

Abstract
Life expectancy for US White men and women declined between 2013 and 2017. Initial explanations for the decline focused on increases in “deaths of despair” (i.e., deaths from suicide, drug use, and alcohol use), which have been interpreted as a cohort-based phenomenon afflicting middle-aged White Americans. There has been less attention on Black mortality trends from these same causes, and whether the trends are similar or different by cohort and period. We complement existing research and contend that recent mortality trends in both the US Black and White populations most likely reflect period-based exposures to 1) the US opioid epidemic and 2) the Great Recession. We analyzed cause-specific mortality trends in the United States for deaths from suicide, drug use, and alcohol use among non-Hispanic Black and non-Hispanic White Americans, aged 20–64 years, over 1990–2017. We employed sex-, race-, and cause-of-death–stratified Poisson rate models and age-period-cohort models to compare mortality trends. Results indicate that rising “deaths of despair” for both Black and White Americans are overwhelmingly driven by period-based increases in drug-related deaths since the late 1990s. Further, deaths related to alcohol use and suicide among both White and Black Americans changed during the Great Recession, despite some racial differences across cohorts.
Keywords: age-period-cohort models, deaths of despair, midlife mortality, mortality trends, opioid, racial/ethnic trends, United States
Abbreviations
- APC
age-period-cohort
- ICD
International Classification of Diseases
Life expectancy in the United States declined between 2013–2017 (1), before increasing by 0.1 years in 2018 (2). To date, explanations for recent trends in US life expectancy have largely focused on midlife deaths attributed to suicide and poisonings from drugs and alcohol (3, 4), especially among the White population (5–9). These popularly proclaimed, “deaths of despair” (i.e., chronic liver disease, suicide, and drug overdoses) were believed to reflect cohort-based cumulative disadvantages related to rising distress, economic insecurity, and chronic pain in the White population (5, 6). A similar narrative was forwarded about Black Americans in the 1980s and 1990s whereby the disappearance of blue-collar jobs might have contributed to rising drug use rates, especially in the inner city (10). To date, research has not discussed these narratives in tandem. Among White Americans, “deaths of despair” trends are primarily driven by period-based drug mortality, which coincides with the increased availability of prescription drugs in the late-1990s and the expanding availability of heroin and synthetic opiates (e.g., fentanyl) in the 2010s (11–14). In the midst of the opioid epidemic, the United States also experienced the Great Recession (2007–2009), the country’s worst financial crisis since the Great Depression, and its slow and unequal recovery during the 2010s. A wealth of research documents the health consequences of these economic downturns, such as rises in suicide, hypertension, diabetes, and poor health behaviors (15–19). Further, research suggests that economic shocks interact with the opioid epidemic, creating an especially volatile environment (20, 21). Thus, between 1990 and 2017, the United States experienced 2 period-based exposures that have contributed to increased mortality and declines in life expectancy: the opioid epidemic and the Great Recession. To complement existing research and to examine the extent to which these exposures have affected both Black and White Americans, we analyzed period- and cohort-based trends in suicide and drug- and alcohol-related mortality.
This addition to the literature is important because recent increases in mortality among the US White population have garnered widespread media (22–24) and research attention, with the coverage generally failing to situate the trends in historical and racial context in the United States. We argue that it is likely that the concerning mortality trends among White Americans have been occurring in the Black population in similar ways. Equally important is the fact that death rates among Black Americans remain much higher than those among White Americans (1, 25), and reports suggest that the opioid crisis is worsening for Black Americans (26). In many areas of the United States, opioid-overdose rates are higher for Black Americans than in the general population (27). Therefore, it is imperative that we extend our considerations of US mortality trends beyond the troubling signs within the US White population to spotlight the impact that recent changes in the US drug environment and the Great Recession have had on US Black mortality.
METHODS
We analyzed trends in US adult Black and White mortality rates for the causes of death associated with “deaths of despair.” Specifically, we examined yearly trends in age-standardized death rates from suicide, drug use, and alcohol use for Black and White Americans, separately by sex, and employed cause-specific age-period-cohort (APC) models to investigate period- and cohort-based trends by race, sex, and cause of death. If an underlying epidemic of pain, economic distress, and despair is unique to more recent cohorts of White Americans (5, 6), we should observe cohort-based increases in death rates from suicide, drug use, and alcohol use among White men and women. In contrast, if the mortality trends from “deaths of despair” are associated with period-based factors such as the rising availability of opioids beginning in the late 1990s and the acute hardships associated with the Great Recession, we should observe period-based increases in mortality for both White and Black men and women coinciding with these exposures. Similar patterning across race and sex would suggest that the trends and potential underlying causes might be shared by Black and White Americans.
