

Abstract
Purpose
Intra-abdominal injury is a major cause of morbidity in children. Computed tomography (CT) is the reference standard for the evaluation of hemodynamically stable abdominal trauma. CT has an increased risk of long-term radiation induced malignancies and a possible risk associated with the use of iodinated contrast media. Contrast-enhanced ultrasound (CEUS) might represent an alternative to CT in stable children with blunt abdominal trauma (BAT). Nonetheless, CEUS in pediatrics remains limited by the lack of strong evidence. The purpose of this study was to offer a systematic review on the use of CEUS in pediatric abdominal trauma.
Methods
Electronic search of PubMed, EMBASE and Cochrane databases of studies investigating CEUS for abdominal trauma in children. The risk of bias was assessed using the ROBINS-I tool.
Results
This systematic review included 7 studies. CEUS was performed with different ultrasound equipment, always with a curvilinear transducer. Six out of seven studies used a second-generation contrast agent. No immediate adverse reactions were reported. The dose of contrast agent and the scanning technique varied between studies. All CEUS exams were performed by radiologists, in the radiology department or at the bedside. No standard training was reported to become competent in CEUS. The range of sensitivity and specificity of CEUS were 85.7 to 100% and 89 to 100%, respectively.
Conclusion
CEUS appears to be safe and accurate to identify abdominal solid organ injuries in children with BAT. Further research is necessary to assess the feasibility of CEUS by non-radiologists, the necessary training, and the benefit-cost ratio of CEUS as a tool to potentially reduce CT scans.
Keywords: Ultrasound, Contrast-enhanced ultrasound, Abdominal trauma, Children
Background
Intra-abdominal injury (IAI) is a major cause of morbidity in children and young adults [1]. Computed tomography (CT) is considered the reference standard for the evaluation of traumatic injuries in hemodynamically stable patients [2]. The early identification of IAIs is essential to avoid complications due to delayed or missed diagnosis. However, the use of CT in children and adolescents comes with the disadvantage of large radiation exposure and the resulting risk of long-term radiation-induced malignancies [3]. The validation of reliable alternatives is essential to reduce the use of CT, at least in selected clinical settings [4, 5].
The focused assessment with sonography for trauma (FAST) examination rapidly identifies bleeding in the abdominal, pericardial, or intrathoracic spaces.
The assessment of solid organ injury is out of the scope of FAST, and its diagnostic performance for intraparenchymal lesions is not equally high [6]. Its use has been associated with improvements in outcomes among adult patients, including reductions in abdominal CT rates, and decreased hospital length of stay [7–9]. However, the validity and usefulness of the FAST exam among hemodynamically stable children is controversial as it was deemed not to improve clinical care or use of resources, the emergency department (ED) length of stay, or the rate of missed intra-abdominal injuries [10, 11].
The introduction of contrast agents to the ultrasound (US) exam may lead to increase the diagnostic accuracy in many organs. Many studies conducted in children demonstrated that contrast-enhanced ultrasound (CEUS) is more sensitive and accurate than baseline US and almost as sensitive as CT in the identification and characterization of IAIs leading to the hypothesis that CEUS might represent a useful alternative to CT in stable children with blunt abdominal trauma (BAT) [12–19].
Despite no significant adverse events being reported for US contrast agents [20–23], their use in children remains limited to few indications, while their use in trauma remains off-labelled, as it is limited by the lack of strong evidence [24].
For this reason, we aimed to review the current literature focusing on CEUS in pediatric abdominal trauma in order to assess its accuracy, feasibility in emergency settings and safety, to clarify if its use is justifiable as a bedside exam.
Methods
A systematic search of PubMed, EMBASE and the Cochrane Central register of Controlled Trials (CENTRAL) was conducted up to April 2021, according to the Preferred Reporting items for Systematic Reviews and Meta-Analyses (PRISMA) statement [25]. An additional research was conducted on Google Scholar and the references of relevant articles were further crosschecked. No publication date restrictions were applied. The search was limited to published articles written in English. Studies were identified using search combinations or a combination of words. The search strategy as well as the keywords and the search details are reported in Table 1. On a first screening stage, duplicates were removed and all identified studies were evaluated by title or abstract. Two investigators (F.P. and G.G.) independently screened titles and abstracts using a standardized form with predefined eligibility criteria. Studies that were considered eligible were assessed in full text independently to determine whether or not they met the inclusion criteria. Discrepancies were resolved by consensus. We considered eligible studies that included pediatric patients (age range 0–18 years), investigated the use of CEUS for the diagnosis of IAIs, used baseline and/or contrast-enhanced abdominal CT as the reference standard, were either retrospective or prospective. We excluded non-diagnostic studies, studies of CEUS investigating condition other than abdominal trauma, studies focusing on adult population and non-original studies (e.g. literature review, comment, duplicate studies, case reports). In studies analyzing CEUS accuracy for IAIs in mixed populations (adult and pediatric), data on true positive (TP), true negative (TN), false positive (FP) and false negative (FN) where extracted to calculate the pooled diagnostic accuracy in pediatric age. In the cases these data were not specified or not referred to a pediatric-only cohort, we contacted the corresponding authors to obtain the missing information. Two independent raters (F.P. and G.G.) assessed the risk of bias of the eligible studies, using the Risk Of Bias In Non-randomized Studies—of Interventions (ROBINS-I) tool [26]. Disagreement was resolved through consultation with the senior author (NP). The primary outcome was the diagnostic accuracy (sensitivity and specificity) for the diagnosis of IAI with CEUS. The systematic literature review was conducted using RAYYAN (Rayyan Systems Inc) [27]. The need for ethical approval was waived by the local Clinical Trial Center due to the non-clinical nature of the study.
