

Abstract
Over the past two decades, topical negative pressure (TNP) wound therapy has gained wide acceptance as a genuine strategy in the treatment algorithm for a wide variety of acute and chronic wounds. Although extensive experimental and clinical evidence exists to support its use and despite the recent emergence of randomised control trials, its role and indications have yet to be fully determined. This article provides a qualitative overview of the published literature appertaining to the use of TNP therapy in the management of acute wounds by an international panel of experts using standard methods of appraisal. Particular focus is applied to the use of TNP for the open abdomen, sternal wounds, lower limb trauma, burns and tissue coverage with grafts and dermal substitutes. We provide evidence‐based recommendations for indications and techniques in TNP wound therapy and, where studies are insufficient, consensus on best practice.
Keywords: Acute wound, Negative pressure wound therapy, Topical negative pressure
Introduction
Over the past two decades, topical negative pressure (TNP) wound therapy has gained wide acceptance as a genuine strategy in the treatment algorithm for a wide variety of acute and chronic wounds. Although extensive experimental and clinical evidence exists to support its use and despite the recent emergence of randomised control trials 1, 2, its role and indications have yet to be fully determined. This article provides a qualitative overview of the published literature appertaining to the use of TNP therapy in the management of acute wounds by an international panel of experts using standard methods of appraisal (3). We provide evidence‐based recommendations for indications and techniques in TNP wound therapy and, where studies are insufficient, consensus on best practice.
Data collection
The databases MEDLINE, EMBASE, CINAHL, BNI, the Cochrane Library and the dedicated Internet resources www.vacuum‐therapy.co.uk and www.woundvac.com were searched using the key words used to describe TNP therapy listed in Table 1. In deference to such a rapidly developing concept, consideration is made of evolving adaptations of the negative pressure wound therapy philosophy and is reflected in the variety of relevant search terms.
Table 1.
TNP therapy: generic terms in common usage
| Terminology |
|---|
| Topical negative pressure (TNP) |
| Subatmospheric pressure therapy (or dressing) |
| Vacuum sealing technique (VST) |
| Vacuum‐assisted closure (VAC) |
| Negative pressure therapy (or dressing) |
| Foam suction dressing |
| Vacuum pack technique (VPT) |
Evolution
The promotion of surgical wound healing through localised suction drainage is accepted practice 4, 5. It has long been suggested that components of excess wound fluid may serve as both physical and chemical deterrents to wound healing (5). Furthermore, the positive manipulation of tissue growth by applied mechanical forces is well established, as in osteogenic distraction and soft tissue expansion. TNP achieves both, that is removes excess fluid and transmits mechanical forces to the surrounding tissue with resultant deformation of the extracellular matrix and cells (6). The practice of exposing a wound to subatmospheric pressure for an extended period to promote debridement and healing was first described by Fleischmann et al. in 1993 and several clinical studies using a variety of systems and designs followed 7, 8, 9, 10, 11, 12, 13. In 1995, the development of microprocessor‐controlled commercial systems allowed the delivery of a programmable level of continuous or intermittent subatmospheric pressure at the wound surface. This facility has allowed a more structured and scientific study of TNP, and in 1997, in a series of animal studies, Morykwas and Argenta were the first to detail the value of polyurethane sponge at the wound suction interface and to systematically investigate the physiological basis for observed clinical effects (14). The evolution of negative pressure from drainage tool to healing modality in its own right was popularised by Fleischmann and Argenta.
Foam has proven critical for the transmission of subatmospheric pressure throughout the dressing (15) and hence a uniform mechanical force across the wound. The application of subatmospheric pressure may be continuous or intermittent and the magnitude of the vacuum can be varied. The recent development of TRAC technology has allowed close control of the pressure exerted at the wound‐dressing interface via a feedback device. The concept of applying a suction force across a wound using a dressing interface is patented and is commercially available as vacuum‐assisted closure (VAC; Kinetic Concepts, Inc., San Antonio, TX, USA) (16).
Much time has been spent studying the effects of varying the dressing substrate, the magnitude of the negative pressure applied and the pressure treatment cycle for specific indications. In the case of infected wounds, TNP therapy may also be used with an irrigation system to facilitate the instillation of local antibiotic or antiseptic solutions (17).
Treatment principles
The use of TNP has been described as an adjunctive therapy to the pre‐ or postoperative surgical patient or as an alternative to surgery in a debilitated patient (15). A comprehensive review of the multimodal action of TNP is beyond the scope of this article; however, a number of scientific and clinical studies collectively support several mechanisms as central to the function of TNP. These include increased dermal perfusion 14, 18, 19, 20, stimulation of granulation tissue formation 14, 21, 22, 23, reduction in oedema and interstitial tissue fluid (14), reverse tissue expansion (16) and reduced bacterial colonisation 16, 24, 25, 26. A further specific property lies in the ability of a vacuum pressure to act as an effective skin graft splint over irregular surfaces 10, 27, 28, 29, 30, 31. Originally conceived as a potential solution to the most challenging of wounds, the past decade has seen an upsurge in its use for a legion of wound types, and in roles from downgrading of wound size and complexity prior to surgical reconstruction, to definitive healing treatment.
Clinical applications
The evidence for the use of TNP in specific acute indications (those summarised in Table 2) is considered in light of evidence in the literature.
Table 2.
Summary of acute indications for topical negative pressure wound therapy
| • Open abdomen |
| • Sternal wounds |
| • Soft tissue defects |
| Trauma, necrotising fasciitis, hydradenitis |
| suppurativa and extravasation injury |
| • Skin graft fixation |
| • Burns |
Abdominal wounds
The open abdomen remains, whether as a result of decompression laparotomy, dehiscence or necrotising fasciitis, a formidable problem for the surgeon and is associated with significant morbidity and a mortality in excess of 25% for all aetiologies (32). Furthermore, the development of the concept of the damage control laparotomy and the understanding of the abdominal compartment syndrome are resulting in increasing incidence of elective temporary open abdomens following trauma (33) [23% of trauma laparotomies in one level 1 centre (34)]. This allows abbreviated operating time in patients already acidotic, coagulopathic and hypothermic, while decompression of visceral or retroperitoneal oedema improves intra‐abdominal organ perfusion as well as allow adequate pulmonary function (35) (Table 3).
Table 3.
Classification of open abdominal wounds (36)
| Classification | Wound type | Prosthetic material status | |
|---|---|---|---|
| I | Superficial; skin defect only | a | Absent |
| II | Deep; exposed bowel or omentum | ||
| III | Complex; presence of intra‐abdominal sepsis | b | Present |
| IV | Complex; presence of enteric fistulae | ||
With the solution to one problem, however, another has been created (34). Several alternatives have been used successfully to protect the viscera and allow serial access to the peritoneum. Current management strategies include the Bogota bag, Wittman patch and the use of prosthetic mesh 13, 32, 37, 38, 39, 40. The reported eventual fascial closure varies from 50% to 70%, depending on the technique. All these methods have in common the problem of the inability to obtain primary fascial closure beyond 7–10 days (32). After this, the viscera have adhered to the abdominal wall and the fascia has retracted. This situation requires the creation of a planned ventral hernia and eventual abdominal wall reconstruction in the ensuing months at increased cost, risk and morbidity (34). Over recent years, TNP has evolved in the management of the open abdominal wound without the need to resort to deep tension sutures or prosthetic material. TNP satisfies the fundamental aims of managing the open abdomen (36). In particular, it prevents the abdominal compartment syndrome (41) while using the concept of reverse tissue expansion to optimise both skin and fascial approximation (Table 4).
Table 4.
Objectives of topical negative pressure in the management of open abdominal wounds
| • Prevention of abdominal compartment syndrome |
| • Protection of abdominal contents, with facilitation of reexploration |
| • Removal of intra‐abdominal fluid |
| Quantification of third space losses |
| Infection management |
| • Reduction of tissue and bowel oedema |
| • Preservation of the peritoneal space, allowing delayed primary fascial closure after prolonged time intervals |
| • Reverse tissue expansion aiding both skin and fascial approximation |
Of the above classification, the use of TNP in the management of abdominal wounds types II and III has been most extensively studied, reflecting their prevalence and perhaps inadequacy of current treatment options. The first large series (112 patients) was reviewed by Barker et al. (32). In an early modification of a vacuum pack technique (VPT), they used a perforated polyethylene sheet covered with a surgical towel, suction drains and an impervious adhesive drape. Although developed simply to protect the viscera (42), fascial closure rate using this standard VPT in 88 surviving patients was 70%. Twenty‐five (28%) patients underwent mesh repairs, one was closed with skin only and two were closed by secondary intervention. They had five fistulae and five intra‐abdominal abscesses. The VPT was used universally in all open abdomens, resulting in a mean time to closure of 7 days (range 1–9 days). The downside of this and other techniques may be best summed up by Dr Barker in the discussion of their article in 2000: ‘If a patient goes over 6 days, the probability of being able to do a primary fascial closure is markedly decreased.’
Vacuum‐assisted fascial closure (VAFC) was first muted by Miller et al. as a potential solution to the problem of persistent open abdomens in a 5‐year retrospective analysis of all 148 patients managed in a level 1 trauma unit with an open abdomen. Their modification of the VPT by use of a foam dressing and portable suction was used in 71 survivors with open abdomens. VAFC was successful in 69% of those patients in whom it was applied, and 22 patients were successfully closed at ≥9 days after initial surgery. Of note, they were successful in achieving closure up to 49 days post‐injury, and, compared with patients who underwent planned ventral hernia repair, complication rates were uniformly low for dehiscence, intra‐abdominal infection and fistula formation. The requirement for delayed abdominal wall reconstruction was obviated (33). The ability to close the abdomen at such a late interval was heralded as a significant improvement over earlier techniques. Indeed, in a small retrospective study by Stonerock et al. (43) in which a similar TNP system was applied to 15 trauma patients with either abdominal compartment syndrome (ACS) or visceral oedema preventing closure, the technique was abandoned after 12 days, which may explain the slightly reduced success rate of 67% fascial closure.