We used official death counts from the multiple cause-of-death mortality files as the numerator. These data come from the restricted-use National Vital Statistics System (NVSS) Multiple Cause-of-Death files (28) and are compiled by the National Association for Public Health Statistics and Information Systems (NAPHSIS). We used official population counts from the US Census Bureau, compiled by Surveillance, Epidemiology, and End Results (SEER), as the denominator. Data are restricted to years 1990–2017, given that Hispanic ethnicity is specified in population counts beginning in 1990. Our analytical sample is composed of non-Hispanic White (White) and non-Hispanic Black (Black) men and women. We restricted our sample to ages 20–64 years because our focus is on external causes of mortality for working-aged Americans (29). Cause-specific mortality trends are analyzed in 3 separate age groups—20–34 years, 35–49 years; and 50–64 years—in order to examine age-based differences in the mortality trends. APC models are fitted to all ages, 20–64 years. Foreign residents are excluded from these analyses.
We examined cause-specific mortality trends separately for deaths from intentional self-harm or suicide, drug use, and alcohol use. In line with previous research, we also analyzed the sum of the rates from the 3 causes as “deaths of despair” (5). Causes of death are coded using underlying cause-of-death codes from the International Classification of Diseases (ICD). In 1999 ICD codes change from the ninth revision (ICD-9) to the tenth revision (ICD-10), so we standardized across these 2 separate time periods. We classified the 3 categories of deaths using the following ICD codes: suicide (ICD-9: 950–959.9; ICD-10: U03, X60–X84.9, Y87.0), drug-related deaths (ICD-9: 304, 850–858, 962, 980–980.5; ICD-10: F11–F16, F19, X40–X45, X85, Y10–Y15), and alcohol-related deaths (ICD-9: 291, 303, 571; ICD-10: F10, K70, K73–K74) (11, 12).
We fitted Poisson rate models to annual counts of death occurring in single-year ages to estimate cause-specific age-standardized death rates for US Black and White men and women aged 20–34 years, 35–49 years, and 50–64 years. Models were fitted separately according to race, sex, and cause of death and included single-year indicators to estimate yearly trends in the age-standardized mortality rates. The models were structured as:
 |
The hazard rate for the ith age in the jth year is expressed as a function of a set of i age groups,  = (age1, age2,…, agei) and associated parameters,
= (age1, age2,…, agei) and associated parameters,  = (
= ( , j time periods,
, j time periods,  = (year1, year2,…, yearj) and associated parameters,
= (year1, year2,…, yearj) and associated parameters,  = (
= ( , and the log exposure,
, and the log exposure,  , is declared an offset term in the model where
, is declared an offset term in the model where  is the estimated July 1 population for age group i during time period j. Poisson models were fitted to each cause of death separately for Black and White men and women and separately in the 3 age groups. The Poisson rate models estimate the conditional expectation (i.e., mean rate) of the death rate for a given age in a given year (30). As such, fitting Poisson rate models to mortality trends that include single-age fixed effects is comparable to estimating age standardized mortality rates for the US Black and White men and women aged 20–34 years, 35–49 years, and 50–64 years (see Web Appendix 1 and Web Figures 1–3 for results illustrating this point, available at https://doi.org/10.1093/aje/kwab088).
is the estimated July 1 population for age group i during time period j. Poisson models were fitted to each cause of death separately for Black and White men and women and separately in the 3 age groups. The Poisson rate models estimate the conditional expectation (i.e., mean rate) of the death rate for a given age in a given year (30). As such, fitting Poisson rate models to mortality trends that include single-age fixed effects is comparable to estimating age standardized mortality rates for the US Black and White men and women aged 20–34 years, 35–49 years, and 50–64 years (see Web Appendix 1 and Web Figures 1–3 for results illustrating this point, available at https://doi.org/10.1093/aje/kwab088).
We also fitted APC models using the intrinsic estimator constraint to separately estimate period-based variation and cohort-based variation in mortality rates from “deaths of despair” (31–34). Period-based factors in mortality trends are exposures thought to affect all age groups in a population, such as public health interventions, policy changes, and economic contractions (31). For example, the rapid increase in the US supply of opioid-based painkillers during the late 1990s and early 2000s is thought to have spurred a period-based increase in drug-related deaths and fueled a 3-wave opioid epidemic in the United States (12–13, 35–36). In contrast, cohort-based factors in mortality trends stem from historical exposures shared by members of a birth cohort (34, 37) or members of labor market cohorts (38). The mortality consequences of cohort effects manifest as trends in death rates that vary considerably across age groups. For example, it has been argued that birth cohorts’ varying exposures to cumulative socioeconomic disadvantages (39) might be responsible for the rising “deaths of despair” among younger and middle-aged White Americans (5, 6). We fitted all APC models using 15 3-year age groups (20–22, 23–25, …, 59–61, 62–64) and 14 2-year periods (1990–1991, 1992–1993, … 2014–2015, 2016–2017), resulting in 210 age × period cells covering 28 birth cohorts. The intrinsic estimator is an appropriate and widely used constraint for APC models fitted to tabular rate data (i.e., age-specific rates by time periods), in which birth cohort is perfectly linearly dependent on age and period (i.e., period – age = cohort) (31–34, 40).
