

Abstract
BACKGROUND
Several interventions and techniques are suggested to improve the outcome of embryo transfer (ET) in assisted conception. However, there remains no consensus on the optimal practice, with high variations among fertility specialists.
OBJECTIVE AND RATIONALE
We conducted a comprehensive systematic review and meta-analyses of randomized controlled trials (RCTs) aiming to identify effective interventions that could be introduced around the time of ET to improve reproductive outcomes.
SEARCH METHODS
We searched the electronic databases (MEDLINE, EMBASE and Cochrane CENTRAL) from inception until March 2021 using a multi-stage search strategy of MeSH terms and keywords, and included all RCTs that evaluated an intervention in the 24-h period before/after ET in women undergoing IVF/ICSI. Our primary outcome was clinical pregnancy rate post-ET confirmed as viable pregnancy on ultrasound scan. We assessed the risk of bias in included trials and extracted data in duplicate. We pooled data using a random-effect meta-analysis and reported using risk ratio (RR) with 95% CI. We explored publication bias and effect modifiers using subgroup analyses.
OUTCOMES
Our search yielded 3685 citations of which we included 188 RCTs (38 interventions, 59 530 participants) with a median sample size of 200 (range 26–1761). The quality of included RCTs was moderate with most showing a low risk of bias for randomization (118/188, 62.8%) and attrition (105/188, 55.8%) but there was a significant risk of publication bias (Egger’s test P = 0.001). Performing ET with ultrasound guidance versus clinical touch (n = 24, RR 1.265, 95% CI 1.151–1.391, I2 = 38.53%), hyaluronic acid versus routine care (n = 9, RR 1.457, 95% CI 1.197–1.261, I2 = 46.48%) and the use of a soft versus hard catheter (n = 27, RR 1.122, 95% CI 1.028–1.224, I2 = 57.66%) led to higher clinical pregnancy rates. Other pharmacological add-ons also showed a beneficial effect including granulocyte colony-stimulating factor (G-CSF: n = 4, RR 1.774, 95% CI 1.252–2.512, I2 = 0), Atosiban (n = 7, RR 1.493, 95% CI 1.184–1.882, I2 = 68.27%) and hCG (n = 17, RR 1.232, 95% CI 1.099–1.382, I2 = 57.76%). Bed rest following ET was associated with a reduction in clinical pregnancy (n = 6, RR 0.857, 95% CI 0.741–0.991, I2 = 0.01%). Other commonly used interventions, such as non-steroidal anti-inflammatory drugs, prophylactic antibiotics, acupuncture and cervical mucus removal, did not show a significant benefit on reproductive outcomes. Our effect estimates for other important outcomes, including miscarriage and live birth, were limited by the varied reporting across included RCTs.
WIDER IMPLICATIONS
Using ultrasound guidance, soft catheters and hyaluronic acid at the time of ET appears to increase clinical pregnancy rates. The use of Atosiban, G-CSF and hCG showed a trend towards increased clinical pregnancy rate, but larger trials are required before adopting these interventions in clinical practice. Bed rest post-ET was associated with a reduction in clinical pregnancy and should not be recommended.
Keywords: embryo transfer, assisted conception, IVF, ICSI, systematic review, meta-analysis
Introduction
Rapid developments in ART offered hope to many subfertile couples, with more than 8 million ART babies conceived worldwide (Steptoe and Edwards, 1978; Zegers-Hochschild et al., 2009; Cardona Barberán et al., 2020). ART treatments are complex, comprising several interrelated steps often with high stress and psychological bearings on couples under treatment (Malina and Pooley, 2017). Numerous interventions or ‘add-on’ therapies have been introduced over the last few decades to optimize the outcome of ART treatments and assisted conception rates (Farquhar, 2019). However, the effectiveness and safety of several add-ons remain unclear raising concerns about patients’ safety and the vulnerability to profiteering (Galiano et al., 2021).
Embryo transfer (ET) is a crucial component to the success of ART treatments (Mains and van Voorhis, 2010). While seemingly a simple procedure, ET is operator dependent with suboptimal practice often linked to cycle failure and reduced pregnancy rates (Yao et al., 2009a). Some add-ons are proposed at the time of ET to increase the chances of conception, such as the use of ultrasound guidance (Cozzolino et al., 2018), pharmacological interventions aimed to minimize uterine contractility at the time of the transfer (Ng et al., 2019; Schwarze et al., 2020) and also pre-transfer acupuncture and relaxation techniques (Smith et al., 2019). Currently, the practice of ET varies among fertility specialists with no consensus on the optimal ET technique (Nancarrow et al., 2021).
The American Society for Reproductive Medicine (ASRM) guideline recommends several ET techniques and add-ons including the use of ultrasound guidance, soft catheters and avoidance of bed rest (Penzias et al., 2017a). Since its publication in 2016, several new add-ons have been proposed, with more than 20 relevant randomized controlled trials (RCTs) reported. Contemporary evidence synthesis is, therefore, needed to inform and update the current knowledge gap on ET practice.
To address this research need, we conducted a comprehensive systematic review and meta-analyses of randomized trials evaluating any intervention introduced at the time of ET to improve reproductive outcomes in couples undergoing ART.
Methods
We conducted a systematic review using a prospectively registered protocol (PROSPERO: CRD42020216199) and reported in line with established guidelines (Page et al., 2021).
Search strategy
We searched the electronic databases (MEDLINE, EMBASE and Cochrane CENTRAL) from inception until March 2021 for all RCTs that evaluated an intervention introduced at the time of ET in women undergoing ART treatment. We used a multi-stage search strategy using MeSH terms and keywords, and combined them using the Boolean operators AND/OR to identify relevant citations (Supplementary Data). We did not apply any search filters or language restrictions. We screened the bibliographies of relevant articles and performed complementary searches in Google Scholar and Scopus to identify any missed citations and grey literature.
Review selection and inclusion process
Two authors (B.T. and H.W.) independently screened the titles and abstracts to identify relevant citations. Full-text articles were then screened against our inclusion criteria. Any discrepancies were resolved through consultation with the senior author (B.H.A.). We included all RCTs that evaluated any clinical intervention introduced at the time of ET (within 24 h of the procedure) following any ART treatment (IVF and/or ICSI) with the aim to improve implantation rate irrespective of the cause of subfertility. Interventions were defined as ‘add-ons’ if they were introduced as supplementary to a standardized ART protocol in both groups of comparisons in the 24-h period before/after ET. Comparison groups in included trials received the same ART protocol versus control with no additional treatment (standard care), placebo or sham treatment.
Studies reporting intra-uterine sperm injection or ovulation induction treatments were excluded. Articles not in English were translated and included if deemed relevant. We also excluded quasi, non-randomized, observational and animal studies. Review articles and RCTs that did not report on any reproductive outcomes were also excluded.
Data extraction
Data extraction was performed in duplicate (B.T. and H.W.) using a piloted electronic data collection tool with the following characteristics collected: study publication year and journal, inclusion–exclusion criteria, type of intervention and comparison evaluated, characteristics of the included study population and the evaluated ART treatments and all reproductive outcomes.
Our primary outcome was clinical pregnancy rate post-ET confirmed as viable pregnancy on ultrasound scan. We also reported live birth, ongoing pregnancy (a viable pregnancy beyond 12 weeks of gestation) and on biochemical pregnancy (confirmed with a positive βhCG test).
Quality assessment and confidence of evidence
The quality of published literature was assessed by two independent reviewers (B.T. and H.W.) using the Cochrane Risk of Bias assessment tool (ROB2; Sterne et al., 2019). Studies were assessed in five domains: randomization process (randomization bias), deviations from intended interventions (allocation bias), performance bias, missing outcome data (attrition bias), measurement of the outcome (detection bias) and selection of the reported result (reporting bias). Each domain was assessed to have a high, medium or low risk of bias. Due to the nature of the intervention, we did not penalize unblinded trials but reported on assessors blinding. In case of uncertainty, consensus was established with input from a third reviewer (J.T.).
We employed the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach (GRADE Working Group, 2004) to evaluate the confidence in available evidence for each intervention and aid translation into clinical practice. Two independent reviewers (H.W. and J.T.) assessed the certainty of the evidence for the following domains: risk of bias in primary studies for each intervention, inconsistency across included trials, indirectness or imprecision in the pooled effect estimates. A final overall assessment was made for each intervention as high, moderate, low or very low in consultation with a third reviewer (B.H.A.).
Statistical analysis
We reported on dichotomous outcomes using summary risk ratio (RR) with 95% CI and continuous outcomes using weighted mean difference. We pooled data using a random-effect meta-analysis and applied a restricted maximum likelihood model (Lin et al., 2013). Study heterogeneity among included trials was assessed using the I2 statistics. We also assessed the publication bias and small study effect using a funnel plot for each pairwise comparison and performed Egger’s test to assess its statistical significance (Sterne and Harbord, 2004). We planned a sensitivity meta-regression and subgroup analyses to investigate potential effect modifiers where relevant (Harbord and Higgins, 2009). All statistical analyses were conducted in Stata V13 (StataCorp, TX, USA) and Open Meta-analyst software (Brown University; Providence, RI, USA).
Results
Our electronic search identified 3685 titles and abstracts of which we screened 228 articles in full against our inclusion criteria. We identified a further 65 additional records from screening bibliographies and supplementary searches. In total, we included 188 RCTs reporting on 59 530 participants (Fig. 1). The median sample size across the studies was 200 (range 26–1761). About half of the included studies were conducted in European countries (62/188, 33%) followed by the USA (23/188, 12.2%) and Iran (17/188, 9%). More than a third of included studies performed an ET at Day 2–3 (cleavage stage; 76/188, 40.4%), 8.5% at Day 5–6 (blastocyst; 16/188, 8.5%) and a third did not specify (69/188, 36.7%). Most studies performed a fresh ET (96/188, 51.1%), about a 10th performed either a frozen or fresh ET (21/188, 11.2%; Supplementary Tables SI and SII).
Figure 1.

Selection and inclusion process for randomized controlled trials evaluating interventions at the time of embryo transfer in women undergoing assisted reproduction.
Quality assessment
Overall, the quality of included RCTs was moderate with most studies assessed as low risk of bias for randomization (118/188, 62.8%) and attrition (105/188, 56.4%). Almost half of the studies were at low risk of bias for outcome reporting (85/188, 45.2%) and one-third were low risk for allocation (58/188, 30.9%) and detection bias (62/188 33.0%). Performance bias was judged to be high in one-third of the included studies (54/188, 28.7%; Fig. 2).
Figure 2.

Risk of bias in included randomized controlled trials evaluating interventions at the time of embryo transfer in women undergoing assisted reproduction.
Our funnel plots showed significant variations in effect size and standard error across included RCTs with evidence of small study effect (Fig. 3). We explored this further by removing interventions that were evaluated by a single RCT, which reduced the distribution of the funnel plot (Supplementary Fig. S1). Egger’s test showed significant publication bias with a P-value of 0.001.
Figure 3.
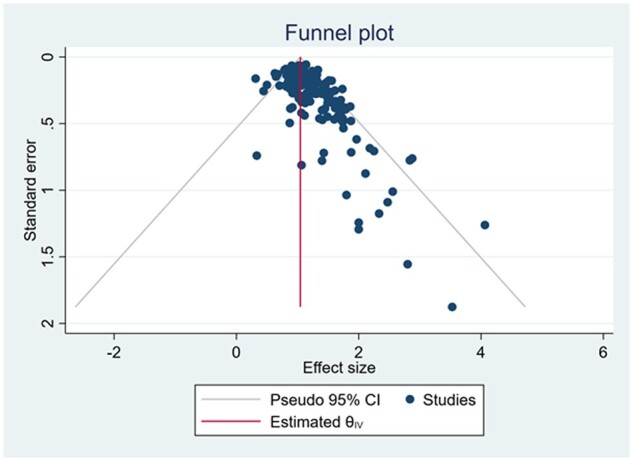
Funnel plot evaluating the risk of publication bias in randomized controlled trials evaluating interventions at the time of embryo transfer in women undergoing assisted reproduction.
Pharmacological interventions
Antibiotics
We identified two RCTs that evaluated the effects of using antibiotics at the time of ET (Peikrishvili et al., 2004; Brook et al., 2006; n = 625 participants). The pooled effect estimate showed no significant benefit for the use of antibiotics compared to standard care on the rate of clinical pregnancy (RR 1.008, 95% CI 0.812–1.251, I2 = 0; Supplementary Fig. S2a). Ongoing pregnancy and miscarriage were reported only in one study (Peikrishvili et al., 2004) showing no significant benefit (RR 0.840, 95% CI 0.570–1.239 and RR 1.255, 95% CI 0.499–3.157, respectively).
Atosiban
Seven RCTs assessed the effectiveness of Atosiban to promote uterine relaxation at the time of ET (Ahn et al., 2009; Moraloglu et al., 2010; Song et al., 2013; Ng et al., 2014; He et al., 2016; Hebisha et al., 2016; Yuan et al., 2019) using varied doses and preparations (n = 1646 participants). The pooled effect estimate showed a significant increase in clinical pregnancy with the use of Atosiban compared to placebo (RR 1.493, 95% CI 1.184–1.882, I2 = 68.27%; Supplementary Fig. S3a).
Ongoing pregnancy was shown to increase with the use of Atosiban in three RCTs (RR 1.137, 95% CI 1.007, 1.283, P = 0.435, I2 = 0%; Ng et al., 2014; Visnova et al., 2018; Bosch et al., 2019) while there was no significant effect on live birth (n = 1, RR 1.05, 95% CI 0.879–1.240; Ng et al., 2014), miscarriage (n = 5, RR 1.080, 95% CI 0.748–1.561, I2 = 0%; 24, 26–29) or biochemical pregnancy (n = 2, RR 1.741, 95% CI 0.664–4.567, I2 = 92.92%; 27, 29; Supplementary Fig. S3b–d).
A subgroup analysis showed a persistent improvement in clinical pregnancy associated with the use of a medium dose Atosiban (35–50 mg; n = 5, RR 1.591, 95% CI 1.110–1.714, I2 = 76.68%; Ahn et al., 2009; Moraloglu et al., 2010; Song et al., 2013; Ng et al., 2014; Yuan et al., 2019) and as well as a low dose (5–10 mg; n = 2, RR 1.380, 95% CI 1.110–1.714, I2 = 68.27%; He et al., 2016; Hebisha et al., 2016; Supplementary Fig. S3e).
Nifedipine
Only one study with low risk of bias evaluated the use of Nifedipine for uterine relaxation at the time of ET (Ng et al., 2019). There was no improvement in clinical pregnancy (RR 1.115, 95% CI 0.548–2.267), live birth (RR 1.115, 95% CI 0.548–2.267) or miscarriage (RR 1.022, 95% CI 0.105–6.951) with using Nifedipine compared to placebo.