Garner et al. used TNP more uniformly, although over a shorter period than the initial Wake Forest report (44). Over 12 months, TNP was applied to all patients with open abdomens, both general surgical and trauma, which failed to close at second look laparotomy. Early definitive fascial closure was achieved in 13 (92%) patients at a mean of 9·9 days (range 3–21). There were no significant complications, and the cost of dressings changes was found comparable to that of other methods. Following these promising results, TNP became standard procedure at Herman for abdomens open at second laparotomy, and an ongoing report over a 26‐month period was published in 2003 (45). The TNP system was used in one third of all shock resuscitation patients of which 29 patients (83%) survived hospitalisation. Definitive fascial closure was achieved in 25 patients (86% survivors), with a low overall rate of complications [two fistulae (7%)], thus avoiding the need for delayed closure of large ventral herniae. Furthermore, although the technique again allowed closure at as late as 18 days, 65% were closed by post‐injury day 11.
More recently, Stone et al. conducted a similar retrospective study of trauma patients in which TNP via a sponge interface was used in 48 patients from initial laparotomy. Fascial closure was achieved in 72% (23) of the 32 patients who survived to discharge. Again, two people with an open abdomen for greater than a week successfully underwent primary closure (46).
These retrospective analyses proved sufficiently promising to encourage a 19‐month prospective evaluation of TNP for open abdomen, conducted by Miller et al. (34). An algorithm involving placement of a sponge at second look laparotomy was applied to 43 patients of whom 38 (88%) were successfully closed. Despite no differences in the patient population characteristics, this was significantly higher than the 69% closure rate seen in the previous study from Wake Forest (33). Again, the authors cited as beneficial the ability of the TNP system in late fascial closure, with 21 patients (48%) undergoing closure at >9 days. No intra‐abdominal abscesses were seen, but two patients (4·6%) with successful fascial closure developed wound dehiscence and were successfully reclosed. Mean follow‐up on the closed patients was 185 days (range 14–708 days), during which time, although relatively short, only one patient had been found to have a ventral hernia. The group were unable to discern any factors predicting the failure to achieve closure in five patients.
In those patients for whom despite early aggressive management, TNP failed to completely close the abdominal fascia, Scott et al. (47) achieved hernia‐free skin closure in 37 such patients (30% of all open abdomens), by filling the fascial defect with a bioprosthetic material, human acellular dermal matrix, and using TNP to rapidly close the skin. Although a descriptive study by experienced surgeons, and lacking long‐term follow‐up, no other techniques were required to close open abdomens during this study, eliminating the need for ventral hernia formation or mesh repairs with potential for erosion. Technical points included avoidance of subsequent laxity by stretching the graft and to avoid tension at the graft‐fascial seam by including the abdominal wall in a full‐thickness fascial suture.
The use of TNP for open abdominal wounds following damage control laparotomy in a paediatric population has been reported by Markley and coworkers (48). Over a 3‐year period, six patients, aged 1 month to 4 years, were managed by this technique. A single fatality occurred secondary to overwhelming intra‐abdominal sepsis, however, abdominal closure was achieved in the remainder in a mean of 8 days.
Thus, TNP in the management of open abdomen is well established, particularly in the trauma situation, although Fenn and Butler (49), Cedidi et al. (50) and Shaer (11) have all reported success in abdominal wounds in the non trauma setting. Observed criteria for optimal abdominal wound management met by the application of subatmospheric pressure include reduction in bowel oedema, bacterial counts and inflammatory substances found in open abdominal wounds while eliminating the need for frequent dressing changes, maintaining intact skin and improving fluid management via observation of third space losses (51).
Recommendations
There is now good evidence that the continuous medial pressure created by a controlled foam dressing conduit and vacuum force prevents both fascial retraction and visceral adherence. This permits continuing attempts at closure several weeks after laparotomy and likely accounts for the higher closure rate seen. Most authors have used the opportunity during dressing changes at 48–72 hours to progressively approximate the fascial edges at the superior and inferior edges. The panel also support the increasing use of an occlusive interposition dressing between the fascia and the visceral contents, which both enhances fascial mobility and protects underlying structures. Multiple dressing sheet perforations permit the desired intra‐abdominal fluid and oedema evacuation. For the open abdomen, as for other indications in which the importance of drainage may outweigh granulation tissue formation, continuous negative pressures of up to −175 mmHg have been favoured in the literature. Further work will determine if this improves quality of subsequent primary or secondary skin closure by virtue of improved granulation. With increasing experience, confidence in TNP application at initial laparotomy has grown, and it is important to consider the modality as integral to immediate management and prevention of complications rather than a solution when all else fails. In many units, this will require increased collaboration of general and plastic surgery teams, which may represent a departure from current ethos in the management of this problem.
On the basis of the discussed evidence and authors’ experience, the following algorithm is suggested for the management of the open abdomen (Table 5; Figure 1).
Table 5.
Specific recommendations for use of topical negative pressure (TNP) in the open abdomen
| • A TNP system should be applied from initial laparotomy to maximise benefits to overall patient care |
| • Optimum wound results may take 21 days or more to achieve. We see no deleterious effect of allowing continuation of vacuum‐assisted closure while the patient continues to make physiological progress |
| • For grade II abdominal wounds and above, a fenestrated non adherent apron should be placed over the abdominal viscera and beneath the peritoneum |
| • Caution with high‐output abdominal fistulae. Use recommended in specialised units only |
| (Grade B, level III) |
Figure 1.
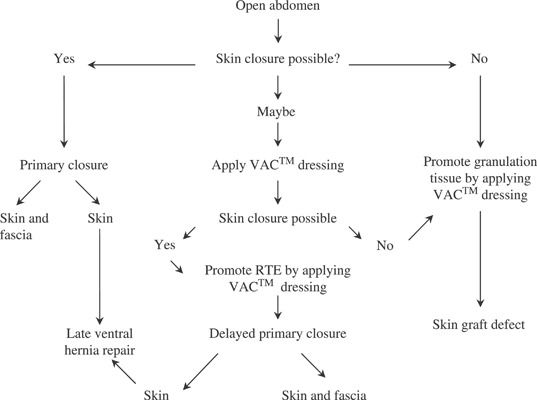
Algorithm for the management of the open abdomen. RTE, reverse tissue expansion; VAC, vacuum‐assisted closure.
Enterocutaneous fistulae
A postoperative enterocutaneous fistula poses significant problems for both patient and surgeon alike. Conventional non surgical therapies require at least 4–6 weeks of treatment to achieve a closure rate of approximately 70%, with an associated mortality of approximately 20% 52, 53. While the use of TNP in the management of such complex wounds is not yet an established technique, a number of successful case reports are cited in the literature that evidence expedited wound healing. Hyon and colleagues first reported the successful use of the vacuum sealing method in a high‐output small bowel fistula (54). Further reports include a series of three patients with small bowel fistulae successfully managed with vacuum‐assisted closure (55), a Crohn’s patient (56), and an extensive complex fistula in a patient with advanced ovarian cancer (57). Subatmospheric pressure dressing therapy has also been successfully used in the management of lymphocutaneous fistulae of the groin (58). The above reports are encouraging, but insufficient evidence exists to recommend the use of TNP as primary management strategy for entercutaneous fistulae outside specialist units.
Open sternal wounds
Post‐sternotomy mediastinitis occurs in 1%–5% of patients following midline sternotomy (59) and, albeit infrequent, is a dreaded complication with a high morbidity and mortality. The treatment of sternal wound infections has evolved since 1969, when Payne and Larson (60) described the technique of wound debridement, primary sternal closure and closed mediastinal catheter irrigation. This was followed in the early 1980s by the use of muscle flaps to fill dead space in the mediastinum and to cover the traumatised sternum (61). Myocutaneous flaps have allowed early closure and healing of sternal wounds; however, the mortality rate associated with mediastinitis remains between 10% and 20% (61). For this reason, the use of TNP has been embraced by many cardiac centres. Evaluation of their collective experiences proves difficult as, in common with other nascent technologies, initial protocols vary considerably, not least treatment aims, ranging from thoracic stabilisation and infection control prior to soft tissue reconstruction to ultimate avoidance of flap procedures altogether. Good results in several studies with more modest treatment goals, however, reflect the progressive potential of TNP in this indication (Figure 2).
Figure 2.
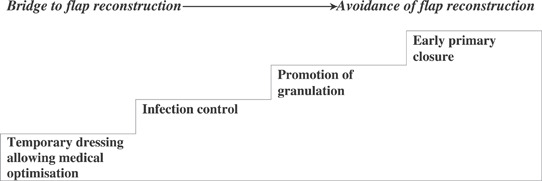
Stepwise role progression of topical negative pressure in the management of sternal wound infections.
Several initial observational studies reported that the use of the technique can be safe and successful in these severely ill patients. Obdeijn and colleagues published a series of three patients with post‐sternotomy mediastinitis treated with TNP therapy, where the mean duration of treatment was 21–49 days (62). The authors cited the requirement for fewer dressing changes as being a significant benefit, but the study also showed that TNP applied to all patients made it possible to obviate the requirement for myocutaneous flap reconstruction. In addition, there was no apparent interference with the retrosternal structures, and no complications in wound healing were seen at a mean follow‐up of 20 months. An early case report described the safe and successful application of intermittent 50 mmHg TNP to a 1·7‐kg baby with post‐sternotomy mediastinitis following an aterial switch operation (63). Similar observations were reported in a study by Tang and colleagues (64) in which 15 patients with varying severity of post‐sternotomy wound infection were treated with TNP. They reported complete wound healing in all survivors, including three who had sternal dehiscence infected with methicillin‐resistant Staphylococcus aureus. In addition, skin grafting was needed in two patients who had sternal dehiscence with mediastinitis. Luckraz et al. managed 27 mediastinal infections with the intention to also use TNP‐only treatment (65). After a mean on 13·5 days, 13 of these patients still required myocutaneous flap reconstruction or primary surgical wound closure, a rate which may have been related to inconsistent initial surgical debridement (66). The group did, however, achieve an overall mortality of 18% comparing to 30% in the year prior to instigating TNP therapy. Furthermore, in terms of cost of treatment, TNP proved approximately 20% cheaper than standard rewiring and closed irrigation used previously.
