

Abstract
Objectives
This scoping review aims to summarize the diagnostic value of saliva assessed from current studies that (1) compare its performance in reverse transcriptase‐polymerase chain reaction testing to nasopharyngeal swabs, (2) evaluate its performance in rapid and point‐of‐care COVID‐19 diagnostic tests, and (3) explore its use as a specimen for detecting anti‐SARS‐CoV‐2 antibodies.
Materials and Methods
A systematic search was performed on the following databases: Medline and Embase (Ovid), World Health Organization, Centers for Disease Control and Prevention, and Global Health (Ovid) from January 2019 to September 2021. Of the 657 publications identified from the searches, n = 146 articles were included in the final scoping review.
Results
Our findings showcase that salivary samples exceed nasopharyngeal swabs in detecting SARS‐CoV‐2 using reverse transcriptase‐polymerase chain reaction testing in several studies. A select number of rapid antigen and point‐of‐care tests from the literature were also identified capable of high detection rates using saliva. Moreover, anti‐SARS‐CoV‐2 antibodies have been shown to be detectable in saliva through biochemical assays.
Conclusion
We highlight the potential of saliva as an all‐rounded specimen in detecting SARS‐CoV‐2. However, future large‐scale clinical studies will be needed to support its widespread use as a non‐invasive clinical specimen for COVID‐19 testing.
Keywords: COVID‐19, COVID‐19 nucleic acid testing, COVID‐19 serological testing, COVID‐19 testing, early diagnosis, point‐of‐care testing
1. INTRODUCTION
COVID‐19 has emerged as an unprecedented challenge for the healthcare industry as well the whole world. While recently approved vaccines have begun distribution in many countries, diagnostic tests for COVID‐19 remain an essential tool to detect and track the transmission of the disease until most of the population become vaccinated. Conventional tests use reverse transcriptase‐polymerase chain reaction (RT‐PCR) techniques to detect the presence of SARS‐CoV‐2 nucleic acids in patient samples, usually from nasopharyngeal swab (NPS) specimens (Udugama et al., 2020). However, NPS collection can be invasive and uncomfortable for patients, and places healthcare workers at risk of infection. NPS sensitivity may also vary depending on time of specimen collection relative to the disease progression of COVID‐19 (Kucirka et al., 2020). All these reasons considered, it is crucial to investigate other promising methods of detection that are less invasive and more accurate for diagnosing COVID‐19.
Saliva and oral fluids have been increasingly used for the detection of various systemic diseases and infections (Javaid et al., 2016). With respect to COVID‐19, there is currently evidence showing multiple pathways through which SARS‐CoV‐2 can show presence in saliva: through spread from the upper/lower respiratory tract, from gingival crevicular fluid, or from direct infection of the salivary glands which can then act as a viral reservoir (Han & Ivanovski, 2020). Moreover, saliva collection is economical, is less invasive and more comfortable for patients, and utilizes minimal equipment (Khurshid et al., 2020). Early studies evaluating SARS‐CoV‐2 RT‐PCR using saliva samples reported detection rates of viral ribonucleic acid (RNA) as high as 90% (To et al., 2020) as well as high sensitivity and specificity values at 0.88 and 0.92, respectively (Atieh et al., 2021). Further studies have demonstrated that saliva specimens show positive test results even when other respiratory specimens of the same patient test negative for SARS‐CoV‐2 (Hamid et al., 2020). Saliva may also provide information regarding the course of the disease. Viral load has been found to be highest in saliva specimens during the first week of symptom manifestation and serum antibodies against SARS‐CoV‐2 have been detected in patients while viral RNA was still detectable in saliva (Hamid et al., 2020). Although the extent of COVID‐19 antibodies in saliva is still largely unknown, salivary immunoglobin G (IgG) profiles in general have been shown to be highly similar to plasma IgG profiles for a large number of antigens (Ceron et al., 2020). Therefore, saliva may have the potential to play a major role in COVID‐19 diagnosis and disease progression monitoring, from detecting viral loads not evident in respiratory specimens to screening for immunity. However, large‐scale evaluation of saliva‐based COVID‐19 diagnostic tests compared to the current standard NPS‐based tests have yet to be conducted. Furthermore, the role of saliva as a sample for use in rapid antigen and point‐of‐care (POC) tests may also require further investigation.
The aim of this review was to provide insight on the current available evidence regarding the efficacy of saliva as a specimen in RT‐PCR‐based COVID‐19 diagnostic tests compared to NPS specimens, as a specimen for rapid antigen/POC COVID‐19 diagnostic tests, and its potential for COVID‐19 immunity screening.
2. METHODS
2.1. Study design
A scoping review was conducted using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta‐Analyses) Extension for Scoping Reviews checklist (Tricco et al., 2018).
2.2. Search strategy
A systematic search was performed on the following databases: Ovid Medline and Embase, World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), and Ovid Global Health. The following key terms were used: (exp Coronavirus/OR coronavirus.mp. OR 2019‐nCoV.mp. OR Covid‐19.mp. OR Sars‐CoV‐2.mp. OR novel coronavirus.mp.) AND (exp Diagnosis/OR screen*.tw. OR detect*.tw.) AND (exp Saliva/OR salivary fluid.tw. OR salivary biomarkers.tw. OR saliva.tw. OR saliva sample.tw. OR oral fluid.tw.)
2.3. Eligibility criteria and selection of manuscripts
The following inclusion criteria were used for screening search results: Articles must be primary research studies, within the publication range 01/01/2019–09/27/2021, in the English language, and contain a study sample of at least 10 confirmed COVID‐19‐positive patients. Included articles were grouped into the following three categories: (1) Saliva as a RT‐PCR Specimen for SARS‐CoV‐2; (2) Rapid antigen/POC COVID‐19 Testing with Saliva; and (3) SARS‐CoV‐2 Antibody Testing with Saliva. Review articles, case studies, animal studies, and letters to the editor were excluded from the study.
2.4. Screening and data extraction
Screening of search results was performed independently by three authors (Y.W., A.U., and P.K.) on Rayyan QCRI. Each author was blinded from the screening results of the other two authors, and all three authors convened after completing independent screening to resolve disagreements through discussion to reach the final decision on included articles. Duplicate articles were excluded. One investigator was assigned to each of the three categories (A.U., Y.W., and P.K.) to extract data from the articles. The final sets of included articles were summarized in Figure 1 and Tables 1, 2, 3 along with their relevant details.
FIGURE 1.
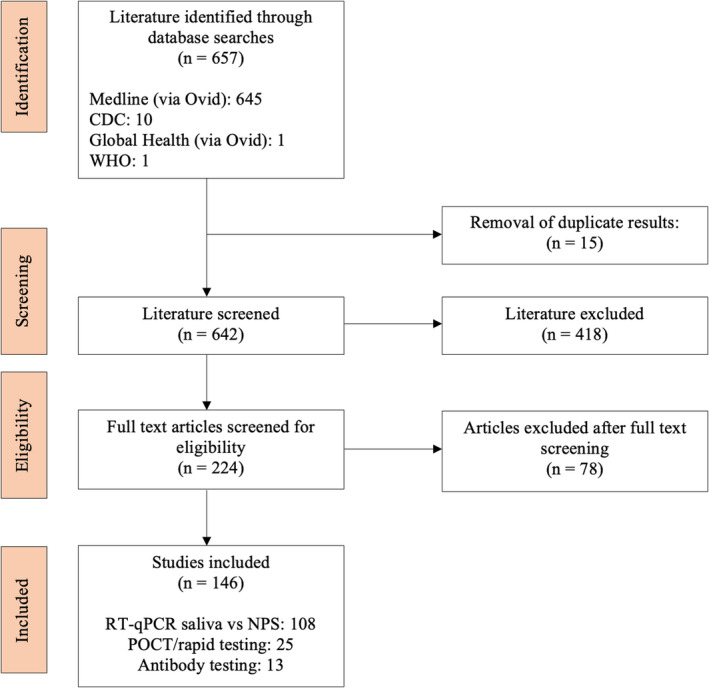
Flow diagram of study selection in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta‐Analyses) guidelines
TABLE 1.
Brief description of included studies with saliva as a diagnostic tool using RT‐qPCR technology (n = 108)
| References | Number of patients | Sample & saliva collection method | Target | Results |
|---|---|---|---|---|
| Azzi et al. (2020a, 2020b) | 25 (17 males, 8 females) | Saliva and NPS; Drooling method | N gene | Ct cycles below 33 for saliva samples |
| Chau et al. (2020) | 30 (17 symptomatic, 13 asymptomatic) | Saliva and NPS/throat swabs; Not mentioned | E gene and RdRp gene | Saliva samples 7 of 11 (64%) positive in the asymptomatic group and 13 of 16 (81%) in the symptomatic group (p = 0.56) |
| Fukumoto et al. (2020) | 71 | Saliva, sputum, and NPS; Spit method | ORF1ab and N gene | 53% (95% CI 83.8%–99.4%) for NPS samples, 95.5% (95% CI 77.2%–99.9%) for saliva samples, and 85.7 (95% CI 42.1%–99.6%) for sputum samples |
| Guest et al. (2020) | 153 | OPS, saliva, and DBS | RNase P | Assessed quality of samples for prospective use |
| Hanson et al. (2020) | 354 | Saliva, NP‐ ANS; Straight saliva | ORF1ab | Number of cases detected‐ NPS (80), Saliva (81) and ANS (70) |
| Hung et al. (2020) | 18 | POPS and NPS; Throat clearing | E gene | Early morning saliva samples have highest viral load |
| Iwasaki et al. (2020) | 76 | Saliva and NPS; Pool and spit | N gene | Ct values higher in saliva in later stages |
| Alainna J. Jamal et al. (2020) | 91 | Saliva and NPS; Spit method | N gene | NPS was 17% more sensitive than saliva overall |
| Kim et al. (2020) | 15 | Saliva and NPS; Spit method | E gene and RdRp gene | Sensitivity of saliva lower (64%) than NPS (77%) |
| Landry et al. (2020) | 134 | Saliva and NPS; Pool and spit | N1, N2 gene | Rate of detection in saliva 85.7% |
| Leung et al. (2020) | 95 | DTS and NPS; Throat clearing | E gene and RdRp gene | Rate of detection in DTS (53.7%) comparable with NPS (47.4%) |
| McCormick‐Baw et al. (2020) | 156 | Saliva and NPS; Spit method | E and N2 gene | Comparable sensitivity of saliva and NPS |
| Moreno‐Contreras et al. (2020) | 253 | Saliva and OPS/NPS; Spit method | E gene | Rate of detection in saliva (86.2%) and OPS/NPS (65%) |
| Pasomsub et al. (2020) | 200 | Saliva and NPS; Spit method | ORF1ab and N gene | Sensitivity of saliva sample 84.2% (95% CI 60.4%–96.6%) |
| Rao et al. (2020) | 217 | DTS and NPS; Throat clearing | E gene and RdRp gene | Detection rate higher in saliva compared to NPS testing (93.1%, 149/160 vs 52.5%, 84/160, p < 0.001) |
| Williams et al. (2020) | 522 | Saliva and NPS; Pool and spit | ORF1ab | Ct value significantly less in NPS than saliva |
| Wong et al. (2020) | 95 | POPS and NPS; Throat clearing | E gene | POPS 61.6% (95% CI 55.1%–67.6%) and NPS 53.3% (95% CI 46.8%–59.6%) |
| Wyllie et al. (2020) | 70 patients and 495 healthcare workers | Saliva and NPS; Spit method | N1, N2 gene | Rate of detection in saliva 81% (95% CI, 71–96) vs NPS 71% (95% CI, 67–94) |
| Jamal et al. (2021) | 91 | Saliva and NPS; Paired sample, Spit | RdRp, E, and N genes | Overall, NPS was more sensitive than saliva by 17% for SARS‐CoV‐2 detection especially in the later weeks of infection. |
| Yokota et al. (2021) | 42 | Saliva and NPS; self‐collected saliva | N1, N2 gene | Rates of detection in saliva are 90% compared to 81% in NPS. |
| Sun et al. (2021) | 20 paired samples, 77 positive saliva samples, and 85 positive NPS samples | Saliva and NPS, Paired and pooled sample, spit | E, N, O, and RNase P gene | Ct values of E, N, and O gene were comparable between NPS and saliva samples by Wilcoxon signed rank test and the concordance of NPS/saliva was about 80% (16/20) with no significant difference (p = 0.13). |
| Pasomsub et al. (2021) | 19 | Saliva and NPS, throat swab. Paired samples, spit | ORF1 ab and N gene, RNase P control | Ct values of the ORF1ab and N genes were 32.7 (28.5–35.0) and 31.8 (28.4–33.7), respectively, in saliva specimens, and 32.0 (27.4–34.3) and 30.5 (26.1–32.3), respectively, in NPS and throat swabs. |
| Barra et al. (2021) | 10 | Saliva and NPS; Paired samples, spit | N1 gene | The median (min–max) N1 Cq values were 21.01 (14.53–27.59) for NPS and 29.51 (24.50–40) for saliva, suggesting a lower diagnostic capability of SARS‐CoV‐2 in saliva. |
| Sahajpal et al. (2021) |
68 (Phase 1) 95 (Phase 2) |
Saliva and NPS; paired samples, spit | N and ORF1ab |
Phase 1: Detection rate was higher in NPS (89.7%) compared to saliva (50%). Phase 2: Detection rate was higher in saliva (97.8%) compared to NPS (78.9%). |
| Van Vinh Chau et al. (2020) | 30 | Saliva and NPS/throat samples (NTS), spit | E and RdRp gene | Higher viral load (p = 0.031) and (p = 0.064) was observed in NTS than in saliva in both asymptomatic and symptomatic patients. |
| Yu et al. (2021) | 68 | Saliva, NPS and OPS, Spit sample | ORF1ab and N gene | Viral load was in saliva [292.30 copies/test (IQR 20.20–8628.55)] and NPS [274.40 copies/test (IQR 33.10–2836.45)] with RT‐PCR A. |
| Rao et al. (2021) | 217 | Saliva and NPS; paired sample, deep throat saliva | E and RdRp gene | The detection rate for SARS‐CoV−2 was higher in saliva compared to NPS testing (93.1%, 149/160 vs 52.5%, 84/160, p < 0.001) |
| Gaur et al. (2021) | 73 | Saliva, NPS and Buccal swabs, spit | E and RNase P genes | The mean Ct values of NPS, and saliva samples were 24.92 ± 6.51, and 28.16 ± 4.48, respectively. A slight positive correlation was observed between NPS and saliva Ct values (r = 0.359; p = 0.025). |
| Wong et al. (2020) | 229 | POPS and NPS; spit, paired samples | E gene | POPS and NPS paired samples showed a positivity of 61.5% (95% confidence interval [CI] 55.1–67.6%) and 53.3% (95% CI 46.8–59.6%), respectively. |
| Teo et al. (2021) | 200 | Naso‐OP saliva and NPS, spit samples | Sars‐CoV‐2 genome | The percentage of test‐positive saliva was higher than NPS and NS swabs. |
| Aydin et al. (2021) | 128 | Saliva and Oro‐NPS, spit | ORF1ab and N gene | There is a moderately significant positive correlation between Ct value/NPS and Ct value/saliva (r = 0.402, p < 0.0001). The Ct value/saliva was found to be significant in predicting disease severity (Eta coefficient 0.979). |
| Ota et al. (2021) | 123 | Saliva and NPS; Spit | N2 gene | The positive rate was 19.5% (24/123) for NPS and 38.2% (47/123) for saliva (p = 0.48). The quantified viral copies (mean ± SEM copies/5 μl) were 9.3 ± 2.6 in NPS and 920 ± 850 in saliva (p = 0.0006) |
| Goldfarb et al. (2021) | 40 | Saliva, NPS and saline gargle samples | E and RdRp gene | Saliva samples were both significantly less sensitive and less acceptable than mouth rinse/gargle samples |
| Fernandez‐Gonzalez et al. (2021) | 120 | Saliva, self‐collected (SC) vs supervised (SVC) and NPS; paired samples, pool and spit collection | E gene | Sensitivity for NPS specimens was 95% [95% CI, 88.9%–97.9%)]. SVC showed the best case detection rate with significantly higher sensitivity than SC samples (86% [95% CI, 72.6%–93.7%] versus 66.7% [95% CI, 50.4%–80%]; p = 0.027) |
| Carrouel et al. (2021) | 31 | Saliva and NPS; self‐collected | RdRp‐IP2 and IP4 gene | Viral load was significantly correlated (r = 0.72). The concordance probability was estimated at 73.3%. In symptomatic adults, SCPS performance was similar to that of NPS (Percent Agreement = 74.1%; p = 0.11) |
| Ku et al. (2021) | 42 | Saliva and NPS; self‐collected | E gene | With reference to NPS, the saliva test had PPA 66.7%, NPA 91.7%, and OA 69.0%; the buccal swab had PPA 56.7%, NPA 100%, and OA 73.8%. Self‐collected saliva tests and buccal swabs showed moderate agreement with HCW‐collected NPS. |
| Masse et al. (2021) | 51 | POPS and NPS; spit | N, S and ORF1ab gene | Positive and negative results were concordant between saliva samples and NPS in 51 (96.2%) and in 85 (94.4%) patients, respectively, with a Cohen's Kappa coefficient of 0.89 (95% CI 0.82–0.97, p < 0.001). |
| Yee et al. (2021) | 300 | Saliva and NPS; paired samples, spit | N, S and ORF1ab gene | The overall concordance for saliva and NPS was 91.0% (273/300) and 94.7% (284/300), respectively. The PPA for saliva and NPS was 81.4% (79/97) and 89.7% (87/97), respectively. Saliva detected 10 positive cases that were negative by NPS. |
| Echavarria et al. (2021) | 174 | Saliva and NPS; paired sample,spit | E gene | Kappa Cohen's coefficient agreement between NPS and saliva was 0.96 (95% CI, 0.90–0.99). Median Ct values in NPS versus saliva were 18.88 (IQR, 15.60–23.58; range, 11.97–38.10) versus 26.10 (IQR, 22.75–30.06; range, 13.78–39.22), respectively (p < 0.0001). |
| Leung et al. (2021) | 29 | DTS and NPS; paired sample, spit | E gene | In general, DTS samples had a higher positive detection rate than NPS samples, although there were no statistically significant differences between the two sampling methods (p > 0.05). |
| Griesemer et al. (2021) | 93 | NS, Saliva and NPS; drool and spit | N1 gene | The second cohort (Total, n = 227, n = 93 for SARS‐CoV‐2 positive) had a positivity rate of 41%, with sensitivity in NPS, NS, and saliva of 97.9%, 87.1%, and 87.1%, respectively. |
| Herrera et al. (2021) | 130 (for NPS pools), 255 (for saliva pools) | Saliva and NPS; paired and pooled samples, self‐collected | N1 and N2 gene | Concordance between NPS and saliva results was 95.2% (kappa 0.727, p = 0.0001) and 97.9% without considering inconclusive results (kappa 0.852, p = 0.0001). Saliva had a lower number of inconclusive results than NPS (0.9% vs 1.9%). Furthermore, saliva showed a significantly higher concentration of both total RNA and viral copies than NPS |
