

Abstract
The etiology and outcomes of posterior reversible encephalopathy syndrome (PRES) in children with cancer are not well understood. We aim to determine the incidence of PRES, describe associated morbidity and mortality, and better understand risk factors in this patient population. 473 children with a hematologic malignancy or post-allogeneic hematopoietic cell transplantation (HCT) between June 2015 and June 2020 were screened for PRES to determine incidence and whether age or underlying diagnosis are associated with development of PRES. We conducted a case-control study to evaluate whether comorbidities or chemotherapeutic agents are associated with PRES. Children with PRES were matched with two controls based on age and underlying diagnosis to identify additional risk factors. Fourteen patients developed PRES, with an incidence of 5.9/1000 people/year. Those diagnosed with PRES had commonly described PRES symptoms: hypertension, seizures, nausea/vomiting, altered mental status, and headaches. All patients received an MRI, and most had findings consistent with PRES. HCT was associated with the development of PRES. The use of Etoposide was associated with PRES but comorbidities, steroids and calcineurin inhibitors were not. While PRES was infrequent in this population, it is associated with high morbidity and mortality, with ICU admissions and an overall hospital mortality, due to secondary causes, of 29%.
Keywords: PRES, pediatric oncology, case-control, retrospective cohort
Introduction
Posterior reversible encephalopathy syndrome (PRES) is a clinical diagnosis, often consisting of hypertension and neurologic changes. It is typically characterized by headache, altered mental status, visual changes, hypertension, and encephalopathy with brain magnetic resonance imaging (MRI) changes.1,2 Risk factors associated with development of PRES may include receiving immunosuppressive or cytotoxic therapies, autoimmune diseases, renal diseases, anemia, organ transplantation, and oncologic diagnoses.2,3,4 While it has been observed in children with various diagnoses, children with cancer or who are post-allogeneic hematopoietic cell transplant (HCT) seem to be a vulnerable population for development of PRES.5,6,7
The epidemiology of PRES is not well understood, especially in children with cancer. Studies1,8,9 have attempted to determine the incidence of PRES in specific pediatric populations. Definitions vary, specific risk factors are largely unknown, a definitive diagnostic test is not available, and the consequences of treatment are poorly understood. Further, the diagnosis of PRES is associated with significant morbidity as it often results in an ICU admission and cessation or reduction of ongoing cancer directed or immunosuppressive therapies. Despite often being reversible with rapid treatment, certain findings, such as seizures, may not resolve.1–2,4,5 Therefore, we aim to describe the incidence and characteristics of PRES in children with hematologic malignancies or who had received an allogeneic hematopoietic cell transplant for any indication at a single institution, Riley Hospital for Children. We also explored specific risk factors, treatments, and outcomes by quantifying the incidence, morbidity, and mortality of PRES in this patient population.
Materials and Methods
We conducted a retrospective cohort study of 473 children and young adults, aged 1 month to 25 years, diagnosed with a hematological malignancy or who were status-post allogeneic HCT for any indication between June 1, 2015 and June 1, 2020 at our institution. Hematological malignancies included leukemia and lymphoma. All allogeneic HCTs, regardless of indication, were included. Patients were screened for PRES during the study timeframe by two methods: 1) patients admitted to the ICU with a diagnosis of PRES, hypertensive emergency and/or encephalopathy, using ICD9 and 10 codes. and 2) all patients who received an MRIs. The electronic medical record was then thoroughly reviewed to determine diagnosis of PRES and to ensure inclusion criteria were met. The diagnosis of PRES was determined by documentation of a clinical diagnosis and/or radiographic evidence with supporting clinical symptoms in the electronic medical record. Patients with a clinical diagnosis of hypertension or who were on chronic anti-hypertensive medications were excluded. All data were collected using electronic medical records and stored on Research Electronic Data Capture10 (REDCap) system at Indiana University. IRB approval for this protocol was obtained prior to the start of the study.
Fourteen children were determined to have PRES. From this cohort we then conducted a case-control study to aid in exploring potential risk factors associated with the development of PRES. Fourteen children who developed a single episode of PRES were matched with two controls based on age, underlying malignancy or transplant status, and category of indication for transplant (malignancy, immunodeficiency, and non-malignant condition. Demographic information such as age, gender, race, and ethnicity was collected for all patients within the case-control group. Age of cancer diagnosis was recorded, as well as admission weight. Weight at time of hospital admission for oncology diagnosis (control group) or PRES diagnosis (PRES group). Multiple comorbidities, including renal disease, hemoglobinopathies, chronic pulmonary disease, prematurity, graft vs. host disease, and congenital heart disease were evaluated for their association with PRES. Chemotherapy, including all agents ever given and route of administration, was documented and investigated for an association with development of PRES.
Additional data were collected on the 14 patients who developed PRES. Age at PRES diagnosis and clinical symptoms of PRES were recorded. Vital signs, including systolic, diastolic, and mean arterial blood pressures, laboratory values, and fluid balance were collected on day 0, 1, and 2 of diagnosis. Lab values included a complete blood count (CBC) with differential and basic metabolic profile (BMP). Computerized tomography (CT) and MRI findings were examined. Antihypertensive agents use was recorded. PICU admission, length of stay, and interventions including intubation and arterial line placement were collected for relevant patients. Date of death and/or hospital discharge was also noted.
