

Abstract
The emergency food system (EFS) is a critical part of the United States’ social safety net. Using 2015–2020 Current Population Survey Food Security Supplement data, we identified trends in EFS use among food insecure, low-income households by estimating the probability of EFS use adjusting for demographics using multivariable logistic regression. From 2015–2019, between 31.0% and 34.4% of households received emergency food, while 42.4% did in 2020. EFS use did not increase in 2020 compared to prior years for older adults and non-metropolitan households. Targeted outreach should be used to expand the reach of this resource to underserved and marginalized populations.”
Keywords: Food insecurity, Emergency food, Food assistance, Current Population Survey
Introduction
Food insecurity, which occurs when a household has limited or uncertain access to sufficient amounts of nutritious foods to support an active and healthy lifestyle,(1) can negatively impact both individuals and communities. Individuals who experience food insecurity have a higher risk of developing various nutrition related chronic diseases such as type 2 diabetes, hypertension, cardiovascular disease, and osteoporosis.(2–4) Individuals who experience food insecurity tend to have higher healthcare costs,(5, 6) which could further contribute to food insecurity by limiting household resources. When food insecurity elevates healthcare costs at the population level,(7) there are further implications for communities that bear the brunt of these costs. There are also racial and ethnic inequities around food access,(8) food security,(9, 10) and nutrition related chronic diseases(10–12) likely due to ingrained, societal, and systematic factors that are outside of individual control and require large scale solutions to address.
The federal government implements a variety of food assistance programs aimed to meet the food needs of low-income households. The primary governmental program is the Supplemental Nutrition Assistance Program (SNAP), which provides benefits to participants that can be used to purchase qualifying food items though an Electronic Benefits Transfer card. SNAP has been shown to be effective in ameliorating food insecurity,(13, 14) but SNAP’s overall effectiveness is limited by low participation rates among some eligible demographic groups,(15) inadequate benefits to completely eliminate food insecurity among participants,(16–18) and barriers to program participation such as stigma(17, 19) and administrative burdens.(20) Other government programs vary in scope and often target specific demographic groups, for example children (e.g., the National School Lunch Program and School Breakfast Program) or older adults (e.g., the Congregate and Home Delivered Nutrition Services). While there is evidence these programs can be effective at addressing food insecurity,(21–23) similar issues with access(24–27) and stigma (28) exist with these programs as well.
Because of the persistence of unmet food needs in the United States, the emergency food system (EFS) has stepped in to provide low- or no-cost food to in-need households through community-based organizations.(29, 30) The terms charitable food system, food banking system, and emergency food system have been used interchangeably and refer to the same system. In the EFS, foods are procured by food banks, which are large organizations that distribute food to client-facing organizations such as food pantries, food programs, or meal sites. The EFS is a complex network of autonomous but interconnected organizations that operate across government (administering The Emergency Food Assistance Program or TEFAP; a United States Department of Agriculture (USDA) nutrition program designed to purchase surplus food from producers and provide it to low-income households), private (securing donated and purchased food from food producers, distributors, and retailers), and non-profit (distributing food to client-facing organizations and clients) sectors to source and distribute food to in need households. To give an idea of the complexity of this system and food sources, a food bank may receive USDA-sourced TEFAP foods, donated shelf-stable items from national producers and retailers, donated produce from a local producer, and purchased produce from a local vendor which are then sorted, packaged, and distributed to a food pantry that provides food to community members. While originally intended to address acute situations of limited food access, such providing food to affected households following a natural disaster, use of the EFS has become increasingly chronic and many households regularly rely upon the EFS to acquire food.(30) To give context of the scope of the EFS in the United States, Feeding America, one of the largest food banking organizations in the United States, distributed approximately 5.2 billon meals to more than 40 million people in 2019 with a cost of approximately $3.4 billion.(31) In the same year, SNAP served slightly fewer people, approximately 36 million, but provided about $55.6 billion in benefits to participants.(32)
Because EFS use is a function of both need and accessibility, one indicator of the effectiveness of the EFS is the extent to which food insecure households utilize it, especially in underserved and marginalized populations. In this manuscript, underserved refers to any populations that have been excluded from accessing food assistance services and proper nutrition for any reason and marginalized refers specifically to underserved groups which have been excluded from accessing food assistance services and proper nutrition due to unequal power dynamics and systemic discrimination in the form of racism, sexism, and/or ageism, specifically households led by Black non-Hispanic, Hispanic, female, or aged members.
