

Abstract
Advanced and recurrent gynecological cancers are associated with a poor prognosis and there is still a lack of effective treatments. Immune checkpoint blockade (ICB) therapy is an important element of cancer‐targeted therapy and immunotherapy. The programed cell death protein 1 (PD‐1) and cytotoxic T‐lymphocyte‐associated antigen 4 (CTLA‐4) pathways are the two main targets of ICB. In this study, we provide a comprehensive review of clinical evidence concerning ICB therapy in gynecological cancers and discuss future implications. All clinical trials of ICB therapy in gynecological cancers were reviewed. We searched ClinicalTrials.gov to collect data from completed and ongoing clinical trials. The clinical evidence regarding the efficacy of ICB agents in gynecological cancers were discussed. Six phase III clinical trials have reported their results of primary outcomes, and a total of 25 phase II clinical trials have been completed. As revealed in phase III trials, pembrolizumab (a PD‐1 antibody) improved the overall survival and progression‐free survival in endometrial cancer patients with mismatch repair deficiency and cervical cancer patients with expressions of PD‐L1. Based on these findings, pembrolizumab was approved by the Food and Drug Administration and European Medicines Agency as a cancer medication used to treat certain patients with endometrial cancer or cervical cancer. Other PD‐1 antibodies, including dostarlimab and cemiplimab, also showed antitumor efficacy in clinical trials. Dostarlimab treatment showed an encouraging response rate in endometrial cancer patients with mismatch repair deficiency. Cemiplimab treatment led to a longer overall survival and a lower risk of death than chemotherapy among patients with recurrent cervical cancer. Three completed phase III trials investigated anti‐PD‐L1 agents (atezolizumab and avelumab) in the treatment of ovarian cancer. The results were not encouraging. Other strategies of ICB therapy which had showed potential clinical benefit in the treatment of gynecological cancers in early‐phase trials need to be further evaluated in late‐stage trials. The antitumor efficacy of ICB therapy is promising, and the key to making further progress in the treatment of gynecological cancers is to identify more biomarkers and explore innovative combination treatments with other targeted therapies.
Keywords: cervical cancer, clinical trials, endometrial cancer, immune checkpoint blockades, ovarian cancer
Abbreviations
- CPS
combined positive score
- CTLA‐4
cytotoxic T‐lymphocyte‐associated antigen 4
- dMMR
deficient mismatch repair
- FDA
Food and Drug Administration
- HPV
human papillomavirus
- ICB
immune checkpoint blockade
- MMR
mismatch repair
- MSI‐H
microsatellite instability hypermutated
- ORR
objective response rate
- OS
overall survival
- PARPi
poly adenosine diphosphate‐ribose polymerase inhibitor
- PD‐1
programed death protein 1
- PD‐L1
programed death protein ligand 1
- PFS
progression‐free survival
- POLE
polymerase epsilon
Key message.
This review provides a comprehensive clinical evidence concerning immune checkpoint blockades in the treatment of gynecological cancers and discusses future implications.
1. INTRODUCTION
In the discipline of gynecological oncology, endometrial cancer, cervical cancer and ovarian cancer are the three main malignant diseases, widely affecting the health of women around the world. Despite advances in conventional treatments (eg curative surgery, chemotherapy and radiotherapy), the prognosis is still very poor in patients with advanced‐stage or recurrent gynecological cancers. Nevertheless, the use of targeted therapies has provided new therapeutic opportunities for these patients.
The immune checkpoint blockade (ICB) is an important class of targeted therapy and immunotherapy. Immune checkpoint molecules are inhibitory receptors that are expressed on the membranes of immune cells. The expression of immune checkpoint receptors works on the negative regulation of immune response, which is an essential mechanism to maintain self‐tolerance and prevent autoimmunity under physiological conditions. However, in the tumor microenvironment, the expression of immune checkpoint receptors is dysregulated to evade antitumor immune response. 1 The immunotherapeutic mechanism of ICB as a promising cancer therapy is demonstrated in Figure 1.
FIGURE 1.
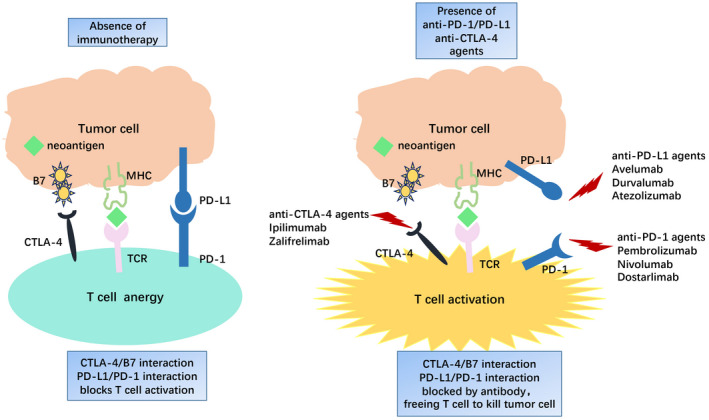
The mechanism of immune checkpoint blockade therapy.
ICBs are agents (mainly antibodies) that target and block immune checkpoint molecules. Cytotoxic T‐lymphocyte‐associated antigen 4 (CTLA‐4) antibody is the first of this class of immunotherapeutics to be approved for clinical use in the treatment of melanoma. 2 CTLA‐4 is an inhibitory receptor expressed on T cells that counteracts the activity of CD28, which is a co‐stimulatory receptor of T cells. Thus, the expression of CTLA‐4 inhibits the activation of T cells. 3 Conversely, the blockade of CTLA‐4 enhances the activation of T cells, as well as the immune response. 4 Programed cell death protein 1 (PD‐1) is another immune checkpoint receptor expressed on T cells. There are two main ligands for PD‐1: PD‐1 ligand 1 (PD‐L1) and PD‐L2, both of which are members of the B7 family. 5 In several different human tumors, PD‐1 is expressed on tumor‐infiltrating lymphocytes, and the PD‐1 ligands are upregulated on the tumor cell surface. 6 The PD‐1 pathway plays an important role in immune resistance within the tumor microenvironment, thus the blockade of the PD‐1 pathway may enhance antitumor response. 7
Numerous clinical trials have investigated the antitumor efficacy of ICBs in gynecological cancers. Based on existing clinical evidence, several ICB drugs have been approved as cancer medications to treat patients with certain forms of gynecological cancer. This review summarizes important clinical evidence concerning ICBs in the treatment of gynecological cancers and discusses the future development of ICB therapy.