Data were analyzed to determine the incidence of PRES within the cohort over the 5-year period. Data are presented in medians and interquartile ranges or as frequencies and percentages. Continuous variables were compared with a Mann Whitney U test and categorical variables were compared with Chi Squared or Fisher Exact Test where appropriate. An exploratory multivariate logistic regression was completed for variables that were significantly associated with the development of PRES on univariable analysis.
Results
Demographic information for the cohort is represented in Table 1a. Out of 473 patients, 14 developed a single episode of PRES. Compared with patients without PRES, the median age of patients with PRES was lower, however, this was not statistically significant (p=0.421). Fewer patients with lymphoblastic leukemia developed PRES. Having received an allogeneic HCT was associated with the development of PRES (p=0.011) (Table 1a). Graft vs. host disease and use of steroids were not associated with the development of PRES. Table 1b illustrates the demographics of the case-control groups. Gender, race, and ethnicity were not associated with the development of PRES. Multiple comorbidities were assessed, but none were significantly associated PRES. Any prior use of Etoposide was associated with the development of PRES (p=0.008)(Table 1b). Having received intrathecal (IT) chemotherapy was not associated with PRES (p=0.386). In a multivariate model including the two variables of etoposide use and being post allogeneic HCT, etoposide remained significant [OR=9.0 (95% CI: 1.5, 53.9), p= 0.016]. Being post-allogeneic HCT was no longer significant.
Table 1:
Demographics of cohort (a). Demographics of case-control (b).
| Demographics of cohort | |||
|---|---|---|---|
| PRES n=14 |
No-PRES n=459 |
p value | |
| Age (years) | 14 (IQR: 11.0, 17.3) | 9.6 (IQR: 3.8, 15.4) | 0.421 |
| Diagnosis: | 0.019 | ||
| Lymphoid leukemia | 3 (21%) | 260 (57%) | |
| Myeloid leukemia | 2 (14%) | 53 (12%) | |
| Hodgkin’s lymphoma | 2 (14%) | 53 (12%) | |
| Non-Hodgkin’s lymphoma | 2 (14%) | 47 (10%) | |
| Post-allogeneic HCT | 5 (36%) | 46 (10%) | |
| Demographics of case control study | |||
| PRES n=14 |
No-PRES n=28 |
p value | |
| Age (years) | 14 (IQR: 11.0, 17.3) | 15 (IQR: 11.8, 17.3) | 0.726 |
| Females | 7 (50%) | 9 (35%) | 0.343 |
| Males | 7 (50%) | 17 (65%) | |
| Race: | 0.686 | ||
| White | 12 (86%) | 20 (77%) | |
| Black | 2 (14%) | 5 (19%) | |
| Other | 1 (4%) | ||
| Hispanic | 2 (14%) | 1 (4%) | 0.289 |
| Chemotherapeutics | |||
| Busulfan | 3 (21%) | 6 (23%) | 0.905 |
| Vincristine | 6 (43%) | 11 (42%) | 0.973 |
| Methotrexate | 5 (36%) | 10 (39%) | 0.864 |
| Cyclophosphamide | 7 (50%) | 12 (46%) | 0.816 |
| Fludarabine | 4 (29%) | 9 (35%) | 0.697 |
| ATG | 4 (29%) | 3 (11%) | 0.214 |
| TBI | 1 (7%) | 1 (4%) | 1.000 |
| Thiotepa | 1 (7%) | 0 | 0.350 |
| Melphalan | 0 | 1 (4%) | 1.000 |
| Steroids | 9 (64%) | 12 (46%) | 0.273 |
| Asparaginase | 3 (21%) | 3 (11%) | 0.646 |
| Daunorubicin | 3 (21%) | 4 (15%) | 0.679 |
| Doxorubicin | 2 (14%) | 8 (31%) | 0.251 |
| 6-MP | 3 (21%) | 1 (4%) | 0.077 |
| Ara-C | 4 (29%) | 4 (15%) | 0.320 |
| TKI | 1 (7%) | 2 (8%) | 1.000 |
| Etoposide | 6 (43%) | 2 (8%) | 0.008 |
| IT Chemotherapy | 9 (64%) | 14 (50%) | 0.386 |
| Comorbidities | |||
| Renal disease | 1 (7%) | 0 | 0.350 |
| Hemoglobinopathy | 1 (7%) | 3 (11%) | 1.000 |
| Congenital Heart Disease | 1 (7%) | 0 | 0.350 |
| Prematurity | 1 (7%) | 0 | 0.350 |
| GVHD | 1 (7%) | 0 | 0.350 |
| CPD | 0 | 1 (4%) | 1.000 |
| Osteopetrosis | 1 (7%) | 0 | 0.333 |
| GERD | 1 (7%) | 0 | 0.333 |
| Autism | 1 (7%) | 1 (4%) | 0.999 |
| Fanconi Anemia | 1 (7%) | 0 | 0.333 |
| Evans Syndrome | 1 (7%) | 0 | 0.333 |
| Kostmann Syndrome | 0 | 1 (4%) | 0.999 |
| Thrombosis | 0 | 1 (4%) | 0.999 |
| SCIDS | 0 | 2 (8%) | 0.545 |
Results are presented in medians (IQR: interquartile range) for continuous variables or as counts (%) for categorical variables. HCT=hematopoietic cell transplantation, ATG=Antithymocyte globulin, TBI=Total body irradiation, 6-MP=6-Mercaptapurine, Ara-C=Cytarabine, TKI=Tyrosine kinase inhibitor, IT = Intrathecal, GVHD=Graft vs. host disease, CPD=Chronic pulmonary Disease, GERD=Gastroesophageal reflux disease, and SCIDS=Severe combined immunodeficiency syndrome.
