

Heart transplantation continues to be limited by a paucity of donor organs despite innovations in organ procurement and organ preservation, greater willingness to accept marginal hearts (such as those from older donors with medical comorbidities such as diabetes and hypertension, left ventricular [LV] hypertrophy, and LV dysfunction), and use of hearts from donors who died of a drug overdose, donors with hepatitis C viremia, and donors after circulatory death.1,2 These developments have expanded the donor pool and have changed perceptions and practices with respect to consideration of heart transplant donors. The goal of this focused report is to document the changes that have taken place in the adult heart transplant donor pool over the years and to identify important donor characteristics and transplant processes that influence post-transplant outcomes.
This 37th annual adult heart transplant report is based on data submitted to the International Society for Heart and Lung Transplantation (ISHLT) Thoracic Organ Transplant (TTX) Registry on 108,034 adult recipients of deceased donor heart transplants between January 1992 and June 2018. In response to the changing regulatory environment, the ISHLT Registry is currently updating the processes involved in data acquisition from contributing transplant centers and collectives; the patient cohort examined in this report is derived from the same database or datasets used in the 2019 annual report.3 We refer the reader to the 2019 report for a detailed description of the cohort and additional core analyses not directly related to this year’s report focus.
Statistical methods
Data collection, conventions, and statistical methods
The 2020 ISHLT International TTX Registry report, as in past years, was developed using the data submitted to the Registry from national and multinational transplant collectives as well as individual transplant centers. It is estimated that the data submitted to the Registry represents approximately 75% of the worldwide thoracic transplant activity. Since the Registry’s inception, 481 adult heart transplant centers have contributed data.
This report presents an overview of deceased donor characteristics and their associations with recipient outcomes, with a particular focus on how the donor profile has changed over time when available data allows such examinations. Owing to the variability in data capturing and reporting, certain characteristics of clinical interest to readers, such as donor drug use and donor hypertension, cannot be provided in more detail (e.g., by region). The results reported herein seek to provide as granular details as possible with data retained in the ISHLT International TTX Registry for transplantations through June 30, 2018.
In addition to the data presented within the primary manuscript, extended analyses are presented in the online slide sets (https://ishltregistries.org/registries/slides.asp). The ISHLT website also contains slide sets for previous annual reports. This report references specific online electronic slides (e-slides) when particular data are discussed but not shown owing to space limitations. E-slide H(a) numbers refer to the online adult heart transplant slides.
The ISHLT International TTX Registry website (https://ishlt.org/research-data/registries/ttx-registry) provides detailed spreadsheets of the data elements collected in the Registry. The Registry requires the submission of core donor, recipient, and transplant procedure variables at baseline (i.e., at the time of transplantation) and at annual follow-up, and these variables, therefore, have low rates of missingness. Nevertheless, data quality depends on the accuracy and completeness of reporting. Rates of missingness may significantly increase for Registry variables that depend on voluntary reporting. The Registry uses various quality control measures to ensure acceptable data quality and completeness before including data for analyses.