Non-steroidal anti-inflammatory drugs
We identified seven studies that evaluated the use of different non-steroidal anti-inflammatory drugs (NSAIDs) at the time of ET, including Piroxicam (n = 4; Moon et al., 2004; Dehghani Firouzabadi et al., 2006; Prato and Borini, 2009; Zarei et al., 2021), Indomethacin (n = 1; Bernabeu et al., 2006), Aspirin (n = 1; Duvan et al., 2006) and Ibuprofen (n = 1; Fekih et al., 2013). A pooled effect estimates for all types of NSAIDs (n = 1207 participants) showed no significant effect on clinical pregnancy (RR 1.294, 95% CI 0.973–1.721, I2 = 63.92%; Supplementary Fig. S4a), miscarriage (n = 4, RR 0.787, 95% CI 0.391–1.582, I2 = 0%; Dehghani Firouzabadi et al., 2006; Prato and Borini, 2009; Fekih et al., 2013; Zarei et al., 2021) and biochemical pregnancy (n = 5, RR 1.032, 95% CI 0.840–1.268, I2 = 26.69%; Bernabeu et al., 2006; Dehghani Firouzabadi et al., 2006; Duvan et al., 2006; Prato and Borini, 2009; Zarei et al., 2021; Supplementary Fig. S4b and c). Subgroup meta-analyses per type of NSAIDs showed similar results with no overall benefit (Supplementary Fig. S4d).
Steroids
Only one study evaluated the effect of Prednisone on reproductive outcomes at the time of ET (Duvan et al., 2006) which had no significant effect on clinical pregnancy (RR 1.064, 95% CI 0.484–2.337).
hCG
Supplementing hCG at the time of ET was the most commonly evaluated pharmacological intervention in 17 RCTs, given as an intrauterine infusion with or without embryo culture media (Mansour et al., 2011; Cambiaghi et al., 2013; Leao et al., 2013; HoNg et al., 2014; Santibañez et al., 2014; Singh and Singh, 2014; Zarei et al., 2014; Aaleyasin et al., 2015; Wirleitner et al., 2015a,b; Dehghani Firouzabadi et al., 2016; Eskandar et al., 2016; Hosseini et al., 2016; Mostajeran et al., 2017; Hafezi et al., 2018; Laokirkkiat et al., 2019; WaNg et al., 2019; Supplementary Fig. S5a). The pooled data showed a significant increase in clinical pregnancy with hCG use (n = 17, RR 1.232, 95% CI 1.099–1.382, I2 = 57.76%).
We pooled data from nine RCTs that evaluated the provision of intrauterine hCG compared to standard care, which showed a significant improvement in clinical pregnancy with hCG use (n = 9, RR 1.269, 95% CI 1.092–1.474, I2 = 43.92%; Mansour et al., 2011; Cambiaghi et al., 2013; Leao et al., 2013; Santibañez et al., 2014; Dehghani Firouzabadi et al., 2016; Eskandar et al., 2016; Hosseini et al., 2016; Mostajeran et al., 2017; WaNg et al., 2019). Eight of the included studies compared hCG injections to a controlled intrauterine injection of embryo culture medium, which did not show a significant improvement in clinical pregnancy rates (n = 8, 1.193, 95% CI 0.996–1.428, I2 = 69.7%; HoNg et al., 2014; Singh and Singh, 2014; Zarei et al., 2014; Aaleyasin et al., 2015; Wirleitner et al., 2015a,b; Hafezi et al., 2018; Laokirkkiat et al., 2019; Supplementary Fig. S5g).
Overall, hCG supplementation did not significantly increase live birth (n = 7, RR 1.132, 95% CI 0.924–1.387, I2 = 73.37%; Supplementary Fig. S5e; Mansour et al., 2011; Singh and Singh, 2014; Aaleyasin et al., 2015; Wirleitner et al., 2015a,b; Hafezi et al., 2018; Laokirkkiat et al., 2019), ongoing pregnancy (n = 2, RR 1.339, 95% CI 0.947–1.893, I2 = 78.24%; Supplementary Fig. S5c; HoNg et al., 2014; Aaleyasin et al., 2015), or miscarriage rates (n = 9, RR 1.092, 95% CI 0.846–1.408, I2 = 0%; Supplementary Fig. S5d; Mansour et al., 2011; HoNg et al., 2014; Singh and Singh, 2014; Zarei et al., 2014; Aaleyasin et al., 2015; Wirleitner et al., 2015a,b; Dehghani Firouzabadi et al., 2016; Hosseini et al., 2016; Hafezi et al., 2018). However, there was a significant increase in biochemical pregnancy rate (n = 5, RR 1.241, 95% CI 1.012–1.521, I2 = 70.33%; Supplementary Fig. S5b; Santibañez et al., 2014; Aaleyasin et al., 2015; Wirleitner et al., 2015a; Hafezi et al., 2018; Laokirkkiat et al., 2019). Several hCG doses were used ranging from 100 to 6500 IU (Supplementary Table SI). However, the most commonly used dose was 500 IU (dissolved in embryo culture medium) evaluated in 15 studies, which showed a consistent increase in clinical pregnancy rates (n = 15, RR 1.275, 95% CI 1.119, 1.4521, I2 = 60.05%; Supplementary Fig. S5f; Mansour et al., 2011; Cambiaghi et al., 2013; Leao et al., 2013; HoNg et al., 2014; Santibañez et al., 2014; Singh and Singh, 2014; Aaleyasin et al., 2015; Wirleitner et al., 2015a,b; Dehghani Firouzabadi et al., 2016; Eskandar et al., 2016; Hosseini et al., 2016; Hafezi et al., 2018; Laokirkkiat et al., 2019; WaNg et al., 2019).
Hyaluronic acid
In total, nine RCTs evaluated the use of hyaluronic acid (HA) at the time of ET compared to no intervention/placebo (Feichtinger et al., 1992; Simon et al., 2003; Friedler et al., 2005, 2007; Korosec et al., 2007; Mahani and Davar, 2007; Tomari et al., 2014; Fasano et al., 2016; Perez et al., 2019). The random-effect meta-analysis showed a significant increase in clinical pregnancy with the administration of HA versus placebo (RR 1.457, 95% CI 1.197–1.261, I2 = 46.48%; Fig. 4a;Feichtinger et al., 1992; Simon et al., 2003; Friedler et al., 2005, 2007; Korosec et al., 2007; Mahani and Davar, 2007; Tomari et al., 2014; Fasano et al., 2016; Perez et al., 2019). Compared to no intervention, HA was seen to significantly increase live birth rate (n = 4, RR 1.471, 95% CI 1.092–1.982, I2 = 4.89%; Fig. 4b;Supplementary Fig. S6c; Simon et al., 2003; Korosec et al., 2007; Kandari, 2019; Perez et al., 2019), but did not affect ongoing pregnancy rate (n = 4, RR 1.170, 95% CI 0.894–1.532, I2 = 0.01%; Supplementary Fig. S6b; Feichtinger et al., 1992; Simon et al., 2003; Friedler et al., 2007; Korosec et al., 2007).
Figure 4.

Summary forest plots of effect estimates of evaluated interventions at the time of embryo transfer on the reproductive outcomes in women undergoing assisted reproduction. G-CSF, granulocyte colony-stimulating factor; TA, transabdominal; TV, transvaginal; CT, computerized tomography; NSAID, non-steroidal anti-inflammatory drug; RCT, randomized controlled trial; HA, hyaluronic acid.
Twelve RCTs compared the use of a high- versus low-dose HA at the time of ET (Schoolcraft et al., 2002; Balaban et al., 2004; Yakin et al., 2004; Ravhon et al., 2005; Walker et al., 2005; Valojerdi et al., 2006; Morbeck, 2007; Urman et al., 2008; Dittmann-Műller et al., 2009; Fancsovits et al., 2011, 2015; Yung et al., 2021), which was associated with a mild increase in clinical pregnancy (RR 1.097, 95% CI 1.028–1.169, I2 = 0.00%; Supplementary Fig. S7a; Schoolcraft et al., 2002; Balaban et al., 2004; Yakin et al., 2004; Ravhon et al., 2005; Walker et al., 2005; Valojerdi et al., 2006; Morbeck, 2007; Urman et al., 2008; Dittmann-Műller et al., 2009; Fancsovits et al., 2011, 2015; Yung et al., 2021), but had no significant effect on other reproductive outcomes (ongoing pregnancy rate (n = 2, RR 0.918, 95% CI 0.714–1.179, I2 = 3.63%; Morbeck, 2007; Yung et al., 2021) and live birth rate (n = 6, RR 1.134, 95% CI 1.000–1.285, I2 = 22.17%; Valojerdi et al., 2006; Morbeck, 2007; Urman et al., 2008; Fancsovits et al., 2011, 2015; Yung et al., 2021; Supplementary Fig. S7b, c)).
Granulocyte colony-stimulating factor
Our meta-analysis of four RCTs evaluating the effects of using granulocyte colony-stimulating factor (G-CSF) at the time of ET compared to placebo (Singh et al., 2015; Obidniak et al., 2016; Arefi et al., 2018; Singh and Singh, 2018) showed a significant increase in clinical pregnancy (RR 1.774, 95% CI 1.252–2.512, I2 = 0; Fig. 4a, Supplementary Fig. S8). Only one RCT reported on each of live birth (RR 1.518, 95% CI 0.769–2.997; Arefi et al., 2018), miscarriage (RR 1.272, 95% CI 0.123–13.177; Arefi et al., 2018) and ongoing pregnancy (RR 2.473, 95% CI 1.131–5.405; Singh and Singh, 2018), all showing mixed benefit of using G-CSF with low evidence quality (Supplementary Table SIV).
Seminal fluid
The use of seminal fluid was assessed in two RCTs (Aflatoonian et al., 2009; Karimian et al., 2010) of medium risk of bias (Supplementary Table SIII). There was no significant benefit to improve biochemical pregnancy (n = 2, RR 1.138, 95% CI 0.912, 1.420, I2 = 0%; Supplementary Fig. S9), clinical pregnancy (RR 1.205, 95% CI 0.717–2.025) or live birth (RR 1.281, 95% CI 0.908–1.808; Aflatoonian et al., n.d.; Karimian et al., 2010).
Culture medium
One RCT (Sigalos et al., 2018) evaluated the impact of ET low versus high volumes of culture medium, which showed no benefit on clinical pregnancy (RR 0.862, 95% CI 0.662–1.125) or ongoing pregnancy (RR 0.833, 95% CI 0.586–1.185).
Plasma infusion
The study by Obidniak et al. (2017) evaluated the effects of plasma infusion at the time of ET (n = 90 participants) reporting a 2-fold increase in clinical pregnancy compared to placebo (RR 2.182, 95% CI 1.219–3.904). Confidence in this evidence was judged to be low (Supplementary Table SIII).
17-Hydroxyprogesterone caproate
We identified one RCT (Abu-Musa et al., 2008) that evaluated the effectiveness of providing one injection of 17-hydroxyprogesterone caproate (17-HPC) compared to placebo at the time of ET (n = 125 participants). There was no significant effect on clinical pregnancy with 17-HPC injection versus placebo (RR 0.902, 95% CI 0.569, 1.429).
Powdered gloves
A single RCT evaluated the difference in using powdered versus unpowdered gloves at the time of ET (n = 712 participants; Hannoun et al., 2009). There was no difference in clinical pregnancy rate across both groups (RR 1.008, 95% CI 0.834–1.218).
ET techniques
Use of ultrasound
A large body of evidence was captured evaluating the different ultrasound modalities used at the time of ET. We pooled data from 24 RCTs that compared ET under ultrasound guidance to ET guided by clinical touch, which showed a significant increase in clinical pregnancy (n = 24, RR1.265, 95% CI 1.151–1.391, I2 = 8.53%; Fig. 4a;Wisanto et al., 1989; Prapas et al., 1995; Kan et al., 1999; Coroleu et al., 2000, 2002b; Abdelmassih et al., 2001; Garcı’a-Velasco et al., 2001, 2002; Tang et al., 2001; Matorras et al., 2002; Sallam et al., 2002; Bar-Hava et al., 2003; Marconi et al., 2003; Weissman et al., 2003; de Camargo Martins et al., 2004; Moraga-Sanchez et al., 2004; Li et al., 2005; Maldonado et al., 2005; Chen et al., 2007; Davar et al., 2007; Kosmas et al., 2007; Drakeley et al., 2008; Eskandar et al., 2008; Ammar et al., 2013), ongoing pregnancy (n = 8, RR 1.369, 95% CI 1.144–1.639, I2 = 51.34% (Supplementary Fig. S10c; Coroleu et al., 2000; Tang et al., 2001; Matorras et al., 2002; Marconi et al., 2003; Davar et al., 2007; Drakeley et al., 2008; Eskandar et al., 2008; Ammar et al., 2013), biochemical pregnancy (n = 2, RR 1.496, 95 CI: 1.174–1.906; Supplementary Fig. S10b; Coroleu et al., 2000; Kosmas et al., 2007), and live birth (n = 2, RR 1.744, 95% CI 1.163–2.706, I2 = 79.97%; Fig. 4b;Supplementary Fig. S10e; Eskandar et al., 2008; Azmy et al., 2009) with the use of ultrasound. There was no difference in miscarriage rates between both groups (n = 12, RR 1.145, 95% CI 0.883–1.484, I2 = 0%; Supplementary Fig. S10d; Garcı’a-Velasco et al., 2001, 2002; Tang et al., 2001; Coroleu et al., 2002b; Matorras et al., 2002; Weissman et al., 2003; de Camargo Martins et al., 2004; Davar et al., 2007; Kosmas et al., 2007; Eskandar et al., 2008; Azmy et al., 2009; Ammar et al., 2013).
We included seven RCTs that compared the use of transabdominal versus transvaginal ultrasound at the time of ET (Porat et al., 2010; Bodri et al., 2011; Deep et al., 2013; Hauzman et al., 2013; Dalal et al., 2014; Revelli et al., 2016; Karavani et al., 2017). There was no difference between both groups on clinical pregnancy (n = 7, RR 1.004, 95% CI 0.924–1.090, I2 = 0%; Supplementary Fig. S10f; Porat et al., 2010; Bodri et al., 2011; Deep et al., 2013; Hauzman et al., 2013; Dalal et al., 2014; Revelli et al., 2016; Karavani et al., 2017), ongoing pregnancy (n = 5, RR 1.029, 95% CI 0.922–1.148, I2 = 0.01%; Supplementary Fig. S10h; Porat et al., 2010; Bodri et al., 2011; Hauzman et al., 2013; Revelli et al., 2016; Karavani et al., 2017), biochemical pregnancy (n = 2, RR 0.977, 95% CI 0.712–1.341; Supplementary Fig. S10g; Bodri et al., 2011; Hauzman et al., 2013), miscarriage (n = 3, RR 0.835, 95% CI 0.575–1.211, I2 = 0%; Supplementary Fig. S10i; Bodri et al., 2011; Revelli et al., 2016; Karavani et al., 2017) and live birth (n = 1, RR 0.789, 95% CI 0.444–1.403; Karavani et al., 2017). One RCT by Saravelos et al. (2016) evaluated the use of 3-dimensional versus 2-dimensional ultrasound at the time of ET (n = 474 participants), which showed no difference for clinical pregnancy (RR 0.981, 95% CI 0.800–1.202) or any of the other secondary outcomes.
Bladder fullness
Three RCTs compared the difference in reproductive outcomes following ET on a full versus empty bladder (n = 1069 participants; Mitchell et al., 1989; Lewin et al., 1997; Lorusso et al., 2005). Overall, there was no difference across both groups for clinical pregnancy (n = 3, RR 1.266, 95% CI 0.884–1.813, I2 = 50.68%; Supplementary Fig. S11a; Mitchell et al., 1989; Lewin et al., 1997; Lorusso et al., 2005), ongoing pregnancy (n = 2, RR 1.276, 95% CI 0.874–1.863; Supplementary Fig. S11b; Lewin et al., 1997; Lorusso et al., 2005) or miscarriage (n = 1, RR 1.047, 95% CI 0.467–2.346; Lorusso et al., 2005).
