

Abstract
Purpose:
Sentinel lymph node biopsy (SLNB) is omitted in older women (≥ 70 years old) with clinical lymph node (LN)-negative hormone receptor-positive breast cancer as it does not influence adjuvant treatment decision-making. However, older women are heterogenous in frailty while the chance of recurrence increase with improving longevity. Therefore, a biomarker that identifies LN metastasis may facilitate treatment decision-making. RUFY3 is associated with cancer progression. We evaluated RUFY3 expression level as a biomarker for LN-positive breast cancer in older women.
Methods:
Clinical and transcriptomic data of breast cancer patients were obtained from the Molecular Taxonomy of Breast Cancer International Consortium (METABRIC, n=1,903) and The Cancer Genome Atlas (TCGA, n=1,046) Pan-Cancer study cohorts.
Results:
A total of 510 (METABRIC) and 211 (TCGA) older women were identified. LN-positive breast cancer, which represented 51.4% (METABRIC) and 48.4% (TCGA), demonstrated worse disease-free, disease-specific, and overall survival. RUFY3 levels were significantly lower in LN-positive tumors regardless of age. The area under the curve for the receiver operator characteristic (AUC-ROC) curves showed RUFY3 predicted LN metastasis. Low RUFY3 enriched oxidative phosphorylation, DNA repair, MYC targets, unfolded protein response, and mtorc1 signaling gene sets, was associated with T helper type 1 cell infiltration, and with intratumor heterogeneity and fraction altered. Low RUFY3 expression was associated with LN-positive breast cancer and with worse disease specific survival amongst older women.
Conclusion:
Older women with breast cancers with low expression level of RUFY3 were more frequently diagnosed with LN-positive tumors, which translated into worse prognosis.
Keywords: RUFY3, geriatric oncology, lymph node, breast cancer
Introduction
Older women [(≥ 70 years old (yo)] account for 30% of all newly diagnosed breast cancer patients [1]. Older women generally have tumors with favorable features such as small size, clinically node negative, and hormone receptor (HR)-positive [2], which translate into a more than 98% ten-year breast cancer-specific survival [3]. Consequently, decision-making must be carefully planned out in older women. The patient’s breast cancer features should be weighed against other unique features in this age group, including competing comorbidities [4], increased vulnerability to cancer treatment toxicities [5], and treatment goals primarily focused on maximizing quality over quantity [6]. Several studies including the Cancer and Leukemia Group B (CALGB) 9343 trial and PRIME II have shown that in older women (≥70yo) with HR receptor-positive T1 (≤2 cm) breast cancer, disease-free survival (DFS) is not compromised by omitting surgical staging of the axilla, but only if the patient receives adjuvant endocrine therapy [7–10]. Both the Society for Surgical Oncology (SSO) [11] and the American Society for Breast Surgeons (ASBrS) [12] added measures to the Choosing Wisely campaign of the American Board of Internal Medicine Foundation (ABIM) [13] recommending against routine sentinel lymph node biopsy (SLNB) in older women (≥70yo) with early-stage HR-positive HER2-negative invasive breast cancer. More recent studies have confirmed the selective use of SLNB in older women with invasive breast cancer [14–17].
Efforts to minimize the use of lymph node (LN) surgery in older women with breast cancer could have substantial value through eliminating the risk of lymphedema, pain, and nerve damage [18]. The data on small clinically LN negative HR-negative breast cancers cannot be extrapolated to those with larger tumors and to those with HR-negative cancers and HER2-positive cancers. Furthermore, all HER2-positive cancers should receive systemic therapy, with limited exceptions. Given that the purpose of LN surgery is primarily to provide prognostic information to guide adjuvant therapy, alternative means of predicting LN involvement could be valuable. Tumor genomic profiling with the 21-gene RT-PCR assay OncotypeDx® provides reliable prognostic information and prediction of chemotherapy effect in women with ER-positive/HER2-negative cancer with both negative nodes and 1–3 positive nodes [19–21]. For larger HR-positive tumors as well as HER2-positive tumors, there is real potential value of a means to predict LN involvement without axillary surgery.
Nomograms to predict LN-positive tumors have been proposed [22–28]. While these tools have a wide range of age groups, they have a particularly small sample of older women. For example, using data from 36,441 older women with HR-positive breast cancer, the Mayo Clinic group developed a clinical predictive model to identify older women at low risk of LN-positive breast cancer with goal of identifying those who most warrant omission of SLNB [22]. There are not data on the use of these algorithms to impact use of LN surgery or on outcome.
Developing a robust diagnostic marker that predicts LN metastasis for older women with clinically LN-negative invasive breast cancer is necessary. This information could help establish the need for adjuvant systemic treatment while avoiding the morbidity of surgically staging the axilla. Several biomarkers have been identified as predictors of LN status, nevertheless, limitations are always inevitable [29]. An in silico translational approach allows measuring intratumor biomarkers when comprehensive gene expression profile is available. We hypothesize that there may be an intratumor biomarker that predicts LN-positive breast cancer in older women.
RUFY3 (RUN and FYVE domain containing 3), also known as Rap2 interacting protein X (RIPX) or single axon-related1 (Singar1), is a 469-amino-acid protein. Although RUFY3 is classically known for its role in neuronal development [30,31], recent studies have evaluated its pathophysiologic role in cancer. This has been supported by data showing its involvement in cell migration [32], actin cytoskeleton dynamics [33], lipid modification [34], membrane trafficking [35], and cell signaling [36,37]. Several studies have confirmed RUFY3 is also involved in cancer cell regulation and cellular proliferation [38–42]. These studies showed that tumors with high RUFY3 levels are associated with more advanced disease and have worse overall survival (OS) compared to patients with normal RUFY3 levels. To date, there is no data on the role of RUFY3 in breast cancer. This study aims to evaluate RUFY3 intratumor expression levels as a predictive biomarker for LN metastasis in older women (≥70yo) with invasive breast cancer.
Methods
Clinical and gene expression data of breast cancer cohorts
Institutional review board (IRB) approval at Roswell Park Comprehensive Cancer Center (Buffalo, NY, United States) was waived as publicly available deidentified databases were used. The publicly available cBioPortal [43] was accessed to obtain clinical and transcriptome data from breast cancer patient in The Cancer Genome Atlas (TCGA) Pan-Cancer study (n=1,046) [44] and the Molecular Taxonomy of Breast Cancer International Consortium (METABRIC) [45] study (n=1,903). Data of adult females with invasive breast cancer was obtained, including age and LN metastasis status. Race/ethnicity data was not available from either cohort database. The average value was used for the genes with multiple probes. Older women were defined as women ≥70yo as proposed by the Breast International Group [46].
Gene Set Enrichment Analysis (GSEA)
Gene set enrichment analysis (GSEA) [47] with hallmark gene sets of the Molecular Signatures Database was performed to explore the signaling pathways related to high and low RUFY3 expression in breast cancer with a similar approach we previously reported [48–60]. Each cohort was divided into high and low groups by the median expression levels of RUFY3 gene. GSEA is a publicly available software that allows determines whether an a priori defined set of genes shows statistically significant, concordant differences between two biological states (Broad Institute, http://software.broadinstitute.org/gsea/index.jsp). A false discovery rate (FDR) of <0.25 was considered statistically significant as recommended by the developer of GSEA.
Cytolytic activity score (CYT)
CYT was defined as the sum of expression of granzyme A (GZMA) and perforin (PRF1) as previously described [60–62]. CYT was used to evaluate overall anti-cancer immune cell killing in the tumor microenvironment. The threshold of dichotomization of the CYT-high and low groups was determined by the median of the CYT.
Immune Cell Fraction Estimation
The level of tumor infiltrating immune cells was estimated using the xCell algorithm [63] in a similar fashion we previously reported [48–51, 52 54, 64–68]. xCell algorithm was used to examine whole-tumor transcriptome to score the relative abundance of 64 types of immune and stromal cells across tumors, as previously described [69–72]. The xCell score for each sample was calculated using R software (version 4.0.1, R Project for Statistical Computing), as previously reported [58, 73–75].