Analytic conventions
Unless otherwise specified, analyses of combined heart–lung transplantations are not included in analyses of heart transplantations. The Registry does not capture the exact occurrence date for most secondary outcomes (e.g., cardiac allograft vasculopathy [CAV]), but it does capture the window of occurrence. For the report’s analyses, we use the midpoint between the annual followups as a surrogate for the event date (i.e., the event occurred between the first and the second annual follow-up visits). On the follow-up where a death is reported, some underreporting of secondary outcomes and other information is highly probable. Thus, to reduce the potential for underestimating event rates or other outcomes, some analyses are restricted to include only surviving recipients. For time-to-event analyses, we censored the follow-up of recipients who did not experience the event of interest at the last time the recipient was reported not to have had the event, which would either be the most recent annual follow-up or the time of retransplantation. We truncated time-to-event graphs (e.g., survival graphs) when the number of individuals at risk was <10. Previous Registry reports provide more detail regarding specific donor and recipient characteristics and outcomes.3–5
Focus theme: Deceased donor characteristics
Donor characteristics
The demand for suitable donor hearts for transplantation continues to outstrip the supply of available organs, which has led to changes over the years in the definition of an acceptable donor heart. This, combined with changes in population demographics, has led to significant changes in donor characteristics over time, as shown in Table 1. In this report, we divided adult heart transplants into 3 eras: 1992–2000, 2001–2009, and 2010–2018, with a similar number of transplantations performed in each era. Over time, the percentage of transplantations performed in North America increased from 50.8% to 55.0%, the percentage of transplantations from Other countries and regions (e.g., South America, Asia, the Middle East, Australia, and others) increased from 4.9% to 9.4%, and the percentage of transplantations from Europe decreased from 44.3% to 35.6%.
Table 1.
Donor Characteristics by Transplant Era (January 1992–June 2018)
| Characteristic | Jan 1992–Dec 2000 (N = 37,616) | Jan 2001–Dec 2009 (N = 33,588) | Jan 2010–June 2018 (N = 36,830) | p-value |
|---|---|---|---|---|
| Geographic location: | <0.0001 | |||
| Europe, n (%) | 16,663 (44.3) | 14,161 (42.2) | 13,103 (35.6) | |
| North America, n (%) | 19,119 (50.8) | 17,186 (51.2) | 20,265 (55.0) | |
| Other, n (%) | 1,834 (4.9) | 2,241 (6.7) | 3,462 (9.4) | |
| Age, years, median (percentiles) | 31 (15–54) | 34 (16–56) | 35 (17–58) | <0.0001 |
| Male, n (%) | 68.5 | 69.4 | 67.9 | 0.0001 |
| BMI, kg/m2, median (percentiles) | 24.1 (18.8–32.5)a | 25.1 (19.6–35.2) | 26.0 (19.9–37.5) | <0.0001 |
| Blood type, n (%): | <0.0001 | |||
| A | 40.0 | 38.8 | 38.1 | <0.0001 |
| AB | 2.9 | 2.4 | 2.5 | |
| B | 10.0 | 10.1 | 10.7 | |
| 0 | 47.1 | 48.7 | 48.7 | |
| Cause of death, n (%): | <0.0001 | |||
| Anoxia | 4.4 | 9.2 | 25.7 | <0.0001 |
| CVA/stroke | 35.0 | 32.7 | 25.5 | |
| Head trauma | 52.0 | 55.6 | 46.4 | |
| Other | 8.5 | 2.6 | 2.4 | |
| CMV antibody positive, n (%) | 58.0 | 60.7 | 60.6 | <0.0001 |
| EBV antibody positive, n (%) | — | 92.6b | 93.1 | 0.2036 |
| Hep B antibody positive, n (%) | 3.0 | 2.7 | 1.8 | <0.0001 |
| Hep C antibody positive, n (%) | 1.6 | 0.4 | 1.1 | <0.0001 |
| Smoking history, n (%) | 37.9a | 25.9 | 14.5 | <0.0001 |
| Alcohol use, n (%) | — | 15.0c | 16.3 | 0.0048 |
| Cocaine use, n (%) | — | 13.0 | 18.5 | <0.0001 |
| Other drugs use, n (%) | — | 32.3 | 48.9 | <0.0001 |
| Hypertension, n (%) | 10.8a | 12.3 | 15.4 | <0.0001 |
| Diabetes, n (%) | 1.5a | 2.3 | 3.5 | <0.0001 |
| LVEF <50%, n (%) | — | 2.3 | 1.6 | <0.0001 |