Pressure on cervix
Two RCTs evaluated the effect of mechanical effect on the cervix by unscrewing the speculum to apply gentle pressure during ET (n = 716 participants), which showed no significant effect for clinical pregnancy (n = 2, RR 1.175, 95% CI 0.817–1.690; Supplementary Fig. S12; Mansour, 2005; Amui et al., 2011) or ongoing pregnancy (n = 1, RR 0.843, 95% CI 0.485–1.468; Amui et al., 2011).
Pump regulated transfer
One study (Caanen et al., 2016) compared the use of a pump regulated transfer to manual ET (n = 599 participants), which showed no difference between methods for clinical pregnancy (RR 1.201, 95% CI 0.904–1.596) or ongoing pregnancy (RR 1.234, 95% CI 0.884–1.722).
Cervical mucus removal
Removing the cervical mucus before ET was assessed in six studies (Ruhlman et al., 1999; Soroka et al., 1999; Glass et al., 2000; Berkkanoglu et al., 2006; Visschers et al., 2007; Moini et al., 2011) compared to standard practice (n = 1157 participants) using different tools including cotton swabs (Moini et al., 2011), cervical brush (Visschers et al., 2007), aspirators (Ruhlman et al., 1999; Soroka et al., 1999) or flushing with culture media solution (Berkkanoglu et al., 2006) or their combination (Glass et al., 2000). Our meta-analysis showed no significant effect of cervical mucus removal on clinical pregnancy (n = 5, RR 1.029, 95% CI 0.753–1.405, I2 = 5.89%; Supplementary Fig. S13a; Ruhlman et al., 1999; Soroka et al., 1999; Glass et al., 2000; Berkkanoglu et al., 2006; Moini et al., 2011), biochemical pregnancy (n = 2, RR 0.933, 95% CI 0.774–1.125; Supplementary Fig. S13b; Visschers et al., 2007; Moini et al., 2011), ongoing pregnancy (n = 2, RR 1.068, 95% CI 0.849–1.344; Supplementary Fig. S13c; Berkkanoglu et al., 2006; Visschers et al., 2007), miscarriage (n = 2, RR 0.790, 95% CI 0.487–1.282; Supplementary Fig. S13d; Visschers et al., 2007; Moini et al., 2011) or live birth (n = 2, RR 1.506, 95% CI 0.908–2.499; Supplementary Fig. S13e; Visschers et al., 2007; Moini et al., 2011).
ET catheters
A total of 27 RCTs compared ET outcomes using soft versus hard catheters (Gilberto Almodin et al., n.d.; Wisanto et al., 1989; Al-Shawaf et al., 1993; Perin et al., 1997; Grunert et al., 1998; Amorcho et al., 1999; Ghazzawi et al., 1999; Mayer et al., 1999; Boone et al., 2001; Curfs et al., 2001; Lavery et al., 2001; Karande et al., 2002; Levi-Setti et al., 2002; McDonald and Norman, 2002; Mortimer et al., 2002; van Weering et al., 2002; Foutouh et al., 2003; McIlveen et al., 2005; Baris et al., 2007; Rhodes et al., 2007; El-Shawarby et al., 2008; Saldeen et al., 2008; Yao et al., 2009b; Allahbadia et al., 2010; Talwar et al., 2011; Nihat Candan et al., 2014). Overall, there was a significant increase in clinical pregnancy with the use of a soft catheter (RR 1.122, 95% CI 1.028–1.224, I2 = 57.66%; Fig. 4a;Supplementary Fig. S14a) but no difference was found for ongoing pregnancy (n = 3, RR 1.138, 95% CI 0.904–1.432, I2 = 32.46%; Supplementary Fig. S14b; Karande et al., 2002; Levi-Setti et al., 2002; Baris et al., 2007) or live birth rates (n = 2, RR 2.222, 95% CI 0.457–10.806, I2 = 94.13%; Fig. 4b;Supplementary Fig. S14c; Perin et al., 1997; Saldeen et al., 2008).
Using a double compared to a single lumen ET catheter seemed to reduce clinical pregnancy rate in a small RCT of 66 participants (RR 0.314, 95% CI 0.129–0.764; Meriano et al., 2000). Similarly, using a straight versus a bent tip catheter seemed to also reduce clinical pregnancy in another small RCT (Ocal et al., 2003; RR 0.648, 95% CI 0.421–0.999). The use of an echogenic versus standard ET catheter did not affect the rate of clinical pregnancy in both groups (RR 1.302, 95% CI 0.966–1.756; Coroleu et al., 2006). Confidence in evidence sought on these interventions was low (Table I, Supplementary Table SIV). Yayla Abide et al. (2018) suggested that catheter rotation at the time of ET compared to standard practice yielded a higher clinical pregnancy rate (RR 1.560, 95% CI 1.026–2.371) with no difference reported for ongoing pregnancy (RR 1.435, 95% CI 0.911–2.260) or biochemical pregnancy (RR 1.577, 95% CI 1.051–2.366). This RCT showed a moderate risk of bias and its results showed be interpreted with caution (Supplementary Table SIII).
Table I.
GRADE assessment of evidence from randomised trials evaluating interventions at the time of embryo transfer in women undergoing assisted reproduction
| Certainty assessment |
Summary of findings |
|||||||
|---|---|---|---|---|---|---|---|---|
| Participants (studies) Follow up | Risk of bias | Inconsistency | Indirectness | Imprecision | Overall certainty of evidence | Study event rates (%) |
Relative effect (95% CI) | |
| With Comparison | With Interventions at the time of ET | |||||||
|
Higher confidence and significant effect size:
| ||||||||
| Hyaluronic acid versus no HA | ||||||||
| 2453 | not serious | not serious | not serious | not serious | ⊕⊕⊕⊕ | 286/1305 (21.9%) | 387/1148 (33.7%) | RR 1.457 |
| (9 RCTs) | HIGH | (1.197 to 1.773) | ||||||
| Ultrasound guided ET versus clinical touch | ||||||||
| 7256 | not serious | not serious | not serious | serious a | ⊕⊕⊕◯ | 986/3587 (27.5%) | 1245/3669 (33.9%) | RR 1.265 |
| (24 RCTs) | MODERATE | (1.151 to 1.391) | ||||||
| Softer versus harder catheters | ||||||||
| 10688 | not serious | not serious | serious b | not serious | ⊕⊕⊕◯ | 1704/5248 (32.5%) | 1969/5440 (36.2%) | RR 1.122 |
| (27 RCTs) | MODERATE | (1.028 to 1.224) | ||||||
|
Lower confidence and significant effect size:
| ||||||||
| G-CSF versus placebo/no G-CSF | ||||||||
| 292 | serious c | not serious | not serious | serious a | ⊕⊕◯◯ | 35/154 (22.7%) | 58/138 (42.0%) | RR 1.774 |
| (4 RCTs) | LOW | (1.252 to 2.512) | ||||||
| Atosiban versus placebo/no atosiban | ||||||||
| 1646 | not serious | serious d | not serious | serious a | ⊕⊕◯◯ | 325/823 (39.5%) | 426/823 (51.8%) | RR 1.493 |
| (7 RCTs) | LOW | (1.184 to 1.882) | ||||||
| hCG versus placebo/no hCG | ||||||||
| 4653 | serious e | serious f | not serious | not serious | ⊕⊕◯◯ | 883/2298 (38.4%) | 1052/2355 (44.7%) | RR 1.232 |
| (16 RCTs) | LOW | (1.099 to 1.382) | ||||||
|
High confidence and no significant effect:
| ||||||||
| Transvaginal ultrasound versus transabdominal ultrasound | ||||||||
| 2942 | not serious | not serious | not serious | not serious | ⊕⊕⊕⊕ | 620/1457 (42.6%) | 638/1485 (43.0%) | RR 1.004 |
| (7 RCTs) | HIGH | (0.924 to 1.090) | ||||||
|
Some positive associations with clinical pregnancy rate:
| ||||||||
| NSAID's versus placebo/no NSAID's | ||||||||
| 1207 | not serious | not serious | serious h | not serious | ⊕⊕⊕◯ | 166/599 (27.7%) | 222/608 (36.5%) | RR 1.294 |
| (7 RCTs) | MODERATE | (0.973 to 1.721) | ||||||
| Acupuncture versus placebo/no acupuncture | ||||||||
| 6496 | not serious | serious i | not serious | not serious | ⊕⊕⊕◯ | 1379/3409 (40.5%) | 1379/3087 (44.7%) | RR 1.121 |
| (18 RCTs) | MODERATE | (0.988 to 1.273) | ||||||
| Air versus fluid in catheter tip | ||||||||
| 408 | serious c | serious j | not serious | serious a | ⊕◯◯◯ | 58/203 (28.6%) | 76/205 (37.1%) | RR 1.361 |
| (3 RCTs) | VERY LOW | (0.844 to 2.195) | ||||||
| Full bladder versus empty bladder | ||||||||
| 1069 | serious c | serious k | not serious | very serious g | ⊕◯◯◯ | 102/525 (19.4%) | 148/544 (27.2%) | RR 1.266 |
| (3 RCTs) | VERY LOW | (0.884 to 1.813) | ||||||
|
Lower confidence and no real associations with clinical pregnancy rate:
| ||||||||
| Music versus no music | ||||||||
| 409 | not serious | not serious | not serious | very serious g | ⊕⊕◯◯ | 101/209 (48.3%) | 102/200 (51.0%) | RR 1.052 |
| (3 RCTs) | LOW | (0.866 to 1.279) | ||||||
| Nurse versus doctor | ||||||||
| 655 | not serious | not serious | not serious | very serious g | ⊕⊕◯◯ | 115/327 (35.2%) | 111/328 (33.8%) | RR 0.961 |
| (2 RCTs) | LOW | (0.778 to 1.187) | ||||||
| Pressure on cervix versus no pressure | ||||||||
| 716 | serious c | not serious | not serious | very serious g | ⊕◯◯◯ | 172/359 (47.9%) | 221/357 (61.9%) | RR 1.175 |
| (2 RCTs) | VERY LOW | (0.817 to 1.690) | ||||||
| Site of deposition: further from fundus (15-20mm) versus closer (<12mm) | ||||||||
| 2170 | serious c | serious l | very serious m | very serious g | ⊕◯◯◯ | 176/921 (19.1%) | 256/1249 (20.5%) | RR 1.089 |
| (3 RCTs) | VERY LOW | (0.828 to 1.431) | ||||||
| Delayed versus immediate catheter withdrawal | ||||||||
| 672 | serious c | not serious | not serious | very serious g | ⊕◯◯◯ | 129/339 (38.1%) | 128/333 (38.4%) | RR 1.039 |
| (3 RCTs) | VERY LOW | (0.868 to 1.243) | ||||||
| Cervical mucus removal versus no removal | ||||||||
| 1157 | serious c | serious o | not serious | very serious g | ⊕◯◯◯ | 225/597 (37.7%) | 229/560 (40.9%) | RR 1.029 |
| (5 RCTs) | VERY LOW | (0.753 to 1.405) | ||||||
| Antibiotics versus no antibiotics | ||||||||
| 625 | serious c | not serious | serious p | very serious g | ⊕◯◯◯ | 109/317 (34.4%) | 107/308 (34.7%) | RR 1.008 |
| (2 RCTs) | VERY LOW | (0.812 to 1.251) | ||||||
| Mindfulness versus no mindfulness | ||||||||
| 500 | serious c | not serious | not serious | very serious g | ⊕◯◯◯ | 121/247 (49.0%) | 113/253 (44.7%) | RR 0.911 |
| (2 RCTs) | VERY LOW | (0.755 to 1.098) | ||||||
|
Significant negative association with clinical pregnancy rates:
| ||||||||
| Bed rest versus shorter/no bed rest | ||||||||
| 1180 | serious c | not serious | not serious | serious a | ⊕⊕◯◯ | 217/591 (36.7%) | 185/589 (31.4%) | RR 0.857 |
| (6 RCTs) | LOW | (0.741 to 0.991) | ||||||
The table presents evidence summary for interventions evaluated in two or more randomised trials.
GRADE: Grading of Recommendations Assessment, Development and Evaluation, CI: Confidence interval; RR: Risk ratio, ET: embryo transfer, G-CSF: granulocyte colony-stimulating factor,HA: hyaluronic acid. NSAID: non-steroidal anti-inflammatory drug
Explanations
Wide confidence intervals
Significant heterogeneity in study design: lots of different catheter types compared which we believe may have impacted outcomes
Downgraded due to concerns about whole risk of bias
Downgraded due to high heterogeneity: I2 = 68.27%
Downgraded due to concerns about allocation concealment and lack of blinding
Downgraded due to high heterogeneity: I2 = 57.76%
Very wide confidence intervals
Significant heterogeneity in study design: lots of different NSAID's and length of treatment
Downgraded due to high heterogeneity: I2 = 75.14%
Downgraded due to high heterogeneity: I2 = 61.16%
Downgraded due to high heterogeneity: I2 = 50.68%
Downgraded due to high heterogeneity: I2 = 60.99%
Significant heterogeneity in study design, not consistent site of deposition in any of them
Downgraded due to high heterogeneity: I2 = 75.89%
Three RCTs compared the use of air or fluid in the transfer catheter (Krampl et al., 1995; Moreno et al., 2004; Madani et al., 2010). Both interventions had a similar effect on clinical pregnancy rate (RR 1.361, 95% CI 0.844–2.195) with moderate inconsistency (I2 = 61.16%; Supplementary Fig. S15). We included three RCTs that compared early versus delayed catheter withdrawal after ET (Martínez et al., 2001; Arvas et al., 2014; Devranoğlu et al., 2018). Both techniques yielded a similar clinical pregnancy rate (n = 3, RR 1.039, 95% CI 0.868–1.243, I2 = 0%; Supplementary Fig. S16; Martínez et al., 2001; Arvas et al., 2014; Devranoğlu et al., 2018), ongoing pregnancy (n = 1, RR 0.889, 95% CI 0.594–1.329; Devranoğlu et al., 2018) and biochemical pregnancy (n = 1, RR 1.014, 95% CI 0.728–1.413; Devranoğlu et al., 2018).
The site of embryo deposition (>15 mm versus <15 mm from the fundus) was assessed in three RCTs (Nazari et al., 1993; Coroleu et al., 2002a; Franco et al., 2004). Our pooled effect estimate showed no difference between both groups for clinical pregnancy (n = 3, RR 1.089, 95% CI 0.828–1.431, I2 = 60.99%; Supplementary Fig. S17a; Nazari et al., 1993; Coroleu et al., 2002a; Franco et al., 2004), ongoing pregnancy (n = 3, RR 1.191, 95% CI 0.858–1.653, I2 = 65.08%; Supplementary Fig. S17b; Nazari et al., 1993; Coroleu et al., 2002a; Franco et al., 2004), miscarriage (n = 2, RR 0.916, 95% CI 0.446–1.881; Supplementary Fig. S17c; Coroleu et al., 2002a; Franco et al., 2004) or live birth (n = 3, RR 1.201, 95% CI 0.855–1.687, I2 = 66.36%; Supplementary Fig. S17d; Nazari et al., 1993; Coroleu et al., 2002a; Franco et al., 2004). One small RCT (Groutz et al., 1997; n = 40 participants) compared the outcome of transmyometrial to transcervical ultrasound-guided ET showing no difference in the rate of clinical pregnancy (RR 0.333, 95% CI 0.038–2.939) or ongoing pregnancy (RR 0.143, 95% CI 0.008–2.599).
