

Abstract
Objectives:
To determine if changes in pelvic trauma care and treatment protocols has affected overall mortality rates after pelvic ring injury.
Design:
Retrospective chart review.
Setting:
Level I trauma center.
Patients/Participants:
A total of 3314 patients with pelvic ring injuries who presented to a single referral center from 1999 through 2018.
Intervention:
Cohort comparison (years 1999 through 2006) and (years 2007 through 2018).
Main Outcome Measurements:
Change in patient demographic data, fracture characteristics, date of injury, associated injuries, length of hospital stay, Abbreviated Injury Severity Score (AIS), and in-hospital mortality.
Results:
The composite mortality rate was 6.5% (214/3314). The earliest cohort presented a mortality rate of 9.1% (111/1224; 95% confidence interval [CI], 7.6–10.8%) compared to the more recent cohort mortality rate of 4.9% (103/2090; 95% CI, 4.1–5.9%). Overall mortality was significantly lower in the more recent time period, a risk difference of 4.1% (95% CI, 2.3–6.1%; P < 0.01). After adjusting for age and AIS of the brain, chest, and abdomen, the mortality reduction was more pronounced with an adjusted risk difference of 6.4% (95% CI, 4.7–8.1%; P < 0.01).
Conclusion:
Significant improvement in the mortality rate of pelvic ring injuries has been demonstrated in recent years (4.9% versus 9.1%). Improvement coincides chronologically with changes in trauma resuscitation and implementation of adjuvant treatments for managing patients with severe hemorrhagic shock. Although the exact benefit of each treatment awaits further research, this data might indicate improved care for these difficult patients.
Level of Evidence:
Therapeutic Level III. See Instructions for Authors for a complete description of levels of evidence.
Keywords: pelvic ring injuries, mortality rates, pelvic ring fractures
INTRODUCTION
Fractures of the pelvic ring are relatively rare, but often offer a significant challenge in terms of management.1 Trauma patients with pelvic fractures typically have multiple injuries contributing to the difficulty of managing these patients and frequently having a significant impact on patient outcome.2-4 Pelvic ring injuries typically result from high-energy trauma and numerous investigations have noted a high mortality and complication rate associated with them.5-9
In one of the original investigations regarding pelvis fractures, Burgess et al.10 reported a mortality of 8.6%. In a similar investigation performed at the same trauma center 15 years later, Manson et al.4 reported a nearly identical mortality rate associated with these fractures at 9.1%. This data would suggest that over the course of two decades little progress was made in terms of decreasing the mortality of patients sustaining pelvic ring fractures. Naturally, this raises the question as to whether any current progress has been made within this realm.
Management of the critically ill patient has evolved over the course of recent years with new data and techniques available to guide treatment. In the past decade changes in resuscitation strategy, and more frequent use of tranexamic acid (TXA), resuscitative endovascular balloon occlusion of the aorta (REBOA), and dedicated trauma angiography rooms might have affected the mortality associated with pelvic ring injuries.9,11-19 The primary goal of this investigation was to evaluate the mortality rate of pelvic ring fractures in recent years while making comparisons to prior publications. Our hypothesis is that despite changes in pelvic trauma care, the overall mortality after pelvic ring injury remains unchanged.
METHODS
This study was performed by retrospectively reviewing consecutive patient charts from a prospectively maintained trauma database at a single Level I trauma center. After receiving institutional review board approval, patients with pelvic ring fractures were identified using Current Procedural Terminology (CPT) codes (CPT 27193, 27194, 27216, 27217, 27218) over a 19-year study period from January 1999 through January 2018.
