meier analysis.
MINS occurred in 35 patients (14.1%). Multivariate logistic regression analysis showed that early diastolic transmitral filling velocity (E)/early diastolic septal mitral annular velocity (E’) ratio (odds ratio = 1.102, 95% confidence interval [1.009–1.203], P = .031) and large volume blood transfusion (odds ratio = 2.745, 95% confidence interval [1.131–6.664], P = .026) were significantly associated with MINS in high-risk patients who underwent radical cystectomy. Major adverse cardiac events and 1-year mortality were significantly higher in the MINS group than in the non-MINS group (17.1% vs 6.1%, P = .035; 28.6% vs 12.7%, P = .021, respectively). Kaplan–Meier analysis showed significantly lower 1-year survival in the MINS group than in the non-MINS group (P = .010).
MINS occurred in 14.1% of patients. High E/E’ ratio and large volume blood transfusion were risk factors for MINS in high-risk patients who underwent radical cystectomy. Postoperative major adverse cardiac events and 1-year mortality were significantly higher in the MINS group than in the non-MINS group. Preoperative evaluation of risk factors for MINS may provide useful information to detect cardiovascular complications after radical cystectomy in high-risk patients.
Keywords: high-risk patients, myocardial injury after non-cardiac surgery, radical cystectomy
1. Introduction
Radical cystectomy is considered the standard treatment for patients with muscle-invasive bladder tumors.[1] This major abdominal surgery has high postoperative complication rates in the range of 28% to 64% among urological surgeries.[2] Due to the nature of bladder cancer, radical cystectomy is usually performed in elderly patients who have multiple comorbidities.[3,4] Older patients with multiple comorbidities have a significantly higher incidence of complications after radical cystectomy.[3] Importantly, high-risk patients such as those ≥45 years of age with a history of coronary artery disease, stroke, or peripheral artery disease or those ≥65 years of age are associated with short- and long-term mortality in non-cardiac surgery.[5] Therefore, meticulous care and attention should be given during anesthesia and surgical procedures to such high-risk patients during the perioperative period of radical cystectomy.
Myocardial injury after non-cardiac surgery (MINS) is an emerging issue that results in increased morbidity, mortality, and hospital costs.[5] Cardiac complication is a common postoperative complication after radical cystectomy.[6,7] However, typical cardiac ischemic symptoms such as chest pain or discomfort may be obscured in the postoperative period due to postoperative pain management. MINS, defined as a serum troponin I concentration ≥0.04 mg/L within postoperative 3 days,[8] can be easily diagnosed based on elevated troponin level. The reported incidence of MINS after major abdominal surgery is around 10%.[9,10] The incidence of MINS is higher in older patients (over 70 years of age) or those with a history of cardiovascular disease than in the general population in cases of open major vascular surgery.[11] Therefore, it is important to detect MINS early to reduce morbidity and mortality in high-risk patients. However, to the best of our knowledge, no previous studies have investigated MINS in high-risk cystectomy patients.
We hypothesized that perioperative factors might affect MINS in radical cystectomy. Therefore, we assessed the incidence and risk factors of MINS in high-risk patients who underwent radical cystectomy. We also compared postoperative outcomes between high-risk patients who developed MINS (MINS group) and those who did not (non-MINS group).
2. Methods
2.1. Patients
We retrospectively reviewed consecutive patients who underwent open radical cystectomy due to bladder cancer at Asan Medical Center in Seoul, Republic of Korea, between January 2007 and February 2019. We included high-risk patients, defined as those ≥45 years of age with a history of coronary artery disease, stroke, or peripheral artery disease or those ≥65 years of age.[5] We excluded patients without troponin I measurements and those who underwent radical cystectomy combined with other surgeries. The study was approved by the Institutional Review Board of Asan Medical Center (approval no. 2020-0410), which waived the requirement for written informed consent.