Use of the EFS has steadily increased over time for all food insecure households from about 20% in 2005(33) to about 28% in 2019,(34) with a large increase to 35% during the COVID-19 pandemic in 2020.(35) There are also a substantial number of food insecure households that do not use the EFS,(35) which may be related to the presence of serious barriers to accessing these resources, including accessibility of services,(36–38) stigma,(39) and the nutritional quality of the foods available.(29, 40, 41) These barriers could prevent underserved and marginalized groups from receiving emergency food to a greater extent than the general population and result in disparities in use. For example, already marginalized groups may be less likely to engage in behaviors that are stigmatized. Additionally, having limited hours and days of operation may have disproportionate impact on underserved, low-income households without access to reliable transportation or who have a conflicting, non-flexible work schedule. It is unclear the extent to which increasing trends in use of the EFS were similar for members of underserved and marginalized groups. Since the EFS has become an important part of the food safety net in the United States, it is crucial for policymakers and stakeholders in the EFS to understand the extent to which this system is reaching in-need households and the characteristics of who uses and who does not use this resource.
To address the aforementioned gaps in understanding the use of the EFS by low-income, food insecure households in the United States, we analyzed national data collected as part of the Current Population Survey (CPS) between 2015 and 2020. We sought to describe food insecure, low-income households that use the EFS and answer the following research questions: 1) What proportion of low-income, food insecure Americans received food from an emergency food provider between 2015 and 2020? 2) Were there differences in the proportion of low-income, food insecure Americans receiving food from an emergency food provider for subpopulations of interest: households with children, with an older adult household respondent, with a non-white or Hispanic household respondent, with a female household respondent, or households in non-metropolitan areas? and 3) Across survey years, were there differences in receipt of food from an emergency food provider by demographic characteristics such as racial or ethnic identity, educational attainment, participation in government food assistance programs, or household income? Because of the impact food insecurity has on health and well-being, understanding who does and who does not use the EFS among low-income, food insecure Americans can help to identify populations that underuse this resource. This knowledge can be used to implement more effective outreach efforts, help the EFS and other food assistance services better reach underserved and marginalized households and communities, and provide direction for investigating systemic and societal barriers to use.
Methods
Data and Sample
The data for this study came from the CPS Food Security Supplement from 2015 to 2020. The CPS is a monthly survey of the non-institutionalized population conducted by the United States Census Bureau and Bureau of Labor Statistics. The CPS samples about 60,000 Americans yearly and collects data on a wide variety of economic and social characteristics.(42) The CPS uses a probability-based, multi-stage, stratified sampling design to generate state-level and nationally representative samples of the noninstitutional population aged 16 years and older.(42) The CPS uses a longitudinal design, where each household is surveyed for four consecutive months, not surveyed for the subsequent eight months, and then once again surveyed each month for four rounds, after which their participation in the CPS ends.(42) The CPS uses a combination of in-person and telephone interviews depending on the households month in sample and other considerations (e.g., a respondent requests a telephone interview for the first interview at initial contact).(42) Generally, in-person interviews take place during the first month of each of 4-month interview period while other months are conducted over the telephone.(42) Previous research has shown that interview mode does not significantly affect the validity of the food security measure used in the CPS.(43) The CPS interviewer identifies one knowledgeable member of the household to be the “household respondent”.(42) The household respondent provides information on themselves (i.e., it is self-reported) and all other members of the household (i.e., it is collected by proxy).
