

Abstract
Stroke is a leading cause of the adult disability epidemic in the US, with a major contribution from post-stroke cognitive impairment and dementia (PSCID), the rates of which are disproportionally high among the health disparity populations. Despite the PSCID’s overwhelming impact on public health, a knowledge gap exists with regard to the complex interaction between the acute stroke event and highly prevalent pre-existing brain pathology related to cerebrovascular and Alzheimer’s disease, or related dementia. Understanding the factors that modulate PSCID risk in relation to index stroke event is critically important for developing personalized prognostication of PSCID, targeted interventions to prevent it, and for informing future clinical trial design. The Determinants of Incident Stroke Cognitive Outcomes and Vascular Effects on RecoverY (DISCOVERY), a collaborative network of thirty clinical performance clinical sites with access to acute stroke populations and the expertise and capacity for systematic assessment of PSCID will address this critical challenge. DISCOVERY is a prospective, multi-center, observational, nested-cohort study of 8,000 nondemented ischemic and hemorrhagic stroke patients enrolled at the time of index stroke and followed for a minimum of 2 years, with serial cognitive evaluations and assessments of functional outcome, with subsets undergoing research MRI and PET and comprehensive genetic/genomic and fluid biomarker testing. The overall scientific objective of this study is to elucidate mechanisms of brain resilience and susceptibility to PSCID in diverse US populations based on complex interplay between life-course exposure to multiple vascular risk factors, pre-existing burden of microvascular and neurodegenerative pathology, the effect of strategic acute stroke lesions, and the mediating effect of genomic and epigenomic variation.
Post-stroke Cognitive Impairment and Dementia: the Scope of the Problem
Stroke results in an epidemic of adult disability in the United States (US).1,2 Cognitive impairment and dementia after stroke are highly prevalent (15 to 70%)3–8 and disabling9–11, and the US populations experiencing health disparities carry a disproportionate burden of this disability with distinct phenotypes.4,12,13 Therefore, understanding the mechanisms and determinants of post-stroke cognitive impairment and dementia (PSCID) is of utmost clinical importance, is a critical public health priority, and key to delivering equitable health care to diverse US populations.
Cerebrovascular disease and Alzheimer’s pathologies are key contributors to the overall burden of dementia, and the need to understand their relationship is a national research priority14. As traditionally defined, vascular dementia accounts for ≥20% of all dementia diagnoses.15 This figure, however, substantially underestimates the vascular contributions to cognitive impairment and dementia (VCID), particularly the high burden of concomitant Alzheimer disease (AD) and AD-related dementia (AD/ADRD) pathologies.16–18 There is strong evidence of additive or possibly synergistic interactions between cerebrovascular and AD pathology predisposing to dementia, such as reports that: 1) patients with mixed versus single pathology are three times more likely to be demented;18 2) vascular pathology lowers the threshold of AD pathology required for dementia;19,20 and 3) the presence of AD pathology21 contributes to cognitive decline in VCID.22 An analysis of 1079 individuals in the clinical-pathologic Religious Orders Study and Memory and Aging Project found isolated AD in only 9% versus 40% with AD plus an advanced vascular pathology (macroscopic infarcts, cerebral amyloid angiopathy, atherosclerosis, or arteriolosclerosis) and 44% with AD, vascular, and another neurodegenerative pathology.23 These studies indicate that overlapping vascular and neurodegenerative pathologies are the rule rather than the exception in age-related dementia.
The differential and relative contributions of cerebrovascular and neurodegenerative disease to PSCID is currently unknown. The US National Institutes of Health (NIH) created the MarkVCID consortium to validate biomarkers for VCID due to cerebral small vessel disease (SVD)24,25; similarly, a number of large-scale international collaborations including STROKOG (Stroke and Cognition Consortium), SVDs@target (Small Vessel Diseases-at-target), and the HBC (Heart-Brain Connection) have focused on the mechanisms of post-stroke VCID.26 Among these, STROKOG consortium represents a truly global effort reporting 32 member studies with a total of 18,000 individuals and representing 18 countries.27 In a recent decade, the global consortia and independent studies have made progress in the conceptualization and definitions of VCID,28,29 including the risk, trajectory of PSCID30–32 and exploratory associations with imaging and fluid biomarkers.33–35 However, no biomarkers have yet been demonstrated to reliably differentiate between neurodegenerative and cerebrovascular disease. Thus, understanding the relationships between the two remains a high priority to enable targeting of underlying mechanisms and reducing the overall burden of cognitive impairment and dementia.21,22
An acute stroke insult to a brain with pre-existing microvascular (SVD) and neurodegenerative changes likely initiates a series of pathological events leading to PSCID. The features of stroke, in combination with pre-existing cerebrovascular and AD/ADRD pathologies predispose to PSCID; however, the mechanisms and interactions of these effects are unclear. A critical limiting factor in this is lack of consensus on how and when to define PSCID, given: 1) no clear pre-stroke cognitive status data in most studies and 2) the time course of cognitive changes in the early months after stroke, which leads to inconsistent estimates of post-stroke dementia occurrence. Individuals who experience a first-ever stroke have worse cognitive performance even before the stroke, as compared to their counterparts without stroke.36 In most studies, however, cognitive change cannot be evaluated, so estimates of PSCID may not adequately account for any cognitive dysfunction which was actually present pre-stroke, or may not account for any decline which was underway before the stroke onset. Despite this challenge, in those studies in which cognition has been evaluated pre-stroke, such as the REGARDS study, stroke patients do appear to experience steeper decline after a stroke.36
The chronology of when to evaluate PSCID is a second major challenge. If cognition is considered in the very early period post-stroke, estimates of impairment can seem remarkably high (91.5% at two weeks, in one series).37 Although early cognitive decline may be common, most individuals improve within the first six months post-stroke,38 and therefore true post-stroke dementia may be an inappropriate label for these early fluctuations in cognition that are so common to stroke patients.
Despite these limitations in the field, however, several studies have converged with evidence for patterns which might increase the likelihood of developing PSCID. The size and location of the stroke have been implicated in the development of PSCID, with greater likelihood of PSCID for individuals experiencing larger strokes or those in supratentorial regions, or, specifically, the anterior circulation.39–41 Beyond lesion topography, the acute injury from stroke may induce secondary neurodegenerative changes in anatomically linked regions of cortex, presenting a plausible mechanism for PSCID.42 Regarding pre-existing burden of disease, several different studies of non-demented, stroke-free adults have shown an association between chronic microvascular injury and global cognition and performance in specific cognitive domains,43–45 and chronic microvascular disease and its progression are strongly associated with an increased risk of incident stroke.46,47 Further, radiographic markers of SVD such as peak width skeletonized mean diffusivity and free water modeling on diffusion tensor imaging (DTI), have been linked to white matter (WM) structural integrity, extracellular edema, and cognitive status in stroke-free adults with SVD.48,49 Thus, in the setting of acute stroke, the burden and location of pre-existing SVD disease is an important risk factor for development of PSCID.50,51 Similarly, evidence of AD pathology,21 or the presence of the APOE ε4 allele,52,53 further increases PSCID risk. In total, these findings suggest that combined analyses of acute stroke features and pre-existing SVD and neurodegeneration holds significant potential to elucidate the mechanisms of early and late PSCID.
Despite the established relationships between stroke and dementia, PSCID is vastly understudied because of the lack of infrastructure and combined expertise to characterize this complex phenotype with sufficient statistical power and to identify its determinants. Although clinical evidence has linked acute stroke and pre-existing brain pathology to development of PSCID, a large-scale, multicenter, prospective study with systematic ascertainment of clinical and radiographic variables accompanied by longitudinal neuropsychological evaluations is essential in order to elucidate the specific stroke characteristics that cause PSCID in distinct populations. The Determinants of Incident Stroke Cognitive Outcomes and Vascular Effects on RecoverY (DISCOVERY) funded jointly by the National Institute of Neurological Disorders and Stroke and National Institute on Aging is designed to fill this knowledge gap.
PSCID in Populations Experiencing Health Disparities
Cognitive decline after stroke disproportionally affects populations experiencing health disparities in the US. Stroke is a disease of disparities with Blacks followed by LatinX populations experiencing significantly greater incidence, and poorer outcomes after stroke.54 A body of literature linking social determinants of health to stroke disparities has been growing and multiple social determinants including lack of social support, low educational status, health access, community level poverty, discrimination and stigma have likewise been associated with stroke disparities55,56. Little has been reported about race-ethnic disparities, social determinants and PSCID; however, studies show that stroke is more frequently associated with dementia five years post-stroke in African-Americans versus Whites, despite a younger age of incident stroke,57 and also with greater cognitive decline post-stroke, even after accounting for any additional interim strokes.58 Furthermore, cognition before stroke, as stated above, is associated with greater risk of stroke, and this association is even more pronounced in Black versus White patients.59 In addition, individuals born in a high stroke mortality state are at greater risk for dementia than those born elsewhere, and this association was strongest for Black versus White individuals (with greatest dementia risk among Blacks born in a high stroke mortality state).60
Acute Stroke Trials with Cognitive Outcomes – Experience to Date
DISCOVERY is occurring in the context of a greater appreciation of the clinical importance of cognition as an outcome in trials focused on stroke prevention. Cognitive outcomes have been part of phase III stroke prevention trials since at least the Vitamin Intervention for Stroke Prevention (VISP) trial, which began enrolling patients in September 1996.61,62 In VISP, sites administered the Mini Mental State Exam (MMSE) locally to participants and no significant difference was found in the rates of ≥2 point decline in MMSE at 1 year between treatment groups (17.7% vs. 19.1%), consistent with the absence of an effect on stroke events. Since then, investigators have developed a better appreciation for and different approaches to assess PSCID. Harmonized standards have been put forth to evaluate vascular cognitive impairment, in hopes of reducing risk of false negative results and facilitating cross-study comparisons.63
Trials of blood pressure lowering have chosen to use cognitive testing to measure incidence rates of mild cognitive impairment and dementia. The HYVET (Hypertension in the Very Elderly)-COG trial had local research staff assess MMSE and a fall to <24 points or >3 points in 1 year triggered further evaluations to assess for dementia.64 HYVET-COG found that antihypertensive treatment in elderly patients did not significantly reduce incident dementia. The SPRINT-MIND trial65 was ancillary to the Systolic Blood Pressure Intervention Trial) SPRINT (NCT01206062).66 Participants were randomized to a systolic blood pressure goal of either less than 120 mm Hg (intensive treatment) or less than 140 mm Hg (standard treatment). SPRINT demonstrated that intensive blood pressure control was associated with significant reductions in the primary composite endpoint of myocardial infarction, other coronary syndromes, stroke, heart failure, or death from cardiovascular cause. This led to stopping the trial after a median follow-up of 3.26 years. In SPRINT-MIND, 8563 patients completed at least one cognitive follow-up. Cognitive testing (Montreal Cognitive Assessment [MOCA] and additional tests) was performed by local research staff. SPRINT-MIND did not find a significant therapeutic effect on dementia, but did find that intensive blood pressure control significantly reduced the risk of mild cognitive impairment (HR, 0.81). These two large blood pressure lowering studies illustrate the insensitivity of the dementia endpoint relative to milder cognitive decline.
Some trials have opted to administer cognitive testing centrally by telephone. This has the advantage of reducing measurement variability and local research coordinator burden. ARCADIA CSI, a sub-study of ARCADIA (NCT03192215), illustrates this approach. In the parent study, a target of 1100 patients with cryptogenic stroke and atriopathy are randomized to either apixaban or aspirin and study for secondary prevention of stroke. ARCADIA CSI plans to randomize 500 patients. The patients have to be >3 months post index stroke, have no history of pre-existing dementia and have at least an 8th grade education. Cognition is assessed using a centrally administered telephone battery estimated to take <30 minutes, and the cognitive outcome will assess change over 3 years.
Stroke trials with cognitive outcomes are not limited to those with pharmacological interventions. CREST-2 is an ongoing trial of revascularization plus intensive medical therapy versus intensive medical therapy alone.67 The risk factor targets of centrally directed intensive medical therapy are LDL cholesterol <70 mg/dl and systolic blood pressure <140 mmHg. The primary outcome is the composite of stroke and death within 44 days following randomization and stroke ipsilateral to the target vessel thereafter, up to four years. Change in cognition is a secondary outcome. As with ARCADIA-CSI, cognitive assessments are performed centrally and by telephone. CREST-H (NCT03121209)68 a sub-study of CREST-2, tests the hypothesis that the magnitude of treatment differences (revascularization vs. medical management alone) with regard to cognition will differ between those with flow impairment compared to those without flow impairment identified and characterized by CT or MR perfusion studies.