Statistical Analysis
Statistical analyses were performed using R software. Groups were compared using Mann-Whitney U test. Receiver operating characteristic (ROC) curve with area under the curve (AUC) value was used to evaluate accuracy. Survival was plotted by the Kaplan-Meier method and compared using log-rank test. Statistical significance was set at a p < 0.05.
Results
Cohort tumor characteristics
Table 1 summarizes the tumor characteristics of older women in the METABRIC and TCGA cohorts. Of 1,903 women in the METABRIC cohort, 510 were older women, of which 51.4% were LN-positive. Of 1,046 women in the TCGA cohort, 211 were older women, of whom 48.8% were LN-positive. In the METABRIC cohort, patients with LN-positive breast cancer had significantly higher rates of high-grade tumors compared to LN-negative tumors (43.5% versus 37.1%, p=0.04). The TCGA cohort confirmed that patients with LN-positive breast cancer had significantly higher rates of advanced stage tumors compared to LN-negative tumors (55.3% versus 0.9%, p<0.001). LN involvement was not statistically different according to molecular subtype in neither the METABRIC (p=0.2) nor TCGA cohorts (p=0.1).
Table 1.
Tumor characteristics of older women breast cancer patients in the METABRIC and TCGA cohorts
| Variable | LN-negative | LN-positive | p-value |
|---|---|---|---|
| METABRIC (n = 510) | n = 248 | n = 262 | |
| Molecular subtype | |||
| ER+/HER2− | 202 (81.4) | 225 (85.9) | |
| TNBC | 26 (10.5) | 17 (6.5) | 0.2 |
| HER2+ | 20 (8.1) | 19 (7.2) | |
| Unknown | 0 (0) | 1 (0.4) | |
| Nottingham Grade | |||
| 1 | 29 (11.7) | 15 (5.7) | |
| 2 | 117 (47.2) | 120 (45.8) | 0.04 |
| 3 | 92 (37.1) | 114 (43.5) | |
| Unknown | 10 (4.0) | 13 (5.0) | |
| AJCC stage | |||
| 0 | 1 (0.4) | 0 (0) | |
| I | 73 (29.4) | 0 (0) | <0.001 |
| II | 81 (32.7) | 155 (59.2) | |
| III | 4 (1.6) | 27 (10.3) | |
| IV | 2 (0.8) | 1 (0.4) | |
| Unknown | 87 (35.1) | 79 (30.1) | |
| TCGA (n = 211) | n = 108 | n = 103 | |
| Molecular subtype | |||
| ER+/HER2− | 68 (62.9) | 56 (54.4) | |
| TNBC | 14 (12.9) | 7 (6.8) | 0.1 |
| HER2+ | 16 (14.8) | 23 (22.3) | |
| Unknown | 10 (9.3) | 17 (16.5)) | |
| T category | |||
| T1 | 39 (36.1) | 18 (17.5) | |
| T2 | 57 (52.8) | 52 (50.5) | <0.001 |
| T3 | 11 (10.2) | 22 (21.3) | |
| T4 | 1 (0.9) | 11 (10.7) | |
| Unknown | 0 (0) | 0 (0) | |
| AJCC stage | |||
| I | 39 (36.1) | 0 (0) | |
| II | 68 (62.9) | 40 (38.8) | <0.001 |
| III | 1 (0.9) | 57 (55.3) | |
| IV | 0 (0) | 2 (1.9) | |
| Unknown | 0 (0) | 4 (3.9) |
Abbreviation: AJCC, American Joint Committee on Cancer; ER, estrogen receptor; HER2, human epidermal growth factor 2; LN, lymph node; METABRIC, Molecular Taxonomy of Breast Cancer International Consortium; TCGA, the Cancer Genome Atlas; TNBC: triple negative breast cancer
Older women with LN-positive breast cancer are significantly associated with worse survival.
To assess whether LN involvement affected oncologic outcomes, both the METABRIC (n = 1,903) and TCGA (n = 1,046) cohorts were queried. Figure 1 compares the DFS, disease-specific survival (DSS), and OS according to LN status in the whole cohort (Fig. 1a) and older women (Fig. 1b). Patients with LN-positive breast cancer had significantly lower DFS, DSS, and OS compared to patients with LN-negative breast cancer (Fig. 1A). LN-positive breast cancer had significantly lower DFS, DSS, and OS compared to LN-negative breast cancer among older women (Fig. 1B).
FIG 1. Oncologic survival outcomes of patients in the Molecular Taxonomy of Breast Cancer International Consortium (METABRIC) and the Cancer Genome Atlas (TCGA) cohorts by axillary lymph node (LN) status involvement.
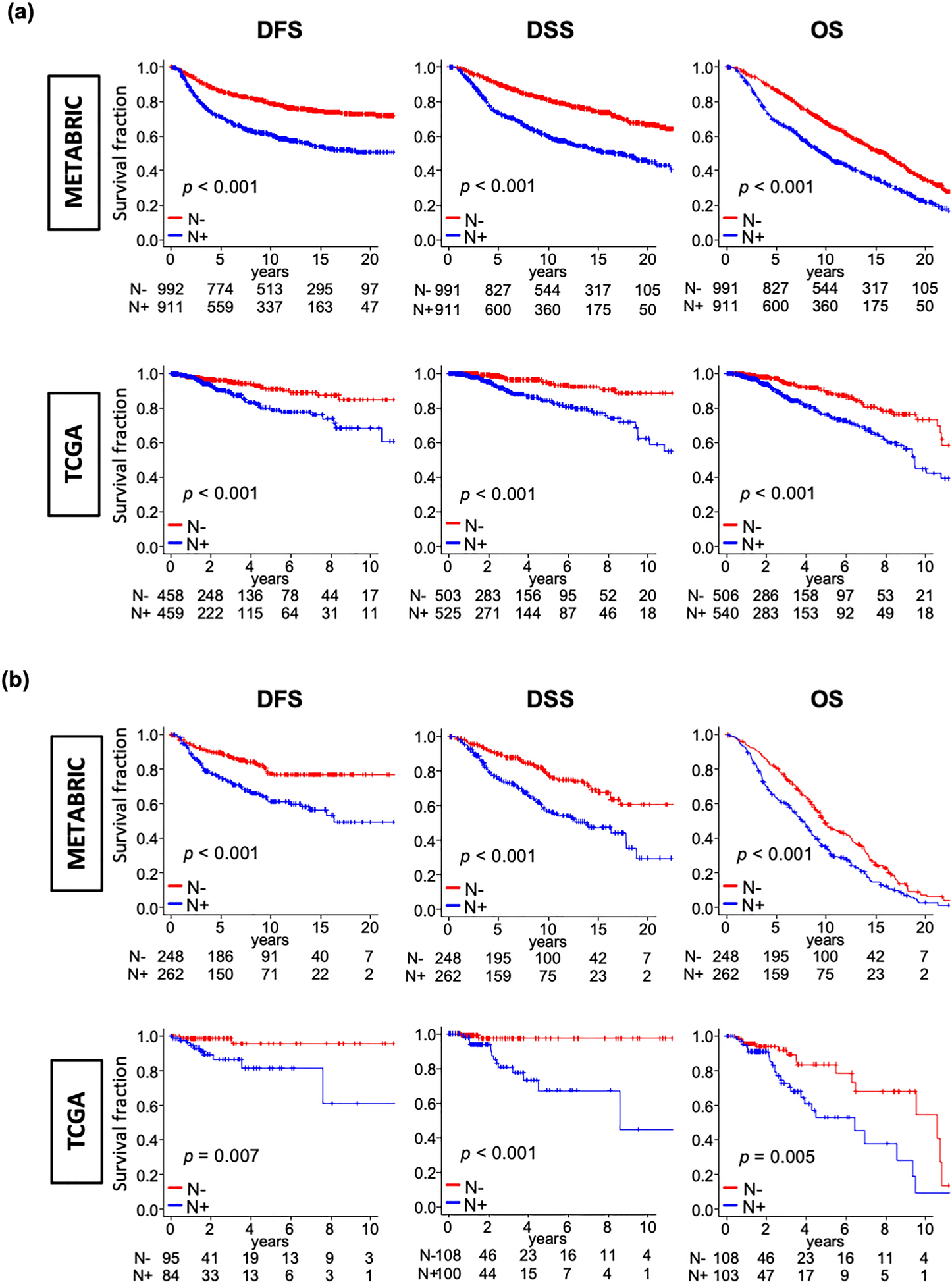
Kaplan-Meier disease-free survival (DFS), disease-specific survival (DSS), and overall survival (OS) curves of the whole cohort (A) and older women (≥70 years old) in the METABRIC and TCGA cohorts. Comparison between LN-positive (blue line) and LN-negative (red line) patients was performed using log-rank test. The bottom one-third was used as cut-off value to divide two groups within cohorts.