Symptoms found in patients with PRES were investigated to better characterize this disease (Figure 1). All patients diagnosed with PRES experienced hypertension. Seizures were the second most common symptom occurring in almost 80% of patients, followed by nausea and vomiting, altered mental status, headaches, fatigue, and visual changes. One patient experienced dizziness.
Figure 1: Percentage of symptoms experienced by patients with PRES.
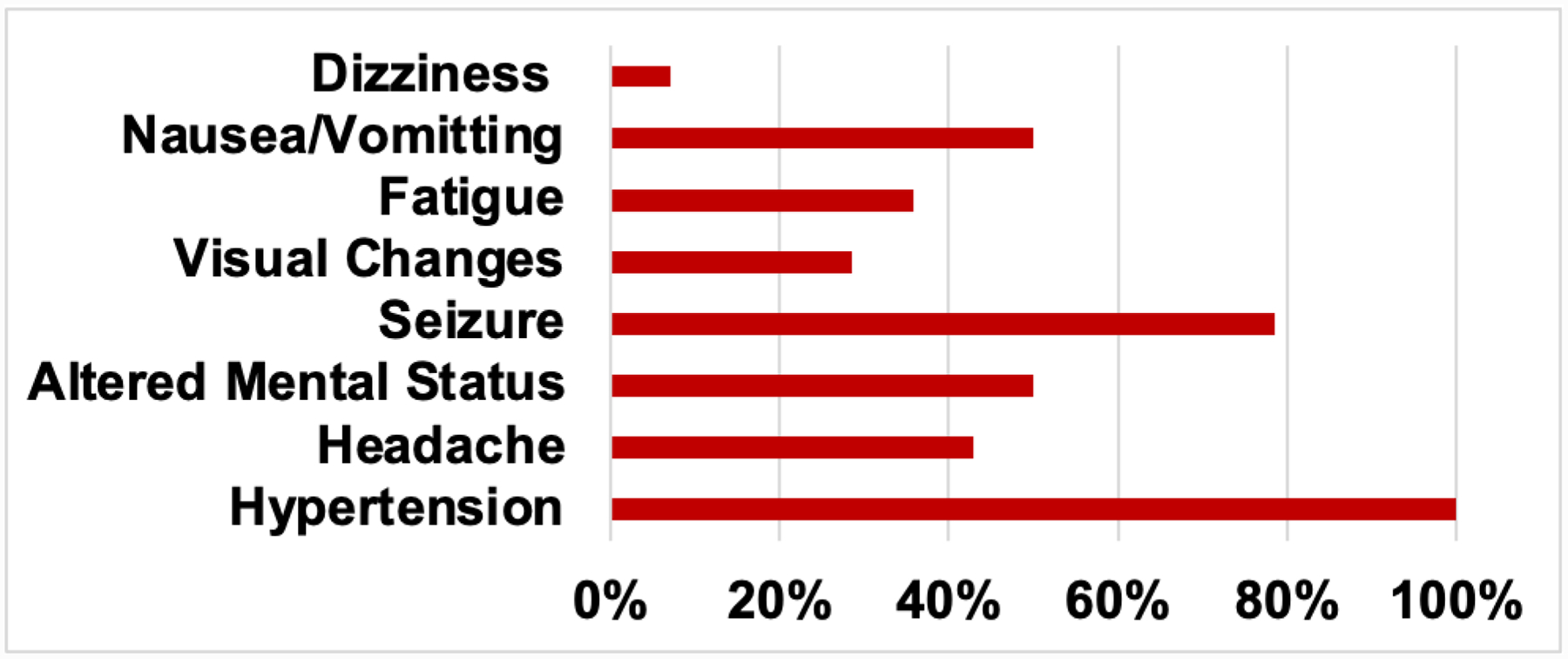
These symptoms were assessed for all patients with the diagnosis of PRES. Results are presented as percentage of patients with PRES.
All patients diagnosed with PRES underwent evaluation with MRI (Figure 2). The majority of findings (79%) in our cohort were consistent with PRES. MRI findings most commonly included involvement of parietal, frontal, and occipital lobes. The majority of scans (64%) showed bilateral findings.