A literature search was performed on PubMed, including articles and reviews of clinical trials. We also searched ClinicalTrials.gov to collect data regarding all completed and ongoing clinical trials. The websites of the European Medicines Agency (EMA) and the U.S. Food and Drug Administration (FDA) were queried for information concerning each approved drug. Search terms included “gynecological cancers”, “endometrial cancer”, “cervical cancer”, “ovarian cancer”, “immune checkpoint blockade”, “PD‐1”, “PD‐L1”, “PD‐L2”, “CTLA‐4”, and each name of the ICB agents (eg “pembrolizumab”, “nivolumab”, and “ipilimumab”). We also visited the websites of the European Society for Medical Oncology (ESMO) and the American Society of Clinical Oncology (ASCO) to extract preliminary results from ongoing trials. All of the searches were performed up to February 28, 2022. All studies identified by the search strategy were assessed separately by two authors. The qualities of randomized controlled trials (RCTs) were evaluated using the Jadad scale.
Table 1 provides a summary of currently approved ICBs in the treatment of gynecological cancers. Six phase III clinical trials have reported primary outcomes (Table 2); a total of 25 phase II trials have been completed (Table 3). All phase III studies involved were RCTs with high quality. According to ClinicalTrials.gov, there are a further 19 ongoing phase III trials (Table 4) and dozens of ongoing phase II trials. The study design and status of the ongoing phase II trials are listed in the Tables S1 and S2.
TABLE 1.
Approval anti‐PD‐1 targeted drugs for gynecological cancers
| Target | Drug | Approval year | Approval | Indication | Administration | |
|---|---|---|---|---|---|---|
| Anti‐PD‐1 | Pembrolizumab (Keytruda, Merck) | 2015 | EMA | EC | Endometrial carcinoma | 200 mg IV every 3 weeks or 400 mg every 6 weeks |
| Anti‐PD‐1 | Pembrolizumab (Keytruda, Merck) | 2017 | FDA | EC | Unresectable or metastatic EC, with a biomarker as MSI‐H or dMMR | 200 mg IV every 3 weeks or 400 mg every 6 weeks |
| Anti‐PD‐1 + VEGFi | Pembrolizumab (Keytruda, Merck) + lenvatinib (Lenvima, Eisai) | 2021 | FDA/EMA | EC | Advanced EC cases who have disease progression following prior systemic therapy but who are not candidates for curative surgery or radiation | Lenvatinib 20 mg orally once daily with pembrolizumab 200 mg IV every 3 weeks |
| Anti‐PD‐1 | Pembrolizumab (Keytruda, Merck) | 2021 | FDA | CC | Persistent, recurrent or metastatic CC cases whose tumors express PD‐L1 (CPS≥1) | 200 mg IV every 3 weeks or 400 mg every 6 weeks |
| Anti‐PD‐1 | Dostarlimab (Jemperli, Glaxo Smith Kline) | 2021 a | FDA/EMA | EC | Recurrent or advanced EC, with a biomarker as dMMR | 500 mg IV, 4 doses every 3 weeks followed by 1000 mg IV every 6 weeks |
Abbreviations: CC, cervical cancer; CPS, combined positive score; dMMR, deficient mismatch repair; EC, endometrial cancer; EMA, European Medicines Agency; FDA, Food and Drug Administration; IV, intravenous infusion; MSI‐H, microsatellite instability high; PD‐1, programed death protein 1; VEGFi, vascular endothelial growth factor inhibitor.
Accelerated approval.
TABLE 2.
Completed phase III trials of anti‐PD‐1/PD‐L1 agents in gynecological cancers
| ID | Cancer/condition | No. | Intervention | mOS (months) | mPFS (months) | SAEs (%) | Refs |
|---|---|---|---|---|---|---|---|
|
KEYNOTE‐775 |
EC/dMMR | 827 |
1) Physician's choice 2) Pembrolizumab + lenvatinib |
12.0 17.4, p < 0.01 |
3.8 7.2, p < 0.01 |
73 89 |
[12] |
|
KEYNOTE‐826 |
CC/persistent, recurrent, or metastatic | 548 |
1) Pembrolizumab + chemotherapy 2) Placebo + chemotherapy |
24‐month OS: 53.0% 24‐month OS: 41.7%, p < 0.001 |
10.4 8.1, p < 0.001 |
42 36 |
[21] |
| NCT03257267 | CC/recurrent | 608 |
1) Celiplimab 2 Single‐agent chemotherapy |
12.0 8.5, p < 0.001 |
2.8 2.9, p < 0.001 |
45 53 |
[22] |
|
JAVELIN Ovarian 200 |
OC/platinum‐resistant, or ‐refractory recurrent | 361 |
1) Avelumab 2) Avelumab + PLD 3) PLD |
18.2 18.4 17.4, p > 0.1 |
1.9 3.7 3.5, p > 0.99 |
28 36 19 |
[37] |
|
IMagyn050 |
OC/stage III‐IV | 1300 |
1) Atezolizumab + PC + bevacizumab 2) Placebo + PC + bevacizumab |
— |
19.5 18.4, p = 0.038 |
51 52 |
[35] |
|
JAVELIN Ovarian 100 |
OC/untreated | 988 |
1) PC 2) PC+ avelumab, avelumab maintenance 3) PC, avelumab maintenance |
Terminated due to the futility of efficacy | [36] | ||
Abbreviations: CC, cervical cancer; dMMR, mismatch repair deficient; EC, endometrial cancer; mOS, median overall survival; mPFS, median progression‐free survival; No., number of participants; OC, ovarian cancer; OS, overall survival; PC, paclitaxel + carboplatin; PLD, pegylated liposomal doxorubicin; Refs, references; SAEs, serious adverse events.
TABLE 3.