Inclusion Criteria
Patients were included in the study if they were 18 years of age or greater and had sustained a blunt pelvic ring injury. Both operatively treated and nonoperatively managed fractures were included. Patients had to have initial injury radiographs and/or computed tomography (CT) imaging completed. All included patients had the pelvic ring injury classified by a fellowship-trained orthopaedic trauma surgeon in accordance with the Young-Burgess classification.10
Exclusion Criteria
Patients were excluded from the study if they had a fracture of the acetabulum. Additionally, patients who underwent surgical stabilization of the pelvis for pathologic instability, nonunion or malunion, or lumbopelvic instability were excluded. Ballistic pelvic ring injuries were also excluded, as were those injuries that did not disrupt the pelvic ring, such as isolated injuries to the iliac wing or avulsion fractures of the iliac spine.
Study Group
The database was queried to determine patient demographic data, fracture characteristics, date of injury, associated injuries, length of hospital stay, Abbreviated Injury Severity Score (AIS), mechanism of injury, and in-hospital mortality. A previously published cohort (years 1999 through 2006) was compared to a more recent cohort (years 2007 through 2018) of patients. Abbreviated Injury Severity scores were calculated by trained trauma registrars who manually assigns these values.
In total 3314 patients who sustained a fracture of the pelvic ring were identified. The distribution of fractures per Young-Burgess classification10 was as follows: 2025 lateral compression (LC) type 1, 347 LC-2, 218 LC-3, 59 anteroposterior compression (APC) type 1, 426 APC-2, 145 APC-3, 30 vertical shear, and 57 combined mechanism injuries (Figure 1).
Figure 1.
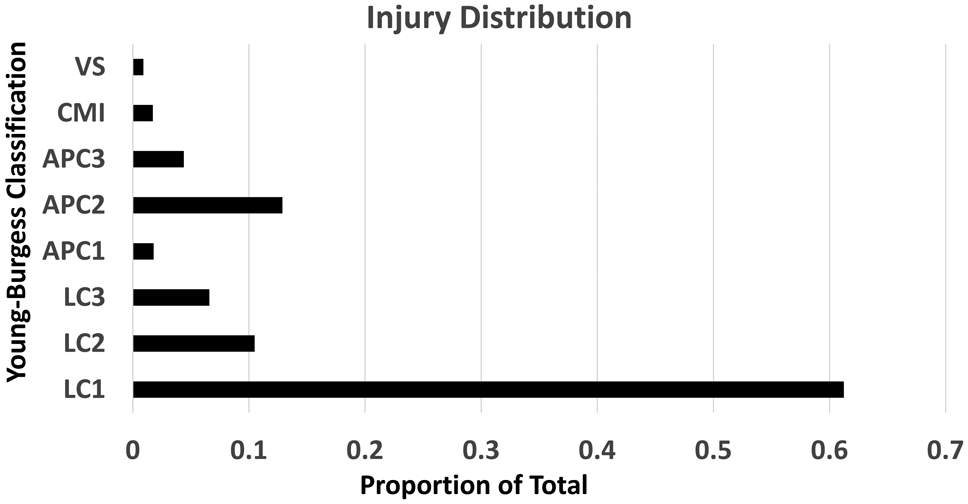
Injury distribution for all injuries.
Statistical Analysis
Patient characteristics were described using means with standard deviations for continuous variables, and with counts and proportions for categorical variables. Generalized linear regression was used to determine the absolute and relative differences in mortality between the new data and previously reported data. Absolute effects were reported as the risk difference. Relative effects were reported as odds ratios. Crude and standardized results were reported for all models. The standardized models were adjusted for patient age, and AIS score for the brain, thorax, and abdominal regions. All analyses were performed using R version 3.6.1 (Vienna, Austria).
RESULTS
The mean patient age for the study was 42.5 years (standard deviation, 20.2). Males represented 55.3% of the patients. The previous cohort had 1224 patients with a mean age of 39.1 years of which 54.6% were male (Table 1). The more recent cohort included 2090 patients with an average age of 44.4 years with 55.8% of these patients being male. Hospital length of stay did not differ between the groups at 10.6 and 10.7 days, respectively. AIS scores were also similar between the 2 groups.
TABLE 1.