Abbreviations: BMI, body mass index; CMV, cytomegalovirus; CVA, cerebrovascular accident; Dec, December; EBV, Epstein-Barr virus; Hep, hepatitis; Jan, January; LVEF, left ventricular ejection fraction.
Summary statistics excluded transplants with missing data.
Continuous characteristics are expressed as median (5th–95th percentiles).
Comparisons for categorical variables were made using chi-square statistic.
Comparisons for continuous variables were made using Wilcoxon’s rank-sum test.
Based on April 1994–December 2000 transplants.
Based on April 2006–December 2009 transplants.
Based on July 2004–December 2009 transplants.
From the 1992–2000 era to the 2010–2018 era, the median donor age increased from 31 to 35 years worldwide. This increase in donor age was particularly driven by changes in European transplant practice, as shown in Figure 1a, where median donor age increased from 31 to 45 years. Increases in donor age were also seen in Other regions (26.0–34.5 years) but were less apparent in North America (28–31 years) over the same time period. The aging of the donor population likely reflects the increase in the median age of the general population, the relative scarcity of donor organs (leading to increased acceptance of older donor hearts), and the differences in donor cause of death, as discussed below. Similar to the increase in donor age over time, donor body mass index also increased over time from a median of 24.1 kg/m2 in the 1992–2000 era to 26.0 kg/m2 in the 2010–2018 era. As shown in Figure 1b, this increase was seen mainly in North America and to a lesser extent in Europe and reflects the overall rising prevalence of obesity in the general population.6,7
Figure 1.
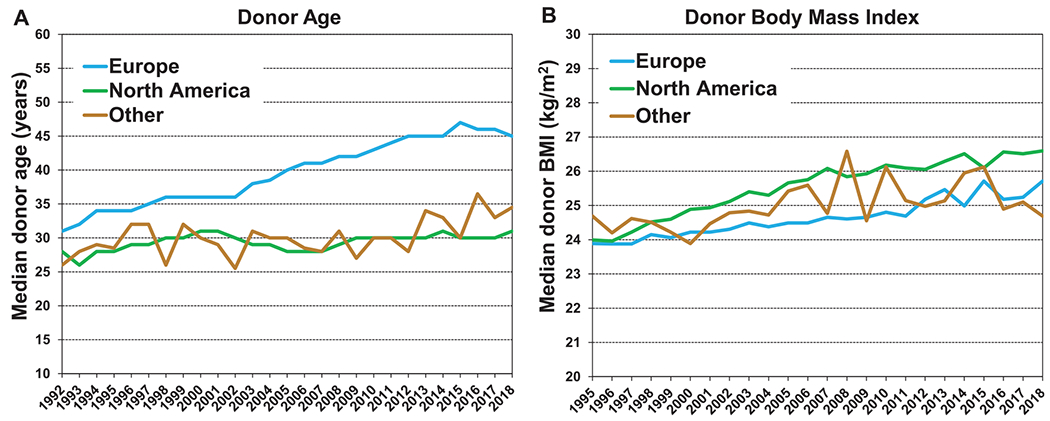
Median donor (a) age by year and geographic location (transplants: January 1992–June 2018) and (b) BMI by year and geographic location (transplants: January 1995–June 2018). BMI, body mass index.
The sex distribution of heart transplant donors has been relatively stable over time, with approximately 70% male and 30% female donors, a slight increase in the proportion of female donors over time in Europe, and a slight decrease in the proportion of females in Other regions, as shown in eSlide H(a) 7. The distribution of donors by blood type has also been stable, with approximately 38%–40% of donors being blood type A, 2%–3% blood type AB, 10% blood type B, and 47%–49% blood type O (Table 1 and eSlide H[a] 8).
Donor cause of death has changed significantly in Europe and North America over the past 3 decades (Figure 2). In Europe, donors are predominantly dying from cerebrovascular accident (CVA)/stroke, whereas head trauma deaths are on the decline. These observations likely reflect fewer deaths related to motor vehicle accidents8 and gun violence, whereas the aging donor population is more likely to succumb to neurologic events. In North America, in contrast, head trauma remains the most common cause of death, whereas deaths due to anoxia have increased in number and proportion, likely owing to the opioid epidemic and drug overdose deaths.9
Figure 2.
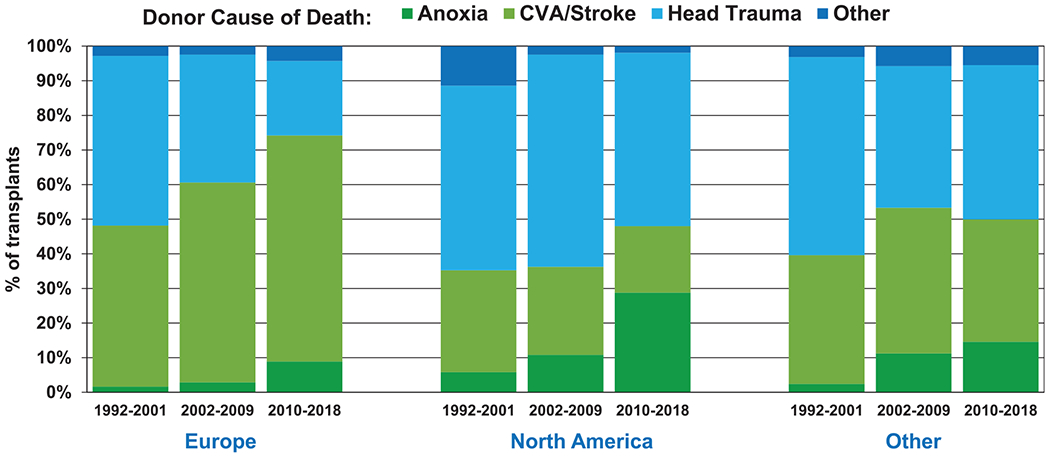
Donor cause of death by geographic location and era (transplants: January 1992–June 2018). CVA, cerebrovascular accident.
Examination of donor substance use reveals several notable changes over time. For example, the percentage of donors with a history of cigarette smoking (≥20 pack-years) declined quite precipitously from a high of 40% in 1995 to 15% in 2018 (Figure 3a), whereas alcohol use (≥2 alcoholic drinks per day) remained relatively stable (Figure 3b). Donors with cocaine use increased from 11% in 2000 to 27% in 2018, whereas donors with use of other drugs (non-intravenous street drugs such as crack, marijuana, prescription narcotics, sedatives, hypnotics, or stimulants) more than doubled from 25% to 57% over the same period of time (Figure 4). Unfortunately, it is not possible to examine the changes in donor drug use by geographic region owing to constraints in data collection and recording.
Figure 3.