Figure 2: Percentage of MRI findings associated with patients with PRES.
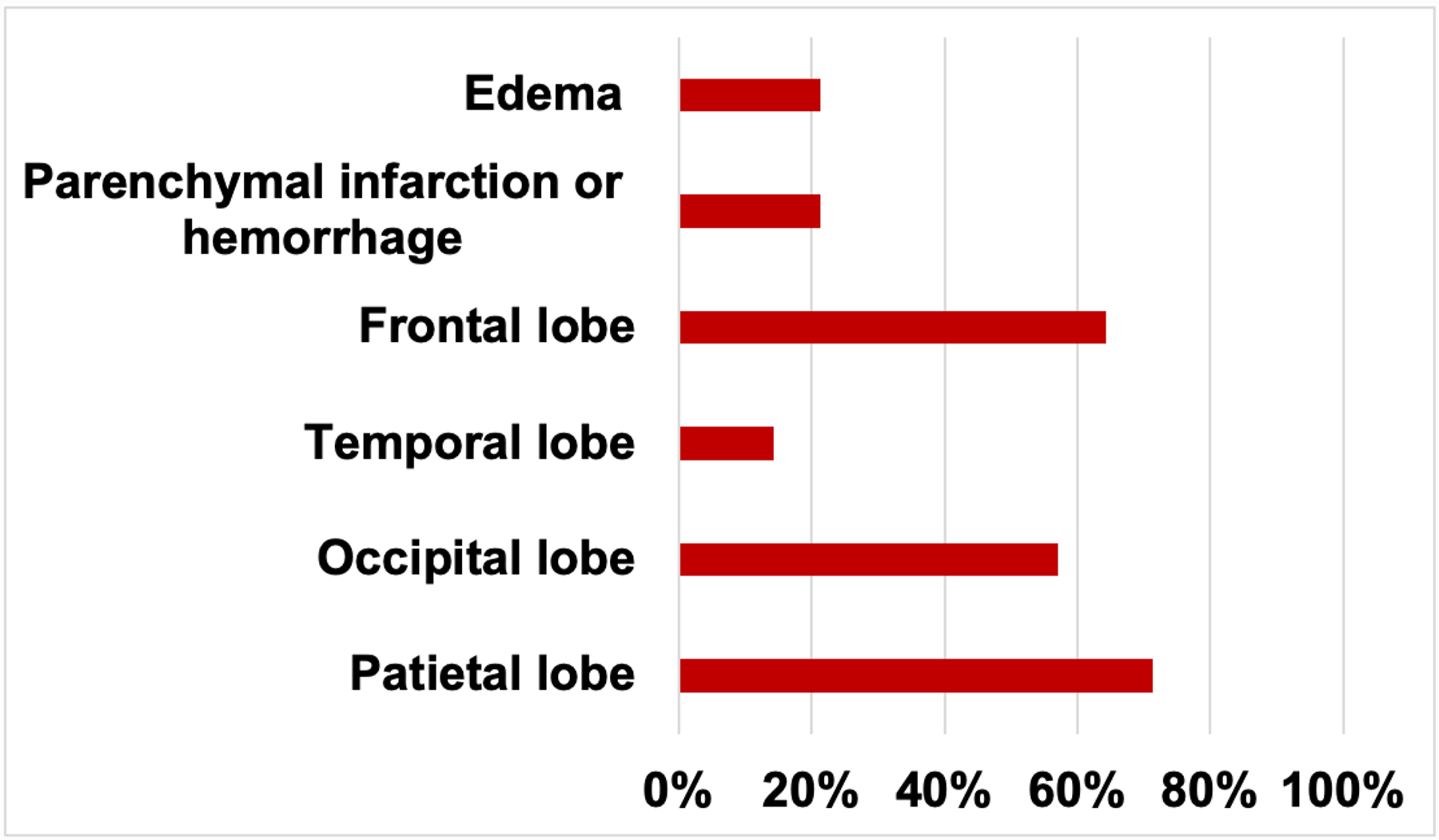
MRI findings were assessed in patients with a diagnosis of PRES. The results are presented as percentage of patients with PRES.
Median blood pressures, laboratory values and fluid status are described in Table 2. Blood pressure measurements were the highest on the day of diagnosis. Patients did not experience significant fluid overload during the first 3 days of PRES diagnosis, and urine output remained within normal limits over the study time. As expected by nature of the underlying diagnoses and associated treatment, the median blood cell counts demonstrated mild anemia and thrombocytopenia. Most patients were not neutropenic during their PRES diagnosis.