Overall, early attempts to incorporate cognitive outcomes or cognitively based diagnostic outcomes (e.g., dementia) have been mixed or are ongoing and have focused on homogeneous stroke or at-risk populations. DISCOVERY takes advantage of clinic-based assessments for performing detailed cognitive testing and the advantage of telephone-based assessments for scalability, site-burden, and standardization. As such, DISCOVERY will provide essential information on cognitive trajectories for the global stroke population, and this should greatly help in planning future trials targeting cognitive impairment.
Etiologic Stroke Subtype and Risk of Post-Stroke Cognitive Decline
Prior studies have suggested that cortical, as opposed to subcortical strokes, are more frequently associated with cognitive impairment,41 with support from studies demonstrating higher rates of impairment in individuals with large-vessel or cardioembolic strokes.37 However, few longitudinal studies have systematically examined the association of stroke subtype with PSCID, and even fewer studies studied ethnically diverse US populations13 or the differential effect of stroke subtype on the domains of cognitive impairment.69 Of all the ischemic stroke subtypes, lacunar (SVD) has been the most extensively studied. In the Secondary Prevention of Small Subcortical Strokes (SPS3) Trial, neuropsychological testing was performed at study entry, 2 weeks to 6 months following the index stroke. Among the 1636 who received testing in English, 47 % were classified as having mild cognitive impairment (MCI).70 Among the 117 who received testing in Spanish, 40 % were classified as having mild cognitive impairment.13 A meta-analysis of 24 studies with 7575 patients found the prevalence of MCI or dementia post-stroke to be similar between lacunar (29%) and non-lacunar stroke (24%) (OR 0.72; 95% CI 0.43 to 1.20), but data were limited by short follow-up, subtype classification methods and confounding and there was substantial heterogeneity between studies.71 Some72,73 but not all studies found PSCID to be more common in Oxfordshire subtype categories of total or partial anterior circulation infarction compared with lacunar or posterior circulation infarction. Few studies have compared cognitive outcomes across Trial of ORG 10172 in Acute Stroke Treatment (TOAST) subtype categories. A study in China found an increased risk of PSCID at 3 months post-stroke for large artery compared to lacunar stroke (OR 1.42; 95% CI 1.06-1.90).73 A study in Norway found no differences in cognitive impairment at 3 and 18 months among TOAST subtypes in a global statistical test, but the risk was also lowest in lacunar stroke.69
Hemorrhagic stroke (HS) is the most severe form of stroke, accounting for ~50% of stroke related morbidity and mortality.74,75 Intracerebral hemorrhage (ICH) and aneurysmal subarachnoid hemorrhage (aSAH) account for over 90% of all HS events and lead to clinically significant cognitive decline in up to 50% of HS survivors.76–79 Despite their impact on post-stroke cognitive outcomes, HS subtypes have been the topic of limited dedicated PSCID investigations to date. As previously mentioned, stroke anatomical location is likely to affect risk of PSCID. Because ICH/aSAH anatomical location is not defined by arterial or venous vascular territories (as in ischemic stroke), larger hematomas may well affect multiple brain area/networks relevant to PSCID. These considerations prompted incorporation of dedicated methodologies in DISCOVERY HS sub-study. In addition, specific pathophysiology mechanisms are likely to be relevant to PSCID risk after ICH or aSAH. Because of the pathophysiological role played by cerebral SVD in primary ICH, imaging and neuropathology markers of microvascular disease presence / severity have been associated with dementia risk after ICH.76,77 However, the exact mechanisms linking SVD to PSCID after primary ICH remains poorly understood. In aSAH, delayed cerebral ischemia (DCI) has been identified as a key predictor of PSCID, but the biological mechanisms accounting for these findings are poorly understood at best.79 DISCOVERY offers novel, targeted strategies to identify HS survivors at high risk for PSCID, explore relevant biological mechanisms, and therefore guide future investigative efforts aimed at improving long-term cognitive outcomes after HS.
Pathophysiology of Post-Stroke Cognitive Impairment/Dementia and Gaps in Knowledge
There is a consensus that cognitive impairment or dementia resulting from a vascular insult of any type constitutes vascular cognitive impairment (VCI) or vascular dementia.80 Whether caused by progressive, insidious accumulation of subcortical microvascular pathology burden (including “silent” brain infarcts, diffuse white matter disintegration detected on T2-MRI as white matter hyperintensities (WMH), cerebral microbleeds, enlarged perivascular spaces, and cortical microinfarcts) or caused by a single stroke event that affects brain structures critical for cognition, vascular contribution to cognitive impairment and dementia is now broadly recognized as a highly prevalent yet significantly understudied entity.81 Further, since VCID may be modifiable, there is a great impetus for rapid advancement in knowledge in this field.82 Despite the established associations between stroke, neurodegenerative pathology, and dementia, there is however a lack of knowledge regarding the specific stroke subtypes (ischemic versus hemorrhagic, vessel types and sizes, anatomical locations) and magnitude of stroke events which cause PSCID (Figure 1).83,84 Further, the complexity of interaction between the pre-existing pathology in the brain and an acute stroke insult serving as a trigger or accelerator of cognitive decline in the vulnerable brain requires the scope, size, and a systematic approach offered by DISCOVERY.85
Figure 1. Brain susceptibility to post-stroke cognitive impairment and dementia.

A complex interaction between life-course exposures to multiple vascular risks and socio-demographic factors, pre-existing burden of cerebral small vessel disease and Alzheimer’s and related neurodegenerative pathology in the brain, the effect of strategic acute stroke lesions, and the mediating effect of genomic and epigenomic variation contribute to brain susceptibility (or resilience) to cognitive decline after stroke. An acute stroke event, whether ischemic or hemorrhagic, likely initiates or exacerbates/accelerates a series of pathological events leading to post-stroke cognitive impairment or dementia.
At the center of any brain dysfunction related to vascular insult is the neurovascular unit (NVU), the smallest building block of the brain parenchyma that emphasizes the unique, interdependent relationship between the brain cells and the cerebral vasculature.86–88 The NVU’s ability to withstand or succumb to the insults related to cerebrovascular dysfunction, metabolic disarray, proteinopathy, or inflammatory responses constitutes what has been recently referred to as “brain health.”89 Mechanisms of disease in this case includes the NVU as the common final pathway, but the specific etiologies define potentially identifiable targets for interventions to prevent brain’s susceptibility to dementia, stroke and other prevalent ways of health failures.90
Several cell types including neurons, glia (astrocytes, microglia and oligodendrocytes), and vascular cells (endothelial cells, pericytes and vascular smooth muscle cells) comprise NVU.91 Some of the most critical roles of the NVU are to regulate cerebral blood flow in response to increasing functional demands and to ensure intact brain parenchymal milieu serving as the building block of the blood-brain barrier (BBB).92,93 Bidirectional molecular transport across the BBB is highly regulated with exception of the essential deliveries (e.g., diffusion of oxygen and carbon dioxide, small liposoluble particles <400kDa). Associated with increased BBB permeability, microvascular dysfunction contributes to impaired mechanisms of clearance as well as “unauthorized entry” by neurotoxic molecules from the blood stream, which ultimately leads to neurodegeneration.88,89 Specifically, cerebrovascular damage – such as that from the impact of life-course exposure to multiple vascular risk factors like hypertension, diabetes mellitus, or smoking – serves as the primary insult to the NVU and the BBB, which is both necessary and sufficient to initiate neuronal injury and neurodegeneration through resting CBF reductions and accumulation of neurotoxic plasma proteins (fibrinogen, plasminogen, thrombin etc).94,95 However, it may also facilitate accumulation of the Alzheimer’s toxin, amyloid-β peptide (Aβ), in the brain through diminished clearance and increased production of Aβ.96,97 These two pathways referred to respectively as Aβ-independent and Aβ-dependent, predictably interact in the brain and a largely considered to be synergistic in the brain that ultimately succumbs to cognitive impairment/dementia.88,89
While there is general agreement that specific stroke events may either accelerate processes of AD/ADRD and microvascular dysfunction in a vulnerable brain, or unmask their pre-existing burden, leading to PSCID, the mechanisms of susceptibility to cognitive dysfunction after stroke remain unclear.83,84 Conversely, data are lacking on the protective factors that constitute brain’s ability to withstand the effects of acute insult or allow the brain to recover fully and rapidly to its pre-stroke level of function, i.e. the mechanisms of brain resilience in stroke. We identified a number of important questions to be addressed systematically by DISCOVERY to bridge the existing gap in knowledge in the field of PSCID (Table 1).
Table 1.
Knowledge gaps in post-stroke cognitive decline to be addressed by DISCOVERY.
| Knowledge gap | Plans to address in DISCOVERY |
|---|---|
| The role of an acute insult on outcomes after stroke | |
| 1.The effects of acute stroke type (ischemic and hemorrhagic), lesion size, and location | Detailed acute imaging characterization including vascular territory, vessel size, vascularity status assessment, infarct and hematoma characteristics including cortical-subcortical, lobar-deep, multiplicity of lesions, brain structures affected, hemorrhagic transformation, edema, vascular occlusions, joint multi-modal modeling using machine learning and radiomics analysis |
| 2. Etiologic stroke subtype and the combined effect of vascular risk profile, antecedent co-morbidities, and functional baseline | Analysis of age, sex, race, ethnicity and other sociodemographic determinants, vascular risk factors, other co-morbidities, baseline functional status, social support structure |
| 3. The effects of acute stroke magnitude (clinical stroke severity) and post-stroke course (hospitalization and long-term) | Include acute treatments, complications, discharge destination, recurrent events, social supports, depression, functional recovery. |
| 4. The interaction with pre-existing burden of disease | MRI and CT markers of white matter disease and other SVD, brain volume and atrophy, ventricular size, prior silent brain infarcts, SVD score, vascularity |
| 5. The effect of genetic susceptibility | Whole exome sequencing at baseline, DNA methylation at Follow-up 1 & 2 (genome-wide and epigenome-wide association studies) |
| 6.The role of blood biomarkers of neurodegeneration, inflammation, neuroaxonal and vascular injury | Blood draw at baseline, and at 3-6 and 18 months after stroke |
| The mechanisms underlying PSCID | |
| 1.Synergistic effects of AD features (Aβ and tau) | PET and plasma biomarkers with acute stroke features |
| 2.Progression of chronic neurodegeneration and SVD pathology in relation to PSCID | 3T MRI with morphometric, structural and functional connectivity, and perfusion MRI assessment in relation to acute stroke features, stroke subtypes, patient characteristics, and personalized “multi-omics” signature |
|
Personalized approach to prediction and prevention of PSCID | |
| 1.A practical “bedside” clinical tool | Development of the DISCOVERY Score, a clinical prediction tool |
| 2.A tool for selection of the patients into clinical trials | Developing a sophisticated, granular characterization of disease subtype using multimodal personalized biomarker data |
Abbreviations: AD – Alzheimer’s disease, CT – computer tomography, MRI – magnetic resonance imaging, PET – positron emission tomography, PSCID – post-stroke cognitive impairment and dementia, SVD – small vessel disease
Scientific Objectives & Specific Aims of DISCOVERY
The central hypothesis in DISCOVERY is that a stroke event (including acute ischemic stroke, AIS; ICH; or aSAH), in an already vulnerable brain, precipitates cascading pathological events ultimately resulting in PSCID. To address this hypothesis, we proposed the DISCOVERY Network, a collaborative of 30 clinical sites with access to large diverse acute stroke populations and expertise and capacity to systematically assess for PSCID (Figure 2). This is the first time a project of such scale has brought together the components of a multi-center acute stroke clinical trial (including screening and enrollment of patients at the time of index stroke hospital admission) and a longitudinal nested-cohort study with cognitive and functional assessments and multidimensional/multimodal research tools, including blood and imaging biomarkers. Developing the scientific framework of DISCOVERY required expertise in acute stroke, SVD, VCID, AD/ADRD, health disparities, and multi-center research.
Figure 2. The DISCOVERY Network.
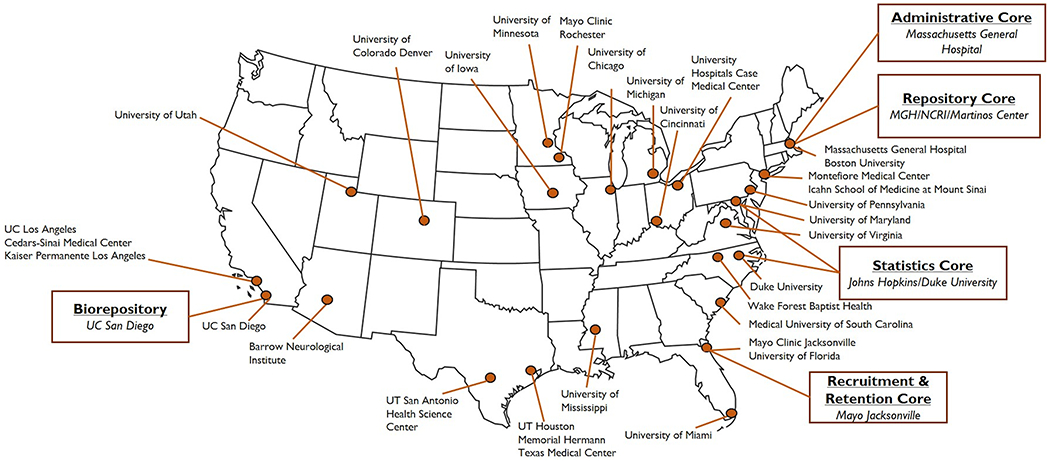
The network is comprised of four study cores (Administrative, Recruitment and Retention, Statistical, and Repository) and thirty clinical performance sites across the United States.