Bed rest
We performed a meta-analysis of six RCTs that evaluated the effect of bed rest following ET compared to immediate ambulation or no rest (Botta and Grudzinskas, 1997; Rezábek et al., 2001; Amarin and Obeidat, 2004; Purcell et al., 2007; Gaikwad et al., 2013; Malhotra and Sarkar, 2019). Overall, there was a reduction in clinical pregnancy rates in the bed rest group (RR 0.857, 95% CI 0.741–0.991, I2 = 0.01%; Fig. 4a, Supplementary Fig. S18a) while there was no significant difference for biochemical pregnancy (n = 2, RR 0.823, 95% CI 0.538–1.259; Supplementary Fig. S18b; Amarin and Obeidat, 2004; Gaikwad et al., 2013), ongoing pregnancy (n = 4, RR 0.870, 95% CI 0.656–1.153, I2 = 50.53%; Supplementary Fig. S18c; Botta and Grudzinskas, 1997; Amarin and Obeidat, 2004; Purcell et al., 2007; Gaikwad et al., 2013), miscarriage (n = 3, RR 1.076, 95% CI 0.466–2.483, I2 = 61.84%; Supplementary Fig. S18d; Botta and Grudzinskas, 1997; Amarin and Obeidat, 2004; Gaikwad et al., 2013) or live birth (n = 3, RR 0.800, 95% CI 0.626–1.022, I2 = 21.93%; Fig. 4b;Supplementary Fig. S18e; Rezábek et al., 2001; Gaikwad et al., 2013; Malhotra and Sarkar, 2019).
Nurse versus doctor
Two RCTs compared ET outcomes when performed by a nurse or a doctor (n = 655 participants) showing no significant difference between both groups for clinical pregnancy (n = 2, RR of 0.961, 95% CI 0.778–1.187; Supplementary Fig. S19; Bjuresten et al., 2003; Rinaldi et al., 2014) or ongoing pregnancy (n = 1, RR 0.981, 95% CI 0.728–1.324; Rinaldi et al., 2014).
Relaxation interventions
Acupuncture
Eighteen RCTs evaluated the effect of acupuncture interventions on clinical pregnancy (n = 6437 participants) including 16 studies on needle acupuncture (Paulus et al., 2002, 2003; Benson et al., 2006; Westergaard et al., 2006; Craig et al., 2007, 2014; Fratterelli et al., 2008; Domar et al., 2009; So et al., 2009, 2010; Andersen et al., 2010; Madaschi et al., 2010; Omodei et al., 2010; Moy et al., 2011; Qu et al., 2014; Dehghani et al., 2020), two on laser acupuncture (Benson et al., 2006; Fratterelli et al., 2008) and two on transcutaneous electrical acupoint stimulation (TEAS; Zhang et al., 2011; Zhong and Zhang, 2017). Eight studies compared acupuncture to sham acupuncture therapy (Paulus et al., 2003; Benson et al., 2006; Fratterelli et al., 2008; So et al., 2009, 2010; Andersen et al., 2010; Moy et al., 2011; Zhang et al., 2011), whilst 12 of the studies compared acupuncture to no treatment (Paulus et al., 2002; Benson et al., 2006; Westergaard et al., 2006; Craig et al., 2007, 2014; Fratterelli et al., 2008; Domar et al., 2009; Madaschi et al., 2010; Omodei et al., 2010; Qu et al., 2014; Zhong and Zhang, 2017; Dehghani et al., 2020). Overall, acupuncture interventions did not increase the rate of clinical pregnancy (RR 1.121, 95% CI 0.988–1.273, I2 = 75.14%; Supplementary Fig. S20a). Subgroup analysis showed a similar effect for needle (n = 16, RR 1.076, 95% CI 0.919–1.260, I2 = 73.44%) and laser acupuncture (n = 2, RR 1.193, 95% CI 0.996–1.430, I2 = 0%) whilst TEAS showed some improvement in clinical pregnancy rate (n = 2, RR 1.345, 95% CI 1.039–1.741, I2 = 62.66%) but confidence in this evidence was low (Supplementary Fig. S20f).
Compared to standard care or sham intervention, acupuncture showed some benefit in increasing the rate of biochemical pregnancy (n = 8, RR 1.150, 95% CI 1.002–1.321, I2 = 70.45%; Benson et al., 2006; Westergaard et al., 2006; Craig et al., 2007; Fratterelli et al., 2008; Domar et al., 2009; Zhang et al., 2011; Zhong and Zhang, 2017; Dehghani et al., 2020) though evidence was of poor quality with high heterogeneity. There was no difference for ongoing pregnancy (n = 11, RR 1.130, 95% CI 0.931–1.371, I2 = 75.16%; Paulus et al., 2002, 2003; Westergaard et al., 2006; Fratterelli et al., 2008; So et al., 2009, 2010; Andersen et al., 2010; Madaschi et al., 2010; Omodei et al., 2010; Seto et al., 2017; Dehghani et al., 2020), miscarriage (n = 10, RR 1.073, 95% CI 0.828–1.391, I2 = 0.0%; Paulus et al., 2002, 2003; Westergaard et al., 2006; So et al., 2009, 2010; Andersen et al., 2010; Madaschi et al., 2010; Omodei et al., 2010; Zhang et al., 2011; Craig et al., 2014) or live birth (n = 11, RR 1.176, 95% CI 0.929–1.488, I2 = 80.92%; Paulus et al., 2002, 2003; So et al., 2009, 2010; Andersen et al., 2010; Madaschi et al., 2010; Omodei et al., 2010; Zhang et al., 2011; Craig et al., 2014; Qu et al., 2014; Seto et al., 2017; Fig. 4b, Supplementary Fig. S20b–e). There were no significant differences in clinical pregnancy rates observed between studies using a sham acupuncture control (n = 8, RR 1.056, 95% CI 0.890–1.252); or those with no placebo comparison (n = 12, RR 1.177, 95% CI 0.988–1.273; Supplementary Fig. S20g).
Listening to music during ET was assessed in three RCTs compared to standard care (Murphy et al., 2014; Stocker et al., 2016; Aba et al., 2017). Overall, this did not increase the rate of clinical pregnancy (RR 1.052, 95% CI 0.866–1.279, I2 = 0.00%; Supplementary Fig. S21). Similarly, the use of mindfulness was assessed in two RCTs (Benson et al., 2006; Fratterelli et al., 2008) also showing no difference in clinical pregnancy (RR 0.911, 95% CI 0.755–1.098, I2 = 0.00%) or biochemical pregnancy rate (RR 0.912, 95% CI 0.780–1.066, I2 = 0%; Supplementary Fig. S22a and b, respectively). The effect of mindfulness on ongoing pregnancy rate was reported in one study (Fratterelli et al., 2008) showing no significant increase was seen (RR 0.946, 95% CI 0.738–1.211).
One study measured the effect of porcine relaxin compared to a placebo (MacLennan et al., 1985). There was no increase in clinical pregnancy (RR 0.882, 95% CI 0.405–1.924) or ongoing pregnancy rate (RR 1.177, 95% CI 0.442–3.134) or miscarriage rate (RR 0.441, 95% CI 0.085–2.296). Similarly, one study measured the effect of glyceryl trinitrate compared to a placebo (Shaker et al., 1993) also showing no increase in clinical pregnancy rate (RR 0.947, 95% CI 0.554–1.620).
There was one study that investigated massage therapy as an intervention compared to standard care (Gavrizi and Skillern, 2019). The results from this study showed no significant increase in live birth with massage (RR 1.371, 95% CI 0.881–2.133). Catoire et al. (2013) compared the effect of hypnosis on the day of ET to the use of benzodiazepine in 93 women, which did not report a significant difference for clinical pregnancy (RR 1.032, 95% CI 0.595–1.790) or live birth (RR 1.015, 95% CI 0.509–2.03).
Discussion
Summary of main findings
In this comprehensive systematic review, we identified a large number of competing interventions proposed to increase the chances of conception following ET. Overall, the quality of evidence was low with significant concerns regarding trial methodology and risk of publication bias. Several interventions do seem, however, to significantly improve the chances of conception (Table I).
The use of ultrasound guidance and soft ET catheters are commonly used in clinical practice with good quality evidence to support their effectiveness. We identified several promising pharmacological agents that also seem to aid embryo implantation and increase clinical pregnancy including HA, G-CSF, atosiban and hCG. A common mechanistic effect across these interventions could be through maximizing uterine relaxation at the time of ET and optimizing endometrial receptivity (Mains and van Voorhis, 2010). Evidence for these interventions largely stems from small trials and further evaluation in larger trials is warranted before adopting them into routine clinical practice.
Recommending bed rest post-ET was the only intervention in this review that significantly reduced clinical pregnancy rates. This is consistent with ASRM Guidance, which recommends against this intervention (Penzias et al., 2017a). We identified a substantial number of unnecessary interventions that lack sufficient evidence in support of their effectiveness and safety. Such interventions should not be routinely recommended in clinical practice pending assessment in future randomized trials.
Strengths and limitations
The strengths of our review stem from its pragmatic design and comprehensive search strategy, therefore, offering the most up to date evidence on ET techniques and interventions. We employed a standard methodology and assessed the risk of bias in included trials following a prospectively registered protocol. We conducted subgroup analyses to explore potential effect modifiers, assessed publication bias and employed the GRADE approach to aid evidence translation into clinical practice.
Our findings have several methodological limitations. The quality of included trials was often suboptimal with almost half showing a high risk of bias for outcome reporting (44.9%). This limited our ability to synthesize evidence on all outcomes of interest, particularly live birth. We addressed this perceived bias by downgrading confidence in available evidence in our GRADE assessment of the evaluated interventions; however, this remains a subjective judgement of evidence quality and certainty.
Several effect modifiers could impact the outcome of ET including the operator’s experience, patient characteristics (age, BMI, uterine anomalies, etc.), number of embryos transferred and the transfer of fresh versus frozen embryos. Clearly, the technology and practice of assisted conception have also progressed significantly over the time span of included trials (1989–2021) leading to inherent variations in evaluated ART protocols (Supplementary Table SI). We were unable to explore certain effect modifiers due to reporting limitations, however, we attempted to address this by implementing a random-effect model to adjust our pooled effect estimate (Cornell et al., 2014). Further evaluation using individual patient data (IPD) is, therefore, warranted to synthesize higher-quality evidence.
Implications for clinical practice
Currently, a large number of add-on treatments are proposed to couples undergoing ART, yet the debate on their effectiveness and safety prevail (Zemyarska, 2019; Lensen et al., 2021). We detected many RCTs conducted within the last 20 years evaluating many different interventions focused on optimizing ET success. This highlights the important role of robust evidence synthesis to inform clinical practice and minimize the risk of exposing patients to potentially harmful or unnecessary interventions.
Most of the published systematic reviews on ET techniques are clustered around interventions commonly used in current practice such as ultrasound guidance (Teixeira et al., 2015; Cozzolino et al., 2018) and acupuncture (El-Toukhy et al., 2008; Gu et al., 2019; Smith et al., 2019). While helpful, systematic reviews focused on evaluating singular interventions can lead to fragmented evidence synthesis and an underappreciation of the body of evidence relevant to a particular health condition. To that end, we implemented a comprehensive search strategy, which helped us to detect several interventions of uncertain benefit that were evaluated in one or two RCTs only. We, therefore, caution against the routine uptake of such ‘experimental’ interventions into clinical practice pending further evaluation in larger, well-conducted RCTs. Although we detected several ET interventions that appear to improve chances of conception, the current body of evidence remains imprecise, and these interventions should be offered in research settings only.
Publication bias and selective outcomes reporting are major barriers to robust evidence synthesis (Sutton et al., 2000) specifically in the context of high stakes interventions such as ET. We chose to report primarily on clinical pregnancy rate to offer the most comprehensive evidence synthesis as most of the included trials did not report on key additional outcomes such as live birth. Bed rest is an important example where varied outcomes reported in primary RCTs (Botta and Grudzinskas, 1997; Rezábek et al., 2001; Amarin and Obeidat, 2004; Purcell et al., 2007; Gaikwad et al., 2013; Malhotra and Sarkar, 2019) could have contributed to the delay in identifying its adverse impact on clinical pregnancy rate following ET. As such, robust evaluation of the confidence in available evidence is crucial before introducing changes to clinical practice (Pottie et al., 2012).
Professional societies should champion the concurrent evaluation of available evidence to regularly update clinical practice guidelines. For example, the most up to date ASRM guidelines on ET recommend cervical mucus removal based on ‘fair’ evidence at the time (one RCT and one cohort study; Penzias et al., 2017a). Still, our findings summarizing evidence from five RCTs showed no benefit of this intervention.
Finally, the process of ET involves several steps immediately before, during and after where the operator technique seems to significantly impact the final outcome (Cirillo et al., 2020). Establishing a standardized protocol of best practice may facilitate training and reduce variation in practice across fertility clinics (Penzias et al., 2017b).
Future research need
The majority of the included RCTs in our review had a relatively small sample size with a moderate risk of bias specifically for outcome reporting. This significantly hinders efficient evidence synthesis and increases the risk of small study effect (Harbord et al., 2009). While several of the evaluated interventions seem to have a promising effect in improving clinical pregnancy rate (e.g. Atosiban and hCG), there is a need to evaluate their effectiveness and safety in well-powered RCTs and prospective IPD meta-analyses to inform clinical practice at scale (Tierney et al., 2015).
In this review, we focused on interventions within 24 h of the ET to increase homogeneity across pooled RCTs. However, several interventions aimed to improve endometrial receptivity and the implantation window could improve the outcome ET outcome such as endometrial scratching and different methods of luteal support (Mains and van Voorhis, 2010). Further evidence synthesis is, therefore, required to advise on the best practice in preparation for ET.
Finally, the majority of the included RCTs did not engage lay consumers in their design, conduct or reporting. Patient engagement is particularly relevant when evaluating anti-anxiety and relaxation interventions during ART treatments, which to date seem to have been based on anecdotal practice (Mahlstedt et al., 1987). Future trials should aim to engage all relevant stakeholders in the ART process to improve the permeation of research into clinical practice.
Conclusion
Using ultrasound guidance, soft catheters and HA at the time of ET appears to increase pregnancy rates. The use of atosiban, G-CSF and hCG showed a trend towards increased clinical pregnancy rate, but larger trials are required before adopting these interventions in clinical practice. Bed rest post-ET was associated with a reduction in clinical pregnancy and should not be recommended.
Supplementary data
Supplementary data are available at Human Reproduction Update online.
Data availability
Some or all datasets generated during and/or analysed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Authors’ roles
B.T., H.W. and J.T. conducted the data extraction, primary analysis, data illustration and drafted the first manuscript. S.D.K., D.M. and E.Y. supervised the project conduct and provided critical input to the final manuscript. B.H.A. conceived the idea, wrote the protocol, supervised the analysis and edited the final manuscript.