2.2. Perioperative protocol
No patients were administered premedication. Anticoagulant agents were discontinued according to the standard protocol before radical cystectomy.[12,13] General anesthesia was performed according to our institutional standards for radical cystectomy.[14–16] Anesthesia was induced with propofol or thiopental sodium and rocuronium and was maintained with sevoflurane. The concentration of sevoflurane was set to maintain a bispectral index of 40 to 60. The administration of fluids and vasopressors or inotropic agents was performed to maintain a mean arterial blood pressure of above 65 mm Hg. The heart rate was maintained at 60 to 100 beats/min. Hemodynamic changes in high-risk patients were minimized by close perioperative monitoring. Crystalloids such as lactated Ringer's solution or plasma solution A (CJ Pharmaceutical, Seoul, Korea) and colloids such as 6% hydroxyethyl starch or 5% albumin were used for fluid administration. Ephedrine, phenylephrine, or norepinephrine were used as vasopressors or inotropic agents. Red blood cells (RBCs) were transfused when the hemoglobin concentration was <8 g/dL. A neostigmine-glycopyrrolate mixture or sugammadex was used to reverse neuromuscular blockade at the discretion of the anesthesiologist. Patient-controlled intravenous analgesia based on fentanyl was used to manage postoperative pain. Based on anesthesiologist and urologist determination, the evaluation of coronary artery disease-related symptoms, troponin I measurement, and electrocardiogram monitoring were performed after radical cystectomy.
Radical cystectomy with standard or extended pelvic lymphadenectomy was performed according to our institutional management protocol.[17,18] Standard pelvic lymph node dissection included the distal common iliac, external iliac, internal iliac, obturator, and perivesical lymph nodes. Extended lymph node dissection included the lymph nodes extending to the proximal common iliac artery, distal aorta, and inferior vena cava. Urinary diversion (ileal neobladder or ileal conduit) was subsequently performed according to the urologist's judgment. Ileal neobladder reconstruction was performed as follows: Depending on the type of neobladder, a specific length of the distal ileum (15–20 cm from the ileocecal valve) was harvested to create an orthotopic continent diversion (ileal neobladder). Continuity of the remnant bowel was re-established by ileo-ileostomy. Ileal conduit reconstruction was performed as follows: An ileal segment 20 cm in length was harvested, sparing the distal 15 cm of the ileum, and the remaining ileal segment was re-anastomosed. Both ureters were implanted in the conduit. The stoma was formed at the selected site on the surface of the abdomen. Five highly experienced surgeons performed all the surgeries.
2.3. Definition of MINS and measurement of troponin I
MINS was defined as serum troponin I concentration ≥0.04 mg/L within postoperative 3 days.[8] Postoperative troponin I measurement was planned before surgery according to patient characteristics or was determined during surgery in case of the occurrence of specific events such as electrocardiogram change, hemodynamic instability, and a large volume of blood loss. Serum troponin was measured daily on postoperative days 0 and 1 for all high-risk patients and repeatedly from postoperative day 2 for patients with abnormal serum troponin levels.
2.4. Data collection and definitions
Data on patient demographics and clinical characteristics were collected, including sex; age; body mass index; American Society of Anesthesiologists Physical Status; comorbidities (diabetes mellitus, hypertension, atrial fibrillation, coronary artery disease, cerebrovascular disease, chronic obstructive pulmonary disease, end-stage renal disease, and number of associated comorbidities); tumor T, N, and M stages; tumor grade; tumor pathology; neoadjuvant chemotherapy; preoperative laboratory tests (white blood cell count, hemoglobin concentration, platelet count, and serum albumin, creatinine, sodium, potassium, chloride, uric acid, and glucose levels); preoperative transthoracic echocardiography parameters (left ventricular end-diastolic volume; left ventricular ejection fraction; mitral deceleration time; early diastolic septal mitral annular velocity (E’); late diastolic septal mitral annular velocity (A’); systolic septal mitral annular velocity (S’); early diastolic transmitral filling velocity (E); late diastolic transmitral filling velocity (A); E/A ratio, E/E’ ratio; valvulopathies including aortic regurgitation, aortic stenosis, mitral regurgitation, and tricuspid regurgitation; and study period.