Completed phase II trials of anti‐PD‐1/PDL‐1 agents in gynecological cancers
| ID | Cancer/condition | No. | Intervention | ORR (%) | mPFS (months) | mOS (months) | Conclusion | Refs |
|---|---|---|---|---|---|---|---|---|
|
KEYNOTE146 |
EC/advanced | 54 | Pembrolizumab + lenvatinib | 39.6 | 7.4 | — | Benefited | [11] |
| NCT02899793 | EC/recurrent, dMMR | 25 | Pembrolizumab:
|
100 44.0 |
3‐year PFS: 100% 30% |
3‐year OS: 100% 43% |
Benefited | [13] |
| NCT02549209 | EC/recurrent | 46 | Pembrolizumab + PC | 77.8 | 10.55 | Benefited | [14] | |
|
TOPIC |
EC/advanced, recurrent or metastatic | 51 | Pembrolizumab + doxorubicin | 32.0 | 6.5 | 18.5 | Benefited | [42] |
|
PRIMMO |
CC or EC | 43 | Pembrolizumab | — | — | — | — | No data, unpublished |
|
KEYNOTE158 |
CC/advanced | 98 | Pembrolizumab | 12.2 | — | — | Benefited | [20] |
|
KEYNOTE100 |
OC/advanced or recurrent | 376 | Pembrolizumab | 8.0 | 2.1 | 17.6 | — | [30] |
|
KEYNOTE191 |
OC/recurrent | 78 |
Pembrolizumab + ACP‐196 |
2.9 9.1 |
— | — | — | Unpublished |
| NCT02440425 | OC/platinum‐resistant | 37 | Pembrolizumab + paclitaxel | 51.4 | — | 26.3 | — | Unpublished |
|
PemCiGem |
OC/platinum‐resistant | 24 | Pembrolizumab + standard treatment | 60.0 | 6.2 | 11.3 | Not benefited | [31] |
| NCT02865811 | OC/platinum‐resistant | 26 | Pembrolizumab + doxorubicin | 26.1 | 8.1 | 13.8 | Benefited | [43] |
| NCT02901899 | OC/recurrent | 38 | Pembrolizumab + gemcitabine | 27.0 | — | — | Modest activity | [44] |
| OC/recurrent | 40 | Pembrolizumab + bevacizumab + cyclophosphamide | 47.5 | 10 | — | Benefited | Unpublished | |
| NCT02900560 | OC/platinum‐resistant | 34 | Pembrolizumab + azacytidine vs pembrolizumab | — | — | — | — | No data, unpublished |
| NCT03367741 | EC/recurrent | 76 |
1)Nivolumab + cabozantinib 2)Nivolumab |
25.0 16.7 |
5.3 1.9 |
— | Benefited | [45] |
|
CheckMate 358 trial |
CC/recurrent or metastatic | 19 | Nivolumab | 26.0 | — | 21.9 | Benefited | [23] |
| NCT02498600 | OC/persistent or recurrent |
49 51 |
1)Nivolumab 2)Nivolumab + ipilimumab (anti‐CTLA‐4) |
12.2 31.4 |
2 3.9 |
— | Benefited | [38] |
| NCT02873962 | OC/recurrent | 38 | Nivolumab + bevacizumab | 28.9 | 8.1 | Benefited | [34] | |
| NCT02431559 | OC/platinum‐resistant | 40 | Durvalumab + PLD | 15.0 | 5.5 | — | Benefited | [46] |
| NCT02811497 | OC/advanced | 28 | Durvalumab + DNA hypomethylating agent | 7.2 | 1.9 | 5.0 | Not benefited | [47] |
| NCT03899610 | OC/advanced | 23 | Durvalumab + tremelimumab + chemotherapy | 100.0 | — | — | Benefited | [39] |
| NCT02912572 | EC/recurrent or persistent | 33 | Avelumab | 26.7 | — | — | Benefited | [48] |
| NCT02921269 | CC/recurrent | 22 | Atezolizumab + bevacizumab | 0 | 2.9 | 8.9 | Not benefited | [25] |
| NCT03816553 | CC/recurrent, persistent, or metastatic | 45 | Camrelizumab + apatinib | 55.6 | 8.8 | — | Benefited | [49] |
|
OPAL |
OC/recurrent | 41 | Dostarlimab + niraparib + bevacizumab | 17.9 | 7.6 | — | Benefited | [33] |
Abbreviations: CC, cervical cancer; CTLA‐4, cytotoxic T‐lymphocyte‐associated antigen 4; dMMR, deficient mismatch repair; EC, endometrial cancer; mOS, median overall survival; mPFS, median progression‐free survival; No., number of participants; OC, ovarian cancer; PC, paclitaxel + carboplatin; PLD, pegylated liposomal doxorubicin; Refs, references.
TABLE 4.
Ongoing phase III trials of anti‐PD‐1/PD‐L1 in gynecological cancers
| ID | Cancer/condition | No. | Start date | Targeting | Intervention | Status |
|---|---|---|---|---|---|---|
|
ENGOT‐en9 |
EC/recurrent or stage III‐IV | 720 | 2019.4 | PD‐1 + VEGF |
1) Pembrolizumab + lenvatinib 2) Chemotherapy |
Recruiting |
| NCT03914612 | EC/advanced or recurrent | 810 | 2019.7 | PD‐1 |
1) Pembrolizumab + PC 2) Placebo + PC |
Recruiting |
|
Keynote‐B21 |
EC/high risk | 990 | 2020.11 | PD‐1 |
|
Recruiting |
|
China extension study |
EC/ recurrent or stage III‐IV | 875 | 2021.4 | PD‐1 + VEGF |
1) Pembrolizumab + lenvatinib 2) Chemotherapy |
Recruiting |
|
ENGOT‐en15 |
EC/dMMR, advanced or recurrent | 350 | 2022.2 | PD‐1 |
1) Pembrolizumab 2) Chemotherapy |
Recruiting |
|
Keynote‐A18 |
CC/advanced | 980 | 2020.1 | PD‐1 |
|
Recruiting |
|
KEYLYNK‐001/ENGOT‐ov43 |
OC/fist‐line treatment | 1086 | 2018.12 | PD‐1 + PARP |
1) Pembrolizumab + olaparib 2) Pembrolizumab + placebo 3) Placebo + PC + bevacizumab |
Recruiting |
| NCT05092360 | OC/platinum‐resistant | 376 | 2021.10 | PD‐1 + IL‐2 |
1) Pembrolizumab + nemvaleukin 2) Pembrolizumab 3) Nemvaleukin |
Not recruiting |
| NCT04679064 | OC/recurrent | 427 | 2020.12 | PD‐1 + PARP |
1) Pembrolizumab + niraparib 2) PC + bevacizumab |
Recruiting |
|
ATHENA |
OC/stage III‐IV | 1012 | 2018.5 | PD‐1 + PARP |
1) Nivolumab + rucaparib 2) Rucaparib + placebo 3) Nivolumab + placebo 4) Placebo |
Recruiting |
| NCT03353831 | OC/platinum‐resistant | 664 | 2018.9 | PD‐L1 |
1) Atezolizumab 2) Placebo + paclitaxel or PLD |
Recruiting |
| NCT03556839 | CC/stage IVb | 404 | 2018.9 | PD‐L1 |
1) Atezolizumab 2) Placebo + PC+ bevacizumab |
Recruiting |
|
AtTEnd |
EC/advanced | 550 | 2018.10 | PD‐L1 |
1) Atezolizumab 2) Placebo + PC |
Recruiting |
|
DUO‐O |
OC/stage III‐IV | 1056 | 2019.1 | PD‐L1 + PARP |
1) Durvalumab + olaparib 2) Durvalumab + placebo 3) Placebo + PC + bevacizumab |
Recruiting |
|
CALLA |
CC/locally advanced | 714 | 2019.2 | PD‐L1 |
1) Durvalumab 2) Placebo + chemoradiation |
Recruiting |
|
RUBY |
EC/recurrent or stage III‐IV | 470 | 2019.7 | PD‐1 + PARP |
1) Dostarlimab 2) Placebo + PC |
Recruiting |
|
ENGOT‐0 V44 /FIRST |
OC/stage III‐IV | 912 | 2018.10 | PD‐1 + PARP |
|
Recruiting |
|
NSGO/AVANOVA‐Triplet |
OC/platinum‐sensitive | 337 | 2019.6 | PD‐1 + VEGF + PARP |
1) Dostarlimab + niraparib+ bevacizumab 2) Niraparib + bevacizumab 3) Chemotherapy |
Withdrawn |
|
DOMENICA |
EC/dMMR | 142 | 2022.1 | PD‐1 |
|
Not recruiting |
|
FERMATA |
CC/advanced | 316 | 2019.9 | PD‐1 |
|
Recruiting |
Abbreviations: CC, cervical cancer; dMMR, mismatch repair deficient; EC, endometrial cancer; No., number of participants; OC, ovarian cancer; PARPi, poly adenosine diphosphate‐ribose polymerase inhibitor; PC, paclitaxel + carboplatin; PD‐1, programed death protein 1; PD‐L1, programed death protein ligand 1; PLD, pegylated liposomal doxorubicin; Refs, references; VEGFi, vascular endothelial growth factor inhibitor.
