

Antimicrobial resistance is one of the biggest challenges facing modern medicine. Because the management of COVID-19 is increasingly becoming dependent on pharmacological interventions, there is greater risk for accelerating the evolution and spread of antimicrobial resistance. A study in a tertiary hospital environment revealed concerning colonisation patterns of microbes during extended periods.1 It also highlighted the diversity of antimicrobial resistance gene reservoirs in hospitals that could facilitate the emergence and transmission of new modes of antibiotic resistance.
Admission and release of patients from tertiary hospitals have risen dramatically in the past year due to the COVID-19 pandemic, with many hospitals expanding beyond capacity. With hospitalisations exceeding normal capacity due to COVID-19 combined with impaired immune function in patients, risks of co-infections have substantially increased.2, 3 The gap in a comprehensive understanding of co-infection and comorbidity caused by COVID-19 has led to rapidly changing protocols for patient handling, including administering multiple drugs around the world (figure ).4 The use of antiparasite, antiviral, antibacterial, and anti-inflammatory drugs for preventing secondary infections in patients with COVID-19 during a prolonged pandemic will inevitably invite future complications, including aggravation of antimicrobial resistance. This is particularly relevant in light of the successive emergence of mutations that increase SARS-CoV-2 fitness, which could be responsible for recurrent COVID-19 waves.5 Of note, because most of these drugs are used for other target pathogens, we might not only increase resistance in COVID-19 but also face challenges in the treatment of other bacterial and viral infections.
Figure.
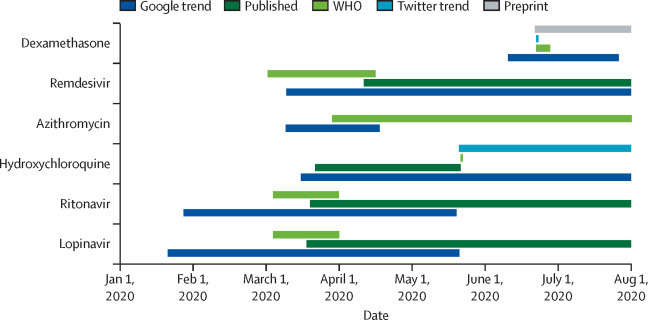
Use of multiple COVID-19 drugs in practice
Timeline of first appearance of major antiparasite, antiviral, antibacterial, and anti-inflammatory drugs for the treatment of COVID-19 in preprints, in a peer-reviewed article, as a Google search trend, as a worldwide Twitter trend, and the first time mentioned by WHO in situation reports. The other essential drugs for supportive care were first mentioned by WHO on April 14, 2020, as a part of the COVID-19 Essential Supplies Forecasting Tool.
With drugs frequently replaced by new therapeutic options (figure), the fear of increased antimicrobial resistance evolution and spread are a reality. There was an increasing demand for and misuse of various drugs in the treatment of COVID-19 irrespective of paucity of scientific evidence.6 This has even been exacerbated by rapid publication of some papers without extensive peer-review and their recommendations by WHO and the centres for disease control and prevention across the world without evaluations.4 Social media has also played an alarming role in increasing the popularity (both negative and positive) of some drugs, including a number of pharmacological substances with no proven effects.7 As an additional threat, imperfect drug penetration to patients with COVID-19 might lead to rapid evolution of multidrug resistance.8 This might be worsened by alterations observed in the gut microbiota of patients hospitalised with COVID-19, which represents a propitious dysbiotic environment for the emergence and dissemination of multidrug resistance.9
Nosocomial transmission of SARS-CoV-2 from patients to health-care workers was reported at the Wuhan Union Hospital, Wuhan, China, as early as Jan 16, 2020.10 However, investigations on accompanying multidrug-resistant infections have not been done in these and other studies. This is of note because there is substantial push towards administration of convalescent plasma therapy as a COVID-19 treatment option on the basis of success reported during previous global outbreaks, such as severe acute respiratory syndrome, Middle East respiratory syndrome, and H1N1 Influenza.11
We must be vigilant and cautious that the fight against COVID-19 does not invite another significant threat to humankind.
Acknowledgments
We declare no competing interests.
References
- 1.Chng KR, Li C, Bertrand D. Cartography of opportunistic pathogens and antibiotic resistance genes in a tertiary hospital environment. Nature Med. 2020;26:1–11. doi: 10.1038/s41591-020-0894-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cox MJ, Loman N, Bogaert D, O'grady J. Co-infections: potentially lethal and unexplored in COVID-19. Lancet Microbe. 2020;1:e11. doi: 10.1016/S2666-5247(20)30009-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sterenczak KA, Barrantes I, Stahnke T, Stachs O, Fuellen G, Undre N. Co-infections: testing macrolides for added benefit in patients with COVID-19. Lancet Microbe. 2020;1:e313. doi: 10.1016/S2666-5247(20)30170-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.WHO Coronavirus disease (COVID-19) weekly epidemiological update and weekly operational update. 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports
- 5.Korber B, Fischer WM, Gnanakaran S. Tracking changes in SARS-CoV-2 Spike: evidence that D614G increases infectivity of the COVID-19 virus. Cell. 2020;182:812–827. doi: 10.1016/j.cell.2020.06.043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Vetter P, Kaiser L, Calmy A, Agoritsas T, Huttner A. Dexamethasone and remdesivir: finding method in the COVID-19 madness. Lancet Microbe. 2020;1:e309–e310. doi: 10.1016/S2666-5247(20)30173-7. [DOI] [PubMed] [Google Scholar]
- 7.Tuccori M, Convertino I, Ferraro S. The impact of the COVID-19 “infodemic” on drug-utilization behaviors: implications for pharmacovigilance. Drug Saf. 2020;43:699–709. doi: 10.1007/s40264-020-00965-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Moreno-Gamez S, Hill AL, Rosenbloom DIS, Petrov DA, Nowak MA, Pennings PS. Imperfect drug penetration leads to spatial monotherapy and rapid evolution of multidrug resistance. Proc Natl Acad Sci USA. 2015;112:e2874–e2883. doi: 10.1073/pnas.1424184112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Zuo T, Zhang F, Lui GCY. Alterations in gut microbiota of patients with COVID-19 during time of hospitalization. Gastroenterology. 2020;159:944–955. doi: 10.1053/j.gastro.2020.05.048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wang X, Zhou Q, He Y. Nosocomial outbreak of COVID-19 pneumonia in Wuhan, China. Eur Respir J. 2020;55 doi: 10.1183/13993003.00544-2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Duan K, Liu B, Li C. Effectiveness of convalescent plasma therapy in severe COVID-19 patients. Proc Natl Acad Sci U S A. 2020;117:9490–9496. doi: 10.1073/pnas.2004168117. [DOI] [PMC free article] [PubMed] [Google Scholar]