Patient Characteristics
| Previous Data (1999-2006) (n=1224) |
Recent Data (2007-2018 (n=2090) |
Overall (n=3314) |
|
|---|---|---|---|
| Age (years)* | 39.1 (18.7) | 44.4 (20.8) | 42.5 (20.2) |
| Sex, Male (%) | 668 (54.6%) | 1166 (55.8%) | 1834 (55.3%) |
| Pelvis classification (%) | |||
| APC1 | 31 (2.5%) | 28 (1.3%) | 59 (1.8%) |
| APC2 | 141 (11.5%) | 285 (13.6%) | 426 (12.9%) |
| APC3 | 54 (4.4%) | 91 (4.4%) | 145 (4.4%) |
| CMI | 38 (3.1%) | 19 (0.9%) | 57 (1.7%) |
| LC1 | 763 (62.3%) | 1269 (60.7%) | 2025 (61.1%) |
| LC2 | 105 (8.6%) | 242 (11.6%) | 347 (10.5%) |
| LC3 | 74 (6.0%) | 144 (6.9%) | 218 (6.6%) |
| VS | 18 (1.5%) | 12 (0.6%) | 30 (0.9%) |
| Hospital Length of Stay (days)* | 10.6 (14.4) | 10.7 (13.4) | 10.7 (13.7) |
| ICU Stay (days)* | 5.4 (11.8) | 5.1 (11.2) | 5.3 (11.4) |
| AIS Brain* | 0.9 (1.6) | 1.1 (1.6) | 1.1 (1.6) |
| AIS Face* | 0.5 (0.7) | 0.5 (0.7) | 0.5 (0.7) |
| AIS Neck* | 0.03 (0.2) | 0.2 (0.6) | 0.1 (0.5) |
| AIS Thorax* | 1.6 (1.6) | 1.7 (1.7) | 1.7 (1.7) |
| AIS Abdomen* | 1.0 (1.4) | 1.3 (1.5) | 1.2 (1.4) |
| AIS Upper Extremity* | 0.9 (1.1) | 1.0 (1.1) | 1.0 (1.1) |
| AIS Lower Extremity* | 2.6 (0.7) | 2.7 (0.7) | 2.7 (0.7) |
| Mechanism (%) | |||
| Motor Vehicle/Motorcycle | 820 (67%) | 1442 (68.9%) | 1962 (59.2%) |
| Fall | 135 (11%) | 209 (10%) | 344 (10.4%) |
| Pedestrian Struck | 201 (16.4%) | 323 (15.5%) | 524 (15.8%) |
| Heavy Machinery | 9 (0.7%) | 15 (0.7%) | 24 (0.7%) |
| Assault | 6 (0.4%) | 4 (0.1%) | 10 (0.3%) |
| Other | 53 (4.3%) | 397 (19%) | 450 (13.6%) |
| Transfusion | 171 (14%) | 261 (12.5%) | 432 (13%) |
Represent mean (standard deviation)
APC, anteroposterior compression; CMI, combined mechanism injuries; LC, lateral compression; VS, vertical shear; AIS, Abbreviated Injury Severity Score.
The composite mortality rate of the study cohort was 6.5% (214/3314). In the cohort from 1999 through 2006 the mortality rate was 9.1% (111/1224; 95% confidence interval [CI], 7.6–10.8%) compared to the more recent cohort mortality rate of 4.9% (103/2090; 95% CI, 4.1–5.9%). The overall mortality was significantly lower in the more recent time period (risk difference, 4.1%; 95% CI, 2.3–6.1%; P < 0.01). After adjusting for age and AIS of the brain, chest, and abdomen, the mortality reduction was more pronounced with an adjusted risk difference of 6.4% (95% CI, 4.7–8.1%; P < 0.01) (Table 2). When adjusting for fracture type (APC-3, VS, CMI) the adjusted risk difference remained nearly identical at 4.1% (95% CI: 2.3% to 6.0%, P < 0.01). A total of 171 (14%) patients received a transfusion from 1999 to 2006 compared to 261 (12.5%) patients from 2007 to 2018 (P = 0.12).
TABLE 2.