2. ENDOMETRIAL CANCER
Endometrial cancer is categorized into four separate molecular subtypes according to The Cancer Genome Atlas (TCGA), as follows: polymerase epsilon (POLE) ultra‐mutated, microsatellite instability hypermutated (MSI‐H), copy‐number low and copy‐number high, each with a distinct prognosis. 8 MSI‐H is a phenotype of the deficient mismatch repair (dMMR) pathway, which accelerates the accumulation of DNA mutations. ICB therapy has shown particular efficacy in solid tumors with MSI‐H, dMMR and/or high concentrations of tumor‐infiltrating lymphocytes.
Pembrolizumab is a humanized monoclonal IgG4 antibody and is a well‐known PD‐1 inhibitor. 9 In May 2017, the FDA granted accelerated approval of pembrolizumab for the treatment of patients with unresectable or metastatic MSI‐H or dMMR solid tumors. The recommended dose is 200 mg intravenously every 3 weeks or 400 mg every 6 weeks. This approval was based on the findings of five clinical trials (KEYNOTE‐016, KEYNOTE‐164, KEYNOTE‐012, KEYNOTE‐028 and KEYNOTE‐158), which included endometrial cancer patients with MSI‐H and/or dMMR. 10 This was the first time that the FDA had approved a cancer treatment based on a common biomarker rather than the origin of the tumor. For patients with advanced endometrial cancer that is not of the MSI‐H or dMMR type, the FDA granted accelerated approval of pembrolizumab combined with lenvatinib, a multikinase inhibitor, in September 2019, based on the findings from a phase II study (KEYNOTE‐146). 11 The goal of a phase III study (KEYNOTE‐775) was to verify the clinical benefits of this accelerated approval. The results of KEYNOTE‐775 demonstrated that endometrial cancer patients receiving pembrolizumab plus lenvatinib after chemotherapy exhibited 2.8 months longer progression‐free survival (PFS), 5.4 months longer overall survival (OS) and 15% higher objective response rate (ORR; the proportion of patients who had a partial or complete response to therapy) than those receiving chemotherapy alone (p < 0.001). 12 Based on these results, the FDA granted full approval to pembrolizumab plus lenvatinib for cases of advanced endometrial cancer in July 2021. Two other phase II trials evaluated the antitumor activity of pembrolizumab in endometrial cancer patients and provided updated results. The first study investigated pembrolizumab as a monotherapy in recurrent cases with dMMR and/or MSI‐H. The median follow‐up time was 25.8 months with an ORR of 58%. Notably, in patients with Lynch‐like syndrome (LLS), the ORR was 100%. 13 The other study explored the addition of pembrolizumab to chemotherapy for advanced or recurrent disease. Results indicated an ORR of 77.8%, with a median PFS of 10.55 months. 14 In addition, three ongoing phase III clinical trials are evaluating the role of pembrolizumab in the treatment of endometrial cancer. Two studies aim to compare the efficacy of pembrolizumab plus lenvatinib in patients with advanced or recurrent endometrial cancer. It is hypothesized that the combination of pembrolizumab and lenvatinib is superior to chemotherapy alone. The other study (Keynote‐B21) is investigating the effect of pembrolizumab plus chemotherapy in newly diagnosed endometrial cancer after curative surgery.
Dostarlimab (TSR‐042) is another PD‐1 monoclonal IgG4 antibody. In April 2021, the FDA granted accelerated approval to dostarlimab for adult patients with recurrent or advanced dMMR endometrial cancer. This approval was based on results from cohort A1 in the GARNET trial, which included 71 patients with dMMR whose cancer had progressed during or after platinum‐containing chemotherapy. The confirmed ORR was 42.3%, the complete response rate was 12.7%, and the partial response rate was 29.6%. 15 An ongoing phase III trial (RUBY) is assessing the efficacy of adding dostarlimab to chemotherapy in patients with advanced or recurrent endometrial cancer. This study is expected to report long‐term data in 2026.
Atezolizumab is a PD‐L1 blocking IgG1 antibody that is used in the treatment of urothelial carcinoma, non‐small cell lung cancer and triple‐negative breast cancer. For endometrial cancer, atezolizumab monotherapy in recurrent disease had an ORR of 13% in a phase Ia study, demonstrating durable clinical benefits. 16 Furthermore, an ongoing phase III trial (AtTEnd/ENGOT‐en7) is currently recruiting women to assess atezolizumab combined with chemotherapy in the treatment of advanced or recurrent endometrial cancer.
Besides atezolizumab, avelumab is another PD‐L1 blocking IgG1 antibody that is used to treat certain types of cancers such as urothelial carcinoma and renal cell carcinoma. For endometrial cancer, a phase II trial for avelumab showed an ORR of 6.25% in patients with microsatellite stable disease and an ORR of 26.7% in patients with MSI or POLE mutated disease. 17 Microsatellite and POLE status appeared to be correlated with avelumab response, even in PD‐L1‐negative patients. An ongoing phase II trial (MITO END‐3) aims to evaluate the activity of avelumab in combination with chemotherapy in patients with advanced or recurrent endometrial cancer. Another phase II trial exploring the efficacy of avelumab combined with talazoparib (a poly [ADP‐ribose] polymerase inhibitor, PARPi) in recurrent endometrial cancer is currently recruiting patients.
Ipilimumab is a CTLA‐4 blocking IgG1 antibody used for the treatment of melanoma and renal cell carcinoma. CTLA‐4 and PD‐1 are two different pathways that regulate the activation of T cells. A combined blockade of CTLA‐4 and PD‐1 has been reported to amplify antitumor T‐cell response and provide synergistic activity. This combination therapy has been investigated in phase III clinical trials for cancer treatment. 18 In July 2018, the FDA granted accelerated approval to the combined use of ipilimumab and nivolumab for the treatment of MSI‐H or dMMR metastatic colorectal cancer based on the CHECKMATE 142 study. 19 This combination of PD‐1 and CTLA‐4 blocking is also being investigated regarding gynecological cancers. In addition, two ongoing phase II trials (NCT05112601, NCT02982486) are focusing on the efficacy of this combination in the treatment of recurrent endometrial cancer with dMMR.