RESULTS
Table 1 reports age-standardized death rates from “deaths of despair,” together and separately by cause of death for suicides, drug-related deaths, and alcohol-related deaths. Mortality trends from “deaths of despair” among Black Americans are both similar to and different from trends among White Americans. First, mortality rates from “deaths of despair” increased between 1990 and 2017 in all age groups and for all race-sex populations, except Black men and women aged 35–49 years. Among Black men aged 35–49 years, “deaths of despair” mortality decreased by 36.2 deaths per 100,000 and decreased by 3.0 deaths for Black women. These declines in total “deaths of despair” mortality were overwhelmingly driven by substantial declines in death rates from alcohol use. Second, the largest increases in “deaths of despair” mortality for White men and women occurred in the same age group (35–49 years), increasing by 41.8 deaths and 77.1 deaths per 100,000, respectively. Third, increases in drug-related deaths account for the overwhelming share of increases in “deaths of despair” mortality among both US Black and White populations. Grouping the separate causes into one “deaths of despair” category masks the fact that increases in drug-related deaths account for 60%–90% of all increases in “deaths of despair” death rates among White Americans, depending on age (to calculate: “deaths of despair” deaths attributable to drug-related mortality = (2017(drug) − 1990(drug))/(2017(deaths of despair) − 1990(deaths of despair))). This proportion is the highest for Whites aged 20–34 years (88% for women and 89% for men) and lowest for Whites aged 50–64 years (61% for women and 58% for men). For Black men and women, drug-related deaths account for 100% of increases in “deaths of despair” death rates, regardless of age group.
Table 1.
Age-Standardized Mortality Rates per 100,000 from “Deaths of Despair” by Age, Race, and Sex, United States, 1990–2017
| Cause and Age Group, years | White Women | Black Women | White Men | Black Men | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1990 | 2004 | 2017 | 1990 | 2004 | 2017 | 1990 | 2004 | 2017 | 1990 | 2004 | 2017 | |
| Deaths of despaira | ||||||||||||
| 20–34 | 7.9 | 14.0 | 36.0 | 9.5 | 6.9 | 17.4 | 33.7 | 49.2 | 106.5 | 35.3 | 29.2 | 52.2 |
| 35–49 | 16.2 | 34.5 | 58.0 | 35.6 | 27.4 | 32.6 | 51.7 | 80.7 | 128.8 | 107.0 | 60.3 | 70.8 |
| 50–64 | 28.4 | 33.7 | 69.3 | 40.3 | 29.7 | 49.8 | 79.5 | 90.3 | 155.5 | 145.0 | 115.9 | 152.7 |
| Suicide | ||||||||||||
| 20–34 | 5.5 | 5.3 | 8.1 | 3.2 | 3.0 | 4.3 | 27.1 | 25.2 | 34.1 | 20.0 | 17.7 | 20.7 |
| 35–49 | 7.8 | 9.2 | 12.6 | 3.9 | 2.7 | 4.1 | 26.2 | 29.7 | 39.0 | 15.3 | 10.9 | 14.4 |
| 50–64 | 8.3 | 8.4 | 13.5 | 2.6 | 1.9 | 2.7 | 27.5 | 26.9 | 39.0 | 10.6 | 9.3 | 9.4 |
| Alcohol | ||||||||||||
| 20–34 | 0.9 | 0.6 | 1.7 | 2.6 | 0.4 | 0.5 | 1.8 | 1.5 | 2.6 | 6.9 | 1.7 | 1.0 |
| 35–49 | 6.5 | 9.5 | 12.2 | 27.2 | 8.2 | 7.8 | 20.3 | 23.2 | 23.5 | 76.3 | 21.6 | 13.6 |
| 50–64 | 18.5 | 17.2 | 29.1 | 36.3 | 18.4 | 19.8 | 50.7 | 51.7 | 70.8 | 129.2 | 73.7 | 58.3 |
| Drug use | ||||||||||||
| 20–34 | 1.5 | 8.1 | 26.2 | 3.7 | 3.5 | 12.5 | 4.8 | 22.5 | 69.8 | 8.4 | 9.8 | 30.5 |
| 35–49 | 1.9 | 15.8 | 33.2 | 4.5 | 16.5 | 20.7 | 5.2 | 27.8 | 66.3 | 15.4 | 27.8 | 52.8 |
| 50–64 | 1.6 | 8.1 | 26.7 | 1.4 | 9.4 | 27.3 | 1.3 | 11.7 | 45.7 | 5.2 | 32.9 | 85.0 |
a Aggregate mortality rates from suicide, alcohol use, and drug use.
Given the large influence of drug-related deaths in shaping “deaths of despair” trends in both the US Black and White populations, we plotted age-standardized mortality rates from drug use according to 5-year age group, race, and sex (Figure 1). We observed increases in drug-related death rates for all age, race, and sex groups. These findings show, first, that across age groups, mortality rates for White men are similar in their rate of change until roughly 2013. That is, rates of drug-related mortality have been steadily increasing for all White men since the mid-1990s, with a pronounced increase in 2013 for White men aged 20–34 and 35–49 years. Drug-related death rates among White women are similar across age group in both the level and rate of change. Second, for Black men and women, we observe different patterns by age group. For older Black men, ages 50–64, we see increases similar to those observed in the White population. Among younger Black men, ages 20–34, the increase in drug-related mortality does not take off until 2013. Together, these different trends by age strongly suggest period effects in drug-related mortality among White Americans and both period and cohort effects among Black Americans. We further investigated period and cohort-based trends in the 3 “deaths of despair” causes using APC models. These types of analyses are helpful in disentangling whether the mortality increases are unique to specific cohorts or are shared among all ages (i.e., period-based).