Table 1.
Search strategy
| Pubmed | (((((("wounds and injuries"[MeSH Terms] OR ("wounds"[All Fields] AND "injuries"[All Fields])) OR "wounds and injuries"[All Fields]) OR ("wounds"[All Fields] AND "injury"[All Fields])) OR "wounds and injury"[All Fields]) AND ((("contrast media"[Pharmacological Action] OR "contrast media"[MeSH Terms]) OR ("contrast"[All Fields] AND "media"[All Fields])) OR "contrast media"[All Fields])) AND ((((("diagnostic imaging"[MeSH Subheading] OR ("diagnostic"[All Fields] AND "imaging"[All Fields])) OR "diagnostic imaging"[All Fields]) OR "ultrasonography"[All Fields]) OR "ultrasonography"[MeSH Terms]) OR "ultrasonographies"[All Fields])) AND (((((((((("abdomen"[MeSH Terms] OR "abdomen"[All Fields]) OR "abdomens"[All Fields])) OR "abdominal cavity"[MeSH Terms]) OR ("abdominal"[All Fields] AND "cavity"[All Fields])) OR "abdominal cavity"[All Fields]) OR ((("liver"[MeSH Terms] OR "liver"[All Fields]) OR "livers"[All Fields]) OR "liver s"[All Fields])) OR ((("spleen"[MeSH Terms] OR "spleen"[All Fields]) OR "spleens"[All Fields]) OR "spleen s"[All Fields])) OR (("pancrea"[All Fields] OR "pancreas"[MeSH Terms]) OR "pancreas"[All Fields])) OR ((("kidney"[MeSH Terms] OR "kidney"[All Fields]) OR "kidneys"[All Fields]) OR "kidney s"[All Fields])) |
| Embase | ('abdominal injury' OR 'liver injury' OR 'pancreas injury' OR 'kidney injury') AND 'echography' AND 'contrast medium' |
| Cochrane | ‘CEUS’ |
Results
This study’s PRISMA search is summarized in Fig. 1. The search identified 11 articles. Three were excluded due to an overlap of the cohort described and eight were included in the analysis: three prospective cohort studies [12–14], four retrospective cohort studies [15–18], and one study [19] whose design was not described. Four studies [12, 14, 16, 17] included only pediatric patients, whereas three studies [13, 15, 19] even if focusing on adults, included children, and were therefore included in the analysis. In one study, the age of the included patients was not specified and therefore the study was excluded [18]. A total of seven studies were finally included in our review [12–17, 19]. The total number of children evaluated with CEUS due to abdominal trauma was 234. Six studies [12–14, 16–18] included exclusively patients with BAT, while one study [15] included even penetrating trauma and non-traumatic emergencies. The most frequently diagnosed injuries occurred to the liver, spleen, and kidney. In the study of Valentino et al. [12], pancreatic and adrenal lesions were reported, while in the study of Catalano et al. [15], five abdominal aorta aneurysm ruptures, one ruptured splenic angiosarcoma, and two post-surgery bleedings were detected by CEUS. Demographics and clinical characteristics of the included studies are reported in Table 2. CEUS exams were performed with a curvilinear transducer (frequency range 1–7 MHz) [12, 13, 15, 17, 19] or with a linear transducer (frequency range 9 MHz) [16, 17]. The timing of the CEUS was reported in six studies [12–16, 19], and in four of these, the CEUS was performed immediately after the FAST exam or radiological US evaluation [12, 13, 16, 19]. The time from the trauma to CEUS execution was not specified in any study (Table 3). Six studies [12, 13, 15–17, 19] reported having used a contrast agent constituted by a gas core of Sulphur-hexafluoride encapsulated by a phospholipid shell, while in one [14] the contrast media was Perfluorobutane encapsulated by an albumin shell. Currently, both contrast agents are not labeled for the use under discussion. The reported doses of Sulphur-hexafluoride were similar in most studies ranging from 2.4 to 4.8 ml, the latter divided in 2 single doses of 2.4 ml to complete a full CEUS exam [12, 13, 15–17, 19]. Yusuf et al. [17] reported the dose regimen according to patient’s age (range 0.1 to 4.8 ml). The dose of Perfluorobutane ranged from 0.3 to 0.5 ml repeated twice [14].