3. CERVICAL CANCER
Cervical cancer is one of the most common gynecological malignancies among women, and persistent human papillomavirus (HPV) infection is involved in its development. Despite significant advances in early detection and prophylactic vaccinations, the poor prognosis for patients with advanced, recurrent or metastasized disease remains a major issue. ICBs are one of the most prominent representatives of novel therapeutics that are being extensively researched in the treatment of cervical cancer.
Pembrolizumab is currently the only FDA‐approved drug for the treatment of cervical cancer. KEYNOTE‐158 is a phase II basket study that investigated the antitumor activity of pembrolizumab in multiple cancer types. The results of this trial showed durable antitumor activity in patients with previously treated advanced cervical cancer. 20 Based on these results, in 2018 the FDA granted accelerated approval of pembrolizumab for patients with advanced PD‐L1‐positive cervical cancer. In September 2021, the results of the KEYNOTE‐826 phase III trial were published. 21 That trial assessed the relative benefits of adding pembrolizumab to chemotherapy with or without bevacizumab, a well‐known antiangiogenic agent, among patients with persistent, recurrent or metastatic cervical cancer. The PFS and OS rates increased significantly in the pembrolizumab group, not only in the PD‐L1‐positive group but also among the intention‐to‐treat population. In the pembrolizumab group, PFS was 2.2 months longer (p < 0.001) than in the placebo group among the PD‐L1‐positive population. Moreover, OS at 24 months was 53.0% with pembrolizumab vs 41.7% without (p < 0.001). 21 Based on these promising results, in October 2021 the FDA approved pembrolizumab combined with chemotherapy for patients with persistent, recurrent or metastatic cervical cancer, whose tumors expressed PD‐L1 with a combined positive score (CPS) of 1 or more. The CPS is defined as the number of PD‐L1‐positive cells divided by the number of viable tumor cells, multiplied by 100. 21 One ongoing phase III trial (Keynote‐A18) is exploring the efficacy of adding pembrolizumab to concurrent chemoradiotherapy in patients with newly diagnosed locally advanced cervical cancer.
Cemiplimab is a high‐affinity PD‐1‐blocking monoclonal IgG4 antibody approved to treat lung and skin cancers, which showed antitumor activity in cervical cancer as well. A phase III trial (EMPOWER‐Cervical 1) revealed that cemiplimab treatment led to a 3.5‐month longer OS (p < 0.001) than chemotherapy among patients with recurrent cervical cancer who had had disease progression after first‐line chemotherapy. As compared with chemotherapy, cemiplimab treatment resulted in a 31% lower risk of death in the overall population. 22
Another anti‐PD‐1 IgG4 antibody, nivolumab, has also been assessed for the treatment of cervical cancer. The CheckMate 358 trial is a phase I/II study that assessed nivolumab monotherapy in patients with virus‐associated tumors. The results of that study in patients with recurrent or metastatic cervical cancer were promising, with an ORR of 26.3% and a median OS of 21.9 months. 23 However, another phase II trial revealed that nivolumab monotherapy exhibited low antitumor activity in persistent or recurrent cervical cancer, with an ORR of only 4% and a median duration of stable disease of 5.7 months. 24
At present, there is limited clinical evidence for using anti‐PD‐L1 agents in the treatment of cervical cancer. Atezolizumab, avelumab and durvalumab are three anti‐PD‐L1 agents that are currently undergoing clinical trials. A phase II trial (NCT02921269) investigated the combined activity of atezolizumab and bevacizumab in the treatment of advanced cervical cancer. However, the combination of bevacizumab and atezolizumab did not meet the predefined efficacy endpoint, with an ORR of 0%. 25 One ongoing phase III trial (NCT0355683) is recruiting patients to determine whether the addition of atezolizumab to front‐line treatments could improve oncological outcomes in patients with metastatic, recurrent or persistent cervical cancer. This study is expected to report mature data in 2023. Another phase II trial (NCT03260023) is evaluating the activity of avelumab combined with TG4001 (an HPV vaccine) in a group of patients with recurrent or metastatic HPV‐16‐positive advanced malignancies. Although durable responses have been observed, 26 patient follow‐up is still ongoing. Durvalumab is a selective, high‐affinity IgG1 monoclonal antibody blocking PD‐L1 that was given accelerated approval by the FDA for treating urothelial carcinoma. Furthermore, a phase III trial (CALLA; NCT03830866) is evaluating the efficacy of adding durvalumab to concurrent chemoradiotherapy in locally advanced cervical cancer.
Concerning anti‐CTLA‐4 agents, a phase I study (GOG‐9929) examined the efficacy of ipilimumab following chemoradiotherapy for newly diagnosed node‐positive HPV‐related disease. 27 Results revealed an increased expression of activation markers on T cells after ipilimumab treatment. The 12‐month OS was 90% and the 12‐month PFS was 81%. 28 These findings suggest that the use of immunotherapy after chemoradiotherapy is effective. A phase II trial (NCT01693783) is in progress to assess the safety of ipilimumab in eligible patients with recurrent or metastatic cervical cancer. Zalifrelimab is a new checkpoint inhibitor (anti‐CTLA‐4) that has emerged as an investigational agent for the treatment of cervical cancer. In addition, a phase II study (GOG‐3028) is evaluating balstilimab (anti‐PD‐1) combined with zalifrelimab in patients with advanced cervical cancer whose condition progressed after first‐line chemotherapy. Initial data from this study demonstrated an ORR of 26.5%. 29
4. OVARIAN CANCER
Ovarian cancer has the highest mortality rate of all gynecological malignancies, and the majority of women with ovarian cancer (more than 70%) are diagnosed at an advanced stage. Moreover, fewer than 30% of these patients will not experience disease recurrence. Furthermore, there is a high frequency of resistance to current treatments among patients with recurrent disease. Although there have been a series of developments in the treatment of ovarian cancer since the approval of PARPi, research into immunotherapy for ovarian cancer is still in its infancy.
As shown by the results of clinical trials, the antitumor activity of anti‐PD‐1 agents has been less satisfactory than expected. In a phase II study (KEYNOTE‐100), pembrolizumab monotherapy did not show any advantage over chemotherapy in advanced and recurrent ovarian cancer. 30 In this study, the ORR was 8% in the pembrolizumab group. However, higher PD‐L1 expression was correlated with a higher response rate, since the ORR was 17.1% in patients with PD‐L1 and CPS ≥10. Another phase II study evaluated the addition of pembrolizumab to chemotherapy in platinum‐resistant recurrent ovarian cancer. 31 That trial was abandoned when researchers discovered that pembrolizumab did not provide better clinical results than chemotherapy alone. Despite the failure of pembrolizumab monotherapy in ovarian cancer, several studies have explored the combination therapy of pembrolizumab with other targeted therapies. For example, the preliminary results of the TOPACIO study showed that a combination of pembrolizumab and niraparib (a PARPi) displayed promising antitumor activity for patients with recurrent ovarian cancer who had limited treatment options. These positive results applied to all patients, regardless of platinum status, biomarker status or prior bevacizumab treatment, thus advocating further investigations. 32 The phase III trial of pembrolizumab plus niraparib in the treatment of recurrent ovarian cancer (NCT04679064) is currently enlisting patients. Another phase III trial (NCT05092360) is investigating the efficacy of pembrolizumab plus nemvaleukin, a novel engineered interleukin‐2 variant immunotherapy, in patients with platinum‐resistant ovarian cancer.