| Cassinari et al. (2021) | 130 | Saliva and NPS; drool samples | RdRp gene | RT‐qPCR analysis of 14 samples yielded a sensitivity of 62% (8/14) in saliva vs 100% (14/14) in NPS, respectively, and the 6‐plex RT‐ddPCR for these 14 samples had a sensitivity of 85% (13/14) in saliva and 100% in NPS. |
| Barat et al. (2020) | 449 | Saliva and NPS; paired and pooled samples, drool. | N1 and N2 gene | The percentages of PPA and NPA of saliva compared to nasopharyngeal swab were 81.1% (95% CI, 65.8% to 90.5%) and 99.8% (95% CI, 98.7% to 100%), respectively. |
| Paliksa et al. (2021) | 58 | Saliva and NPS; saliva collection kit | ORF1ab and S | The PPA was 98.28% (CI 90.76%–99.96%) and NPA was 98.11% (CI 89.93%–99.95%). A statistically significant (p < 0.05) and moderately strong (R = 0.53) correlation between Ct values in saliva and NPS samples. |
| Mendoza et al. (2021) | 20 | Saliva and NPS; drool | ORF1ab, N, S, and MS2 | 100% agreement between the results of saliva versus nasopharyngeal swab diagnostic testing. The median Ct value for ORF1ab of the nasopharyngeal swab was 30.35 and only 21.04 in Saliva indicating, higher viral load in the saliva, higher sensitivity of the saliva test, better viral recovery, and/or stability using saliva collection. |
| Braz‐Silva et al. (2020) | 70 | Saliva and NOP; chew on cotton pad and collect | E and S gene | Sensitivities of 74.2% (95% CI; 63.7%–83.1%) for NOP and 78.6% (95% CI; 67.6%–86.6%) for saliva. |
| Norizuki et al. (2021) | 51 | Saliva and NPS; spit | ORF1ab and E gene | Sensitivities for saliva RT‐qPCR (84.7–100), quantitative NPS antigen (84.7–100) saliva LAMP (84.7–100), and qualitative NPS antigen (84.7–100). 90.9% for quantitative saliva antigen (75.7–98.1), 81.8% for saliva direct RT‐qPCR (64.5–93.0) |
| Ana Laura et al. (2021) |
156 for OP/NP 122 for saliva |
Saliva and NPS/OPS; spit | RdRp, E and N gene | Viral loads did not show a significant difference between NPS/OPS and saliva |
| Sutjipto et al. (2020) | 73 | Saliva and NPS; Spit, drooling method | N and ORF1ab gene |
Clinical sensitivity for NPS and saliva was 95%, and 44%–56%, respectively |
| Huber et al. (2021) | 273 | Saliva and NPS; Throat clearing/spit | E and ORF1 gene | Detection of SARS‐CoV‐2 in saliva fared well compared to NPS (PPA = 92.5%). SARS‐CoV‐2 infections were more often detected in saliva than NPS (positive predictive value = 84.8%) |
| Tapia et al. (2021) | 112 | Saliva, MTS and NPS; spit | RdRp, N and E genes | Saliva samples showed a lower percentage of SARS‐Cov‐2 detection compared to NPS samples, (85.7 vs. 96.4%). In average, saliva samples showed higher Ct values for all tested target genes, compared to those from NPS. |
| Nacher et al. (2021) | 162 | Saliva and NPS; pooled samples, saliva sputum | RdRp, N and E genes | The sensitivity of RT‐PCR on saliva vs. NPS varied depending on the patient groups considered or on Ct thresholds. There were 10 (6.2%) patients with a positive saliva sample and a negative NPS, all of whom had Ct values <25 for three genes. |
| Trobajo‐Sanmartin et al. (2021) | 337 | Saliva and NPS; paired samples, collect in mouth, swish, and spit in tube. | E gene | The virus detection in saliva compared to NPS was 51.9% (95% CI: 46.3%–57.4%) and increased to 91.6% (95% CI: 86.7%–96.5%) when Ct was ≤30. |
| Senok et al. (2020) | 35 | Saliva and NPS; drool | RdRp and N gene | The sensitivity and specificity of saliva were 73.1% (95% CI 52.2%–88.4%) and 97.6% (95% CI 95.5%–98.9%) while the PPA and NPA were 67.9% (95% CI 51.5%–80.8%) and 98.1% (95% CI 96.5%–99.0%), respectively. |
| Altawalah et al. (2020) | 344 for NPS, 305 for Saliva | Saliva and NPS; deep cough viscous saliva | ORF1ab, N and S gene | An analysis of the agreement between the NPS and saliva specimens demonstrated 91.25% observed agreement (κ coefficient = 0.814, 95% CI, 0.775–0.854). |
| Matic et al. (2021) | 74 | Saliva and NPS; paired samples, spit | E gene | Saliva demonstrated good concordance with paired NPS for SARS‐CoV‐2 detection in 67/74 cases (90.5%). |
| Binder et al. (2020) | 20 | Saliva, NPS and rectal swab | N gene | The agreement between NPS and saliva positivity was substantial (89.5%, Kappa: 0.79). |
| Kandel et al. (2020) | 432 | Saliva and NPS; paired samples | E gene | The sensitivity of NPS was 0.93 (95% CI 0.81–0.99) and that of saliva 0.91 (95% CI 0.79–0.98). Cycle threshold values obtained from saliva were higher than those from NPS (median difference in Ct 2.76; 95% CI 0.36–5.15, p = 0.03). |
| von Linstow et al. (2021) | 20 | Saliva and Nasal swabs | N gene | In children, positivity and viral load in saliva was 25% (5/20) compared to 79% (15/19) in nasal swabs. |
| Potter et al. (2021) | 49 | Saliva and NPS; paired samples, spit | Pp1ab | The PPA between the original NPS and the saliva specimen was 63.2% (31/49), and the NPA between the original NPS and saliva specimen was 100% (262/262). |
| Migueres et al. (2021) | 55 | Saliva and NPS; spit | RdRp, ORF1ab genes | Global sensitivity of saliva and NPS were 80% [95% CI: 67.0%−89.6%] and 96.4% [95% CI: 87.5%−99.6%], respectively. |
| Alkhateeb et al. (2021) | 48 | Saliva and NPS; | ORF1ab and S | Saliva had an overall sensitivity of 59%, a specificity of 95%, and a NPA of 98%. Saliva demonstrated higher sensitivity in symptomatic (80%) vs. asymptomatic individuals (36%) (p = 0.006), Ct values in NPS specimens were higher in saliva‐negative vs. saliva‐positive cases (p = 0.02 and <0.001). |
| Mestdagh et al. (2021) | 2850 | NPS and saliva (Spitting and oral swab) | E gene | Sensitivity for saliva spitting and 21.9% (95% CI, 14.4%–31.0%) for saliva swabbing. But for subjects with medium to high viral load, sensitivity saliva increased to 93.9% (95% CI, 79.8%–99.3%) and 76.9% (95% CI, 56.4%–91.0%) for spitting and swabbing, respectively, regardless of symptomatic status. |
| Gupta et al. (2021) | 29 | NTS, saliva and gargle |
ORF1ab, N and Egenes |
The positivity rates of rRT‐PCR in NTS, saliva, and gargle lavage samples were 82.7 (24/29), 79.3 (23/29), and 86.2% (25/29). Positivity rate was more in fresh gargle than the stored 1‐day samples. |
| de Paula Eduardo et al. (2021) | 55 | NPS, unstimulated saliva, and oral swab | ORF1ab, N | 48 (87.3%) were also positive with self‐collected unstimulated saliva. Forty‐one patients also provided oral swab samples, and of those, 27 patients (65.9%) were positive for SARS‐CoV‐2 RNA detection |
| Sasaki et al. (2021) | 13 | NPS, saliva and oral swabs | N gene | 61.5% agreement of saliva and 76.9% of oral swabs with standard NPS |
| Bidkar et al. (2021) | 80 | NPS and saliva | ORF1ab, E gene | 24.4% sensitivity in saliva samples |
| Kojima et al. (2020) | 45 | NPS and saliva (Supervised and unsupervised) | N1, N2 | Clinician‐supervised oral fluid swab specimens detected 90% of infected individuals, clinician‐supervised nasal swab specimens 85%, clinician‐collected posterior NPS specimens detected 79%, and unsupervised self‐collected oral fluid swab specimens detected 66%. |
| Oliver et al. (2021) | 1050 | NPS and saliva |
ORF−1 and ORF−8 genes |
PPA was 72% [95% CI 58–84%] for saliva and 63% [49–76%] for NPS (p = 0.398) |
| Plantamura et al. (2021) | 1205 | Oral swabs, NPS, saliva | ORF1ab, N, S, |
Saliva for symptomatic patients (n = 653), sensitivity, specificity, and kappa coefficient were 89.4 (95% CI 84.9–93.9), 96.2 (95% CI 94.5–97.9), and 0.86 (95% CI 0.82–0.90) For asymptomatic outpatients, sensitivity decreased to 79.2% (95% CI 62.9–95.4) Oral swab sensitivity of 61.1% (95% CI 52.7–69.4), a specificity of 98.9% (95% CI 52.7–69.4), a PPV of 91.9%, and a NPV of 92.5%. |
| De Santi et al. (2021) | 308 | NPS, saliva | Rdrp, N1 gene |
94.3% sensitivity (95% CI 87.2–97.5%), and 95.9% specificity (95% CI 92.4–97.8%) in saliva when paired with NPS |
| Costa et al. (2021) | 196 | NPS, saliva | N gene | Saliva samples revealed a low sensitivity of 45.2% |
| Vaz et al. (2020) | 155 | NPS, OPS | E, Rdrp gene | The sensitivity and specificity of RT‐PCR using saliva samples were 94.4% (95% CI 86.4–97.8) and 97.62% (95% CI 91.7–99.3). 96.1% agreement between NPS and OPS |
| Guclu et al. (2020) | 64 | Saliva, NPS | genesis RT‐PCR SARS‐CoV‐2 (Primer Design, UK) kit | 35.9% agreement between saliva and NPS samples |
| Procop et al. (2020) | 224 | Saliva, NPS | N gene |
100% PPA, 99.4% NPA. The CT values from RT‐PCRs from the saliva from this discordant specimen were 34.4 cycles for N1, 34.7 cycles for N2, and 34.6 cycles for N3, indicating low viral load. |
| Hanson et al. (2020) | 354 | NPS, ANS, saliva | Hologic SARS‐CoV‐2 assay |
PPA‐ NPS and ANS or saliva was 86.3% (95% confidence interval [CI], 76.7%–92.9%) and 93.8% (95% CI, 86.0%–97.9%) NPA‐ 9.6% (95% CI, 98.0%–100.0%) for NPS versus ANS and 97.8% (95% CI, 95.3%–99.2%) for NPS versus saliva. More cases were detected by the use of NPS (n = 80) and saliva (n = 81) than by the use of ANS (n = 70) |
| Kim et al. (2020) | 53 | NPS/OPS, saliva | E and RdRp gene | Saliva sensitivity was 64% (34/53), While NPS/OPS 77% (41/53). The sensitivity of rRT‐PCR using saliva was especially lower in early stage of symptom onset (1–5 days; 8/15; 53%) and in patients who did not have sputum (12/22; 55%) |
| Nacher et al. (2021) | 1028 | Saliva and NPS | E, N, RdRp | The median Ct for the positive N gene target was 21.5 NPS samples versus 26.1 in saliva, p = 0.003; for the E gene target, the median was 21.5 in NPS samples versus 24.6 in saliva, p = 0.02; for the RdRp gene target the median was 22.5 in NPS versus 26.3 in saliva samples, p = 0.005. |
| Fernandes et al. (2021) | 452 | NPS and saliva | N, E and ORF1ab | No detection in 13 saliva (direct) of the 80 positive NPS samples and in 16 saliva (RNA) of a total of 76 NPS positive samples. An average increase in 7.3 Ct values in saliva samples in comparison to NPS |
| Mohd Thabit et al. (2021) | 96 | NPS and saliva |
E, RdRp, and N2 |
Saliva samples had high sensitivity (80.4%) and specificity (90.0%) with a high positive predictive value of 91.8%, 89.3% agreement with NPS. Detection highest for the N2 gene and E gene provided the highest viral load |
| Johnson et al. (2021) | 60 | NPS and saliva | N1 and N2 | 88% concordance of saliva samples with NPS |
| Fan et al. (2021) | 103 | NPS and Saliva | N1, N2, S, ORF1ab | 97% agreement between saliva and NPS |
| Poukka et al. (2021) | 40 | Gargle, NPS, spit and sputum | E gene | All specimens had comparable sensitivity to NPS, with morning spit sample with highest among them |
| Callahan et al. (2021) | 385 | NPS, saliva | Not specified | High concordance among saliva and NPS samples. But viral load higher in NPS |
| Al Suwaidi et al. (2021) | 476 | NPS, saliva | N, E, RdRp |
Sensitivity and specificity of saliva RT‐PCR was 87.7% (95% confidence interval (CI) 78.5–93.9) and 98.5% (95% CI 96.8–99.5). The positive and negative predictive values were 92.2% (95% CI 84.2–96.3) and 97.6% (95% CI 95.7–98.6), with a kappa coefficient of 0.879 (95% CI 0.821–0.937) |
| Jamal et al. (2021) | 91 | NPS, saliva | N, E, RdRp |
Sensitivity was 89% for nasopharyngeal swabs and 72% for saliva |
| Goncalves et al. (2021) | 364 | Saliva, gingival fluid, NPS | N1, N2 gene | For saliva samples, the concordance rate was 67.6% among positive samples, 42.9% among inconclusive, and 96.8% among negative ones. |
| Boerger et al. (2021) | 282 |
NPS, patient‐collected MTS, and patient‐collected saliva specimens |
N gene | Compared to NPS, saliva exhibited a sensitivity of 90.9% (30/33) and specificity of 99.2% (246/248), while patient‐collected MTS exhibited a sensitivity of 93.9% (31/33) and specificity of 99.2% (246/248) |
| de Oliveira et al. (2021) | 403 | OPS, saliva |
S, N and ORF1ab |
Saliva had 92% of sensitivity and 97% of specificity on onset of symptoms. Low sensitivity, 82% in asymptomatic cases |
| Smith‐Jeffcoat et al. (2021) | 1076 | ANS, saliva, NPS | N1 and N2 genes |
Compared with NPS samples, ANS samples had 59% sensitivity (95% CI 47%–70%), 100% specificity (95% CI 100%–100%), 100% PPV (95% CI 92%–100%), and 97% NPV (95% CI 95%–98%) Compared with NPS samples, saliva had 68% sensitivity (95% CI 55%–78%), 99% specificity (95% CI 99%–100%), 90% PPV (95% CI 79%–97%), and 97% NPV (95% CI 96%–98%). |
| Yokota et al. (2021) | 1924 | NPS, saliva | N2 gene | The sensitivity of NPS and saliva specimens were 86% and 92% (83%−97%), respectively, with specificities >99.9%. The true concordance probability between the NPS and saliva tests was estimated at 0.998 |
| Mahmoud et al. (2021) | 600 | NPS, saliva | ORF1ab | Saliva sensitivity, 85.34%, specificity, 95.04%, positive predictive value (PPV) 91.67%, negative predictive value (NPV) 91.03% in comparison to NPS. The difference in mean Ct value for saliva samples, and NPS was not found to be statistically significant. |
| Labbe et al. (2021) | 125 | OPS/NPS, saliva | Multiple kits | Saliva had comparable sensitivity as compared to NPS, but false‐negative chances higher in low viral load samples due to high Ct values. |
| LeBlanc et al. (2021) | 38 | OPS/NPS, self‐collected OPS/NPS, and self‐collected saline gargles | Various kits | Sensitivity of self‐collected OPS/NPS swabs and saline gargles was comparable to healthcare worker collected OPS/NPS samples |
| (Fougere et al., 2021) | 397 | NPS, saliva | E gene |
Sensitivity of saliva was 85.2% (95%CI: 78.2%–92.1%) when using NP as the standard But, viral loads were lower with saliva than NPS |
| Sasikala et al. (2021) | 3018 outpatients, 101 hospitalized patients | OPS/NPS, self‐collected OPS/NPS, and saliva | N, S, ORF1ab |
Out patients: Sensitivity of detection was 60.9% (55.4–66.3%, CI 95%), with a negative predictive value of 36% (32.9–39.2%, CI 95%) Hospitalized patients: Sensitivity of detection was 60.9% (55.4–66.3%, CI 95%), with a negative predictive value of 36% (32.9–39.2%, CI 95%) |
| Marx et al. (2021) | 730 |
Self‐collected: Saliva, ANS Healthcare worker: NPS |
N1 and N2 |
Sensitivity for SARS‐CoV−2 detection by rRT‐PCR appeared higher for SS than for ANS (85% vs 80%) and higher among symptomatic participants than among those without symptoms (94% vs 29% for SS; 87% vs 50% for ANS) |
| Gable et al. (2021) | 17 | ANS, OPS, saliva | N1 and N2 gene | ANS and OPS samples were more concordant in comparison to saliva, because saliva showed more positives over the period of infection. Lower Ct values in saliva than OPS and ANS in patients positive for more than 10 days |
| Hitzenbichler et al. (2021) | 34 hospitalized patients | Throat washing, NS, OPS | E gene | Sensitivity: 85% for NS, 79% for OPS and 85% for TW. Median viral load: OPS 7.3 × 103 cp/mL, NS 4.1 × 103, Saliva 3.4 × 103, and TW 2.7 × 103 |
| Justo et al. (2021) | 76 healthcare workers | Saliva, NPS | RdRp, E, N gene | 97.56% agreement of saliva with NPS samples for positives, while 100% agreement for negatives |
| Tutuncu et al. (2021) | 53 | Saliva, NPS | RdRp gene | 90.56% agreement of saliva with NPS samples |
| Babady et al. (2021) | 285 healthcare workers | Oral rinse, POPS, NPS | N1, N2 gene | Oral rinse had 85.7% agreement, and POPS 97.7% |
| Hanege et al. (2021) | 38 positive patients | NPS, saliva, tear, cerumen | N1, N2 gene | Of all the NPS positive patients, saliva had the highest sensitivity, 76.3%, followed by tear (55.3%) and cerumen (39.5%) |
| Bhattacharya et al. (2021) | 78 symptomatic patients | NPS, saliva | ORF1 gene | Ct value for saliva 27.07 (CI 95%), not significantly different from NPS, mean 28.24 (CI 95%) |
| Castelain et al. (2021) | 501 | NPS, saliva | RdRp and N gene | Only 2 saliva‐positive samples out of 26 NP positive. |
| Rao et al. (2021) | 562 asymptomatic participants | NPS+OPS, saliva | N, ORF1 gene | 96.1% agreement of saliva with NPS (65 of 562, κ coefficient 0.78, 95% CI 0.69–0.87, p < 0.05). C t values of N and ORF1a genes were 30.6 ± 7.06 and 30.0 ± 6.86, respectively, in NPS + OPS, and 29.2 ± 7.87 and 28.5 ± 7.70, respectively, in random saliva |
| Dogan et al. (2021) | 200 | NPS, OPS and saliva | ORF1ab | Higher positivity for NPS and OPS samples at 83%, for saliva it was 63% (p < 0.001). |
Abbreviations: ANS, anterior nasal swab; CI, confidence interval; DBS, dried blood swab; DTS, deep throat saliva; HCW, healthcare worker; IQR, Interquartile range; MTS, mid‐turbinate swab; NOP, nasal‐oropharyngeal; NPA, negative percent agreement; NPS, nasopharyngeal swab; NS, nasal swab; NTS, Nasal throat swab; OA, overall agreement; OPS, oropharyngeal swab; PPA, positive percent agreement; POPS, posterior oropharyngeal saliva; RdRp, RNA‐dependent RNA polymerase.