Fig. 1.
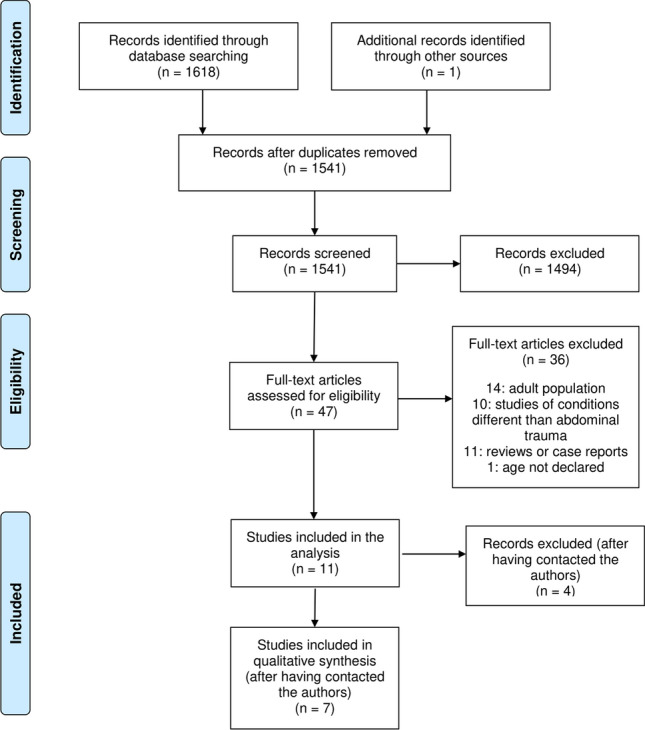
PRISMA flow chart of study inclusion
Table 2.
Demographics, characteristics and diagnostic accuracy of CEUS for intra-abdominal injury, in included studies
| Design | Patients, total (0–18 years) | Age range, years | Mean age, years | Study population | Intra-abdominal Injury | US | CEUS | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BAT | Penetrating trauma | Non-traumatic emergencies | Other | Liver | Spleen | Kidney | Other | Sens | Spec | PPV | NPV | Sens | Spec | PPV | NPV | |||||
| Catalano 2003 [19] | n.a | 25 (1) | 3–79 | 28 | 25 | 0 | 0 | 0 | 0 | 25 | 0 | 0 | n.a | n.a | n.a | n.a | 94.4 | 100 | 100 | 87.5 |
| Catalano 2005 [15]c | Re | 153 (1) | 8–67 | 33 | 75 | 8 | 70 | 0 | 3 | 8 | 1 | 8a | n.a | n.a | n.a | n.a | 100 | 100 | n.a | n.a |
| Valentino 2008 [12] | Pr | 27 (27) | 4–13 | 8.9 | 27 | 0 | 0 | 0 | 4 | 7 | 1 | 2b | 57.1 | 86.7 | 80 | 68.4 | 92.9 | 100 | 100 | 93.8 |
| Catalano 2009 [13] | Pr | 156 (1) | 15–90 | n.a | 156 | 0 | 0 | 0 | 38 | 43 | 26 | 0 | 79 | 82 | 89 | 69 | 94 | 89 | 94 | 89 |
| Menichini 2015 [16] | Re | 73 (73) | n.a | 8.7 | 73 | 0 | 0 | 0 | 21 | 26 | 20 | 0 | 38.8 | 100 | 100 | 12.8 | 100 | 100 | 100 | 100 |
| Yusuf 2016 [17] | Re | 305 (305) | 1–18 | 11.7 | 113 | 0 | 0 | 192 | 113 | 0 | 0 | 0 | n.a | n.a | n.a | n.a | n.a | n.a | n.a | n.a |
| Armstrong 2017 [14] | Pr | 18 (18) | 7–18 | 13.3 | 18 | 0 | 0 | 0 | 3 | 14 | 4 | 0 | 45.2 | 96.4 | 79.2 | 85.3 | 85.7 | 98.6 | 94.7 | 95.8 |
BAT blunt abdominal trauma, CEUS contrast enhancement ultrasound, Pr prospective, Re retrospective, n.a. not available (data not available in the original article or not available after request to the authors), Sens sensitivity, Spec specificity, PPV positive predictive value, NPV negative predictive value
aIncludes five abdominal aorta aneurism ruptures, one ruptured splenic angiosarcoma, and two post-surgery bleedings
bPancreatic and adrenal lesion
cCT correlation of CEUS findings available only in 91/153 (53.5%)
Table 3.