Table 2:
Description of blood pressures, fluid status and laboratory values over the first three days of PRES diagnosis
| Day PRES diagnosis | |||
|---|---|---|---|
| Day 0 | Day 1 | Day 2 | |
| Blood pressures | |||
| Systolic Pressure (mmHg) | 135 (120, 141) | 124 (116, 136) | 123 (116, 132) |
| Diastolic Pressure (mmHg) | 96 (82, 99) | 85 (75, 94) | 86 (79, 92) |
| Mean Arterial Pressure (mmHg) | 106 (91, 111) | 97 (93, 106) | 95 (88, 101) |
| Fluid | |||
| % Fluid overload | 0.48 (−0.17, 2.0) | 2.6 (−0.27, 5.2) | 1.6 (−1.5, 7.0) |
| Urine output (mL/kg/hour) | 1.8 (1.3, 2.5) | 2.0 (1.5, 2.5) | 1.8 (1.3, 2.6) |
| Lab Values | |||
| Hemoglobin (g/dL)_ | 10.2 (9.1, 11.6) | 10.1 (9.1, 10.9) | 10.1 (9.6, 10.6) |
| Hematocrit (%) | 30.1 (25.6, 32.4) | 29.6 (26.4, 31.4) | 29.3 (27.9, 20.9) |
| White Blood Cells × 103/μL | 3.8 (1.2, 6.7) | 2.5 (0.9, 5.5) | 2.4 (0.6, 6.0) |
| Absolute Neutrophil × 103/μL | 3.6 (1.1, 5.2) | 1.4 (0.5, 4.1) | 2.7 (0.8, 4.3) |
| Platelets 103/μL | 75 (29, 169) | 83 (47, 122) | 85 (56, 98) |
| Sodium (mEq/L) | 138 (136, 144) | 142 (137, 145) | 139 (138, 143) |
| Potassium (mEq/L) | 3.6 (3.5, 4.7) | 3.7 (3.4, 4.2) | 3.7 (3.1, 4.3) |
| Chloride (mEq/L) | 107 (102, 110) | 109 (105, 110) | 110 (106, 111) |
| Bicarbonate (mEq/L) | 24 (22, 26) | 24 (22, 27) | 23 (21, 24) |
| BUN (mg/dL) | 20 (11, 34) | 20 (14, 30) | 20 (12, 28) |
| Creatinine (mg/dL) | 0.44 (0.26, 0.70) | 0.56 (0.34, 0.97) | 0.71 (0.38, 0.85) |
| Glucose (mg/dL) | 101 (94, 113) | 126 (111, 157) | 111 (104, 146) |
Blood pressures on day 0 represent the measurement closest to PRES diagnosis. Blood pressures measurements on day 1 and 2 were identified as the highest mean arterial pressure on that day with corresponding systolic and diastolic measurements. % Fluid overload was initially calculated on day 0 and the cumulative fluid balance was used for day 1 and 2. The following equation was used (total input in liters – total output in liters)/weight in kilograms × 100.
Table 3 shows therapies, monitoring, and supportive care used in the treatment of PRES. Various approaches were used to control hypertension including continuous infusion, intermittent IV and oral antihypertensives. Calcium channel blockers, specifically Nicardipine, were most commonly administered for those requiring a continuous infusion of an antihypertensive medication. Vasodilators, specifically Hydralazine, were often given for patients receiving intermittent IV antihypertensives. Calcium channel blockers were the most common oral medication. One patient had an arterial line placed. More than one-third of patients with PRES were intubated. As seizures were a common symptom, 43% were monitored with neurotelemetry and 14% received a routine EEG (Table 3).
Table 3:
Treatments and therapies for patients diagnosed with PRES.
| Therapy | n (%) |
|---|---|
| Continuous infusion of antihypertensive agent | 8 (57%) |
| Nicardipine | 8 (57%) |
| Esmolol | 1 (7%) |
| Labetalol | 1 (7%) |
| Intermittent IV antihypertensive agent | 12 (86%) |
| Hydralazine | 11 (79%) |
| Labetalol | 4 (29%) |
| Oral antihypertensive agent | 12 (86%) |
| Ca2+ channel blockers | 11 (79%) |
| ACE inhibitor | 5 (36%) |
| Beta blocker | 2 (14%) |
| K+ channel blocker | 1 (7%) |
| Alpha agonist | 1 (7%) |
| Intubation | 5 (36%) |
| Arterial line placement | 1 (7%) |
| Neurotelemetry | 5 (43%) |
| Routine EEG | 2 (14%) |
Results are presented as counts (%). Antihypertensive agents were recorded from onset of PRES to resolution of symptoms. Intubation and arterial line placement were recorded for patients with PRES that were admitted to the pediatric intensive care unit (PICU). ACE= Angiotensin converting enzyme and EEG=Electroencephalogram.
Outcomes of patients with PRES are described in Table 4. We evaluated interruptions in chemotherapy. For patients in who were in need of ongoing chemotherapy, chemotherapeutic agents were held for some time after being diagnosed with PRES. The majority of patients were admitted to the ICU and the median ICU stay was 5 days. Four of the patients diagnosed with PRES died while in the hospital. One patient died from acute hypoxic and hyper-carbic respiratory failure, which was secondary to fungal pneumonia. Another suffered multi-organ system failure due to bacteremia from bowel ischemia. The third patient’s cause of death was acute on chronic renal failure and acute respiratory failure. The last patient died from septic shock with multi-organ dysfunction from disseminated viremia
Table 4:
Outcomes of PRES diagnosis and associated patient percentages.
| Outcome | Patient Data n=14 |
|---|---|
| Stopped Chemotherapy | 5 (36%) |
| 1–2 weeks | 2 (14%) |
| Admitted the PICU | 11 (79%) |
| Length of PICU stay | 5 (IQR: 0.75, 18.5) |
| Hospital Mortality | 4 (29%) |
Results are presented as counts (%) or medians (IQR: interquartile range). PICU=pediatric intensive care unit. Hospital mortality was associated with causes secondary to PRES.