TABLE 2.
Brief description of included studies with saliva as a diagnostic specimen for POC/rapid antigen testing (n = 25)
| Reference | Number of patients | Sample‐to‐readout time | Type of test | Target | Results |
|---|---|---|---|---|---|
| Amendola et al. (2021) | 127 | 35 min | Rapid antigen: CLEIA (Lumipulse) | Nucleocapsid protein | 52.4% sensitivity, 94.1% specificity (sensitivity >90% when Ct < 25, specificity 100% after excluding recovered COVID‐19 patients) |
| Audigé et al. (2021) | 307 | 18 min | Rapid antigen: ECLIA (Elecsys) | Nucleocapsid protein | 40.2% PPA and 99.5% NPA with NPS RT‐PCR; 100% PPA for Ct < 26 samples |
| Azmi et al. (2021) | 40 | 1 h | CRISPR‐based (CASSPIT) | S gene and N gene |
98% PPA with RT‐PCR data for Ct < 35 samples |
| Basso et al. (2021) | 127 | 30 min | Rapid antigen: CLEIA (Lumipulse) & ICA (Panbio & Espline) | Nucleocapsid protein | CLEIA: 72% sensitivity, 97% specificity; ICA: 13% sensitivity (only satisfactory for Ct < 25 samples) |
| Chen et al. (2020) | 58 | 50 min | RT‐qPCR (Xpert Xpress) | E gene and N2 gene | No significant difference in detection rates between NPS (94.8%) and POPS (89.7%) |
| Courtellemont et al. (2021) | 14 | 15 min | Rapid antigen: ICA (COVID‐VIRO) | Nucleocapsid protein | 0% sensitivity |
| Chow et al. (2020) | 67 | 1 h | RT‐LAMP | ORF3a gene and E gene | DTS/sputum samples showed sensitivities of 94.03% at 60 min and 97.02% at 90 min, and specificity of 100% |
| de Puig et al. (2021) | 48 | 1 h | CRISPR‐based (miSHERLOCK) | N gene | 96% sensitivity and 95% specificity at threshold of 2000 RFUs |
| Ganguli et al. (2021) | 34 | 1 h | RT‐LAMP | Not specified | 100% sensitivity with two‐step method, 3 false positives |
| Ishii et al. (2021) | 229 | 30 min | Rapid antigen: ICA (Espline) & CLEIA (Lumipulse) | Nucleocapsid protein | ICA: 33% sensitivity, 100% specificity; CLEIA: 89% sensitivity, 96.9% specificity |
| Kobayashi et al. (2021) | 91 | 1 h | RT‐LAMP | E1 gene and As1e gene | 77.2% overall sensitivity, 97% specificity |
| Nagura‐Ikeda et al. (2020) | 103 |
30 min (ICA) 35 min (RT‐LAMP) |
Rapid antigen: ICA (Espline); RT‐LAMP (Loopamp) | Nucleocapsid protein; N1 gene, N2 gene, ORF1 gene, and E gene | Rapid antigen test showed significantly lower sensitivity (11.7%) compared to RT‐LAMP and RT‐qPCR tests for saliva |
| Ptasinska et al. (2021) | 19,461 | 30 min | RT‐LAMP (LamPORE) | N2 gene, E gene, ORF1ab gene | 99.58% sensitivity, 99.46% specificity |
| Saeed et al. (2021) | 100 | 15 min | Rapid antigen: ICA (Lepu Medical) | Nucleocapsid protein | Overall sensitivity: 21%; (males 21%, females 23%, children 0%) |
| Stokes et al. (2021) | 41 | 20 min | Rapid antigen: ICA (Panbio) | Nucleocapsid protein | 2.6% sensitivity; saliva collection terminated early due to low sensitivity |
| Toppings et al. (2021) | 123 | 50 min | RT‐LAMP | Not specified | 100% PPA and 96.7% NPA with NPS RT‐PCR; 93.3% PPA and 100% NPA with saliva RT‐PCR |
| Uwamino et al. (2021) | 73 | 30 min | Rapid antigen: ICA (Espline) | Nucleocapsid protein | Low sensitivity and low concordance with NPS, but high concordance with viral cultures (95.1%) |
| Vaz et al. (2021) | 40 | 50 min | RT‐qPCR (Xpert Xpress) | E gene and N2 gene | 100% concordance with conventional RT‐qPCR |
| Wong et al. (2020) | 120 | 50 min | RT‐qPCR (Xpert Xpress) | E gene and N2 gene | DTS showed very good agreement (PPA = 98.86%, NPA = 100%) between Xpert Xpress and NAAT |
| Xun et al. (2021) | 104 | 30 min | RT‐LAMP + PfAgo | N gene and E gene |
93.3% sensitivity, 98.6% specificity |
| Yamazaki et al. (2021) | 44 | 45 min | RT‐LAMP | ORF1ab gene, S gene, ORF7a gene | 82.6% sensitivity, 100% specificity |
| Yang et al. (2021) | 573 | 1 h | RT‐LAMP | N gene and ORF1ab gene |
94% sensitivity, 100% specificity |
| Yokota et al. (2021) | 17 | 30 min | Rapid antigen: ICA (Espline) & CLEIA (Lumipulse) | Nucleocapsid protein | ICA: 24% sensitivity; CLEIA: 82% sensitivity |
| Yokota et al. (2021) | 288 | 35 min | Rapid antigen: CLEIA (Lumipulse) | Nucleocapsid protein | 99.2% sensitivity |
| Yokota et al. (2021) | 2056 | 35 min | Rapid antigen: CLEIA (Lumipulse) | Nucleocapsid protein | 98.2% concordance with RT‐qPCR results |
Abbreviations: CLEIA, chemiluminescence enzyme immunoassay; ICA, immunochromatographic assay; NPA, negative percent agreement; PPA, positive percent agreement.
TABLE 3.
Brief description of included studies with saliva as a diagnostic tool using SARS‐CoV‐2 antibody testing (n = 13)
| Reference | Number of patients | Saliva collection method | Type of test | Target | Results |
|---|---|---|---|---|---|
| Aita et al. (2020) | 43 COVID‐19 inpatients and 326 screening subjects |
NPS and saliva collection (Salivette). Saliva collected after one minute using a cotton swab. |
ELISA | Salivary IgA and serum IgA, IgG, IgM | 100% specificity, sensitivity not mentioned |
| Alkharaan et al. (2021) | 256 saliva samples from convalescent patients (n = 74, cohort 1), undiagnosed individuals with self‐reported questionnaires (n = 147, cohort 2), and individuals sampled prepandemic (n = 35, cohort 3). | Using expectorated unstimulated whole saliva, samples were self‐collected following standardized instructions and sample tubes provided | Multiplex bead‐based array platform (Multiple for Spike‐f, S1,NC‐C, Combination antigen, etc.) | IgG and IgA |
The best results declared by the authors were as: Spike‐f showed 88% sensitivity and 100% specificity. NC‐C showed 66% sensitivity and 100% specificity. The spike‐f, S1, NC‐C triple combination, showed 72% sensitivity and 100% specificity. |
| Caulley et al. (2021) | 70 | Swab | Automated immunoassay platform by the Roche anti‐SARS‐ CoV‐2 qualitative assay (Roche Diagnostics, Laval Quebec). | IgM, IgG |
Not Mentioned. |
| Elledge et al. (2020) | 42 | Not mentioned. | IgG and IgM (to a much less extent) | Above 98% sensitivity, 99% specificity as quick as 5 min with low input sample (1ul per reaction) | |
| Faustini et al. (2021) | Hospitalized subjects (HS, N = 14), confirmed PCR; non‐hospitalized convalescent (NHC, N = 39) confirmed by PCR but were not hospitalized; and asymptomatic non‐hospitalized convalescent patients (AS, N = 6), no reported symptoms with a positive by PCR. As a negative control group, they used sera taken before 2019 (Pre19, N = 22). |
Whole saliva samples collected by passive dribble into saliva collection tubes for a timed period of 4 min |
ELISA, Using trimeric spike glycoprotein, rather than nucleocapsid. | IgG, IgA, and IgM | Sensitivity of 98.4% and specificity of 97.6% |
| Isho et al. (2020) | 128 | Some used chewing swabs provided by Salivette® and some expectorated in a conical tube | snELISA | IgG, IgM and to a lesser extent IgA |
The sensitivity for IgG antibodies to spike and RBD were 89% and 85%, respectively, while the sensitivity of the assays for IgA antibodies to spike and RBD were 51% and 30%, respectively, and the sensitivity of the assays for IgM antibodies to spike and RBD were 57% and 33%, respectively. |
| Keuning et al. (2021) | 517 | Saliva was collected using a buccal swab | Luminex assay in serum and saliva | SARS‐CoV‐2 spike (S), receptor‐binding domain (RBD), and nucleocapsid (N)‐specific IgG and IgA |
Sensitivity of 96.7% and specificity of 97.5% |
| Liu et al. (2020) | 62 positive and 384 negative |
Saliva samples were collected by spitting into a plastic tube |
Near‐infrared‐fluorescence amplification by nanostructured plasmonic gold substrates | IgM, IgG, and IgG avidity against the S1 subunit of the spike protein |
The pGOLD SARS‐CoV‐2 IgG/IgM showed near 100% sensitivity 99.78% specificity |
| MacMullan et al. (2020) | 149 | By swabbing the inside of the cheeks, and the top and bottom gums, under the tongue, and on the tongue, to gather a sufficient amount of saliva for viral RNA and Orasure oral specimen collection devices for oral fluid | ELISA | IgG and IgA | Sensitivity of 84.2% and a specificity of 100%. If the population is limited to samples over the age of 40, sensitivity of 91.5% and specificity of 100% are also achieved. |
| MacMullan et al. (2021) | 147 | Oral fluid swab for viral RNA and Orasure oral fluid | OraSure Technologies oral antibody collection de‐ vice (OACD) and ELISA | IgG, IgA, IgM | 93.94% sensitive and 100% specific on the EuroImmun kit and 78.79% sensitive and 100% specific on the GSD kit |
| Martinez‐Fleta et al. (2020) | 36 | Not specified. | ELISA | IgG, IgM, and IgA Ab responses to the Cys‐like protease from SARS‐CoV‐2, also known as 3CLpro or Mpro | Multiple for IgG, IgA, and IgM and for RBD, Mpro, and NP |
| Saeed et al. (2021) | 100 | Not mentioned | Rapid testing kit | Not mentioned | 52% sensitivity for NPS Rapid test and 21% for saliva Rapid test |
| Ter‐Ovanesyan et al. (2021) | The samples were divided into three groups: prepandemic control samples (left, n = 2), saliva samples from patients who tested negative by RT‐qPCR from nasopharyngeal swabs (NP‐PCR negative, middle, n = 7) and saliva samples from patients who tested positive by RT‐qPCR from nasopharyngeal swabs (NP‐PCR positive, right, n = 3). | Swab | saliva RNA extraction method and combined it with an ultrasensitive antibody test based on single‐molecule array (Simoa) technology. | IgG, IgA and IgM | Not mentioned |
3. RESULTS
Details of the study selection process are described in the PRISMA flow diagram presented by Figure 1. In summary, a total of 657 publications were found through search results from databases. After title and abstract screening and removing duplicates, 224 articles were retrieved along with full text versions for manual assessment. Finally, a total of 146 eligible articles were included in the present review.
3.1. Saliva as a RT‐PCR specimen for SARS‐CoV‐2
A plethora of literature has followed utilizing saliva as a diagnostic tool, owing to the evidence of SARS‐CoV‐2 presence in saliva (Table 1). Studies that made the cutoff criteria for number of patients had sample sizes ranging from 13 to 3000. The cohorts included symptomatic as well as asymptomatic patients, patients tested in outpatient departments, general surveys, hospitalized patients, and healthcare workers. Genes amplified for RT‐PCR detection were most commonly the E (Envelope) (n = 38), N (Nucleocapsid) (n = 34), ORF1ab (Open Reading Frame) (n = 31), RdRp (RNA‐dependent RNA polymerase) (n = 24), N1 and N2 (n = 18), S (Spike) (10), and ORF8 (n = 1). Samples collected varied from saliva, naso‐oropharyngeal swabs, anterior nasal swabs, deep throat swabs, gargles, rinses, and cerumen. Different sampling techniques for saliva included drool, spit, gingival fluid, and sputum, and were either self‐collected or collected under healthcare worker supervision/assistance. A few cases included a sample‐specific collection time, such as morning only samples. The disease states extended from general population and healthcare worker surveys in asymptomatic individuals, to symptomatic and hospitalized patients at the convalescent phase of the disease.
Sensitivity recorded for saliva samples included values from 44% (Sutjipto et al., 2020), 64% (Kim et al., 2020), and 95.5% (Fukumoto et al., 2020). Specificity for SARS‐CoV‐2 in saliva ranged from 98.5% (95% CI 96.8–99.5) to 99% (Smith‐Jeffcoat et al., 2021). When compared to standard NPS samples, saliva showed a positive predictive value (PPV) of 90% (95% CI 79%–97%) and a negative predictive value (NPV) 97% (95% CI 96%–98%) (Smith‐Jeffcoat et al., 2021). Cycle threshold (Ct) values range in saliva around 24–40 (Azzi et al., 2020a, 2020b; Barra et al., 2021), with 28.5–35 for the ORF1ab gene and 28.4–33.7 for the N gene as observed by Pasomub and colleagues (Pasomsub et al., 2021). Early morning samples had the highest viral load in hospitalized patients (Hung et al., 2020). Better detection in later stages was also suggested, as dual testing in both positive and recovering patients may limit the spread from such patients by ensuring an appropriate isolation period (Iwasaki et al., 2020; Sahajpal et al., 2021). There is a positive correlation between saliva and NPS samples (Aydin et al., 2021; Matic et al., 2021) with positive percent agreement (PPA) ranging from 66.7% (Ku et al., 2021; Senok et al., 2020) to 100% (Cassinari et al., 2021; Mendoza et al., 2021). More concordance was seen for negative results with negative percent agreement (NPA) values at 91.7% (Ku et al., 2021), 98% (Paliksa et al., 2021; Senok et al., 2020), and 100% (Potter et al., 2021).
As is the case of Ct values/viral load, current evidence regarding the detection rates between saliva and NPS samples is debatable. Moreno‐Contreras and colleagues concluded saliva samples to be more reliable than NPS samples, with detection rates of 86.2% versus 65%, respectively (Moreno‐Contreras et al., 2020). Similarly, Iwasaki and colleagues observed a detection rate of 95.5% in saliva samples, 87.5% for sputum, and 53% for NPS (Iwasaki et al., 2020). Similar conclusions were made by several authors with variable sample sizes (Ota et al., 2021; Rao et al., 2020; Rao et al., 2021; Teo et al., 2021; Wong et al., 2020; Wyllie et al., 2020; Yokota et al., 2021). No significant difference between the sensitivity or Ct values of saliva and NPS samples was observed on various instances as well (Sun et al., 2021). On the contrary, NPS was found to be 17% more sensitive than saliva by Jamal and colleagues (Jamal et al., 2020) while neither a single NPS nor single saliva sample was 100% sensitive for COVID‐19 detection in another study (Kim et al., 2020). The median Ct values observed by Barra and colleagues were 21.01 (14.53–27.59) for NPS and 29.51 (24.50–40) for saliva, suggesting a lower diagnostic capability of SARS‐CoV‐2 in saliva (Barra et al., 2021). Higher viral load in the NPS samples was evident in multiple cohorts (Tapia et al., 2021; Van Vinh Chau et al., 2020). Furthermore, alternatives such as mouth rinses and gargles were also observed to give a better diagnosis of the infection over saliva samples (Goldfarb et al., 2021).
3.2. POC COVID‐19 testing with saliva
A select number of studies have investigated the potential of saliva to be used as a sample for POC COVID‐19 testing (Table 2). With RT‐PCR being the current standard test for detection of SARS‐CoV‐2, one area of interest for the implementation of POC testing using saliva has been automated RT‐PCR‐based assays. One such assay, the Xpert Xpress SARS‐CoV‐2 (Cepheid), is a molecular test that offers a sample‐to‐answer time of approximately 45 min and was granted Emergency Use Authorization from the FDA. The assay targets the N2 gene and E gene of SARS‐CoV‐2, yielding a positive result if both targets or if the N2 gene alone are detected and a presumptive positive result if the E gene alone is detected. With nasopharyngeal specimens currently being the only validated specimens for the Xpert Xpress SARS‐CoV‐2 assay, 3/146 of the included studies in this scoping review attempted to validate the use of the Xpert Xpress SARS‐CoV‐2 assay using saliva as a biological specimen. A diagnostic accuracy study involving 58 COVID‐19‐positive patients compared the sensitivities of NPS specimens and posterior oropharyngeal saliva specimens using the Xpert Xpress SARS‐CoV‐2 assay (Chen et al., 2020). The study found no significant difference between NPS (94.8%) and saliva (89.7%) detection rates, but a significantly earlier median Ct value was observed for NPS (26.8) compared to saliva (29.7). In another study, a sample of 120 deep throat saliva specimens tested with the Xpert Xpress SARS‐CoV‐2 assay showed high PPA (98.86%) and NPA (100%) with the standard‐of‐care nucleic acid amplification test (Wong et al., 2020). A study by Vaz and colleagues found similar high concordance between the Xpert Xpress SARS‐CoV‐2 assay results and RT‐PCR results (100%), in addition to the Xpert Xpress SARS‐CoV‐2 assay yielding lower median Ct values for its gene targets (29.7 for E gene and 31.6 for N2 gene) compared to the RT‐PCR median Ct values (34.9 for E gene and 38.3 for RdRp gene) (Vaz et al., 2021).
An alternative testing method that has the potential to offer rapid, highly sensitive and specific SARS‐CoV‐2 detection is the colorimetric reverse transcriptional loop‐mediated isothermal amplification (RT‐LAMP) assay. In this scoping review, 9/146 of the included studies attempted to validate the performance of RT‐LAMP‐based tests to detect SARS‐CoV‐2 RNA in clinical saliva samples. 8 of these studies reported high‐sensitivity values of their respective RT‐LAMP tests ranging from 74.8% to 100% and specificity values ranging from 70.9% to 100% (Chow et al., 2020; Ganguli et al., 2021; Kobayashi et al., 2021; Nagura‐Ikeda et al., 2020; Ptasinska et al., 2021; Xun et al., 2021; Yamazaki et al., 2021; Yang et al., 2021). Another study compared the results of RT‐LAMP with RT‐PCR using 30 positive and 30 negative clinical saliva samples and found a 100% PPA and a 96.7% NPA between the two different tests (Toppings et al., 2021).