Percentage of donors with a history of (a) smoking (transplants: January 1995–June 2018) and (b) alcohol use (transplants: January 2005–June 2018).
Figure 4.

Percentage of donors with a history of cocaine and other drug use (transplants: January 2000–June 2018).
We also saw notable changes in donor medical comorbidities over time. The proportion of donors with diabetes increased from 1.1% in 1995 to 4.5% in 2018. This increase is likely a reflection of the aging donor pool, the increasing prevalence of this disease in the general population, rising obesity rates, and a greater willingness to accept donors with higher risk features. Similarly, the prevalence of hypertension in heart transplant donors increased from 9.3% to 17.4% over the same period of time (Figure 5a). Interestingly, only 1.3% of donor hearts transplanted in 2018 had LV dysfunction (LV ejection fraction [LVEF] of <50%) compared with 2.4% in 2005 (Figure 5b). This suggests that relatively few hearts with LV dysfunction are being accepted for transplant in light of the estimates that 15%–24% of donors have LV dysfunction after brain death10,11 and despite the evidence that LV dysfunction in this setting is often due to neurocardiogenic injury and is highly reversible, and that the use of these hearts usually results in acceptable post-transplant clinical outcomes.12,13 The decline in the use of hearts with LV dysfunction may reflect transplant centers’ desire to avoid early post-transplant complications such as primary graft dysfunction14 as well changes in other donor characteristics over time, such as the rise in donor age, which may render these hearts less desirable.
Figure 5.

Percentage of donors with (a) diabetes and hypertension (transplants: January 1995–June 2018) and (b) LVEF <50% (transplants: January 2005–June 2018). LVEF, left ventricular ejection fraction.
Survival analyses
1-year survival
We next examined unadjusted associations between donor risk factors and 1-year post-transplant survival. Multivariable analyses were not included in this report; however, a number of multivariable analyses are available in the 2019 annual report.3
As shown in eSlide H(a) 14, older donor age is associated with reduced post-transplant survival, and most of this effect is seen within the first month after transplantation. Examination of donor and recipient age group combinations (Figure 6) shows that the early impact of donor age on recipient post-transplant survival is seen across recipient age groups, with consistently higher early mortality seen in recipients of older donor hearts. Older donor age was also associated with higher recipient mortality across geographic regions (eSlide H[a] 16); however, 1-year survival was consistently higher in North America than in Europe and Other regions, perhaps owing to other donor and recipient characteristics.
Figure 6.

Kaplan–Meier survival within 12 months by donor and recipient age (transplants: January 2000–June 2017).
Significant differences were seen in recipient 1-year survival when examined according to donor cause of death, as shown in Figure 7a. Recipients of donors who died from anoxia or head trauma had the highest 1-year survival (89.9%), whereas the lowest 1- year survival (84.1%) was seen in recipients of donors who died from CVA/stroke. As was observed with donor age, the impact of donor cause of death on recipient survival was mainly seen within the first month after transplantation.
Figure 7.

Kaplan–Meier survival within 12 months by donor (a) cause of death (transplants: January 2000–June 2017) and (b) LVEF (transplants: January 2005–June 2017). CVA, cerebrovascular accident; LVEF, left ventricular ejection fraction.
Of interest was the observation that recipients of donor hearts with LV dysfunction (defined as LVEF of <50%) had similar 1-year survival when compared with recipients of donor hearts with normal LV systolic function (89.2% vs 89.6%, Figure 7b). This slight difference in survival was mainly apparent between 1 and 6 months after transplantation, and whereas it is borderline significant (p = 0.049), it is unlikely to be clinically meaningful. It should be noted that only 507 donor hearts with LV dysfunction were transplanted between January 2005 and June 2017, compared with 26,511 donor hearts with normal LV function; thus, donor hearts with LVEF <50% that were accepted for transplantation were likely a selected group with other favorable features, such as young donor age and lack of medical comorbidities. Indeed, the mean age of donors with LVEF <50% was 27.5 years, compared with 32.2 years for donors with normal LV function. These findings should, therefore, be viewed with caution and are best examined in dedicated analyses with multivariable adjustment, as has been performed previously.12,13
We next examined recipient 1-year survival by donor substance abuse. As seen in Figure 8a, receipt of a heart from a donor with a history of smoking (more 20 pack-years) was associated with 3% lower 1-year survival, whereas receipt of a heart from a donor with a history of alcohol abuse (defined as 2 or more alcoholic drinks per day) was not associated with increased mortality (Figure 8b). Donor cocaine use did not have a significant impact on recipient 1-year survival, whereas the use of other drugs (non-intravenous street drugs such as crack, marijuana or prescription narcotics, sedatives, hypnotics, or stimulants) was associated with marginally higher recipient 1-year survival (90.1% vs 87.8%, eSlide H[a] 19). This is likely a confounded effect related to the younger age of donors who abused other drugs and who probably had fewer medical comorbidities than older donors who did not abuse street drugs.
Figure 8.