An interesting approach to the use of TNP is described in a study by Hersh and colleagues (67). By contrast to the above attempts to avoid myocutaneous reconstruction altogether, this group uses the technique more as a bridging method to improve outcomes in those patients with sternal infection considered destined to require flap procedures. TNP was electively applied from the time of initial debridement and discontinued when resolution of infection permitted closure with regional muscle flaps. All surviving patients went on to successful wound healing, with a mean inpatient stay of 16·7 days, and the authors cited several advantages over traditional methods. They noted improvement in sternal wound stabilisation during the perioperative period and a decreased need for paralysis and mechanical ventilation. Wound management was improved by avoiding the need to perform repeated debridement or to make dessicating dressing changes to an open sternum. Moreover, these elements combined may lessen the risk for ventricular rupture (67). Fleck et al. also used infection control to guide TNP therapy in 11 patients with post‐sternotomy infection (68). TNP was used for a mean of 9·3 days – until signs of systemic sepsis resolved and quantitative microbiological cultures were negative. Delayed primary closure was achievable with five patients, while six patients required a pectoralis muscle flap. There were no mortalities.
The regimens applied by these groups imply a philosophy of TNP as primarily an infection control modality, a bridge to planned flap reconstruction. Although seemingly less ambitious than early hopes to limit complex reconstruction procedures, such an approach has achieved this very result for Gustafsson and colleagues (69). Using their well‐defined regimen using C‐Reactive Protein (CRP) levels as a guide to TNP application, they reported complete closure in 40 consecutive patients with deep sternal infections, with a mean TNP therapy duration of 10 days. All sternums were preserved and closure was achieved in all patients without the use of muscle or omental flap surgery (70).
Song et al. also use TNP as a bridge between debridement and delayed definitive closure (71). A retrospective review of 35 consecutive patients with sternal wounds over a 2‐year period compared ‘traditional’ twice daily dressing changes (18 patients) with the TNP system applied after initial debridement (17 patients). The TNP‐treated group required reconstructive flaps in all but one surviving patient, but it is significant that TNP was only applied for a relatively short time. The mean interval from debridement to closure was shorter in the VAC group (6·2 versus 8·5 days) with fewer dressing changes required (a mean of 3 versus 17). Despite this abbreviated treatment, the complexity of reconstruction was significantly diminished compared with treated than the traditional group (0·9 soft tissue flaps versus 1·5). This group went on to implement an algorithm for the management of all sternal wounds with TNP as a first‐line treatment. Their follow‐up retrospective review of 103 patients (72) is hitherto the largest series reported and the first include both superficial wounds and sterile ‘open sternums’ (because of cardiac compromise with primary closure) in significant numbers (36%). Again using TNP extensively as a temporising measure, 56% of their patients eventually required some form of flap closure, with an average TNP time of 11 days. A relatively high mortality rate of 28% was attributed to a high‐risk patient population, although the lack of illness severity scores undermines this conclusion. Nevertheless, as no patient died from TNP‐related causes, the group concluded that TNP was safe to use as first‐line management.
Another comparative study by Fuchs et al. analysed 68 sequential patients with post‐sternotomy wound infections of which 35 were treated using the VAC system following initial aggressive debridement. This group focused on the medical outcomes of their patients, achieving earlier freedom from infection, more rapid decline in CRP levels and earlier rewiring. No patient required a flap or omentoplasty, likely because in part of allowing a significantly longer duration of VAC therapy (mean 21 days; interquartile range 15–32 days) (73). Scholl et al. similarly used TNP therapy specifically to medically optimise 14 patients with infected sternal wounds prior to flap reconstruction and achieved complete closure in all patients. The fundamental role of TNP therapy duration may be illustrated by their single patient who, refusing further surgery, took 2 months of TNP treatment with antibiotics to finally achieve sternal closure (74).
Domkowski and colleagues also favour TNP application at the time of initial debridement of the infected sternum. After only 5–7 days of TNP, 55% of their 96 patient cohort managed to avoid vascular flap reconstruction, but most impressively, the mortality from mediastinitis in this series was 3·7%, significantly lower than this unit’s previous figures (75). Similar results were achieved in a retrospective review of 22 patients by Cowan et al. following prompt sternal irrigation and debridement, application of TNP avoided flap reconstruction in 64%, with a 4% mortality. This group have also attempted to quantify the effects of TNP on sternal wounds and at 14 days showed a 54% reduction in wound size, extending to 80% reduction at cessation of TNP therapy at mean 37 days. High‐risk EuroSCORES conferred a longer treatment time prognosis, but with an equally favourable final outcome (76).
Sjogren et al. recently examined this potential survival benefit implicated by the past two studies. Over 5 years, all 46 patients with culture‐verified mediastinitis (0·95%) were treated with TNP therapy. When corrected for mortality risk from cardiac surgery as defined by EuroSCORE, TNP was found to diminish the catastrophic effect of mediastinitis on early and late survival following coronary artery bypass grafting (77). Thus, in experienced hands, coronary artery bypass grafting (CABG) patients with TNP‐treated mediastinitis may have similar long‐term survival as patients without mediastinitis.
Recommendations
TNP has been used extensively in the treatment of sternal wound infections and is indicated before primary closure, as preparation for secondary closure with vascularised tissue, and as an adjunct to flap healing. The literature favours TNP applied in a continuous fashion (to optimise the sternal splinting effect) at levels around −125 mmHg. In the awake setting, this may optimise patient comfort. The panel also support the concept, as stated by Harlan, that an interposition dressing with lubricant properties, be it silicone or paraffin based, may protect mediastinal structures from direct contact with TNP. In common with the abdominal dressing, full‐thickness perforations, whether intrinsic or added by the surgeon, are required to allow transmission of negative pressure through the dressing. Such a dressing may also negate potential haemodynamic consequences of TNP applied close to the heart; although no detrimental effect has been observed clinically, one animal study suggests that sternal wound TNP applied directly to the heart decreases cardiac output and interposition of a rectus flap rectified this haemodynamic influence (78). A double‐layer foam dressing enables optimal thoracic stabilisation (sternal layer) combined with even distribution of negative pressure over the entire wound surface (subcutaneous layer). Care should be taken not to overlap the foam on intact skin. Skin sutures spanning the foam dressing may assist with placement, as may incremental negative pressure application (70).
Controlled randomised studies are underway which will elucidate the exciting prospect of a mortality and morbidity benefit compared with historical treatment modalities. In a speciality under scrutiny, this data are crucial, but in parallel with management of the open abdomen, sufficient evidence already exists to stimulate a climate change in which cardiac surgeons must allow the involvement of reconstructive professionals at the earliest indication of a sternal wound complication (Table 6).
Table 6.
Recommendations for the use of topical negative pressure (TNP) in sternal wound infections
| • Diagnosis of sternal infection warrants early involvement of a plastic surgical team |
| • Early aggressive debridement to include removal of all sternal wires and/or foreign material |
| • Risks to underlying structures should be minimised by the use of a perforated protective sheet material with lubricant properties |
| • A double‐layer foam dressing enables optimal thoracic stabilisation (sternal layer) combined with even distribution of negative pressure over the entire wound surface (subcutaneous layer) |
| • Dressing changes should be performed three times a week, unless CRP levels are rising. Changes under general anaesthetic allow debridement of demarcated tissues |
| • Duration of TNP application may be best guided by stable low CRP (30–70 g/dl) together with visual assessment of adequate granulation |
| • Active bleeding or anticoagulation beyond therapeutic range precludes the use of TNP |
| (Grade B, level III) |
CRP = C‐Reactive Protein
Skin graft fixation
Skin grafting relies on adequately securing the undersurface of graft to the recipient bed during the critical period of inosculation and capillary ingrowth between days 2 and 5. While a tie‐over dressing is usually adequate, problems may arise when attempting to graft irregular surfaces (such as the perineum and inguinal fold regions), areas prone to movement or exudative recipient beds. Shear forces between graft and bed or fluid collections resulting in separation of the two surfaces result in interruption of the revascularisation process and hence a reduction in graft ‘take’. Optimal take occurs in clean, granulating defects. TNP may be used for wound bed preparation to help reduce size and to assist tissue granulation in the wound (31) (Table 7).
Table 7.
Objectives of topical negative pressure use in skin grafts
| Wound bed preparation |
| • Downsize/downgrade defect |
| • Improve granulation |
| • Infection control |
| Application to graft |
| • Evacuation of serous fluid/haematoma |
| • Bolstering of the graft to the bed |
| • Increased rate of angiogenesis |
| • Splinting of graft bed in difficult areas |
| • Easier dressings management |
Nakayama first proposed the use of a version of negative pressure for securing skin grafts in 1990 (10). A number of non comparative series and case reports since proposed the use of TNP as a modality for improving split‐thickness graft take. The largest of these was a review by Schneider and colleagues, of their experience of using TNP therapy in securing skin grafts, particularly over difficult recipient beds (30). The authors advocated the use of meshed split‐thickness skin graft to minimise the risk of sequestered fluid (serum or blood) beneath the graft. The VAC system was applied in the standard fashion with an interpositional barrier (such as Vaseline gauze) placed between the graft and the sponge. A continuous vacuum of 125 mmHg was applied for a period of 3–4 days. Their experience extends to more than 100 wounds, both acute and chronic, of all aetiologies, in a wide selection of anatomical sites in patients aged 2 months to 97 years. All but two patients with these anatomically awkward wounds showed complete graft take.
Ensuing non comparative studies have continued to address the particular value of TNP in securing skin grafts onto wounds challenging in terms of size, site and recipient bed. Molnar and colleagues used TNP to bolster Split‐thickness skin grafts (STSGs) to the cranium in four patients, where it met with 100% successful graft take in this notoriously difficult region (29). Elwood and Bolitho reported the case of two patients with bilateral axillary hydradenitis suppurativa who underwent radical excision of the affected tissue and underwent delayed split skin grafting with subsequent application of TNP therapy to ensure adequate bolstering of the graft (79). At 1 week post‐surgery, graft take was greater than 90% in both patients. Avery and colleagues published a series of 25 patients requiring free radial forearm flap harvesting (79). The forearm donor site was managed with split‐ or full‐thickness skin graft and TNP therapy. The incidence of initial graft take was 96% at day 5 and 100% at 1 month, with a mean time to donor site healing of 14 days. It is difficult to ascertain whether their excellent results are subsequent to preservation of the deep forearm fascia, but by comparison with other published results, they propose TNP‐mediated avoidance of haematoma as a key factor. Similarly, where copious exudates initially prevented skin graft take, TNP salvaged a case of bilateral neck dissection following cervicofascial necrotising fasciitis (80).