Mandated by the National Institutes of Health, the Network’s overarching goals are to determine: 1) which specific subsets of stroke events cause (or do not cause) PSCID and 2) which additional demographic (sex, race, and ethnicity), clinical factors and comorbidities that synergize with the acute stroke to result in or prevent PSCID. Expanding well beyond these goals, the overall scientific objective of DISCOVERY is to elucidate mechanisms of brain resilience and/or susceptibility to PSCID in diverse US populations based on complex interplay between life-course exposure to multiple vascular risk factors, pre-existing burden of SVD and AD/ADRD pathology, the effect of strategic acute stroke lesions, and the mediating effect of genomic and epigenomic variation. Specifically, the DISCOVERY aims to: 1) identify the independent and combined effects of the acute stroke lesion, pre-existing SVD and AD/ADRD burden, and baseline markers of brain resilience on PSCID, 2) determine the role of acute stroke as a critical factor in accelerating AD/ADRD and SVD pathology leading to PSCID, and 3) develop generalizable personalized-medicine models for individual patient outcome prediction and patient selection for clinical trials.
Overall Study Design and Timeline
DISCOVERY is a prospective, multi-center, observational, cohort study that will enroll 8,000 non-demented race/ethnically diverse patients with incident AIS, ICH, or aSAH admitted across 30 high-volume US stroke centers and will follow the participants for ≥2 years, with serial cognitive and functional evaluations, with subgroups undergoing detailed MR and PET imaging (Figure 3). Recruitment projections and statistical power considerations in DISCOVERY are included in supplemental material (Figure I). All patients will have standard-of-care (SOC) stroke evaluation and treatment on admission, and will undergo pre-stroke dementia screening before enrollment. During the inpatient phase, subjects will undergo baseline cognitive and functional outcomes assessments (Table 2). Baseline SOC parenchymal and vascular imaging, clinical variables and blood specimens for biomarker studies will be entered in the study database. In the outpatient phase, participants will be followed for ≥2 years through a series of in-person and telephone visits. Every participant who initially failed cognitive screen during their hospital admission will be re-screened by telephone within 6 weeks of the index stroke and will re-enter the study in the outpatient phase, if eligible. During the outpatient phase, all surviving subjects will be seen in two in-person clinic follow-up visits (at 3 to 6 months and 18 months). All clinic follow-up visits will occur at the DISCOVERY Network Clinical Performance Sites (CPS) that will be designated as Tier 1, 2, or 3 (Figure 2) based on infrastructure, resources, and proficiency to perform in-depth neurocognitive assessments, advanced 3T protocol MRI scans, and Aβ and tau PET imaging. Every DISCOVERY participant will undergo serial centralized telephone-based cognitive and functional outcomes assessments conducted by the Telephonic Assessment Center (TAC) team at the Mayo Clinic (Jacksonville, FL) at 12 months post-stroke, and annually thereafter for the study’s duration. DISCOVERY participants who are unable to attend in-person assessments at 3 to 6 or 18 months will be assessed via Virtual Visit (teleneurology), or by phone (TAC), in order to compile the minimum necessary PSCID dataset for analysis. The DISCOVERY study design offers solutions for a number of key methodological challenges often faced by the previous studies of post-stroke cognitive impairment and dementia (Table I).
Figure 3. The DISCOVERY Study schema.
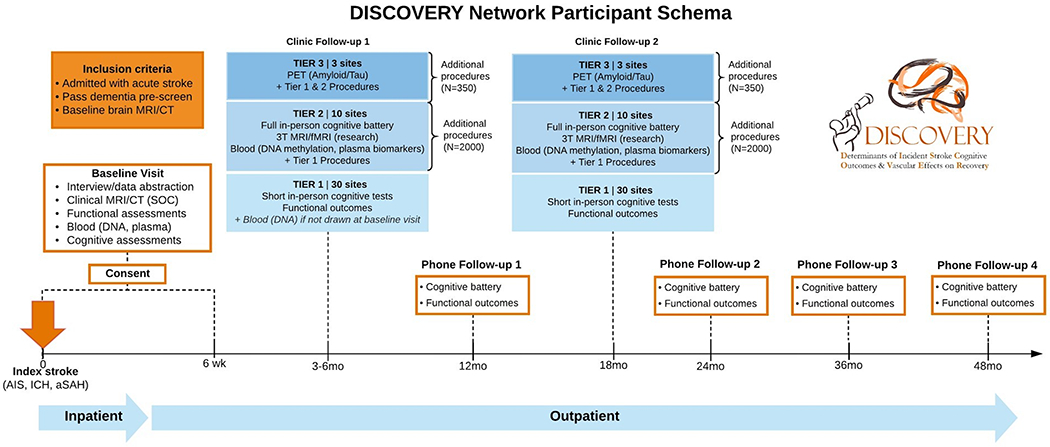
Patients diagnosed with acute ischemic stroke, intracranial hemorrhage, and aneurysmal subarachnoid hemorrhage will be enrolled during the index stroke admission (Inpatient Phase), undergo baseline cognitive and functional outcomes assessments, and will be followed for ≥2 years through a series of in-person and phone research visits (Outpatient Phase). During the outpatient phase, all surviving subjects will be seen in two clinic follow-up visits (at 3-6 months and 18 months). All clinic follow-up visits will occur at the DISCOVERY Network Clinical Sites that will be designated as Tier 1, 2, or 3 based on infrastructure, resources, and proficiency to perform in-depth neurocognitive assessments, advanced 3T protocol MRI scans, and PET imaging. Every DISCOVERY subject will have serial centralized phone-based cognitive and functional outcomes assessments at 12 months post-stroke, and annually thereafter for the study’s duration.
Table 2.
Cognitive and functional assessments in DISCOVERY.
| Baseline | Clinic Follow-Up 1 & 2 | Telephonic Assessment | ||||
|---|---|---|---|---|---|---|
| Cognitive | Functional | Cognitive | Functional | Cognitive | Functional | |
| Tier 1 | DISCOVERY t-MoCA,* Line cancellation test |
Pre-stroke and discharge mRS, BI, NIHSS, PROMIS-10 Global Health, | DISCOVERY t-MoCA* | NIHSS, mRS, BI, PROMIS-10 Global Health, SSQ-short, PHQ-9 | DISCOVERY t-MoCA,* AD8 (informant) |
T-NIHSS, mRS, PROMIS-10 Global Health, SMF |
| Tier 2/3 | DISCOVERY full cognitive battery,** ORRT |
|||||
DISCOVERY t-MoCA Battery: MoCA (domain: global); CERAD Word List Memory Task (domain: immediate, delayed memory); Number Span Test - Forward/Backward (domain: attention).
DISCOVERY Full Cognitive Battery: MoCA (domain: global), CERAD Word List Memory Task – Immediate/Delayed (domain: memory); Benson Complex Figure Copy – Immediate/Delayed (domain: visuospatial); Trail Making Test – A/B (domain: executive function/processing speed); Letter Digit Substitution (domain: : executive function/processing speed); Number Span Test - Forward/Backward (domain: attention); Craft 21 Story Recall – Immediate/Delayed (domain: memory); Verbal Fluency – Phonemic (domain: executive function/processing speed); Category Fluency (domain: language); CES-D (domain: depression); CDR (informant) (domain: cognitive status); MBI-C (informant)(domain: neuropsychiatric status).
Abbreviations: AD – Alzheimer’s Dementia, BI – Barthel index, CDR – Clinical Dementia Rating scale, CES-D – Centers for Epidemiologic Studies Depression scale, MBI-C – Mild Behavioral Impairment Checklist, MoCA – Montreal Cognitive Assessment scale, NIHSS – National Institutes of Health Stroke Scale, ORRT – Oral Reading Recognition Test, PHQ – Patient Health Questionnaire, PROMIS – Patient-Reported Outcomes Measurement Information System, SMF – Subjective memory Form, SSQ – Social Support Questionnaire, t-MoCA – telephonic MoCA, T-NIHSS – telephonic NIHSS.
Approach to Cognitive Assessment in DISCOVERY
Evaluation of cognition in the post-stroke setting must consider: 1) the role and value of repeated cognitive assessment; 2) the timing of the assessment and the pre-stroke cognitive status, and 3) the problem of attrition, in general, cognitive change, as can be analyzed with repeated cognitive assessment, allows less confounded measurement of cognitive performance, due to less reliance on sociodemographic factors than when cognition is measured at a single time point. Cognitive performance at a single time point is related to social and demographic factors, including educational level98 and childhood cognitive function;99 this relationship is especially pronounced in Blacks (vs Whites), in whom the benefit in performance from education is especially large.8 Risk of dementia is >60% higher in the Atherosclerosis Risk in Community (ARIC)’s least vs most educated participants,100 but when change in cognition is considered, education does not impact 20-year cognitive decline.101 Consideration of cognitive change, however, is not possible for pre to post-stroke evaluation in a study that recruits at the time of the incident stroke, such as in DISCOVERY, but repeated assessments over the years post-stroke will allow consideration of these trajectories. In addition, it is critical to consider appropriate normative data, to more accurately adjudicate PSCID in relevant disparities populations.
To account for pre-stroke cognitive status, because DISCOVERY is a study of post-stroke dementia, it is critical to exclude any individuals who already have dementia at the time of stroke, even if not formally diagnosed by a physician. The use of the IQCODE102 allows to exclude those individuals with probable pre-existing dementia, and truly measure incident PSCID after index stroke. As data are collected on individuals throughout the course of the study, their cognitive performance will be tracked and adjudicated, using standardized definitions of MCI and dementia whenever possible, with the understanding that the post-stroke setting may require distinct consideration of time course and functional impairment, as many patients experience functional impairment for non-cognitive reasons post-stroke. The first year post-stroke may represent a time when early cognitive impairment is identified but when we cannot confidently give a diagnosis of dementia, and in DISCOVERY, we hope to understand the link between these early changes and a persistent dementia diagnosis beyond that time period.
Finally, attrition is a highly important consideration in any longitudinal study of cognition. Studies evaluating long-term cognitive trajectories are potentially susceptible to attrition, from death as well as dropout. Importantly, cognitive impairment is a risk factor for attrition,103 as is stroke, even among enrollees in clinical trials.104 Thus, the potential risk of attrition in the stroke population is especially high, and if those individuals at greatest risk for a poor outcome are less likely to attend visits, dementia rates could appear lower, as shown in the OXVASC study, where 17% of individuals with TIA and stroke who came to full clinic follow-ups were diagnosed with dementia, vs 45% in the TIA and stroke population without complete in-person assessment.105 Other studies report similar discrepancies, with higher rates of dementia among the non-examined. 106,107 Thus, evaluation of cognitive outcomes in a stroke cohort must include not only a robust retention plan, but also appropriate statistical methods to account for attrition, as some of it may be unavoidable (e.g. due to death or other competing illness). Such methods include inverse probability of attrition weighting (IPAW), which up-weights a study population to its original makeup.108,109 Multiple Imputation with Chained Equations (MICE), another approach to addressing attrition, reduces the impact of missingness (from attrition or death) by imputing results, including outcome, for missing data points.
Building a Data Management System for Future Success
The management and sharing of multi-modal data generated by multi-site projects is a challenging endeavor. Making data useful within the project means creating a data management infrastructure that integrates, rather than silos, data through meticulously documenting, collecting and making available metadata from multiple project domains. Interest in data sharing has driven the construction of repositories and tools that recognize the challenges of integration and the importance of well-documented metadata and has led to guiding principles such as FAIR from Force11 that address these issues.110 FAIR stands for “findable”, “accessible”, “interoperable”, and “reusable”. The DISCOVERY Repository follows the FAIR principles and we expect that adherence to those principles will maximize utilization of this unique data set.
The DISCOVERY Repository system provides a web portal that serves as the main entry point into the project’s data management capabilities. The portal provides project information, access to project documents, as well as modules to register the acquisition of imaging and biofluid data and record clinical and neuropsychological assessment instrument data. The Repository is built to provide fully integrated access to all the data generated in DISCOVERY. The DISCOVERY Repository leverages and integrates the Entrepôt image management system, NeuroBank electronic data capture system and Virtual Biorepository (Figure II), with the infrastructure and experience of the Biospecimens repository developed to build an integrated management infrastructure that can store, move, and share data from all DISCOVERY domains. In addition, DISCOVERY uses the Globus data transfer service for movement of project data, both for the collection of data from the Clinical Performing Sites and for the distribution to the various Cores and analysis centers. We also deploy an extensive suite of tools to for quality control for data, biospecimens and images as well as tools and workflows for integrity checking of the integrated data.