In addition to the studies on RT‐PCR and RT‐LAMP‐based tests, two studies reported on novel SARS‐CoV‐2 POC detection assays based on CRISPR (clustered regularly interspaced short palindromic repeats)/Cas technology. de Puig et al. (2021) developed and evaluated a novel POC diagnostic test, miSHERLOCK (minimally instrumented specific high‐sensitivity enzymatic reporter unlocking), that utilized CRISPR/Cas technology to target a highly conserved region of the SARS‐CoV‐2 N gene. With a 1‐h sample‐to‐readout time, the miSHERLOCK diagnostic reported a 95% sensitivity and 96% specificity using a sample size of 27 positive and 21 negative unprocessed saliva samples. A study by Azmi and colleagues combined CRISPR‐Cas13a‐based RNA detection and lateral flow assay readouts, CASSPIT (Cas13 Assisted Saliva‐based and Smartphone Integrated Testing) for unprocessed saliva‐based detection of SARS‐CoV‐2 (Azmi et al., 2021). Using 40 saliva samples from COVID‐19‐positive patients, the authors reported a 98% PPA with RT‐PCR data for samples with Ct values under 35.
3.3. Rapid antigen COVID‐19 testing with saliva
The use of COVID‐19 rapid antigen tests has especially amassed an increasing demand throughout the course of the pandemic, and as a result, several studies have investigated the use of saliva as a testing specimen for commercial SARS‐CoV‐2 antigen detection assays. 12/146 of the included studies in this scoping review evaluated the performance of saliva samples in commercial SARS‐CoV‐2 rapid antigen tests. Immunochromatographic assays, such as the Espline SARS‐CoV‐2 rapid antigen test (Fujirebio), were one of the more commonly tested SARS‐CoV‐2 POC tests in these studies using saliva as a biological specimen. 3/5 studies that tested the Espline SARS‐CoV‐2 assay reported low sensitivity values ranging from 11.7% to 33.0% (Ishii et al., 2021; Nagura‐Ikeda et al., 2020; Yokota et al., 2021). However, another study reported a concordance rate of 95.1% with viral culture results. (Uwamino et al., 2021). A different study found similar results, reporting that satisfactory sensitivity values for the Espline SARS‐CoV‐2 assay were achieved only for high viral load samples with Ct values below 25 for NPS RT‐qPCR results (Basso et al., 2021). Another three studies evaluated the clinical performance of three other immunochromatography‐based POC COVID‐19 tests, the COVID‐VIRO assay (AAZ), the Panbio assay (Abbott), and the Lepu SARS‐CoV‐2 test kit (Lepu Medical Technology). A study by Courtellemont and colleagues that evaluated the diagnostic performance of the COVID‐VIRO assay for NPS samples collected a subset of 14 COVID‐19‐positive saliva samples that reported a dismal 0% sensitivity using the assay (Courtellemont et al., 2021). Meanwhile, a study by Stokes and colleagues reported a 2.6% sensitivity of the Panbio assay before saliva sample collection was terminated due to poor detection rates compared to NPS (Stokes et al., 2021). Finally, a study by Saeed and colleagues reported an overall sensitivity of 21% when using the Lepu SARS‐CoV‐2 test kit on a saliva sample size of 100 COVID‐19‐positive patients, including men, women, and children (Saeed et al., 2021).
Chemiluminescent enzyme immunoassays, such as the Lumipulse SARS‐CoV‐2 antigen kit (Fujirebio), are another subset of rapid antigen tests for COVID‐19 that have been tested using saliva samples in several studies. Of the 6 studies included in this scoping review that assessed the diagnostic performance of the Lumipulse SARS‐CoV‐2 antigen kit, 4 studies reported high‐sensitivity values ranging from 72.0% to 99.2% while one study reported a low sensitivity value of 52.4% (Amendola et al., 2021; Basso et al., 2021; Ishii et al., 2021; Yokota et al., 2021, 2021). With respect to specificity values, the studies that measured specificity using COVID‐19‐negative saliva samples reported values of 94.1%, 96.9%, and 98.6% (Amendola et al., 2021; Basso et al., 2021; Ishii et al., 2021). Furthermore, one study compared the diagnostic performance of the Lumipulse SARS‐CoV‐2 antigen kit to RT‐qPCR with a saliva sample size of 2056 and found a 98.2% concordance rate between the two diagnostic tests (Yokota et al., 2021). The Elecsys SARS‐CoV‐2 Antigen assay (Roche), a electrochemiluminescence immunoassay, was also evaluated using saliva specimens in a study that found 100% PPA with RT‐PCR of NPS samples having Ct values of less than 26 only, while the overall PPA was reported to be 40.2% (Audigé et al., 2021).
3.4. SARS‐CoV‐2 antibody testing with saliva
Some studies included in this scoping review have explored techniques using saliva for anti‐SARS‐CoV‐2 antibody screening (Table 3). Our findings confirmed that, combined with direct SARS‐CoV‐2 detection methods used for identifying currently infected COVID‐19 patients, anti‐SARS‐CoV‐2 antibody detection using saliva could provide a rapid and non‐invasive alternative method for differentiating between non‐infected, previously infected, and presently infected patients. To readily identify antibody responses in serum and saliva of SARS‐CoV‐2 patients, standard ELISA (enzyme‐linked immunosorbent assay) methods have been modified to be more sensitive to the high‐quality S protein and used as a tool for short‐term and long‐term humoral immunity (Faustini et al., 2021). MacMullan and colleagues concluded that following their optimized protocol in saliva samples, antibodies against SARS‐CoV‐2 were detectable with a sensitivity of at least 84.2% and a specificity of 100% in symptomatic patients (MacMullan et al., 2020). In another study, MacMullan and a group of colleagues found that the OraSure test (OraSure), an oral antibody detection technology and its paired ELISA, have comparable sensitivity and specificity with the serum‐based ELISAs and offers potential for self‐collection (MacMullan et al., 2021).
Caulley and colleagues evaluated patients that tested positive on saliva/swab PCR tests and compared their presence of serum SARS‐CoV‐2‐specific antibodies. They found that the PCR‐based tests have limitations as participants demonstrated seropositivity 5 months post‐infection (Caulley et al., 2021). Thus, some studies argue that a combination of RNA detection with antibody testing may be required for optimal detection (Ter‐Ovanesyan et al., 2021). In one study, Ter‐Ovanesyan and colleagues entertained the idea of using the same saliva sample to develop an efficient saliva RNA extraction and an antibody test. In doing so, they used single‐molecule array (SIMOA) technology and concluded that the RNA and antibody‐paired detection identifies the virus at a higher sensitivity than each method alone (Ter‐Ovanesyan et al., 2021).
In this regard, Faustini and colleagues attest that without such a sensitive method, detection of responses in asymptomatic patients may be suboptimal and less reliable than the PCR tests (Faustini et al., 2021). They suggest that a native‐like, trimeric S antigen is preferred to the N antigen for detection of antibodies and that, if the detection of one Ig is run in parallel with others, their combined detection enhances antibody recognition (Faustini et al., 2021). The persistence of serum and saliva antibody responses to SARS‐CoV‐2 spike antigens in patients was confirmed by Isho and colleagues as they indicated that those antibodies, especially IgG, may be maintained in patients for months post‐symptom onset (Isho et al., 2020). Based on their findings, they suggested that IgG responses in saliva are a good representative measure for systemic immunity to SARS‐CoV‐2 due to the correlation with the serum IgG responses. As a complementary population‐based approach, surveys on mucosal immunity revealed that salivary IgG against SARS‐CoV‐2 persists even at 9 months after mild COVID‐19 infections (Alkharaan et al., 2021). Moreover, salivary IgA appeared to be short‐lived, while specific salivary IgG was stable after mild COVID‐19 and therefore presents an opportunity for non‐invasive, self‐collective saliva testing (Alkharaan et al., 2021). Liu and colleagues quantified the antibody avidities and its accurate detection of SARS‐CoV‐2 antibodies in serum and saliva using a high‐performance semi‐quantitative assay (Liu et al., 2020). They specifically detected IgG, IgM, and IgA avidity against the S1 subunit of the spike protein and the RBD (receptor‐binding domain) of the virus. Another study verified standardized saliva collection as a suitable approach for detecting and monitoring SARS‐CoV‐2 infection by measuring anti‐SARS‐CoV‐2 IgA to replace NPS testing (Aita et al., 2020).
Furthermore, SARS‐CoV‐2 protease molecules have recently proven significant to COVID‐19 research. A study done by Martinez‐Fleta and colleagues explored salivary cysteine‐like protease antibodies as a detectable agent in COVID‐19‐seropositive patients (Martinez‐Fleta et al., 2020). One of these agents is Mpro (main protease), which undertakes a critical role in viral replication, releases mature proteins for the virus, and can be detected using ELISA. The authors concluded that COVID‐19 patients show higher titers IgG, IgM, and IgA antibody responses to the cysteine‐like protease molecule from SARS‐CoV‐2, Mpro, and that such response can be quantified noninvasively and rapidly from saliva as a seropositivity test (Martinez‐Fleta et al., 2020).
4. DISCUSSION
RT‐qPCR is widely known today as a laboratory technique during which an RNA sequence is reverse transcribed to make complimentary DNA, which is further amplified by polymerase chain reaction. For SARS‐CoV‐2, as described earlier, RT‐PCR is considered the standard for diagnosis as several specific mRNAs can be targeted for its detection, such as the mRNAs of ORF1b and the N and E structural proteins (Figure 2). Thus, various recommendations have been made for diagnostic testing of COVID‐19 by different organizations (Corman et al., 2020; Okamaoto et al., 2020). From the selected articles, there is a clear ambiguity in the method of sample collection and the target for SARS‐CoV‐2 detection using saliva. Some researchers used drooling saliva to collect the samples as it eliminated the mucous secretions from the oropharynx and lower respiratory tract (Azzi et al., 2020a, 2020b). Others collected patient saliva by clearing of throat as soon as possible after waking up, before breakfast and brushing to include both bronchopulmonary secretions and nasopharyngeal secretions (Leung et al., 2020; Wong et al., 2020). Furthermore, the time point of sample collection, the severity, and stage of disease have also been variable across the studies (Hung et al., 2020). There is uncertainty in the evidence for assessing the potential of saliva as a diagnostic tool, attributing to the variabilities in methodologies. In conclusion, it can be said that saliva is a reliable tool for COVID‐19 detection but both NPS and saliva specimens should be taken for screening and diagnosis, while gargle and mouth rinse can be another alternative.
FIGURE 2.
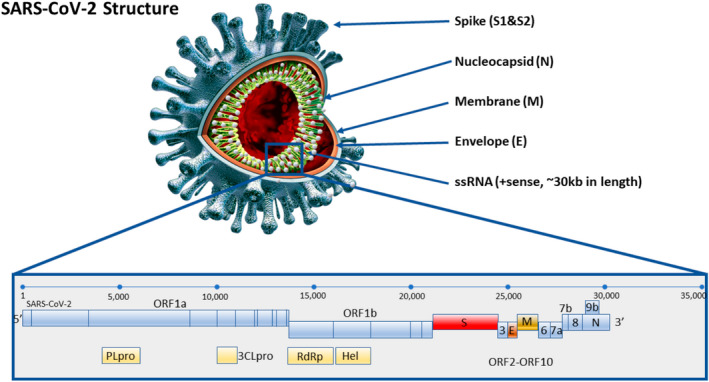
Image of SARS‐CoV‐2 showing its structural and genetic composition. Real‐time PCR COVID‐19 tests utilize the gene expression signal by detecting the mRNA for various structural proteins including spike (S), envelope (E), or nucleocapsid (N), and non‐structural proteins such as ORF1ab. The magnified view shows the RNA expression sequence of the SARS‐CoV‐2 coronavirus with localization of various mRNA targets. Image derived from Kubina and Dziedzic (2020)
POC testing has been defined in the literature as diagnostic tests that are conducted “outside the laboratory at or near the site of patient care, including the patient's bedside, the doctor's office, and the patient's home” (Khurshid, 2018). As the current method of testing that is most well‐documented and accepted by medical staff and the scientific community, RT‐PCR testing continues to be the most well‐established methodology for COVID‐19 diagnostics and offers the highest reliability among POC testing options. However, the high equipment cost, training required for interpretation of results, and longer turnaround time continue to limit its use mostly to mass‐testing facilities with access to trained laboratory personnel and equipment (Carter et al., 2020). Current RT‐PCR‐based POC COVID‐19 tests require specialized equipment for analyzing results that may only be attainable in healthcare and laboratory settings. In comparison, RT‐LAMP‐based tests offer results that may be easily interpreted by non‐laboratory trained staff and faster turnaround time relative to RT‐PCR‐based tests but lack the research background and large‐scale clinical validation needed to scale‐up its usage (Dao Thi et al., 2020). The low cost and high reliability of currently available RT‐LAMP POC test kits may potentially allow employment of this testing method in hospital, clinical, and pre‐travel settings. However, challenges behind building, distributing, and administering RT‐LAMP‐based tests may not favor their use in common workplace or social settings compared to rapid antigen tests.
Rapid antigen tests are another method through which one targets a specific macromolecule of the virus, such as the highly conserved spike protein (Jacobs et al., 2020). The sampling method is similar to PCR‐based methods in that detection depends on the viral load but is advantageous in that it requires no specific equipment nor highly trained personnel. In this method, just like any other chromatographic method, a mobile phase (buffer mixed with the biological specimen) migrates through a stationary phase (e.g., nitrocellulose) tagged with antibodies against the viral antigens. If the viral antigens are present, they attach the antibodies and their accumulation can be detected by a visible chemical reaction which appears on the nitrocellulose membrane. The current CDC (Centers for Disease Control and Prevention) guidelines state that rapid antigen tests are commonly employed in congregate settings such as dormitories, nursing homes, correctional facilities, and homeless shelters to screen for COVID‐19 infections. Due to the low turnaround time ranging from 15 to 30 min and low cost per test, rapid antigen tests offer the main benefit of rapidly identifying infected individuals in the community and workplace setting to prevent transmission and assist infection control measures. However, the overall lower sensitivity of rapid antigen tests suggests that asymptomatic individuals who test negative may require confirmatory laboratory testing using nucleic acid amplification tests (Corman et al., 2021).
From this scoping review, it is evident that the current literature supports the use of saliva as an alternative specimen when compared to NPS for SARS‐CoV‐2 detection. Utilizing an optimized, saliva‐based, rapid or POC kit may help overcome many current pandemic challenges while dealing with the newly emerging SARS‐CoV‐2 variants.
CONFLICT OF INTEREST
None to declare.
AUTHOR CONTRIBUTIONS
Yifei Wang: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Validation; Visualization; Writing – original draft; Writing – review & editing. Akshaya Upadhyay: Data curation; Formal analysis; Investigation; Methodology; Project administration; Resources; Validation; Visualization; Writing – original draft; Writing – review & editing. Sangeeth Gopakumar Pillai: Data curation; Formal analysis; Investigation; Methodology; Project administration; Validation; Visualization; Writing – original draft; Writing – review & editing. Parisa Khayambashi: Data curation; Formal analysis; Investigation; Methodology; Project administration; Validation; Visualization; Writing – original draft; Writing – review & editing. Simon D Tran: Conceptualization; Funding acquisition; Project administration; Resources; Software; Supervision; Writing – review & editing.
PEER REVIEW
The peer review history for this article is available at https://publons.com/publon/10.1111/odi.14216.