Figure 1.
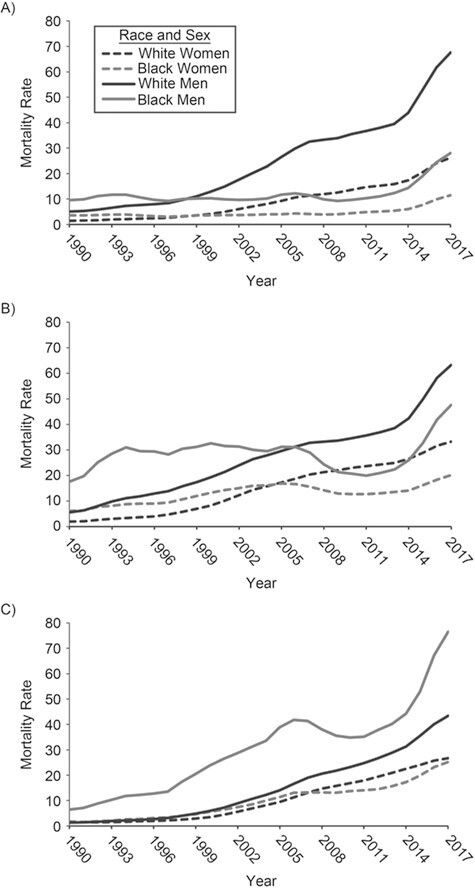
Age-standardized mortality rates per 100,000 from drug-related mortality according to race and sex, United States, 1990–2017. A) Ages 20–34 years; B) ages 35–49; C) ages 50–64.
Figures 2 (women) and 3 (men) plot cohort- and period-based variation in death rates from suicide, alcohol use, and drug use, separately by race/ethnicity. All graphs from APC models are plotted at the means. These results highlight several similarities in US Black and White mortality trends from “deaths of despair.” First, alcohol-related mortality has declined across US Black and White men’s and women’s birth cohorts, but the reductions have been greater for White men and women than for Black men and women. However, it is possible that the youngest cohorts have not yet had the exposure time necessary to warrant death from alcohol-related conditions, given that rates increase with age (41). Second, beginning in the late 2000s, there are steady period-based increases in alcohol-related death rates among Black and White men and women. Yet, among White men and women, these period-based increases in alcohol-related deaths followed years in which alcohol-related deaths were stable. In contrast, the increases among Black men and women reversed a long-term period trend of consistent reductions in alcohol-related deaths. Third, Figures 2 and 3 suggest significant period-based increases in drug-related mortality for all 4 race/sex groups, although some differences in the trends exist. For example, rates are estimated to have rapidly increased beginning in the late 1990s, with a steeper rate of increase observed for the White population than for the Black population during the 1990s and 2000s. However, across more recent years, period-based increases in drug-related mortality have been more pronounced among Black Americans than White Americans. Additionally, results suggest a more pronounced cohort effect on drug-related death trends among the Black population, whereby there were increases for cohorts born between 1941 and 1956. Further, period-based suicide for White men and women increased modestly beginning in 2005. Yet, rates suggest no period-based or cohort-based increases in suicide for Black men and women. As such, the observed suicide trends provide the greatest difference in “deaths of despair” trends across race.
Figure 2.
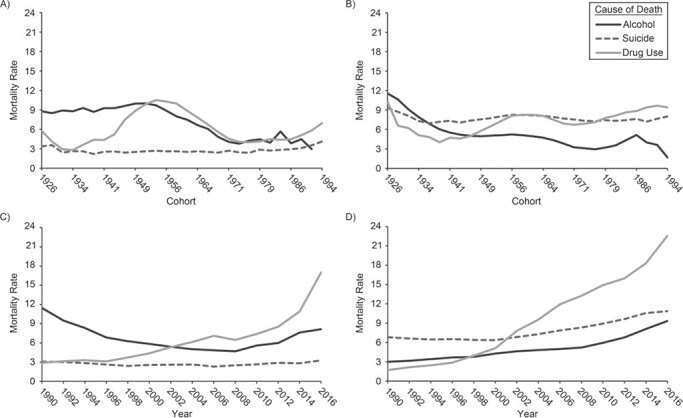
Women’s cohort- and period-based variation in “deaths of despair” mortality, United States, years 1990–2017 and cohorts 1926–1994. A) Black women, cohort; B) White women, cohort; C) Black women, period; D) White women, period. Estimates are mortality rates per 100,000 person-years.
Figure 3.