The scientific aims of the DISCOVERY Repository are to: 1) create an integrated data management infrastructure that follows the best practices for data management established by MarkVCID consortium and NIH guidance documents, 2) develop a repository infrastructure that will allow data to be “findable” and “accessible”, and 3) create a metadata infrastructure that will allow data to be “interoperable” and “reusable”. In this last aim, the DISCOVERY repository leverages work by other NIH repositories and ontology-development groups to create metadata that maximizes interoperability, using well-established terms and common data elements wherever possible, so that data consumers are able to understand and successfully reuse DISCOVERY data. The rich set of metadata will be used not only to aid in the development of processing and analysis pipelines, but will also be used by both the Statistics and Recruitment and Retention Cores to generate operational reports and track participants.
Neuroimaging Biomarkers of Post-Stroke Cognitive Impairment/Dementia
Neuroimaging is a key research tool in DISCOVERY (Figure III), with neuroimage analysis strategy built upon the existing body of evidence regarding the effects of pre-existing MRI-detectable brain disease and its role in functional and cognitive outcomes following a superimposed acute stroke event.
Acute image analysis.
The acute images obtained during hospitalization of every eligible stroke patient in DISCOVERY will serve as the largest to-date, prospective clinical stroke imaging repository linked to the rich clinical and detailed outcome assessment data. An acute infarct on DWI MRI will be confirmed during enrollment of AIS patients, while hemorrhagic stroke patients are expected to have an ICH or aSAH on computer tomography (CT)/CT angiogram (CTA). Sequential images obtained during the index admission or imaging including additional modalities (MR angiography, digital subtraction angiography, CT or MR perfusion images) will be also collected, if available. These data will be critical in several lines of analytical inquiries within DISCOVERY including: (1) the effect of size and topography of acute stroke lesion on stroke severity and outcomes, (2) the effect of pre-existing brain pathology on stroke severity and outcomes, (3) the contribution of imaging to stroke subtyping and disease classification in DISCOVERY, and (4) the interaction between clinical and neuroimaging phenotypes on outcomes in complex models of novel constructs such as effective brain reserve, rich-club organization, lesion network mapping, vascularity assessment, and brain health assessment. These data will be analyzed using multi-modal, automated, big-data approaches to large, multi-center imaging repositories comprised of 1.5T MRI and CT scans obtained as part of hospital care and will utilize novel computational approached developed to address the challenges of this type of high-volume, low-quality imaging data.
Longitudinal MRI analysis and PET imaging.
Cerebrovascular and AD/ADRD pathologies frequently coexist, 111 altering cognitive trajectories of aging adults112. Data are however lacking on the impact of acute stroke event on either accelerating or unmasking – the pathologic cascades in the brain leading to PSCID. Using research MRI and PET protocols, we will focus on discerning the underlying brain mechanisms that lead to PSCID.
3T MRI imaging.
Longitudinal analyses of 3T research protocol MRI for a subset of DISCOVERY participants (n=2000) with representative stroke subtypes and health disparity populations at two timepoints (3-6months and 18 months post-stroke) presents an experimental framework for assessment of the MRI markers of cognitive decline. We will acquire high quality imaging data using multi-site implementation of MR protocols that will leverage cutting edge image acquisition (e.g. multi-band acceleration) and also employ reproducible processing methodologies that can measure subtle changes across the two time-points. Specifically, we will acquire the following data: structural MRI (sMRI) for brain structure changes, FLAIR MRI and SWI for vascular assessments, diffusion MRI for microstructural changes and structural connectivity changes (using traditional DTI models as well as advanced biophysical models such as neurite orientation and dispersion and density imaging, NODDI), resting-state functional (rsfMRI) for functional connectivity changes, and arterial spin labeling perfusion (ASL) methods for perfusion changes. These detailed structural and functional changes on 3T MRI scans will play an important role for mapping post-stroke brain changes and identifying key features predictive of PSCID.
PET imaging.
Leveraging recent standardization efforts15,113–116 and using the emerging plasma as well as PET biomarkers for AD, we have a unique opportunity to investigate how AD pathophysiology and the acute stroke impact cognitive decline and neurodegenerative processes. In a subset of 350 subjects selected from the nested cohort of 2,000 stroke survivors at Tier 3 Network sites, we will conduct PET imaging at two time points (3-6 and 18 months) to assess for synergistic effects of acute stoke features and AD biomarkers (Aβ and tau) on cognitive decline and burden of AD/ADRD pathology progression. This longitudinal PET substudy is complementary to the multi-tier approach to testing the hypothesis regarding acute stroke events accelerating, or unmasking, the burden of AD/RD pathology in the brain and would allow for a rare mechanistic evaluation of underlying biology of PSCID. In addition to testing the effect of baseline plasma amyloid and tau on cognitive decline in the entire DISCOVERY cohort (Tier 1), and the relationship between plasma amyloid and tau and structural/functional MRI markers of SVD/ND progression at Tier 2 studies, we will also use composite metrics for baseline amyloid and tau levels on PET and evaluate the association of the PET biomarkers with stroke event in predicting future PSCID, trajectories of cognitive decline, and association with MRI disease progression (Tier 3). This study will also test if the acute stroke event accelerates the accumulation of amyloid and tau longitudinally. The availability of both plasma biomarkers and PET scans in the same subjects will also allow us to correlate the PET composite metrics for amyloid and tau with plasma amyloid and tau measures to validate the plasma biomarkers we use in the first two tiers of hypothesis testing.
DISCOVERY Study Fluid Biomarker Strategy
Fluid-based biomarkers are readily accessible to a greater subset of the healthcare environment and offer a promise of personalized medicine117, when tested as a targeted, hypothesis-driven tool for screening and validation of underlying disease biology in stroke populations. The DISCOVERY study’s fluid biomarker strategy is designed to interrogate the contribution of multiple potential pathways that may converge to drive PSCID (Figure 4):
Figure 4. The DISCOVERY Network Fluid Biomarker Strategy.
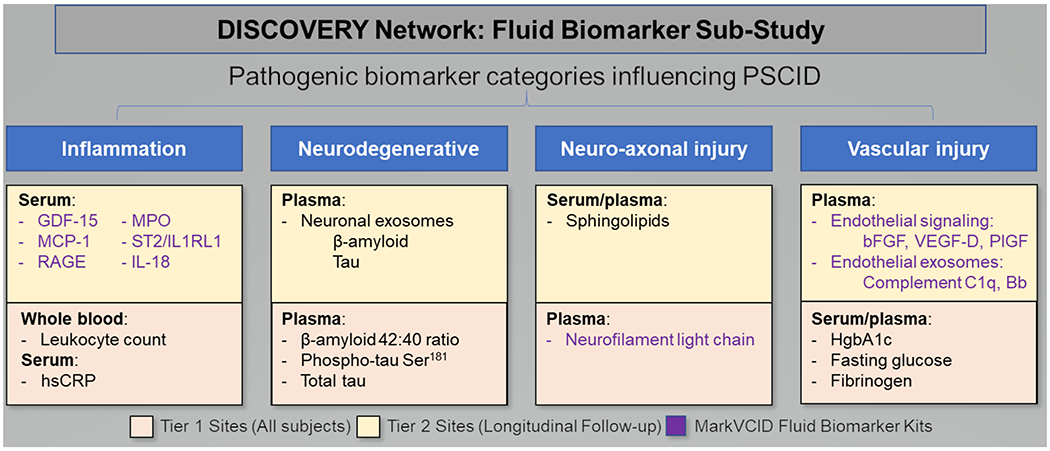
All enrolled subjects (Tier 1) will undergo a baseline measure of circulating biomarkers in the proposed pathogenic categories influencing post-stroke cognitive impairment/dementia. Tier 2 subjects will participate in longitudinal biomarker assessment using emerging biomarkers including several biomarker kits established by the MarkVCID Consortium.
Inflammation.118,119
Emerging data from MarkVCID and ARIC suggests that an aggregate serum measure of peripheral inflammatory markers is associated with WMH and silent cerebrovascular injury.120,121 Therefore, baseline measurements of inflammation will be critical to identifying individuals at risk for PSCID. Moreover, the degree of inflammation appears to vary among racial and ethnic groups;122,123 thus, measures of inflammation may serve an valuable role in evaluating differences in PSCID among racial and ethnic groups.
Neurodegeneration.
Concurrence of AD/ADRD and cerebrovascular (SVD) pathologies on post-mortem studies and neuroimaging of patients with stroke and dementia124–126 compels our team to study the burden of ND changes at stroke onset and how it modifies the development of PSCID. CSF measures of neurodegeneration are quite reliable 127, however, obtaining CSF in post-stroke subjects is burdensome, potentially dangerous (given the use of anticoagulants/dual antiplatelet agents), and likely to introduce a selection bias for less-affected individuals. Existing data suggest that low plasma β-amyloid ratios (42:40)128,129 and plasma total and phosphorylated isoforms of tau (p-tau181, p-tau217)130–132 are predictive of cognitive decline in cognitively normal or MCI subjects.133,134
Neuro-axonal injury.
Plasma neurofilament light chain (pNfl) level is emerging as a sensitive indicator for neuro-axonal injury in acute stroke, SVD135 and AD/ADRD136,137. While pNfl lacks specificity, its utility in evaluating PSCID will be to quantitatively define the baseline burden of SVD and/or AD/ADRD pathologies while also helping to determine if stroke alone triggers a progressive axonal degeneration that identify those at increased risk for PSCID.
Vascular injury.
Individuals presenting with stroke often have an underlying risk profile that favors ongoing cerebrovascular injury due to hypertension, diabetes, other VRFs, also linked with poor cognition.65 In addition, endothelial-specific (CD31+/CD146+) exosomes (EDEs) shed with higher levels of brain-specific cargo proteins are enriched in individuals with WMH138 and EDEs are also undergoing biomarker validation in MarkVCID. Understanding the contribution of ongoing endothelial injury can drive therapeutic interventions aimed at tightening risk factor control thereby minimizing the risk for PSCID.
A targeted fluid-based biomarker strategy offers a novel, thorough, hypothesis-driven approach to insight into pathophysiologic mechanisms of PSCID and building personalized outcome prediction models.
Genetics and Genomics Strategy in DISCOVERY
Mechanisms of brain resilience to PSCID are based on the complex interplay between genetic susceptibility and environmental factors (life-course exposure to multiple vascular risks (VRFs), or use of protective lifestyle factors) that can be interrogated using a systematic and informed “omics” and fluid biomarker strategy. The DISCOVERY investigators have been instrumental in defining the landscape of genetic discovery in large-scale, population-based studies of stroke139, VCID-related phenotypes140,141, and dementia, including multiethnic genome-wide association study (GWAS)142–146, and a recent GWAS highlighting the role of common variation in post-stroke outcomes147,148.
GWAS and next-generation (whole exome sequencing, WES) studies have made substantial progress towards identifying the genetic loci that influence risk of stroke and its subtypes149, AD150, MRI-defined endophenotypes of VCID143,151, and their VRFs. Certain genes such as APOE152, FOXF2146 and ATP5H153 have been independently related to both the risks of stroke and AD. Such genetic information provides powerful means to examine mechanisms of PSCID risk and trajectories and their link to VRFs, stroke subtypes, and AD/ADRD and MRI-related endophenotypes.
Injury and recovery after stroke are dependent on a set of processes that involve altered orchestrated gene expression.
The epigenome describes the set of dynamic molecular modifications that regulate gene expression independent of gene sequence.154 DNA methylation (DNAm) is the most studied epigenetic modification, is “plastic” and highly sensitive to interventions and changes over time.155,156 Using epigenome-wide DNAm profiles in African-American ARIC participants, a unique DNAm signature (accelerated epigenetic aging) has been identified in association with increased WMH burden, an MRI-phenotype highly relevant to VCID and post-stroke dementia.145 Changes in global DNAm following a stroke have been described and suggest that DNAm influences cell death post-stroke through silencing of neuroprotective genes, but is also implicated in repair mechanisms such as synaptic plasticity and neurogenesis.157 Whether these global changes in DNAm influences trajectories of PSCID has not been investigated, nor have specific epigenetic signatures of the trajectories of PSCID been identified.