Characteristics of CEUS evaluation in the included studies
| US equipment | Transducer (frequency) | Timing of CEUS | Contrast agent (dose) | Scanning technique | Operator (experience) | Setting | |
|---|---|---|---|---|---|---|---|
| Catalano 2003 [19] | EsaTune (Esaote) | Curvilinear (2.5–5 MHz) | Immediately after baseline US | Sulfur hexafluoride (4.8 ml) | Left upper quadrant continuously scanned for 3–4 min | Radiologist (n.a.) | Radiology |
| Catalano 2005 [15] | EsaTune or Technos (Esaote) | Curvilinear (3.5 MHz) | < 24 h from admission | Sulfur hexafluoride (2.4–4.8 ml) | Left kidney, right kidney, and liver, ending with spleen | Radiologist (n.a.) | ED, bedside in the hospitala, radiology |
| Valentino 2008 [12] | ATL HDI 5000 (Philips) | Curvilinear (2–5 MHz) | Immediately after baseline US | Sulfur hexafluoride (2.4 ml × 2) |
1st dose: left kidney, spleen 2nd dose: right kidney, liver, pancreas |
Radiologist (14 years) | Radiology |
| Catalano 2009 [13] | EsaTune (Esaote), Technos (Esaote), or ATL HDI 5000 (Philips) | Curvilinear (2.5 or 3.5 MHz) | Immediately after baseline US | Sulfur hexafluoride (2.4 ml × 2) |
1st dose: right kidney, adrenal, liver (1–3 min) 2nd dose: left kidney, adrenal, pancreas, spleen (3–4 min) |
Radiologist (n.a.) | Radiology |
| Menichini 2015 [16] | Acuson Sequoia 512 (Siemens) | Curvilinear/linear (n.a.) | Immediately after baseline US | Sulfur hexafluoride (1.2 ml × 2) | Right and left kidney, liver and pancreas, last the spleen | Radiologist (> 10 years) | Radiology |
| Yusuf 2016 [17] | Acuson S2000 or S3000 (Siemens) or RS80A (Samsung) | Curvilinear (3-7 MHz or 6 MHz) or linear (9 MHz) | n.a | Sulfur hexafluoride (0.1–4.8 mL) | n.a | Radiologist (> 10 years) | Radiology |
| Armstrong 2017 [14] | LOGIQ E9 (GE Healthcare) | Curvilinear (1–5 MHz) | < 48 h from trauma | Perfluorobutane (0.3–0.5 ml × 2) |
1st dose: liver, right kidney and pancreas 2nd dose: spleen and left kidney |
Radiologist (brief tutorial in CEUS) | Radiology |
US ultrasound, CEUS contrast enhanced ultrasound, n.a. not available, ED emergency department
aSurgical department, ICU, operating room
All studies except one [17] described the scanning technique adopted to complete a full CEUS evaluation of the abdomen, and these were heterogeneous. In most cases, when two doses were administered, a half of the abdomen was scanned for each dose, variably beginning by left or right quadrants (Table 3 and Fig. 2).
Fig. 2.

CEUS scanning technique. A Right kidney, liver, and pancreas images are obtained after the first dose of contrast agent, spleen and left kidney images are acquired after the second dose (e.g., according to Armstrong et al. [14] or Catalano et al. [13, 15, 19]). A variant of such technique was proposed by Valentino et al. [12] who scanned first the left quadrants and then the right ones. B Right and left kidney, liver, pancreas, and spleen, according to Menichini et al. [16]. The same technique was described by Miele et al. [30] in adult patients
All exams were performed by radiologists. Competences were expressed in term of years of experience without giving any detail of credentialing to perform CEUS. In the paper of Armstrong et al. [14], the authors declared that the CEUS was performed by radiologist trained with a brief tutorial in CEUS. In the majority of the studies, CEUS was performed in the radiology department [12–14, 16, 17, 19] and in one case [15] in the ED or at the bedside in the hospital (Table 3).
No immediate adverse reactions were reported in the studies considered in our review. Yusuf et al. [17] reported delayed adverse reactions in 2 patients (one transient tachycardia and one transient hypertension) which did not required treatment.
Figure 3 presents the risk of bias in the included studies according to the ROBINS-I tool [26]. Three studies [14, 15, 17] presented a moderate risk of bias due to confounding. In the study of Armstrong et al. [14] participants were selected between children with a positive CT for IAI and conventional US and CEUS were performed within 48 h of injury which constitutes a pre-intervention factor that predicts individuals receiving the intervention (CEUS). In the other two studies [15, 17] the cohorts reported either patients with traumatic and non-traumatic emergencies. A bias due to selection of participants was present in five studies [12, 14–17]. In two studies [12, 16] the reference standard CT was not performed to all patients of the cohort, while in three out of five studies [14, 15, 17] criteria to order a CT scan were not declared. Overall, all the included studies, had a low risk of bias in all the following domains: classification of interventions, deviation from intended interventions, measurement of outcomes and selection of reported result. Five out of seven studies presented a moderate risk of bias due to missing data.