Tumor stage was defined according to the 2010 American Joint Committee on Cancer tumor-node-metastasis staging system.[19] Tumor grade was defined according to the 2016 World Health Organization grading system.[20] Neoadjuvant chemotherapy was applied with one of the following combinations: gemcitabine and carboplatin; gemcitabine and cisplatin; methotrexate and vinblastine; or sulfate, cisplatin, and doxorubicin. The study duration was divided into period 1 (January 2007 to December 2012) and period 2 (January 2013 to February 2019).
Intraoperative and postoperative data included anesthesia and operation durations, crystalloid and colloid amounts, RBC transfusion rate, RBC transfusion amount, large volume blood transfusion, intraoperative hypotension, agent used to reverse neuromuscular blockade, urethrectomy, urinary diversion type, and adjuvant chemotherapy. Large volume blood transfusion was defined as an intraoperative transfusion of four or more units of RBCs.[21] Intraoperative hypotension was defined as a mean arterial blood pressure <65 mm Hg for >5 minutes noted in the intraoperative anesthesia records.[23] Postoperative outcomes included acute kidney injury (AKI), hospital stay duration (from surgery to discharge), intensive care unit (ICU) admission rate, ICU stay duration, major adverse cardiac events (MACEs), and 1-year mortality. AKI was defined by applying the Kidney Disease: Improving Global Outcomes criteria.[22] Postoperative MACEs were defined according to the European Perioperative Clinical Outcome definitions[24] and were recorded if a patient had one or more of the following complications within 6 months after radical cystectomy: arrhythmia, nonfatal cardiac arrest, acute myocardial infarction, heart failure, or cerebrovascular accident.
2.5. Statistical analysis
Categorical variables were examined by chi-square or Fisher exact tests, and continuous variables were examined by Student t- or Mann–Whitney U-test between the MINS and non-MINS groups. Categorical variables are expressed as number (percentage), and continuous variables as mean ± standard deviation. Univariate and multivariate logistic regression analyses were performed to identify independent risk factors for MINS in high-risk patients who underwent radical cystectomy. The most relevant factors associated with MINS in radical cystectomy were included in the univariate logistic regression analysis. Multivariate logistic regression analysis using the backward conditional method was performed for all factors with P <.05 in the univariate logistic regression analyses. To estimate multicollinearity, the variance inflation factor was calculated before performing multivariate logistic regression analyses. Multicollinearity was considered to be present if the variance inflation factor was above 10. To measure the calibration and discrimination of the logistic regression model, the Hosmer–Lemeshow goodness-of-fit statistic and C-statistic were performed.
Kaplan–Meier analysis was performed to estimate the distribution of survival time within 1 year after radical cystectomy. Log-rank test was performed to assess the differences in survival rates between the MINS and non-MINS groups. All statistical analyses were performed using IBM SPSS Statistics for Windows, version 21.0 (IBM Corp., Armonk, NY), with P < .05 considered statistically significant.
3. Results
Between January 2007 and February 2019, 455 high-risk patients underwent radical cystectomy. A total of 207 patients were excluded (195 patients due to lack of troponin I data and 12 patients due to having other surgeries combined with radical cystectomy). Thus, 248 patients were finally analyzed, of whom 35 (14.1%) experienced MINS (Fig. 1).
Figure 1.

Flowchart of the study patients. High-risk patients were defined as those ≥45 years of age with a history of coronary artery disease, stroke, or peripheral artery disease or those ≥65 years of age. MINS was defined as serum troponin I concentration ≥0.04 mg/L within postoperative 3 days. MINS = myocardial injury after non-cardiac surgery.