The Food Security Supplement is a supplemental CPS survey that asks a sub-set of households about topics related to unmet food needs. It is co-sponsored by the USDA Food and Nutrition Service and has been annually conducted in December since 2004.(42) The CPS provides household- and person-level sampling weights for the Food Security Supplement that adjust for baseline probability of selection, supplement nonresponse, and population characteristics.(42)
We analyzed data collected between 2015 and 2020. Because of the longitudinal design of CPS, some households complete the Food Security Supplement twice. To reduce the relatedness of responses across years, we only include households who were in the first four-month interview period for each year. Therefore, we can assume each year represents a cross-sectional, independent, and representative sample of the US population. We accessed data through the Integrated Public Use Microdata Series (IPUMS), an online data repository run by the Minnesota Population Center at the University of Minnesota that provides integrated and harmonized data from the CPS from 1962 to present.(44) Our population of interest consisted of households who made less than 185% of the Federal Poverty Level (FPL) and who were identified as food insecure based on the 18-item USDA food security module.(34) Because food acquisition behaviors and food security are generally household-level phenomena, our unit of analysis was the household, and we selected the household respondent to be included in the analytic sample. This resulted in a sample of 8,617 households. We also examined five subpopulations of interest: households with children (n=3,945), households with a household respondent over age 60 (n=2,446), households with a non-White or Hispanic household respondent (n=3,805), households with a female household respondent (n=5,471), and households in non-metropolitan areas (n=2,144).
Measures
Our primary outcome was use of the EFS based on two survey questions reflecting major sources of emergency food. The two questions are “In the last 12 months, did you or other adults in your household ever get emergency food from a church, a food pantry, or food bank” and “In the last 12 months, did you or other adults in your household ever eat any meals at a soup kitchen or shelter?” Our outcome was a dichotomous indicator where an affirmative response to either question was coded as EFS use and the variable was coded as no EFS use otherwise.
We included variables for year and demographics characteristics to examine the association between these factors and emergency food use. Year was a categorical variable for each year from 2015 to 2020. Household-level demographics characteristics were household size (continuous), income (Under $20,000, $20,000-$29,999, $30,000-$39,999, $40,000+), geographic region (Northeast, South, Midwest, or West), household food security status (low or very low), and participation in food assistance programs (yes/no for each: SNAP in the previous year, Free or Reduced Lunch (FRL) in the previous year, and Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) in the previous month). Respondents who replied they did not know if they participated in a program or who refused to answer the question were coded as not participating in the program. Variables for respondent-level demographic characteristics were based on the household respondent. These were age (34 or younger, 35 to 59, and 60 or older), sex (male or female), racial identification (White; Black; American Indian/Alaskan Native, Asian, Native Hawaiian and other Pacific Islander; or Multiracial), Hispanic ethnicity (Hispanic or non-Hispanic), marital status (married, separated/divorced, widowed, or never married), education (less than high school, high school or equivalent, some college or associates degree, or bachelor’s degree or higher), and employment status (employed, unemployed, or not in labor force). We consider the sex, racial identification, and Hispanic ethnicity variables as proxies for systemic and institutionalized discrimination (whether that be sexism and/or racism), as there are practices and policies within institutions related to food access and food assistance services that may negatively affect individuals and households with these identities.(45, 46) We do not consider the age variable to be a direct proxy for ageism because of the existence of economic and other supports that influence food access for older adults (e.g., receiving income supports through Social Security retirement benefits) that co-occur alongside systemic and institutionalized discrimination of older adults and our inability to disentangle groups who are and who are not affected by each, but this context should be considered when interpreting results regarding older adults.
Analysis
To examine use of the emergency food system over time, we calculated the unadjusted proportion of emergency food users in each year overall and for each subpopulation of interest. Next, to examine how use of the emergency food system differed by year and demographic characteristics, we used multivariable logistic regression to model use of the emergency food system as a function of age, marital status, race, Hispanic ethnicity, employment status, participation in governmental food assistance programs, food security status, household income, household size, geographic region, and year. We then calculated the predicated probability of using the emergency food system to produce an adjusted proportion of emergency food users in each year and for each demographic characteristic. To examine if these associations were consistent across different household types, we repeated this analysis with each subpopulation of interest (households with children, households with a household respondent over age 60, households with a non-White or Hispanic household respondent, households with a female household respondent, and households in non-metropolitan areas). We utilized the Food Security Supplement household-level sampling weights for each analysis to account for the complex survey design and non-response bias and all probabilities presented below are weighted percents. Stata 17 was used for all analyses.(47)
Results
Demographic characteristics of the analytic sample
Demographic characteristics of the overall sample and the subpopulations of interest in this study are shown in Table 1. In this sample of food insecure households with incomes less than 185% of the federal poverty level, about half of household respondents were in the 35 to 59 age group, followed by 34 and under with about a third, and the fewest were in the 60 and over age group. Household respondents were mostly female (62.7%), White (67.0%), and non-Hispanic (77.0%). Under half of the household respondents were employed and most households earned under $20,000 per year. Households were mostly located in South (43.6%), followed by the West (21.2%) and Midwest (21.0%), and the fewest were in the Northeast (14.2%). About 40% of the sample experienced very low food security. Overall, 50% participated in SNAP, about 30% participated in FRL, and 10% in WIC. Participation in nutrition assistance programs increased or decreased in subpopulations where it would be expected due to the household’s characteristics. For example, participation in WIC was about 20% in households with children.