In DISCOVERY, we will examine whether PSCID risk after specific stroke subtype is linked to genetic susceptibility (detected via WES, GWAS, and epigenome-wide association studies). We will undertake genetic and multi-omic studies in DISCOVERY to: (a) identify the genetics and biological pathways that determine resilience and recovery from an acute stroke, thus potentially identifying novel biomarkers and drug targets; (b) utilize polygenic risk scores as prognostic indicators for risk stratification in clinical trials and as aggregate measures of genetic propensity to explore gene-environment interactions; (c) use Mendelian randomization strategies, wherein genetic determinants of a putative risk factor or biomarker (related to stroke outcomes) are used as instrumental variables to examine whether observed association is causal. Identifying the genetics of recovery from stroke, DNAm signatures of PSCID trajectories, and integrating the “omics” data has the potential to uncover novel molecular targets that reflect the contribution of genetic and non-genetic risk factors to post-stroke outcomes.
Summary: The Promise of DISCOVERY
The vision of DISCOVERY is to dramatically reduce the rates on post-stroke disability by preventing cognitive decline and dementia in high-risk US populations based on their stroke events type or the underlying vulnerability to PSCID. The limitations to consider for this study in achieving its aims include potential selection bias in enrollment and follow-up, limited statistical power for subgroup analyses (e.g., PET imaging), the constraints of cognitive assessment in aphasic patients, and as of recent, the potential impact of the COVID-19 pandemic on the diverse study populations. However, the fundamental success of this project will be ensured by the key innovations and central elements of the study including the collective experience and expertise of the study scientific leadership team, the geographically and populationally diverse high-volume network clinical performance site structure, and the innovative two-pronged approach of combining a large-scale prospective cohort study with multi-tiered highly mechanistic sub-studies nested within. Within the framework of DISCOVERY, a rigorous, multimodal, and systematic characterization of stroke events and comorbid factors that increase susceptibility to PSCID will serve as the starting point for future work developing personalized post-stroke interventions for PSCID, including prevention, treatment and rehabilitation. Further, a large-scale study such as DISOCVERY will allow consideration of race and ethnicity in PSCID and address key disparities in rates of not only stroke but also dementia.
Supplementary Material
Acknowledgement
We would like to thank the DISCOVERY study research personnel and collaborators at the Administrative, Recruitment and Retention, Statistical/Cognitive, and Repository Cores, and the DISCOVERY clinical performance sites. Further, we are grateful to our colleagues locally, nationally, and around the globe for continuous support and council.
Funding:
DISCOVERY is jointly supported by the NINDS and NIA (U19NS115388).
Disclosures:
Dr. Rost is in part supported by NINDS/NIA U19NS115388, NINDS R01NS082285, NINDS R01NS086905, and she serves as Associate Editor of Stroke.
Dr. Meschia is in part supported by the NINDS/NIA U19NS115388, NINDS U01NS080168, and he serves as Section Editor for Genetics, Genomics, and Precision Medicine of Stroke.
Dr. Gottesman is in part supported by NINDS/NIA U19NS115388, NHLBI U01HL096812, NIA R01AG040282, K24AG052573, RF1AG050745, and she served as past Associate Editor of Neurology.
Dr. Wruck is in part supported by NINDS/NIA U19NS115388.
Dr. Helmer is in part supported by NINDS/NIA U19NS115388.
Dr. Greenberg is in part supported by NINDS/NIA U19NS115388, NINDS U24NS107154, U24NS100591, R01NS096730, and NIA R01AG026484.
Non-standard Abbreviations and Acronyms
- AD/ADRD
Alzheimer disease/Alzheimer disease-related dementia
- AIS
acute ischemic stroke
- ARIC
the atherosclerosis risk in community study
- ARCADIA-CSI
the atrial cardiopathy and antithrombotic drugs in prevention after cryptogenic stroke – cognition and silent infarcts trial
- ASL
arterial spin labeling
- aSAH
aneurysmal subarachnoid hemorrhage
- BBB
blood-brain barrier
- CPS
clinical performance site
- CREST
the carotid revascularization endarterectomy versus stenting trial
- CSF
cerebrospinal fluid
- CT/A
computer tomography/angiography
- DISCOVERY
the determinants of incident stroke cognitive outcomes and vascular effects on recovery study
- DNAm
deoxyribonucleic acid methylation
- DTI
diffusion tensor imaging
- DWI
diffusion weighted imaging
- EDE
endothelial-specific endosomes
- FLAIR
fluid attenuated inversion recovery
- GWAS
genome-wide association study
- HS
hemorrhagic stroke
- ICH
intracerebral hemorrhage
- IPAW
inverse probability of attrition weighting
- IQCODE
the informant questionnaire on cognitive decline in the elderly
- HYVET-COG
the hypertension in the very elderly cognition trial
- MCI
mild cognitive impairment
- MICE
multiple imputation with chained equations
- MoCA
the Montreal cognitive assessment test
- MMSE
mini-mental state exam
- MRI
magnetic resonance imaging
- ND
neurodegeneration
- NIH
National Institutes of Health
- NODDI
neurite orientation and dispersion and density imaging
- NVU
neurovascular unit
- OXVASC
the Oxford vascular study
- PET
positron emission tomography
- pNFL
plasma neurofilament light chain
- PSCID
post-stroke cognitive impairment and dementia
- SOC
standard of care
- SPRINT-MIND
the systolic blood pressure intervention trial
- SVD
small vessel disease
- SWI
susceptibility weighted imaging
- TAC
the telephonic assessment center
- TIA
transient ischemic attack
- TOAST
the trial of ORG 10172 in acute stroke treatment
- VCID
vascular cognitive impairment/dementia
- VISP
the vitamin intervention for stroke prevention trial
- VRF
vascular risk factor
- WES
whole exome sequencing
- WMH
white matter hyperintensity
- US
the United States
APPENDIX (Study Group): The DISCOVERY Investigators
Kevin Barrett, MD (Mayo Clinic Jacksonville);
Alessandro Biffi, MD (Massachusetts General Hospital);
Bernadette Boden-Albala, PhD (UC Irvine);
Myriam Fornage, PhD (University of Texas Houston);
Mark Etherton MD, PhD (Massachusetts General Hospital);
Polina Golland, PhD (Massachusetts Institute of Technology);
Jonathan Graff-Radford, MD (Mayo Clinic Rochester);
Jason Hinman, MD, PhD (University of California Los Angeles);
Cliff Jack Jr, MD (Mayo Clinic Rochester);
Jayashree Kalpathy-Cramer, PhD (MGH Martinos Center for Biomedical Imaging);
David Knopman, MD (Mayo Clinic Rochester);
Steven Kittner, MD (U of Maryland);
Val Lowe, MD (Mayo Clinic Rochester);
Jennifer Manly, PhD (Columbia University);
Thomas Mosley, PhD (University of Mississippi);
Ronald Petersen, MD (Mayo Clinic Rochester);
Robert Rissman, PhD (University of California San Diego);
Markus Schirmer, PhD (Massachusetts General Hospital);
Kristin Schwab (Massachusetts General Hospital);
Sudha Seshadri, MD (University of Texas San Antonio);
Alexander Sherman (Massachusetts General Hospital);
Prashanthi Vemuri, PhD (Mayo Clinic Rochester);
Anand Viswanathan, MD, PhD (Massachusetts General Hospital).
REFERENCES
- 1.Kyu HH, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, Abbastabar H, Abd-Allah F, Abdela J, Abdelalim A, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet. 2018;392:1859–1922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, De SF, Floyd J, Fornage M, Gillespie C, et al. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation. 2017;135:e146–e603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rist PM, Chalmers J, Arima H, Anderson C, Macmahon S, Woodward M, Kurth T, Tzourio C. Baseline cognitive function, recurrent stroke, and risk of dementia in patients with stroke. Stroke. 2013;44:1790–1795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Douiri A, Rudd AG, Wolfe CDA. Prevalence of poststroke cognitive impairment: South London Stroke Register 1995–2010. Stroke. 2013;44:138–145. [DOI] [PubMed] [Google Scholar]
- 5.Ihle-Hansen H, Thommessen B, Wyller TB, Engedal K, Øksengård AR, Stenset V, Løken K, Aaberg M, Fure B. Incidence and subtypes of MCI and dementia 1 year after first-ever stroke in patients without pre-existing cognitive impairment. Dement Geriatr Cogn Disord. 2011;32:401–407. [DOI] [PubMed] [Google Scholar]
- 6.Jacquin A, Binquet C, Rouaud O, Graule-Petot A, Daubail B, Osseby G- V, Bonithon-Kopp C, Giroud M, Béjot Y. Post-stroke cognitive impairment: high prevalence and determining factors in a cohort of mild stroke. J. Alzheimers Dis. 2014;40:1029–1038. [DOI] [PubMed] [Google Scholar]
- 7.Sachdev PS, Brodaty H, Valenzuela MJ, Lorentz L, Looi JCL, Berman K, Ross A, Wen W, Zagami AS. Clinical determinants of dementia and mild cognitive impairment following ischaemic stroke: the Sydney Stroke Study. Dement Geriatr Cogn Disord. 2006;21:275–283. [DOI] [PubMed] [Google Scholar]
- 8.Ivan CS, Seshadri S, Beiser A, Au R, Kase CS, Kelly-Hayes M, Wolf PA. Dementia after stroke: the Framingham Study. Stroke. 2004;35:1264–1268. [DOI] [PubMed] [Google Scholar]
- 9.Mok VCT, Wong A, Lam WWM, Fan YH, Tang WK, Kwok T, Hui ACF, Wong KS. Cognitive impairment and functional outcome after stroke associated with small vessel disease. J. Neurol. Neurosurg. Psychiatry. 2004;75:560–566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zietemann V, Georgakis MK, Dondaine T, Müller C, Mendyk A-M, Kopczak A, Hénon H, Bombois S, Wollenweber FA, Bordet R, et al. Early MoCA predicts long-term cognitive and functional outcome and mortality after stroke. Neurology. 2018;91:e1838–e1850. [DOI] [PubMed] [Google Scholar]
- 11.Melkas S, Oksala NKJ, Jokinen H, Pohjasvaara T, Vataja R, Oksala A, Kaste M, Karhunen PJ, Erkinjuntti T. Poststroke dementia predicts poor survival in long-term follow-up: influence of prestroke cognitive decline and previous stroke. J. Neurol. Neurosurg. Psychiatry. 2009;80:865–870. [DOI] [PubMed] [Google Scholar]
- 12.Levine DA, Wadley VG, Langa KM, Unverzagt FW, Kabeto MU, Giordani B, Howard G, Howard VJ, Cushman M, Judd SE, et al. Risk Factors for Poststroke Cognitive Decline: The REGARDS Study (Reasons for Geographic and Racial Differences in Stroke). Stroke. 2018;49:987–994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jacova C, Pearce LA, Roldan AM, Arauz A, Tapia J, Costello R, McClure LA, Hart RG, Benavente OR. Cognitive performance following lacunar stroke in Spanish-speaking patients: results from the SPS3 trial. Int J Stroke. 2015;10:519–528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Montine TJ, Koroshetz WJ, Babcock D, Dickson DW, Galpern WR, Glymour MM, Greenberg SM, Hutton ML, Knopman DS, Kuzmichev AN. Recommendations of the Alzheimer’s disease–related dementias conference. Neurology. 2014;83:851–860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gorelick PB, Scuteri A, Black SE, Decarli C, Greenberg SM, Iadecola C, Launer LJ, Laurent S, Lopez OL, Nyenhuis D, et al. Vascular contributions to cognitive impairment and dementia: a statement for healthcare professionals from the american heart association/american stroke association. Stroke. 2011;42:2672–2713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kalaria RN. Neuropathological diagnosis of vascular cognitive impairment and vascular dementia with implications for Alzheimer’s disease. Acta Neuropathol. 2016;131:659–685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Vemuri P, Lesnick TG, Przybelski SA, Knopman DS, Preboske GM, Kantarci K, Raman MR, Machulda MM, Mielke MM, Lowe VJ, et al. Vascular and amyloid pathologies are independent predictors of cognitive decline in normal elderly. Brain. 2015;138:761–771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Schneider JA, Arvanitakis Z, Bang W, Bennett DA. Mixed brain pathologies account for most dementia cases in community-dwelling older persons. Neurology. 2007;69:2197–2204. [DOI] [PubMed] [Google Scholar]