Kaplan–Meier survival within 12 months by donor history of (a) smoking (transplants: January 2000–June 2017) and (b) alcohol use (transplants: January 2005–June 2017).
Not surprisingly, recipients of hearts from donors with diabetes and hypertension (eSlide H[a] 20) had significantly lower 1-year survival than recipients of hearts from donors without these medical conditions. It is important to note, however, that these differences were often quite small. For example, recipients of hearts from diabetic donors had 87.7% 1-year survival compared with 88.5% 1-year survival in recipients of hearts from non-diabetic donors. Ideally, acceptance of donor hearts should weigh donor risk factors against the recipient’s risk of dying on the waitlist if a heart is declined for transplantation.
We then examined the effect of ischemic time, in combination with donor risk factors, on recipient 1-year survival. Previous studies, including the 2017 ISHLT Registry Report for adult heart transplantation,5,15 have shown that allograft ischemic time ≥4 hours is associated with increased recipient mortality. Figure 9 demonstrates that this association is modified by donor age, whereby recipients of younger donor hearts have improved survival relative to recipients of older donor hearts, regardless of whether ischemic time was <4 hours or ≥4 hours. We also observed that donor hypertension is associated with worse survival among recipients with allograft ischemic time <4 hours, but there was no significant survival difference between recipients of hearts from donors with and without hypertension when ischemic time was ≥4 hours, as shown in eSlide H(a) 23. However, it should be noted that there were relatively few donors with both hypertension and prolonged ischemic time in this analysis compared with the other categories, which may limit the precision of this analysis. Rather, this observation suggests a general avoidance of hearts from donors with prolonged ischemic time combined with other high-risk features.
Figure 9.

Kaplan–Meier survival within 12 months by allograft ischemic time and donor age (transplants: January 2000–June 2017).
We finally examined the effect of donor LV dysfunction, in combination with ischemic time, on recipient 1-year survival. As can be seen in Figure 10, recipients of donor hearts with both LVEF <50% and ischemic time ≥4 hours have worse survival when compared with the other 3 LVEF–ischemic time combinations. However, the statistical power of the pairwise comparisons is once again limited by the small number of recipients with donor LVEF <50% and ischemic time ≥4 hours (n = 91), again reflecting avoidance of this high-risk combination.
Figure 10.

Kaplan–Meier survival within 12 months by allograft ischemic time and donor LVEF (transplants: January 2005–June 2017). LVEF, left ventricular ejection fraction.
5-year survival, conditional on survival to 1 year
To examine associations between donor characteristics and longer-term recipient survival, we analyzed 5-year survival conditional on survival to 1 year (i.e., excluding recipients who died within the first year after transplant). As seen in eSlide H(a) 26 and 28, younger donor age is associated with improved 5-year conditional survival, both overall and by region. Further breakdown by recipient age categories (eSlide H[a] 27) shows that the benefit conferred by young donor age (donor aged <35 years) is seen primarily in recipients who are at least 40 years old, whereas younger recipients (aged 18–39 years) do not derive conditional survival benefit from receiving a young donor heart. This observation suggests that in younger recipients, recipient-level factors (such as heart disease diagnosis) may play a larger role than donor factors in determining survival between 1 and 5 years after transplantation.
Similar to the analyses of recipient 1-year survival, donor diabetes (Figure 11a) and hypertension (Figure 11b) continue to be associated with reduced recipient 5-year survival. It is possible that these comorbidities contribute to endothelial dysfunction in the donor coronary arteries, which then sets the stage for the development of CAV and reduced survival after transplantation.16,17
Figure 11.

Kaplan–Meier survival within 5 years conditional on survival to 1 year by donor history of (a) diabetes (transplants: January 2000–June 2013) and (b) hypertension (transplants: January 2000–June 2013).
Unlike analyses of recipient 1-year survival, donor cause of death is no longer associated with recipient survival between 1 and 5 years (Figure 12a). This is likely due to the fact that, as discussed previously (eSlide H[a] 17), the detrimental effect of donor CVA on recipient survival is primarily seen within the first month after transplantation.
Figure 12.