Sposato and colleagues introduced the use of a portable TNP device to provide the requisite continuous negative pressure for five postoperative days in seven patients who had undergone split skin grafting of nine chronic lower limb defects (81). Graft take was 100% in seven wounds, but the main advantage cited by this study was a dramatically earlier ambulation.
While the above studies all report subjectively improved graft take, Scherer et al. conducted the first comparative study to address quantitative and qualitative graft outcomes (31). Sixty‐one consecutive patients undergoing STSG because of traumatic or thermal tissue loss were reviewed. Thirty‐four patients were managed with TNP and 27 with bolster dressings. No difference was seen between the groups in wound type, age, percentage of graft take or length of hospital stay. The non TNP group did have a slightly larger graft size overall, but this factor appeared to be insignificant within the failing grafts. The TNP group required significantly fewer repeated STSGs (3% versus 19%), and by this measure of clinically important graft failure, the authors concluded that the use of TNP resulted in improved overall graft survival.
The donor site wound allowed Genecov and colleagues to study a more uniform clinical objective with controls. The authors used TNP therapy to increase the rate of skin graft donor site reepithelialisation both in a porcine model and in humans (82). Ten patients underwent thigh harvest of split skin graft using a dermatome. Each patient provided a control and experimental donor site in order that a direct comparison could be made between Opsite and VAC (with an interposed sheet of petroleum‐impregnated gauze) dressings. VAC therapy was applied for a total of 7 days. Based on sequential donor site tissue biopsies, the VAC treated donor sites were noted to reepithelialise faster than the Opsite‐treated control sites by day 7, with no reported difference in pain associated with either treatment.
Encouraged by the above positive experiences with the adjunctive use of TNP with skin grafting, Moisidis and colleagues conducted a prospective, blinded and controlled clinical trial designed to assess whether STSG take is improved with TNP compared with standard bolster dressings (2). Over 1 year, 22 patients with acute wounds requiring skin grafting were randomised to either treatment and assessed 2 weeks later by a single observer blinded to the randomisation. Skin grafts receiving TNP displayed epithelialisation rates equal to or better than those in control grafts in 75% of cases. Skin grafts in the TNP group were equal to or better than control grafts in 85%. Thus, although the quantitative improvement was not significant, in this randomised controlled trial, TNP significantly improved the qualitative appearance of split‐thickness skin grafts as compared with standard bolster dressings.
Dermal substitutes
The use of Integra artificial skin in reconstruction of soft tissue defects is an evolving modality. A critical factor in the success of this product is that the collagen/glycosaminoglycan matrix becomes vascularised and metabolically incorporated into the body in a manner similar to that of composite of full‐thickness skin grafts. Clinicians continue to report new techniques in an effort to optimise tissue colonisation of Integra, but no consistent standard exists 83, 84 and the rate of engraftment remains lower than with autografts (84). There is consensus, however, that minimising haematoma and seroma formation, optimising contact of the dermal matrix with the underlying tissue bed and avoiding infections and shear forces until the tissue substitute is fully integrated are essential for optimal engraftment (85). Encouraged by the well‐documented success of these very properties of TNP in improving skin graft take, Molnar et al. conducted a laboratory study showing and improved peel strength and vascularisation at 3 days compared with controls (86). After clinical success with a degloved foot and necrotising fasciitis of the leg, an initial series of eight patients with bone, joint, tendon and bowel exposed in the wound was conducted, resulting in an average rate of matrix product vascularisation of 7·25 days, with 96% take rate and STSG take rate of 93%. These results are comparable to or better than the highest take rates in the literature, including the original series of Burke et al. (87), while the matrix was vascularised in a fraction of the time (usually 21–28 days as per product recommendation). Dziewulski achieved similar results in large burn reconstructions, with additional improvements in patient compliance and comfort (88). Using a combination of fibrin sealant and 4 days continuous TNP, versus conventional dressings, Jeschke et al. achieved an Integra take rate of 98% compared with 78% in controls. Time to skin transplantation was reduced by 60% from mean 24 days to mean 10 days, with an associated reduction in hospital stay (89).
Recommendations
In contrast to the significant disparity between the technical details of TNP application found in some wound genres, particularly sternal wounds, its use in skin grafting has been remarkably standard in terms of protocol and lengths of treatment. This may be because of historically regimented scheduling of graft assessment. This does facilitate comparison between different trials and studies, and a central theme is appearing that it is the more challenging wound areas to graft, which benefit most from adjunctive TNP therapy. Removal of fluid and splinting of the graft to its recipient bed are particular benefits of TNP in this setting and negative pressure should be applied continuously (at −100 to −125 mmHg) to reflect these. The majority of studies using TNP for wound bed preparation have also favoured a continuous mode over intermittent pressure cycling. However, in contrast to graft fixation, the latter setting requires optimum granulation, and experimental studies suggesting repeated cell stretch improves granulation formation (14) justify further clinical assessment of intermittent therapy here. A limiting factor of pressure cycling is patient tolerance, which may prove negotiable by softening the gradient and therefore sensation of pressure changes.
Similar principles have been applied attempting to enhance Integra take, and TNP may prove central to optimising success of this currently underachieving modality. Further randomised controlled trials will define targets with the most to gain from widespread application (Table 8).
Table 8.
Recommendations for use of topical negative pressure (TNP) in skin graft application
| • TNP is indicated to prepare a wound bed for grafting, where the wound and its donor site may be potentially downgraded or where infection or poor granulation prevents immediate graft application |
| • TNP may be safely used where available for all skin grafts but should be considered standard care for grafts at particular risk of low take secondary to excess mobility, exudate or anatomical configuration |
| (Grade C, level III) |
| • TNP treatment for securing a graft or dermal substitute should be used continuously at −100 to −125 mmHg for 3–4 days prior to inspection |
| • Sheet perforation/meshing of dermal substitute prior to TNP therapy does not hinder take and may prevent fluid collections |
| (Grade C, level IV) |
Burns
Although the use of TNP in burns is in its infancy, thermal injuries may yet prove its paramount indication. Many of the physiological advantages are in common with other indications and involve removal of wound oedema, infectious and inflammatory materials and improvement in wound perfusion. Particularly pertinent is the prevention of burn progression in partial‐thickness burns. The impairment of blood flow within the zone of stasis is because of the oedema‐mediated capillary stasis and thence capillary thrombosis 90, 91. Microcirculation seems maximally compromised at 12–24 hours post‐burn and resulting tissue hypoxia, ischaemia and cell death is manifest as progression to full‐thickness burn (92) (Table 9).
Table 9.
Objectives of topical negative pressure in burn wound care
| • Prevention of progression |
| • Fixation of skin grafts and dermal substitutes |
| • Splinting of wound bed/joints |
| • Expedite donor site healing for repeat harvesting |
| • Delivery of topical antimicrobials |
The literature available to support the use of TNP in burns is concise yet consistent. Several experimental studies support the quantitative effects of TNP on wound perfusion. Using needle probe laser Doppler flowmetry in an excisional porcine wound model, subatmospheric pressures of 125 mmHg resulted in a fourfold increase in blood flow in ten wounds (14). Negative pressure wound therapy was also used to treat 32 burns in a porcine deep dermal burn wound model. Despite a delay in treatment of 6 hours, a statistically significant increase in dermal blood flow in burns treated for 72 hours was shown (93). In a recent observational study of seven patients with bilateral hand burns, Kamolz et al. treated the clinically worse hand with VAC, while the other was managed conservatively (94). The VAC system supported splinting in the optimal intrinsic plus position, while hyperperfusion of VAC treated hands was showed convincingly compared with those conservatively managed. Subatmospheric pressure was applied within 6 hours after injury and for at least 48 hours. These timings are justified to coincide with previously described histological time scales of burn progression (95). The authors argue that the associated increased proportion of intervention with keratinocyte therapy as opposed to full‐thickness grafting represented an improved outcome. This study also quantified intuitive clinical observations that TNP‐mediated fluid extraction reduces wound oedema and reported up to 500 ml removed from the hand burns. Wound effluent has been shown to contain high levels of deleterious substances including proteolytic enzymes, cytokines, acute‐phase proteins (96) and metalloproteinases (97). In burns, in particular, removal of tissue fluid has also helped reduce the systemic response (98), and fewer inflammatory cells and cellular debris have been found in TNP‐treated burn wounds (99). The combination of these experimental findings culminates in a study by Morykwas et al. who found that the application of subatmospheric pressure is capable of preventing progression of partial‐thickness burns in a swine model (100).
Thus, the role of TNP is the management of burns is multifactorial, and, in common with other indications, it is likely that the most difficult injuries with the poorest prognoses stand to gain the most. At this early stage, it is appropriate to recommend further trials within the scope of specialist burns unit environments (Table 10).
Table 10.
Recommendations for topical negative pressure applications in burn wounds
| • Difficult areas should continue to be managed by burn specialists |
| • Subatmospheric pressure should begin as soon as possible, ideally within 6 hours of the injury and continue for at least 48 hours |
| (Grade C, level IV) |
Lower limb trauma
The diversity of wounds found in the lower limb has made accurate assessment of the literature difficult as authors have performed little to classify wounds in their retrospective series, hence hindering analysis. While the pioneering work published by Argenta and Fleischmann contained large series of patients with a broad spectrum of wounds, both chronic and acute, it is impossible to determine from their respective articles which wounds were specifically lower limb and related to acute trauma 15, 101. This shortcoming is repeated in much of the literature, thus limiting the robustness of evidence for this modality in the lower extremity. While anecdotal reports of the successful TNP‐therapy‐based salvage of Gustillo grade IIIB open tibial fractures with concomitant osteomyelitis exist (102), many are sceptical that TNP should be considered as an ‘easy alternative’ to definitive free flap cover in such difficult situations (103).