Patient demographics, clinical characteristics, and intraoperative and postoperative data are shown in Tables 1 and 2. Tumor M stage, preoperative hemoglobin concentration, serum creatinine level, E’, RBC transfusion amount, and large volume blood transfusion differed significantly between the MINS and non-MINS groups. In multivariate logistic regression analysis, E/E’ ratio (odds ratio = 1.102, 95% confidence interval [1.009–1.203], P = .031), and large volume blood transfusion (odds ratio = 2.745, 95% confidence interval [1.131–6.664], P = .026) were significantly associated with MINS in high-risk patients who underwent radical cystectomy (Table 3). All variance inflation factors were <10, indicating a lack of multicollinearity. The Hosmer–Lemeshow goodness-of-fit probability was 0.104 and the C-statistic value for the model was 0.827, demonstrating good calibration and discrimination. In addition, the occurrence of MINS was significantly higher in patients who received large blood transfusion than in those who did not (10/33 patients [30.3%] patients vs 25/215 patients [11.6%], P = .008).
Table 1.
Patient demographics and clinical characteristics.

Table 2.
Intraoperative and postoperative data.

Table 3.
Univariate and multivariate logistic regression analyses of risk factors for MINS in high-risk patients who underwent radical cystectomy.

No significant difference in AKI incidence was observed between the MINS and non-MINS groups (14/35 patients [40.0%] vs 71/213 patients [33.3%], P = .448) (Table 4). ICU admission rate, ICU stay duration, postoperative MACEs, and 1-year mortality were significantly higher in the MINS group than in the non-MINS group (Table 4). Kaplan–Meier analysis demonstrated a significantly lower 1-year survival in the MINS group than in the non-MINS group (P = .010) (Fig. 2).
Table 4.
Postoperative outcomes.

Figure 2.
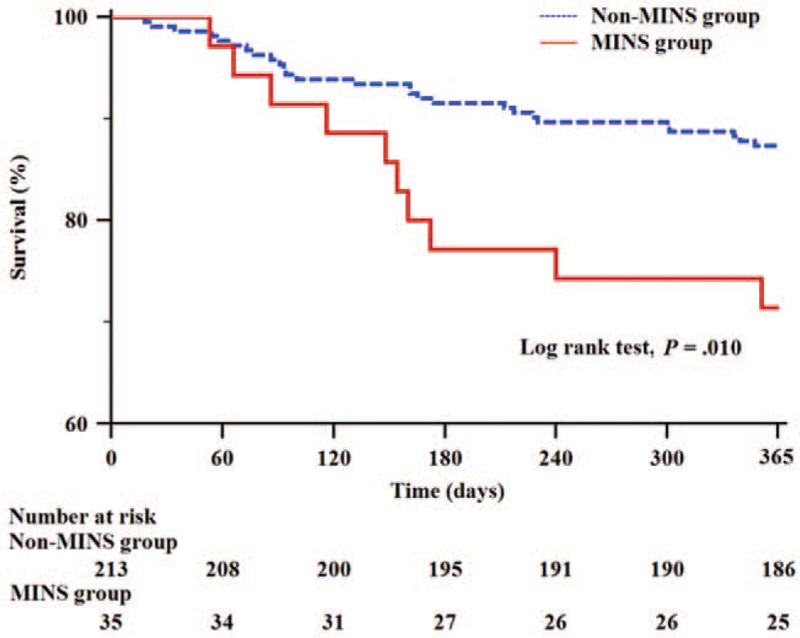
Kaplan–Meier curves of 1-year survival in the non-MINS (blue dashed line) and MINS (red solid line) groups comprising high-risk patients who underwent radical cystectomy. MINS was defined as serum troponin I concentration ≥0.04 mg/L within postoperative 3 days. High-risk patients were defined as those ≥45 years of age with a history of coronary artery disease, stroke, or peripheral artery disease or those ≥65 years of age. MINS = myocardial injury after non-cardiac surgery.
4. Discussion
The results of the present study showed a 14.1% incidence rate of MINS in high-risk patients who underwent radical cystectomy. E/E’ ratio and large volume blood transfusion were independent risk factors associated with MINS in high-risk cystectomy patients. Moreover, ICU admission rate, ICU stay duration, postoperative MACEs, and 1-year mortality were significantly higher in the MINS group than in the non-MINS group.