- 19.Schneider JA, Wilson RS, Bienias JL, Evans DA, Bennett DA. Cerebral infarctions and the likelihood of dementia from Alzheimer disease pathology. Neurology. 2004;62:1148–1155. [DOI] [PubMed] [Google Scholar]
- 20.Toledo JB, Arnold SE, Raible K, Brettschneider J, Xie SX, Grossman M, Monsell SE, Kukull WA, Trojanowski JQ. Contribution of cerebrovascular disease in autopsy confirmed neurodegenerative disease cases in the National Alzheimer’s Coordinating Centre. Brain. 2013;136:2697–2706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Pendlebury ST, Rothwell PM. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: a systematic review and meta-analysis. Lancet Neurol. 2009;8:1006–1018. [DOI] [PubMed] [Google Scholar]
- 22.Ye BS, Seo SW, Kim J-H, Kim GH, Cho H, Noh Y, Kim HJ, Yoon CW, Woo S-Y, Kim SH, et al. Effects of amyloid and vascular markers on cognitive decline in subcortical vascular dementia. Neurology. 2015;85:1687–1693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Boyle PA, Yu L, Wilson RS, Leurgans SE, Schneider JA, Bennett DA. Person‐specific contribution of neuropathologies to cognitive loss in old age. Annals of neurology. 2018;83:74–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Wilcock D, Jicha G, Blacker D, Albert M, D’Orazio L, Elahi F, Fornage M, Hinman J, Knoefel J, Kramer J, et al. MarkVCID cerebral small vessel consortium: I. Enrollment, clinical, fluid protocols. Alzheimers Dement. 2020;in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lu H, Kashani A, Arfanakis K, Caprihan A, DeCarli C, Gold B, Li Y, Maillard P, Satizabal C, Stables L, et al. MarkVCID cerebral small vessel consortium: II. MarkVCID Neuroimaging protocols. Alzheimers Dement. 2020;in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gladman JT, Corriveau RA, Debette S, Dichgans M, Greenberg SM, Sachdev PS, Wardlaw JM, Biessels GJ. Vascular contributions to cognitive impairment and dementia: research consortia that focus on etiology and treatable targets to lessen the burden of dementia worldwide. Alzheimer’s & Dementia: Translational Research & Clinical Interventions. 2019;5:789–796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sachdev PS, Lo JW, Crawford JD, Mellon L, Hickey A, Williams D, Bordet R, Mendyk A-M, Gelé P, Deplanque D. STROKOG (stroke and cognition consortium): An international consortium to examine the epidemiology, diagnosis, and treatment of neurocognitive disorders in relation to cerebrovascular disease. Alzheimer’s & Dementia: Diagnosis, Assessment & Disease Monitoring. 2017;7:11–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sachdev P, Kalaria R, O’Brien J, Skoog I, Alladi S, Black SE, Blacker D, Blazer D, Chen C, Chui H. Diagnostic criteria for vascular cognitive disorders: a VASCOG statement. Alzheimer disease and associated disorders. 2014;28:206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Skrobot OA, Black SE, Chen C, DeCarli C, Erkinjuntti T, Ford GA, Kalaria RN, O’Brien J, Pantoni L, Pasquier F. Progress toward standardized diagnosis of vascular cognitive impairment: guidelines from the Vascular Impairment of Cognition Classification Consensus Study. Alzheimer’s & Dementia. 2018;14:280–292. [DOI] [PubMed] [Google Scholar]
- 30.Narasimhalu K, Ang S, De Silva DA, Wong M-C, Chang H-M, Chia K-S, Auchus AP, Chen C. Severity of CIND and MCI predict incidence of dementia in an ischemic stroke cohort. Neurology. 2009;73:1866–1872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Mok VC, Lam BY, Wang Z, Liu W, Au L, Leung EY, Chen S, Yang J, Chu WC, Lau AY. Delayed-onset dementia after stroke or transient ischemic attack. Alzheimer’s & Dementia. 2016;12:1167–1176. [DOI] [PubMed] [Google Scholar]
- 32.Pendlebury ST, Rothwell PM, Oxford Vascular Study. Incidence and prevalence of dementia associated with transient ischaemic attack and stroke: analysis of the population-based Oxford Vascular Study. Lancet Neurol. 2019;18:248–258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Yang J, Wong A, Wang Z, Liu W, Au L, Xiong Y, Chu WW, Leung EY, Chen S, Lau C. Risk factors for incident dementia after stroke and transient ischemic attack. Alzheimer’s & Dementia. 2015;11:16–23. [DOI] [PubMed] [Google Scholar]
- 34.Hilal S, Chai YL, Ikram MK, Elangovan S, Yeow TB, Xin X, Chong JY, Venketasubramanian N, Richards AM, Chong JP. Markers of cardiac dysfunction in cognitive impairment and dementia. Medicine. 2015;94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Weaver NA, Zhao L, Biesbroek JM, Kuijf HJ, Aben HP, Bae H-J, Caballero MÁ, Chappell FM, Chen CP, Dichgans M. The Meta VCI Map consortium for meta-analyses on strategic lesion locations for vascular cognitive impairment using lesion-symptom mapping: Design and multicenter pilot study. Alzheimer’s & Dementia: Diagnosis, Assessment & Disease Monitoring. 2019;11:310–326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Levine DA, Galecki AT, Langa KM, Unverzagt FW, Kabeto MU, Giordani B, Wadley VG. Trajectory of Cognitive Decline After Incident Stroke. JAMA. 2015;314:41–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Jaillard A, Naegele B, Trabucco-Miguel S, LeBas JF, Hommel M. Hidden dysfunctioning in subacute stroke. Stroke. 2009;40:2473–2479. [DOI] [PubMed] [Google Scholar]
- 38.Turunen KEA, Laari SPK, Kauranen TV, Uimonen J, Mustanoja S, Tatlisumak T, Poutiainen E. Domain-Specific Cognitive Recovery after First-Ever Stroke: A 2-Year Follow-Up. J Int Neuropsychol Soc. 2018;24:117–127. [DOI] [PubMed] [Google Scholar]
- 39.Jaillard A, Grand S, Le Bas JF, Hommel M. Predicting cognitive dysfunctioning in nondemented patients early after stroke. Cerebrovasc. Dis. 2010;29:415–423. [DOI] [PubMed] [Google Scholar]
- 40.Corbetta M, Ramsey L, Callejas A, Baldassarre A, Hacker CD, Siegel JS, Astafiev SV, Rengachary J, Zinn K, Lang CE, et al. Common behavioral clusters and subcortical anatomy in stroke. Neuron. 2015;85:927–941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Nys GMS, van Zandvoort MJE, de Kort PLM, Jansen BPW, de Haan EHF, Kappelle LJ. Cognitive disorders in acute stroke: prevalence and clinical determinants. Cerebrovasc. Dis. 2007;23:408–416. [DOI] [PubMed] [Google Scholar]
- 42.Duering M, Righart R, Wollenweber FA, Zietemann V, Gesierich B, Dichgans M. Acute infarcts cause focal thinning in remote cortex via degeneration of connecting fiber tracts. Neurology. 2015;84:1685–1692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Cremers LGM, de Groot M, Hofman A, Krestin GP, van der Lugt A, Niessen WJ, Vernooij MW, Ikram MA. Altered tract-specific white matter microstructure is related to poorer cognitive performance: The Rotterdam Study. Neurobiol. Aging. 2016;39:108–117. [DOI] [PubMed] [Google Scholar]
- 44.Jacobs HIL, Leritz EC, Williams VJ, Van Boxtel MPJ, van der Elst W, Jolles J, Verhey FRJ, McGlinchey RE, Milberg WP, Salat DH. Association between white matter microstructure, executive functions, and processing speed in older adults: the impact of vascular health. Hum Brain Mapp. 2013;34:77–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.López-Olóriz J, López-Cancio E, Arenillas JF, Hernández M, Dorado L, Dacosta-Aguayo R, Barrios M, Soriano-Raya JJ, Miralbell J, Bargalló N, et al. Diffusion tensor imaging, intracranial vascular resistance and cognition in middle-aged asymptomatic subjects. Cerebrovasc. Dis. 2014;38:24–30. [DOI] [PubMed] [Google Scholar]
- 46.Windham BG, Deere B, Griswold ME, Wang W, Bezerra DC, Shibata D, Butler K, Knopman D, Gottesman RF, Heiss G, et al. Small Brain Lesions and Incident Stroke and Mortality: A Cohort Study. Ann Intern Med. 2015;163:22–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Koton S, Schneider ALC, Windham BG, Mosley TH, Gottesman RF, Coresh J. Microvascular Brain Disease Progression and Risk of Stroke: The ARIC Study. Stroke. 2020;51:3264–3270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Baykara E, Gesierich B, Adam R, Tuladhar AM, Biesbroek JM, Koek HL, Ropele S, Jouvent E, Alzheimer’s Disease Neuroimaging Initiative, Chabriat H, et al. A Novel Imaging Marker for Small Vessel Disease Based on Skeletonization of White Matter Tracts and Diffusion Histograms. Ann. Neurol. 2016;80:581–592. [DOI] [PubMed] [Google Scholar]
- 49.Duering M, Finsterwalder S, Baykara E, Tuladhar AM, Gesierich B, Konieczny MJ, Malik R, Franzmeier N, Ewers M, Jouvent E. Free water determines diffusion alterations and clinical status in cerebral small vessel disease. Alzheimer’s & Dementia. 2018;14:764–774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Wen HM, Mok VCT, Fan YH, Lam WWM, Tang WK, Wong A, Huang RX, Wong KS. Effect of white matter changes on cognitive impairment in patients with lacunar infarcts. Stroke. 2004;35:1826–1830. [DOI] [PubMed] [Google Scholar]
- 51.Zhao L, Wong A, Luo Y, Liu W, Chu WWC, Abrigo JM, Lee RKL, Mok V, Shi L. The Additional Contribution of White Matter Hyperintensity Location to Post-stroke Cognitive Impairment: Insights From a Multiple-Lesion Symptom Mapping Study. Front Neurosci. 2018;12:290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Ballard CG, Morris CM, Rao H, O’Brien JT, Barber R, Stephens S, Rowan E, Gibson A, Kalaria RN, Kenny RA. APOE epsilon4 and cognitive decline in older stroke patients with early cognitive impairment. Neurology. 2004;63:1399–1402. [DOI] [PubMed] [Google Scholar]
- 53.Wagle J, Farner L, Flekkøy K, Wyller TB, Sandvik L, Eiklid KL, Fure B, Stensrød B, Engedal K. Association between ApoE epsilon4 and cognitive impairment after stroke. Dement Geriatr Cogn Disord. 2009;27:525–533. [DOI] [PubMed] [Google Scholar]
- 54.Skolarus LE, Sharrief A, Gardener H, Jenkins C, Boden-Albala B. Considerations in Addressing Social Determinants of Health to Reduce Racial/Ethnic Disparities in Stroke Outcomes in the United States. Stroke. 2020;51:3433–3439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Reshetnyak E, Ntamatungiro M, Pinheiro LC, Howard VJ, Carson AP, Martin KD, Safford MM. Impact of Multiple Social Determinants of Health on Incident Stroke. Stroke. 2020;51:2445–2453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Elkind MSV, Lisabeth L, Howard VJ, Kleindorfer D, Howard G. Approaches to Studying Determinants of Racial-Ethnic Disparities in Stroke and Its Sequelae. Stroke. 2020;51:3406–3416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Clark DG, Boan AD, Sims-Robinson C, Adams RJ, Amella EJ, Benitez A, Lackland DT, Ovbiagele B. Differential Impact of Index Stroke on Dementia Risk in African-Americans Compared to Whites. J Stroke Cerebrovasc Dis. 2018;27:2725–2730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Levine DA, Kabeto M, Langa KM, Lisabeth LD, Rogers MAM, Galecki AT. Does Stroke Contribute to Racial Differences in Cognitive Decline? Stroke. 2015;46:1897–1902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Rajan KB, Schneider JA, Aggarwal NT, Wilson RS, Everson-Rose SA, Evans DA. Racial Differences in Cognitive Function and Risk of Incident Stroke. J Stroke Cerebrovasc Dis. 2015;24:2854–2859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Gilsanz P, Mayeda ER, Glymour MM, Quesenberry CP, Whitmer RA. Association Between Birth in a High Stroke Mortality State, Race, and Risk of Dementia. JAMA Neurol. 2017;74:1056–1062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Spence JD, Howard VJ, Chambless LE, Malinow MR, Pettigrew LC, Stampfer M, Toole JF. Vitamin Intervention for Stroke Prevention (VISP) trial: rationale and design. Neuroepidemiology. 2001;20:16–25. [DOI] [PubMed] [Google Scholar]
- 62.Toole JF, Malinow MR, Chambless LE, Spence JD, Pettigrew LC, Howard VJ, Sides EG, Wang C-H, Stampfer M. Lowering homocysteine in patients with ischemic stroke to prevent recurrent stroke, myocardial infarction, and death: the Vitamin Intervention for Stroke Prevention (VISP) randomized controlled trial. JAMA. 2004;291:565–575. [DOI] [PubMed] [Google Scholar]
- 63.Hachinski V, Iadecola C, Petersen RC, Breteler MM, Nyenhuis DL, Black SE, Powers WJ, DeCarli C, Merino JG, Kalaria RN, et al. National Institute of Neurological Disorders and Stroke-Canadian Stroke Network vascular cognitive impairment harmonization standards. Stroke. 2006;37:2220–2241. [DOI] [PubMed] [Google Scholar]