Discussion
By conducting this study, we were able to determine the incidence of PRES in this patient population over a 5-year period. Fourteen patients were diagnosed with PRES, resulting in an incidence of 5.9/1000 patients/year. We explored potential risk factors, including chemotherapeutics, underlying cancer diagnosis or status post-allogeneic HCT, and comorbidities for a potential association with the development of PRES. Finally, we were able to better characterize the clinical presentation of PRES by identifying most common presenting symptoms and related MRI findings within our cohort.
The incidence of PRES for this cohort was calculated over a 5-year period and found to be 5.9/1000 patients/year. While this incidence may seem low, there remains the challenge that it is difficult to determine a true incidence due to the fact that there is no definitive diagnostic test. Less severely affected patients with PRES may be missed or go undiagnosed without clear diagnostic criteria. Furthermore, clinical and radiological findings may differ between patients diagnosed with PRES. This means that a diagnosis of PRES may be limited by subjectivity. To better quantify the impact of PRES and understand the implications of this disease, a standard definition with stricter criteria for both clinical management and research purposes is needed.
We were able to characterize the clinical presentation of patients diagnosed with PRES in our cohort, using MRI findings and presenting symptoms that are consistent with existing literature describing PRES.3–5,11–13 While often variable, certain symptoms were more consistently found in patients diagnosed with PRES. Parietal, frontal and occipital lobe involvement were common MRI findings. Several patients also showed diffuse edema, infarction or hemorrhage, or temporal lobe involvement. These findings were less common, but may still be important in diagnosing suspected PRES. The most common clinical presentation was hypertension, seizures, altered mental status, nausea/vomiting, and headache. While hypertension was present patients with PRES, it is difficult to determine if this is a symptom or a contributing cause the development of PRES. Such increases in blood pressure may overwhelm the autoregulatory mechanisms in the brain. This effect may be more prominent in children, as autoregulation occurs within a narrower range compared with adults.14,15 Patients with PRES presenting with normal or marginally elevated blood pressure have also been reported. In these cases, cancer or immunosuppressive agents have caused endothelial cell damage, which leads to transient vasoconstriction that can be exacerbated by hypertension or impaired autoregulatory mechanisms.15,16 The symptoms and MRI findings seen consistently in patients with PRES within our cohort may help to better inform a standard definition of PRES, aid in early identification of at-risk patients, and faster initiation of treatment.
Several risk factors, including comorbidities, age, chemotherapeutics, and primary cancer diagnosis or being status post-allogeneic HCT were investigated to determine their association with the development of PRES. Neither comorbidities nor age were associated with the development of PRES. Etoposide was the only chemotherapeutic agent in our cohort that was associated with PRES. Etoposide, a Topoisomerase II inhibitor, is not often associated with neurotoxicity. At high doses, however, confusion, seizures, and transient blindness have been observed.17 While chemotherapeutic agents like Methotrexate, Cisplatin, Cytarabine, or Vincristine have been shown to have an association with the development of PRES, they were not found to be associated in our cohort.2,18,19 This is possibly due to small sample size or institutional practice patterns. Steroids use, which can cause hypertension as an adverse effect, was shown in several studies to be associated with PRES.20–22 While many patients in our cohort received steroids as part of their therapy regimen, it was not significantly linked to the development of PRES. This could be due to our smaller sample size. As seen in table 1, many more patients in the PRES group received steroids compared to the control group, it just did not meet statistical significance. With a larger sample, the study may have had enough power to find a difference.
The use of Etoposide has not been shown to have an association with PRES to the same scale as the previously listed drugs. However, two case studies describe patients taking Etoposide, either alone or in a combination therapy, who later developed PRES.23–24 This suggests that Etoposide is a potential risk factor in the development of PRES in cancer patients. Perhaps Etoposide is contributing to cellular injury, damage, and dysfunction. Endothelial cell damage may lead to disruption of the blood-brain-barrier, a mechanism thought to be associated with development of PRES, and resultant cerebral edema.2–4 Further multicenter studies are needed to better understand this potential risk factor.
Additionally, we noted on univariable analysis, an increased incidence of PRES in patients having received an allogenic HCT when compared with a diagnosis of leukemia or lymphoma. Patients in need of an HCT tend to receive medications for bone marrow ablation or GVHD prophylaxis that may have adverse effects including cellular damage, neurotoxicity, and hypertension.25–27 A previous study showed an association with the development of PRES in individuals who have hypertension, have undergone SCT, or are on immunosuppression.25 While having received an allogeneic HCT did not remain significant on a multivariate analysis, this analysis is limited due to our small sample size. This is an important variable to be investigated in larger studies.