Fig. 3.
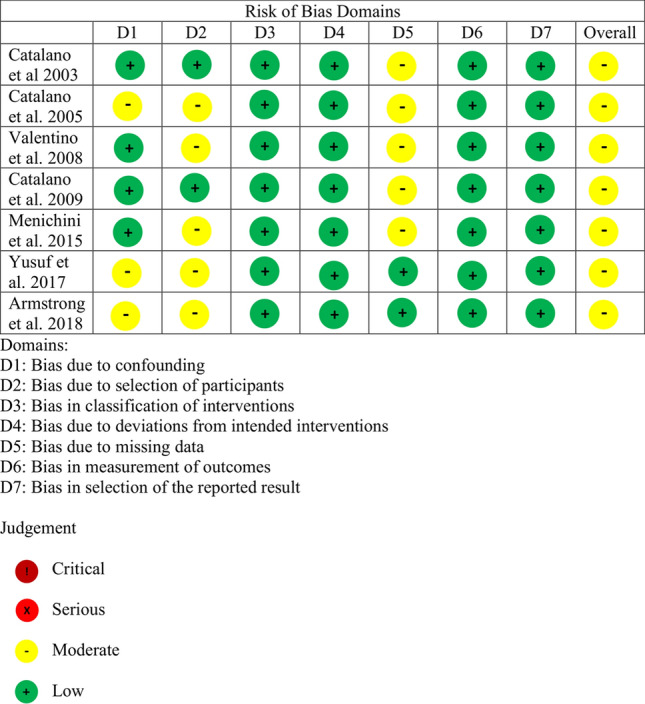
Risk of bias assessment
Available data in the manuscript considered for this review, did not allow a meta-analysis of diagnostic accuracy. Researchers of five studies were contacted to obtain the necessary details to calculate the sensitivity and specificity without response, neither the authors of the manuscript included in our review, responded to our request to have the rough data of their research. For this reason, we report the range of sensitivity and specificity of CEUS, respectively 85.7 to 100% and 89 to 100% (Table 2).
Discussion
Trauma is the leading cause of death in children, with blunt torso trauma substantially contributing [1]. The use of CT scanning in patients with trauma has significantly increased in the recent decades, despite limited evidence supporting such an increase [3]. CT scanning of the abdomen has the significant drawbacks of exposure to high doses of ionizing radiation which determinate a higher risk for developing radiation‐induced malignancies in children [3]. Both the underuse and the overuse of abdominal CT scanning have potential adverse effects that could be reduced by the appropriate targeting of scanning to only those children at risk of clinically important injuries.
Clinical prediction rules to identify children at very low risk for IAI undergoing acute intervention exist, but their strict application could result in a substantial increase in abdominal CT scanning [4]. Unfortunately, these clinical prediction rules exclude FAST, which has already demonstrated its ability to make test ordering more efficient and expedite the decision for laparotomy or thoracotomy [28]. Therefore, it may not apply to hospitals that regularly perform serial examinations on their patients for focused assessment sonography for trauma. Diagnostic imaging utilization in BAT is an important topic and further research into this area is necessary.
In this study, we reviewed the use and accuracy of CEUS in children with BAT presenting to the ED. We focused on this specific condition considering that most children with abdominal trauma and/or solid organ injuries are managed with observation [29]. The availability of an ultrasound contrast agent that could increase the accuracy for IAIs may result in the possibility of a more gradual escalation of care in the approach of stable children with BAT.
Even if we were not able to complete a meta-analysis, the range of sensitivity and specificity for the described intra-abdominal injuries resulted higher than the diagnostic accuracy of FAST exam or baseline radiology performed ultrasound.
Studies reported different protocol of image acquisition and doses of contrast media. All studies of CEUS in trauma described a two split doses regimen, in order to evaluate firstly organs in the right upper quadrant and then organs in the left quadrants or vice versa (Fig. 2), with the entire examination lasting for 4 to 6 min. When using a contrast agent, the sonographer must know that the solid organ parenchymal enhancement depends on the differences in the organ vascularization. The kidneys show a rapid enhancement and should be examined first, while the spleen has a persistent enhancement (up to 8 min) and the liver shows a mounting intensity of enhancement with multiple and different enhancement phases (arterial, portal and late-phase) after contrast injection [30]. Of note, the CEUS examination should commence from the side of the major clinical concern [30, 31] which is not always clinically identifiable. The time from contrast agent injection to the microbubble destruction (wash-out phase), which determine a reduction in enhancement, in image quality and the conclusion of the exam, is the only constraint when performing a CEUS. Currently available technology on modern ultrasound machines, such as plane wave imaging (simultaneous excitation of all available elements in a certain transducer to transmit and collect ultrasonic signals) or software-based technology capable of utilizing more ultrasound data than conventional ultrasound imaging platforms and providing more spatial and contrast resolution, helps generating significantly enhanced images, resulting in greater sensitivity and longer contrast agent duration. This could ultimately reduce the dose of contrast agent used and prolong the time of the exam, which could be particularly useful for novice users of CEUS.