- 64.Peters R, Beckett N, Forette F, Tuomilehto J, Clarke R, Ritchie C, Waldman A, Walton I, Poulter R, Ma S, et al. Incident dementia and blood pressure lowering in the Hypertension in the Very Elderly Trial cognitive function assessment (HYVET-COG): a double-blind, placebo controlled trial. Lancet Neurol. 2008;7:683–689. [DOI] [PubMed] [Google Scholar]
- 65.SPRINT MIND Investigators for the SPRINT Research Group, Williamson JD, Pajewski NM, Auchus AP, Bryan RN, Chelune G, Cheung AK, Cleveland ML, Coker LH, Crowe MG, et al. Effect of Intensive vs Standard Blood Pressure Control on Probable Dementia: A Randomized Clinical Trial. JAMA. 2019;321:553–561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.SPRINT Research Group, Wright JT, Williamson JD, Whelton PK, Snyder JK, Sink KM, Rocco MV, Reboussin DM, Rahman M, Oparil S, et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N Engl J Med. 2015;373:2103–2116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Howard VJ, Meschia JF, Lal BK, Turan TN, Roubin GS, Brown RD, Voeks JH, Barrett KM, Demaerschalk BM, Huston J, et al. Carotid revascularization and medical management for asymptomatic carotid stenosis: Protocol of the CREST-2 clinical trials. Int J Stroke. 2017;12:770–778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Marshall RS, Lazar RM, Liebeskind DS, Connolly ES, Howard G, Lal BK, Huston J, Meschia JF, Brott TG. Carotid revascularization and medical management for asymptomatic carotid stenosis - Hemodynamics (CREST-H): Study design and rationale. Int J Stroke. 2018;13:985–991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Aam S, Einstad MS, Munthe-Kaas R, Lydersen S, Ihle-Hansen H, Knapskog A-B, Ellekjær H, Seljeseth Y, Saltvedt I. Post-stroke Cognitive Impairment-Impact of Follow-Up Time and Stroke Subtype on Severity and Cognitive Profile: The Nor-COAST Study. Front Neurol. 2020;11:699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Jacova C, Pearce LA, Costello R, McClure LA, Holliday SL, Hart RG, Benavente OR. Cognitive impairment in lacunar strokes: the SPS3 trial. Ann Neurol. 2012;72:351–362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Makin SDJ, Turpin S, Dennis MS, Wardlaw JM. Cognitive impairment after lacunar stroke: systematic review and meta-analysis of incidence, prevalence and comparison with other stroke subtypes. J Neurol Neurosurg Psychiatry. 2013;84:893–900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Narasimhalu K, Lee J, Leong YL, Ma L, De Silva DA, Wong MC, Chang HM, Chen C. Inflammatory markers and their association with post stroke cognitive decline. Int J Stroke. 2015;10:513–518. [DOI] [PubMed] [Google Scholar]
- 73.He M, Wang J, Liu N, Xiao X, Geng S, Meng P, Ji N, Sun Y, Xu B, Xu Y, et al. Effects of Blood Pressure in the Early Phase of Ischemic Stroke and Stroke Subtype on Poststroke Cognitive Impairment. Stroke. 2018;49:1610–1617. [DOI] [PubMed] [Google Scholar]
- 74.Poon MTC, Fonville AF, Al-Shahi Salman R. Long-term prognosis after intracerebral haemorrhage: systematic review and meta-analysis. J. Neurol. Neurosurg. Psychiatry. 2014;85:660–667. [DOI] [PubMed] [Google Scholar]
- 75.Zacharia BE, Hickman ZL, Grobelny BT, DeRosa P, Kotchetkov I, Ducruet AF, Connolly ES. Epidemiology of aneurysmal subarachnoid hemorrhage. Neurosurg. Clin. N. Am. 2010;21:221–233. [DOI] [PubMed] [Google Scholar]
- 76.Biffi A, Bailey D, Anderson CD, Ayres AM, Gurol EM, Greenberg SM, Rosand J, Viswanathan A. Risk Factors Associated With Early vs Delayed Dementia After Intracerebral Hemorrhage. JAMA Neurol. 2016;73:969–976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Benedictus MR, Hochart A, Rossi C, Boulouis G, Hénon H, van der Flier WM, Cordonnier C. Prognostic Factors for Cognitive Decline After Intracerebral Hemorrhage. Stroke. 2015;46:2773–2778. [DOI] [PubMed] [Google Scholar]
- 78.Al-Khindi T, Macdonald RL, Schweizer TA. Cognitive and functional outcome after aneurysmal subarachnoid hemorrhage. Stroke. 2010;41:e519–536. [DOI] [PubMed] [Google Scholar]
- 79.Stienen MN, Smoll NR, Weisshaupt R, Fandino J, Hildebrandt G, Studerus-Germann A, Schatlo B. Delayed cerebral ischemia predicts neurocognitive impairment following aneurysmal subarachnoid hemorrhage. World Neurosurg. 2014;82:e599–605. [DOI] [PubMed] [Google Scholar]
- 80.Smith EE. Clinical presentations and epidemiology of vascular dementia. Clin Sci (Lond). 2017;131:1059–1068. [DOI] [PubMed] [Google Scholar]
- 81.Rosenberg GA, Wallin A, Wardlaw JM, Markus HS, Montaner J, Wolfson L, Iadecola C, Zlokovic BV, Joutel A, Dichgans M, et al. Consensus statement for diagnosis of subcortical small vessel disease. J Cereb Blood Flow Metab 2016. January;36(1):6–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Hachinski V, Einhäupl K, Ganten D, Alladi S, Brayne C, Stephan BCM, Sweeney MD, Zlokovic B, Iturria‐Medina Y, Iadecola C, et al. Preventing dementia by preventing stroke: The Berlin Manifesto. Alzheimer’s & Dementia. 2019;15:961–984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Wong A, Mok V. Stroke: Poststroke cognitive impairment—what are we measuring? Nat Rev Neurol. 2015;11:487–488. [DOI] [PubMed] [Google Scholar]
- 84.Casolla B, Caparros F, Cordonnier C, Bombois S, Hénon H, Bordet R, Orzi F, Leys D. Biological and imaging predictors of cognitive impairment after stroke: a systematic review. J Neurol. 2019;266:2593–2604. [DOI] [PubMed] [Google Scholar]
- 85.Moskowitz MA, Lo EH, Iadecola C. The science of stroke: mechanisms in search of treatments. Neuron. 2010;67:181–198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Iadecola C Neurovascular regulation in the normal brain and in Alzheimer’s disease. Nat Rev Neurosci. 2004;5:347–360. [DOI] [PubMed] [Google Scholar]
- 87.Lo EH, Rosenberg GA. The neurovascular unit in health and disease: introduction. Stroke. 2009;40:S2–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Iadecola C The Neurovascular Unit Coming of Age: A Journey through Neurovascular Coupling in Health and Disease. Neuron. 2017;96:17–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Zlokovic BV. Neurovascular pathways to neurodegeneration in Alzheimer’s disease and other disorders. Nat Rev Neurosci. 2011;12:723–738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Iadecola C The pathobiology of vascular dementia. Neuron. 2013;80:844–866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Sweeney MD, Ayyadurai S, Zlokovic BV. Pericytes of the neurovascular unit: key functions and signaling pathways. Nat Neurosci. 2016;19:771–783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Yamazaki Y, Kanekiyo T. Blood-Brain Barrier Dysfunction and the Pathogenesis of Alzheimer’s Disease. Int J Mol Sci. 2017;18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Zhao Z, Nelson AR, Betsholtz C, Zlokovic BV. Establishment and Dysfunction of the Blood-Brain Barrier. Cell. 2015;163:1064–1078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Zlokovic BV. The blood-brain barrier in health and chronic neurodegenerative disorders. Neuron. 2008;57:178–201. [DOI] [PubMed] [Google Scholar]
- 95.Nelson AR, Sweeney MD, Sagare AP, Zlokovic BV. Neurovascular dysfunction and neurodegeneration in dementia and Alzheimer’s disease. Biochim Biophys Acta. 2016;1862:887–900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Sagare AP, Bell RD, Zlokovic BV. Neurovascular defects and faulty amyloid-β vascular clearance in Alzheimer’s disease. J Alzheimers Dis. 2013;33 Suppl 1:S87–100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Ramanathan A, Nelson AR, Sagare AP, Zlokovic BV. Impaired vascular-mediated clearance of brain amyloid beta in Alzheimer’s disease: the role, regulation and restoration of LRP1. Front Aging Neurosci. 2015;7:136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Barnes LL, Wilson RS, Hebert LE, Scherr PA, Evans DA, Mendes de Leon CF. Racial differences in the association of education with physical and cognitive function in older blacks and whites. J Gerontol B Psychol Sci Soc Sci. 2011;66:354–363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Whalley LJ, Starr JM, Athawes R, Hunter D, Pattie A, Deary IJ. Childhood mental ability and dementia. Neurology. 2000;55:1455–1459. [DOI] [PubMed] [Google Scholar]
- 100.Gottesman RF, Albert MS, Alonso A, Coker LH, Coresh J, Davis SM, Deal JA, McKhann GM, Mosley TH, Sharrett AR, et al. Associations Between Midlife Vascular Risk Factors and 25-Year Incident Dementia in the Atherosclerosis Risk in Communities (ARIC) Cohort. JAMA Neurol. 2017;74:1246–1254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Gottesman RF, Rawlings AM, Sharrett AR, Albert M, Alonso A, Bandeen-Roche K, Coker LH, Coresh J, Couper DJ, Griswold ME, et al. Impact of differential attrition on the association of education with cognitive change over 20 years of follow-up: the ARIC neurocognitive study. Am. J. Epidemiol. 2014;179:956–966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Jorm AF. A short form of the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE): development and cross-validation. Psychol Med. 1994;24:145–153. [DOI] [PubMed] [Google Scholar]
- 103.Burke SL, Hu T, Naseh M, Fava NM, O’Driscoll J, Alvarez D, Cottler LB, Duara R. Factors influencing attrition in 35 Alzheimer’s Disease Centers across the USA: a longitudinal examination of the National Alzheimer’s Coordinating Center’s Uniform Data Set. Aging Clin Exp Res. 2018; [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Gencheva E, Sloan M, Leurgans S, Raman R, Harris Y, Gorelick P, AAASPS Investigators. Attrition and non-compliance in secondary stroke prevention trials. Neuroepidemiology. 2004;23:61–66. [DOI] [PubMed] [Google Scholar]
- 105.Pendlebury ST, Chen P-J, Welch SJV, Cuthbertson FC, Wharton RM, Mehta Z, Rothwell PM, Oxford Vascular Study. Methodological Factors in Determining Risk of Dementia After Transient Ischemic Attack and Stroke: (II) Effect of Attrition on Follow-Up. Stroke. 2015;46:1494–1500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Zinn S, Dudley TK, Bosworth HB, Hoenig HM, Duncan PW, Horner RD. The effect of poststroke cognitive impairment on rehabilitation process and functional outcome. Arch Phys Med Rehabil. 2004;85:1084–1090. [DOI] [PubMed] [Google Scholar]
- 107.Desmond DW, Bagiella E, Moroney JT, Stern Y. The effect of patient attrition on estimates of the frequency of dementia following stroke. Arch. Neurol. 1998;55:390–394. [DOI] [PubMed] [Google Scholar]
- 108.Weuve J, Tchetgen Tchetgen EJ, Glymour MM, Beck TL, Aggarwal NT, Wilson RS, Evans DA, Mendes de Leon CF. Accounting for bias due to selective attrition: the example of smoking and cognitive decline. Epidemiology. 2012;23:119–128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Gottesman RF, Schneider ALC, Albert M, Alonso A, Bandeen-Roche K, Coker L, Coresh J, Knopman D, Power MC, Rawlings A, et al. Midlife hypertension and 20-year cognitive change: the atherosclerosis risk in communities neurocognitive study. JAMA Neurol. 2014;71:1218–1227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.The Future of Research Communications and e-Scholarship. The FAIR Data Principles [Internet]. FORCE11. 2014. [cited 2019 Apr 13];Available from: https://www.force11.org/group/fairgroup/fairprinciples