Funding
No funding was received towards this work directly. B.H.A. holds a personal development award from the National Institute of Health Research.
Conflict of interest
Nothing to disclose.
Supplementary Material
Contributor Information
Bede Tyler, UCL Institute for Women's Health, University College London, London, UK.
Hugo Walford, UCL Institute for Women's Health, University College London, London, UK.
Jennifer Tamblyn, Institute of Metabolism and Systems Research (IMSR), University of Birmingham, Birmingham, UK.
Stephen D Keay, Centre for Reproductive Medicine, University Hospital of Coventry & Warwickshire, Coventry, UK.
Dimitrios Mavrelos, UCL Institute for Women's Health, University College London, London, UK; Reproductive Medicine Unit, Elizabeth Garrett Anderson Wing, University College London Hospitals, London, UK.
Ephia Yasmin, UCL Institute for Women's Health, University College London, London, UK; Reproductive Medicine Unit, Elizabeth Garrett Anderson Wing, University College London Hospitals, London, UK.
Bassel H Al Wattar, UCL Institute for Women's Health, University College London, London, UK; Reproductive Medicine Unit, Elizabeth Garrett Anderson Wing, University College London Hospitals, London, UK.
References
- Aaleyasin A, Aghahosseini M, Rashidi M, Safdarian L, Sarvi F, Najmi Z, Mobasseri A, Amoozgar B.. In vitro fertilization outcome following embryo transfer with or without preinstillation of human chorionic gonadotropin into the uterine cavity: a randomized controlled trial. Gynecol Obstet Invest 2015;79:201–205. [DOI] [PubMed] [Google Scholar]
- Aba YA, Avci D, Guzel Y, Ozcelik SK, Gurtekin B.. Effect of music therapy on the anxiety levels and pregnancy rate of women undergoing in vitro fertilization-embryo transfer: a randomized controlled trial. Appl Nurs Res 2017;36:19–24. [DOI] [PubMed] [Google Scholar]
- Abdelmassih VG, Abdelmassih ST, Nagy ZP, Abdelmassih R, Balmaceda J.. The effect of ultrasound (US) guided embryo transfer (ET) and the choice of catheter on the outcome of IVF. Fertil Steril 2001;76:S88–S89. [Google Scholar]
- Abu-Musa A, Usta I, Nassar A, Hajami F, Hannoun A.. Effect of 17α-hydroxyprogesterone caproate before embryo transfer on the outcome of in vitro fertilization and embryo transfer: a randomized trial. Fertil Steril 2008;89:1098–1102. [DOI] [PubMed] [Google Scholar]
- Aflatoonian A, Ghandi S, Tabibnejad N.. The effect of intercourse around embryo transfer on pregnancy rate in assisted reproductive technology cycles. Int J Fertil Steril 2009;2:169–72. [Google Scholar]
- Ahn J, Kim C, Kim S, Jeon G, Kim S, Chae H.. Effects of administration of oxytocin antagonist on implantation and pregnancy rates in patients with repeated failure of IVF/ICSI treatment—clinical and experimental reproductive medicine. Korean J Reprod Med 2009;36:275–281. [Google Scholar]
- Allahbadia GN, Kadam K, Gandhi G, Arora S, Valliappan JB, Joshi A, Allahbadia S, Wolman I.. Embryo transfer using the SureView catheter-beacon in the womb. Fertil Steril 2010;93:344–350. [DOI] [PubMed] [Google Scholar]
- Al-Shawaf T, Dave R, Harper J, Linehan D, Riley P, Craft I.. Transfer of embryos into the uterus: how much do technical factors affect pregnancy rates? J Assist Reprod Genet 1993;10:31–36. [DOI] [PubMed] [Google Scholar]
- Amarin ZO, Obeidat BR.. Bed rest versus free mobilisation following embryo transfer: a prospective randomised study. BJOG 2004;111:1273–1276. [DOI] [PubMed] [Google Scholar]
- Ammar A, Mousa K, Hamed Rabei Galal NN.. A. Effect of ultrasound guided embryo transfer on pregnancy rates. New York Sci J 2013;6:79–83. [Google Scholar]
- Amorcho B, Gomez E, Pontes L, Campos I, Landeras J, Munoz M, Ballesteros A, Remohí J, Pellicer A.. Does the selection of catheter for embryo transfer affect the success rate of an ART unit? Hum Reprod 1999;14:205. [Google Scholar]
- Amui J, Check JH, Brasile D.. Speculum retention during embryo transfer does not improve pregnancy rates following embryo transfer—a randomized study. Clin Exp Obstet Gynecol 2011;38:333–334. [PubMed] [Google Scholar]
- Andersen D, Løssl K, Andersen AN, Fürbringer J, Bach H, Simonsen J, Larsen EC.. Acupuncture on the day of embryo transfer: a randomized controlled trial of 635 patients. Reprod Biomed Online 2010;21:366–372. [DOI] [PubMed] [Google Scholar]
- Arefi S, Fazeli E, Esfahani M, Borhani N, Yamini N, Hosseini A, Farifteh F.. Granulocyte-colony stimulating factor may improve pregnancy outcome in patients with history of unexplained recurrent implantation failure: an RCT. Int J Reprod BioMed 2018;16:299–304. [PMC free article] [PubMed] [Google Scholar]
- Arvas A, Karacan M, Ulug M, Cebi Z, Berberoglugil M, Batukan M, Çamlibel T.. A 20-second wait or immediate withdrawal of the catheter following ultrasound-guided blastocyst transfer. Fertil Steril 2014;102:e30. [Google Scholar]
- Azmy O, Taha T, Bibars M, Refaat M. Ultrasound guided versus blind touch embryo transfer: the Egyptian experience. In: Proceedings of the 15th World Conference of IVF and 4th Congress of IVM2009, p.9–12. http://www.edlearning.it/proceedings/moreinfo/20090419.htm (October 2021, date last accessed).
- Balaban B, Urman B, Yakin K, Isiklar A, Kilic Y, Aksoy S.. High pregnancy and implantation rates can be achieved in blastocyst transfers using hyaluronan enriched culture and transfer medium. Fertil Steril 2004;82:S221. [Google Scholar]
- Bar-Hava I, Meltzer S, Rabinson J, Ayash I, Sega S, Tur-Kaspa I.. Ultrasound guided versus blind tactile embryo transfer: a prospective randomised study. Hum Reprod 2003;18:xviii7. [Google Scholar]
- Baris D, Ata AB, Isiklar A, Balaban B, Urman B.. Prospective randomized comparison of Wallace and Labotect embryo transfer catheters. Reprod Biomed Online 2007;14:471–476. [DOI] [PubMed] [Google Scholar]
- Benson MR, Elkind-Hirsch KE, Theall A, Fong K, Hogan RB, Scott RT.. P-18: impact of acupuncture before and after embryo transfer on the outcome of in vitro fertilization cycles: a prospective single blind randomized study. Fertil Steril 2006;86:S135. [Google Scholar]
- Berkkanoglu M, Isikoglu M, Seleker M, Ozgur K.. Flushing the endometrium prior to the embryo transfer does not affect the pregnancy rate. Reprod Biomed Online 2006;13:268–271. [DOI] [PubMed] [Google Scholar]
- Bernabeu R, Roca M, Torres A, Ten J.. Indomethacin effect on implantation rates in oocyte recipients. Hum Reprod 2006;21:364–369. [DOI] [PubMed] [Google Scholar]
- Bjuresten K, Hreinsson JG, Fridström M, Rosenlund B, Ek I, Hovatta O.. Embryo transfer by midwife or gynecologist: a prospective randomized study. Acta Obstet Gynecol Scand 2003;82:462–466. [DOI] [PubMed] [Google Scholar]
- Bodri D, Colodrón M, García D, Obradors A, Vernaeve V, Coll O.. Transvaginal versus transabdominal ultrasound guidance for embryo transfer in donor oocyte recipients: a randomized clinical trial. Fertil Steril 2011;95:2263–2268.e1. [DOI] [PubMed] [Google Scholar]
- Boone WR, Johnson JE, Blackhurst DM, Crane MM.. Short communication: Cook versus EdwardsWallace: are there differences in flexible catheters? J Assist Reprod Genet 2001;18:15–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bosch E, Aasted H, Klein BM, Arce J-C.. A randomized, double-blind, placebo-controlled, multi-center, phase 2 trial to investigate the effect of barusiban on implantation in IVF/ICSI patients. Fertil Steril 2019;112:e179. [Google Scholar]
- Botta G, Grudzinskas G.. Is a prolonged bed rest following embryo transfer useful? Hum Reprod 1997;12:2489–2492. [DOI] [PubMed] [Google Scholar]
- Brook N, Khalaf Y, Coomarasamy A, Edgeworth J, Braude P.. A randomized controlled trial of prophylactic antibiotics (co-amoxiclav) prior to embryo transfer. Hum Reprod 2006;21:2911–2915. [DOI] [PubMed] [Google Scholar]
- Caanen MR, van der Houwen LE, Schats R, Vergouw CG, de Leeuw B, Lambers MJ, Groeneveld E, Lambalk CB, Hompes PG.. Embryo transfer with controlled injection speed to increase pregnancy rates: a randomized controlled trial. Gynecol Obstet Invest 2016;81:394–404. [DOI] [PubMed] [Google Scholar]
- Cambiaghi AS, Leao RBF, Alvarez AV, Nascimento PF.. Intrauterine injection of human chorionic gonadotropin before embryo transfer may improve clinical pregnancy and implantation rates in blastocysts transfers. Fertil Steril 2013;100:S121. [Google Scholar]
- Cardona Barberán A, Boel A, Vanden MF, Stoop D, Heindryckx B.. Diagnosis and treatment of male infertility-related fertilization failure. J Clin Med 2020;9:3899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Catoire P, Delaunay L, Dannappel T, Baracchini D, Marcadet-Fredet S, Moreau O, Pacaud L, Przyrowski D, Marret E.. Hypnosis versus diazepam for embryo transfer: a randomized controlled study. Am J Clin Hypn 2013;55:378–386. [DOI] [PubMed] [Google Scholar]
- Chen S-C, Lai T-H, Lee F-K.. The influence of abdominal ultrasound-guided embryo transfer on pregnancy rate: a preliminary report. Fertil Steril 2007;87:1235–1237. [DOI] [PubMed] [Google Scholar]
- Cirillo F, Patrizio P, Baccini M, Morenghi E, Ronchetti C, Cafaro L, Zannoni E, Baggiani A, Levi-Setti PE.. The human factor: does the operator performing the embryo transfer significantly impact the cycle outcome? Hum Reprod 2020;35:275–282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cornell J, Mulrow C, Localio R, Stack C, Meibohm A, Guallar E, Goodman S.. Random-effects meta-analysis of inconsistent effects: a time for change. Ann Intern Med 2014;160:267–270. [DOI] [PubMed] [Google Scholar]
- Coroleu B, Barri PN, Carreras O, Belil I, Buxaderas R, Veiga A, Balasch J.. Effect of using an echogenic catheter for ultrasound-guided embryo transfer in an IVF programme: a prospective, randomized, controlled study. Hum Reprod 2006;21:1809–1815. [DOI] [PubMed] [Google Scholar]
- Coroleu B, Barri PN, Carreras O, Martínez F, Parriego M, Hereter L, Parera N, Veiga A, Balasch J.. The influence of the depth of embryo replacement into the uterine cavity on implantation rates after IVF: a controlled, ultrasound-guided study. Hum Reprod 2002a;17:341–346. [DOI] [PubMed] [Google Scholar]
- Coroleu B, Barri PN, Carreras O, Martínez F, Veiga A, Balasch J.. The usefulness of ultrasound guidance in frozen–thawed embryo transfer: a prospective randomized clinical trial. Hum Reprod 2002b;17:2885–2890. [DOI] [PubMed] [Google Scholar]
- Coroleu B, Carreras O, Veiga A, Martell A, Martinez F, Belil I, Hereter L, Barri PN.. Embryo transfer under ultrasound guidance improves pregnancy rates after in-vitro fertilization. Hum Reprod 2000;15:616–620. [DOI] [PubMed] [Google Scholar]
- Cozzolino M, Vitagliano A, di Giovanni MV, Laganà AS, Vitale SG, Blaganje M, Drusany Starič K, Borut K, Patrelli TS, Noventa M.. Ultrasound-guided embryo transfer: summary of the evidence and new perspectives. A systematic review and meta-analysis. Reprod Biomed Online 2018;36:524–542. [DOI] [PubMed] [Google Scholar]
- Craig L, Rubin L, Peck J, Anderson M, Marshall L, Soules M.. Acupuncture performed before and after embryo transfer: a randomized controlled trial. J Reprod Med 2014;59:313–320. [PubMed] [Google Scholar]
- Craig LB, Criniti AR, Hansen KR, Marshall LA, Soules MR.. Acupuncture lowers pregnancy rates when performed before and after embryo transfer. Fertil Steril 2007;88:S40. [Google Scholar]
- Curfs MH, Cleine JH, van Kamp AA, Kruse-Blankestijn ME, Hondelink MN, Leerentveld RA.. Comparison of the Wallace versus TDT embryo-transfer catheter: a prospective, randomized study. InThird Biennial Alpha Conference 2001. pp. 8–11. [Google Scholar]
- Dalal R, Pai H, Palshetkar N.. Comparison of transabdominal (TA) versus transvaginally (TV) guided embryo transfer in oocyte recipient cycles: a prospective randomised trial. BJOG 2014;121:82.24102880 [Google Scholar]
- Davar R, Ghandi S, Tayebi N.. Does transabdominal ultrasound-guided embryo transfer improve pregnancy rates in ART cycles? Iran J Reprod Med 2007;5:95–98. [Google Scholar]
- de Camargo Martins AMV, Baruffi RLR, Mauri AL, Petersen C, Oliveira JBA, Contart P, Pontes A, Franco JG.. Ultrasound guidance is not necessary during easy embryo transfers. J Assist Reprod Genet 2004;21:421–425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deep JP, Li Y, Liu H.. The effect of embryo transfer on IVF treatment: comparing the trans-vaginal versus transabdominal ultrasound approach. J Minimally Invasive Gynecol 2013;20:S42–S43. [Google Scholar]
- Dehghani AS, Homayouni K, Kanannejad Z, Kanannejad Z.. The effect of acupuncture on the day of embryo transfer on the in vitro fertilization outcomes: an RCT. Int J Reprod Biomed 2020;18:209–214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dehghani Firouzabadi R, Ghandi S, Tayebi N.. Effect of administration of single dose piroxicam before embryo transfer on implantation and pregnancy rates in IVF cycles. J Biol Sci 2006;7:123–126. [Google Scholar]
- Dehghani Firouzabadi R, Janati S, Razi MH.. The effect of intrauterine human chorionic gonadotropin injection before embryo transfer on the implantation and pregnancy rate in infertile patients: a randomized clinical trial. Int J Reprod Biomed 2016;14:657–664. [PMC free article] [PubMed] [Google Scholar]