Other anti‐PD‐1 agents, such as dostarlimab and nivolumab, have shown clinical benefits in early phase trials for the treatment of ovarian cancer. A phase II trial assessed the triple therapy effect of dostarlimab, niraparib and bevacizumab in patients with platinum‐resistant ovarian cancer, achieving an ORR of 17.9% and a median PFS of 7.6 months. 33 A further phase III trial (NCT03603859) aims to evaluate first‐line treatment combined with niraparib plus dostarlimab in ovarian cancer. As for nivolumab, a phase II trial assessed its role in the treatment of recurrent ovarian cancer, and the results revealed that the ORR was 28.9% in patients who received combined nivolumab and bevacizumab treatment. 34 This combination treatment had an even higher ORR (40%) in platinum‐sensitive patients. An ongoing phase III trial (NCT03522246) is evaluating nivolumab plus rucaparib (a PARPi) as maintenance treatment following a response to front‐line treatment in newly diagnosed cases of advanced ovarian cancer.
The clinical findings of anti‐PD‐L1 agents in the treatment of ovarian cancer are not encouraging. A phase III trial (IMagyn050) evaluated the addition of atezolizumab to chemotherapy plus bevacizumab in newly diagnosed cases of advanced ovarian cancer. The median PFS was 19.5 months with atezolizumab vs 18.4 months without (p = 0.28). Therefore, this result did not support the use of atezolizumab in newly diagnosed patients. 35 Currently, there are two ongoing phase III trials (NCT02891824 and NCT03353831) investigating the role of atezolizumab in instances of recurrent disease. A phase III study of avelumab combined with chemotherapy for previously untreated disease (JAVELIN Ovarian 100) was terminated in 2018 due to a lack of efficacy. 36 This result does not support the use of avelumab in newly diagnosed cases of ovarian cancer. Another phase III trial (JAVELIN Ovarian 200) focused on avelumab for platinum‐resistant/refractory recurrent disease. Patients were placed in randomized groups to receive treatment with avelumab, avelumab plus pegylated liposomal doxorubicin (PLD), or PLD alone. Results indicated ORR values of 14.3%, 5.6% and 0%, respectively. 37 Thus, this trial did not meet its primary endpoint. A phase II trial (NCT02431559) revealed that the combination of durvalumab and doxorubicin was associated with an ORR of 15% in platinum‐resistant recurrent ovarian cancer. There are also two phase III trials currently investigating durvalumab in gynecological cancers, one of which (DUO‐O; NCT03737643) is exploring the combined treatment of chemotherapy, bevacizumab, durvalumab and a olaparib in ovarian cancer.
The combination therapy of anti‐CTLA‐4 agents with anti‐PD‐1/PD‐L1 agents is also being investigated in clinical trials as a potential treatment strategy for ovarian cancer. A phase II study allocated 100 patients with recurrent or persistent disease to receive either nivolumab or nivolumab plus ipilimumab. 38 Compared with nivolumab alone, the combination treatment resulted in a superior response rate and longer PFS (3.9 vs 2.0 months). Tremelimumab is a monoclonal IgG2 antibody that targets CTLA‐4; a phase II study assessed neoadjuvant chemotherapy plus durvalumab and tremelimumab in the treatment of advanced‐stage ovarian cancer. 39 A complete response to treatment was achieved in 13% of patients, and 87% experienced a partial response. These data highlight the clinical activity of this combination therapy in the treatment of ovarian cancer.
5. SAFETY
Since these anti‐immune agents target immunity, they may result in abnormal immune reactions and generate toxicity that affects the skin, gut, lung, liver and other tissues. Data from one meta‐analysis showed that the most common immune‐related adverse events for pembrolizumab are arthralgia, pneumonitis and hepatic toxicities, for nivolumab they are endocrine toxicities, for atezolizumab they are hypothyroidism, and for ipilimumab they are dermatological, gastrointestinal and renal toxicities. 40 ICBs were discontinued because of adverse reactions in 10% of patients with pembrolizumab and 8.7% of patients with cemipilimab. 12 , 22 However, adverse events that are mostly transient and mild, and do not translate into clinically meaningful differences in health‐related quality of life. The incidence of severe adverse events due to the combination of anti‐CTLA‐4 and anti‐PD‐1 agents is reported to be 55%, 41 which is significantly higher than either agent individually and leads to discontinuation of treatment in one‐third of patients. Nevertheless, more preclinical and clinical investigations are required to elucidate the key mechanisms and predictive biomarkers of the efficacy and safety of these agents and to limit the risk of adverse reaction.
6. CONCLUSIONS
Considering the immune landscape of cervical cancer and the molecular indicators identified in endometrial cancer, we anticipate that ICB therapy will play an important role in the treatment of certain patients. The distinct outcomes among patients with different MMR or PD‐L1 statuses suggest that the key to making progress in ICB therapies is to identify more biomarkers. With the development of HPV therapeutic vaccines, a combination of vaccines and ICBs may be a prospective strategy for treating cervival cancer. Currently, however, the clinical outcomes of ICBs as a primary treatment for ovarian cancer are not promising. Given that PARPi has been a remarkable breakthrough in the treatment of ovarian cancer and is a synergistic partner for ICBs, future clinical trials regarding ovarian cancer should focus on combining ICBs with PARPi therapy and determining the role of ICBs in the treatment of platinum‐resistant recurrent disease. However, the safety profile of these combination therapies represents a new concern that will have to be considered.
AUTHORS' CONTRIBUTIONS
QW and HP did the literature searching and screening. HP drafted the manuscript. QW and XH reviewed and revised the draft. All authors approved the final manuscript.
FUNDING INFORMATION
Department of Science and Technology of Sichuan Province, 2018JY0609.