Difference in In-Hospital Mortality Rate Between New and Current Data
| N | Mortality Rate | OR (95% CI) | Adjusted OR* | Risk Difference (95% CI) |
Adjusted Risk Difference* |
|
|---|---|---|---|---|---|---|
| Previous Data (1999 – 2006) | 111/1224 | 9.1 (7.6 to 10.8) | Ref (1.00) | Ref (1.00) | Ref (0.00) | Ref (0.00) |
| New Data (2007-2018) | 103/2090 | 4.9 (4.1 to 5.9) | 0.52 (0.39 to 0.69) | 0.34 (0.25 to 0.46) | −4.1% (−6.1 to −2.3) | −6.4% (−8.1 to 4.7%) |
Adjusted for age, Abbreviated Injury Severity Score brain, Abbreviated Injury Severity Score thorax, and Abbreviated Injury Severity Score abdomen.
OR, odds ratio; CI, confidence interval.
From 1999 through 2006 the crude mortality rate was below 8% only twice, in 2001 and 2006. However, from 2007 to 2018 the mortality rate only exceeded 8% in a single year (2018) and was below 5% for a majority of that timeframe (Figure 2).
Figure 2.
Crude mortality by year.
DISCUSSION
Initial studies which provided the groundwork for the Young-Burgess classification of pelvic ring injuries noted a significant mortality rate associated with these injuries at 8.6%.10,20 Subsequent to this, and nearly 20 years following this landmark work, Manson et al.4 reported on a much larger cohort of pelvic fractures managed at the same trauma center while noting a very similar mortality rate at 9.1%. Additional studies performed around this time also noted a mortality of roughly 10%, suggesting a significant mortality across multiple centers in the United States.21-23 The results of the present study suggest that we have made significant gains in terms of the mortality associated with pelvic ring injuries, reducing the mortality rate to under 5%. This finding, which opposes our initial hypothesis, likely has an etiology which is multifactorial in nature.
Looking at the mortality trends on a yearly basis might be subject to anomalous findings and study fragility; however, the overall trend is quite stark. Beyond a single year (2002) mortality rates from 1999 through 2006 were at least 9%, but from 2007 through 2018 the rates remained well below 9% and were only above 8% once in 2018. Near the time of mortality rate improvement, resuscitation strategies in the trauma patient changed.16,24-28 Over the past 13 years substantial knowledge has been gained in the understanding of both coagulopathy and resuscitation strategies in trauma care.
Balanced resuscitation, which includes permissive hypotension, limited use of crystalloid, and transfusion of blood products in similar ratios to whole blood has set the new standard of care.16,24-29 These strategies which came into favor around the mid-2000s have helped to minimize the impact of trauma-induced coagulopathy and reduce the complications that occur with aggressive crystalloid resuscitation. In turn, the morbidity and mortality of patients with trauma in hemorrhagic shock has improved which may, in part, explain the improvement in mortality rates associated with pelvic ring injuries noted in the present study.
More recently, the addition of TXA to the treatment algorithm of the bleeding trauma patient has proven to be a valuable tool.19,30,31 Early administration of TXA to trauma patients with, or at risk of, significant bleeding reduces the risk of death from hemorrhage, with no apparent increased risk of vascular occlusive events.19,30,31 The effect of this intervention is quite pronounced, as prompt treatment with TXA reduces the risk of bleeding to death by about one-third.19,30,31 Furthermore, this appears to be a cost effective and widely available strategy that has been adopted by our center adding to the potential mortality benefit seen in this study. TXA use in trauma patients was adopted at surgeon discretion following some of the premiere studies in this arena around 2013.
Pelvic fractures presenting with hemodynamic instability present an additional level of complexity. The mortality of these injuries in the presence of hemorrhagic shock ranges from 40% to 60% and management of these patients should be multidisciplinary.32-37 Angiography and embolization in combination with temporary pelvic stabilization is a safe, effective, and widely accepted treatment tactic for pelvic fracture hemorrhage.37-41 Early access to angiography has been associated with reduced mortality with a delay in angiography and embolization portending a worse outcome.42-44 Interestingly, a new hybrid angiography suite was designated at our trauma center in 2015, decreasing trauma patient time to angiography and subsequent embolization. This combined with improvements in resuscitation strategies and the implementation of TXA, appears to be translating toward a mortality benefit in this challenging patient population.