RUFY3 expression levels are predictive of LN involvement in older women with breast cancer.
To test whether RUFY3 predicts LN involvement, RUFY3 expression levels were measured in women with breast cancer and compared according to LN involvement (Fig. 2). RUFY3 expression levels were significantly lower amongst women with LN-positive breast cancer in the METABRIC cohort (all age, p = 0.002 and older women p < 0.001). However, there was no significant difference in the TCGA cohort for either women of all ages (p = 0.7) or older women (p = 0.1) (Fig. 2A). Receiver operator characteristic (ROC) curves showing the predictive sensitivity and specificity of RUFY3 are shown in Figure 2B. The area under the curve (AUC) for the ROC curves showed RUFY3 predicted LN involvement (METABRIC cohort: all ages AUC = 0.542 and older AUC = 0.627; TCGA cohort all ages AUC = 0.504 and older AUC = 0.577).
FIG 2. RUFY3 is associated with lymph node metastasis in patients with breast cancer.
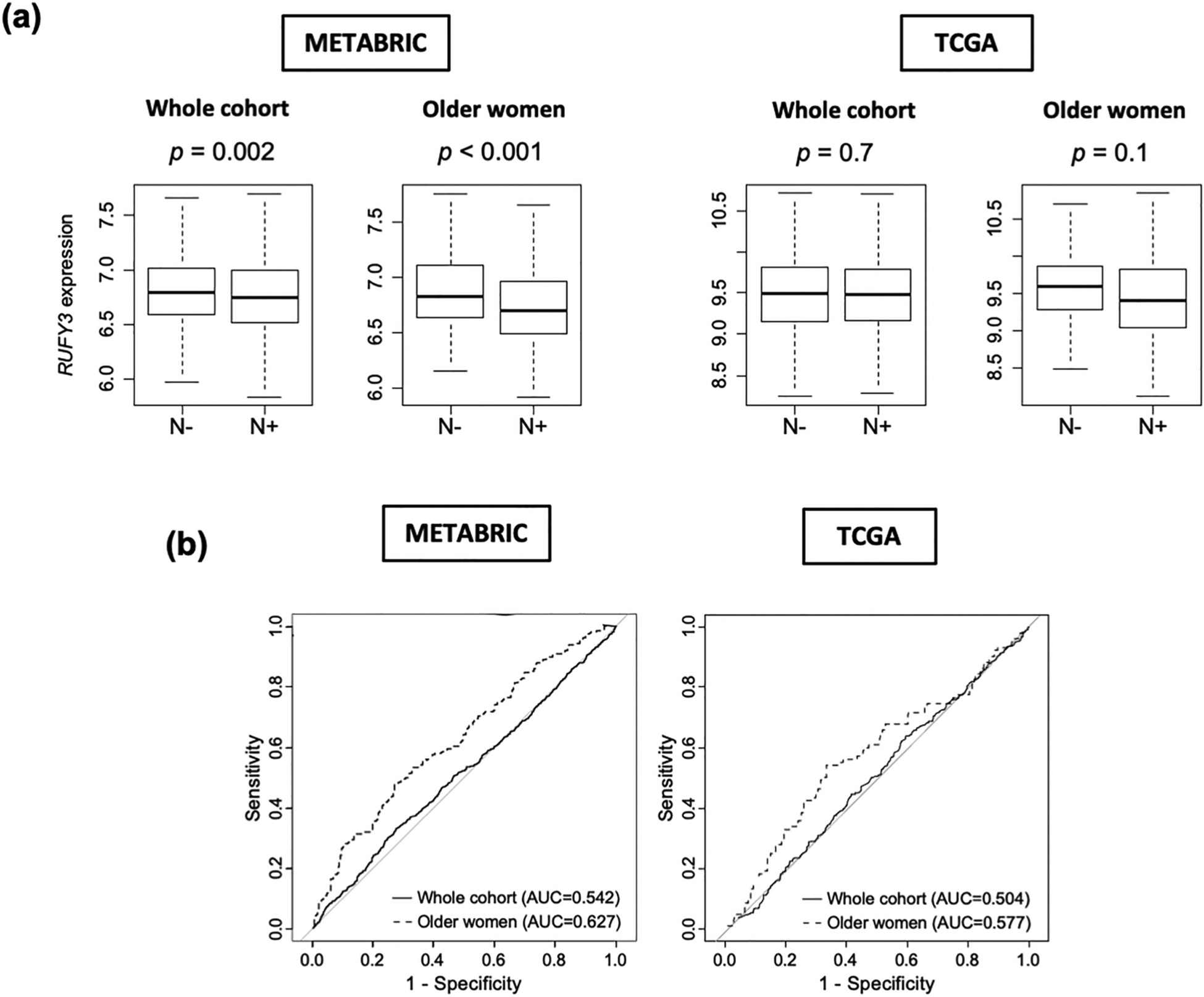
(a) Box plots depicting RUFY3 expression stratified lymph node involvement in the Molecular Taxonomy of Breast Cancer International Consortium (METABRIC) and the Cancer Genome Atlas (TCGA) cohorts. P-values were calculated by Mann-Whitney U test. (b) Receiver operator characteristic (ROC) curve showing the sensitivity and specificity of RUFY3 amongst older women and all age women. Abbreviations: N−, lymph node-negative; N+, lymph node-positive.
RUFY3 expression level is not associated with pathological grade and molecular subtypes.
Table 2 summarizes tumor characteristics of older women with breast cancer according to RUFY3 expression levels. In both the METABRIC and TCGA cohorts, patients with low and high expression of RUFY3 had similar age at diagnosis (METABRIC: 75yo versus 76yo, p = 0.7; TCGA: 75yo versus 77yo, p = 0.07) and distribution of molecular subtypes (METABRIC p = 0.9; TCGA p = 0.1). The METABRIC confirmed RUFY3 expression level was not associated with pathologic grade (p = 0.6).
Table 2.