Wang, Y. , Upadhyay, A. , Pillai, S. , Khayambashi, P. , & Tran, S. D. (2022). Saliva as a diagnostic specimen for SARS‐CoV‐2 detection: A scoping review. Oral Diseases, 00, 1–29. 10.1111/odi.14216
REFERENCES
- Aita, A. , Basso, D. , Cattelan, A. M. , Fioretto, P. , Navaglia, F. , Barbaro, F. , Stoppa, A. , Coccorullo, E. , Farella, A. , Socal, A. , Vettor, R. , & Plebani, M. (2020). SARS‐CoV‐2 identification and IgA antibodies in saliva: One sample two tests approach for diagnosis. Clinica Chimica Acta, 510, 717–722. 10.1016/j.cca.2020.09.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Al Suwaidi, H. , Senok, A. , Varghese, R. , Deesi, Z. , Khansaheb, H. , Pokasirakath, S. , Chacko, B. , Abufara, I. , Loney, T. , & Alsheikh‐Ali, A. (2021). Saliva for molecular detection of SARS‐CoV‐2 in school‐age children. Clinical Microbiology & Infection, 27(9), 1330–1335. 10.1016/j.cmi.2021.02.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alkharaan, H. , Bayati, S. , Hellström, C. , Aleman, S. , Olsson, A. , Lindahl, K. , Bogdanovic, G. , Healy, K. , Tsilingaridis, G. , De Palma, P. , Hober, S. , Månberg, A. , Nilsson, P. , Pin, E. , & Sällberg Chen, M. (2021). Persisting salivary IgG against SARS‐CoV‐2 at 9 months after mild COVID‐19: A complementary approach to population surveys. Journal of Infectious Diseases, 224(3), 407–414. 10.1093/infdis/jiab256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alkhateeb, K. J. , Cahill, M. N. , Ross, A. S. , Arnold, F. W. , & Snyder, J. W. (2021). The reliability of saliva for the detection of SARS‐CoV‐2 in symptomatic and asymptomatic patients: Insights on the diagnostic performance and utility for COVID‐19 screening. Diagnostic Microbiology & Infectious Disease, 101(3), 115450. 10.1016/j.diagmicrobio.2021.115450 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Altawalah, H. , AlHuraish, F. , Alkandari, W. A. , & Ezzikouri, S. (2020). Saliva specimens for detection of severe acute respiratory syndrome coronavirus 2 in Kuwait: A cross‐sectional study. Journal of Clinical Virology, 132, 104652. 10.1016/j.jcv.2020.104652 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Amendola, A. , Sberna, G. , Lalle, E. , Colavita, F. , Castilletti, C. , Menchinelli, G. , Posteraro, B. , Sanguinetti, M. , Ippolito, G. , Bordi, L. , & Capobianchi, M. ; On Behalf Of Inmi Covid‐Study Group . (2021). Saliva is a valid alternative to nasopharyngeal swab in chemiluminescence‐based assay for detection of SARS‐CoV‐2 antigen. Journal of Clinical Medicine, 10(7), 1471. 10.3390/jcm10071471 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ana Laura, G.‐O. , Abraham Josué, N.‐R. , Briceida, L.‐M. , Israel, P.‐O. , Tania, A.‐F. , Nancy, M.‐R. , Lourdes, J.‐B. , Daniela, D.‐Z. , Fernando, O.‐R. , Carlos Mauricio, J.‐E. , Sergio René, B.‐P. , Irineo, R.‐T. , Horacio, M.‐G. , Oscar, M.‐C. , & Héctor, Q. (2021). Sensitivity of the molecular test in saliva for detection of COVID‐19 in pediatric patients with concurrent conditions. Frontiers in Pediatrics, 9, 642781. 10.3389/fped.2021.642781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Atieh, M. A. , Guirguis, M. , Alsabeeha, N. H. M. , & Cannon, R. D. (2021). The diagnostic accuracy of saliva testing for SARS‐CoV‐2: A systematic review and meta‐analysis. Oral Diseases. 10.1111/odi.13934 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Audigé, A. , Böni, J. , Schreiber, P. W. , Scheier, T. , Buonomano, R. , Rudiger, A. , Braun, D. L. , Eich, G. , Keller, D. I. , Hasse, B. , Berger, C. , Günthard, H. F. , Manrique, A. , Trkola, A. , & Huber, M. (2021). Reduced relative sensitivity of the Elecsys SARS‐CoV‐2 antigen assay in saliva compared to nasopharyngeal swabs. Microorganisms, 9(8), 1700. 10.3390/microorganisms9081700 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aydin, S. , Benk, I. G. , & Geckil, A. A. (2021). May viral load detected in saliva in the early stages of infection be a prognostic indicator in COVID‐19 patients? Journal of Virological Methods, 294, 114198. 10.1016/j.jviromet.2021.114198 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Azmi, I. , Faizan, M. I. , Kumar, R. , Raj Yadav, S. , Chaudhary, N. , Kumar Singh, D. , Butola, R. , Ganotra, A. , Datt Joshi, G. , Deep Jhingan, G. , Iqbal, J. , Joshi, M. C. , & Ahmad, T. (2021). A saliva‐based RNA extraction‐free workflow integrated with Cas13a for SARS‐CoV‐2 detection. Frontiers in Cellular & Infection Microbiology, 11, 632646. 10.3389/fcimb.2021.632646 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Azzi, L. , Baj, A. , Alberio, T. , Lualdi, M. , Veronesi, G. , Carcano, G. , Ageno, W. , Gambarini, C. , Maffioli, L. , Saverio, S. D. , Gasperina, D. D. , Genoni, A. P. , Premi, E. , Donati, S. , Azzolini, C. , Grandi, A. M. , Dentali, F. , Tangianu, F. , Sessa, F. , … Fasano, M. (2020a). Rapid salivary test suitable for a mass screening program to detect SARS‐CoV‐2: A diagnostic accuracy study. The Journal of Infection, 81(3), e75–e78. Retrieved from http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=medl&NEWS=N&AN=32579988 10.1016/j.jinf.2020.06.042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Azzi, L. , Carcano, G. , Gianfagna, F. , Grossi, P. , Gasperina, D. D. , Genoni, A. , Fasano, M. , Sessa, F. , Tettamanti, L. , Carinci, F. , Maurino, V. , Rossi, A. , Tagliabue, A. , & Baj, A. (2020b). Saliva is a reliable tool to detect SARS‐CoV‐2. Journal of Infection, 81(1), e45–e50. 10.1016/j.jinf.2020.04.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Babady, N. E. , McMillen, T. , Jani, K. , Viale, A. , Robilotti, E. V. , Aslam, A. , Diver, M. , Sokoli, D. , Mason, G. , Shah, M. K. , Korenstein, D. , & Kamboj, M. (2021). Performance of severe acute respiratory syndrome coronavirus 2 real‐time RT‐PCR tests on oral rinses and saliva samples. Journal of Molecular Diagnostics, 23(1), 3–9. 10.1016/j.jmoldx.2020.10.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barat, B. , Das, S. , De Giorgi, V. , Henderson, D. K. , Kopka, S. , Lau, A. F. , & Frank, K. M. (2020). Pooled saliva specimens for SARS‐CoV‐2 testing. MedRxiv: the Preprint Server for Health Sciences. 10.1101/2020.10.02.20204859 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barra, G. B. , Santa Rita, T. H. , Mesquita, P. G. , Jacomo, R. H. , & Nery, L. F. A. (2021). Overcoming supply shortage for SARS‐CoV‐2 detection by RT‐qPCR. Genes, 12(1), 90. 10.3390/genes12010090 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Basso, D. , Aita, A. , Padoan, A. , Cosma, C. , Navaglia, F. , Moz, S. , Contran, N. , Zambon, C.‐F. , Maria Cattelan, A. , & Plebani, M. (2021). Salivary SARS‐CoV‐2 antigen rapid detection: A prospective cohort study. Clinica Chimica Acta, 517, 54–59. 10.1016/j.cca.2021.02.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bhattacharya, D. , Parai, D. , Rout, U. K. , Dash, P. , Nanda, R. R. , Dash, G. C. , Kanungo, S. , Palo, S. K. , Giri, S. , Choudhary, H. R. , Kshatri, J. S. , Turuk, J. , Mishra, B. K. , Lenka, R. K. , Dash, S. , & Pati, S. (2021). Saliva for diagnosis of SARS‐CoV‐2: First report from India. Journal of Medical Virology, 93(4), 2529–2533. 10.1002/jmv.26719 [DOI] [PubMed] [Google Scholar]
- Bidkar, V. , Mishra, M. , Gade, N. , & Selvaraj, K. (2021). Conventional Naso‐oropharyngeal sampling versus self‐collected saliva samples in COVID‐19 testing. Indian Journal of Otolaryngology & Head & Neck Surgery, 1–7. 10.1007/s12070-021-02571-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Binder, R. A. , Alarja, N. A. , Robie, E. R. , Kochek, K. E. , Xiu, L. , Rocha‐Melogno, L. , Abdelgadir, A. , Goli, S. V. , Farrell, A. S. , Coleman, K. K. , Turner, A. L. , Lautredou, C. C. , Lednicky, J. A. , Lee, M. J. , Polage, C. R. , Simmons, R. A. , Deshusses, M. A. , Anderson, B. D. , & Gray, G. C. (2020). Environmental and aerosolized severe acute respiratory syndrome coronavirus 2 among hospitalized coronavirus disease 2019 patients. Journal of Infectious Diseases, 222(11), 1798–1806. 10.1093/infdis/jiaa575 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boerger, A. C. , Buckwalter, S. , Fernholz, E. C. , Jannetto, P. J. , Binnicker, M. J. , Reed, K. , Walchak, R. , Woodliff, E. , Johnson, M. , & Pritt, B. S. (2021). Evaluation of self‐collected midturbinate nasal swabs and saliva for detection of SARS‐CoV‐2 RNA. Journal of Clinical Microbiology, 59(9), e0084821. 10.1128/JCM.00848-21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Braz‐Silva, P. H. , Mamana, A. C. , Romano, C. M. , Felix, A. C. , de Paula, A. V. , Fereira, N. E. , Buss, L. F. , Tozetto‐Mendoza, T. R. , Caixeta, R. A. V. , Leal, F. E. , Grespan, R. M. Z. , Bizário, J. C. S. , Ferraz, A. B. C. , Sapkota, D. , Giannecchini, S. , To, K. K. , Doglio, A. , & Mendes‐Correa, M. C. (2020). Performance of at‐home self‐collected saliva and nasal‐oropharyngeal swabs in the surveillance of COVID‐19. Journal of Oral Microbiology, 13(1), 1858002. 10.1080/20002297.2020.1858002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Callahan, C. , Ditelberg, S. , Dutta, S. , Littlehale, N. , Cheng, A. , Kupczewski, K. , McVay, D. , Riedel, S. , Kirby, J. E. , & Arnaout, R. (2021). Saliva is comparable to nasopharyngeal swabs for molecular detection of SARS‐CoV‐2. Microbiology Spectrum, 9(1), e0016221. 10.1128/Spectrum.00162-21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carrouel, F. , Valette, M. , Perrier, H. , Bouscambert‐Duchamp, M. , Dussart, C. , Tramini, P. , & Bourgeois, D. (2021). Performance of self‐collected saliva testing compared with nasopharyngeal swab testing for the detection of SARS‐CoV‐2. Viruses, 13(5), 895. 10.3390/v13050895 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carter, L. J. , Garner, L. V. , Smoot, J. W. , Li, Y. , Zhou, Q. , Saveson, C. J. , Sasso, J. M. , Gregg, A. C. , Soares, D. J. , Beskid, T. R. , Jervey, S. R. , & Liu, C. (2020). Assay techniques and test development for COVID‐19 diagnosis. ACS Central Science, 6(5), 591–605. 10.1021/acscentsci.0c00501 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cassinari, K. , Alessandri‐Gradt, E. , Chambon, P. , Charbonnier, F. , Gracias, S. , Beaussire, L. , Alexandre, K. , Sarafan‐Vasseur, N. , Houdayer, C. , Etienne, M. , Caron, F. , Plantier, J. C. , & Frebourg, T. (2021). Assessment of multiplex digital droplet RT‐PCR as a diagnostic tool for SARS‐CoV‐2 detection in nasopharyngeal swabs and saliva samples. Clinical Chemistry, 67(5), 736–741. 10.1093/clinchem/hvaa323 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Castelain, S. , Francois, C. , Demey, B. , Aubry, A. , Lanoix, J. P. , Duverlie, G. , & Brochot, E. (2021). Comparison of nasopharyngeal and saliva swabs for the detection of RNA SARS‐CoV‐2 during mass screening (SALICOV study). New Microbiologica, 44(1), 59–61. https://proxy.library.mcgill.ca/login?url=http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=med18&AN=33582823; http://mcgill.on.worldcat.org/atoztitles/link?sid=OVID:medline&id=pmid:33582823&id=doi:&issn=1121‐7138&isbn=&volume=44&issue=1&spage=59&pages=59‐61&date=2021&title=New+Microbiologica&atitle=Comparison+of+nasopharyngeal+and+saliva+swabs+for+the+detection+of+RNA+SARS‐CoV‐2+during+mass+screening+%28SALICOV+study%29.&aulast=Castelain [PubMed] [Google Scholar]
- Caulley, L. , Shaw, J. , Corsten, M. , Hua, N. , Angel, J. B. , Poliquin, G. , Whelan, J. , Antonation, K. , & Johnson‐Obaseki, S. (2021). Salivary testing of COVID‐19: evaluation of serological testing following positive salivary results. BMC Infectious Diseases, 21(1), 410. 10.1186/s12879-021-06108-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ceron, J. , Lamy, E. , Martinez‐Subiela, S. , Lopez‐Jornet, P. , Capela‐Silva, F. , Eckersall, P. , & Tvarijonaviciute, A. (2020). Use of saliva for diagnosis and monitoring the SARS‐CoV‐2: A general perspective. Journal of Clinical Medicine, 9(5), 1491. 10.3390/jcm9051491 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chau, N. V. V. , Thanh Lam, V. , Thanh Dung, N. , Yen, L. M. , Minh, N. N. Q. , Hung, L. M. , Ngoc, N. M. , Dung, N. T. , Man, D. N. , Nguyet, L. A. , Nhat, L. T. , Nhu, L. N. T. , Ny, N. T. H. , Hong, N. T. T. , Kestelyn, E. , Dung, N. T. P. , Xuan, T. C. , Hien, T. T. , & Phong, N. T. … … (2020). The natural history and transmission potential of asymptomatic SARS‐CoV‐2 infection. Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America, 71(10), 2679–2687. 10.1093/cid/ciaa711 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen, J.‐K. , Yip, C.‐Y. , Poon, R.‐S. , Chan, K.‐H. , Cheng, V.‐C. , Hung, I.‐N. , Chan, J.‐W. , Yuen, K.‐Y. , & To, K.‐W. (2020). Evaluating the use of posterior oropharyngeal saliva in a point‐of‐care assay for the detection of SARS‐CoV‐2. Emerging Microbes & Infections, 9(1), 1356–1359. 10.1080/22221751.2020.1775133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chow, F.‐N. , Chan, T.‐Y. , Tam, A. R. , Zhao, S. , Yao, W. , Fung, J. , Cheng, F.‐K. , Lo, G.‐S. , Chu, S. , Aw‐Yong, K. L. , Tang, J.‐M. , Tsang, C.‐C. , Luk, H.‐H. , Wong, A.‐P. , Li, K.‐M. , Zhu, L. , He, Z. , Tam, E. W. T. , Chung, T.‐H. , … Lau, S.‐P. (2020). A rapid, simple, inexpensive, and mobile colorimetric assay COVID‐19‐LAMP for mass on‐site screening of COVID‐19. International Journal of Molecular Sciences, 21(15), 5380. 10.3390/ijms21155380 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corman, V. M. , Haage, V. C. , Bleicker, T. , Schmidt, M. L. , Mühlemann, B. , Zuchowski, M. , Jo, W. K. , Tscheak, P. , Möncke‐Buchner, E. , Müller, M. A. , Krumbholz, A. , Drexler, J. F. , & Drosten, C. (2021). Comparison of seven commercial SARS‐CoV‐2 rapid point‐of‐care antigen tests: a single‐centre laboratory evaluation study. The Lancet. Microbe, 2(7), e311–e319. 10.1016/s2666-5247(21)00056-24 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corman, V. M. , Landt, O. , Kaiser, M. , Molenkamp, R. , Meijer, A. , Chu, D. K. , Bleicker, T. , Brünink, S. , Schneider, J. , Schmidt, M. L. , Mulders, D. G. J. C. , Haagmans, B. L. , van der Veer, B. , van den Brink, S. , Wijsman, L. , Goderski, G. , Romette, J.‐L. , Ellis, J. , Zambon, M. , … Drosten, C. (2020). Detection of 2019 novel coronavirus (2019‐nCoV) by real‐time RT‐PCR. Euro Surveillance: Bulletin Europeen Sur Les Maladies Transmissibles = European Communicable Disease Bulletin, 25(3). 10.2807/1560-7917.ES.2020.25.3.2000045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costa, M. M. , Benoit, N. , Tissot‐Dupont, H. , Million, M. , Pradines, B. , Granjeaud, S. , & Almeras, L. (2021). Mouth washing impaired SARS‐CoV‐2 detection in saliva. Diagnostics, 11(8), 1509. 10.3390/diagnostics11081509 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Courtellemont, L. , Guinard, J. , Guillaume, C. , Giaché, S. , Rzepecki, V. , Seve, A. , Gubavu, C. , Baud, K. , Le Helloco, C. , Cassuto, G. N. , Pialoux, G. , Hocqueloux, L. , & Prazuck, T. (2021). High performance of a novel antigen detection test on nasopharyngeal specimens for diagnosing SARS‐CoV‐2 infection. Journal of Medical Virology, 93(5), 3152–3157. 10.1002/jmv.26896 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dao Thi, V. L. , Herbst, K. , Boerner, K. , Meurer, M. , Kremer, L. P. M. , Kirrmaier, D. , Freistaedter, A. , Papagiannidis, D. , Galmozzi, C. , Stanifer, M. L. , Boulant, S. , Klein, S. , Chlanda, P. , Khalid, D. , Barreto Miranda, I. , Schnitzler, P. , Kräusslich, H.‐G. , Knop, M. , & Anders, S. (2020). A colorimetric RT‐LAMP assay and LAMP‐sequencing for detecting SARS‐CoV‐2 RNA in clinical samples. Science Translational Medicine, 12(556). 10.1126/scitranslmed.abc7075 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Oliveira, C. M. , Brochi, L. , Scarpelli, L. C. , Lopes, A. C. W. , & Levi, J. E. (2021). SARS‐CoV‐2 saliva testing is a useful tool for Covid‐19 diagnosis. Journal of Virological Methods, 296, 114241. 10.1016/j.jviromet.2021.114241 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Paula Eduardo, F. , Bezinelli, L. M. , de Araujo, C. A. R. , Moraes, J. V. V. , Birbrair, A. , Pinho, J. R. R. , Hamerschlak, N. , Al‐Hashimi, I. , & Heller, D. (2021). Self‐collected unstimulated saliva, oral swab, and nasopharyngeal swab specimens in the detection of SARS‐CoV‐2. Clinical Oral Investigations, 13, 13. 10.1007/s00784-021-04129-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Puig, H. , Lee, R. A. , Najjar, D. , Tan, X. , Soenksen, L. R. , Angenent‐Mari, N. M. , Donghia, N. M. , Weckman, N. E. , Ory, A. , Ng, C. F. , Nguyen, P. Q. , Mao, A. S. , Ferrante, T. C. , Lansberry, G. , Sallum, H. , Niemi, J. , & Collins, J. J. (2021). Minimally instrumented SHERLOCK (miSHERLOCK) for CRISPR‐based point‐of‐care diagnosis of SARS‐CoV‐2 and emerging variants. Science Advances, 7(32), 08. 