Finally, the development and implementation of REBOA has also occurred over the study period with initial use at our center starting in early 2013.3,11-13,15,17,18,45 Although the use of REBOA continues to evolve, its primary application is in carefully selected patients with signs of near cardiac arrest from non-compressible hemorrhage. The value of this tool in managing the unstable patient with a pelvic ring injury is becoming more evident as an increasing number of trauma centers adopt the use of this catheter-based technology.3 Trauma center treatment algorithms are now incorporating the use of REBOA as a bridge to definitive hemostatic treatment in patients with severe pelvic trauma.3,46
Thromboelastography (TEG) is another technology which has been developed in recent years and is currently being used at our center. This test allows for surgeons to obtain a snapshot of a patient’s coagulation profile by evaluating clotting factors.47 TEG is now being used to assess coagulopathy and guide resuscitation. The adoption of this technology and use of this TEG blood test is another tool that may be contributing to the improved mortality seen in the present study.
Trauma patients with fractures of the pelvic ring are noted to have a higher mortality than those without pelvis fractures.48,49 Massive non-compressible hemorrhage remains the primary cause of death in trauma patients with pelvic ring injuries and thus, it makes sense that the various protocols focused on reducing the burden of hemorrhage (balanced resuscitation, use of TXA, improved access to angiography, and use of REBOA) have curtailed the mortality of these injuries.6,40
The variables of this study were collected in a prospective fashion; however, this does not eliminate the limitations resulting from its retrospective study design. Furthermore, we are limited by physician variability in terms of adoption and implementation of certain protocols. Although easy to determine when evidence of new resuscitation strategies and use of TXA was available to guide care, it is less clear when individual providers at our trauma center began to incorporate these strategies into patient management. Additionally, other unmeasured variables that have changed over time contributing to improved mortality in this patient population might exist, which we are simply failing to acknowledge. A certain number of patients present to the trauma center in extremis, and soon thereafter succumb to their injuries prior to the identification of a pelvis fracture, who therefore are not included in this study. As a result, we might be under-reporting the true mortality of these injuries.
Furthermore, in hospital mortality was a primary endpoint of interest and the mortality beyond this (i.e., 30-day mortality or mortality at 1-year) cannot be extrapolated from our data. Thus any improvements or setbacks in mortality following admission remain unknown. Comorbidity data for each cohort was not compared between the two cohorts and could certainly influence the results of this study as well; however, there is no indication to suggest that population health has drastically changed over the study period. The primary concern for mortality as it relates to pelvic ring injuries comes in the form of hemorrhage. However, we did not delineate the exact cause of death, and other variables such as head or solid organ injury play a critical, and often more important, role in mortality. Lack of specific causes of death does present limitations regarding the exact role hemorrhage plays in this outcome. Finally, our study reflects the experience at a single institution and the results may not be generalizable given that protocols and the adoption of new technology and treatments may vary between hospitals.
The findings of this study are strengthened by a large cohort of patients investigated and the use of a comparison group from the same trauma center. This remains the third such investigation at a single trauma center providing some consistency to the patient population and potentially providing a level of stability to the unmeasurable variables. This investigation highlights the importance of a multidisciplinary approach to treating patients with pelvic ring injuries, and also emphasizes how patient management changes outside the realm of orthopaedic surgery undoubtably has a large impact on our patients.
CONCLUSION
This study demonstrates a significant improvement in the mortality rate of pelvic ring injuries in recent years (4.8% versus 9.1%). This improvement does coincide chronologically with changes in trauma resuscitation and the implementation of adjuvant treatments for managing patients with severe hemorrhagic shock. Although the exact benefit of each treatment awaits further research, this data is certainly encouraging and might indicate improvement in care for these difficult patients.