Myocardial injury is the most common cardiovascular complication after non-cardiac surgery and is around 30 times more common than postoperative myocardial infarction in patients with increased cardiovascular risk.[25] Many patients with myocardial injury do not satisfy the diagnostic criteria for myocardial infarction.[26] However, as myocardial injury has a poor prognosis, timely diagnosis and treatment are important.[27] MINS can be detected based on increased perioperative levels of cardiac troponin I,[8] which is a myocardial regulatory protein that is a highly sensitive and specific biomarker for myocardial damage. The incidence of MINS is approximately 8% in the general population after major non-cardiac surgery.[28] However, the present study included only high-risk patients, defined as those ≥45 years of age with a history of coronary artery disease, stroke, or peripheral artery disease or those ≥65 years of age.[5] In this study, the incidence of MINS in high-risk patients who underwent radical cystectomy was 14.1%, which was higher than that in the general population after major non-cardiac surgery. These findings are consistent with those of a previous study by Puelacher et al, who reported an incidence of MINS in high-risk patients of 16% after non-cardiac surgery such as visceral, orthopedic, traumatic, vascular, and thoracic surgeries.[5] Therefore, preoperative evaluation of independent risk factors for MINS and postoperative monitoring of serum troponin I may be needed for the early detection of MINS in high-risk patients undergoing radical cystectomy.
In the present study, E/E’ ratio was a risk factor for MINS in high-risk cystectomy patients. The tissue Doppler-derived parameter (E/E’ ratio) indicates left ventricular filling pressure[29] and is used to predict cardiovascular events and assess the prognosis of patients with cardiac disease.[30,31] Preoperative diastolic dysfunction, which is assessed using E/E’ ratio, is also reportedly associated with cardiac complications after non-cardiac surgery.[6,32] Coronary blood flow predominantly occurs during the diastole period. Diastolic dysfunction (impairment of left ventricle relaxation) reduces early diastolic coronary flow and could provoke myocardial injury in the perioperative period.[33] Therefore, the preoperative evaluation of E/E’ ratio by transthoracic echocardiography may be important for the prediction of MINS in high-risk cystectomy patients. Meticulous anesthetic management, especially preventing fluid volume overload, should be performed during radical cystectomy in high-risk patients.
We found that large volume blood transfusion, defined as four or more units of RBC transfusion during radical cystectomy,[21] to be significantly associated with MINS in high-risk cystectomy patients. Four units of RBCs is around 1000 mL; this volume of RBC transfusion may be associated with severe blood loss and significant increases in perioperative morbidity and mortality.[21,34] Large volume blood transfusion has been linked to poor outcomes with increased overall morbidity including cardiovascular complications in large retrospective studies of non-cardiac surgery.[35,36] The mechanisms by which large volume blood transfusion increases the risk of cardiovascular complications have not been well elucidated. However, circulatory derangement and metabolic, inflammatory, and coagulopathic complications caused by the transfusion of large volumes of RBCs could be involved. Moreover, these events may aggravate pre-existing medical conditions such as cardiovascular disease. Therefore, careful anesthetic management (ie, stopping anticoagulant use before surgery, maintaining a normal coagulation state, and avoiding volume overload) and meticulous surgical management should be performed to reduce large volume blood transfusion during radical cystectomy.