Kaplan–Meier survival within 5 years conditional on survival to 1 year by donor (a) cause of death (transplants: January 2000–June 2013) and (b) LVEF (transplants: January 2005–June 2013). CVA, cerebrovascular accident; LVEF, left ventricular ejection fraction; NS, non-significant.
In contrast to donor age, donor LV dysfunction (LVEF <50%) has a greater impact on recipient 5-year survival than on recipient 1-year survival. As seen in Figure 12b, the survival curves separate at 2 years after transplantation, after which recipients of donors with LV dysfunction have worse overall survival. It is possible that peri-operative events that contribute to donor LV dysfunction, such as the myocardial stunning and contraction band necrosis that occurs in the setting of neurocardiogenic injury,18 may contribute to longer-term graft dysfunction and eventual development of CAV. Further studies on the mechanisms whereby donor LV dysfunction contributes to longer-term recipient mortality are needed.
Similar to 1-year survival analyses, donor smoking history continues to be associated with reduced recipient 5-year survival (eSlide H[a] 30). Donor alcohol use, which was not a predictor of mortality at 1-year, is however associated with slightly increased 5-year mortality (eSlide H[a] 30). As with 1-year survival, donor cocaine use is not associated with 5-year survival (eSlide H[a] 31), and donor history of other drug use (non-intravenous street drugs) is not associated with 5-year survival (eSlide H[a] 31). These analyses suggest that donor substance use may have differential short-term and long-term effects on the transplanted heart—such effects are best studied in dedicated analyses using multivariable models in order to account for potential confounders.
We finally examined the interplay of allograft ischemic time with other donor risk factors and 5-year survival conditional on recipient survival to 1 year after transplantation. We found no difference in 5-year conditional survival between donors with ischemic time <4 hours and donors with ischemic time ≥4 hours, which suggests that the detrimental effect of prolonged ischemic time on recipient survival is seen mainly within the first year after transplantation. As seen in eSlide H(a) 33, older donor age (especially age ≥50 years) is associated with reduced survival, both for recipients of allografts with <4 hours and for those with ≥4 hours ischemic time. In contrast to the 1-year survival end-point, the combination of donor hypertension and prolonged ischemic time did not result in significantly lower 5-year conditional survival, as demonstrated in Figure 13. Finally, recipients of donor hearts with LV dysfunction appeared to have reduced 5-year conditional survival compared with recipients of hearts with normal LV function (eSlide H[a] 34) regardless of ischemic time; however, these comparisons did not meet our a priori significance threshold, likely because of the small number of patients in the high-risk categories. These results underscore the importance of weighing donor risk factors in aggregate when evaluating organ offers rather than evaluating each characteristic independently.
Figure 13.

Kaplan–Meier survival within 5 years conditional on survival to 1 year by allograft ischemic time and donor history of hypertension (transplants: January 2000–June 2013). NS, non-significant.
Freedom from CAV, conditional on survival to discharge
CAV is a leading cause of long-term graft dysfunction and graft loss after heart transplantation.19 Although our understanding of CAV pathogenesis remains incomplete, it is apparent that both donor and recipient risk factors predispose the heart transplant recipient to the development of CAV.20 We therefore examined the associations between donor risk factors and CAV development in this focus theme report. It should be noted that definitions of CAV may have varied between centers and collectives submitting data to the ISHLT TTX Registry—a standardized definition, such as the ISHLT CAV grading system,21 was not required.
We first examined freedom from CAV development by donor age. As seen in Figure 14, older donor age is associated with the development of CAV, such that 50% of recipients of donor hearts aged ≥50 years had CAV by 7 years after transplantation. This is in contrast to the recipients of donor hearts aged <35 years, 50% of whom developed CAV by approximately 13 years after transplantation. Older donors have different causes of death compared with younger donors and likely have a longer duration of substance use and medical comorbidities that may contribute to CAV development. We, therefore, examined these individual risk factors, as described below.
Figure 14.

Kaplan–Meier freedom from CAV conditional on survival to discharge by donor age (transplants: January 2000–June 2017). CAV, cardiac allograft vasculopathy.
Figure 15a demonstrates that the donor cause of death is significantly associated with CAV development, with CVA/stroke having the strongest association. CVA/stroke is more common in older donors, and this mode of death (especially subarachnoid hemorrhage) results in unusually high systemic catecholamine levels that can have toxic effects on the donor heart, which may eventually predispose to CAV development.22 Counter to this argument, however, is the observation that LV dysfunction in the donor heart (which is often seen after stroke or subarachnoid hemorrhage) was not associated with CAV (Figure 15b).
Figure 15.