While PRES was infrequent in this population, it carries a high morbidity, including high rate of PICU admission, seizures, and intubation. Furthermore, it has a high associated hospital mortality at 29%. The four patients in our cohort died of various infections and organ dysfunction. Clearly, the patients are not dying solely of PRES, but there may be an association between their death and PRES. PRES may be precipitating an inflammatory response or organ dysfunction that may contribute to their death weeks or months later. Previous studies support this consideration, having suggested that PRES leads to immune system activation and secretion of inflammatory cytokines.28–30 In fact, immune system activation from previous infection, sepsis, or shock may make a person more likely to develop PRES, especially if gram-positive bacteria are involved.30 The response to infection is complex and results in several systemic changes. In cancer patients, the immune response is often dampened due to immunosuppressive therapy or underlying immune dysregulation, potentially allowing inflammatory processes to progress unrestricted and lead to systemic infection.30 Furthermore, endothelial cell injury is a major component of infection and has been linked to potential mechanisms of PRES.2–4,31
While this study has some limitations, the outcomes remain important. The large cohort studied over a 5-year period encompassed several pediatric malignancies, but focused on a single center. While this limits the generalizability of our results, our detailed results on the patients’ clinical presentations and treatments of PRES adds to the literature to better understand the diagnosis, therapies, and outcomes of PRES. The small sample size within our case-control prohibited multivariate analysis and the study could clearly be improved with an expansion to a multicenter cohort, as well as follow up data on the discussed cohort. This small sample size also precluded matching on more numerous variables such as conditioning regimen, use of calcineurin inhibitors, or use of steroids for GVHD prophylaxis, which are important considerations. Additionally, conducting a retrospective study meant that we were limited by data already recorded in medical records. Future studies should focus on multiple centers and multivariate analysis.
Conclusion
PRES continues to be challenging to identify, therefore there exists a need to define clear clinical criteria to better diagnose patients with PRES. Clear diagnostic criteria can aid in the improved understanding of the burden of disease in this population, detection of specific risk factors, targeted therapies, and implications of PRES on outcomes of children with cancer.
Conflicts of Interest and Sources of Funding
This project was funded, in part, with support from the Indiana Clinical and Translational Sciences Institute funded, in part by UL1TR002529 from the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors have no conflicts of interest or funding to disclose.
References
- 1.Khan RB, Sadighi ZS, Zabrowski J, et al. Imaging Patterns and Outcome of Posterior Reversible Encephalopathy Syndrome During Childhood Cancer Treatment. Pediatr Blood Cancer. 2016;63(3):523–526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bartynski WS. Posterior Reversible Encephalopathy Syndrome, Part 1: Fundamental Imaging and Clinical Features. AJNR Am J Neuroradiol. 2008; 6:1036–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Raj S, Overby P, Erdfarb A, et al. Posterior reversible encephalopathy syndrome: incidence and associated factors in a pediatric critical care population. Pediatr Neurol. 2013;49(5):335–9. [DOI] [PubMed] [Google Scholar]
- 4.Thavamani A, Umapathi KK, Puliyel M, et al. Epidemiology, comorbidities, and outcomes of posterior reversible encephalopathy syndrome in children in the United States. Pediatr Neurol. 2019;103:21–6. [DOI] [PubMed] [Google Scholar]
- 5.Morris EB, Laningham FH, Sandlund JT, et al. Posterior reversible encephalopathy syndrome in children with cancer. Pediatr Blood Cancer. 2007;48(2):152–159. [DOI] [PubMed] [Google Scholar]
- 6.Musioł K, Waz S, Boroń M, et al. PRES in the course of hemato-oncological treatment in children. Childs Nerv Syst. 2018. Apr;34(4):691–699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Khan SJ, Arshad AA, Fayyaz MB, et al. Posterior Reversible Encephalopathy Syndrome in Pediatric Cancer: Clinical and Radiologic Findings. J Glob Oncol. 2018. Sep;4:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Thompson D, Harrington Y, de la Fuente J. The incidence of reversible encephalopathy syndrome is increased in BMT for hemoglobinopathies. Blood. 2013; 122: 4579. [Google Scholar]