CONFLICT OF INTEREST
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
Supporting information
Table S1‐S2
Peng H, He X, Wang Q. Immune checkpoint blockades in gynecological cancers: A review of clinical trials. Acta Obstet Gynecol Scand. 2022;101:941‐951. doi: 10.1111/aogs.14412
REFERENCES
- 1. Zahn LM. Effects of the tumor microenvironment. Science. 2017;355:1386‐1388. [DOI] [PubMed] [Google Scholar]
- 2. Neoadjuvant PD‐1 Blockade in Resectable Lung Cancer; Nivolumab and ipilimumab in advanced melanoma; overall survival with combined nivolumab and ipilimumab in advanced melanoma; prolonged survival in stage III melanoma with ipilimumab adjuvant therapy; combined nivolumab and ipilimumab or monotherapy in untreated melanoma; combined nivolumab and ipilimumab or monotherapy in untreated melanoma; nivolumab and ipilimumab versus ipilimumab in untreated melanoma; rapid eradication of a bulky melanoma mass with one dose of immunotherapy; genetic basis for clinical response to CTLA‐4 blockade; genetic basis for clinical response to CTLA‐4 blockade in melanoma; nivolumab plus ipilimumab in advanced melanoma; safety and tumor responses with lambrolizumab (anti‐PD‐1) in melanoma; hepatotoxicity with combination of vemurafenib and ipilimumab. N Engl J Med. 2018;379(22):2185. [DOI] [PubMed] [Google Scholar]
- 3. Oyewole‐Said D, Konduri V, Vazquez‐Perez J, Weldon SA, Levitt JM, Decker WK. Beyond T‐cells: functional characterization of CTLA‐4 expression in immune and non‐immune cell types. Front Immunol. 2020;11:608024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Vogel I, Kasran A, Cremer J, et al. CD28/CTLA‐4/B7 costimulatory pathway blockade affects regulatory T‐cell function in autoimmunity. Eur J Immunol. 2015;45:1832‐1841. [DOI] [PubMed] [Google Scholar]
- 5. Chaudhri A, Xiao Y, Klee AN, Wang X, Zhu B, Freeman GJ. PD‐L1 binds to B7‐1 only in cis on the same cell surface. Cancer Immunol Res. 2018;6:921‐929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Satelli A, Batth IS, Brownlee Z, et al. Potential role of nuclear PD‐L1 expression in cell‐surface vimentin positive circulating tumor cells as a prognostic marker in cancer patients. Sci Rep. 2016;6:28910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Jia L, Gao Y, Zhou T, et al. Enhanced response to PD‐L1 silencing by modulation of TME via balancing glucose metabolism and robust co‐delivery of siRNA/resveratrol with dual‐responsive polyplexes. Biomaterials. 2021;271:120711. [DOI] [PubMed] [Google Scholar]
- 8. Batte BA, Bruegl AS, Daniels MS, et al. Consequences of universal MSI/IHC in screening ENDOMETRIAL cancer patients for lynch syndrome. Gynecol Oncol. 2014;134:319‐325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Taylor MH, Betts CB, Maloney L, et al. Safety and efficacy of pembrolizumab in combination with Acalabrutinib in advanced head and neck squamous cell carcinoma: phase 2 proof‐of‐concept study. Clin Cancer Res. 2022;28:903‐914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Marabelle A, Le DT, Ascierto PA, et al. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/mismatch repair‐deficient cancer: results from the phase II KEYNOTE‐158 study. J Clin Oncol. 2020;38:1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Makker V, Rasco D, Vogelzang NJ, et al. Lenvatinib plus pembrolizumab in patients with advanced endometrial cancer: an interim analysis of a multicentre, open‐label, single‐arm, phase 2 trial. Lancet Oncol. 2019;20:711‐718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Makker V, Colombo N, Casado Herráez A, et al. O008/#785 a multicenter, open‐label, randomized, phase 3 study to compare the efficacy and safety of lenvatinib in combination with pembrolizumab vs treatment of physician's choice in patients with advanced endometrial cancer: study 309/keynote‐775. Int J Gynecol Cancer. 2021;31:A4‐A5. [Google Scholar]
- 13. Bellone S, Roque DM, Siegel ER, et al. A phase II evaluation of pembrolizumab in recurrent microsatellite instability‐high (MSI‐H) endometrial cancer patients with lynch‐like versus MLH‐1 methylated characteristics (NCT02899793). Ann Oncol. 2021;32:1045‐1046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Pineda MJ, Schilder J, Hill EK, et al. A big ten cancer research consortium phase II trial of pembrolizumab with carboplatin and paclitaxel for advanced or recurrent endometrial cancer. J Clin Oncol. 2020;38:6022. [Google Scholar]
- 15. Oaknin A, Tinker AV, Gilbert L, et al. Clinical activity and safety of the anti‐PD‐1 monoclonal antibody dostarlimab for patients with recurrent or advanced dMMR endometrial cancer. Future Oncol. 2021;17:3781‐3785. [DOI] [PubMed] [Google Scholar]
- 16. Liu JF, Gordon M, Veneris J, et al. Safety, clinical activity and biomarker assessments of atezolizumab from a phase I study in advanced/recurrent ovarian and uterine cancers. Gynecol Oncol. 2019;154:314‐322. [DOI] [PubMed] [Google Scholar]
- 17. Konstantinopoulos PA, Luo W, Liu JF, et al. Phase II study of Avelumab in patients with mismatch repair deficient and mismatch repair proficient recurrent/persistent endometrial cancer. J Clin Oncol. 2019;37:2786‐2794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Rizvi NA, Cho BC, Reinmuth N, et al. Durvalumab with or without Tremelimumab vs standard chemotherapy in first‐line treatment of metastatic non–small cell lung cancer: the MYSTIC phase 3 randomized clinical trial. JAMA Oncol. 2020;6:661‐674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Morse MA, Overman MJ, Hartman L, et al. Safety of nivolumab plus low‐dose ipilimumab in previously treated microsatellite instability‐high/mismatch repair‐deficient metastatic colorectal cancer. Oncologist. 2019;24:1453‐1461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Chung HC, Ros W, Delord JP, et al. Efficacy and safety of pembrolizumab in previously treated advanced cervical cancer: results from the phase II KEYNOTE‐158 study. J Clin Oncol. 2019;37:1470‐1478. [DOI] [PubMed] [Google Scholar]
- 21. Colombo N, Dubot C, Lorusso D, et al. Pembrolizumab for persistent, recurrent, or metastatic cervical cancer. New Engl J Med. 2021;385:1856‐1867. [DOI] [PubMed] [Google Scholar]
- 22. Tewari KS, Monk BJ, Vergote I, et al. Survival with Cemiplimab in recurrent cervical cancer. N Engl J Med. 2022;386:544‐555. [DOI] [PubMed] [Google Scholar]