- Devranoğlu B, Özdamar Ö, Çakıroğlu Y, Küçükbaş M, Eken MK, Doğer E.. The timing of embryo transfer catheter removal: should it be delayed or done immediately? A prospective randomized trial. Gynecol Obstet Invest 2018;83:29–34. [DOI] [PubMed] [Google Scholar]
- Dittmann-Műller X, Zollner K, Zollner U.. Prospective randomised clinical trial about the efficacy of a human embryo transfer medium (EmbryoGlue(R)). Hum Reprod 2009;24:167. [Google Scholar]
- Domar AD, Meshay I, Kelliher J, Alper M, Powers RD.. The impact of acupuncture on in vitro fertilization outcome. Fertil Steril 2009;91:723–726. [DOI] [PubMed] [Google Scholar]
- Drakeley AJ, Jorgensen A, Sklavounos J, Aust T, Gazvani R, Williamson P, Kingsland CR.. A randomized controlled clinical trial of 2295 ultrasound-guided embryo transfers. Hum Reprod 2008;23:1101–1106. [DOI] [PubMed] [Google Scholar]
- Duvan CI, Ozmen B, Satıroglu H, Atabekoglu CS, Berker B.. Does addition of low-dose aspirin and/or steroid as a standard treatment in nonselected intracytoplasmic sperm injection cycles improve in vitro fertilization success? A randomized, prospective, placebo-controlled study. J Assist Reprod Genet 2006;23:15–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- El-Shawarby SA, Ravhon A, Skull J, Ellenbogen A, Trew G, Lavery SA.. Prospective randomized controlled trial of Wallace and Rocket embryo transfer catheters. Reprod Biomed Online 2008;17:549–552. [DOI] [PubMed] [Google Scholar]
- El-Toukhy T, Sunkara SK, Khairy M, Dyer R, Khalaf Y, Coomarasamy A.. A systematic review and meta-analysis of acupuncture in in vitro fertilisation. BJOG 2008;115:1203–1213. [DOI] [PubMed] [Google Scholar]
- Eskandar M, Abou-Setta AM, Almushait MA, El-Amin M, Mohmad SEY.. Ultrasound guidance during embryo transfer: a prospective, single-operator, randomized, controlled trial. Fertil Steril 2008;90:1187–1190. [DOI] [PubMed] [Google Scholar]
- Eskandar M, Al-Emain M, Atwan Y, Bakar S.. Does intrauterine injection of human chorionic gonadotropin before embryo transfer improve the pregnancy rate in vitro fertilization/intracytoplasmic sperm injection (IVFICSI) cycles? A prospective randomized controlled trial. Reprod Sci 2016;23:102A. [Google Scholar]
- Fancsovits P, Lehner A, Murber A, Kaszas Z, Rigo J, Urbancsek J.. Effect of hyaluronan-enriched embryo transfer medium on IVF outcome: a prospective randomized clinical trial. Arch Gynecol Obstet 2015;291:1173–1179. [DOI] [PubMed] [Google Scholar]
- Fancsovits P, Murber A, Gilan Z, Rigo J, Urbancsek J.. Effect of hyaluronan containing transfer media on pregnancy and implantation rates in human IVF-ET cycles. A prospective randomized study. Hum Reprod 2011;26:124. [Google Scholar]
- Farquhar C. Introduction: add-ons for assisted reproductive technology: can we be honest here? Fertil Steril 2019;112:971–972. [DOI] [PubMed] [Google Scholar]
- Fasano G, Antonacci R, Biramane J, Mbongolo G, Thi Vanhelleputte NM.. C. Clinical outcomes after use of embryo-glue as a human embryo transfer (ET) medium in warming cycles. Hum Reprod 2016;31:204–205. [Google Scholar]
- Feichtinger W, Strohmer H, Radner KM, Goldin M.. The use of fibrin sealant for embryo transfer: development and clinical studies. Hum Reprod 1992;7:890–893. [DOI] [PubMed] [Google Scholar]
- Fekih M, Chachia S, Zarrouk W, Khairi H.. Effect of ibuprophen administration before embryo transfer on IVF outcome: a randomized controlled trial. Fertil Steril 2013;100:S122. [Google Scholar]
- Foutouh I, Youssef M, Tolba M, Rushdi M, Nakieb A, Meguid W.. Does embryo transfer catheter type affect pregnancy rate? Middle East Fertil Soc 2003;8:154–158. [Google Scholar]
- Franco JG, Martins AMVC, Baruffi RLR, Mauri AL, Petersen CG, Felipe V, Contart P, Pontes A, Oliveira JBA.. Best site for embryo transfer: the upper or lower half of endometrial cavity? Hum Reprod 2004;19:1785–1790. [DOI] [PubMed] [Google Scholar]
- Fratterelli JL, Leondires MR, Fong K, Theall A, Locatelli S, Scott RT.. Laser acupuncture before and after embryo transfer improves ART delivery rates: results of a prospective randomized double-blinded placebo controlled five-armed trial involving 1000 patients. Fertil Steril 2008;90:S105. [Google Scholar]
- Friedler S, Raziel A, Schachter M, Strassburger D, Kasterstein E, Komaroversusky D.. Efficacy of hyaluronan-enriched embryo transfer medium in patients with repeated IVF-ET failures. Hum Reprod 2005;20:159. [Google Scholar]
- Friedler S, Schachter M, Strassburger D, Esther K, Ron El R, Raziel A.. A randomized clinical trial comparing recombinant hyaluronan/recombinant albumin versus human tubal fluid for cleavage stage embryo transfer in patients with multiple IVF-embryo transfer failure. Hum Reprod 2007;22:2444–2448. [DOI] [PubMed] [Google Scholar]
- Gaikwad S, Garrido N, Cobo A, Pellicer A, Remohi J.. Bed rest after embryo transfer negatively affects in vitro fertilization: a randomized controlled clinical trial. Fertil Steril 2013;100:729–735.e2. [DOI] [PubMed] [Google Scholar]
- Galiano V, Orvieto R, Machtinger R, Nahum R, Garzia E, Sulpizio P, Marconi AM, Seidman D.. “Add-Ons” for assisted reproductive technology: do patients get honest information from fertility clinics’ websites? Reprod Sci 2021;28:3466–3472. [DOI] [PubMed] [Google Scholar]
- Garcı’a-Velasco JA, Isaza V, Martinez-Salazar J, Landazábal A, Requena A, Remohı’ J, Simón C, Transabdominal ultrasound-guided embryo transfer does not increase pregnancy rates in oocyte recipients. Fertil Steril 2002;78:534–539. [DOI] [PubMed] [Google Scholar]
- Garcı’a-Velasco JA, Martinez-Salazar J, Isaza V, Landazabal A, Requena A, Simón C.. Does ultrasound guidance at embryo transfers improve pregnancy rates in oocyte recipients? Fertil Steril 2001;76:S75–S76. [DOI] [PubMed] [Google Scholar]
- Gavrizi SZ, Skillern A.. Does massage therapy immediately prior to embryo transfer improve clinical pregnancy rate in IVF-PGT-A (in-vitro fertilization-preimplantation genetic testing for aneuploidy) cycles? Fertil Steril 2019;112:e184–e185. [Google Scholar]
- Ghazzawi IM, Al-Hasani S, Karaki R, Souso S.. Transfer technique and catheter choice influence the incidence of transcervical embryo expulsion and the outcome of IVF. Hum Reprod 1999;14:677–682. [DOI] [PubMed] [Google Scholar]
- Gilberto Almodin C, Cibele V, Câmara M, Gonçalves P, Pereira C, Lopes Paixão C, Nakano R. Estudo comparativo entre dois cateteres diferentes usados para transferência de embriões [Comparative study between different catheters for embryo transfer]. n.d. JBRA Assist. Reprod 2009;13.4. Available online at: http://materbaby.com.br/wp-content/uploads/2020/01/Artigo-Estudo-comparativo-entre-dois-cateteres-diferentes-usados-para-transfer%C3%AAncia-de-embri%C3%B5es.pdf (October 2021, date last accessed).
- Glass KB, Green CA, Fluker MR, Schoolcraft WB, McNamee PI, Meldrum DR.. Multicenter randomized controlled trial of cervical irrigation at the time of embryo transfer. Fertil Steril 2000;74:S31. [Google Scholar]
- GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ 2004;328:1490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Groutz A, Lessing JB, Wolf Y, Azem F, Yovel I, Amit A.. Comparison of transmyometrial and transcervical embryo transfer in patients with previously failed in vitro fertilization-embryo transfer cycles and/or cervical stenosis. Fertil Steril 1997;67:1073–1076. [DOI] [PubMed] [Google Scholar]
- Grunert GM, Dunn RC, Valdes CT, Wun CC, Wun WSA.. Comparison of Wallace, Frydman DT and Cook embryo transfer catheter for IVF: a prospective randomised study [abstract]. Fertil Steril 1998;70:O–322. [Google Scholar]
- Gu YE, Zhang X, Zhang Q, Dai MC, Wu Y, Zhou Y, Qu F.. The effects of acupuncture on pregnancy outcomes of in vitro fertilization with embryo transfer: an interdisciplinary systematic review. J Gynecol Obstet Hum Reprod 2019;48:677–684. [DOI] [PubMed] [Google Scholar]
- Hafezi M, Madani T, Arabipoor A, Zolfaghari Z, Sadeghi M, Ramezanali F.. The effect of intrauterine human chorionic gonadotropin flushing on live birth rate after vitrified-warmed embryo transfer in programmed cycles: a randomized clinical trial. Arch Gynecol Obstet 2018;297:1571–1576. [DOI] [PubMed] [Google Scholar]
- Hannoun A, Zreik TG, Ghaziri G, Abu Musa A, Awwad J.. Effect of powdered gloves, worn at the time of embryo transfer, on the pregnancy outcome of IVF cycles. J Assist Reprod Genet 2009;26:25–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harbord R, Higgins J. METAREG: Stata module to perform meta-analysis regression. Statistical Software Components. Boston College Department of Economics, 2009. https://ideas.repec.org/c/boc/bocode/s446201.html (October 2021, date last accessed).
- Harbord RM, Harris RJ, Sterne JAC.. Updated tests for small-study effects in meta-analyses. Stata J 2009;9:197–210. [Google Scholar]
- Hauzman E, Kohls G, Barrio A, Martinez-Salazar J, Iglesias C, Garcia-Velasco JA.. Comparison of embryo transfer in egg donation recipients with transvaginal and transabdominal ultrasound: a randomized pilot study. Hum Reprod 2013;28:241.23081868 [Google Scholar]
- He Y, Wu H, He X, Xing Q, Zhou P, Cao Y, Wei Z.. Administration of atosiban in patients with endometriosis undergoing frozen–thawed embryo transfer: a prospective, randomized study. Fertil Steril 2016;106:416–422. [DOI] [PubMed] [Google Scholar]
- Hebisha SA, Aboelazm BA, Adel HM, Ahmed AI.. Impact of the oxytocin receptor antagonist (ATOSIBAN) administered shortly before embryo transfer on pregnancy outcome after intracytoplasmic sperm injection (ICSI). Fertil Steril 2016;106:e88–e89. [Google Scholar]
- Hong KH, Forman EJ, Werner MD, Upham KM, Gumeny CL, Winslow AD, Kim TJ, Scott RT.. Endometrial infusion of human chorionic gonadotropin at the time of blastocyst embryo transfer does not impact clinical outcomes: a randomized, double-blind, placebo-controlled trial. Fertil Steril 2014;102:1591–1595.e2. [DOI] [PubMed] [Google Scholar]
- Hosseini RS, Farzad L, Abdollahi S, Nouri M, Ghasemzadeh A, Hamdi K, Soleimanpour H.. Effect of intrauterine injection of human chorionic gonadotropin before frozen-thawed embryo transfer on implantation and clinical pregnancy rate: a randomized controlled trial. Int J Womens Health Reprod Sci 2016;4:200–203. [Google Scholar]
- Kan AKS, Abdalla HI, Gafar AH, Nappi L, Ogunyemi BO, Thomas A, Ola-Ojo OO.. Embryo transfer: ultrasound-guided versus clinical touch. Hum Reprod 1999;14:1259–1261. [DOI] [PubMed] [Google Scholar]
- Kandari S. Time lapse selected elective single embryo transfer in hyaluronan enriched transfer medium in PCOS improves live birth rates compared to use of conventional embryo transfer media. a possible alternative to freeze-all cycles in PCOS. Fertil Steril 2019;112:e47–e48. [Google Scholar]
- Karande V, Hazlett D, Vietzke M, Gleicher N.. A prospective randomized comparison of the Wallace catheter and the Cook Echo-Tip® catheter for ultrasound-guided embryo transfer. Fertil Steril 2002;77:826–830. [DOI] [PubMed] [Google Scholar]
- Karavani G, Ben-Meir A, Shufaro Y, Hyman JH, Revel A.. Transvaginal ultrasound to guide embryo transfer: a randomized controlled trial. Fertil Steril 2017;107:1159–1165. [DOI] [PubMed] [Google Scholar]
- Karimian L, Naghibi ZH, Yazdi PE, Moini A, Valojerdi MR, Akhondi MM, Shahverdi AH, Movaghar B, Hassani F, Sedighi-Gilani MA.. 147 The effect of intercourse on b HCG level and pregnancy outcome after IVF cycles retrospective evaluation of mechanical and laser assisted hatching efficiency in two different age groups. Reprod Biomed Online 2010;20:S65. [Google Scholar]
- Korosec S, Virant-Klun I, Tomazevic T, Zech NH, Meden-Vrtovec H.. Single fresh and frozen–thawed blastocyst transfer using hyaluronan-rich transfer medium. Reprod Biomed Online 2007;15:701–707. [DOI] [PubMed] [Google Scholar]
- Kosmas IP, Janssens R, Munck L, de Turki H, Al Elst J, van der Tournaye H, Devroey P.. Ultrasound-guided embryo transfer does not offer any benefit in clinical outcome: a randomized controlled trial. Hum Reprod 2007;22:1327–1334. [DOI] [PubMed] [Google Scholar]
- Krampl E, Zegermacher G, Eichler C, Obruca A, Strohmer H, Feichtinger W.. Air in the uterine cavity after embryo transfer. Fertil Steril 1995;63:366–370. [DOI] [PubMed] [Google Scholar]
- Laokirkkiat P, Thanaboonyawat I, Boonsuk S, Petyim S, Prechapanich J, Choavaratana R.. Increased implantation rate after intrauterine infusion of a small volume of human chorionic gonadotropin at the time of embryo transfer: a randomized, double-blind controlled study. Arch Gynecol Obstet 2019;299:267–275. [DOI] [PubMed] [Google Scholar]
- Lavery S, Ravhon A, Skull J, Ellenbogen A, Winston R.. A prospective randomized controlled trial of Wallace and Rocket embryo transfer catheters in an IVF–embryo transfer programme [abstract]. Hum Reprod 2001;16:124. [DOI] [PubMed] [Google Scholar]
- Leao R, Cambiaghi A, Leao B, Alvarez A, Figueiredo P. Intrauterine injection of human chorionic gonadotropin before embryo transfer may improve the pregnancy rates in in vitro fertilization cycles of patients with repeated implantation failures. In: Proceedings of the 5th IVI International Congress.2013. Seville, Spain. Available online at: https://www.comtecmed.com/ivi/2013/Uploads/Editor/abstract_66.pdf (October 2021, date last accessed).