Footnotes
Conflict of Interest and Source of Funding:
R. V. O’Toole is a paid consultant for Lincotek and Smith & Nephew, receives stock options from Imagen, and receives royalties from Lincotek, all unrelated to this work. The remaining authors have no conflicts of interest to disclose. No external funding was received for this work.
REFERENCES
- 1.Court-Brown CM, Caesar B Epidemiology of adult fractures: a review. Injury. 2006;37:691–697. [DOI] [PubMed] [Google Scholar]
- 2.Chen HT, Wang YC, Hsieh CC, et al. Trends and predictors of mortality in unstable pelvic ring fracture: a 10-year experience with a multidisciplinary institutional protocol. World J Emerg Surg. 2019;14:61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Magee GA, Fox CJ, Moore EE Resuscitative endovascular balloon occlusion of the aorta in pelvic ring fractures: the Denver health protocol. Injury. 2020. Jan 31; pii: S0020-1383(20)30072-3. [Online ahead of print] [DOI] [PubMed] [Google Scholar]
- 4.Manson T, OʼToole RV, Whitney A, et al. Young-Burgess Classification of pelvic ring fractures: Does it predict mortality, transfusion requirements, and non-orthopaedic injuries? J Orthop Trauma. 2010;24:603–609. [DOI] [PubMed] [Google Scholar]
- 5.Bakhshayesh P, Weidenhielm L, Enocson A Factors affecting mortality and reoperations in high-energy pelvic fractures. Eur J Orthop Surg Traumatol. 2018;28:1273–1282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Holstein JH, Culemann U, Pohlemann T Working group mortality in pelvic fracture patients. What are predictors of mortality in patients with pelvic fractures? Clin Orthop Relat Res. 2012;470:2090–2097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Giannoudis PV, Grotz MRW, Tzioupis C, et al. Prevalence of pelvic fractures, associated injuries, and mortality: the United Kingdom perspective. J Trauma. 2007;63:875–883. [DOI] [PubMed] [Google Scholar]
- 8.Demetriades D, Karaiskakis M, Toutouzas K, et al. Pelvic fractures: epidemiology and predictors of associated abdominal injuries and outcomes. J Am Coll Surgeons. 2002;195:1–10. [DOI] [PubMed] [Google Scholar]
- 9.Khanna P, Phan H, Hardy AH, et al. Multidisciplinary management of blunt pelvic trauma. Semin Intervent Rad. 2012;29:187–191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Burgess AR, Eastridge BJ, Young JW, et al. Pelvic ring disruptions: effective classification system and treatment protocols. J Trauma. 1990;30:848–856. [PubMed] [Google Scholar]
- 11.McGreevy DT, Abu-Zidan FM, Sadeghi M, et al. Feasibility and clinical outcome of reboa in patients with impending traumatic cardiac arrest. Shock. 2019: Dec 16. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 12.Borger van der Burg BLS, van Dongen TTCF, Morrison JJ, et al. A systematic review and meta-analysis of the use of resuscitative endovascular balloon occlusion of the aorta in the management of major exsanguination. Eur J Trauma Emerg Surg. 2018;44:535–550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Pieper A, Thony F, Brun J, et al. Resuscitative endovascular balloon occlusion of the aorta for pelvic blunt trauma and life-threatening hemorrhage: a 20-year experience in a level I trauma center. J Trauma Acute Care. 2018;84:449–453. [DOI] [PubMed] [Google Scholar]
- 14.Harris T, Davenport R, Mak M, et al. The evolving science of trauma resuscitation. Emerg Med Clin N Am. 2018;36:85–106. [DOI] [PubMed] [Google Scholar]
- 15.Napolitano LM Resuscitative Endovascular balloon occlusion of the aorta. Crit Care Clin. 2017;33:55–70. [DOI] [PubMed] [Google Scholar]