10.1126/sciadv.abh2944 [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Santi, C. , Jacob, B. , Kroich, P. , Doyle, S. , Ward, R. , Li, B. , Donnelly, O. , Dykes, A. , Neelakant, T. , Neary, D. , McGuinness, R. , Cafferkey, J. , Ryan, K. , Quadu, V. , McGrogan, K. , Garcia Leon, A. , Mallon, P. , Fitzpatrick, F. , Humphreys, H. , … Cavalleri, G. L. (2021). Concordance between PCR‐based extraction‐free saliva and nasopharyngeal swabs for SARS‐CoV‐2 testing. HRB Open Research, 4, 85. 10.12688/hrbopenres.13353.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dogan, O. A. , Kose, B. , Agaoglu, N. B. , Yildiz, J. , Alkurt, G. , Demirkol, Y. K. , Irvem, A. , Doganay, G. D. , & Doganay, L. (2021). Does sampling saliva increase detection of SARS‐CoV‐2 by RT‐PCR? Comparing saliva with oro‐nasopharyngeal swabs. Journal of Virological Methods, 290, 114049. 10.1016/j.jviromet.2020.114049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Echavarria, M. , Reyes, N. S. , Rodriguez, P. E. , Ypas, M. , Ricarte, C. , Rodriguez, M. P. , Perez, M. G. , Seoane, A. , Martinez, A. , Videla, C. , Stryjewski, M. E. , & Carballal, G. (2021). Self‐collected saliva for SARS‐CoV‐2 detection: A prospective study in the emergency room. Journal of Medical Virology, 93(5), 3268–3272. 10.1002/jmv.26839 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elledge, S. K. , Zhou, X. X. , Byrnes, J. R. , Martinko, A. , Lui, I. , Pance, K. , Lim, S. A. , Glasgow, J. E. , Glasgow, A. A. , Turcios, K. , Iyer, N. S. , Torres, L. , Peluso, M. J. , Henrich, T. J. , Wang, T. T. , Tato, C. M. , Leung, K. K. , Greenhouse, B. , & Wells, J. A. (2020). Engineering luminescent biosensors for point‐of‐care SARS‐CoV‐2 antibody detection. MedRxiv: The Preprint Server for Health Sciences. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=prem&NEWS=N&AN=32839788 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fan, G. , Qin, X. , Streblow, D. N. , Hoyos, C. M. , & Hansel, D. E. (2021). Comparison of SARS‐CoV‐2 PCR‐based detection using saliva or nasopharyngeal swab specimens in asymptomatic populations. Microbiology Spectrum, 9(1), e0006221. 10.1128/Spectrum.00062-21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Faustini, S. E. , Jossi, S. E. , Perez‐Toledo, M. , Shields, A. M. , Allen, J. D. , Watanabe, Y. , Newby, M. L. , Cook, A. , Willcox, C. R. , Salim, M. , Goodall, M. , Heaney, J. L. , Marcial‐Juarez, E. , Morley, G. L. , Torlinska, B. , Wraith, D. C. , Veenith, T. V. , Harding, S. , Jolles, S. , … Richter, A. G. (2021). Development of a high‐sensitivity ELISA detecting IgG, IgA and IgM antibodies to the SARS‐CoV‐2 spike glycoprotein in serum and saliva. Immunology, 164(1), 135–147. 10.1111/imm.13349 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fernandes, P. A. D. C. , Ferreira, F. A. D. C. , Morais, O. M. , Ramos, C. M. T. , Fernandes, É. M. R. , Rocha, S. A. A. D. , Rocha, R. J. A. , Monteiro, V. J. P. , Vilar, P. S. G. , Romão, A. M. , & Alves, M. R. A. (2021). Performance of saliva as a specimen to detect SARS‐CoV‐2. Journal of Clinical Virology, 142, 104913. 10.1016/j.jcv.2021.104913 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fernández‐González, M. , Agulló, V. , de la Rica, A. , Infante, A. , Carvajal, M. , García, J. A. , Gonzalo‐Jiménez, N. , Cuartero, C. , Ruiz‐García, M. , de Gregorio, C. , Sánchez, M. , Masiá, M. , & Gutiérrez, F. (2021). Performance of saliva specimens for the molecular detection of SARS‐CoV‐2 in the community setting: does sample collection method matter? Journal of Clinical Microbiology, 59(4), 19. 10.1128/JCM.03033-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fougère, Y. , Schwob, J. M. , Miauton, A. , Hoegger, F. , Opota, O. , Jaton, K. , Brouillet, R. , Greub, G. , Genton, B. , Gehri, M. , Taddeo, I. , D’Acremont, V. , & Asner, S. A. (2021). Performance of RT‐PCR on Saliva specimens compared with nasopharyngeal swabs for the detection of SARS‐CoV‐2 in children: A prospective comparative clinical trial. Pediatric Infectious Disease Journal, 40(8), e300–e304. 10.1097/INF.0000000000003198 [DOI] [PubMed] [Google Scholar]
- Fukumoto, T. , Iwasaki, S. , Fujisawa, S. , Hayasaka, K. , Sato, K. , Oguri, S. , Taki, K. , Nakakubo, S. , Kamada, K. , Yamashita, Y. U. , Konno, S. , Nishida, M. , Sugita, J. , & Teshima, T. (2020). Efficacy of a novel SARS‐CoV‐2 detection kit without RNA extraction and purification. International Journal of Infectious Diseases, 98, 16–17. 10.1016/j.ijid.2020.06.074 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gable, P. , Huang, J. Y. , Gilbert, S. E. , Bollinger, S. , Lyons, A. K. , Sabour, S. , Surie, D. , Biedron, C. , Haney, T. , Beshearse, E. , Gregory, C. J. , Seely, K. A. , Clemmons, N. S. , Patil, N. , Kothari, A. , Gulley, T. , Garner, K. , Anderson, K. , Thornburg, N. J. , … Ata Ur Rasheed, M. (2021). A comparison of less invasive severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) diagnostic specimens in nursing home residents‐Arkansas, June‐August 2020. Clinical Infectious Diseases, 73(Suppl 1), S58–S64. 10.1093/cid/ciab310 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ganguli, A. , Mostafa, A. , Berger, J. , Lim, J. , Araud, E. , Baek, J. , Stewart de Ramirez, S. A. , Baltaji, A. , Roth, K. , Aamir, M. , Aedma, S. , Mady, M. , Mahajan, P. , Sathe, S. , Johnson, M. , White, K. , Kumar, J. , Valera, E. , & Bashir, R. (2021). Reverse transcription loop‐mediated isothermal amplification assay for ultrasensitive detection of SARS‐CoV‐2 in saliva and viral transport medium clinical samples. Analytical Chemistry, 93(22), 7797–7807. 10.1021/acs.analchem.0c05170 [DOI] [PubMed] [Google Scholar]
- Gaur, R. , Verma, D. K. , Mohindra, R. , Goyal, K. , Gupta, S. , Singla, V. , Sahni, V. , Ghosh, A. , Soni, R. K. , Bhalla, A. , Gauba, K. , & Singh, M. P. (2021). Buccal swabs as non‐invasive specimens for detection of severe acute respiratory syndrome coronavirus‐2. Journal of International Medical Research, 49(5), 3000605211016996. 10.1177/03000605211016996 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldfarb, D. M. , Tilley, P. , Al‐Rawahi, G. N. , Srigley, J. A. , Ford, G. , Pedersen, H. , Pabbi, A. , Hannam‐Clark, S. , Charles, M. , Dittrick, M. , Gadkar, V. J. , Pernica, J. M. , & Hoang, L. M. N. (2021). Self‐collected saline gargle samples as an alternative to health care worker‐collected nasopharyngeal swabs for COVID‐19 diagnosis in outpatients. Journal of Clinical Microbiology, 59(4), 19. 10.1128/JCM.02427-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gonçalves, C. C. A. , Barroso, S. P. C. , Herlinger, A. L. , Galliez, R. D. M. , de Almeida, T. B. , Boullosa, L. T. , Nascimento, E. R. D. S. , de Almeida, J. M. , da Costa, R. M. D. S. C. , da Paixão, T. M. , Couceiro, J. N. D. S. S. , Frauches, T. S. , de Souza Jr, W. R. , Costa, A. R. , Faffe, D. S. , Leitão, I. D. C. , da Silva, B. O. , de Lira, G. S. A. , de Almeida, I. L. C. , … Tanuri, A. (2021). COVID‐19 diagnosis by RT‐qPCR in alternative specimens. Memorias do Instituto Oswaldo Cruz, 116, e210085. 10.1590/0074-02760210085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Griesemer, S. B. , Van Slyke, G. , Ehrbar, D. , Strle, K. , Yildirim, T. , Centurioni, D. A. , Walsh, A. C. , Chang, A. K. , Waxman, M. J. , & St. George, K. (2021). Evaluation of specimen types and saliva stabilization solutions for SARS‐CoV‐2 testing. Journal of Clinical Microbiology, 59(5), 20. 10.1128/JCM.01418-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guclu, E. , Koroglu, M. , Yurumez, Y. , Toptan, H. , Kose, E. , Guneysu, F. , & Karabay, O. (2020). Comparison of saliva and oro‐nasopharyngeal swab sample in the molecular diagnosis of COVID‐19. Revista Da Associacao Medica Brasileira, 66(8), 1116–1121. 10.1590/1806-9282.66.8.1116 [DOI] [PubMed] [Google Scholar]
- Guest, J. L. , Sullivan, P. S. , Valentine‐Graves, M. , Valencia, R. , Adam, E. , Luisi, N. , Nakano, M. , Guarner, J. , del Rio, C. , Sailey, C. , Goedecke, Z. , Siegler, A. J. , & Sanchez, T. H. (2020). Suitability and sufficiency of telehealth clinician‐observed, participant‐collected samples for SARS‐CoV‐2 testing: The iCollect cohort pilot study. JMIR Public Health and Surveillance, 6(2), e19731. 10.2196/19731 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gupta, A. , Mittal, A. , Dhakad, S. , Brijwal, M. , Soneja, M. , Srigyan, D. , & Wig, N. (2021). Gargle lavage & saliva: Feasible & cheaper alternatives to nasal & throat swabs for diagnosis of COVID‐19. Indian Journal of Medical Research, 20, 20. 10.4103/ijmr.IJMR_4209_20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamid, H. , Khurshid, Z. , Adanir, N. , Zafar, M. S. , & Zohaib, S. (2020). COVID‐19 pandemic and role of human saliva as a testing biofluid in point‐of‐care technology. European Journal of Dentistry, 14(S 01), S123–S129. 10.1055/s-0040-1713020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Han, P. , & Ivanovski, S. (2020). Saliva‐friend and foe in the COVID‐19 outbreak. Diagnostics, 10(5), 290. 10.3390/diagnostics10050290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanege, F. M. , Kocoglu, E. , Kalcioglu, M. T. , Celik, S. , Cag, Y. , Esen, F. , & Agalar, C. (2021). SARS‐CoV‐2 presence in the saliva, tears, and cerumen of COVID‐19 patients. Laryngoscope, 131(5), E1677–E1682. 10.1002/lary.29218 [DOI] [PubMed] [Google Scholar]
- Hanson, K. E. , Barker, A. P. , Hillyard, D. R. , Gilmore, N. , Barrett, J. W. , Orlandi, R. R. , & Shakir, S. M. (2020). Self‐collected anterior nasal and saliva specimens versus healthcare worker‐collected nasopharyngeal swabs for the molecular detection of SARS‐CoV‐2. Journal of Clinical Microbiology, 58(11), e01824‐20. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=medp&NEWS=N&AN=32817233 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herrera, L. A. , Hidalgo‐Miranda, A. , Reynoso‐Noverón, N. , Meneses‐García, A. A. , Mendoza‐Vargas, A. , Reyes‐Grajeda, J. P. , Vadillo‐Ortega, F. , Cedro‐Tanda, A. , Peñaloza, F. , Frías‐Jimenez, E. , Arriaga‐Canon, C. , Ruiz, R. , Angulo, O. , López‐Villaseñor, I. , Amador‐Bedolla, C. , Vilar‐Compte, D. , Cornejo, P. , Cisneros‐Villanueva, M. , Hurtado‐Cordova, E. , … Escobar‐Escamilla, N. (2021). Saliva is a reliable and accessible source for the detection of SARS‐CoV‐2. International Journal of Infectious Diseases, 105, 83–90. 10.1016/j.ijid.2021.02.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hitzenbichler, F. , Bauernfeind, S. , Salzberger, B. , Schmidt, B. , & Wenzel, J. J. (2021). Comparison of throat washings, nasopharyngeal swabs and oropharyngeal swabs for detection of SARS‐CoV‐2. Viruses, 13(4), 653. 10.3390/v13040653 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huber, M. , Schreiber, P. W. , Scheier, T. , Audigé, A. , Buonomano, R. , Rudiger, A. , Braun, D. L. , Eich, G. , Keller, D. I. , Hasse, B. , Böni, J. , Berger, C. , Günthard, H. F. , Manrique, A. , & Trkola, A. (2021). High efficacy of saliva in detecting SARS‐CoV‐2 by RT‐PCR in adults and children. Microorganisms, 9(3), 642. 10.3390/microorganisms9030642 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hung, D.‐L. , Li, X. , Chiu, K.‐Y. , Yip, C.‐Y. , To, K.‐W. , Chan, J.‐W. , Sridhar, S. , Chung, T.‐H. , Lung, K.‐C. , Liu, R.‐T. , Kwan, G.‐W. , Hung, I.‐N. , Cheng, V.‐C. , & Yuen, K.‐Y. (2020). Early‐morning vs spot posterior oropharyngeal saliva for diagnosis of sars‐cov‐2 infection: implication of timing of specimen collection for community‐wide screening. Open Forum Infectious Diseases, 7(6), ofaa210. 10.1093/ofid/ofaa210 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ishii, T. , Sasaki, M. , Yamada, K. , Kato, D. , Osuka, H. , Aoki, K. , Morita, T. , Ishii, Y. , & Tateda, K. (2021). Immunochromatography and chemiluminescent enzyme immunoassay for COVID‐19 diagnosis. Journal of Infection & Chemotherapy, 27(6), 915–918. 10.1016/j.jiac.2021.02.025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Isho, B. , Abe, K. T. , Zuo, M. , Jamal, A. J. , Rathod, B. , Wang, J. H. , Li, Z. , Chao, G. , Rojas, O. L. , Bang, Y. M. , Pu, A. , Christie‐Holmes, N. , Gervais, C. , Ceccarelli, D. , Samavarchi‐Tehrani, P. , Guvenc, F. , Budylowski, P. , Li, A. , Paterson, A. , … Gingras, A.‐C. (2020). Persistence of serum and saliva antibody responses to SARS‐CoV‐2 spike antigens in COVID‐19 patients. Science Immunology, 5(52), 08. 10.1126/sciimmunol.abe5511 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iwasaki, S. , Fujisawa, S. , Nakakubo, S. , Kamada, K. , Yamashita, Y. U. , Fukumoto, T. , Sato, K. , Oguri, S. , Taki, K. , Senjo, H. , Sugita, J. , Hayasaka, K. , Konno, S. , Nishida, M. , & Teshima, T. (2020). Comparison of SARS‐CoV‐2 detection in nasopharyngeal swab and saliva. Journal of Infection, 81(2), e145–e147. 10.1016/j.jinf.2020.05.071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jacobs, J. , Kühne, V. , Lunguya, O. , Affolabi, D. , Hardy, L. , & Vandenberg, O. (2020). Implementing COVID‐19 (SARS‐CoV‐2) rapid diagnostic tests in Sub‐Saharan Africa: A review. Frontiers in Medicine, 7, 557797. 10.3389/fmed.2020.557797 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jamal, A. J. , Mozafarihashjin, M. , Coomes, E. , Anceva‐Sami, S. , Barati, S. , Crowl, G. , Faheem, A. , Farooqi, L. , Kandel, C. E. , Khan, S. , Li, A. X. , Mistry, H. , Paterson, A. , Plenderleith, S. , Prost, K. , Poutanen, S. , Powis, J. , Schryer, R. , Taylor, M. , … Mubareka, S. (2021a). Sensitivity of midturbinate versus nasopharyngeal swabs for the detection of severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2). Infection Control & Hospital Epidemiology, 42(8), 1001–1003. 10.1017/ice.2020.1326 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jamal, A. J. , Mozafarihashjin, M. , Coomes, E. , Powis, J. , Li, A. X. , Paterson, A. , Anceva‐Sami, S. , Barati, S. , Crowl, G. , Faheem, A. , Farooqi, L. , Khan, S. , Prost, K. , Poutanen, S. , Taylor, M. , Yip, L. , Zhong, X. Z. , McGeer, A. J. , Mubareka, S. , … Walmsley, S. (2020). Sensitivity of nasopharyngeal swabs and saliva for the detection of severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2). Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America, 72(6), 1064–1066. 10.1093/cid/ciaa848 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jamal, A. J. , Mozafarihashjin, M. , Coomes, E. , Powis, J. , Li, A. X. , Paterson, A. , Anceva‐Sami, S. , Barati, S. , Crowl, G. , Faheem, A. , Farooqi, L. , Khan, S. , Prost, K. , Poutanen, S. , Taylor, M. , Yip, L. , Zhong, X. Z. , McGeer, A. J. , Mubareka, S. , … Walmsley, S. (2021b). Sensitivity of nasopharyngeal swabs and saliva for the detection of severe acute respiratory syndrome coronavirus 2. Clinical Infectious Diseases, 72(6), 1064–1066. 10.1093/cid/ciaa848 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Javaid, M. A. , Ahmed, A. S. , Durand, R. , & Tran, S. D. (2016). Saliva as a diagnostic tool for oral and systemic diseases. Journal of Oral Biology and Craniofacial Research, 6(1), 67–76. 10.1016/j.jobcr.2015.08.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson, A. J. , Zhou, S. , Hoops, S. L. , Hillmann, B. , Schomaker, M. , Kincaid, R. , Daniel, J. , Beckman, K. , Gohl, D. M. , Yohe, S. , Knights, D. , & Nelson, A. C. (2021). Saliva testing is accurate for early‐stage and presymptomatic COVID‐19. Microbiology Spectrum, 9(1), e0008621. 10.1128/Spectrum.00086-21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Justo, A. F. O. , Bueno, M. S. , Barbosa, G. R. , Perosa, A. H. , Carvalho, J. M. , & Bellei, N. (2021). Comparison of viral load between saliva and nasopharyngeal swabs for SARS‐CoV2: The role of days of symptoms onset on diagnosis. Memorias do Instituto Oswaldo Cruz, 116, e210018. 10.1590/0074-02760210018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kandel, C. , Zheng, J. , McCready, J. , Serbanescu, M. , Racher, H. , Desaulnier, M. , Powis, J. , Vojdani, K. , Finlay, L. , Sheldrake, E. , Vermeiren, C. , Katz, K. , McGeer, A. , Kozak, R. , & Goneau, L. (2020). Detection of SARS‐CoV‐2 from saliva as compared to nasopharyngeal swabs in outpatients. Viruses, 12(11), 1314. 10.3390/v12111314 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keuning, M. W. , Grobben, M. , de Groen, A.‐E. , Berman‐de Jong, E. P. , Bijlsma, M. W. , Cohen, S. , Felderhof, M. , de Groof, F. , Molanus, D. , Oeij, N. , Rijpert, M. , van Eijk, H. W. M. , Koen, G. , van der Straten, K. , Oomen, M. , Visser, R. , Linty, F. , Steenhuis, M. , Vidarsson, G. , … Pajkrt, D. (2021). Saliva SARS‐CoV‐2 antibody prevalence in children. Microbiology Spectrum, 9(2), e0073121. 10.1128/Spectrum.00731-21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khurshid, Z. (2018). Salivary point‐of‐care technology. European Journal of Dentistry, 12(1), 1–2. 