- Lensen S, Chen S, Goodman L, Rombauts L, Farquhar C, Hammarberg K.. IVF add-ons in Australia and New Zealand: a systematic assessment of IVF clinic websites. Aust N Z J Obstet Gynaecol 2021;61:430–438. [DOI] [PubMed] [Google Scholar]
- Levi-Setti PE, Albani E, Baggiani AM, Zannoni E, Colombo G, Liprandi V.. Prospective randomized study comparing two soft catheters for embryo transfer. Fertil Steril 2002;78:S234–S235. [Google Scholar]
- Lewin A, Schenker JG, Avrech O, Shapira S, Safran A, Friedler S.. The role of uterine straightening by passive bladder distension before embryo transfer in IVF cycles. J Assist Reprod Genet 1997;14:32–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li R, Lu L, Hao G, Zhong K, Cai Z, Wang W.. Abdominal ultrasound-guided embryo transfer improves clinical pregnancy rates after in vitro fertilization: experiences from 330 clinical investigations. J Assist Reprod Genet 2005;22:3–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lin B, Pang Z, Jiang J.. Fixed and random effects selection by REML and pathwise coordinate optimization. J Comput Graph Stat 2013;22:341–355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lorusso F, Depalo R, Bettocchi S, Vacca M, Vimercati A, Selvaggi L.. Outcome of in vitro fertilization after transabdominal ultrasound–assisted embryo transfer with a full or empty bladder. Fertil Steril 2005;84:1046–1048. [DOI] [PubMed] [Google Scholar]
- MacLennan AH, Kerin JFP, Kirby C, Grant P, Warnes GM, Cox LW, Bryant‐Greenwood G, Greenwood F.. The effect of porcine relaxin vaginally applied at human embryo transfer in an in vitro fertilization programme. Aust N Z J Obstet Gynaecol 1985;25:68–71. [DOI] [PubMed] [Google Scholar]
- Madani T, Ashrafi M, Jahangiri N, Abadi AB, Lankarani N.. Improvement of pregnancy rate by modification of embryo transfer technique: a randomized clinical trial. Fertil Steril 2010;94:2424–2426. [DOI] [PubMed] [Google Scholar]
- Madaschi C, Braga DPAF, de Cássia Savio Figueira R, Iaconelli A, Borges E.. Effect of acupuncture on assisted reproduction treatment outcomes. Acupunct Med 2010;28:180–184. [DOI] [PubMed] [Google Scholar]
- Mahani IM, Davar R.. Hyaluronic acid versus albumin in human embryo transfer medium. East Mediterr Health J 2007;13:876–880. [PubMed] [Google Scholar]
- Mahlstedt PP, Macduff S, Bernstein J.. Emotional factors and the in vitro fertilization and embryo transfer process. J in Vitro Fert Embryo Transf 1987;4:232–236. [DOI] [PubMed] [Google Scholar]
- Mains L, van Voorhis BJ.. Optimizing the technique of embryo transfer. Fertil Steril 2010;94:785–790. [DOI] [PubMed] [Google Scholar]
- Maldonado LG, Ajzen SA, Busato WC, Iaconelli A, Bibancos M, Borges E.. Impact of previous hysterossonometry on embryo transfer. Fertil Steril 2005;84:S364. [Google Scholar]
- Malhotra N, Sarkar P.. Pregnancy outcome after bed rest versus early ambulation following embryo transfer during IVF/ICSI cycles-a randomised controlled study. Fertil Steril 2019;112:e146. [Google Scholar]
- Malina A, Pooley JA.. Psychological consequences of IVF fertilization—review of research. Ann Agric Environ Med 2017;24:554–558. [DOI] [PubMed] [Google Scholar]
- Mansour R. Minimizing embryo expulsion after embryo transfer: a randomized controlled study. Hum Reprod 2005;20:170–174. [DOI] [PubMed] [Google Scholar]
- Mansour R, Tawab N, Kamal O, El-Faissal Y, Serour A, Aboulghar M, Serour G.. Intrauterine injection of human chorionic gonadotropin before embryo transfer significantly improves the implantation and pregnancy rates in in vitro fertilization/intracytoplasmic sperm injection: a prospective randomized study. Fertil Steril 2011;96:1370–1374.e1. [DOI] [PubMed] [Google Scholar]
- Marconi G, Young E, Vilela M, Bello A, Young E, Sueldo C.. Prospective randomized comparison of an ultrasound-guided embryo transfer versus a blind catheter placement. Fertil Steril 2003;80:130. [Google Scholar]
- Martínez F, Coroleu B, Parriego M, Carreras O, Belil I, Parera N, Hereter L, Buxaderas R, Barri PN.. Ultrasound-guided embryo transfer: immediate withdrawal of the catheter versus a 30 second wait. Hum Reprod 2001;16:871–874. [DOI] [PubMed] [Google Scholar]
- Matorras R, Urquijo E, Mendoza R, Corcóstegui B, Expósito A, Rodríguez-Escudero F.. Ultrasound-guided embryo transfer improves pregnancy rates and increases the frequency of easy transfers. Hum Reprod 2002;17:1762–1766. [DOI] [PubMed] [Google Scholar]
- Mayer JF, Nehchiri F, Jones EC, Weedon VM, Kalin HL, Lanzendorf SE, Oehinger SC, Toner JP, Muasher SJ.. Prospective randomized analysis of the impact of two different transfer catheters on clinical pregnancy rates [abstract]. Fertil Steril 1999;1:144–145. [Google Scholar]
- McDonald JA, Norman RA.. Randomized controlled trial of a soft double lumen embryo transfer catheter versus a firm single lumen catheter: significant improvements in pregnancy rates. Hum Reprod 2002;17:1502–1506. [DOI] [PubMed] [Google Scholar]
- McIlveen M, Lok FD, Pritchard J, Lashen H.. Modern embryo transfer catheters and pregnancy outcome: a prospective randomized trial. Fertil Steril 2005;84:996–1000. [DOI] [PubMed] [Google Scholar]
- Meriano J, Weissman A, Greenblatt EM, Ward S, Casper RF.. The choice of embryo transfer catheter affects embryo implantation after IVF. Fertil Steril 2000;74:678–682. [DOI] [PubMed] [Google Scholar]
- Mitchell JD, Wardle PG, Foster PA, Hull MGR.. Effect of bladder filling on embryo transfer. J In Vitro Fert Embryo Transf 1989;6:263–265. [DOI] [PubMed] [Google Scholar]
- Moini A, Kiani K, Bahmanabadi A, Akhoond M, Akhlaghi A.. Improvement in pregnancy rate by removal of cervical discharge prior to embryo transfer in ICSI cycles: a randomised clinical trial. Aust N Z J Obstet Gynaecol 2011;51:315–320. [DOI] [PubMed] [Google Scholar]
- Moon HS, Park SH, Lee JO, Kim KS, Joo BS.. Treatment with piroxicam before embryo transfer increases the pregnancy rate after in vitro fertilization and embryo transfer. Fertil Steril 2004;82:816–820. [DOI] [PubMed] [Google Scholar]
- Moraga-Sanchez R, Saucedo-De La Llata E, Batiza-Resendiz V, Santos-Haliscak R, Galache-Vega P.. Ultrasound influence and 30 second wait in embryo transfer. Hum Reprod 2004;19:127. [Google Scholar]
- Moraloglu O, Tonguc E, Var T, Zeyrek T, Batioglu S.. Treatment with oxytocin antagonists before embryo transfer may increase implantation rates after IVF. Reprod Biomed Online 2010;21:338–343. [DOI] [PubMed] [Google Scholar]
- Morbeck D. Prospective randomized clinical trial of novel implantation promoting medium (EmbryoGlue) to improve IVF success rates [NTC00588250] ClinicalTrialsgov. 2007. Available at: https://www.clinicaltrials.gov/ct2/show/NCT00588250 (Date last accessed October 2021).
- Moreno V, Balasch J, Vidal E, Calafell JM, Cívico S, Vanrell JA.. Air in the transfer catheter does not affect the success of embryo transfer. Fertil Steril 2004;81:1366–1370. [DOI] [PubMed] [Google Scholar]
- Mortimer ST, Fluker M, Yuzpe A.. Effect of embryo transfer catheter on implantation rates. Fertil Steril 2002;78:S17–S18. [Google Scholar]
- Mostajeran F, Godazandeh F, Ahmadi SM, Movahedi M, Jabalamelian SA.. Effect of intrauterine injection of human chorionic gonadotropin before embryo transfer on pregnancy rate: a prospective randomized study. J Res Med Sci 2017;22:6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moy I, Milad M, Barnes R, Confino E, Kazer R, Zhang X.. Randomized controlled trial: effects of acupuncture on pregnancy rates in women undergoing in vitro fertilization. Fertil Steril 2011;95:583–587. [DOI] [PubMed] [Google Scholar]
- Murphy EM, Nichols J, Somkuti SG, Sobel M, Braverman A, Barmat LI.. Randomized trial of harp therapy during in vitro fertilization-embryo transfer. J Evid Based Complementary Altern Med 2014;19:93–98. [DOI] [PubMed] [Google Scholar]
- Nancarrow L, Tempest N, Drakeley AJ, Homburg R, Russell R, Hapangama DK.. National survey highlights the urgent need for standardisation of embryo transfer techniques in the UK. J Clin Med 2021;10:2839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nazari A, Askari HA, Check JH, O'Shaughnessy A.. Embryo transfer technique as a cause of ectopic pregnancy in in vitro fertilization. Fertil Steril 1993;60:919–921. [PubMed] [Google Scholar]
- Ng EHY, Li RHW, Chen L, Lan VTN, Tuong HM, Quan S.. A randomized double blind comparison of atosiban in patients undergoing IVF treatment. Hum Reprod 2014;29:2687–2694. [DOI] [PubMed] [Google Scholar]
- Ng KKL, Rozen G, Stewart T, Agresta F, Polyakov A.. Does nifedipine improve outcomes of embryo transfer? Interim analysis of a randomized, double blinded, placebo-controlled trial. Medicine (Baltimore) 2019;98:e14251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nihat Candan Z, Avcil F, Özden H, Uslu H, Karaman Y.. Comparing the performance of the Cook and the Prodimed embryo transfer catheters. Reprod Biomed Online 2014;28:S15. [Google Scholar]
- Obidniak D, Gzgzyan A, Dzhemlikhanova L, Feoktistov A.. Effect of colony-stimulating growth factor on outcome of frozen-thawed embryo transfer in patients with repeated implantation failure. Fertil Steril 2016;106:e134–e135. [Google Scholar]
- Obidniak D, Gzgzyan A, Feoktistov A, Niauri D.. Randomized controlled trial evaluating efficacy of autologous platelet-rich plasma therapy for patients with recurrent implantation failure. Fertil Steril 2017;108:e370. [Google Scholar]
- Ocal P, Cepni I, Idil MH, Salihoglu F, Irez T, Aksu F.. Appropriate embryo transfer technique improves the pregnancy rate in human in vitro fertilization. Middle East Fertil Soc J 2003;8:65–68. [Google Scholar]
- Omodei U, Piccioni G, Tombesi S, Dordoni D, Fallo L, Ghilardi F.. Effect of acupuncture on rates of pregnancy among women undergoing in vitro fertilization. Fertil Steril 2010;94:266. [Google Scholar]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE.. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paulus W, Zhang M, Strehler E, El-Danasouri I, Sterzik K.. Influence of acupuncture on the pregnancy rate in patients who undergo assisted reproduction therapy. Fertil Steril 2002;77:721–724. [DOI] [PubMed] [Google Scholar]
- Paulus W, Zhang M, Strehler E, Seybold B, Sterzik K.. Placebo-controlled trial of acupuncture effects in assisted reproduction therapy. Hum Reprod 2003;18:18–19. [Google Scholar]
- Peikrishvili R, Evrard B, Pouly JL, Janny L.. L’antibiothérapie prophylactique (amoxicilline + acide clavulanique) avant transfert pour fécondation in vitro est inutile: résultats d’une étude randomisée. J Gynécol Obstét Biol Reprod 2004;33:713–719. [DOI] [PubMed] [Google Scholar]
- Penzias A, Bendikson K, Butts S, Coutifaris C, Falcone T, Fossum G, Gitlin S, Gracia C, Hansen K, La Barbera A. et al. Performing the embryo transfer: a guideline. Fertil Steril 2017a;107:882–896. [DOI] [PubMed] [Google Scholar]
- Penzias A, Bendikson K, Butts S, Coutifaris C, Falcone T, Fossum G, Gitlin S, Gracia C, Hansen K, Mersereau J. et al. ; Practice Committee of the American Society for Reproductive Medicine. Electronic address: ASRM@asrm.org. Standard embryo transfer protocol template: a committee opinion. Fertil Steril 2017b;107:897–900. [DOI] [PubMed] [Google Scholar]
- Perez O, Adriaanse H, Tilley B, Navarrete G, Lay L, Little LM, Gada R, Lawrence L, Lee K, Thomas MR.. The effect of extended blastocyst exposure of hyaluronan enriched transfer media on implantation rate in frozen embryo transfers. Fertil Steril 2019;112:e438. [Google Scholar]
- Perin PM, Neves PA, Maluf M.. The influence of two different transfer catheters on the pregnancy rate in a human in vitro fertilization/embryo transfer program. Fertil Steril 1997;1997:220. [Google Scholar]
- Porat N, Boehnlein LM, Schouweiler CM, Kang J, Lindheim SR.. Interim analysis of a randomized clinical trial comparing abdominal versus transvaginal ultrasound-guided embryo transfer. J Obstet Gynaecol Res 2010;36:384–392. [DOI] [PubMed] [Google Scholar]
- Pottie K, Gorber SC, Joffres M, Lindsay P, Brauer P, Jaramillo A, Tonelli M.. Estimating benefits and harms of screening across subgroups: the Canadian Task Force on Preventive Health Care integrates the GRADE approach and overcomes minor challenges. J Clin Epidemiol 2012;65:1245–1248. [DOI] [PubMed] [Google Scholar]
- Prapas Y, Prapas N, Hatziparasidou A, Prapa S, Nijs M, Vanderzwalmen P, Vlassis G, Jones EE.. The echoguide embryo transfer maximizes the IVF results. Acta Eur Fertil 1995;26:113–115. [PubMed] [Google Scholar]
- Prato LD, Borini A.. Effect of piroxicam administration before embryo transfer on IVF outcome: a randomized controlled trial . Reprod Biomed Online 2009;19:604–609. [DOI] [PubMed] [Google Scholar]
- Purcell KJ, Schembri M, Telles TL, Fujimoto VY, Cedars MI.. Bed rest after embryo transfer: a randomized controlled trial. Fertil Steril 2007;87:1322–1326. [DOI] [PubMed] [Google Scholar]
- Qu F, Zhang D, Chen L-T, Wang F-F, Pan J-X, Zhu Y-M, Ma C-M, Huang Y-T, Ye X-Q, Sun S-J. et al. Auricular acupressure reduces anxiety levels and improves outcomes of in vitro fertilization: a prospective, randomized and controlled study. Sci Rep 2014;4:5028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ravhon A, Nahum H, Weissman A, Biran G, Umansky N, Levran D.. Embryo transfer in hyaluronan enriched transfer medium does not improve pregnancy rate in IVF treatment. Fertil Steril 2005;84:S376–S377. [Google Scholar]
- Revelli A, Rovei V, Dalmasso P, Gennarelli G, Racca C, Evangelista F, Benedetto C.. Large randomized trial comparing transabdominal ultrasound-guided embryo transfer with a technique based on uterine length measurement before embryo transfer. Ultrasound Obstet Gynecol 2016;48:289–295. [DOI] [PubMed] [Google Scholar]