Characteristics of older women with breast cancer according to RUFY3 expression levels in the METABRIC and TCGA cohorts
| Variable | RUFY3 low | RUFY3 high | p-value |
|---|---|---|---|
| METABRIC (n = 510) | n = 168 | n = 342 | |
| Age (yo), median (IQR) | 75 (73–80) | 76 (73–79) | 0.7 |
| Molecular subtype | |||
| ER+/HER2− | 141 (83.9) | 286 (83.6) | |
| TNBC | 12 (7.1) | 27 (7.9) | 0.9 |
| HER2+ | 14 (8.3) | 29 (8.5) | |
| Unknown | 1 (0.6) | 0 (0) | |
| Nottingham Grade | |||
| 1 | 12 (7.1) | 32 (9.3) | |
| 2 | 79 (47.0) | 158 (46.1) | 0.6 |
| 3 | 72 (42.8) | 134 (39.1) | |
| Unknown | 5 (2.9) | 18 (5.2) | |
| AJCC stage | |||
| 0 | 0 (0) | 1 (0.3) | |
| I | 1 (0.6) | 59 (17.2) | <0.001 |
| II | 8148.2 | 155 (45.3) | |
| III | 15 (8.9) | 16 (4.6) | |
| IV | 1 (0.6) | 2 (0.5) | |
| Unknown | 57 (33.9) | 109 (31.9) | |
| TCGA (n = 211) | n = 70 | n = 141 | |
| Age (yo), median (IQR) | 75 (72–79) | 77 (73–80) | 0.07 |
| Molecular subtype | |||
| ER+/HER2- | 36 (51.4) | 88 (62.4) | |
| TNBC | 10 (14.2) | 11 (7.8) | 0.1 |
| HER2+ | 16 (22.8) | 23 (16.3) | |
| Unknown | 8 (11.4) | 19 (13.4) | |
| T category | |||
| T1 | 12 (17.1) | 45 (31.9) | |
| T2 | 44 (62.8) | 65 (46.1) | 0.06 |
| T3 | 9 (12.8) | 24 (17.0) | |
| T4 | 5 (7.1) | 7 (4.9) | |
| Unknown | 0 (0) | 0 (0) | |
| AJCC stage | |||
| I | 7 (10.0) | 32 (22.7) | |
| II | 36 (51.4) | 72 (61.0) | 0.03 |
| III | 26 (37.1) | 32 (22.7) | |
| IV | 1 (1.4) | 1 (0.7) | |
| Unknown | 0 (0) | 4 (2.8) |
Abbreviation: AJCC, American Joint Committee on Cancer; ER, estrogen receptor; HER2, human epidermal growth factor 2; IQR, interquartile range; LN, lymph node; METABRIC, Molecular Taxonomy of Breast Cancer International Consortium; TCGA, the Cancer Genome Atlas; TNBC, triple negative breast cancer; yo, years old
Breast cancers with low expression of RUFY3 enriched oxidative phosphorylation, DNA repair, MYC targets v1, unfolded protein response, and mtorc1 signaling
GSEA was used to study the enrichment of hallmark gene sets according to RUFY3 expression level amongst older women with breast cancer in the METABRIC and TCGA cohorts (Fig. 3). Older women with tumors that had low expression of RUFY3 showed enrichment of oxidative phosphorylation, DNA repair, MYC targets v1, unfolded protein response, and mtorc1 signaling genes.
FIG 3. Gene Set Enrichment Analysis (GSEA) according to RUFY3 expression level in older women with breast cancer in the METABRIC and TCGA cohorts.
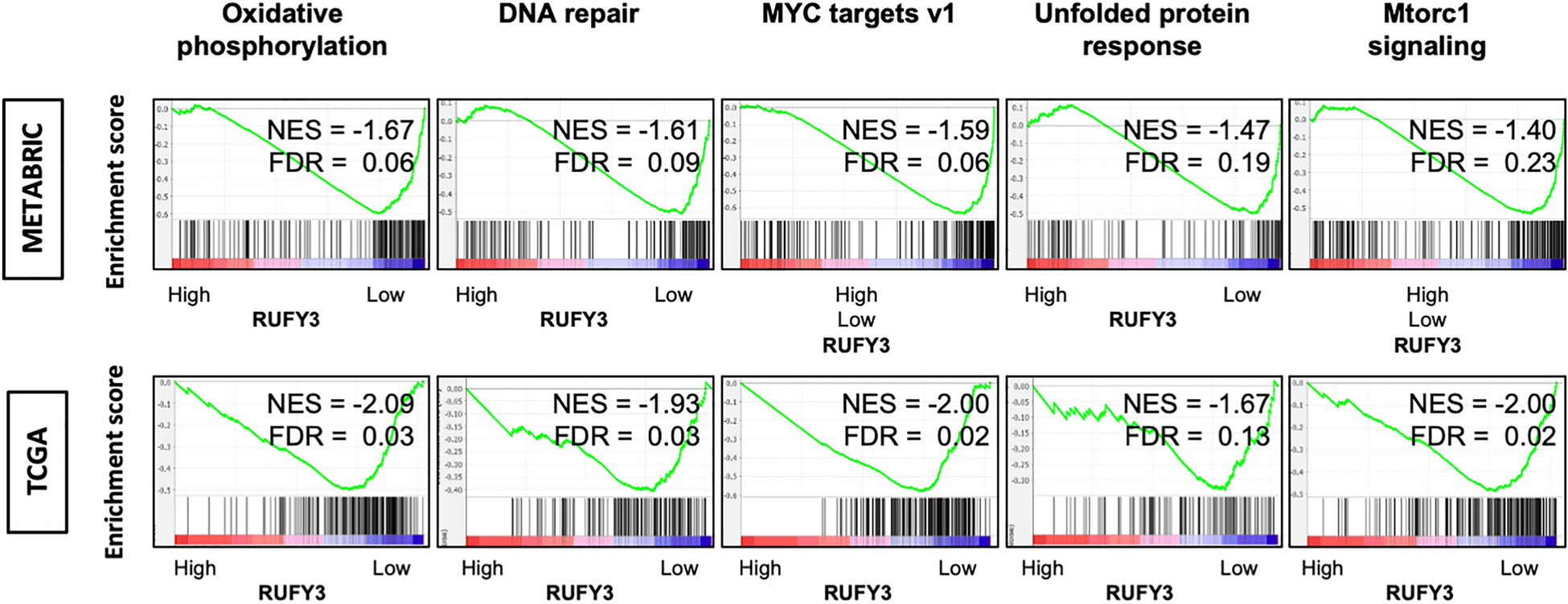
Enrichment plots with normalized enrichment score (NES) and false discovery rate (FDR) of hallmark gene sets which were significantly enriched in the low RUFY3 groups in both cohorts. Bottom one-third was used as cut-off value to divide two groups within cohorts.
Breast cancers with low expression of RUFY3 are associated with a high fraction of T helper type1 (Th1) and type2 (Th2) cells, Tregs, and M1 macrophages and high level of intratumor heterogeneity and fraction altered.
It has been described that oncogene c-Myc can induce DNA damage, increase reactive oxygen species, and genetic instability [76], which may lead to elevated mutation load and neoantigens that attracts immune cells. Given that breast cancers with low expression of RUFY3 enriched MYC targets, DNA repair and oxidative phosphorylation gene sets in the GSEA, it was of interest to assess whether there was immune cells infiltration in the tumor microenvironment. To evaluate this, level of tumor infiltrating immune cells was estimated using the xCell algorithm. Cohorts of primary breast cancer were used to analyze RUFY3 expression differences between immune (T cells, B cells and myeloid cells), tumor, and stromal cells (Fig. 4). Compared to breast cancers with high expression level of RUFY3, those with low expression level had a significantly higher fraction of Th1 cells (p = 0.04) and Th2 cells (p < 0.001), and low Tregs fractions (p = 0.01) in the METABRIC cohort (Fig. 4A). In the TCGA cohort, breast cancers with low expression of RUFY3 had high fraction of Th1 cells (p = 0.04) and M1 macrophages (p < 0.001) compared to tumors with high expression level of RUFY3 (Fig. 4A). CYT did not significantly vary depending on the RUFY3 expression level in either cohort (Fig. 4B). Breast cancers with low expression of RUFY3 had significantly higher levels of intratumor heterogeneity (p = 0.001) and fraction altered (p = 0.005) compared to tumors with high expression level of RUYF3 (Fig. 4C).
FIG 4. Association of RUFY3 expression level with immune fraction in the tumor microenvironment, immune activity, intratumor heterogeneity, and mutation load.