One of the aims of our review was to report on the safety of CEUS in the specific population of children with abdominal trauma. In pediatric imaging, the risk to benefit ratio should be very low to consider as acceptable the risk of adverse reactions.
A major safety consideration is that ultrasound contrast agents, are not excreted through the kidneys, and can be safely administered to patients with renal insufficiency with no risk of contrast-related nephropathy. This determinate that there is no need for blood tests prior to ultrasound contrast agent use [32].
In the population that we explored only 2 (0.7%) late adverse reactions were reported [17].
Minor events after intravenous delivery of ultrasound contrast agent for non-cardiac applications in pediatrics were described with an incidence of transient adverse events of 0.1–0.5% [21].
Further data on safety of contrast agents in children described three cases of hypotension and three skin rashes all of which resolved spontaneously over 312 patients [20] and one case of anaphylactic shock and nine mild transitory adverse events which included altered taste, lightheadedness, headaches and transient nausea over 502 children [22]. Similar results were described by Rosado et al. [23].
Ultrasound contrast agents have a very low rate of anaphylactoid reactions (1:7000 patients, 0.014%), which is significantly lower than the rate with iodinated CT agents [32].
Published analysis of safety of the mostly used contrast agent (Sulfur-hexafluoride) for abdominal indications in adults reported a rate of 0.0086% for adverse events, with no fatal events recorded [31].
The lack of specific studies of safety could be a reason for having the Sulfur-hexafluoride approved by the FDA only for few indications in pediatric age (imaging of liver tumors, echocardiography, imaging of urinary tract for vesicoureteral reflux) while its use is still off label in Europe, despite a specific position statement was published [22]. The more limited safety data in children suggests that adverse events are similar in adults and children and that CEUS in pediatrics is acceptable from a safety standpoint.
CEUS studies were mostly performed in Radiology settings. This is obvious since all authors describing CEUS in pediatric patients were radiologists. Nonetheless, in the paper of Catalano et al. [15] a number of exams were performed at the bedside (even in the ED), and in one of the excluded papers all enrolled patients with abdominal trauma were studied in the ED [18].
This could lead the possibility to a wider use of CEUS even in the ED immediately after the FAST exam, in selected situations. Among them, hemodynamically stable patients who sustained isolated BAT or patients with indeterminate or normal CT findings and suspicious laboratory tests might be included [23]. Another possible reason for having only radiologists performing CEUS could be the need of ultrasound machines which could result bigger than portable ultrasound equipment, more suitable in emergency settings. Lastly, the training required to perform CEUS, which was not reported in any of the considered manuscripts, could be a limitation to the rapid adoption of CEUS in the ED by clinicians performing ultrasound. Several technical and procedural parameters have a significant influence on the quality of CEUS images and should be carefully controlled to obtain good image quality and a reliable diagnosis. Achieving the proper balance between the respective parameters is a matter of technical knowledge and experience. Appropriate training and education should be mandatory for every investigator performing CEUS examinations. To this end, the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) recommends that CEUS should be performed by operators that have achieved competence Level 1, as it has been recognized that the diagnostic performance of CEUS is dependent on the observer’s level of experience.
Conclusion
CEUS showed superior diagnostic accuracy to baseline ultrasound or FAST exam for the diagnosis of IAIs and almost as accurate as abdominal CT scan. Future research in CEUS should clarify if the use of US contrast agents is feasible in an emergency setting by non-radiologist as well as the necessary training to complete a full CEUS exam with an acceptable accuracy. Research should even considerate a benefit–cost ratio of using CEUS in abdominal trauma in light of a potential reduction of exposure to ionizing radiations versus the current standard consisting of FAST and CT, while assessing for the safety of the contrast agents (Fig. 4).
Fig. 4.

Perspective of research in CEUS
Acknowledgements
We gratefully acknowledge Marco Dardi Eng, Clinical & Sales Application, Medical Care System for his technical support and critical advice in reviewing the manuscript.
Author contributions
FP performed the literature search and screened the literature, performed the analysis and the risk of bias assessment, drafted the initial manuscript, and reviewed and revised the manuscript. GG performed the literature search and screened the literature, performed the analysis and the risk of bias assessment, drafted the initial manuscript, and reviewed and revised the manuscript. MG coordinated and supervised data collection, critically reviewed and revised the manuscript, and overviewed the revisions of the manuscript. NP conceptualized and designed the study, drafted the initial manuscript, reviewed the risk of bias assessment, and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declarations
Conflict of interest
None declared.