We found that MINS was significantly associated with higher ICU admission rate, ICU stay duration, postoperative MACEs, and 1-year mortality in high-risk patients who underwent radical cystectomy. To our knowledge, the present study is the first to demonstrate the clinical effect of MINS on postoperative outcomes among high-risk cystectomy patients. Previous studies have reported the long-term and short-term prognostic significance of MINS in vascular, orthopedic, thoracic, and abdominal surgeries.[28,37,38] Ausset et al demonstrated that MINS was an independent predictor of postoperative MACEs in hip surgery, a finding consistent with that of the present study.[38] Levy et al conducted a meta-analysis of the long-term prognostic value of MINS,[37] reporting 1-year mortality rates after surgery of 6.2% and 30.4%, respectively, among patients without and with MINS.[37] In the present study, the 1-year mortality after radical cystectomy was significantly higher in the MINS group than in the non-MINS group (28.6% vs 12.7%). These results suggest that MINS had a negative effect on postoperative outcomes among high-risk patients who underwent radical cystectomy. Therefore, serum troponin I measurement is necessary to evaluate MINS, especially in high-risk cystectomy patients.
This study has several limitations. First, the retrospective observational design meant that we could not evaluate all potential confounding factors that may affect our results. However, we collected and analyzed all possible factors to minimize bias and obtain reliable results. Second, this study could have been affected by a selection bias because we only included patients whose postoperative troponin I levels were measured at the discretion of the anesthesiologists and urologists. Therefore, our findings should be interpreted with caution before wider generalization.
5. Conclusion
The results of this study demonstrated that MINS occurred in 14.1% of patients and that E/E’ ratio and large volume blood transfusion were independent risk factors for MINS in high-risk patients who underwent radical cystectomy. Furthermore, postoperative MACEs and 1-year mortality were significantly higher in the MINS group than in the non-MINS group. These results suggest that preoperative evaluation of risk factors for MINS may provide useful information to detect postoperative cardiovascular complications in high-risk patients undergoing radical cystectomy.
Author contributions
Conceptualization: Jihion Yu, Jun-Young Park, Bumsik Hong, Jai-Hyun Hwang, Young-Kug Kim.
Data curation: Jihion Yu, Bumjin Lim, Yongsoo Lee, Jun-Young Park.
Formal analysis: Jihion Yu, Bumjin Lim, Yongsoo Lee, Jun-Young Park, Young-Kug Kim.
Project administration: Bumsik Hong, Jai-Hyun Hwang.
Supervision: Young-Kug Kim.
Writing – original draft: Jihion Yu.
Writing – review & editing: Jai-Hyun Hwang, Young-Kug Kim.
Footnotes
Abbreviations: A’ = late diastolic septal mitral annular velocity, A = late diastolic transmitral filling velocity, AKI = acute kidney injury, E’ = early diastolic septal mitral annular velocity, E = early diastolic transmitral filling velocity, ICU = intensive care unit, MACE = major adverse cardiac event, MINS = myocardial injury after non-cardiac surgery, RBC = red blood cell, S’ = systolic septal mitral annular velocity.
How to cite this article: Yu J, Lim B, Lee Y, Park JY, Hong B, Hwang JH, Kim YK. Risk factors and outcomes of myocardial injury after non-cardiac surgery in high-risk patients who underwent radical cystectomy. Medicine. 2020;99:43(e22893).