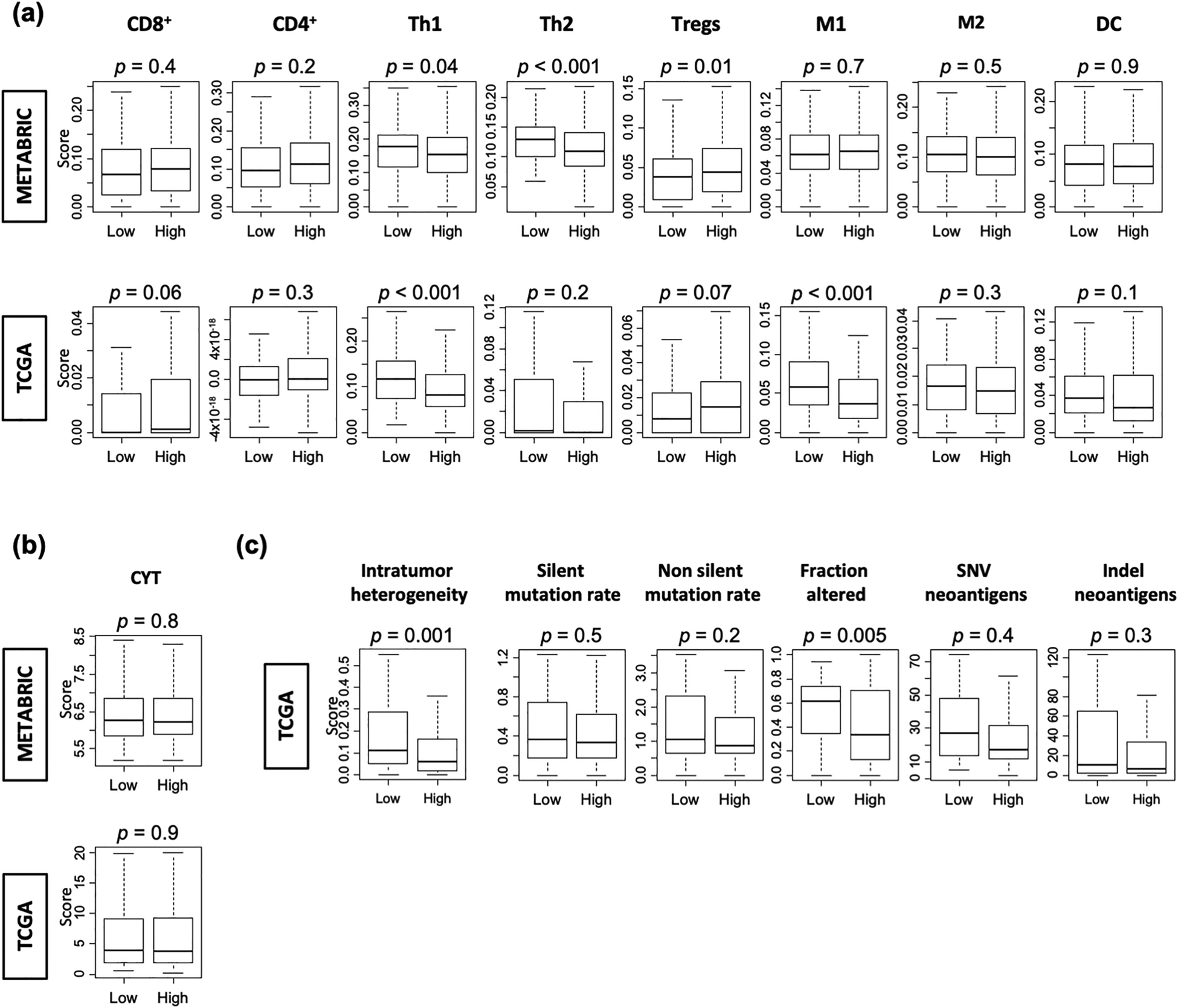
Boxplots of (a) the infiltrating fraction of immune cells [CD8+ T cells, CD4+ T cells, T helper type1 (Th1) and type2 (Th2) cells, regulatory, M1 and M2 macrophages, and dendritic cells (DC)]; (b) cytolytic activity score (CYT); and (c) intratumor heterogeneity and mutation-related score [silent and non-silent mutation rate, fraction altered, single nucleotide variant (SNV) and indel neoantigens] stratified by RUFY3 expression level in older women with breast cancer.
Breast cancers with low expression of RUFY3 are significantly associated with LN involvement and confer worse prognosis particularly in older women
To determine the clinical implication of RUFY3, LN involvement was measured by RUFY3 expression levels in the METABRIC and TCGA cohorts (Fig. 5). In both cohorts, older women with breast cancer that had low expression of RUFY3 had significantly higher rates of LN involvement, but not in the whole cohorts (Fig. 5A; METABRIC, whole cohort p = 0.002, older women p < 0.001; TCGA, whole cohort p = 0.9, older women p = 0.04, respectively). The association of RUFY3 expression levels with survival was assessed by plotting the DSS in the whole population and older women. As shown in Figure 5B, older women with breast cancers that had low expression of RUFY3 had significantly worse DSS (p = 0.03).
FIG 5. Association of RUFY3 expression level on LN involvement and patient survival.
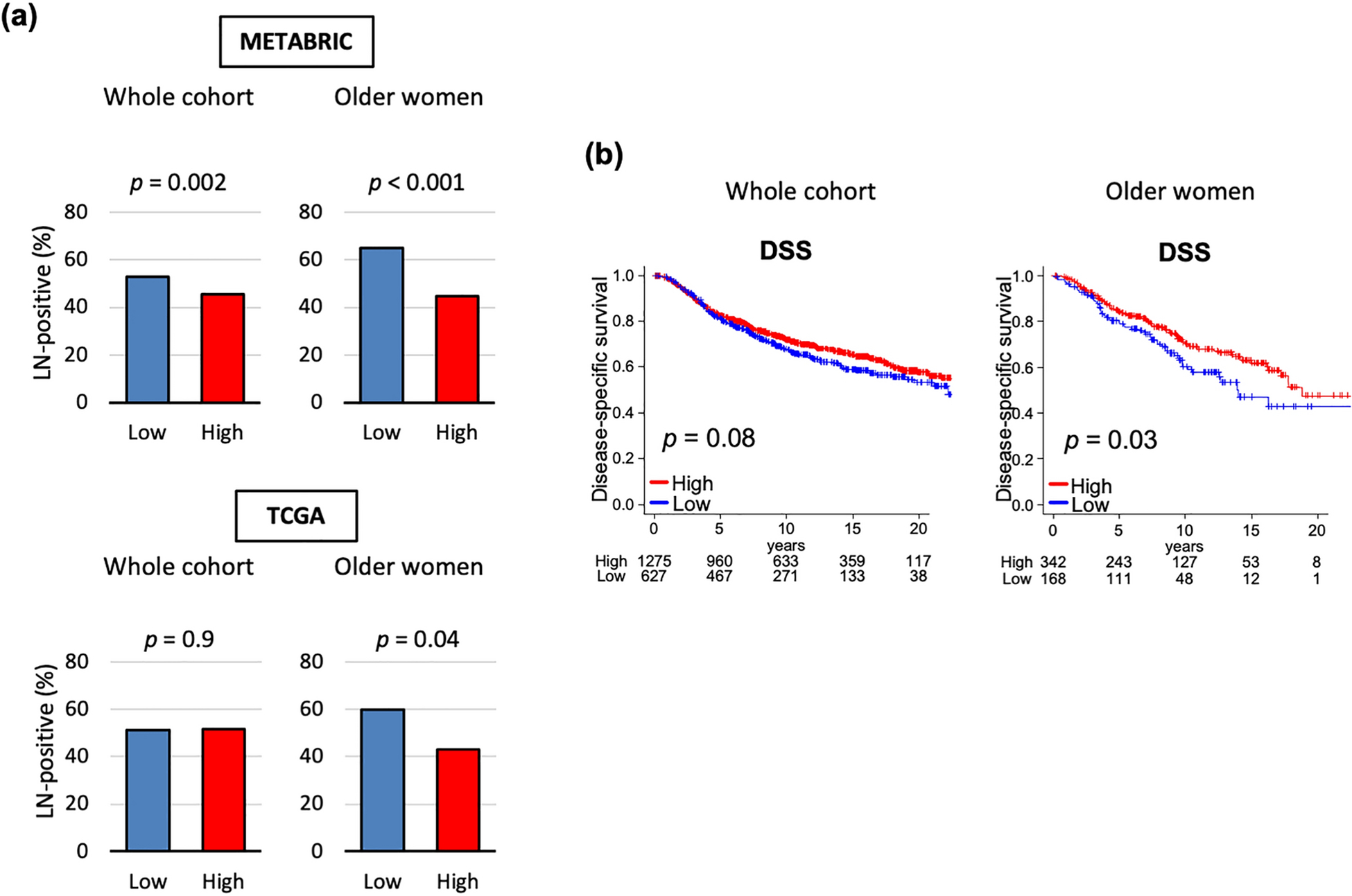
(a) Bar plots of lymph node metastasis rate by low and high RUFY3 level in whole age cohort and older women in the METABRIC and TCGA cohorts. (b) Kaplan-Meier curves of disease-specific survival in whole age and older women cohorts of the METABRIC cohort.