- 16.Holcomb JB, Tilley BC, Baraniuk S, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313:471–482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Morrison JJ, Ross JD, Rasmussen TE, et al. Resuscitative endovascular balloon occlusion of the aorta: a gap analysis of severely injured UK combat casualties. Shock. 2014;41:388–393. [DOI] [PubMed] [Google Scholar]
- 18.Brenner ML, Moore LJ, DuBose JJ, et al. A clinical series of resuscitative endovascular balloon occlusion of the aorta for hemorrhage control and resuscitation. J Trauma Acute Care. 2013;75:506–511. [DOI] [PubMed] [Google Scholar]
- 19.Roberts I, Shakur H, Coats T, et al. The crash-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Heal Technol Assess. 2013;17:1–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dalal SA, Burgess AR, Siegel JH, et al. Pelvic fracture in multiple trauma: classification by mechanism is key to pattern of organ injury, resuscitative requirements, and outcome. J Trauma. 1989;29:981–1000; discussion 1000-2. [PubMed] [Google Scholar]
- 21.Rommens PM, Hessmann MH Staged reconstruction of pelvic ring disruption: differences in morbidity, mortality, radiologic results, and functional outcomes between b1, b2/b3, and c-type lesions. J Orthop Trauma. 2002;16:92–98. [DOI] [PubMed] [Google Scholar]
- 22.Starr AJ, Griffin DR, Reinert CM, et al. Pelvic ring disruptions: prediction of associated injuries, transfusion requirement, pelvic arteriography, complications, and mortality. J Orthop Trauma. 2002;16:553–561. [DOI] [PubMed] [Google Scholar]
- 23.O’Sullivan REM, White TO, et al. Major pelvic fractures: identification of patients at high risk. J Bone Jt Surg Br. 2005;87:530–533. [DOI] [PubMed] [Google Scholar]
- 24.Holcomb JB, Jenkins D, Rhee P, et al. Damage control resuscitation directly addressing the early coagulopathy of trauma. J Trauma. 2007;62:307–310. [DOI] [PubMed] [Google Scholar]
- 25.Holcomb JB, Wade CE, Michalek JE, et al. Increased plasma and platelet to red blood cell ratios improves outcome in 466 massively transfused civilian trauma patients. Ann Surg. 2008;248:447–458. [DOI] [PubMed] [Google Scholar]
- 26.Malone DL, Hess JR, Fingerhut A Massive transfusion practices around the globe and a suggestion for a common massive transfusion protocol. J Trauma. 2006;60(6 Suppl):S91–S96. [DOI] [PubMed] [Google Scholar]
- 27.Ho AM, Karmakar MK, Dion PW Are we giving enough coagulation factors during major trauma resuscitation? Am J Surg. 2005;190:479–484. [DOI] [PubMed] [Google Scholar]
- 28.Gunter OL, Au BK, Isbell JM, et al. Optimizing outcomes in damage control resuscitation: identifying blood product ratios associated with improved survival. J Trauma. 2008;65:527–534. [DOI] [PubMed] [Google Scholar]
- 29.Cantle PM, Cotton BA Balanced resuscitation in trauma management. Surg Clin North Am. 2017;97:999–1014. [DOI] [PubMed] [Google Scholar]
- 30.CRASH-2 collaborators, Roberts I, Shakur H, et al. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the crash-2 randomised controlled trial. Lancet. 2011;377:1096–1101.e2. [DOI] [PubMed] [Google Scholar]
- 31.CRASH-2 trial collaborators, Shakur H, Roberts I, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (crash-2): a randomised, placebo-controlled trial. Lancet. 2010;376:23–32. [DOI] [PubMed] [Google Scholar]