Kaplan–Meier freedom from CAV conditional on survival to discharge by donor (a) cause of death (transplants: January 2000–June 2017) and (b) LVEF (transplants: January 2005–June 2017). CAV, cardiac allograft vasculopathy; CVA, cerebrovascular accident; LVEF, left ventricular ejection fraction; NS, non-significant.
Not surprisingly, donor medical comorbidities and the use of toxic substances were strongly associated with CAV development. Figure 16a and b shows that recipients of hearts from donors with diabetes and hypertension are more likely to develop CAV, and similar associations were also seen with donor smoking and alcohol use (Figure 17a and b). These risk factors likely contribute to coronary artery endothelial dysfunction in the donor heart that sets the stage for inflammation and vascular remodeling in the transplant recipient. Interestingly, donor cocaine use was not associated with CAV development (eSlide H[a] 41), despite this drug’s known adverse cardiovascular effects, including vessel wall injury, increased endothelin-1 production, and creation of a prothrombotic state.23 It is worth noting, however, that the ISHLT TTX Registry collects data on whether the donor ever abused or was dependent on cocaine and does not capture the amount or duration of donor cocaine use.
Figure 16.

Kaplan–Meier freedom from CAV conditional on survival to discharge by donor history of (a) diabetes (transplants: January 2000–June 2017) and (b) hypertension (transplants: January 2000–June 2017). CAV, cardiac allograft vasculopathy.
Figure 17.