- 9.Noe A, Cappelli B, Biffi A, et al. High incidence of severe cyclosporine neurotoxicity in children affected by heamoglobinopathies undergoing myeloablative heamatopoeitic stem cell transplantation: early diagnosis and prompt intervention ameliorates neurological outcome. Ital J Pediatr. 2010; 36: 1–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap) – A metadata-driven methodology and workflow process for providing translational research informatics support, J Biomed Inform. 2009. Apr;42(2):377–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Moon S-N, Jeon SJ, Choi SS, et al. Can clinical and MRI findings predict the prognosis of variant and classical type of posterior reversible encephalopathy syndrome (PRES)? Acta Radiologica, 2013;54(10):1182–1190. [DOI] [PubMed] [Google Scholar]
- 12.Raman R, Devaramane R, Jagadish GM, et al. Various Imaging Manifestations of Posterior Reversible Encephalopathy Syndrome (PRES) on Magnetic Resonance Imaging (MRI). Pol J Radiol. 2017. Feb 7;82:64–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hugonnet E, Da Ines D, Boby H, et al. Posterior reversible encephalopathy syndrome (PRES): features on CT and MR imaging Diagn Interv Imaging, 2013; 94: 45–52 [DOI] [PubMed] [Google Scholar]
- 14.Siebert E, Bohner G, Endres M, Liman TG. Clinical and radiological spectrum of posterior reversible encephalopathy syndrome: does age make a difference? –A retrospective comparison between adult and pediatric patients. PLoS ONE. (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chen TH. Childhood Posterior Reversible Encephalopathy Syndrome: Clinicoradiological Characteristics, Managements, and Outcome. Front Pediatr. 2020. Sep 11;8:585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.de Laat P, Te Winkel ML, Devos AS, Catsman-Berrevoets CE, Pieters R, van den Heuvel-Eibrink MM. Posterior reversible encephalopathy syndrome in childhood cancer. Ann Oncol. (2011) 22:472. [DOI] [PubMed] [Google Scholar]
- 17.Forsyth P, Cascino T. Neurological complications of chemotherapy. In: Neurological Complications of Cancer, Wiley R (Ed), Marcel Dekker, Inc., New York: 1995: 241. [Google Scholar]
- 18.Bartynski WS. Posterior reversible encephalopathy syndrome, part 2: controversies surrounding pathophysiology of vasogenic edema. AJNR Am J Neuroradiol 2008; 29: 1043–1049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Tsukamoto S, Takeuchi M, Kawajiri C, Tanaka S, Nagao Y, et al. (2012) Posterior reversible encephalopathy syndrome in an adult patient with acute lymphoblastic leukemia after remission induction chemotherapy. Int J Hematol 95: 204–208. [DOI] [PubMed] [Google Scholar]
- 20.Sukumaran S, George B, Nair HP, et al. Posterior reversible encephalopathy syndrome as a consequence of high dose steroid administration after autologous PBSCT. Bone Marrow Transplant. 2010. Apr;45(4):779–80. [DOI] [PubMed] [Google Scholar]
- 21.Parikh NS, Schweitzer AD, Young RJ, et al. Corticosteroid therapy and severity of vasogenic edema in posterior reversible encephalopathy syndrome. J Neurol Sci. 2017. Sep 15;380:11–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Morrow SA, Rana R, Lee D, et al. Posterior Reversible Encephalopathy Syndrome due to High Dose Corticosteroids for an MS Relapse. Case Rep Neurol Med. 2015;2015:325657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Khanal P, Awan F, Nguyen V. Etoposide-induced posterior reversible encephalopathy syndrome. Ann Hematol. 2013. Apr;92(4):561–2. [DOI] [PubMed] [Google Scholar]
- 24.Floeter AE, Patel A, Tran M, et al. Posterior Reversible Encephalopathy Syndrome Associated With Dose-adjusted EPOCH (Etoposide, Prednisone, Vincristine, Cyclophosphamide, Doxorubicin) Chemotherapy. Clin Lymphoma Myeloma Leuk. 2017. Apr;17(4):225–230. [DOI] [PubMed] [Google Scholar]
- 25.Gaziev J, Marziali S, Paciaroni K, et al. Posterior reversible encephalopathy syndrome after hematopoietic cell transplantation in children with hemoglobinopathies. Biol Blood Marrow Transplant, 2017; 23:1531–1540. [DOI] [PubMed] [Google Scholar]
- 26.Hammerstrom AE, Howel J, Gulbis A., et al. Tacrolimus-associated posterior reversible encephalopathy syndrome in hematopoietic allogeneic stem cell transplantation. Am J Hematol. 2013; 88: 301–305. [DOI] [PubMed] [Google Scholar]
- 27.Wong R, Beguelin GZ, De Lima M, et al. Tacrolimus-associated posterior reversible encephalopathy syndrome after allogeneic haematopoietic stem cell transplantation. Br J Haematol. 2003; 122: 128–134. [DOI] [PubMed] [Google Scholar]
- 28.Orhun G Posterior Reversible Encephalopathy Syndrome and Septic Encephalopathy: Neuroimaging, Inflammation and Neurodegeneration Findings. Noro Psikiyatr Ars. 2019. Oct 9;57(1):80–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Chen Z, Shen GQ, Lerner A, et al. Immune system activation in the pathogenesis of posterior reversible encephalopathy syndrome. Brain Res Bull. 2017; 131:93–99. [DOI] [PubMed] [Google Scholar]
- 30.Bartynski WS, Boardman JF, Zeigler ZR, et al. Posterior Reversible Encephalopathy Syndrome in Infection, Sepsis, and Shock. American Journal of Neuroradiology Nov 2006; 27(10): 2179–2190. [PMC free article] [PubMed] [Google Scholar]
- 31.Munford RS. Sepsis, severe sepsis, and septic shock. In: Mandell GL, Bennett JE, Dolin R eds. Principles and Practice of Infectious Disease. Philadelphia: Elsevier; 2005; 906–26. [Google Scholar]