In 1997, Mullner and coworkers published a prospective clinical trial using the vacuum sealing technique to promote the healing of a variety of soft tissue defects (7). The disparate nature of the anatomical sites affected, aetiology of the traumatic insult and delay in presentation, and the infective pathogen, make summarising the results of this study fraught with difficulty. However, of 12 patients with acute lower limb soft tissue defects of varying aetiology, all ‘responded’ to TNP therapy, with a mean healing time of 16 days. While of 16 patients who developed an infected soft tissue defect involving exposed bone and/or implants following rigid stabilisation of a lower extremity fracture, 14 patients responded favourably, again with a mean time to healing of 16 days.
DeFranzo and colleagues presented an extensive series of 75 patients with open wounds of the lower extremity with exposed tendon, bone or hardware, but without frank osteomyelitis (104). The majority of wounds (49 patients) were as a result of trauma, while 26 were non traumatic and of varying aetiology. All non viable tissue was surgically debrided prior to placement of the VAC device, with dressing changes planned every 48 hours. Successful wound closure was obtained in 95% of patients – 12 wounds by delayed primary closure, 58 wounds were closed with a split‐thickness skin graft and 5 wounds with a musculocutaneous or fasciocutaneous flap. No free tissue transfer was required and all wound closures were stable for 6 months to 6 years.
Lang and colleagues presented an interesting series of 96 consecutive patients with severe soft tissue damage of the foot or ankle treated over a 4‐year period (105). The ankle was involved in 55 patients and in the foot in 41 patients. One polytraumatised patient died, and three patients sustained injuries of such severity, that immediate amputation was indicated. At 6 weeks post‐injury, by using TNP therapy, wound closure was achieved in all 92 patients. No free flap reconstruction was required and the overall infection rate was approximately 5%.
Degloving injuries are common and frequently devastating injuries. Their often benign appearance may belie serious underlying soft tissue damage. One recognised approach is to excise the degloved tissue, defat and fenestrate the skin and reapply as a full‐thickness skin graft (106). Meara et al. report a series of nine degloving injuries in five successive patients seen over a 12‐month period (107). The degloved skin was managed as previously described, except that a VAC device was used to then secure the graft in place for a period of 4–12 days. In seven of the nine wounds treated, take of the degloved skin was at least 95%. The authors point out that it is extremely difficult to assess skin viability, and hence, only severely damaged tissue was discarded – skin that was thought to be useful as only a biological dressing subsequently survived. Graft take was poor (60%) in one patient where the degloved region included the calcaneus and plantar fascia. Furthermore, Josty et al. reported the case of a foot degloving injury where a good outcome was achieved by using the TNP bolster technique in a similar fashion to that previously described (108).
Advantages of TNP must extend beyond pure biologically enhanced wound healing to attain widespread approval. In addition to improved ambulation (81) and fewer dressing changes in adults (109), TNP has been used in children and met with success in this challenging group for a variety of indications (110). Mooney et al. showed TNP to be well tolerated in a series of 27 children with soft tissue defects of which 20 were involving an extremity (111). By minimising the need for dressing changes, anaesthetic or sedative exposure was directly reduced. These benefits were additional to the avoidance of microvascular tissue transfer for an estimated 30% of the group, often particularly tricky in the smaller patient. Shilt and colleagues cited similar parasurgical advantages in their recent comparative study (112). Sixteen consecutive children with significant lower limb injuries sustained in lawnmower accidents were retrospectively reviewed and compared with a historical cohort. Nineteen percent of TNP patients required a free flap, while 53% of the patients in the traditional group required this significant intervention. Using a previously described objective scale assessment of functional recovery and chronic pain, more patients in the TNP group experienced a satisfactory outcome (69%) than in the traditional group (50%). Soft tissue infection was eliminated. Although this study lacked statistical power regards healing, this study again showed full device tolerance and reduced (almost tenfold) dressing changes with the use of TNP.
TNP therapy has also met with success in the management of post‐compartment syndrome fasciotomy wounds. Fleischmann and coworkers published a series of 25 consecutive patients with lower limb compartment syndrome (8 thigh, 14 lower leg and 3 foot) treated over a 26‐month period (113). The vacuum sealing technique was applied post‐fasciotomy for a mean of 12·7 days with a mean of 2·1 dressing changes per patient. Twenty wounds were closed by delayed primary closure and five by skin grafting.
Recommendations
Acknowledging the above and overlapping evidence for other indications, particularly skin grafting and wound bed preparation, the consensus view from the literature and the authors is that TNP is most suitable for complex soft tissue injuries in the absence of exposed bone. Tissue loss from the foot, exposed tendons, tissue loss in gunshot wounds and degloving injuries have proven appropriate indications 97, 104, 107, 108, 114. Continuous negative pressure between −50 to −125 mmHg is prevalent in studies where uniformity is important, although where possible, intermittent therapy introduced 48 hours into treatment may prove a greater stimulus to granulation (14).
Early wound debridement and coverage of exposed bone with well‐vascularised tissue, within 72 hours, remains the ‘gold standard’ management of open fractures (97). However, TNP may permit temporisation of open fractures beyond 72 hours pending definitive soft tissue cover, with potential downstaging of the wound. This facilitates medical optimisation of the patient and often less complex surgery (16). The panel accepts that the principle of delayed soft tissue cover remains controversial and long‐term studies are awaited; TNP with exposed metal work and infection remains an exciting prospect in these most difficult of wounds.
Complications of TNP therapy
TNP therapy is generally perceived as a safe modality of treatment. Beyond technical failures in applying the dressing, probably the most frequent reason for discontinuing treatment is pain, which is usually associated with dressing changes (115). In this situation, instillation of a local anaesthetic agent via the drainage tube into the sponge approximately 30 minutes prior to dressing removal may be of great benefit. Pain may also be associated with the negative pressure itself, particularly if applied in a cyclical fashion. By titrating the pressure, or altering the cycling programme, relief can normally be achieved.
Arterial erosion and major haemorrhage have been a theoretical concern because the inception of negative pressure therapy and exposure of a blood vessel is listed by the manufacturer as a contraindication to use of the VAC™ version. Fuchs reported a single death from right ventricular rupture directly attributable to TNP therapy (73). Interestingly, this was early in this unit’s experience and prior to the routine use of a protective silicone sheet between the mediastinal structures and the sternal foam dressing as described by Harlan and colleagues. Bleeding complications noted in the literature are predominantly in reference to minor bleeding from granulation tissue (15). Defranzo et al. reported no bleeding complications using TNP in 75 patients with leg injuries, including 6 patients requiring vascular repair (104). However, a recent report from White et al. describes the erosion of the anterior tibial artery during TNP therapy of an open fibula fracture, 22 days following injury (116). The artery had been showed free from Doppler signal and presumed thrombosed. The wound had previously been infected and the patient was receiving heparin for suspected pulmonary embolus; nevertheless, the authors suggested a similar approach to that now adopted in open abdomen and sternal wounds, in using lubricated protective dressings in the vicinity of vascular structures.
While several studies have specifically targeted TNP to infected wounds with success, some case reports suggest cessation of therapy has been necessary as a result of bacterial infection 2, 104. A single case report of toxic shock syndrome associated with the use of TNP in an open abdominal wound has been reported (117). Chester and Waters cited an anaerobic wound infection during an application of TNP therapy to a dehisced groin wound following an inguinal node clearance. The authors proposed that in this patient, the air‐free environment at the TPN wound interface potentiated the growth of anaerobic bacteria (118). The majority of clinical TNP studies have actually reported a trend towards reduction of bacterial load using semiquantitative superficial swabs 24, 25, 119. Again a significant decrease in the number of bacteria was found in tissue biopsies of pigs (14). Weed et al. dispute any influence of TNP on bacterial clearance from a wound, as measured by serial quantitative cultures, but still report improved healing in their retrospective review of 25 patients (120). Similarly, a small randomised controlled trial by Moues et al., involving 54 patients with both acute and chronic wounds, found no significant effect of TNP therapy on total bacterial load in these wounds, although the bacterial profile was shifted away from gram‐negative rods in favour of S. aureus (26). This study again showed a positive effect of TNP on wound healing, expressed as a significant reduction of wound surface area, and in considering a mild contamination with S. aureus has been reported to stimulate wound healing (121), the authors speculate that this species shift may have a role to play.
Clearly, the applications of TNP in the acute wound have expanded with our collective clinical and scientific experience. However, despite increasing confidence, some situations remain unsuitable for its use. Table 11 outlines areas the panel currently considers to be contraindications for the use of TNP in the acute wound. Other scenarios may present as relative contraindications and TNP must be used in conjunction with clinical judgement. In particular, regular wound reviews enable the identification of wounds that are failing to progress.
Table 11.
Contraindications to the use of topical negative pressure in acute wounds
| • Presence of necrotic tissue |
| • Massive invasive infection |
| • Exposed cortical bone |
| • Active bleeding from the wound site |
| (Grade C, level IV) |
Conclusions
Literature experience of TNP therapy in the acute wound is overwhelmingly positive. Ironically, subjective success has led to units applying TNP to those patients perceived most needy without a strict evidence base, resulting in a paucity of randomised controlled trials in this area. Discipline is required to allow such trials, of multicenter origin, which will determine a more precise identification of patients and wounds with the most to gain. Such trials are underway and early results allow optimism. Only formal definition of clinical and cost‐effectiveness of TNP for wounds of all aetiologies will encourage its use outside specialist centres.