Ethics approval
The need for ethical approval was waived by the local Clinical Trial Center due to the nature of the study.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Heron M. Deaths: leading causes for 2007. Natl Vital Stat Rep. 2011;59:1–95. [PubMed] [Google Scholar]
- 2.Stuhlfaut JW, Anderson SW, Soto JA. Blunt abdominal trauma: current imaging techniques and CT findings in patients with solid organ, bowel, and mesenteric injury. Semin Ultrasound CT MR. 2007;28:115–129. doi: 10.1053/j.sult.2007.01.004. [DOI] [PubMed] [Google Scholar]
- 3.Miglioretti DL, Johnson E, Williams A, et al. The use of computed tomography in pediatrics and the associated radiation exposure and estimated cancer risk. JAMA Pediatr. 2013;167:700–707. doi: 10.1001/jamapediatrics.2013.311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Holmes JF, Lillis K, Monroe D, et al. Identifying children at very low risk of clinically important blunt abdominal injuries. Ann Emerg Med. 2013;62:107–116. doi: 10.1016/j.annemergmed.2012.11.009. [DOI] [PubMed] [Google Scholar]
- 5.Streck CJ, Vogel AM, Zhang J, et al. Identifying children at very low risk for blunt intra-abdominal injury in whom CT of the abdomen can be avoided safely. J Am Coll Surg. 2017;224:449–458. doi: 10.1016/j.jamcollsurg.2016.12.041. [DOI] [PubMed] [Google Scholar]
- 6.Montoya J, Stawicki SP, Evans DC, et al. From FAST to E-FAST: an overview of the evolution of ultrasound-based traumatic injury assessment. Eur J Trauma Emerg Surg. 2016;42:119–126. doi: 10.1007/s00068-015-0512-1. [DOI] [PubMed] [Google Scholar]
- 7.Stengel D, Rademacher G, Ekkernkamp A, et al. Emergency ultrasound-based algorithms for diagnosing blunt abdominal trauma. Cochrane Database Syst Rev. 2015;9(9):CD004446. doi: 10.1002/14651858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Melniker LA, Leibner E, McKenney MG, et al. Randomized controlled clinical trial of point-of-care, limited ultrasonography for trauma in the emergency department: the first sonography outcomes assessment program trial. Ann Emerg Med. 2006;48:227–235. doi: 10.1016/j.annemergmed.2006.01.008. [DOI] [PubMed] [Google Scholar]
- 9.Rose JS, Levitt MA, Porter J, et al. Does the presence of ultrasound really affect computed tomographic scan use? a prospective randomized trial of ultrasound in trauma. J Trauma. 2001;51:545–550. doi: 10.1097/00005373-200109000-00022. [DOI] [PubMed] [Google Scholar]
- 10.Holmes JF, Gladman A, Chang CH. Performance of abdominal ultrasonography in pediatric blunt trauma patients: a meta-analysis. J Pediatr Surg. 2007;42:1588–1594. doi: 10.1016/j.jpedsurg.2007.04.023. [DOI] [PubMed] [Google Scholar]
- 11.Holmes JF, Kelley KM, Wootton-Gorges SL, et al. Effect of abdominal ultrasound on clinical care, outcomes, and resource use among children with blunt torso trauma: a randomized clinical trial. JAMA. 2017;317:2290–2296. doi: 10.1001/jama.2017.6322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Valentino M, Serra C, Pavlica P, et al. Blunt abdominal trauma: diagnostic performance of contrast-enhanced US in children—initial experience. Radiology. 2008;246:903–909. doi: 10.1148/radiol.2463070652. [DOI] [PubMed] [Google Scholar]
- 13.Catalano O, Aiani L, Barozzi L, et al. CEUS in abdominal trauma: multi-center study. Abdom Imaging. 2009;34:225–234. doi: 10.1007/s00261-008-9452-0. [DOI] [PubMed] [Google Scholar]
- 14.Armstrong LB, Mooney DP, Paltiel H, et al. Contrast enhanced ultrasound for the evaluation of blunt pediatric abdominal trauma. J Pediatr Surg. 2018;53:548–552. doi: 10.1016/j.jpedsurg.2017.03.042. [DOI] [PubMed] [Google Scholar]
- 15.Catalano O, Sandomenico F, Raso MM, et al. Real-time, contrast-enhanced sonography: a new tool for detecting active bleeding. J Trauma. 2005;59:933–939. doi: 10.1097/01.ta.0000188129.91271.ab. [DOI] [PubMed] [Google Scholar]
- 16.Menichini G, Sessa B, Trinci M, et al. Accuracy of contrast-enhanced ultrasound (CEUS) in the identification and characterization of traumatic solid organ lesions in children: a retrospective comparison with baseline US and CE-MDCT. Radiol Med. 2015;120:989–1001. doi: 10.1007/s11547-015-0535-z. [DOI] [PubMed] [Google Scholar]