The authors have no funding and conflicts of interests to disclose.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- [1].Stenzl A, Cowan NC, De Santis M, et al. The updated EAU guidelines on muscle-invasive and metastatic bladder cancer. Eur Urol 2009;55:815–25. [DOI] [PubMed] [Google Scholar]
- [2].Tan WS, Lamb BW, Kelly JD. Complications of radical cystectomy and orthotopic reconstruction. Adv Urol 2015;2015:323157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Clark PE, Stein JP, Groshen SG, et al. Radical cystectomy in the elderly: comparison of clincal outcomes between younger and older patients. Cancer 2005;104:36–43. [DOI] [PubMed] [Google Scholar]
- [4].Madeb R, Messing EM. Gender, racial and age differences in bladder cancer incidence and mortality. Urol Oncol 2004;22:86–92. [DOI] [PubMed] [Google Scholar]
- [5].Puelacher C, Lurati Buse G, Seeberger D, et al. Perioperative myocardial injury after noncardiac surgery: incidence, mortality, and characterization. Circulation 2018;137:1221–32. [DOI] [PubMed] [Google Scholar]
- [6].Jun IJ, Kim J, Kim HG, et al. Risk factors of postoperative major adverse cardiac events after radical cystectomy: implication of diastolic dysfunction. Sci Rep 2019;9:14096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Novotny V, Hakenberg OW, Wiessner D, et al. Perioperative complications of radical cystectomy in a contemporary series. Eur Urol 2007;51:397–401. [DOI] [PubMed] [Google Scholar]
- [8].McIlroy DR, Chan MT, Wallace SK, et al. Automated preoperative assessment of endothelial dysfunction and risk stratification for perioperative myocardial injury in patients undergoing non-cardiac surgery. Br J Anaesth 2014;112:47–56. [DOI] [PubMed] [Google Scholar]
- [9].Devereaux PJ, Chan MTV, Alonso-Coello P, et al. Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery. JAMA 2012;307:2295–304. [DOI] [PubMed] [Google Scholar]
- [10].Fleischmann KE, Goldman L, Young B, et al. Association between cardiac and noncardiac complications in patients undergoing noncardiac surgery: outcomes and effects on length of stay. Am J Med 2003;115:515–20. [DOI] [PubMed] [Google Scholar]
- [11].Mackey WC, Fleisher LA, Haider S, et al. Perioperative myocardial ischemic injury in high-risk vascular surgery patients: incidence and clinical significance in a prospective clinical trial. J Vasc Surg 2006;43:533–8. [DOI] [PubMed] [Google Scholar]
- [12].Fleisher LA, Fleischmann KE, Auerbach AD, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014;130:2215–45. [DOI] [PubMed] [Google Scholar]
- [13].Kristensen SD, Knuuti J, Saraste A, et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur Heart J 2014;35:2383–431. [DOI] [PubMed] [Google Scholar]
- [14].Joung KW, Choi SS, Kong YG, et al. Incidence and risk factors of acute kidney injury after radical cystectomy: importance of preoperative serum uric acid level. Int J Med Sci 2015;12:599–604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Joung KW, Kong YG, Yoon SH, et al. Comparison of postoperative acute kidney injury between ileal conduit and neobladder urinary diversions after radical cystectomy: a propensity score matching analysis. Medicine (Baltimore) 2016;95:e4838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Yu J, Hong B, Park JY, et al. Impact of prognostic nutritional index on postoperative pulmonary complications in radical cystectomy: a propensity score-matched analysis. Ann Surg Oncol 2020; 10.1245/s10434-020-08994-6 10.1245/s10434-020-08994-6. Online ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Jeong IG, You D, Kim JW, et al. Outcomes of single lymph node positive urothelial carcinoma after radical cystectomy. J Urol 2011;185:2085–90. [DOI] [PubMed] [Google Scholar]
- [18].Yu J, Hong B, Park JY, et al. Comparison of a significant decline in the glomerular filtration rate between ileal conduit and ileal neobladder urinary diversions after radical cystectomy: a propensity score-matched analysis. J Clin Med 2020;9:2236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol 2010;17:1471–4. [DOI] [PubMed] [Google Scholar]
- [20].Comperat EM, Burger M, Gontero P, et al. Grading of urothelial carcinoma and the new “world health organisation classification of tumours of the urinary system and male genital organs 2016”. Eur Urol Focus 2019;5:457–66. [DOI] [PubMed] [Google Scholar]