- 23. Naumann RW, Hollebecque A, Meyer T, et al. Safety and efficacy of nivolumab monotherapy in recurrent or metastatic cervical, vaginal, or vulvar carcinoma: results from the phase I/II CheckMate 358 trial. J Clin Oncol. 2019;37:2825‐2834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Santin AD, Deng W, Frumovitz M, et al. Phase II evaluation of nivolumab in the treatment of persistent or recurrent cervical cancer (NCT02257528/NRG‐GY002). Gynecol Oncol. 2020;157:161‐166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Friedman CF, Snyder Charen A, Zhou Q, et al. Phase II study of atezolizumab in combination with bevacizumab in patients with advanced cervical cancer. J Immunother Cancer. 2020;8:e001126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Tourneau CL, Cassier P, Rolland F, et al. 793 TG4001 (Tipapkinogene sovacivec) and avelumab for recurrent/metastatic (R/M) human papilloma virus (HPV)‐16+ cancers: clinical efficacy and immunogenicity. J Immunother Cancer. 2020;8(3):A474. [Google Scholar]
- 27. Da Silva DM, Enserro DM, Mayadev JS, et al. Immune activation in patients with locally advanced cervical cancer treated with ipilimumab following definitive chemoradiation (GOG‐9929). Clin Cancer Res. 2020;26:5621‐5630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Mayadev JS, Enserro D, Lin YG, et al. Sequential ipilimumab after chemoradiotherapy in curative‐intent treatment of patients with node‐positive cervical cancer. JAMA Oncol. 2020;6:92‐99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. O'Malley DM, Randall LM, Jackson CG, et al. RaPiDS (GOG‐3028): randomized phase II study of balstilimab alone or in combination with zalifrelimab in cervical cancer. Future Oncol. 2021;17:3433‐3443. [DOI] [PubMed] [Google Scholar]
- 30. Matulonis UA, Shapira‐Frommer R, Santin AD, et al. Antitumor activity and safety of pembrolizumab in patients with advanced recurrent ovarian cancer: results from the phase II KEYNOTE‐100 study. Ann Oncol. 2019;30:1080‐1087. [DOI] [PubMed] [Google Scholar]
- 31. Walsh CS, Kamrava M, Rogatko A, et al. Phase II trial of cisplatin, gemcitabine and pembrolizumab for platinum‐resistant ovarian cancer. PLoS One. 2021;16:e0252665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Konstantinopoulos PA, Waggoner S, Vidal GA, et al. Single‐arm phases 1 and 2 trial of niraparib in combination with pembrolizumab in patients with recurrent platinum‐resistant ovarian carcinoma. JAMA Oncol. 2019;5:1141‐1149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Liu J, Gaillard S, Hendrickson AW, et al. An open‐label phase II study of dostarlimab (TSR‐042), bevacizumab (bev), and niraparib combination in patients (pts) with platinum‐resistant ovarian cancer (PROC): cohort a of the OPAL trial. Gynecol Oncol. 2021;162:S17‐S18. [Google Scholar]
- 34. Liu JF, Herold C, Luo W, et al. A phase II trial of combination nivolumab and bevacizumab in recurrent ovarian cancer. Ann Oncol. 2018;29:viii334‐viii335. [Google Scholar]
- 35. Moore KN, Bookman M, Sehouli J, et al. Atezolizumab, bevacizumab, and chemotherapy for newly diagnosed stage III or IV ovarian cancer: placebo‐controlled randomized phase III trial (IMagyn050/GOG 3015/ENGOT‐OV39). J Clin Oncol. 2021;39:1842‐1855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Monk BJ, Colombo N, Oza AM, et al. Chemotherapy with or without avelumab followed by avelumab maintenance versus chemotherapy alone in patients with previously untreated epithelial ovarian cancer (JAVELIN ovarian 100): an open‐label, randomised, phase 3 trial. Lancet Oncol. 2021;22:1275‐1289. [DOI] [PubMed] [Google Scholar]
- 37. Pujade‐Lauraine E, Fujiwara K, Dychter SS, Devgan G, Monk BJ. Avelumab (anti‐PD‐L1) in platinum‐resistant/refractory ovarian cancer: JAVELIN ovarian 200 phase III study design. Future Oncol. 2018;14:2103‐2113. [DOI] [PubMed] [Google Scholar]
- 38. Zamarin D, Burger RA, Sill MW, et al. Randomized phase II trial of nivolumab versus nivolumab and ipilimumab for recurrent or persistent ovarian cancer: an NRG oncology study. J Clin Oncol. 2020;38:1814‐1823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Lee JY, Kim JW, Lim MC, et al. A phase II study of neoadjuvant chemotherapy plus durvalumab and tremelimumab in advanced‐stage ovarian cancer: a Korean gynecologic oncology group study (KGOG 3046), TRU‐D. J Gynecol Oncol. 2019;30:e112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Ramos‐Casals M, Brahmer JR, Callahan MK, et al. Immune‐related adverse events of checkpoint inhibitors. Nat Rev Dis Primers. 2020;6:38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Kumar V, Chaudhary N, Garg M, Floudas CS, Soni P, Chandra AB. Current diagnosis and Management of Immune Related Adverse Events (irAEs) induced by immune checkpoint inhibitor therapy. Front Pharmacol. 2017;8:49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Piulats J, Fariñas‐Madrid L, Santacana M, et al. 731 biomarker analysis of the phase 2 study of pembrolizumab in combination with doxorubicin in advanced endometrial cancer: TOPIC trial/VHIO10001. Int J Gynecol Cancer. 2021;31(Suppl 3):A118‐A119. [Google Scholar]
- 43. Lee EK, Xiong N, Cheng SC, et al. Combined pembrolizumab and pegylated liposomal doxorubicin in platinum resistant ovarian cancer: a phase 2 clinical trial. Gynecol Oncol. 2020;159:72‐78. [DOI] [PubMed] [Google Scholar]
- 44. Matei D, Pant A, Moroney JW, et al. Phase II trial of guadecitabine priming and pembrolizumab in platinum resistant recurrent ovarian cancer. J Clin Oncol. 2020;38(15_suppl):6025. [Google Scholar]
- 45. Lheureux S, Matei D, Konstantinopoulos PA, et al. A randomized phase II study of cabozantinib and nivolumab versus nivolumab in recurrent endometrial cancer. J Clin Oncol. 2020;38:6010. [Google Scholar]
- 46. O'Cearbhaill RE, Wolfer A, Disilvestro P, et al. A phase I/II study of chemo‐immunotherapy with durvalumab (durva) and pegylated liposomal doxorubicin (PLD) in platinum‐resistant recurrent ovarian cancer (PROC). Ann Oncol. 2018;29:viii337. [Google Scholar]
- 47. Taylor K, Loo Yau H, Chakravarthy A, et al. An open‐label, phase II multicohort study of an oral hypomethylating agent CC‐486 and durvalumab in advanced solid tumors. J Immunother Cancer. 2020;8:e000883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Konstantinopoulos PA, Liu JF, Luo W, et al. Phase 2, two‐group, two‐stage study of avelumab in patients (pts) with microsatellite stable (MSS), microsatellite instable (MSI), and polymerase epsilon (POLE) mutated recurrent/persistent endometrial cancer (EC). J Clin Oncol. 2019;37(15_suppl):5502. [Google Scholar]
- 49. Lan C, He M, Peng H, et al. Genomic profiling of advanced cervical cancer to predict response to PD‐1 inhibitor combination therapy: a secondary analysis of the CLAP trial. Gynecol Oncol. 2021;162:S28. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1‐S2