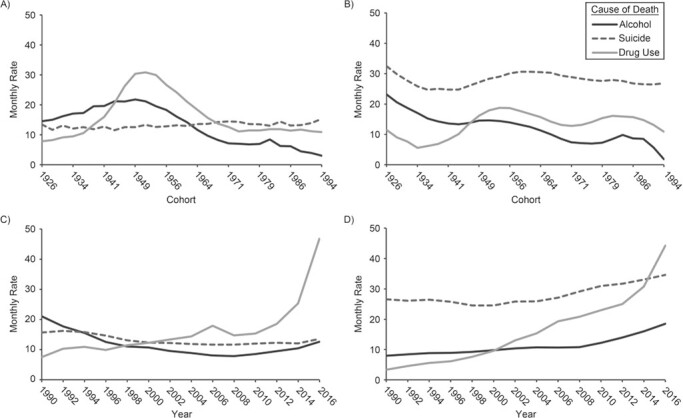
Men’s cohort- and period- based variation in “deaths of despair” mortality, United States, years 1990–2017 and cohorts 1926–1994. A) Black men, cohort; B) White men, cohort; C) Black men, period; D) White men, period. Estimates are mortality rates per 100,000 person-years.
DISCUSSION
Recent life-expectancy declines among the US White population have attracted widespread attention from health researchers, media, and the public. Deaths from suicides, drug use, and alcohol use in midlife have contributed to some of these declines, and scholars have argued that rising “despair” is the underlying driver of these recent trends (5, 6, 42). Yet, in the pursuit of the underlying explanations for rising US White mortality, researchers have largely overlooked Black working-aged mortality from these same causes. Our findings suggest that Black Americans exhibit concerning mortality trends that are similar to those observed in the US White population and that mortality trends in both populations appear to track alongside the timing of the US opioid epidemic and the Great Recession, with the country’s delayed and unequal economic recovery. While we note some age, race, and sex differences in the timing and levels of mortality across certain causes of death (e.g., large cohort effects on trends in Black American’s drug-related mortality), we argue that the drivers of recent declines in working-aged mortality in the United States are likely widespread.
The first takeaway from this study is that period-based increases in drug-related mortality for White and Black Americans provide additional evidence that the opioid epidemic extends beyond just the White population (43). Although research indicates that there are racial differences in the type of medical care received (44), and that Black Americans, on average, are prescribed fewer painkillers (45), our findings suggest that the opioid epidemic and associated changes in the drug environment have affected drug-related death rates among US Black men and women. Indeed, both Black and White Americans experienced period-based drug-related mortality increases that coincide with the shift in the US drug environment as a result of changes in policies and practices regarding the prescription of opioid-based painkillers in the medical industry (46–50). Increases in drug-related mortality in the 1990s and 2000s was observed among White men and women of all ages but only among older Black men and women. Results from APC analyses further suggest that trends in drug-related deaths among Black Americans exhibit a strong cohort component. Future research ought to investigate how and why early increases in drug-related deaths among Black Americans were concentrated among older ages and earlier cohorts. For example, recent research suggests that since 2010, rising opioid mortality among both Black and White Americans is now largely driven by heroin and synthetic opioids (e.g., fentanyl) (43). While recent drug-related mortality among Black and White Americans in the latest wave of the opioid epidemic is certainly concerning, we document rising drug mortality among older cohorts of Black Americans beginning in earlier waves of the epidemic. Future work could consider these distinct waves of the opioid epidemic, examine racial/ethnic mortality differences by drug type, and extend analyses of drug use and overdose beyond opioids (e.g., cocaine, psychostimulants).
Second, period-based trends in Black and White alcohol-related mortality and White suicide track strongly with the timing of the Great Recession, suggesting mortality consequences from the stress and hardships associated with the recession and recovery (51, 52). Although research indicates that socioeconomic status confounds the relationship between race and recession effects (53), our results suggest that the experience of societal-wide economic downturn is a period shock felt by both Black and White Americans. Moreover, while cohort-based alcohol mortality has declined for both White and Black Americans—possibly attributable to the lagged effect of heavy alcohol consumption on risk of mortality (54)—these period-based increases in alcohol-related mortality are troubling and future research should continue to investigate these trends. This study is also not unique in observing higher rates of suicide mortality for White Americans compared with racial/ethnic minorities (55). Explanations for lower rates of suicide mortality among the Black population are varied (55–59) and warrant continued examination given that this remains the largest difference in “deaths of despair” trends across race. Among the White population, the period-based suicide increases are undoubtedly troubling, and these suicide trends might indeed be a result of declines in mental health or rising despair and hopelessness. However, our study cannot attribute these period-based suicide increases to rising distress and despair without data that includes both mental health assessments and follow-up mortality data. As such, we can only conclude that the increases in suicide among the White population seem to coincide with the onset of the Great Recession and reflect existing research documenting the association between suicide and economic downturns (15–18).
Our study is not without limitations. Future research could analyze what social factors, beyond the Great Recession and the opioid epidemic, contribute to the trends documented here. Further, these results likely extend to other racial/ethnic groups beyond those analyzed in this study. Finally, there are some concerns regarding the use of APC models to statistically identify period-based and cohort-based variation in mortality (31, 40, 60–63). Web Appendix 1 and Web Figures 4 and 5 provides sensitivity analyses that test within-method and between-method differences in model estimates and also provide extensive descriptive analyses that are consistent with the APC results presented above.