Discussion
Given the data reported by other studies on the role of RUFY3 in cancer [38–42], we assessed the clinical relevance of RUFY3 as a surrogate for lymph node metastasis with invasive breast cancer. Women with LN-positive breast cancer had significantly lower expression levels of RUFY3 compared to LN-negative patients. RUFY3 expression level was not affected by tumor pathological grade and molecular subtypes. Older women with low expression RUFY3 tumors enriched oxidative phosphorylation, DNA repair, MYC targets v1, unfolded protein response, and mtorc1 signaling gene sets. The same RUFY3 low tumors were associated with a high fraction of T helper type1 (Th1) and type2 (Th2) cells, Tregs, and M1 macrophages and high level of intratumor heterogeneity and fraction altered. Older women with breast cancers who had low expression level of RUFY3 were more frequently diagnosed with LN-positive tumors, which translated into worse prognosis. Altogether low expression level of RUFY3 may be associated with LN status in older women with breast cancer.
The role of RUFY3 family of proteins in cancer has been previously studied by other groups. Xie et al [38] reported that RUFY3 levels were elevated in human colorectal cancer. Patients with a high expression of RUFY3 had worse prognosis than those with a low expression. RUFY3 was shown to play an important role in cancer progression and metastasis in both in vitro and in vivo experiments. Wang et al [39] found that RUFY3 overexpression promoted gastric cancer cell migration and invasion. Men et al [40] reported that high RUFY3 expression was associated with LN metastasis and advanced cancer stage. In patients with LN-positive tumors, expression rate of RUFY3 (65.1%) was much higher than in those LN-negative tumors (43.5%). Although there was no statistically significant difference in the tumor size, there was a statistical difference in the expression of RUFY3 across different cancer stages (p < 0.01). The authors speculated that RUFY3 plays a role in LN metastasis rather than promoting tumor growth. Although the data presented in this current study supports that intratumor RUFY3 protein level is a marker of LN invasion as well as prognosis for breast cancer, these results differ in that low RUFY3 expression levels were associated with these findings. Therefore, the role of RUFY3 in breast cancer is not fully characterized with these data. In vitro and in vivo studies are necessary to understand the biological mechanism that explains these findings.
Data form other studies may be useful to hypothesize potential mechanisms behind the findings herein. In one study overexpression of RUFY3 increased colorectal cancer cell proliferation and promoted colony formation in soft agar in vitro, whereas knockdown of RUFY3 expression by siRNA inhibited colony formation in soft agar, migration, and invasion [41]. The authors concluded that RUFY3 upregulation may be an important mechanism underlying tumor development in colorectal cancer cells. In this same study the authors noted that RUFY3 interacted with FOXK1 in colorectal cancer cells [41]. These results indicated that cancer progression and metastasis were promoted by a key signaling pathway involving a RUFY3-FOXK1 axis. Another study suggested that RUFY3 plays an important role in Ras-like GTPase signaling pathways [37]. In one study RUFY3 overexpression led to the formation of F-actin-enriched protrusive structures at the cell periphery [39]. P21-activated kinase-1 (PAK1) interacts with RUFY3, resulting in RUFY3-induced gastric cancer cell migration [39]. Altogether these studies suggest that overexpression of RUFY3 promotes cancer cell progression, migration, and metastasis. Interestingly, our study shows a unique role for RUFY3 in breast cancer as low expression level is associated with more aggressive clinical features. Future in vitro and in vivo studies are necessary to study understand the how low expression levels of RUFY3 produce negative clinical results.
Several other studies have shown that RUFY3 is associated with poor prognosis [38,40,41]. In these studies, survival analyses showed that there was a negative association between RUFY3 expression and OS across different types of cancers. Interestingly, Men et al [40] showed through a single Cox regression that four clinical characteristics and RUFY3 expression influenced patient prognosis. However, after adjusting for tumor size, LN metastasis, and TNM staging, multiple Cox regression revealed that RUFY3 expression could be considered an independent factor for predicting survival in lung adenocarcinoma patients. On the other hand, RUFY3 expression was not significantly associated with OS whereas age, LN metastasis, and tumor size were, in multivariable Cox regression analysis of the METABRIC breast cancer cohort (data not shown). This is most likely because RUFY3 is a confounding factor of age and LN metastasis.
There are several limitations to this study. Although multiple large patient cohorts were used in this study to validate our findings, the data originated from retrospective studies from a publicly available source, which limit our access to clinical parameters. Furthermore, the cohorts represent a convenience sample of patients with tumors large enough to allow research tissue procurement who were treated at centers with robust tissue procurement programs. The cohorts’ raw data vary in terms of patient demographics and clinical features; therefore, pooled and individual data analyses were performed to assess for heterogeneity. The cohorts also lack relevant clinical information such as comorbidities, functional status, and treatment details. Additionally, data to explain the biological processes that support the findings in this study were not available given the bioinformatics approach.
Conclusion
This study reports a novel role for RUFY3 in breast cancer. Older women with breast cancers who had low expression level of RUFY3 were more frequently diagnosed with LN-positive tumors, which translated into worse prognosis. Low expression level of RUFY3 warrants further evaluation as an intratumor biomarker to predict LN metastasis in older women with invasive breast cancer.
Funding:
This work was supported by US National Institutes of Health/National Cancer Institute grant R01CA160688, R01CA250412, R37CA248018, US Department of Defense BCRP grant W81XWH-19-1-0674, as well as the Edward K. Duch Foundation and Paul & Helen Ellis Charitable Trust to K.T., and US National Cancer Institute cancer center support grant P30-CA016056 to Roswell Park Comprehensive Cancer Center.
Footnotes
Publisher's Disclaimer: This AM is a PDF file of the manuscript accepted for publication after peer review, when applicable, but does not reflect post-acceptance improvements, or any corrections. Use of this AM is subject to the publisher’s embargo period and AM terms of use. Under no circumstances may this AM be shared or distributed under a Creative Commons or other form of open access license, nor may it be reformatted or enhanced, whether by the Author or third parties. See here for Springer Nature’s terms of use for AM versions of subscription articles: https://www.springernature.com/gp/open-research/policies/accepted-manuscript-terms
Conflicts of interest/Competing interests: The authors declare that they have no conflict of interest.
Ethics approval: Institutional review board (IRB) approval at Roswell Park Comprehensive Cancer Center (Buffalo, NY, United States) was waived as publicly available deidentified databases were used.
Availability of data and material (data transparency):
The datasets generated during and analyzed during the current study are available from the original source as they are publicly available deidentified databases.