- 17.Yusuf GT, Sellars ME, Deganello A, et al. Retrospective analysis of the safety and cost implications of pediatric contrast-enhanced ultrasound at a single center. AJR Am J Roentgenol. 2017;208:446–452. doi: 10.2214/AJR.16.16700. [DOI] [PubMed] [Google Scholar]
- 18.Lv F, Tang J, Luo Y, et al. Contrast-enhanced ultrasound imaging of active bleeding associated with hepatic and splenic trauma. Radiol Med. 2011;116:1076–1082. doi: 10.1007/s11547-011-0680-y. [DOI] [PubMed] [Google Scholar]
- 19.Catalano O, Lobianco R, Sandomenico F, et al. Splenic trauma: evaluation with contrast-specific sonography and a second-generation contrast medium: preliminary experience. J Ultrasound Med. 2003;22:467–477. doi: 10.7863/jum.2003.22.5.467. [DOI] [PubMed] [Google Scholar]
- 20.Mao M, Xia B, Chen W, et al. The safety and effectiveness of intravenous contrast-enhanced sonography in chinese children-A single center and prospective study in China. Front Pharmacol. 2019;10:1447. doi: 10.3389/fphar.2019.01447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Darge K, Papadopoulou F, Ntoulia A, et al. Safety of contrast-enhanced ultrasound in children for non-cardiac applications: a review by the Society for Pediatric Radiology (SPR) and the International Contrast Ultrasound Society (ICUS) Pediatr Radiol. 2013;43:1063–1073. doi: 10.1007/s00247-013-2746-6. [DOI] [PubMed] [Google Scholar]
- 22.Piskunowicz M, Kosiak W, Batko T, et al. Safety of intravenous application of second-generation ultrasound contrast agent in children: prospective analysis. Ultrasound Med Biol. 2015;41:1095–1099. doi: 10.1016/j.ultrasmedbio.2014.11.003. [DOI] [PubMed] [Google Scholar]
- 23.Rosado E, Riccabona M. Off-label use of ultrasound contrast agents for intravenous applications in children: analysis of the existing literature. J Ultrasound Med. 2016;35:487–496. doi: 10.7863/ultra.15.02030. [DOI] [PubMed] [Google Scholar]
- 24.Sidhu PS, Cantisani V, Deganello A, et al. Role of Contrast-Enhanced Ultrasound (CEUS) in paediatric practice: an EFSUMB position statement. Ultraschall Med. 2017;38:33–43. doi: 10.1055/s-0042-110394. [DOI] [PubMed] [Google Scholar]
- 25.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62:e1–34. doi: 10.1016/j.jclinepi.2009.06.006. [DOI] [PubMed] [Google Scholar]
- 26.Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. doi: 10.1136/bmj.i4919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ouzzani M, Hammady H, Fedorowicz Z, et al. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5:210. doi: 10.1186/s13643-016-0384-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Noble VE, Blaivas M, Blankenship R, et al. Decision rule for imaging utilization in blunt abdominal trauma—where is ultrasound? Ann Emerg Med. 2010;55:487–489. doi: 10.1016/j.annemergmed.2009.11.030. [DOI] [PubMed] [Google Scholar]
- 29.Wisner DH, Kuppermann N, Cooper A, et al. Management of children with solid organ injuries after blunt torso trauma. J Trauma Acute Care Surg. 2015;79:206–214. doi: 10.1097/TA.0000000000000731. [DOI] [PubMed] [Google Scholar]
- 30.Miele V, Piccolo CL, Galluzzo M, et al. Contrast-enhanced ultrasound (CEUS) in blunt abdominal trauma. Br J Radiol. 2016;89:20150823. doi: 10.1259/bjr.20150823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Piscaglia F, Bolondi L. Italian Society for Ultrasound in Medicine and Biology (SIUMB) Study Group on ultrasound contrast agents. the safety of sonovue in abdominal applications: retrospective analysis of 23188 investigations. Ultrasound Med Biol. 2006;32:1369–1375. doi: 10.1016/j.ultrasmedbio.2006.05.031. [DOI] [PubMed] [Google Scholar]
- 32.Sidhu PS, Cantisani V, Dietrich CF, et al. The EFSUMB guidelines and recommendations for the clinical practice of contrast-enhanced ultrasound (CEUS) in non-hepatic applications: update 2017 (Long Version) Ultraschall Med. 2017;39:e2–e44. doi: 10.1055/a-0586-1107. [DOI] [PubMed] [Google Scholar]