- 111.Schneider JA, Aggarwal NT, Barnes L, Boyle P, Bennett DA. The neuropathology of older persons with and without dementia from community versus clinic cohorts. J. Alzheimers Dis. 2009;18:691–701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Boyle PA, Yang J, Yu L, Leurgans SE, Capuano AW, Schneider JA, Wilson RS, Bennett DA. Varied effects of age-related neuropathologies on the trajectory of late life cognitive decline. Brain. 2017;140:804–812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Wardlaw JM, Smith EE, Biessels GJ, Cordonnier C, Fazekas F, Frayne R, Lindley RI, T O’Brien J, Barkhof F, Benavente OR. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. The Lancet Neurology. 2013;12:822–838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Deramecourt V, Slade JY, Oakley AE, Perry RH, Ince PG, Maurage C-A, Kalaria RN. Staging and natural history of cerebrovascular pathology in dementia. Neurology. 2012;78:1043–1050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Strozyk D, Dickson DW, Lipton RB, Katz M, Derby CA, Lee S, Wang C, Verghese J. Contribution of vascular pathology to the clinical expression of dementia. Neurobiol. Aging. 2010;31:1710–1720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Whitwell JL, Dickson DW, Murray ME, Weigand SD, Tosakulwong N, Senjem ML, Knopman DS, Boeve BF, Parisi JE, Petersen RC. Neuroimaging correlates of pathologically defined subtypes of Alzheimer’s disease: a case-control study. The Lancet Neurology. 2012;11:868–877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Hinman JD, Rost NS, Leung TW, Montaner J, Muir KW, Brown S, Arenillas JF, Feldmann E, Liebeskind DS. Principles of precision medicine in stroke. J. Neurol. Neurosurg. Psychiatry. 2017;88:54–61. [DOI] [PubMed] [Google Scholar]
- 118.Furlan JC, Vergouwen MDI, Fang J, Silver FL. White blood cell count is an independent predictor of outcomes after acute ischaemic stroke. Eur. J. Neurol. 2014;21:215–222. [DOI] [PubMed] [Google Scholar]
- 119.Elkind MSV, Luna JM, McClure LA, Zhang Y, Coffey CS, Roldan A, Del Brutto OH, Pretell EJ, Pettigrew LC, Meyer BC, et al. C-reactive protein as a prognostic marker after lacunar stroke: levels of inflammatory markers in the treatment of stroke study. Stroke. 2014;45:707–716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Walker KA, Gottesman RF, Wu A, Knopman DS, Gross AL, Mosley TH, Selvin E, Windham BG. Systemic inflammation during midlife and cognitive change over 20 years: The ARIC Study. Neurology. 2019;92:e1256–e1267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Altendahl M, Maillard P, Harvey D, Cotter D, Walters S, Wolf A, Singh B, Kakarla V, Azizkhanian I, Sheth SA, et al. An IL-18-centered inflammatory network as a biomarker for cerebral white matter injury. PLoS One. 2020;15:e0227835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Paalani M, Lee JW, Haddad E, Tonstad S. Determinants of inflammatory markers in a bi-ethnic population. Ethn Dis. 2011;21:142–149. [PMC free article] [PubMed] [Google Scholar]
- 123.Nazmi A, Victora CG. Socioeconomic and racial/ethnic differentials of C-reactive protein levels: a systematic review of population-based studies. BMC Public Health. 2007;7:212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Ringman JM, Monsell S, Ng DW, Zhou Y, Nguyen A, Coppola G, Van Berlo V, Mendez MF, Tung S, Weintraub S, et al. Neuropathology of Autosomal Dominant Alzheimer Disease in the National Alzheimer Coordinating Center Database. J. Neuropathol. Exp. Neurol. 2016;75:284–290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.McAleese KE, Firbank M, Dey M, Colloby SJ, Walker L, Johnson M, Beverley JR, Taylor JP, Thomas AJ, O’Brien JT, et al. Cortical tau load is associated with white matter hyperintensities. Acta Neuropathol Commun. 2015;3:60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Kim HJ, Park S, Cho H, Jang YK, San Lee J, Jang H, Kim Y, Kim KW, Ryu YH, Choi JY, et al. Assessment of Extent and Role of Tau in Subcortical Vascular Cognitive Impairment Using 18F-AV1451 Positron Emission Tomography Imaging. JAMA Neurol. 2018;75:999–1007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Blennow K, Hampel H, Weiner M, Zetterberg H. Cerebrospinal fluid and plasma biomarkers in Alzheimer disease. Nat Rev Neurol. 2010;6:131–144. [DOI] [PubMed] [Google Scholar]
- 128.Verberk IMW, Slot RE, Verfaillie SCJ, Heijst H, Prins ND, van Berckel BNM, Scheltens P, Teunissen CE, van der Flier WM. Plasma Amyloid as Prescreener for the Earliest Alzheimer Pathological Changes. Ann. Neurol. 2018;84:648–658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Graff-Radford NR, Crook JE, Lucas J, Boeve BF, Knopman DS, Ivnik RJ, Smith GE, Younkin LH, Petersen RC, Younkin SG. Association of low plasma Abeta42/Abeta40 ratios with increased imminent risk for mild cognitive impairment and Alzheimer disease. Arch. Neurol. 2007;64:354–362. [DOI] [PubMed] [Google Scholar]
- 130.Karikari TK, Pascoal TA, Ashton NJ, Janelidze S, Benedet AL, Rodriguez JL, Chamoun M, Savard M, Kang MS, Therriault J, et al. Blood phosphorylated tau 181 as a biomarker for Alzheimer’s disease: a diagnostic performance and prediction modelling study using data from four prospective cohorts. The Lancet Neurology. 2020;19:422–433. [DOI] [PubMed] [Google Scholar]
- 131.Thijssen EH, La Joie R, Wolf A, Strom A, Wang P, Iaccarino L, Bourakova V, Cobigo Y, Heuer H, Spina S, et al. Diagnostic value of plasma phosphorylated tau181 in Alzheimer’s disease and frontotemporal lobar degeneration. Nature Medicine. 2020;26:387–397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Palmqvist S, Janelidze S, Quiroz YT, Zetterberg H, Lopera F, Stomrud E, Su Y, Chen Y, Serrano GE, Leuzy A, et al. Discriminative Accuracy of Plasma Phospho-tau217 for Alzheimer Disease vs Other Neurodegenerative Disorders. JAMA. 2020;324:772–781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Mielke MM, Hagen CE, Wennberg AMV, Airey DC, Savica R, Knopman DS, Machulda MM, Roberts RO, Jack CR, Petersen RC, et al. Association of Plasma Total Tau Level With Cognitive Decline and Risk of Mild Cognitive Impairment or Dementia in the Mayo Clinic Study on Aging. JAMA Neurol. 2017;74:1073–1080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Pase MP, Beiser AS, Himali JJ, Satizabal CL, Aparicio HJ, DeCarli C, Chêne G, Dufouil C, Seshadri S. Assessment of Plasma Total Tau Level as a Predictive Biomarker for Dementia and Related Endophenotypes. JAMA Neurol. 2019; [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Gattringer T, Pinter D, Enzinger C, Seifert-Held T, Kneihsl M, Fandler S, Pichler A, Barro C, Gröbke S, Voortman M, et al. Serum neurofilament light is sensitive to active cerebral small vessel disease. Neurology. 2017;89:2108–2114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Lin Y-S, Lee W-J, Wang S-J, Fuh J-L. Levels of plasma neurofilament light chain and cognitive function in patients with Alzheimer or Parkinson disease. Sci Rep. 2018;8:17368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Mattsson N, Andreasson U, Zetterberg H, Blennow K, Alzheimer’s Disease Neuroimaging Initiative. Association of Plasma Neurofilament Light With Neurodegeneration in Patients With Alzheimer Disease. JAMA Neurol. 2017;74:557–566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Elahi FM, Casaletto KC, Altendahl M, Staffaroni AM, Fletcher E, Filshtein TJ, Glymour MM, Miller BL, Hinman JD, DeCarli C. “Liquid Biopsy” of White Matter Hyperintensity in Functionally Normal Elders. Frontiers in Aging Neuroscience. 2018;10:343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.NINDS Stroke Genetics Network (SiGN), International Stroke Genetics Consortium (ISGC). Loci associated with ischaemic stroke and its subtypes (SiGN): a genome-wide association study. Lancet Neurol. 2016;15:174–184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Traylor M, Malik R, Nalls MA, Cotlarciuc I, Radmanesh F, Thorleifsson G, Hanscombe KB, Langefeld C, Saleheen D, Rost NS, et al. Genetic variation at 16q24.2 is associated with small vessel stroke. Ann. Neurol. 2017;81:383–394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Traylor M, Tozer DJ, Croall ID, Lisiecka Ford DM, Olorunda AO, Boncoraglio G, Dichgans M, Lemmens R, Rosand J, Rost NS, et al. Genetic variation in PLEKHG1 is associated with white matter hyperintensities (n = 11,226). Neurology. 2019;92:e749–e757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Vojinovic D, Adams HH, Jian X, Yang Q, Smith AV, Bis JC, Teumer A, Scholz M, Armstrong NJ, Hofer E, et al. Genome-wide association study of 23,500 individuals identifies 7 loci associated with brain ventricular volume. Nat Commun. 2018;9:3945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Verhaaren BF, Debette S, Bis JC, Smith JA, Ikram MK, Adams HH, Beecham AH, Rajan KB, Lopez LM, Barral S. Multiethnic genome-wide association study of cerebral white matter hyperintensities on MRI. Circulation: Cardiovascular Genetics. 2015;8:398–409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Richard MA, Huan T, Ligthart S, Gondalia R, Jhun MA, Brody JA, Irvin MR, Marioni R, Shen J, Tsai P-C, et al. DNA Methylation Analysis Identifies Loci for Blood Pressure Regulation. Am. J. Hum. Genet. 2017;101:888–902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Raina A, Zhao X, Grove ML, Bressler J, Gottesman RF, Guan W, Pankow JS, Boerwinkle E, Mosley TH, Fornage M. Cerebral white matter hyperintensities on MRI and acceleration of epigenetic aging: the atherosclerosis risk in communities study. Clin Epigenetics. 2017;9:21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Neurology Working Group of the Cohorts for Heart and Aging Research in Genomic Epidemiology (CHARGE) Consortium, the Stroke Genetics Network (SiGN), and the International Stroke Genetics Consortium (ISGC). Identification of additional risk loci for stroke and small vessel disease: a meta-analysis of genome-wide association studies. Lancet Neurol. 2016;15:695–707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Söderholm M, Pedersen A, Lorentzen E, Stanne TM, Bevan S, Olsson M, Cole JW, Fernandez-Cadenas I, Hankey GJ, Jimenez-Conde J, et al. Genome-wide association meta-analysis of functional outcome after ischemic stroke. Neurology. 2019;92:e1271–e1283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Pfeiffer D, Chen B, Schlicht K, Ginsbach P, Abboud S, Bersano A, Bevan S, Brandt T, Caso V, Debette S, et al. Genetic Imbalance Is Associated With Functional Outcome After Ischemic Stroke. Stroke. 2019;50:298–304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Malik R, Chauhan G, Traylor M, Sargurupremraj M, Okada Y, Mishra A, Rutten-Jacobs L, Giese A-K, van der Laan SW, Gretarsdottir S, et al. Multiancestry genome-wide association study of 520,000 subjects identifies 32 loci associated with stroke and stroke subtypes. Nat. Genet. 2018;50:524–537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Kunkle BW, Grenier-Boley B, Sims R, Bis JC, Damotte V, Naj AC, Boland A, Vronskaya M, van der Lee SJ, Amlie-Wolf A. Genetic meta-analysis of diagnosed Alzheimer’s disease identifies new risk loci and implicates Aβ, tau, immunity and lipid processing. Nature genetics. 2019;51:414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Chauhan G, Adams HH, Satizabal CL, Bis JC, Teumer A, Sargurupremraj M, Hofer E, Trompet S, Hilal S, Smith AV. Genetic and lifestyle risk factors for MRI-defined brain infarcts in a population-based setting. Neurology. 2019;92:e486–e503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152.O’Donnell HC, Rosand J, Knudsen KA, Furie KL, Segal AZ, Chiu RI, Ikeda D, Greenberg SM. Apolipoprotein E genotype and the risk of recurrent lobar intracerebral hemorrhage. N. Engl. J. Med. 2000;342:240–245. [DOI] [PubMed] [Google Scholar]
- 153.Boada M, Antúnez C, Ramírez-Lorca R, DeStefano AL, González-Pérez A, Gayán J, López-Arrieta J, Ikram MA, Hernández I, Marín J, et al. ATP5H/KCTD2 locus is associated with Alzheimer’s disease risk. Mol. Psychiatry. 2014;19:682–687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Heerboth S, Lapinska K, Snyder N, Leary M, Rollinson S, Sarkar S. Use of epigenetic drugs in disease: an overview. Genet Epigenet. 2014;6:9–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Feinberg AP. Phenotypic plasticity and the epigenetics of human disease. Nature. 2007;447:433–440. [DOI] [PubMed] [Google Scholar]
- 156.Busche S, Shao X, Caron M, Kwan T, Allum F, Cheung WA, Ge B, Westfall S, Simon M-M, Multiple Tissue Human Expression Resource, et al. Population whole-genome bisulfite sequencing across two tissues highlights the environment as the principal source of human methylome variation. Genome Biol. 2015;16:290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Kassis H, Shehadah A, Chopp M, Zhang ZG. Epigenetics in Stroke Recovery. Genes (Basel). 2017;8 (3):89. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.