References
- 1.American Cancer Society. Breast cancer facts & figures 2019–2020. Atlanta, GA: American Cancer Society, Inc; 2019. [Google Scholar]
- 2.Lodi M, Scheer L, Reix N, et al. (2017) Breast cancer in elderly women and altered clinico-pathological characteristics: a systematic review. Breast Cancer Res Treat 166:657–668. [DOI] [PubMed] [Google Scholar]
- 3.Hughes KS, Schnaper LA, Bellon JR, et al. (2013) Lumpectomy plus tamoxifen with or without irradiation in women age 70 years or older with early breast cancer: long-term follow-up of CALGB 9343. J Clin Oncol 31:2382–2387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kiderlen M, de Glas NA, Bastiaannet E, et al. (2014) Impact of comorbidity on outcome of older breast cancer patients: a FOCUS cohort study. Breast Cancer Res Treat 145:185–192. [DOI] [PubMed] [Google Scholar]
- 5.Muss HB, Berry DA, Cirrincione C, et al. (2007) Toxicity of older and younger patients treated with adjuvant chemotherapy for node positive breast cancer: the cancer and Leukemia group B experience. J Clin Oncol 25:3699–3704. [DOI] [PubMed] [Google Scholar]
- 6.Angarita FA, Elmi M, Zhang Y, Look Hong N (2018) Patient-reported factors influencing the treatment decision-making process of older women with non-metastatic breast cancer: a systematic review of qualitative evidence. Breast Cancer Res Treat 171:545–564. [DOI] [PubMed] [Google Scholar]
- 7.Hughes KS, Schnaper LA, Berry D, et al. (2004) Lumpectomy plus tamoxifen with or without irradiation in women 70 years of age or older with early breast cancer. N Engl J Med 351:971–977. [DOI] [PubMed] [Google Scholar]
- 8.Martelli G, Boracchi P, De Palo M, et al. (2005) A randomized trial comparing axillary dissection to no axillary dissection in older patients with T1N0 breast cancer: results after 5 years of follow-up. Ann Surg 242:1–9; discussion 7–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.International Breast Cancer Study Group, Rudenstam CM, Zahrieh D, et al. (2006) Randomized trial comparing axillary clearance versus no axillary clearance in older patients with breast cancer: first results of International Breast Cancer Study Group Trial 10–93. J Clin Oncol 24:337–344. [DOI] [PubMed] [Google Scholar]
- 10.Kunkler IH, Williams LJ, Jack WJ, Cameron DA, Dixon JM, PRIME II investigators (2015) Breast-conserving surgery with or without irradiation in women aged 65 years or older with early breast cancer (PRIME II): a randomised controlled trial. Lancet Oncol 16:266–273. [DOI] [PubMed] [Google Scholar]
- 11.Society of Surgical Oncology. https://www.choosingwisely.org/clinician-lists/sso-sentinel-node-https://www.choosingwisely.org/clinician-lists/sso-sentinel-node-biopsy-in-node-negative-women-70-and-over/biopsy-in-node-negative-women-70-and-over/ Accessed 7 March 2021
- 12.Landercasper J, Bailey L, Berry TS, et al. (2016) Measures of appropriateness and value for breast surgeons and their patients: the American Society of Breast Surgeons Choosing Wisely (®) initiative. Ann Surg Oncol 23:3112–3118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Choosing Wisely. An Initiative of the American Board of Internal Medicine (ABIM) Foundation. www.choosingwisely.org Accessed June 16. 2021
- 14.Davey MG, Ryan ÉJ, Burke D, et al. (2021) Evaluating the clinical utility of routine sentinel lymph node biopsy and the value of adjuvant chemotherapy in elderly patients diagnosed with oestrogen receptor positive, clinically node negative breast cancer. Breast Cancer (Auckl). 15:11782234211022203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Thompson J, Le J, Hop A, Melnik M, Paulson J, Wright GP (2021) Impact of Choosing Wisely recommendations on sentinel lymph node biopsy and postoperative radiation rates in women over age 70 years with hormone-positive breast cancer. Ann Surg Oncol 28(10):5716–5722. [DOI] [PubMed] [Google Scholar]
- 16.McKevitt E, Cheifetz R, DeVries K, et al. (2021) Sentinel node biopsy should not be routine in older patients with ER-positive HER2-negative breast cancer who are willing and able to take hormone therapy. Ann Surg Oncol 28:5950–5957. [DOI] [PubMed] [Google Scholar]
- 17.Corso G, Magnoni F, Montagna G, et al. (2021) Long-term outcome and axillary recurrence in elderly women (≥70 years) with breast cancer: 10-years follow-up from a matched cohort study. Eur J Surg Oncol 47:1593–1600. doi: 10.1016/j.ejso.2021.02.027. Epub 2021 Mar 3. [DOI] [PubMed] [Google Scholar]
- 18.Mansel RE, Fallowfield L, Kissin M, et al. (2006) Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: the ALMANAC Trial. J Natl Cancer Inst 98:599–609. [DOI] [PubMed] [Google Scholar]
- 19.Sparano JA, Gray RJ, Makower DF, et al. (2018) Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer. N Engl J Med 379:111–121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Paik S, Shak S, Tang G, et al. (2004) A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med 351:2817–2826. [DOI] [PubMed] [Google Scholar]
- 21.Ramsey SD, Barlow WE, Gonzalez-Angulo AM, et al. (2013) Integrating comparative effectiveness design elements and endpoints into a phase III, randomized clinical trial (SWOG S1007) evaluating oncotypeDX-guided management for women with breast cancer involving lymph nodes. Contemp Clin Trials 34:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Welsh JL, Hoskin TL, Day CN, Habermann EB, Goetz MP, Boughey JC (2017) Predicting nodal positivity in women 70 years of age and older with hormone receptor-positive breast cancer to aid incorporation of a Society of Surgical Oncology Choosing Wisely guideline into clinical practice. Ann Surg Oncol 24:2881–2888 [DOI] [PubMed] [Google Scholar]
- 23.Veerapong J, Boughey J, Mittendorf E, et al. (2011) A validated risk assessment of sentinel lymph node involvement in breast cancer patients. Ann Surg Oncol 18(Suppl 1):S1–S144.21274749 [Google Scholar]
- 24.Yoo TK, Kim SJ, Lee J, et al. (2020) A N0 predicting model for sentinel lymph node biopsy omission in early breast cancer upstaged from ductal carcinoma in situ. Clin Breast Cancer 20:e281–e289. [DOI] [PubMed] [Google Scholar]
- 25.Zhao YX, Liu YR, Xie S, Jiang YZ, Shao ZM (2019) A nomogram predicting lymph node metastasis in t1 breast cancer based on the Surveillance, Epidemiology, and End Results Program. J Cancer 10:2443–2449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cui X, Zhu H, Huang J (2020) Nomogram for predicting lymph node involvement in triple-negative breast cancer. Front Oncol 10:608334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zhang M, Wang B, Liu N, et al. (2021) Nomogram for predicting preoperative regional lymph nodes metastasis in patients with metaplastic breast cancer: a SEER population-based study. BMC Cancer 21:565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hu X, Xue J, Peng S, et al. (2021) Preoperative Nomogram for predicting sentinel lymph node metastasis risk in breast cancer: a potential application on omitting sentinel lymph node biopsy. Front Oncol 11:665240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Gentles AJ, Newman AM, Liu CL, et al. (2015) The prognostic landscape of genes and infiltrating immune cells across human cancers. Nat Med 21:938–945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Mori T, Wada T, Suzuki T, Kubota Y, Inagaki N (2007) Singar1, a novel RUN domain-containing protein, suppresses formation of surplus axons for neuronal polarity. J Biol Chem 282:19884–19893. [DOI] [PubMed] [Google Scholar]
- 31.Wei Z, Sun M, Liu X, Zhang J, Jin Y (2014) Rufy3, a protein specifically expressed in neurons, interacts with actin-bundling protein Fascin to control the growth of axons. J Neurochem 130: 678–692. [DOI] [PubMed] [Google Scholar]
- 32.Vukmirica J, Monzo P, Le Marchand-Brustel Y, Cormont M (2006) The Rab4A effector protein Rabip4 is involved in migration of NIH 3T3 fibroblasts. J Biol Chem 81:36360–36368. [DOI] [PubMed] [Google Scholar]
- 33.Ivan V, Martinez-Sanchez E, Sima LE, et al. (2012) AP-3 and Rabip4’ coordinately regulate spatial distribution of lysosomes. Plos One 7:48142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.He J, Vora M, Haney RM, et al. (2009) Membrane insertion of the FYVE domain is modulated by pH. Proteins 76: 852–860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fukuda M, Kobayashi H, Ishibashi K, Ohbayashi N (2011) Genome-wide investigation of the Rab binding activity of RUN domains: development of a novel tool that specifically traps GTP-Rab35. Cell Struc Funct 36: 155–170. [DOI] [PubMed] [Google Scholar]
- 36.Yamamoto H, Koga H, Katoh Y, Takahashi S, Nakayama K, Shin HW (2010) Functional cross-talk between Rab14 and Rab4 through a dual effector, RUFY1/Rabip4. Mol Biol Cell 21:2746–2755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Yoshida H, Okumura N, Kitagishi Y, Shirafuji N, Matsuda S (2010) Rab5(Q79L) interacts with the carboxyl terminus of RUFY3. Int J Biol Sci 6:187–189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Xie R, Wang J, Tang W, et al. (2017) Rufy3 promotes metastasis through epithelial-mesenchymal transition in colorectal cancer. Cancer Lett 390:30–38. [DOI] [PubMed] [Google Scholar]