- [21].Goudie R, Sterne JA, Verheyden V, et al. Risk scores to facilitate preoperative prediction of transfusion and large volume blood transfusion associated with adult cardiac surgery. Br J Anaesth 2015;114:757–66. [DOI] [PubMed] [Google Scholar]
- [22].Yu J, Park HK, Kwon HJ, et al. Risk factors for acute kidney injury after percutaneous nephrolithotomy: implications of intraoperative hypotension. Medicine (Baltimore) 2018;97:e11580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Kim HY, Kong YG, Park JH, et al. Acute kidney injury after burn surgery: preoperative neutrophil/lymphocyte ratio as a predictive factor. Acta Anaesthesiol Scand 2019;63:240–7. [DOI] [PubMed] [Google Scholar]
- [24].Jammer I, Wickboldt N, Sander M, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European Perioperative Clinical Outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol 2015;32:88–105. [DOI] [PubMed] [Google Scholar]
- [25].van Waes JA, Nathoe HM, de Graaff JC, et al. Myocardial injury after noncardiac surgery and its association with short-term mortality. Circulation 2013;127:2264–71. [DOI] [PubMed] [Google Scholar]
- [26].Ali ZA, Callaghan CJ, Ali AA, et al. Perioperative myocardial injury after elective open abdominal aortic aneurysm repair predicts outcome. Eur J Vasc Endovasc Surg 2008;35:413–9. [DOI] [PubMed] [Google Scholar]
- [27].Devereaux PJ, Goldman L, Cook DJ, et al. Perioperative cardiac events in patients undergoing noncardiac surgery: a review of the magnitude of the problem, the pathophysiology of the events and methods to estimate and communicate risk. CMAJ 2005;173:627–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Khan J, Alonso-Coello P, Devereaux PJ. Myocardial injury after noncardiac surgery. Curr Opin Cardiol 2014;29:307–11. [DOI] [PubMed] [Google Scholar]
- [29].Kidawa M, Coignard L, Drobinski G, et al. Comparative value of tissue Doppler imaging and m-mode color Doppler mitral flow propagation velocity for the evaluation of left ventricular filling pressure. Chest 2005;128:2544–50. [DOI] [PubMed] [Google Scholar]
- [30].Pasquet A, Armstrong G, Beachler L, et al. Use of segmental tissue Doppler velocity to quantitate exercise echocardiography. J Am Soc Echocardiogr 1999;12:901–12. [DOI] [PubMed] [Google Scholar]
- [31].Galderisi M, Cicala S, Caso P, et al. Coronary flow reserve and myocardial diastolic dysfunction in arterial hypertension. Am J Cardiol 2002;90:860–4. [DOI] [PubMed] [Google Scholar]
- [32].Saito S, Takagi A, Kurokawa F, et al. Usefulness of tissue Doppler echocardiography to predict perioperative cardiac events in patients undergoing noncardiac surgery. Heart Vessels 2012;27:594–602. [DOI] [PubMed] [Google Scholar]
- [33].Masuyama T, Uematsu M, Doi Y, et al. Abnormal coronary flow dynamics at rest and during tachycardia associated with impaired left ventricular relaxation in humans: implication for tachycardia-induced myocardial ischemia. J Am Coll Cardiol 1994;24:1625–32. [DOI] [PubMed] [Google Scholar]
- [34].Karkouti K, Wijeysundera DN, Yau TM, et al. The independent association of massive blood loss with mortality in cardiac surgery. Transfusion 2004;44:1453–62. [DOI] [PubMed] [Google Scholar]
- [35].Turan A, Yang D, Bonilla A, et al. Morbidity and mortality after massive transfusion in patients undergoing non-cardiac surgery. Can J Anaesth 2013;60:761–70. [DOI] [PubMed] [Google Scholar]
- [36].Whitson BA, Huddleston SJ, Savik K, et al. Risk of adverse outcomes associated with blood transfusion after cardiac surgery depends on the amount of transfusion. J Surg Res 2010;158:20–7. [DOI] [PubMed] [Google Scholar]
- [37].Levy M, Heels-Ansdell D, Hiralal R, et al. Prognostic value of troponin and creatine kinase muscle and brain isoenzyme measurement after noncardiac surgery: a systematic review and meta-analysis. Anesthesiology 2011;114:796–806. [DOI] [PubMed] [Google Scholar]
- [38].Ausset S, Auroy Y, Lambert E, et al. Cardiac troponin I release after hip surgery correlates with poor long-term cardiac outcome. Eur J Anaesthesiol 2008;25:158–64. [DOI] [PubMed] [Google Scholar]