References
- 1. Armstrong DG, Lavery LA. Negative pressure wound therapy after partial diabetic foot amputation: a multicentre, randomised controlled trial. Lancet 2005;366:1704–10. [DOI] [PubMed] [Google Scholar]
- 2. Moisidis E, Heath T, Boorer C, Ho K, Deva AK. A prospective, blinded, randomized, controlled clinical trial of topical negative pressure use in skin grafting. Plast Reconstr Surg 2004;114:917–22. [DOI] [PubMed] [Google Scholar]
- 3. Bishop JA, Corrie PG, Evans J, Gore ME, Hall PN, Kirkham N, Roberts DL, Anstey AV, Barlow RJ, Cox NH. UK guidelines for the management of cutaneous melanoma. Br J Plast Surg 2002;55:46–54. [DOI] [PubMed] [Google Scholar]
- 4. Fox JW, Golden GT. The use of drains in subcutaneous surgical procedures. Am J Surg 1976;132:673–4. [DOI] [PubMed] [Google Scholar]
- 5. Fay MF. Drainage systems. Their role in wound healing. AORN J 1987;46:442–55. [DOI] [PubMed] [Google Scholar]
- 6. Morykwas MJ. External application of sub‐atmospheric pressure and healing: mechanisms of action. Wound Healing Soc 1998;8:4–5. [Google Scholar]
- 7. Mullner T, Mrkonjic L, Kwasny O, Vecsei V. The use of negative pressure to promote the healing of tissue defects: a clinical trial using the vacuum sealing technique. Br J Plast Surg 1997;50:194–9. [DOI] [PubMed] [Google Scholar]
- 8. Muller G. [Vacuum dressing in septic wound treatment]. Langenbecks Arch Chir Suppl Kongressbd 1997;114:537–41. [PubMed] [Google Scholar]
- 9. Brock WB, Barker DE, Burns RP. Temporary closure of open abdominal wounds: the vacuum pack. Am Surg 1995;61:30–5. [PubMed] [Google Scholar]
- 10. Nakayama Y, Iino T, Soeda S. A new method for the dressing of free skin grafts. Plast Reconstr Surg 1990;86:1216–9. [DOI] [PubMed] [Google Scholar]
- 11. Shaer WD. Inexpensive vacuum‐assisted closure employing a conventional disposable closed‐suction drainage system. Plast Reconstr Surg 2001;107:292–3. [DOI] [PubMed] [Google Scholar]
- 12. Masters J. Reliable, inexpensive and simple suction dressings. Br J Plast Surg 1998;51:267. [DOI] [PubMed] [Google Scholar]
- 13. Wittman DH, Aprahamian C, Bergstein JM. A burr‐like device to facilitate temporary closure in planned multiple laparotomies. Eur J Surg 1993;159:75–9. [PubMed] [Google Scholar]
- 14. Morykwas MJ, Argenta LC, Shelton‐Brown EI, McGuirt W. Vacuum‐assisted closure: a new method for wound control and treatment: animal studies and basic foundation. Ann Plast Surg 1997;38:553–62. [DOI] [PubMed] [Google Scholar]
- 15. Argenta LC, Morykwas MJ. Vacuum‐assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg 1997;38:563–76; discussion 577. [PubMed] [Google Scholar]
- 16. Banwell PE, Teot L. Topical negative pressure (TNP): the evolution of a novel wound therapy. J Wound Care 2003;12:22–8. [DOI] [PubMed] [Google Scholar]
- 17. Fleischmann W, Russ M, Westhauser A, Stampehl M. [Vacuum sealing as carrier system for controlled local drug administration in wound infection]. Unfallchirurg 1998;101:649–54. [DOI] [PubMed] [Google Scholar]
- 18. Skagen K, Henriksen O. Changes in subcutaneous blood flow during locally applied negative pressure to the skin. Acta Physiol Scand 1983;117:411–4. [DOI] [PubMed] [Google Scholar]
- 19. Chen SZ, Li J, Li XY, Xu LS. Effects of vacuum‐assisted closure on wound microcirculation: an experimental study. Asian J Surg 2005;28:211–7. [DOI] [PubMed] [Google Scholar]
- 20. Timmers MS, Le Cessie S, Banwell PE, Jukema GN. The effects of varying degrees of pressure delivered by negative‐pressure wound therapy on skin perfusion. Ann Plast Surg 2005;55:665–71. [DOI] [PubMed] [Google Scholar]
- 21. Morykwas MJ, Faler BJ, Pearce DJ, Argenta LC. Effects of varying levels of subatmospheric pressure on the rate of granulation tissue formation in experimental wounds in swine. Ann Plast Surg 2001;47:547–51. [DOI] [PubMed] [Google Scholar]
- 22. Fabian TS, Kaufman HJ, Lett ED, Thomas JB, Rawl DK, Lewis PL, Summit JB, Merryman JI, Schaeffer TD, Sargent LA, Burns RP. The evaluation of subatmospheric pressure and hyperbaric oxygen in ischemic full‐thickness wound healing. Am Surg 2000;66:1136–43. [PubMed] [Google Scholar]
- 23. Saxena V, Hwang CW, Huang S, Eichbaum Q, Ingber D, Orgill DP. Vacuum‐assisted closure: microdeformations of wounds and cell proliferation. Plast Reconstr Surg 2004;114:1086–96; discussion 1097–8. [DOI] [PubMed] [Google Scholar]
- 24. Pinocy J, Albes JM, Wicke C, Ruck P, Ziemer G. Treatment of periprosthetic soft tissue infection of the groin following vascular surgical procedures by means of a polyvinyl alcohol‐vacuum sponge system. Wound Repair Regen 2003;11:104–9. [DOI] [PubMed] [Google Scholar]
- 25. Deva AK, Buckland GH, Fisher E, Liew SC, Merten S, McGlynn M, Gianoutsos MP, Baldwin MA, Lendvay PG. Topical negative pressure in wound management. Med J Aust 2000;173:128–31. [DOI] [PubMed] [Google Scholar]
- 26. Moues CM, Vos MC, Van Den Bemd GJ, Stijnen T, Hovius SE. Bacterial load in relation to vacuum‐assisted closure wound therapy: a prospective randomized trial. Wound Repair Regen 2004;12:11–7. [DOI] [PubMed] [Google Scholar]
- 27. Nakayama Y, Soeda S. A new dressing method for free skin grafting in hands. Ann Plast Surg 1991;26:499–502. [DOI] [PubMed] [Google Scholar]
- 28. Blackburn JH II, Boemi L, Hall WW, Jeffords K, Hauck RM, Banducci DR, Graham WP III. Negative‐pressure dressings as a bolster for skin grafts. Ann Plast Surg 1998;40:453–7. [DOI] [PubMed] [Google Scholar]
- 29. Molnar JA, DeFranzo AJ, Marks MW. Single‐stage approach to skin grafting the exposed skull. Plast Reconstr Surg 2000;105:174–7. [DOI] [PubMed] [Google Scholar]
- 30. Schneider AM, Morykwas MJ, Argenta LC. A new and reliable method of securing skin grafts to the difficult recipient bed. Plast Reconstr Surg 1998;102:1195–8. [DOI] [PubMed] [Google Scholar]
- 31. Scherer LA, Shiver S, Chang M, Meredith JW, Owings JT. The vacuum assisted closure device: a method of securing skin grafts and improving graft survival. Arch Surg 2002;137:930–3; discussion 933–4. [DOI] [PubMed] [Google Scholar]
- 32. Barker DE, Kaufman HJ, Smith LA, Ciraulo DL, Richart CL, Burns RP. Vacuum pack technique of temporary abdominal closure: a 7‐year experience with 112 patients. J Trauma 2000;48:201–6; discussion 206–7. [DOI] [PubMed] [Google Scholar]
- 33. Miller PR, Thompson JT, Faler BJ, Meredith JW, Chang MC. Late fascial closure in lieu of ventral hernia: the next step in open abdomen management. J Trauma 2002;53:843–9. [DOI] [PubMed] [Google Scholar]
- 34. Miller PR, Meredith JW, Johnson JC, Chang MC. Prospective evaluation of vacuum‐assisted fascial closure after open abdomen: planned ventral hernia rate is substantially reduced. Ann Surg 2004;239:608–14; discussion 614–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Chang M, Miller PR, D’Agostino R Jr, Meredith JW. Effects of abdominal decompression on cardiopulmonary function and visceral perfusion in patients with intra‐abdominal hypertension. J Trauma 1988;44:440–5. [DOI] [PubMed] [Google Scholar]
- 36. Swan MC, Banwell PE. The open abdomen: aetiology, classification and current management strategies. J Wound Care 2005;14:7–11. [DOI] [PubMed] [Google Scholar]
- 37. Aprahamian C, Wittman DH, Bergstein JM. Temporary abdominal closure (TAC) for planned relaparotomy in trauma. J Trauma 1990;30:719–23. [DOI] [PubMed] [Google Scholar]
- 38. Smith PC, Tweddell JS, Bessey PQ. Alternative approaches to abdominal wound closure in severely injured patients with massive visceral edema. J Trauma 1992;32:16–20. [DOI] [PubMed] [Google Scholar]
- 39. Mayberry JC, Mullins RJ, Crass RA, Trunkey DD. Prevention of abdominal compartment syndrome by absorbable mesh prosthesis closure. Arch Surg 1997;132:957–61; discussion 961–2. [DOI] [PubMed] [Google Scholar]
- 40. Fabian TC, Croce MA, Pritchard FE, Minard G, Hickerson WL, Howell RL, Schurr MJ, Kudsk KA. Planned ventral hernia. Staged management for acute abdominal wall defects. Ann Surg 1994;219:643–50; discussion 651–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Saggi BH, Sugerman HJ, Ivatury RR, Bloomfield GL. Abdominal compartment syndrome. J Trauma 1998;45:597–609. [DOI] [PubMed] [Google Scholar]
- 42. Maxwell RA. Response to Miller PR, Meredith JW, Johnson JC, Chang MC. Prospective evaluation of vacuum‐assisted fascial closure after open abdomen: planned ventral hernia rate is substantially reduced. Ann Surg 2004;239:615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Stonerock CE, Bynoe RP, Yost MJ, Nottingham JM. Use of a vacuum‐assisted device to facilitate abdominal closure. Am Surg 2003;69:1030–4; discussion 1034–5. [PubMed] [Google Scholar]
- 44. Garner GB, Ware DN, Cocanour CS, Duke JH, McKinley BA, Kozar RA, Moore FA. Vacuum‐assisted wound closure provides early fascial reapproximation in trauma patients with open abdomens. Am J Surg 2001;182:630–8. [DOI] [PubMed] [Google Scholar]
- 45. Suliburk JW, Ware DN, Balogh Z, McKinley BA, Cocanour CS, Kozar RA, Moore FA, Ivatury RR. Vacuum‐assisted wound closure achieves early fascial closure of open abdomens after severe trauma. J Trauma 2003;55:1155–60; discussion 1160–1. [DOI] [PubMed] [Google Scholar]