Although results must be interpreted with these limitations in mind, our findings clearly suggest that recent mortality trends among working-aged US Black and White men and women are more similar than different. These findings are important because they highlight the need to examine the structural explanations for rising mortality rates in the United States. This important point is overlooked when the causes from “deaths of despair” are bundled together, when the mortality trends are observed across shorter time periods, or when “deaths of despair” are analyzed only among the White population. Overall, the results presented in this study point to shared mortality trends that coincide with 2 period-based structural shocks: the Great Recession and the opioid epidemic. In light of these findings, we continue to advocate that scholars shift their attention away from the elusive search for the drivers of “rising despair” in the White population and instead turn their attention to addressing the roots of recent mortality changes, notably the increasingly concerning drug environment in the United States, and the social and economic inequalities made worse by the Great Recession.
Supplementary Material
ACKNOWLEDGMENTS
Author affiliations: Department of Sociology, University of Colorado Boulder, Boulder Colorado (Andrea M. Tilstra, Daniel H. Simon, Ryan K. Masters); Population Program, CU Population Center, Institute of Behavioral Science, University of Colorado Boulder, Boulder Colorado (Andrea M. Tilstra, Daniel H. Simon, Ryan K. Masters); and Health and Society Program, Institute of Behavioral Science, University of Colorado Boulder, Boulder, Colorado (Ryan K. Masters).
This work was funded by the University of Colorado Population Center grant from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (CUPC project 2P2CHD066613) and the National Institute on Aging (grant NIA R24AG0405061). The National Association for Public Health Statistics and Information Systems and the National Vital Statistics Systems provided data access.
Previous versions of this manuscript were presented at the University of Colorado Boulder Sociology Department’s Population and Health Working Group and at the 2019 annual meeting of the Population Association of America, April 10–13, 2019, Austin, Texas.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Child Health and Human Development, National Institutes of Health, National Institute on Aging, National Association for Public Health Statistics and Information Systems, or the National Vital Statistics Systems.
Conflict of interest: none declared.
REFERENCES
- 1. Murphy SL, Xu JQ, Kochanek KD, et al. Mortality in the United States, 2017. Hyattsville, MD: National Center for Health Statistics. 2018. (NCHS Data Brief, no. 328.) https://www.cdc.gov/nchs/data/databriefs/db328-h.pdf. Accessed February 1, 2020. [Google Scholar]
- 2. Xu J, Murphy SL, Kochanek KD, et al. Mortality in the United States, 2015. Hyattsville, MD: National Center for Health Statistics. 2016. (NCHS Data Brief, no. 267.) https://www.cdc.gov/nchs/data/databriefs/db267.pdf. Accessed February 1, 2020. [Google Scholar]
- 3. Hedegaard H, Curtin SC, Warner M. Suicide rates in the United States continue to increase. Hyattsville, MD: National Center for Health Statistics. 2018. (NCHS Data Brief, no. 309). https://www.cdc.gov/nchs/data/databriefs/db309.pdf. Accessed February 1, 2020. [PubMed] [Google Scholar]
- 4. Hedegaard H, Miniño AM, Warner M. Drug overdose deaths in the United States, 1999–2017. Hyattsville, MD: National Center for Health Statistics. 2018. (NCHS Data Brief, no. 329). https://www.cdc.gov/nchs/data/databriefs/db329-h.pdf. Accessed February 1, 2020. [Google Scholar]
- 5. Case A, Deaton A. Rising morbidity and mortality in midlife among White non-Hispanic Americans in the 21st century. Proc Natl Acad Sci U S A. 2015;112(49):15078–15083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Case A, Deaton A. Mortality and morbidity in the 21st century. Brookings Pap Econ Act. 2017;2017(1):397–476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Kochanek KD, Arias E, Bastian BA The effect of changes in selected age-specific causes of death on non-Hispanic White life expectancy between 2000 and 2014. Hyattsville, MD: National Center for Health Statistics. 2016. (NCHS Data Brief, no. 250.). https://www.cdc.gov/nchs/data/databriefs/db267.pdf. Accessed February 1, 2020. [PubMed] [Google Scholar]
- 8. Meara E, Skinner J. Losing ground at midlife in America. Proc Natl Acad Sci. 2015;112(49):15006–15007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Shiels MS, Chernyavskiy P, Anderson WF, et al. Trends in premature mortality in the USA by sex, race, and ethnicity from 1999 to 2014: an analysis of death certificate data. Lancet. 2017;389(10073):1043–1054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Wilson WJ. When Work Disappears: The World of the New Urban Poor. New York, NY: Vintage Books; 1997. [Google Scholar]