- Rezábek K, Koryntova D, Zivny J.. Does bedrest after embryo transfer cause a worse outcome in in vitro fertilization? Ceska Gynekol 2001;66:175–178. [PubMed] [Google Scholar]
- Rhodes TL, Higdon HL, Boone WR.. Comparison of pregnancy rates for two embryo-transfer catheters. Fertil Steril 2007;87:411–416. [DOI] [PubMed] [Google Scholar]
- Rinaldi L, Floccari A, Selman H.. Ultrasound guidance of embryo transfer: a role for midwife. Sex Reprod Healthc 2014;5:47–49. [DOI] [PubMed] [Google Scholar]
- Ruhlman C, Bisoli C, Terrado G, Rolla ED, Nicholson RE, Gnocchi D.. The inefficacy of cervical mucus aspiration prior to embryo transfer: a prospective randomized trial [abstract]. ASRM/CFAS Conjoint Annual Meeting. Fertil Steril 1999;71:154. [Google Scholar]
- Saldeen P, Abou-Setta AM, Bergh T, Sundström P, Holte J.. A prospective randomized controlled trial comparing two embryo transfer catheters in an ART program. Fertil Steril 2008;90:599–603. [DOI] [PubMed] [Google Scholar]
- Sallam HN, Agameya AF, Rahman AF, Ezzeldin F, Sallam AN.. Ultrasound measurement of the uterocervical angle before embryo transfer: a prospective controlled study. Hum Reprod 2002;17:1767–1772. [DOI] [PubMed] [Google Scholar]
- Santibañez Á, García J, Pashkova O, Colín O, Castellanos G, Sánchez AP, de la Jara JF.. Effect of intrauterine injection of human chorionic gonadotropin before embryo transfer on clinical pregnancy rates from in vitro fertilisation cycles: a prospective study. Reprod Biol Endocrinol 2014;12:9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saravelos SH, Kong GWS, Chung JPW, Mak JSM, Chung CHS, Cheung LP, Li T-C.. A prospective randomized controlled trial of 3D versus 2D ultrasound-guided embryo transfer in women undergoing ART treatment. Hum Reprod 2016;31:2255–2260. [DOI] [PubMed] [Google Scholar]
- Schoolcraft W, Lane M, Stevens J, Gardner DK.. Increased hyaluronan concentration in the embryo transfer medium results in a significant increase in human embryo implantation rate. Fertil Steril 2002;78:S5. [Google Scholar]
- Schwarze JE, Crosby J, Mackenna A.. Atosiban improves the outcome of embryo transfer. A systematic review and meta-analysis of randomized and non-randomized trials. JBRA Assist Reprod 2020;24:421–427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seto MTY, Cheung KW, Lo TK, Ng EHY.. Pregnancy outcomes of women randomized to receive real versus placebo acupuncture on the day of fresh or frozen-thawed embryo transfer. Eur J Obstet Gynecol Reprod Biol 2017;218:119–122. [DOI] [PubMed] [Google Scholar]
- Shaker AG, Fleming R, Jamieson ME, Yates RWS, Coutts JRT.. Infertility: assessments of embryo transfer after in-vitro fertilization: effects of glyceryl trinitrate. Hum Reprod 1993;8:1426–1428. [DOI] [PubMed] [Google Scholar]
- Sigalos GΑ, Michalopoulos Y, Kastoras AG, Triantafyllidou O, Vlahos NF.. Low versus high volume of culture medium during embryo transfer: a randomized clinical trial. J Assist Reprod Genet 2018;35:693–699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simon A, Safran A, Revel A, Aizenman E, Reubinoff B, Porat-Katz A, Lewin A, Laufer N.. Hyaluronic acid can successfully replace albumin as the sole macromolecule in a human embryo transfer medium. Fertil Steril 2003;79:1434–1438. [DOI] [PubMed] [Google Scholar]
- Singh R, Singh M.. Intra‐uterine administration of human chorionic gonadotrophin (hCG) before embryo transfer in recurrent implantation failure (RIF) patients improves implantation and pregnancy rates in IVF‐ICSI cycles. Hum Reprod 2014;29:79. [Google Scholar]
- Singh R, Singh M.. P-296 RCT of intra-uterine administration or subcutanious injection of GCSF (granulocyte colony-stimulating factor) before embryo-transfer on resistant thin endometrium in IVF. Hum Reprod 2018;33:i1–i541. [Google Scholar]
- Singh R, Singh M, Jindal A, Jindal P.. A prospective randomized controlled study (RCT) of intra-uterine administration of granulocyte colony-stimulating factor (G-CSF) before embryo-transfer on resistant thin endometrium in IVF cycles. Hum Reprod 2015;30:120. [Google Scholar]
- Smith CA, Armour M, Shewamene Z, Tan HY, Norman RJ, Johnson NP.. Acupuncture performed around the time of embryo transfer: a systematic review and meta-analysis. Reprod Biomed Online 2019;38:364–379. [DOI] [PubMed] [Google Scholar]
- So E, Ng E, Wong Y, Lau E, Yeung W, Ho P.. A randomized double blind comparison of real and placebo acupuncture in IVF treatment. Hum Reprod 2009;24:341–348. [DOI] [PubMed] [Google Scholar]
- So E, Ng E, Wong Y, Yeung W, Ho P.. Acupuncture for frozen-thawed embryo transfer cycles: a double-blind randomized controlled trial. Reprod Biomed Online 2010;20:814–821. [DOI] [PubMed] [Google Scholar]
- Song Z-R, Zhao X-H, Bai X-H, Lu Y-H, Zhang H-J, Wang Y-X, Lu R.. Application of oxytocin antagonists in thaw embryo transfer. Zhonghua Fu Chan Ke Za Zhi 2013;48:667–670. [PubMed] [Google Scholar]
- Soroka D, Wells G, Kotaba DD.. Does the aspiration of cervical mucus prior to embryo transfer in women undergoing in vitro fertilization and embryo transfer improve pregnancy rates? Fertil Steril 1999;72:S102. [Google Scholar]
- Steptoe PC, Edwards RG.. Birth after the reimplantation of a human embryo. Lancet 1978;2:366. [DOI] [PubMed] [Google Scholar]
- Sterne JAC, Harbord RM.. Funnel plots in meta-analysis. Stata J 2004;4:127–141. [Google Scholar]
- Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge SM.. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019;366:l4898. [DOI] [PubMed] [Google Scholar]
- Stocker LJ, Hardingham KL, Cheong YC.. A randomized controlled trial assessing whether listening to music at time of embryo transfer effects anxiety levels. Gynecol Obstet 2016;6:1–6. [Google Scholar]
- Sutton AJ, Duval SJ, Tweedie RL, Abrams KR, Jones DR.. Empirical assessment of effect of publication bias on meta-analyses. BMJ 2000;320:1574–1577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Talwar P, Naredi N, Sandeep K, Joneja G, Duggal B.. Does catheter choice during embryo transfer alter the pregnancy rate? Med J Armed Forces India 2011;67:311–314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tang OS, Ng EHY, So WWK, Ho PC.. Ultrasound-guided embryo transfer: a prospective randomized controlled trial. Hum Reprod 2001;16:2310–2315. [DOI] [PubMed] [Google Scholar]
- Teixeira DM, Dassuncão LA, Vieira CVR, Barbosa MAP, Coelho Neto MA, Nastri CO, Martins WP.. Ultrasound guidance during embryo transfer: a systematic review and meta-analysis of randomized controlled trials. Ultrasound Obstet Gynecol 2015;45:139–148. [DOI] [PubMed] [Google Scholar]
- Tierney JF, Pignon JP, Gueffyier F, Clarke M, Askie L, Vale CL, Burdett S; Cochrane IPD Meta-analysis Methods Group. How individual participant data meta-analyses have influenced trial design, conduct, and analysis. J Clin Epidemiol 2015;68:1325–1335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tomari H, Honjou K, Kunitake K, Nishimura K, Hidaka N, Nagata Y.. Effect of embryo glue transfer medium during fresh and frozen-thawed embryo transfer. Fertil Steril 2014;102:e313. [Google Scholar]
- Urman B, Yakin K, Ata B, Isiklar A, Balaban B.. Effect of hyaluronan-enriched transfer medium on implantation and pregnancy rates after day 3 and day 5 embryo transfers: a prospective randomized study. Fertil Steril 2008;90:604–612. [DOI] [PubMed] [Google Scholar]
- Valojerdi MR, Karimian L, Yazdi PE, Gilani MAS, Madani T, Baghestani AR.. Efficacy of a human embryo transfer medium: a prospective, randomized clinical trial study. J Assist Reprod Genet 2006;23:207–212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Visnova H, Tournaye HJ, Humberstone A, Terrill P, Macgregor L, Loumaye E.. A placebo-controlled, randomized, double-blind, phase 3 study assessing ongoing pregnancy rates after single oral administration of a novel oxytocin receptor antagonist, nolasiban, prior to single embryo transfer. Fertil Steril 2018;110:e45. [Google Scholar]
- Visschers B, Bots R, Peeters M, Mol B, van Dessel H.. Removal of cervical mucus: effect on pregnancy rates in IVF/ICSI. Reprod Biomed Online 2007;15:310–315. [DOI] [PubMed] [Google Scholar]
- Walker DL, Thornhill AR, Allemand MC, Tatpati LL, Wentworth MA, Tummon IS.. A randomized, controlled, double blinded trial of EmbryoGlue® in frozen embryo transfer cycles: an interim analysis. Fertil Steril 2005;84:S415–S416. [Google Scholar]
- Wang M, Deng H, Ye H.. Intrauterine injection of human chorionic gonadotropin improves pregnancy outcome in patients with repeated implantation failure in frozen-thawed embryo transfer. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2019;44:1247–1251. [DOI] [PubMed] [Google Scholar]
- van Weering HGI, Schats R, McDonnell J, Vink JM, Vermeiden JPW, Hompes PGA.. The impact of the embryo transfer catheter on the pregnancy rate in IVF. Hum Reprod 2002;17:666–670. [DOI] [PubMed] [Google Scholar]
- Weissman A, Farhi J, Steinfeld Z, Mutsafi R, Nahum H, Levran D.. A prospective, randomized study of ultrasound-guided embryo transfer. Fertil Steril 2003;80:122. [Google Scholar]
- Westergaard L, Mao Q, Krogslund M, Sandrini S, Lenz S, Grinsted J.. Acupuncture on the day of embryo transfer significantly improves the reproductive outcome in infertile women: a prospective, randomized trial. Fertil Steril 2006;85:1341–1346. [DOI] [PubMed] [Google Scholar]
- Wirleitner B, Schuff M, Vanderzwalmen P, Stecher A.. O-182 The usefulness of intrauterine hCG administration prior to blastocyst transfer in IVF-patients ≥38 years. Hum Reprod 2015a;30:i1–i501.26207012 [Google Scholar]
- Wirleitner B, Schuff M, Vanderzwalmen P, Stecher A, Okhowat J, Hradecký L, Kohoutek T, Králícková M, Spitzer D, Zech NH.. Intrauterine administration of human chorionic gonadotropin does not improve pregnancy and life birth rates independently of blastocyst quality: a randomised prospective study. Reprod Biol Endocrinol 2015b;13:70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wisanto A, Janssens R, Deschacht J, Camus M, Devroey P, van Steirteghem AC.. Performance of different embryo transfer catheters in a human in vitro fertilization program. Fertil Steril 1989;52:79–84. [DOI] [PubMed] [Google Scholar]
- Yakin K, Balaban B, Isiklar A, Bozdag H, Urman B.. Improved clinical outcome in frozen-thawed embryo transfers with the use of hyaluronan-enriched medium. Hum Reprod 2004;19:89. [Google Scholar]
- Yao Z, Vansteelandt S, Elst J, van der Coetsier T, Dhont M, de Sutter P.. The efficacy of the embryo transfer catheter in IVF and ICSI is operator-dependent: a randomized clinical trial. Hum Reprod 2009a;24:880–887. [DOI] [PubMed] [Google Scholar]
- Yao Z, Vansteelandt S, Elst J, van der Coetsier T, Dhont M, de Sutter P.. The efficacy of the embryo transfer catheter in IVF and ICSI is operator-dependent: a randomized clinical trial. Hum Reprod 2009b;24:880–887. [DOI] [PubMed] [Google Scholar]
- Yayla Abide C, Ozkaya E, Sanverdi I, Bostancı Ergen E, Kurek Eken M, Devranoglu B, Bilgiç BE, Kilicci C, Kayatas Eser S.. Prospective randomized trial comparing embryo transfers of cases with and without catheter rotation during its withdrawal. Gynecol Obstet Invest 2018;83:397–403. [DOI] [PubMed] [Google Scholar]
- Yuan C, Song H, Fan L, Su S, Dong B.. The effect of atosiban on patients with difficult embryo transfers undergoing in vitro fertilization–embryo transfer. Reprod Sci 2019;26:1613–1617. [DOI] [PubMed] [Google Scholar]
- Yung SSF, Lai SF, Lam MT, Lui EMW, Ko JKY, Li HWR, Wong JYY, Lau EYL, Yeung WSB, Ng EHY.. Hyaluronic acid–enriched transfer medium for frozen embryo transfer: a randomized, double-blind, controlled trial. Fertil Steril 2021;116:1001–1009. [DOI] [PubMed] [Google Scholar]
- Zarei A, Homayoon N, Hessami K, Hashemi A, Davoodi S, Razavi B, Ghasempour L, Alamdarloo SM.. Effect of piroxicam administration on outcome of frozen–thawed embryo transfer: a randomized, double-blinded, placebo-controlled trial. J Obstet Gynaecol Res 2021;47:296–301. [DOI] [PubMed] [Google Scholar]
- Zarei A, Parsanezhad ME, Younesi M, Alborzi S, Zolghadri J, Samsami A, Amooee S, Aramesh S.. Intrauterine administration of recombinant human chorionic gonadotropin before embryo transfer on outcome of in vitro fertilization/intracytoplasmic sperm injection: a randomized clinical trial. Iran J Reprod Med 2014;12:1–6. [PMC free article] [PubMed] [Google Scholar]
- Zegers-Hochschild FWorld Health OrganizationAdamson GD, Mouzon J, de Ishihara O, Mansour R, Nygren K, Sullivan E, Vanderpoel S.. International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised glossary of ART terminology, 2009. Fertil Steril 2009;92:1520–1524. [DOI] [PubMed] [Google Scholar]
- Zemyarska MS. Is it ethical to provide IVF add-ons when there is no evidence of a benefit if the patient requests it? J Med Ethics 2019;45:346–350. [DOI] [PubMed] [Google Scholar]
- Zhang R, Feng X-J, Guan Q, Cui W, Zheng Y, Sun W, Han J-S.. Increase of success rate for women undergoing embryo transfer by transcutaneous electrical acupoint stimulation: a prospective randomized placebo-controlled study. Fertil Steril 2011;96:912–916. [DOI] [PubMed] [Google Scholar]
- Zhong J, Zhang L.. [Transcutaneous electrical acupoint stimulation for pregnancy of in vitro fertilization-embryo transfer]. Zhongguo Zhen Jiu 2017;37:253–255. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Some or all datasets generated during and/or analysed during the current study are not publicly available but are available from the corresponding author on reasonable request.