- 39.Wang G, Zhang Q, Song Y, et al. (2015) PAK1 regulates RUFY3-mediated gastric cancer cell migration and invasion. Cell Death Dis 6:e1682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Men W, Li W, Li Y, et al. (2019) RUFY3 predicts poor prognosis and promotes metastasis through epithelial-mesenchymal transition in lung adenocarcinoma. J Cancer 10:6278–6285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Xie R, Wang J, Liu X, et al. (2017) RUFY3 interaction with FOXK1 promotes invasion and metastasis in colorectal cancer. Sci Rep;7:3709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Zhu H, Dai W, Li J, et al. (2019) HOXD9 promotes the growth, invasion and metastasis of gastric cancer cells by transcriptional activation of RUFY3. J Exp Clin Cancer Res 38:412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Cerami E, Gao J, Dogrusoz U, et al. (2012) The cBio cancer genomics portal: an open platform for exploring multidimensional cancer genomics data. Cancer Discovery 2:401–404 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Liu J, Lichtenberg T, Hoadley KA, et al. (2018) An Integrated TCGA Pan-Cancer Clinical Data Resource to Drive High-Quality Survival Outcome Analytics. Cell 173:400–16.e11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Curtis C, Shah SP, Chin SF, et al. (2012) The genomic and transcriptomic architecture of 2,000 breast tumours reveals novel subgroups. Nature 486: 346–352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Biganzoli L, Goldhirsch A, Straehle C, et al. (2004) Adjuvant chemotherapy in elderly patients with breast cancer: a survey of the Breast International Group (BIG). Ann Oncol 15(2):207–210 [DOI] [PubMed] [Google Scholar]
- 47.Subramanian A, Tamayo P, Mootha VK, et al. (2005). Gene set enrichment analysis: a knowledge-based approach for interpreting genome-wide expression profiles. Proc Natl Acad Sci USA 102:15545–15550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Oshi M, Huyser MR, Le L, et al. (2021) Abundance of microvascular endothelial cells is associated with response to chemotherapy and prognosis in colorectal cancer. Cancers (Basel) 23;13:1477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Oshi M, Tokumaru Y, Mukhopadhyay S, et al. (2021) Annexin A1 expression is associated with epithelial-mesenchymal transition (EMT), cell proliferation, prognosis, and drug response in pancreatic cancer. Cells 15;10:653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Le L, Tokumaru Y, Oshi M, et al. (2021) TH2 cell infiltrations predict neoadjuvant chemotherapy response of estrogen receptor-positive breast cancer. Gland Surg 10:154–165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Oshi M, Kim TH, Tokumaru Y, et al. (2021) Enhanced DNA repair pathway is associated with cell proliferation and worse survival in hepatocellular carcinoma (HCC). Cancers (Basel) 13:323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Oshi M, Newman S, Murthy V, et al. (2020) ITPKC as a prognostic and predictive biomarker of neoadjuvant chemotherapy for triple negative breast cancer. Cancers (Basel) 12:2758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Satyananda V, Oshi M, Endo I, Takabe K (2021) High BRCA2 gene expression is associated with aggressive and highly proliferative breast cancer. Ann Surg Oncol May 8. doi: 10.1245/s10434-021-10063-5. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 54.Oshi M, Angarita FA, Tokumaru Y, et al. (2020) High Expression of NRF2 is associated with increased tumor-infiltrating lymphocytes and cancer immunity in ER-positive/HER2-negative breast cancer. Cancers (Basel) 12(12):3856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Gandhi S, Elkhanany A, Oshi M, et al. (2020) Contribution of immune cells to glucocorticoid receptor expression in breast cancer. Int J Mol Sci 21(13):4635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Takahashi H, Oshi M, Asaoka M, Yan L, Endo I, Takabe K (2020) Molecular biological features of nottingham histological grade 3 breast cancers. Ann Surg Oncol 27(11):4475–4485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Tokumaru Y, Asaoka M, Oshi M, et al. (2020) High expression of microRNA-143 is associated with favorable tumor immune microenvironment and better survival in estrogen receptor positive breast cancer. Int J Mol Sc 21(9):3213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Tokumaru Y, Katsuta E, Oshi M, et al. (2020) High Expression of miR-34a associated with less aggressive cancer biology but not with survival in breast cancer. Int J Mol Sci 21(9):3045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Okano M, Oshi M, Butash AL, et al. (2019) Triple-negative breast cancer with high levels of annexin a1 expression is associated with mast cell infiltration, inflammation, and angiogenesis. Int J Mol Sci 20(17):4197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Okano M, Oshi M, Butash AL, et al. (2019) Estrogen receptor positive breast cancer with high expression of androgen receptor has less cytolytic activity and worse response to neoadjuvant chemotherapy but better survival. Int J Mol Sci 20(11):2655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Takahashi H, Kawaguchi T, Yan L, et al. (2020) Immune cytolytic activity for comprehensive understanding of immune landscape in hepatocellular carcinoma. Cancers (Basel) 12(5):1221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Narayanan S, Kawaguchi T, Yan L, Peng X, Qi Q, Takabe K (2018) Cytolytic activity score to assess anticancer immunity in colorectal cancer. Ann Surg Oncol;25(8):2323–2331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Aran D, Hu Z, Butte AJ (2017) xCell: digitally portraying the tissue cellular heterogeneity landscape. Genome Biol 18:220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Tokumaru Y, Oshi M, Patel A, et al. (2021) Organoids Are Limited in Modeling the Colon Adenoma-Carcinoma Sequence. Cells 10:488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Oshi M, Newman S, Tokumaru Y, et al. (2020) Plasmacytoid dendritic cell (pDC) infiltration correlate with tumor infiltrating lymphocytes, cancer immunity, and better survival in triple negative breast cancer (TNBC) more strongly than conventional dendritic cell (cDC). Cancers (Basel) 12:3342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Oshi M, Newman S, Tokumaru Y, et al. (2020) Inflammation is associated with worse outcome in the whole cohort but with better outcome in triple-negative subtype of breast cancer patients. J Immunol Res 5618786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Schulze A, Oshi M, Endo I, Takabe K (2020) MYC targets scores are associated with cancer aggressiveness and poor survival in ER-positive primary and metastatic breast cancer. Int J Mol Sci 21:8127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Oshi M, Asaoka M, Tokumaru Y, et al. (2020) Abundance of regulatory T cell (Treg) as a predictive biomarker for neoadjuvant chemotherapy in triple-negative breast cancer. Cancers (Basel) 12:3038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Oshi M, Takahashi H, Tokumaru Y, et al. (2020) The E2F pathway score as a predictive biomarker of response to neoadjuvant therapy in ER+/HER2-breast cancer. Cells 9:1643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Katsuta E, Rashid OM, Takabe K (2020) Fibroblasts as a biological marker for curative resection in pancreatic ductal adenocarcinoma. Int J Mol Sci 2020;21:3890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Oshi M, Takahashi H, Tokumaru Y, et al. (2020) G2M cell cycle pathway score as a prognostic biomarker of metastasis in estrogen receptor (ER)-positive breast cancer. Int J Mol Sci;21:2921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Tokumaru Y, Oshi M, Katsuta E, et al. (2020) Intratumoral adipocyte-high breast cancer enrich for metastatic and inflammation-related pathways but associated with less cancer cell proliferation. Int J Mol Sci. 21:5744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Oshi M, Katsuta E, Yan L, et al. (2020) A novel 4-gene score to predict survival, distant metastasis and response to neoadjuvant therapy in breast cancer. Cancers 12:1148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Tokumaru Y, Asaoka M, Oshi M, et al. (2020) High expression of microRNA-143 is associated with favorable tumor immune microenvironment and better survival in estrogen receptor positive breast cancer. Int J Mol Sci 21:3213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Katsuta E, Yan L, Takeshita T, et al. (2019) High MYC mRNA expression is more clinically relevant than MYC DNA amplification in triple-negative breast cancer. Int J Mol Sci 21:217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Vafa O, Wade M, Kern S, et al. (2002) c-Myc can induce DNA damage, increase reactive oxygen species, and mitigate p53 function: a mechanism for oncogene-induced genetic instability. Mol Cell 9:1031–1044. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated during and analyzed during the current study are available from the original source as they are publicly available deidentified databases.