Kaplan–Meier freedom from CAV conditional on survival to discharge by donor history of (a) smoking (transplants: January 2000–June 2017) and (b) alcohol use (transplants: January 2005–June 2017). CAV, cardiac allograft vasculopathy.
Conclusions
In this 2020 ISHLT Adult Heart Transplantation report, we closely examined deceased donor trends over time and the impact of deceased donor characteristics on outcomes. We observed many changes, including aging of the donor population (more so in Europe than in other areas) and rising prevalence of medical conditions such as diabetes, hypertension, and obesity in the donor population. Mirroring changes seen in the general population, we saw a striking drop in donor cigarette use over the past 2 decades and an alarming rise in the use of non-intravenous street drugs, likely because of the ongoing opioid epidemic in North America. Consistent with this observation were changes in donor cause of death over time. In univariate analyses, we identified significant associations between donor risk factors and recipient short-term mortality (1-year survival analyses) as well as longer-term mortality (5-year conditional survival) and development of CAV. We hope that these analyses will stimulate further questions and research focused on ways to safely expand the use of available donor hearts for transplantation without compromising recipient outcomes.
Acknowledgments
Disclosure statement
K.K.K. is supported by National Institute of Health/National Heart, Lung, and Blood Institute Award R01HL125303 to study evidence-based strategies for donor heart evaluation and serves as a scientific adviser and speaker for CareDx; L.P. serves as a speaker for Thermofisher, Sandoz, Abbott, and Novartis; J.S. is supported by American Heart Association grant 16SFRN31890003 to study patient health status in disease transitions and serves as a consultant for Medtronic and Abbott; D.C.C. received research funding from Astellas and Boehringer Ingelheim; A.Z. serves on the speakers’ bureau of Paragonix, Mallinckrodt, and Franz Kohler Chemie; and E.H. is supported by National Institute of Health/National Heart, Lung, and Blood Institute Award R01HL141892 to study the disparities in survival among heart transplant candidates and recipients. The remaining authors have no conflicts of interest to disclose.
References
- 1.Khush KK. Donor selection in the modern era. Ann Cardiothorac Surg 2018;7:126–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hsich EM. Matching the market for heart transplantation. Circ Heart Fail 2016;9:e002679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Khush KK, Cherikh WS, Chambers DC, et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: thirty-sixth adult heart transplantation report - 2019; focus theme: donor and recipient size match [published correction appears in J Heart Lung Transplant 2020;39:91]. J Heart Lung Transplant 2019;38:1056–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Khush KK, Cherikh WS, Chambers DC, et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: thirty-fifth adult heart transplantation report-2018; focus theme: multiorgan transplantation. J Heart Lung Transplant 2018;37:1155–68. [DOI] [PubMed] [Google Scholar]
- 5.Lund LH, Khush KK, Cherikh WS, et al. The Registry of the International Society for Heart and Lung Transplantation: thirty-fourth adult heart transplantation report-2017; focus theme: allograft ischemic time. J Heart Lung Transplant 2017;36:1037–46. [DOI] [PubMed] [Google Scholar]
- 6.Hales CM, Fryar CD, Carroll MD, Freedman DS, Ogden CL. Trends in obesity and severe obesity prevalence in US youth and adults by sex and age, 2007-2008 to 2015-2016. JAMA 2018;319:1723–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Pineda E, Sanchez-Romero LM, Brown M, et al. Forecasting future trends in obesity across Europe: the value of improving surveillance. Obes Facts 2018;11:360–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Eurostat, Statistics Explained>File: total number of persons killed in road traffic accidents and EU targets, EU-28.png. Available at:https://ec.europa.eu/eurostat/statistics-explained/index.php?title=File:Total_-number_of_persons_killed_in_road_traffic_accidents_and_EU_targets_EU-28.png. [Google Scholar]
- 9.Mehra MR, Jarcho JA, Cherikh W, et al. The drug-intoxication epidemic and solid-organ transplantation. N Engl J Med 2018;378:1943–5. [DOI] [PubMed] [Google Scholar]
- 10.Khush KK, Menza R, Nguyen J, Zaroff JG, Goldstein BA. Donor predictors of allograft use and recipient outcomes after heart transplantation. Circ Heart Fail 2013;6:300–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Oras J, Doueh R, Norberg E, Redfors B, Omerovic E, Dellgren G. Left ventricular dysfunction in potential heart donors and its influence on recipient outcomes. J Thorac Cardiovasc Surg 2020;159:1333–41.e6. [DOI] [PubMed] [Google Scholar]
- 12.Madan S, Saeed O, Vlismas P, et al. Outcomes after transplantation of donor hearts With improving left ventricular systolic dysfunction. J Am Coll Cardiol 2017;70:1248–58. [DOI] [PubMed] [Google Scholar]
- 13.Sibona A, Khush KK, Oyoyo UE, et al. Long-term transplant outcomes of donor hearts with left ventricular dysfunction. J Thorac Cardiovasc Surg 2019;157:1865–75. [DOI] [PubMed] [Google Scholar]
- 14.Bhatia A, King P, Ji J, Schilling J, Hartupee J, Ewald G. Donor heart transient left ventricular dysfunction is associated with post-transplant primary graft dysfunction. J Heart Lung Transplant 2020;39(Suppl):S265. [Google Scholar]
- 15.John MM, Shih W, Estevez D, et al. Interaction between ischemic time and donor age on adult heart transplant outcomes in the modern era. Ann Thorac Surg 2019;108:744–8. [DOI] [PubMed] [Google Scholar]
- 16.Nagji AS, Hranjec T, Swenson BR, et al. Donor age is associated with chronic allograft vasculopathy after adult heart transplantation: implications for donor allocation. Ann Thorac Surg 2010;90: 168–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Stehlik J, Feldman DS, Brown RN, et al. Interactions among donor characteristics influence post-transplant survival: a multi-institutional analysis. J Heart Lung Transplant 2010;29:291–8. [DOI] [PubMed] [Google Scholar]
- 18.Wybraniec MT, Mizia-Stec K, Krzych Ł. Neurocardiogenic injury in subarachnoid hemorrhage: a wide spectrum of catecholamin-mediated brain-heart interactions. Cardiol J 2014;21:220–8. [DOI] [PubMed] [Google Scholar]
- 19.Chih S, Chong AY, Mielniczuk LM, Bhatt DL, Beanlands RS. Allograft vasculopathy: the Achilles’ heel of heart transplantation. J Am Coll Cardiol 2016;68:80–91. [DOI] [PubMed] [Google Scholar]
- 20.van den Hoogen P, Huibers MM, Sluijter JP, de Weger RA. Cardiac allograft vasculopathy: a donor or recipient induced pathology? J Cardiovasc Transl Res 2015;8:106–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mehra MR, Crespo-Leiro MG, Dipchand A, et al. International Society for Heart and Lung Transplantation working formulation of a standardized nomenclature for cardiac allograft vasculopathy-2010 [published correction appears in J Heart Lung Transplant 2011;30:360]. J Heart Lung Transplant 2010;29:717–27. [DOI] [PubMed] [Google Scholar]
- 22.Berman M, Ali A, Ashley E, et al. Is stress cardiomyopathy the underlying cause of ventricular dysfunction associated with brain death? J Heart Lung Transplant 2010;29:957–65. [DOI] [PubMed] [Google Scholar]
- 23.Havakuk O, Rezkalla SH, Kloner RA. The cardiovascular effects of cocaine. J Am Coll Cardiol 2017;70:101–13. [DOI] [PubMed] [Google Scholar]