- 46. Stone PA, Hass SM, Flaherty SK, DeLuca JA, Lucente FC, Kusminsky RE. Vacuum‐assisted fascial closure for patients with abdominal trauma. J Trauma 2004;57:1082–6. [DOI] [PubMed] [Google Scholar]
- 47. Scott BG, Welsh FJ, Pham HQ, Carrick MM, Liscum KR, Granchi TS, Wall MJ Jr, Mattox KL, Hirshberg A. Early aggressive closure of the open abdomen. J Trauma 2006;60:17–22. [DOI] [PubMed] [Google Scholar]
- 48. Markley MA, Mantor PC, Letton RW, Tuggle DW. Pediatric vacuum packing wound closure for damage‐control laparotomy. J Pediatr Surg 2002;37:512–4. [DOI] [PubMed] [Google Scholar]
- 49. Fenn CH, Butler PE. Abdominoplasty wound‐healing complications: assisted closure using foam suction dressing. Br J Plast Surg 2001;54:348–51. [DOI] [PubMed] [Google Scholar]
- 50. Cedidi C, Berger A, Ingianni G. The two‐stage concept with temporary subcutaneous implantation of a vacuum sealing system: an alternative surgical approach in infected partial abdominal defects after lapratomy or abdominoplasty. Eur J Med Res 2002;7:399–403. [PubMed] [Google Scholar]
- 51. Kaplan M. Managing the open abdomen. Ostomy Wound Manage 2004;50:C2, 1–8, quiz 1p following 8. [PubMed] [Google Scholar]
- 52. Levy E, Frileux P, Cugnenc PH, Honiger J, Ollivier JM, Parc R. High‐output external fistulae of the small bowel: management with continuous enteral nutrition. Br J Surg 1989;76:676–9. [DOI] [PubMed] [Google Scholar]
- 53. Sitges‐Serra A, Jaurrieta E, Sitges‐Creus A. Management of post‐operative enterocutaneous fistulas: the roles of parenteral nutrition and surgery. Br J Surg 1982;69:147–50. [DOI] [PubMed] [Google Scholar]
- 54. Hyon SH, Martinez‐Garbino JA, Benati ML, Lopez‐Avellaneda ME, Brozzi NA, Argibay PF. Management of a high‐output postoperative enterocutaneous fistula with a vacuum sealing method and continuous enteral nutrition. ASAIO J 2000;46:511–4. [DOI] [PubMed] [Google Scholar]
- 55. Cro C, George KJ, Donnelly J, Irwin ST, Gardiner KR. Vacuum assisted closure system in the management of enterocutaneous fistulae. Postgrad Med J 2002;78:364–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Alvarez AA, Maxwell GL, Rodriguez GC. Vacuum‐assisted closure for cutaneous gastrointestinal fistula management. Gynecol Oncol 2001;80:413–6. [DOI] [PubMed] [Google Scholar]
- 57. Erdmann D, Drye C, Heller L, Wong MS, Levin SL. Abdominal wall defect and enterocutaneous fistula treatment with the Vacuum‐Assisted Closure (V.A.C.) system. Plast Reconstr Surg 2001;108:2066–8. [DOI] [PubMed] [Google Scholar]
- 58. Greer SE, Adelman M, Kasabian A, Galiano RD, Scott R, Longaker MT. The use of subatmospheric pressure dressing therapy to close lymphocutaneous fistulas of the groin. Br J Plast Surg 2000;53:484–7. [DOI] [PubMed] [Google Scholar]
- 59. Hugo NE, Sultan MR, Ascherman JA, Patsis MC, Smith CR, Rose EA. Single‐stage management of 74 consecutive sternal wound complications with pectoralis major myocutaneous advancement flaps. Plast Reconstr Surg 1994;93:1433–41. [DOI] [PubMed] [Google Scholar]
- 60. Payne WS, Larson RH. Acute mediastinits. Surg Clin North Am 1969;49:999–1009. [DOI] [PubMed] [Google Scholar]
- 61. Gummert JF, Barten MJ, Hans C, Kluge M, Doll N, Walther T, Hentschel B, Schmitt DV, Mohr FW, Diegler A. Mediastinitis and cardiac surgery – an updated risk factor analysis in 10,373 consecutive adult patients. Thorac Cardiovasc Surg 2002;50:87–91. [DOI] [PubMed] [Google Scholar]
- 62. Obdeijn MC, De Lange MY, Lichtendahl DH, De Boer WJ. Vacuum‐assisted closure in the treatment of poststernotomy mediastinitis. Ann Thorac Surg 1999;68:2358–60. [DOI] [PubMed] [Google Scholar]
- 63. Ramnarine IR, McLean A, Pollock JC. Vacuum‐assisted closure in the paediatric patient with post‐cardiotomy mediastinitis. Eur J Cardiothorac Surg 2002;22:1029–31. [DOI] [PubMed] [Google Scholar]
- 64. Tang AT, Ohri SK, Haw MP. Novel application of vacuum assisted closure technique to the treatment of sternotomy wound infection. Eur J Cardiothorac Surg 2000;17:482–4. [DOI] [PubMed] [Google Scholar]
- 65. Luckraz H, Murphy F, Bryant S, Charman SC, Ritchie AJ. Vacuum‐assisted closure as a treatment modality for infections after cardiac surgery. J Thorac Cardiovasc Surg 2003;125:301–5. [DOI] [PubMed] [Google Scholar]
- 66. Aru GM, Call KD. Limitations on the role of vacuum‐assisted closure in cardiac surgery. J Thorac Cardiovasc Surg 2004;127:604; author reply 604–5. [DOI] [PubMed] [Google Scholar]
- 67. Hersh RE, Jack JM, Dahman MI, Morgan RF, Drake DB. The vacuum‐assisted closure device as a bridge to sternal wound closure. Ann Plast Surg 2001;46:250–4. [DOI] [PubMed] [Google Scholar]
- 68. Fleck TM, Fleck M, Moidl R, Czerny M, Koller R, Giovanoli P, Hiesmayer MJ, Zimpfer D, Wolner E, Grabenwoger M. The vacuum‐assisted closure system for the treatment of deep sternal wound infections after cardiac surgery. Ann Thorac Surg 2002;74:1596–600; discussion 1600. [DOI] [PubMed] [Google Scholar]
- 69. Gustafsson R, Johnsson P, Algotsson L, Blomquist S, Ingemansson R. Vacuum‐assisted closure therapy guided by C‐reactive protein level in patients with deep sternal wound infection. J Thorac Cardiovasc Surg 2002;123:895–900. [DOI] [PubMed] [Google Scholar]
- 70. Gustafsson RI, Sjogren J, Ingemansson R. Deep sternal wound infection: a sternal‐sparing technique with vacuum‐assisted closure therapy. Ann Thorac Surg 2003;76:2048–53; discussion 2053. [DOI] [PubMed] [Google Scholar]
- 71. Song DH, Wu LC, Lohman RF, Gottlieb LJ, Franczyk M. Vacuum assisted closure for the treatment of sternal wounds: the bridge between debridement and definitive closure. Plast Reconstr Surg 2003;111:92–7. [DOI] [PubMed] [Google Scholar]
- 72. Agarwal JP, Ogilvie M, Wu LC, Lohman RF, Gottlieb LJ, Franczyk M, Song DH. Vacuum‐assisted closure for sternal wounds: a first‐line therapeutic management approach. Plast Reconstr Surg 2005;116:1035–40; discussion 1041–3. [DOI] [PubMed] [Google Scholar]
- 73. Fuchs U, Zittermann A, Stuettgen B, Groening A, Minami K, Koerfer R. Clinical outcome of patients with deep sternal wound infection managed by vacuum‐assisted closure compared to conventional therapy with open packing: a retrospective analysis. Ann Thorac Surg 2005;79:526–31. [DOI] [PubMed] [Google Scholar]
- 74. Scholl L, Chang E, Reitz B, Chang J. Sternal osteomyelitis: use of vacuum‐assisted closure device as an adjunct to definitive closure with sternectomy and muscle flap reconstruction. J Card Surg 2004;19:453–61. [DOI] [PubMed] [Google Scholar]
- 75. Domkowski PW, Smith ML, Gonyon DL Jr, Drye C, Wooten MK, Levin LS, Wolfe WG. Evaluation of vacuum‐assisted closure in the treatment of poststernotomy mediastinitis. J Thorac Cardiovasc Surg 2003;126:386–90. [DOI] [PubMed] [Google Scholar]
- 76. Cowan KN, Teague L, Sue SC, Mahoney JL. Vacuum‐assisted wound closure of deep sternal infections in high‐risk patients after cardiac surgery. Ann Thorac Surg 2005;80:2205–12. [DOI] [PubMed] [Google Scholar]
- 77. Sjogren J, Nilsson J, Gustafsson R, Malmsjo M, Ingemansson R. The impact of vacuum‐assisted closure on long‐term survival after post‐sternotomy mediastinitis. Ann Thorac Surg 2005;80:1270–5. [DOI] [PubMed] [Google Scholar]
- 78. Conquest AM, Garofalo JH, Maziarz DM, Mendelson KG, Su Sun Y, Wooden WA, Meadows WM, Nifong W, Chitwood WR. Hemodynamic effects of the vacuum‐assisted closure device on open mediastinal wounds. J Surg Res 2003;115:209–13. [DOI] [PubMed] [Google Scholar]
- 79. Elwood ET, Bolitho DG. Negative‐pressure dressings in the treatment of hidradenitis suppurativa. Ann Plast Surg 2001;46:49–51. [DOI] [PubMed] [Google Scholar]
- 80. Nouraei SA, Hodgson EL, Malata CM. Cervicofacial necrotising fasciitis: management with neck dissection and topical negative pressure. J Wound Care 2003;12:147–9. [DOI] [PubMed] [Google Scholar]
- 81. Sposato G, Molea G, Di Caprio G, Scioli M, La Rusca I, Ziccardi P. Ambulant vacuum‐assisted closure of skin‐graft dressing in the lower limbs using a portable mini‐VAC device. Br J Plast Surg 2001;54:235–7. [DOI] [PubMed] [Google Scholar]
- 82. Genecov DG, Schneider AM, Morykwas MJ, Parker D, White WL, Argenta LC. A controlled subatmospheric pressure dressing increases the rate of skin graft donor site reepithelialization. Ann Plast Surg 1998;40:219–25. [DOI] [PubMed] [Google Scholar]
- 83. Grant I, Green C, Martin R. Strategies to improve the take of commercially available collagen/glycosaminoglycan wound repair material investigated in an animal model. Burns 2001;27:699–707. [DOI] [PubMed] [Google Scholar]
- 84. Clayton MC, Bishop JF. Perioperative and postoperative dressing techniques for Integra artificial skin: views from two medical centers. J Burn Care Rehabil 1998;19:358. [DOI] [PubMed] [Google Scholar]
- 85. Molnar JA, DeFranzo AJ, Hadaegh A, Morykwas MJ, Shen P, Argenta LC. Acceleration of Integra incorporation in complex tissue defects with subatmospheric pressure. Plast Reconstr Surg 2004;113:1339–46. [DOI] [PubMed] [Google Scholar]
- 86. Molnar JA, Shrimanker N, Morykwas MJ, Argenta LC. Improved skin adherence and vascularization of Integra using subatmospheric pressure – a laboratory study. American Burn Association 34th Annual Meeting, Chicago, 24–27 April 2002.