- 32.Biffl WL, Smith WR, Moore EE, et al. Evolution of a multidisciplinary clinical pathway for the management of unstable patients with pelvic fractures. Ann Surg. 2001;233:843–850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Burlew CC, Moore EE, Smith WR, et al. Preperitoneal pelvic packing/external fixation with secondary angioembolization: optimal care for life-threatening hemorrhage from unstable pelvic fractures. J Am Coll Surg. 2011;212:628–635; discussion 635-637. [DOI] [PubMed] [Google Scholar]
- 34.Moreno C, Moore EE, Rosenberger A, et al. Hemorrhage associated with major pelvic fracture: a multispecialty challenge. J Trauma. 1986;26:987–994. [DOI] [PubMed] [Google Scholar]
- 35.Osborn PM, Smith WR, Moore EE, et al. Direct retroperitoneal pelvic packing versus pelvic angiography: a comparison of two management protocols for haemodynamically unstable pelvic fractures. Injury. 2009;40:54–60. [DOI] [PubMed] [Google Scholar]
- 36.Suzuki T, Smith WR, Moore EE Pelvic packing or angiography: competitive or complementary? Injury. 2009;40:343–353. [DOI] [PubMed] [Google Scholar]
- 37.Thorson CM, Ryan ML, Otero CA, et al. Operating room or angiography suite for hemodynamically unstable pelvic fractures? J Trauma Acute Care Surg. 2012;72:364–372. [DOI] [PubMed] [Google Scholar]
- 38.Stein DM, O’Toole R, Scalea TM Multidisciplinary approach for patients with pelvic fractures and hemodynamic instability. Scand J Surg. 2007;96:272–280. [DOI] [PubMed] [Google Scholar]
- 39.Tesoriero RB, Bruns BR, Narayan M, et al. Angiographic embolization for hemorrhage following pelvic fracture: Is it “time” for a paradigm shift? J Trauma Acute Care. 2017;82:18–26. [DOI] [PubMed] [Google Scholar]
- 40.White CE, Hsu JR, Holcomb JB Haemodynamically unstable pelvic fractures. Injury. 2009;40:1023–1030. [DOI] [PubMed] [Google Scholar]
- 41.Velmahos GC, Toutouzas KG, Vassiliu P, et al. A prospective study on the safety and efficacy of angiographic embolization for pelvic and visceral injuries. J Trauma. 2002;53:303–308. [DOI] [PubMed] [Google Scholar]
- 42.Tanizaki S, Maeda S, Matano H, et al. Time to pelvic embolization for hemodynamically unstable pelvic fractures may affect the survival for delays up to 60 min. Injury. 2014;45:738–741. [DOI] [PubMed] [Google Scholar]
- 43.Balogh Z, Caldwell E, Heetveld M, et al. Institutional practice guidelines on management of pelvic fracture-related hemodynamic instability: Do they make a difference? J Trauma. 2005;58:778–782. [DOI] [PubMed] [Google Scholar]
- 44.Agolini SF, Shah K, Jaffe J, et al. Arterial embolization is a rapid and effective technique for controlling pelvic fracture hemorrhage. J Trauma. 1997;43:395–399. [DOI] [PubMed] [Google Scholar]
- 45.Copp J, Eastman JG Novel resuscitation strategies in patients with a pelvic fracture. Injury. 2020. Jan 30. pii: S0020-1383(20)30070-X. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 46.Sepehri A, Sciadini MF, Nascone JW, et al. Initial experience with the t-clamp for temporary fixation of mechanically and hemodynamically unstable pelvic ring injuries. Injury. 2020;51:699–704. [DOI] [PubMed] [Google Scholar]
- 47.Hagedorn JC, Bardes JM, Paris CL, et al. Thromboelastography for the orthopaedic surgeon. J Am Acad Orthop Surg. 2019;27:503–508. [DOI] [PubMed] [Google Scholar]
- 48.Sathy AK, Starr AJ, Smith WR, et al. The effect of pelvic fracture on mortality after trauma: an analysis of 63,000 trauma patients. J Bone Joint Surg Am. 2009;91:2803–2810. [DOI] [PubMed] [Google Scholar]
- 49.Chong KH, DeCoster T, Osler T, et al. Pelvic fractures and mortality. Iowa Orthop J. 1997;17:110–1114. [PMC free article] [PubMed] [Google Scholar]