10.4103/ejd.ejd_376_17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khurshid, Z. , Asiri, F. Y. I. , & Al Wadaani, H. (2020). Human saliva: Non‐invasive fluid for detecting novel coronavirus (2019‐nCoV). International Journal of Environmental Research & Public Health [electronic Resource], 17(7), 2225. 10.3390/ijerph17072225 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim, S. E. , Lee, J. Y. , Lee, A. , Kim, S. , Park, K.‐H. , Jung, S.‐I. , Kang, S.‐J. , Oh, T. H. , Kim, U. J. , Lee, S. Y. , Kee, S.‐J. , & Jang, H.‐C. (2020). Viral load kinetics of SARS‐CoV‐2 infection in saliva in Korean patients: A prospective multi‐center comparative study. Journal of Korean Medical Science, 35(31), e287. 10.3346/jkms.2020.35.e287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kobayashi, G. S. , Brito, L. A. , Moreira, D. D. P. , Suzuki, A. M. , Hsia, G. S. P. , Pimentel, L. F. , de Paiva, A. P. B. , Dias, C. R. , Lourenço, N. C. V. , Oliveira, B. A. , Manuli, E. R. , Corral, M. A. , Cavaçana, N. , Mitne‐Neto, M. , Sales, M. M. , Dell’ Aquila, L. P. , Filho, A. R. , Parrillo, E. F. , Mendes‐Corrêa, M. C. , … Passos‐Bueno, M. R. (2021). A novel saliva RT‐LAMP workflow for rapid identification of COVID‐19 cases and restraining viral spread. Diagnostics, 11(8), 1400. 10.3390/diagnostics11081400 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kojima, N. , Turner, F. , Slepnev, V. , Bacelar, A. , Deming, L. , Kodeboyina, S. , & Klausner, J. D. (2020). Self‐collected oral fluid and nasal swab specimens demonstrate comparable sensitivity to clinician‐collected nasopharyngeal swab specimens for the detection of SARS‐CoV‐2. Clinical Infectious Diseases, 19, 19. 10.1093/cid/ciaa1589 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ku, C. W. , Shivani, D. , Kwan, J. Q. T. , Loy, S. L. , Erwin, C. , Ko, K. K. K. , Ng, X. W. , Oon, L. , Thoon, K. C. , Kalimuddin, S. , & Chan, J. K. Y. (2021). Validation of self‐collected buccal swab and saliva as a diagnostic tool for COVID‐19. International Journal of Infectious Diseases, 104, 255–261. 10.1016/j.ijid.2020.12.080 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kubina, R. , & Dziedzic, A. (2020). Molecular and serological tests for COVID‐19. A comparative review of SARS‐CoV‐2 coronavirus laboratory and point‐of‐care diagnostics. Diagnostics, 10(6), 434. 10.3390/diagnostics10060434 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kucirka, L. M. , Lauer, S. A. , Laeyendecker, O. , Boon, D. , & Lessler, J. (2020). Variation in false‐negative rate of reverse transcriptase polymerase chain reaction–based SARS‐CoV‐2 tests by time since exposure. Annals of Internal Medicine, 173(4), 262–267. 10.7326/M20-1495 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Labbé, A.‐C. , Benoit, P. , Gobeille Paré, S. , Coutlée, F. , Lévesque, S. , Bestman‐Smith, J. , Dumaresq, J. , Lavallée, C. , Houle, C. , Martin, P. , Mak, A. , Gervais, P. , Langevin, S. , Jacob‐Wagner, M. , Gagnon, S. , St‐Hilaire, M. , Lussier, N. , Yechouron, A. , Roy, D. , … Fafard, J. (2021). Comparison of saliva with oral and nasopharyngeal swabs for SARS‐CoV‐2 detection on various commercial and laboratory‐developed assays. Journal of Medical Virology, 93(9), 5333–5338. 10.1002/jmv.27026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landry, M. L. , Criscuolo, J. , & Peaper, D. R. (2020). Challenges in use of saliva for detection of SARS CoV‐2 RNA in symptomatic outpatients. Journal of Clinical Virology, 130, 104567. 10.1016/j.jcv.2020.104567 [DOI] [PMC free article] [PubMed] [Google Scholar]
- LeBlanc, J. J. , Pettipas, J. , Di Quinzio, M. , Hatchette, T. F. , & Patriquin, G. (2021). Reliable detection of SARS‐CoV‐2 with patient‐collected swabs and saline gargles: A three‐headed comparison on multiple molecular platforms. Journal of Virological Methods, 295, 114184. 10.1016/j.jviromet.2021.114184 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leung, E.‐C.‐M. , Chow, V.‐C.‐Y. , Lee, M.‐K.‐P. , & Lai, R.‐W.‐M. (2020). Deep throat saliva as an alternative diagnostic specimen type for the detection of SARS‐CoV‐2. Journal of Medical Virology, 93(1), 533–536. 10.1002/jmv.26258 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leung, E. C. , Chow, V. C. , Lee, M. K. , & Lai, R. W. (2021). Deep throat saliva as an alternative diagnostic specimen type for the detection of SARS‐CoV‐2. Journal of Medical Virology, 93(1), 533–536. 10.1002/jmv.26258 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu, T. , Hsiung, J. , Zhao, S. U. , Kost, J. , Sreedhar, D. , Hanson, C. V. , Olson, K. , Keare, D. , Chang, S. T. , Bliden, K. P. , Gurbel, P. A. , Tantry, U. S. , Roche, J. , Press, C. , Boggs, J. , Rodriguez‐Soto, J. P. , Montoya, J. G. , Tang, M. , & Dai, H. (2020). Quantification of antibody avidities and accurate detection of SARS‐CoV‐2 antibodies in serum and saliva on plasmonic substrates. Nature Biomedical Engineering, 4(12), 1188–1196. 10.1038/s41551-020-00642-4 [DOI] [PubMed] [Google Scholar]
- MacMullan, M. A. , Chellamuthu, P. , Mades, A. , Das, S. , Turner, F. , Slepnev, V. I. , & Ibrayeva, A. (2021). Detection of SARS‐CoV‐2 antibodies in oral fluid obtained using a rapid collection device. Journal of Clinical Microbiology, 59(2), 21. 10.1128/JCM.02510-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacMullan, M. A. , Ibrayeva, A. , Trettner, K. , Deming, L. , Das, S. , Tran, F. , Moreno, J. R. , Casian, J. G. , Chellamuthu, P. , Kraft, J. , Kozak, K. , Turner, F. E. , Slepnev, V. I. , & Le Page, L. M. (2020). ELISA detection of SARS‐CoV‐2 antibodies in saliva. Scientific Reports, 10(1), 20818. 10.1038/s41598-020-77555-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mahmoud, S. A. , Ganesan, S. , Ibrahim, E. , Thakre, B. , Teddy, J. G. , Raheja, P. , & Abbas, W. Z. (2021). Evaluation of RNA extraction‐free method for detection of SARS‐CoV‐2 in salivary samples for mass screening for COVID‐19. BioMed Research International, 2021, 5568350. 10.1155/2021/5568350 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martínez‐Fleta, P. , Alfranca, A. , González‐Álvaro, I. , Casasnovas, J. M. , Fernández‐Soto, D. , Esteso, G. , Cáceres‐Martell, Y. , Gardeta, S. , López‐Sanz, C. , Prat, S. , Mateu‐Albero, T. , Gabrie, L. , López‐Granados, E. , Sánchez‐Madrid, F. , Reyburn, H. T. , Rodríguez Frade, J. M. , & Valés‐Gómez, M. (2020). SARS‐CoV‐2 cysteine‐like protease antibodies can be detected in serum and saliva of COVID‐19‐seropositive individuals. Journal of Immunology, 205(11), 3130–3140. 10.4049/jimmunol.2000842 [DOI] [PubMed] [Google Scholar]
- Marx, G. E. , Biggerstaff, B. J. , Nawrocki, C. C. , Totten, S. E. , Travanty, E. A. , Burakoff, A. W. , Scott, T. , De Hey, J.‐V. , Carlson, J. J. , Wendel, K. A. , Harcourt, J. L. , Tamin, A. , Thomas, J. D. , Rowan, S. E. , Matzinger, S. R. , Hudziec, M. , Hetherington‐Rauth, M. C. , Pysnack, N. J. , Delmonico, C. , … Thornburg, N. (2021). Detection of severe acute respiratory syndrome Coronavirus 2 on self‐collected saliva or anterior nasal specimens compared with healthcare personnel‐collected nasopharyngeal specimens. Clinical Infectious Diseases, 73(Suppl 1), S65–S73. 10.1093/cid/ciab330 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Masse, S. , Bonnet, C. , Vilcu, A.‐M. , Benamar, H. , Swital, M. , van der Werf, S. , Carrat, F. , Hanslik, T. , Blanchon, T. , & Falchi, A. (2021). Are posterior oropharyngeal saliva specimens an acceptable alternative to nasopharyngeal sampling for the monitoring of SARS‐CoV‐2 in primary‐care settings? Viruses, 13(5), 761. 10.3390/v13050761 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matic, N. , Stefanovic, A. , Leung, V. , Lawson, T. , Ritchie, G. , Li, L. , Champagne, S. , Romney, M. G. , & Lowe, C. F. (2021). Practical challenges to the clinical implementation of saliva for SARS‐CoV‐2 detection. European Journal of Clinical Microbiology & Infectious Diseases, 40(2), 447–450. 10.1007/s10096-020-04090-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCormick‐Baw, C. , Morgan, K. , Gaffney, D. , Cazares, Y. , Jaworski, K. , Byrd, A. , Molberg, K. , & Cavuoti, D. (2020). Saliva as an alternate specimen source for detection of SARS‐CoV‐2 in symptomatic patients using cepheid xpert xpress SARS‐CoV‐2. Journal of Clinical Microbiology, 58(8), 23. 10.1128/JCM.01109-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mendoza, R. P. , Bi, C. , Cheng, H.‐T. , Gabutan, E. , Pagaspas, G. J. , Khan, N. , Hoxie, H. , Hanna, S. , Holmes, K. , Gao, N. , Lewis, R. , Wang, H. , Neumann, D. , Chan, A. , Takizawa, M. , Lowe, J. , Chen, X. , Kelly, B. , Asif, A. , … Premsrirut, P. K. (2021). Implementation of a pooled surveillance testing program for asymptomatic SARS‐CoV‐2 infections in K‐12 schools and universities. EClinicalMedicine, 38, 101028. 10.1016/j.eclinm.2021.101028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mestdagh, P. , Gillard, M. , Dhillon, S. K. , Pirnay, J.‐P. , Poels, J. , Hellemans, J. , Hutse, V. , Vermeiren, C. , Boutier, M. , De Wever, V. , Soentjens, P. , Djebara, S. , Malonne, H. , André, E. , Arbyn, M. , Smeraglia, J. , & Vandesompele, J. O. (2021). Evaluating diagnostic accuracy of saliva sampling methods for severe acute respiratory syndrome coronavirus 2 reveals differential sensitivity and association with viral load. Journal of Molecular Diagnostics, 23(10), 1249–1258. 10.1016/j.jmoldx.2021.07.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Migueres, M. , Vellas, C. , Abravanel, F. , Da Silva, I. , Dimeglio, C. , Ferrer, V. , Raymond, S. , Mansuy, J.‐M. , & Izopet, J. (2021). Testing individual and pooled saliva samples for sars‐cov‐2 nucleic acid: A prospective study. Diagnostic Microbiology & Infectious Disease, 101(3), 115478. 10.1016/j.diagmicrobio.2021.115478 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mohd Thabit, A. A. , Peariasamy, K. M. , Kuan, P. X. , Fern Ying, D. K. , Nheu, N. , Cyncynatus, C. , Mu'iz Arifin, M. A. , Shamsuddin, A. N. , Yamin, M. A. , Mohd Padzil, M. A. , Rajasekaram, G. , Giddy, M. , Sivaneson, S. , Lakhbeer Singh, H. K. , Azman, A. , Hassan, A. H. , & Chidambaram, S. K. (2021). Diagnostic accuracy of fresh drooled saliva for SARS‐CoV‐2 in travelers. Travel Medicine & Infectious Disease, 43, 102144. 10.1016/j.tmaid.2021.102144 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moreno‐Contreras, J. , Espinoza, M. A. , Sandoval‐Jaime, C. , Cantu‐Cuevas, M. A. , Baron‐Olivares, H. , Ortiz‐Orozco, O. D. , Muñoz‐Rangel, A. V. , Hernández‐De la Cruz, M. , Eroza‐Osorio, C. M. , Arias, C. F. , & Lopez, S. (2020). Saliva sampling and its direct lysis, an excellent option to increase the number of SARS CoV2 diagnostic tests in settings with supply shortages. Journal of Clinical Microbiology, 58(10), e01659‐20. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=medp&NEWS=N&AN=32703816 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nacher, M. , Mergeay‐Fabre, M. , Blanchet, D. , Benois, O. , Pozl, T. , Mesphoule, P. , Sainte‐Rose, V. , Vialette, V. , Toulet, B. , Moua, A. , Saout, M. , Simon, S. , Guidarelli, M. , Galindo, M. , Biche, B. , Faurous, W. , Chaizemartin, L. , Fahrasmane, A. , Rochemont, D. , … Demar, M. (2021a). Diagnostic accuracy and acceptability of molecular diagnosis of COVID‐19 on saliva samples relative to nasopharyngeal swabs in tropical hospital and extra‐hospital contexts: The COVISAL study. PLoS One [electronic Resource], 16(9), e0257169. 10.1371/journal.pone.0257169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nacher, M. , Mergeay‐Fabre, M. , Blanchet, D. , Benoit, O. , Pozl, T. , Mesphoule, P. , Sainte‐Rose, V. , Vialette, V. , Toulet, B. , Moua, A. , Saout, M. , Simon, S. , Guidarelli, M. , Galindo, M. , Biche, B. , Faurous, W. , Chaizemartin, L. , Fahrasmane, A. , Rochemont, D. , … Demar, M. (2021b). Prospective comparison of saliva and nasopharyngeal swab sampling for mass screening for COVID‐19. Frontiers in Medicine, 8, 621160. 10.3389/fmed.2021.621160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nagura‐Ikeda, M. , Imai, K. , Tabata, S. , Miyoshi, K. , Murahara, N. , Mizuno, T. , Horiuchi, M. , Kato, K. , Imoto, Y. , Iwata, M. , Mimura, S. , Ito, T. , Tamura, K. , & Kato, Y. (2020). Clinical evaluation of self‐collected saliva by quantitative reverse transcription‐PCR (RT‐qPCR), direct RT‐qPCR, reverse transcription‐loop‐mediated isothermal amplification, and a rapid antigen test to diagnose COVID‐19. Journal of Clinical Microbiology, 58(9), 24. 10.1128/JCM.01438-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Norizuki, M. , Hachiya, M. , Motohashi, A. , Moriya, A. , Mezaki, K. , Kimura, M. , Sugiura, W. , Akashi, H. , & Umeda, T. (2021). Effective screening strategies for detection of asymptomatic COVID‐19 travelers at airport quarantine stations: Exploratory findings in Japan. Global Health & Medicine, 3(2), 107–111. 10.35772/ghm.2020.01109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okamaoto, K. , Shirato, K. , Nao, N. , Saito, S. , Kageyama, T. , Hasegawa, H. , Suzuki, T. , Matsuyama, S. , & Takeda, M. (2020). Assessment of real‐time RT‐PCR kits for SARS‐CoV‐2 detection. Japanese Journal of Infectious Diseases, 73(5), 366–368. 10.7883/yoken.JJID.2020.108 [DOI] [PubMed] [Google Scholar]
- Oliver, J. , Tosif, S. , Lee, L.‐Y. , Costa, A.‐M. , Bartel, C. , Last, K. , Clifford, V. , Daley, A. , Allard, N. , Orr, C. , Nind, A. , Alexander, K. , Meagher, N. , Sait, M. , Ballard, S. A. , Williams, E. , Bond, K. , Williamson, D. A. , Crawford, N. W. , & Gibney, K. B. (2021). Adding saliva testing to oropharyngeal and deep nasal swab testing increases PCR detection of SARS‐CoV‐2 in primary care and children. Medical Journal of Australia, 215(6), 273–278. 10.5694/mja2.51188 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ota, K. , Yanagihara, K. , Sasaki, D. , Kaku, N. , Uno, N. , Sakamoto, K. , Kosai, K. , Miyazaki, T. , Hasegawa, H. , Fujita, A. , Tashiro, M. , Tanaka, T. , Izumikawa, K. , Ariyoshi, K. , Mukae, H. , Yasuda, J. , Morita, K. , & Kohno, S. (2021). Detection of SARS‐CoV‐2 using qRT‐PCR in saliva obtained from asymptomatic or mild COVID‐19 patients, comparative analysis with matched nasopharyngeal samples. PLoS One [electronic Resource], 16(6), e0252964. 10.1371/journal.pone.0252964 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palikša, S. , Lopeta, M. , Belevičius, J. , Kurmauskaitė, V. , Ašmenavičiūtė, I. , Pereckaitė, L. , Vitkauskienė, A. , Baliūtytė, I. , Valentaitė, M. , Mickienė, A. , & Gagilas, J. (2021). Saliva testing is a robust non‐invasive method for SARS‐CoV‐2 RNA detection. Infection & Drug Resistance, 14, 2943–2951. 10.2147/IDR.S314491 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pasomsub, E. , Watcharananan, S. P. , Boonyawat, K. , Janchompoo, P. , Wongtabtim, G. , Suksuwan, W. , Sungkanuparph, S. , & Phuphuakrat, A. (2020). Saliva sample as a non‐invasive specimen for the diagnosis of coronavirus disease 2019: A cross‐sectional study. Clinical Microbiology and Infection: The Official Publication of the European Society of Clinical Microbiology and Infectious Diseases, 27(2), 285.e1–285.e4. 10.1016/j.cmi.2020.05.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pasomsub, E. , Watcharananan, S. P. , Boonyawat, K. , Janchompoo, P. , Wongtabtim, G. , Suksuwan, W. , Sungkanuparph, S. , & Phuphuakrat, A. (2021). Saliva sample as a non‐invasive specimen for the diagnosis of coronavirus disease 2019: A cross‐sectional study. Clinical Microbiology & Infection, 27(2), 285.e281–285.e284. 10.1016/j.cmi.2020.05.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plantamura, J. , Bousquet, A. , Otto, M.‐P. , Bigaillon, C. , Legland, A.‐M. , Delacour, H. , Vest, P. , Astier, H. , Valero, E. , Bylicki, O. , Renard, C. , Martin, S. , Verret, C. , Garnotel, E. , Foissaud, V. , Mérens, A. , & Janvier, F. (2021). Performances, feasibility and acceptability of nasopharyngeal swab, saliva and oral‐self sampling swab for the detection of severe acute respiratory syndrome coronavirus 2. European Journal of Clinical Microbiology & Infectious Diseases, 40(10), 2191–2198. 10.1007/s10096-021-04269-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Potter, R. F. , Ransom, E. M. , Wallace, M. A. , Johnson, C. , Kwon, J. H. , Babcock, H. M. , Eby, C. S. , Anderson, N. W. , Parikh, B. A. , & Burnham, C.‐A. (2021). Multiplatform assessment of saliva for SARS‐CoV‐2 molecular detection in symptomatic healthcare personnel and patients presenting to the emergency department. The Journal of Applied Laboratory Medicine, 07, 07. 10.1093/jalm/jfab115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Poukka, E. , Mäkelä, H. , Hagberg, L. , Vo, T. , Nohynek, H. , Ikonen, N. , Liitsola, K. , Helve, O. , Savolainen‐Kopra, C. , & Dub, T. (2021). Detection of SARS‐CoV‐2 infection in gargle, spit, and sputum specimens. Microbiology Spectrum, 9(1), e0003521. 