- 11. Masters RK, Tilstra AM, Simon DH. Mortality from suicide, chronic liver disease, and drug poisonings among middle-aged U.S. White men and women, 1980--2013. Biodemography Soc Biol. 2017;63(1):31–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Masters RK, Tilstra AM, Simon DH. Explaining recent mortality trends among younger and middle-aged White Americans. Int J Epidemiol. 2018;47(1):81–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Ruhm CJ. Drivers of the fatal drug epidemic. J Health Econ. 2019;64:25–42. [DOI] [PubMed] [Google Scholar]
- 14. Alpert AE, Evans WN, Lieber EM, et al. Origins of the opioid crisis and its enduring impacts. Cambridge, MA: National Bureau of Economic Research. 2019. (No. w26500). https://www.nber.org/papers/w26500. Accessed February 1, 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Reeves A, Stuckler D, McKee M, et al. Increase in state suicide rates in the USA during economic recession. Lancet. 2012;380(9856):1813–1814. [DOI] [PubMed] [Google Scholar]
- 16. Coope C, Donovan J, Wilson C, et al. Characteristics of people dying by suicide after job loss, financial difficulties and other economic stressors during a period of recession (2010–2011): a review of coroners′ records. J Affect Disord. 2015;183:98–105. [DOI] [PubMed] [Google Scholar]
- 17. Oyesanya M, Lopez-Morinigo J, Dutta R. Systematic review of suicide in economic recession. World J Psychiatry. 2015;5(2):243–254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Phillips JA, Nugent CN. Suicide and the Great Recession of 2007-2009: the role of economic factors in the 50 U.S. states. Soc Sci Med. 2014;116:22–31. [DOI] [PubMed] [Google Scholar]
- 19. Cassidy J. Why did the death rate rise among middle-aged White Americans. New Yorker. https://www.newyorker.com/news/john-cassidy/why-is-the-death-rate-rising-among-middle-aged-white-americans. Published November 9, 2015 Accessed February 1, 2020. [Google Scholar]
- 20. Pierce JR, Schott PK. Trade liberalization and mortality: evidence from US counties. American Economic Review: Insights. 2020;2(1):47–64. [Google Scholar]
- 21. Venkataramani AS, Bair EF, O’Brien RL, et al. Association between automotive assembly plant closures and opioid overdose mortality in the United States: a difference-in-differences analysis. JAMA Intern Med. 2020;180(2):254–262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Douthat R. The dying of the Whites. New York Times. https://www.nytimes.com/2015/11/08/opinion/sunday/the-dying-of-the-whites.html. Published November 7, 2015 Accessed February 1, 2020. [Google Scholar]
- 23. Krugman P. Despair, American style. New York Times. https://www.nytimes.com/2015/11/09/opinion/despair-american-style.html. Published November 9, 2015. Accessed February 1, 2020. [Google Scholar]
- 24. Kristof ND, WuDunn S. Who killed the Knapp family? New York Times. https://www.nytimes.com/2020/01/09/opinion/sunday/deaths-despair-poverty.html. Published January 9, 2020. Accessed January 9, 2020. [Google Scholar]
- 25. Diez Roux AV. Despair as a cause of death: more complex than it first appears. Am J Public Health. 2017;107(10):1566–1567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Katz J, Goodnough A. The opioid crisis is getting worse, particularly for Black Americans. New York Times. https://www.nytimes.com/interactive/2017/12/22/upshot/opioid-deaths-are-spreading-rapidly-into-black-america.html. Published December 22, 2017. Accessed February 1, 2020. [Google Scholar]
- 27. Schmitz Bechteler S, Kane-Willis K. Whitewashed: The African American Opioid Epidemic. Chicago, IL: The Chicago Urban League. Research and Policy Center. 2017. https://chiul.org/wp-content/uploads/2019/01/Whitewashed-AA-Opioid-Crisis-11-15-17_EMBARGOED_-FINAL.pdf. Accessed February 1, 2020. [Google Scholar]
- 28. National Vital Statistics System . Datasets and related documentation: mortality multiple cause-of-death data. Atlanta, GA: National Center for Health Statistics. https://www.cdc.gov/nchs/nvss/mortality_public_use_data.htm. Accessed June 14, 2021. [Google Scholar]
- 29. Woolf SH, Schoomaker H. Life expectancy and mortality rates in the United States, 1959-2017. JAMA. 2019;322(20):1996–2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Powers D, Xie Y. Statistical Methods for Categorical Data Analysis. Bingley, UK: Emerald Group Publishing; 2008. [Google Scholar]
- 31. Yang YC, Land KC. Age-Period-Cohort Analysis: New Models, Methods, and Empirical Applications. Boca Raton, FL: CRC Press; 2013. [Google Scholar]
- 32. Fu W. Constrained estimators and consistency of a regression model on a Lexis diagram. J Am Stat Assoc. 2016;111(513):180–199. [Google Scholar]
- 33. Masters RK, Powers DA. Clarifying assumptions in age-period-cohort analyses and validating results. PLoS One. 2020;15(10):e0238871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Yang Y, Schulhofer-Wohl S, Fu WJ, et al. The intrinsic estimator for age-period-cohort analysis: what it is and how to use it. Am J Sociol. 2008;113(6):1697–1736. [Google Scholar]
- 35. Van Zee A. The promotion and marketing of oxycontin: commercial triumph, public health tragedy. Am J Public Health. 2009;99(2):221–227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Centers for Disease Control and Prevention . Understanding the epidemic. https://www.cdc.gov/drugoverdose/epidemic/index.html. Accessed February 1, 2020.