- 87. Burke JF, Yannas IV, Quinby WC Jr, Bondoc CC, Jung WK. Successful use of a physiologically acceptable artificial skin in the treatment of extensive burn injury. Ann Surg 1981;194:413–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Dziewulski P. Skin substitutes in acute and reconstructive burn surgery. 1st International TNP Focus Group Meeting Proceedings, London, 4–6 December 2003.
- 89. Jeschke MG, Rose C, Angele P, Fuchtmeier B, Nerlich MN, Bolder U. Development of new reconstructive techniques: use of Integra in combination with fibrin glue and negative‐pressure therapy for reconstruction of acute and chronic wounds. Plast Reconstr Surg 2004;113:525–30. [DOI] [PubMed] [Google Scholar]
- 90. Zawacki BE. The natural history of reversible burn injury. Surg Gynecol Obstet 1974;139:867–72. [PubMed] [Google Scholar]
- 91. Lund T, Wiig H, Reed RK. Acute postburn edema: role of strongly negative interstitial fluid pressure. Am J Physiol 1988;255:H1069–74. [DOI] [PubMed] [Google Scholar]
- 92. Heimbach D, Engrav L, Grube B, Marvin J. Burn depth: a review. World J Surg 1992;16:10–5. [DOI] [PubMed] [Google Scholar]
- 93. Banwell PE, Morykwas MJ, Jennings DA, McGrouther DA, Argenta LC. Dermal microvascular blood flow in experimental partial thickness: the effect of topical sub‐atmospheric pressure. J Burn Care Rehabil 2000;21:S161. [Google Scholar]
- 94. Kamolz LP, Andel H, Haslik W, Winter W, Meissl G, Frey M. Use of subatmospheric pressure therapy to prevent burn wound progression in human: first experiences. Burns 2004;30:253–8. [DOI] [PubMed] [Google Scholar]
- 95. Zawacki BE. The local effects of burn injury. In: Boswick JA, editor. The art and science of burn care. Rockville: Aspen publishing, 1987:25–36. [Google Scholar]
- 96. Banwell PE. The biochemical wound environment and topical negative pressure therapy. 1st International TNP Focus Group Meeting Proceedings, London, 4–6 December 2003. [Google Scholar]
- 97. Banwell PE, Musgrove M. Topical negative pressure therapy: mechanisms and indications. Int Wound J 2004;1:95–106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Kremers L, Wanner MB, Webb K, Argenta J, Morykwas MJ. Effect of subatmospheric pressure treatment of angiotensin I and II levels post burn. American Burn Association Meeting, Miami, 1–4 April 2003. [Google Scholar]
- 99. Banwell PE, Morykwas MJ, Jennings DA, McGrouther DA, Argenta LC. Application of topical subatmospheric pressure modulates inflammatory cell extravasation in experimental partial thickness injury. Wound Repair Regen 1999;7:A287. [Google Scholar]
- 100. Morykwas MJ, David LR, Schneider AM, Whang C, Jennings DA, Canty C, Parker D, White WL, Argenta LC. Use of subatmospheric pressure to prevent progression of partial‐thickness burns in a swine model. J Burn Care Rehabil 1999;20:15–21. [DOI] [PubMed] [Google Scholar]
- 101. Fleischmann W, Becker U, Bischoff M, Hoekstra H. Vacuum sealing: indication, technique and results. Eur J Orthop Surg Trauma 1995;5:563–76. [DOI] [PubMed] [Google Scholar]
- 102. Greer S, Kasabian A, Thorne C, Borud L, Sims CD, Hsu M. The use of a subatmospheric pressure dressing to salvage a Gustilo grade IIIB open tibial fracture with concomitant osteomyelitis to avert a free flap. Ann Plast Surg 1998;41:687. [DOI] [PubMed] [Google Scholar]
- 103. Stewart KJ, Wilson Y, Keating JF. Suction dressings are no substitute for flap cover in acute open fractures. Br J Plast Surg 2001;54:652–3. [DOI] [PubMed] [Google Scholar]
- 104. DeFranzo AJ, Argenta LC, Marks MW, Molnar JA, David LR, Webb LX, Ward WG, Teasdale RG. The use of vacuum‐assisted closure therapy for the treatment of lower‐extremity wounds with exposed bone. Plast Reconstr Surg 2001;108:1184–91. [DOI] [PubMed] [Google Scholar]
- 105. Lang E, Bauer G, Becker U, Bischoff M. The vacuum sealing technique in the treatment of foot and ankle trauma with severe soft‐tissue damage. Aktuelle Traumatol 1997;27:223–7. [Google Scholar]
- 106. McGrouther DA, Sully L. Degloving injuries of the limbs: long‐term review and management based on whole‐body fluorescence. Br J Plast Surg 1980;33:9–24. [DOI] [PubMed] [Google Scholar]
- 107. Meara JG, Guo L, Smith JD, Pribaz JJ, Breuing KH, Orgill DP. Vacuum‐assisted closure in the treatment of degloving injuries. Ann Plast Surg 1999;42:589–94. [DOI] [PubMed] [Google Scholar]
- 108. Josty IC, Ramaswamy R, Laing JH. Vacuum assisted closure: an alternative strategy in the management of degloving injuries of the foot. Br J Plast Surg 2001;54:363–5. [DOI] [PubMed] [Google Scholar]
- 109. Moues CM, Van Den Bemd GJ, Meerding WJ, Hovius SE. An economic evaluation of the use of TNP on full‐thickness wounds. J Wound Care 2005;14:224–7. [DOI] [PubMed] [Google Scholar]
- 110. Caniano DA, Ruth B, Teich S. Wound management with vacuum‐assisted closure: experience in 51 pediatric patients. J Pediatr Surg 2005;40:128–32; discussion 132. [DOI] [PubMed] [Google Scholar]
- 111. Mooney JF III, Argenta LC, Marks MW, Morykwas MJ, DeFranzo AJ. Treatment of soft tissue defects in pediatric patients using the V.A.C. system. Clin Orthop Relat Res 2000;376:26–31. [DOI] [PubMed] [Google Scholar]
- 112. Shilt JS, Yoder JS, Manuck TA, Jacks L, Rushing J, Smith BP. Role of vacuum‐assisted closure in the treatment of pediatric lawnmower injuries. J Pediatr Orthop 2004;24:482–7. [DOI] [PubMed] [Google Scholar]
- 113. Fleischmann W, Lang E, Kinzl L. [Vacuum assisted wound closure after dermatofasciotomy of the lower extremity]. Unfallchirurg 1996;99:283–7. [PubMed] [Google Scholar]
- 114. DeFranzo AJ, Marks MW, Argenta LC, Genecov DG. Vacuum‐assisted closure for the treatment of degloving injuries. Plast Reconstr Surg 1999;104:2145–8. [DOI] [PubMed] [Google Scholar]
- 115. Krasner DL. Managing wound pain in patients with vacuum‐assisted closure devices. Ostomy Wound Manage 2002;48:38–43. [PubMed] [Google Scholar]
- 116. White RA, Miki RA, Kazmier P, Anglen JO. Vacuum‐assisted closure complicated by erosion and hemorrhage of the anterior tibial artery. J Orthop Trauma 2005;19:56–9. [DOI] [PubMed] [Google Scholar]
- 117. Gwan‐Nulla DN, Casal RS. Toxic shock syndrome associated with the use of the vacuum‐assisted closure device. Ann Plast Surg 2001;47:552–4. [DOI] [PubMed] [Google Scholar]
- 118. Chester DL, Waters R. Adverse alteration of wound flora with topical negative‐pressure therapy: a case report. Br J Plast Surg 2002;55:510–1. [DOI] [PubMed] [Google Scholar]
- 119. Van Wicjck R, Manicourt D, Feruzi‐Lukina G. Biological monitoring of wounds treated by negative pressure. ETRS New Technologies Focus Group Meeting, Nice, 13–14 September 2002. [Google Scholar]
- 120. Weed T, Ratliff C, Drake DB. Quantifying bacterial bioburden during negative pressure wound therapy: does the wound VAC enhance bacterial clearance? Ann Plast Surg 2004;52:276–9; discussion 279–80. [DOI] [PubMed] [Google Scholar]
- 121. Levenson SM, Kan‐Gruber D, Gruber C, Molnar JA, Seifter E. Wound healing accelerated by Staphylococcus aureus. Arch Surg 1983;118:310–20. [DOI] [PubMed] [Google Scholar]