10.1128/Spectrum.00035-21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Procop, G. W. , Shrestha, N. K. , Vogel, S. , Van Sickle, K. , Harrington, S. , Rhoads, D. D. , Rubin, B. P. , & Terpeluk, P. (2020). A direct comparison of enhanced saliva to nasopharyngeal swab for the detection of SARS‐CoV‐2 in symptomatic patients. Journal of Clinical Microbiology, 58(11), 21. 10.1128/JCM.01946-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ptasinska, A. , Whalley, C. , Bosworth, A. , Poxon, C. , Bryer, C. , Machin, N. , Grippon, S. , Wise, E. L. , Armson, B. , Howson, E. L. A. , Goring, A. , Snell, G. , Forster, J. , Mattocks, C. , Frampton, S. , Anderson, R. , Cleary, D. , Parker, J. , Boukas, K. , … Beggs, A. D. (2021). Diagnostic accuracy of loop‐mediated isothermal amplification coupled to nanopore sequencing (LamPORE) for the detection of SARS‐CoV‐2 infection at scale in symptomatic and asymptomatic populations. Clinical Microbiology & Infection, 27(9), 1348.e1341–1348.e1347. 10.1016/j.cmi.2021.04.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rao, M. , Rashid, F. A. , Sabri, F. S. A. H. , Jamil, N. N. , Seradja, V. , Abdullah, N. A. , Ahmad, H. , Aren, S. L. , Ali, S. A. S. , Ghazali, M. , Manaf, A. A. , Talib, H. , Hashim, R. , Zain, R. , Thayan, R. , Amran, F. , Aris, T. , & Ahmad, N. (2021a). COVID‐19 screening test by using random oropharyngeal saliva. Journal of Medical Virology, 93(4), 2461–2466. 10.1002/jmv.26773 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rao, M. , Rashid, F. A. , Sabri, F. S. A. H. , Jamil, N. N. , Zain, R. , Hashim, R. , & Ahmad, N. (2020). Comparing nasopharyngeal swab and early morning saliva for the identification of SARS‐CoV‐2. Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America. 10.1093/cid/ciaa1156 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rao, M. , Rashid, F. A. , Sabri, F. S. A. H. , Jamil, N. N. , Zain, R. , Hashim, R. , Amran, F. , Kok, H. T. , Samad, M. A. A. , & Ahmad, N. (2021). Comparing nasopharyngeal swab and early morning saliva for the identification of severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2). Clinical Infectious Diseases, 72(9), e352–e356. 10.1093/cid/ciaa1156 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saeed, U. , Uppal, S. R. , Piracha, Z. Z. , Rasheed, A. , Aftab, Z. , Zaheer, H. , & Uppal, R. (2021). Evaluation of SARS‐CoV‐2 antigen‐based rapid diagnostic kits in Pakistan: formulation of COVID‐19 national testing strategy. Virology Journal, 18(1), 34. 10.1186/s12985-021-01505-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sahajpal, N. S. , Mondal, A. K. , Ananth, S. , Njau, A. , Ahluwalia, P. , Kota, V. , Caspary, K. , Ross, T. M. , Farrell, M. , Shannon, M. P. , Fulzele, S. , Chaubey, A. , Hegde, M. , Rojiani, A. M. , & Kolhe, R. (2021). Clinical validation of a sensitive test for saliva collected in healthcare and community settings with pooling utility for severe acute respiratory syndrome coronavirus 2 mass surveillance. Journal of Molecular Diagnostics, 23(7), 788–795. 10.1016/j.jmoldx.2021.04.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sasaki, T. , Inoue, O. , Ogihara, S. , Kubokawa, K. , Oishi, S. , Shirai, T. , & Suzuki‐Inoue, K. (2021). Detection of SARS‐CoV‐2 RNA using RT‐qPCR in nasopharyngeal swab, saliva, lingual, and buccal mucosal swab. Japanese Journal of Infectious Diseases, 30, 30. 10.7883/yoken.JJID.2021.091 [DOI] [PubMed] [Google Scholar]
- Sasikala, M. , Sadhana, Y. , Vijayasarathy, K. , Gupta, A. , Daram, S. K. , Podduturi, N. C. R. , & Reddy, D. N. (2021). Comparison of saliva with healthcare workers‐ and patient‐collected swabs in the diagnosis of COVID‐19 in a large cohort. BMC Infectious Diseases, 21(1), 648. 10.1186/s12879-021-06343-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- Senok, A. , Alsuwaidi, H. , Atrah, Y. , Al Ayedi, O. , Al Zahid, J. , Han, A. , & Alsheikh‐Ali, A. (2020). Saliva as an alternative specimen for molecular COVID‐19 testing in community settings and population‐based screening. Infection & Drug Resistance, 13, 3393–3399. 10.2147/IDR.S275152 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith‐Jeffcoat, S. E. , Koh, M. , Hoffman, A. , Rebolledo, P. A. , Schechter, M. C. , Miller, H. K. , Sleweon, S. , Rossetti, R. , Kasinathan, V. , Shragai, T. , O’Laughlin, K. , Espinosa, C. C. , Khalil, G. M. , Adeyemo, A. S. O. , Moorman, A. , Bauman, B. L. , Joseph, K. , O’Hegarty, M. , Kamal, N. , … CDC COVID‐19 Response Team . (2021). Effects of patient characteristics on diagnostic performance of self‐collected samples for SARS‐CoV‐2 testing. Emerging Infectious Diseases, 27(8), 2081–2089. 10.3201/eid2708.210667 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stokes, W. , Berenger, B. M. , Portnoy, D. , Scott, B. , Szelewicki, J. , Singh, T. , Venner, A. A. , Turnbull, L. A. , Pabbaraju, K. , Shokoples, S. , Wong, A. A. , Gill, K. , Guttridge, T. , Proctor, D. , Hu, J. , & Tipples, G. (2021). Clinical performance of the Abbott Panbio with nasopharyngeal, throat, and saliva swabs among symptomatic individuals with COVID‐19. European Journal of Clinical Microbiology & Infectious Diseases, 40(8), 1721–1726. 10.1007/s10096-021-04202-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sun, Q. , Li, J. , Ren, H. , Pastor, L. , Loginova, Y. , Madej, R. , Taylor, K. , Wong, J. K. , Zhang, Z. , Zhang, A. , Lu, C. M. , & Sha, M. Y. (2021). Saliva as a testing specimen with or without pooling for SARS‐CoV‐2 detection by multiplex RT‐PCR test. PLoS One [electronic Resource], 16(2), e0243183. 10.1371/journal.pone.0243183 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sutjipto, S. , Lee, P. H. , Tay, J. Y. , Mendis, S. M. , Abdad, M. Y. , Marimuthu, K. , Ng, O. T. , Cui, L. , Chan, M. , Soon, M. , Lin, R. T. P. , Leo, Y.‐S. , De, P. P. , Barkham, T. , Vasoo, S. , Ong, S. W. X. , Ang, B. S. P. , Lye, D. C. , Lim, P. L. , … National Centre for Infectious Diseases COVID‐19 Outbreak Research Team . (2020). The effect of sample site, illness duration, and the presence of pneumonia on the detection of SARS‐CoV‐2 by real‐time reverse transcription PCR. Open Forum Infectious Diseases, 7(9), ofaa335. 10.1093/ofid/ofaa335 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tapia, C. V. , Marcia, C. , Ivone, M. , Nadia, P. , Lesly, M. , Camila, G. , & Fabien, M. (2021). Performance of saliva samples for COVID‐19 diagnosis by using the allplex™ 2019‐nCoV assay kit. Frontiers in Medicine, 8, 617399. 10.3389/fmed.2021.617399 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teo, A. K. J. , Choudhury, Y. , Tan, I. B. , Cher, C. Y. , Chew, S. H. , Wan, Z. Y. , Cheng, L. T. E. , Oon, L. L. E. , Tan, M. H. , Chan, K. S. , & Hsu, L. Y. (2021). Saliva is more sensitive than nasopharyngeal or nasal swabs for diagnosis of asymptomatic and mild COVID‐19 infection. Scientific Reports, 11(1), 3134. 10.1038/s41598-021-82787-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ter‐Ovanesyan, D. , Gilboa, T. , Lazarovits, R. , Rosenthal, A. , Yu, X. U. , Li, J. Z. , Church, G. M. , & Walt, D. R. (2021). Ultrasensitive measurement of both SARS‐CoV‐2 RNA and antibodies from saliva. Analytical Chemistry, 93(13), 5365–5370. 10.1021/acs.analchem.1c00515 [DOI] [PubMed] [Google Scholar]
- To, K.‐W. , Tsang, O.‐Y. , Leung, W.‐S. , Tam, A. R. , Wu, T.‐C. , Lung, D. C. , Yip, C.‐Y. , Cai, J.‐P. , Chan, J.‐C. , Chik, T.‐H. , Lau, D.‐L. , Choi, C.‐C. , Chen, L.‐L. , Chan, W.‐M. , Chan, K.‐H. , Ip, J. D. , Ng, A.‐K. , Poon, R.‐S. , Luo, C.‐T. , … Yuen, K.‐Y. (2020). Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS‐CoV‐2: An observational cohort study. The Lancet Infectious Diseases, 20(5), 565–574. 10.1016/S1473-3099(20)30196-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toppings, N. B. , Mohon, A. N. , Lee, Y. , Kumar, H. , Lee, D. , Kapoor, R. , Singh, G. , Oberding, L. , Abdullah, O. , Kim, K. , Berenger, B. M. , & Pillai, D. R. (2021). A rapid near‐patient detection system for SARS‐CoV‐2 using saliva. Scientific Reports, 11(1), 13378. 10.1038/s41598-021-92677-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tricco, A. C. , Lillie, E. , Zarin, W. , O'Brien, K. K. , Colquhoun, H. , Levac, D. , Moher, D. , Peters, M. D. J. , Horsley, T. , Weeks, L. , Hempel, S. , Akl, E. A. , Chang, C. , McGowan, J. , Stewart, L. , Hartling, L. , Aldcroft, A. , Wilson, M. G. , Garritty, C. , … Straus, S. E. (2018). PRISMA extension for scoping reviews (PRISMA‐ScR): Checklist and explanation. Annals of Internal Medicine, 169(7), 467–473. 10.7326/m18-0850 [DOI] [PubMed] [Google Scholar]
- Trobajo‐Sanmartin, C. , Adelantado, M. , Navascues, A. , Guembe, M. J. , Rodrigo‐Rincon, I. , Castilla, J. , & Ezpeleta, C. (2021). Self‐collection of saliva specimens as a suitable alternative to nasopharyngeal swabs for the diagnosis of SARS‐CoV‐2 by RT‐qPCR. Journal of Clinical Medicine, 10(2), 299. 10.3390/jcm10020299 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tutuncu, E. E. , Ozgur, D. , & Karamese, M. (2021). Saliva samples for detection of SARS‐CoV‐2 in mildly symptomatic and asymptomatic patients. Journal of Medical Virology, 93(5), 2932–2937. 10.1002/jmv.26821 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Udugama, B. , Kadhiresan, P. , Kozlowski, H. N. , Malekjahani, A. , Osborne, M. , Li, V. Y. C. , Chen, H. , Mubareka, S. , Gubbay, J. B. , & Chan, W. C. W. (2020). Diagnosing COVID‐19: The disease and tools for detection. ACS Nano, 14(4), 3822–3835. 10.1021/acsnano.0c02624 [DOI] [PubMed] [Google Scholar]
- Uwamino, Y. , Nagata, M. , Aoki, W. , Nakagawa, T. , Inose, R. , Yokota, H. , Furusawa, Y. , Sakai‐Tagawa, Y. , Iwatsuki‐Horimoto, K. , Kawaoka, Y. , Hasegawa, N. , & Murata, M. (2021). Accuracy of rapid antigen detection test for nasopharyngeal swab specimens and saliva samples in comparison with RT‐PCR and viral culture for SARS‐CoV‐2 detection. Journal of Infection & Chemotherapy, 27(7), 1058–1062. 10.1016/j.jiac.2021.04.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Vinh Chau, N. , Lam, V. T. , Dung, N. T. , Yen, L. M. , Minh, N. N. Q. , Hung, L. M. , Ngoc, N. M. , Dung, N. T. , Man, D. N. H. , Nguyet, L. A. , Nhat, L. T. H. , Nhu, L. N. T. , Ny, N. T. H. , Hong, N. T. T. , Kestelyn, E. , Dung, N. T. P. , Xuan, T. C. , Hien, T. T. , Phong, N. T. , … Oxford University Clinical Research Unit COVID‐19 Research Group . (2020). The natural history and transmission potential of asymptomatic severe acute respiratory syndrome coronavirus 2 infection. Clinical Infectious Diseases, 71(10), 2679–2687. 10.1093/cid/ciaa711 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vaz, S. N. , Santana, D. S. , Netto, E. M. , Pedroso, C. , Wang, W. K. , Santos, F. D. A. , & Brites, C. (2020). Saliva is a reliable, non‐invasive specimen for SARS‐CoV‐2 detection. Brazilian Journal of Infectious Diseases, 24(5), 422–427. 10.1016/j.bjid.2020.08.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vaz, S. N. , Santana, D. S. , Netto, E. M. , Wang, W. K. , & Brites, C. (2021). Validation of the GeneXpert Xpress SARS‐CoV‐2 PCR assay using saliva as biological specimen. Brazilian Journal of Infectious Diseases, 25(2), 101543. 10.1016/j.bjid.2021.101543 [DOI] [PMC free article] [PubMed] [Google Scholar]
- von Linstow, M. L. , Kruse, A. , Kirkby, N. , Marie Soes, L. , Nygaard, U. , & Poulsen, A. (2021). Saliva is inferior to nose and throat swabs for SARS‐CoV‐2 detection in children. Acta Paediatrica, 110(12), 3325–3326. 10.1111/apa.16049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams, E. , Bond, K. , Zhang, B. , Putl, M. , & Williamson, D. A. (2020). Saliva as a noninvasive specimen for detection of SARS‐CoV‐2. Journal of Clinical Microbiology, 58(8). 10.1128/JCM.00776-20. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=medl&NEWS=N&AN=32317257 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wong, R. C. , Wong, A. H. , Ho, Y. I. , Leung, E. C. , & Lai, R. W. (2020a). Evaluation on testing of deep throat saliva and lower respiratory tract specimens with Xpert Xpress SARS‐CoV‐2 assay. Journal of Clinical Virology, 131, 104593. 10.1016/j.jcv.2020.104593 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wong, S. C. Y. , Tse, H. , Siu, H. K. , Kwong, T. S. , Chu, M. Y. , Yau, F. Y. S. , Cheung, I. Y. Y. , Tse, C. W. S. , Poon, K. C. , Cheung, K. C. , Wu, T. C. , Chan, J. W. M. , Cheuk, W. , & Lung, D. C. (2020b). Posterior oropharyngeal saliva for the detection of severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2). Clinical Infectious Diseases, 71(11), 2939–2946. 10.1093/cid/ciaa797 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wyllie, A. L. , Fournier, J. , Casanovas‐Massana, A. , Campbell, M. , Tokuyama, M. , Vijayakumar, P. , Warren, J. L. , Geng, B. , Muenker, M. C. , Moore, A. J. , Vogels, C. B. F. , Petrone, M. E. , Ott, I. M. , Lu, P. , Venkataraman, A. , Lu‐Culligan, A. , Klein, J. , Earnest, R. , Simonov, M. , … Ko, A. I. (2020). Saliva or nasopharyngeal swab specimens for detection of SARS‐CoV‐2. New England Journal of Medicine, 383(13), 1283–1286. 10.1056/NEJMc2016359 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Xun, G. , Lane, S. T. , Petrov, V. A. , Pepa, B. E. , & Zhao, H. (2021). A rapid, accurate, scalable, and portable testing system for COVID‐19 diagnosis. Nature Communications, 12(1), 2905. 10.1038/s41467-021-23185-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yamazaki, W. , Matsumura, Y. , Thongchankaew‐Seo, U. , Yamazaki, Y. , & Nagao, M. (2021). Development of a point‐of‐care test to detect SARS‐CoV‐2 from saliva which combines a simple RNA extraction method with colorimetric reverse transcription loop‐mediated isothermal amplification detection. Journal of Clinical Virology, 136, 104760. 10.1016/j.jcv.2021.104760 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yang, Q. , Meyerson, N. R. , Clark, S. K. , Paige, C. L. , Fattor, W. T. , Gilchrist, A. R. , Barbachano‐Guerrero, A. , Healy, B. G. , Worden‐Sapper, E. R. , Wu, S. S. , Muhlrad, D. , Decker, C. J. , Saldi, T. K. , Lasda, E. , Gonzales, P. , Fink, M. R. , Tat, K. L. , Hager, C. R. , Davis, J. C. , … Sawyer, S. L. (2021). Saliva TwoStep for rapid detection of asymptomatic SARS‐CoV‐2 carriers. eLife, 10(03), 29. 10.7554/eLife.65113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yee, R. , Truong, T. T. , Pannaraj, P. S. , Eubanks, N. , Gai, E. , Jumarang, J. , Turner, L. , Peralta, A. , Lee, Y. , & Dien Bard, J. (2021). Saliva is a promising alternative specimen for the detection of SARS‐CoV‐2 in children and adults. Journal of Clinical Microbiology, 59(2), 21. 10.1128/JCM.02686-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yokota, I. , Hattori, T. , Shane, P. Y. , Konno, S. , Nagasaka, A. , Takeyabu, K. , Fujisawa, S. , Nishida, M. , & Teshima, T. (2021a). Equivalent SARS‐CoV‐2 viral loads by PCR between nasopharyngeal swab and saliva in symptomatic patients. Scientific Reports, 11(1), 4500. 10.1038/s41598-021-84059-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yokota, I. , Sakurazawa, T. , Sugita, J. , Iwasaki, S. , Yasuda, K. , Yamashita, N. , Fujisawa, S. , Nishida, M. , Konno, S. , & Teshima, T. (2021b). Performance of qualitative and quantitative antigen tests for SARS‐CoV‐2 using saliva. Infectious Disease Reports, 13(3), 742–747. 10.3390/idr13030069 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yokota, I. , Shane, P. Y. , Okada, K. , Unoki, Y. , Yang, Y. , Inao, T. , Sakamaki, K. , Iwasaki, S. , Hayasaka, K. , Sugita, J. , Nishida, M. , Fujisawa, S. , & Teshima, T. (2021c). Mass screening of asymptomatic persons for severe acute respiratory syndrome coronavirus 2 using saliva. Clinical Infectious Diseases, 73(3), e559–e565. 10.1093/cid/ciaa1388 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yokota, I. , Shane, P. Y. , Okada, K. , Unoki, Y. , Yang, Y. , Iwasaki, S. , Fujisawa, S. , Nishida, M. , & Teshima, T. (2021d). A novel strategy for SARS‐CoV‐2 mass screening with quantitative antigen testing of saliva: a diagnostic accuracy study. The Lancet Microbe, 2(8), e397–e404. 10.1016/S2666-5247(21)00092-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yokota, I. , Shane, P. Y. , & Teshima, T. (2021e). Logistic advantage of two‐step screening strategy for SARS‐CoV‐2 at airport quarantine. Travel Medicine & Infectious Disease, 43, 102127. 10.1016/j.tmaid.2021.102127 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yu, F. , Xie, G. , Zheng, S. , Han, D. , Bao, J. , Zhang, D. , Feng, B. , Wang, Q. I. , Zou, Q. , Wang, R. , Yang, X. , Chen, W. , Lou, B. , & Chen, Y. U. (2021). Assessment of the diagnostic ability of four detection methods using three sample types of COVID‐19 patients. Frontiers in Cellular & Infection Microbiology, 11, 685640. 10.3389/fcimb.2021.685640 [DOI] [PMC free article] [PubMed] [Google Scholar]