- 37. Masters RK, Hummer RA, Powers DA, et al. Long-term trends in adult mortality for U.S. Blacks and Whites: an examination of period- and cohort-based changes. Demography. 2014;51(6):2047–2073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Cutler DM, Huang W, Lleras-Muney A. When does education matter? The protective effect of education for cohorts graduating in bad times. Soc Sci Med. 2015;127:63–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Crystal S, Shea DG, Reyes AM. Cumulative advantage, cumulative disadvantage, and evolving patterns of late-life inequality. Gerontologist. 2017;57(5):910–920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Masters RK, Powers DA, Hummer RA, et al. Fitting age-period-cohort models using the intrinsic estimator: assumptions and misapplications. Demography. 2016;53(4):1253–1259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Heron MP. Deaths: leading causes for 2017. National Vital Statistics System; 2019. (Volume 68, number 6). https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_06-508.pdf. Accessed February 1, 2020. [PubMed]
- 42. Case A, Deaton A. Deaths of Despair and the Future of Capitalism. Princeton, NJ: Princeton University Press; 2020. [Google Scholar]
- 43. Alexander MJ, Kiang MV, Barbieri M. Trends in Black and White opioid mortality in the United States, 1979–2015. Epidemiology. 2018;29(5):707–715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Epstein AM, Ayanian JZ. Racial disparities in medical care. N Engl J Med. 2001;344(19):1471–1473. [DOI] [PubMed] [Google Scholar]
- 45. Pletcher MJ, Kertesz SG, Kohn MA, et al. Trends in opioid prescribing by race/ethnicity for patients seeking care in US emergency departments. JAMA. 2008;299(1):70–78. [DOI] [PubMed] [Google Scholar]
- 46. Dart RC, Surratt HL, Cicero TJ, et al. Trends in opioid analgesic abuse and mortality in the United States. N Engl J Med. 2015;372(3):241–248. [DOI] [PubMed] [Google Scholar]
- 47. Manchikanti L, Helm 2nd S, Fellows B, et al. Opioid epidemic in the United States. Pain Physician. 2012;15(3):ES9–ES38. [PubMed] [Google Scholar]
- 48. Mularski RA, White-Chu F, Overbay D, et al. Measuring pain as the 5th vital sign does not improve quality of pain management. J Gen Intern Med. 2006;21(6):607–612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Rudd RA, Aleshire N, Zibbell JE, et al. Increases in drug and opioid overdose deaths—United States, 2000–2014. Am J Transplant. 2016;16(4):1323–1327. [DOI] [PubMed] [Google Scholar]
- 50. Volkow ND, Frieden TR, Hyde PS, et al. Medication-assisted therapies—tackling the opioid-overdose epidemic. N Engl J Med. 2014;370(22):2063–2066. [DOI] [PubMed] [Google Scholar]
- 51. Boen C, Yang YC. The physiological impacts of wealth shocks in late life: evidence from the Great Recession. Soc Sci Med. 2016;150:221–230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Yilmazer T, Babiarz P, Liu F. The impact of diminished housing wealth on health in the United States: evidence from the Great Recession. Soc Sci Med. 2015;130:234–241. [DOI] [PubMed] [Google Scholar]
- 53. Pfeffer FT, Danziger S, Schoeni RF. Wealth disparities before and after the Great Recession. Ann Am Acad Pol Soc Sci. 2013;650(1):98–123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Marmot MG, Shipley MJ, Rose G, et al. Alcohol and mortality: a U-shaped curve. Lancet. 1981;317(8220):580–583. [DOI] [PubMed] [Google Scholar]
- 55. Rockett IRH, Wang S, Stack S, et al. Race/ethnicity and potential suicide misclassification: window on a minority suicide paradox? BMC Psychiatry. 2010;10(1):35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Kubrin CE, Wadsworth T, DiPietro S. Deindustrialization, disadvantage and suicide among young Black males. Soc Forces. 2006;84(3):1559–1579. [Google Scholar]
- 57. Rockett IR, Samora JB, Coben JH. The Black–White suicide paradox: possible effects of misclassification. Soc Sci Med. 2006;63(8):2165–2175. [DOI] [PubMed] [Google Scholar]
- 58. Spates K, Slatton BC. I’ve got my family and my faith: black women and the suicide paradox. Socius. 2017;3:237802311774390. [Google Scholar]
- 59. Stack S. The relationship between culture and suicide: an analysis of African Americans. Transcult Psychiatry. 1998;35(2):253–269. [Google Scholar]
- 60. Fosse E, Winship C. Bounding analyses of age-period-cohort effects. Demography. 2019;56(5):1975–2004. [DOI] [PubMed] [Google Scholar]
- 61. Luo L. Assessing validity and application scope of the intrinsic estimator approach to the age-period-cohort problem. Demography. 2013;50(6):1945–1967. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Luo L, Hodges J, Winship C, et al. The sensitivity of the intrinsic estimator to coding schemes: comment on Yang, Schulhofer-Wohl, Fu, and Land. Am J Sociol. 2016;122(3):930–961. [Google Scholar]
- 63. Pelzer B, Te Grotenhuis M, Eisinga R, et al. The non-uniqueness property of the intrinsic estimator in APC models. Demography. 2015;52(1):315–327. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.