Table 1.
Demographic characteristics as weighted mean±standard deviation or weighted proportion for food insecure households with incomes less than 185% of the federal poverty level and for subpopulations of interest between 2015 and 2020 from 2015–2020 Current Population Survey Food Security Supplement data
| Characteristic | Overall (n=8,617) | Household with children (n=3,945) | Older adult led household (n=2,446) | Non-White or Hispanic led household (n=3,805) | Female led household (n=5,471) | Non- metropolitan household (n=2,144) |
|---|---|---|---|---|---|---|
| Household size, mean±standard deviation | 2.7±1.5 | 3.9±1.3 | 1.8±1.2 | 2.9±1.5 | 2.7±1.5 | 2.5±1.7 |
| Age, % | ||||||
| 34 or under | 27.5 | 35.3 | 0.0 | 31.2 | 28.5 | 23.0 |
| 35 to 59 | 47.9 | 55.0 | 0.0 | 47.5 | 47.3 | 48.4 |
| 60 or over | 24.6 | 9.7 | 100.0 | 21.3 | 24.2 | 28.5 |
| Marital status, % | ||||||
| Married | 26.9 | 38.5 | 21.5 | 28.0 | 21.9 | 26.6 |
| Separated/divorced | 29.0 | 24.2 | 36.4 | 23.4 | 31.5 | 33.8 |
| Widowed | 9.0 | 5.6 | 26.3 | 7.2 | 11.4 | 11.8 |
| Never married | 35.1 | 31.7 | 15.8 | 41.3 | 35.2 | 27.8 |
| Sex, % | ||||||
| Male | 37.3 | 27.8 | 38.4 | 36.6 | 0.0 | 39.2 |
| Female | 62.7 | 72.2 | 61.6 | 63.4 | 100.0 | 60.8 |
| Race, % | ||||||
| White | 67.0 | 67.3 | 69.0 | 37.6 | 66.0 | 77.0 |
| Black | 25.0 | 24.6 | 24.2 | 47.2 | 26.5 | 16.2 |
| AI/AN, Asian, NHPI | 5.0 | 5.4 | 4.1 | 9.5 | 4.4 | 4.5 |
| Multiracial | 3.0 | 2.7 | 2.7 | 5.7 | 3.1 | 2.3 |
| Hispanic ethnicity, % | ||||||
| Yes | 23.0 | 30.2 | 16.2 | 43.4 | 22.4 | 7.4 |
| No | 77.0 | 69.8 | 83.8 | 56.6 | 77.6 | 92.6 |
| Education level, % | ||||||
| Less than high school | 24.6 | 24.8 | 30.3 | 30.6 | 22.3 | 24.7 |
| High school or equivalent | 33.8 | 33.8 | 32.0 | 32.1 | 32.9 | 40.5 |
| Some college or associates degree | 31.8 | 32.2 | 27.2 | 28.3 | 34.6 | 29.6 |
| Bachelor’s or higher | 9.8 | 9.2 | 10.5 | 9.0 | 10.2 | 5.2 |
| Yearly income, % | ||||||
| Under $20,000 | 57.5 | 42.4 | 68.9 | 58.4 | 57.9 | 62.3 |
| $20,000 to $29,999 | 22.8 | 24.5 | 21.8 | 21.5 | 22.8 | 20.8 |
| $30,000 to $39,999 | 12.6 | 19.5 | 6.7 | 12.6 | 12.8 | 12.0 |
| $40,000+ | 7.1 | 13.6 | 2.6 | 7.5 | 6.5 | 4.9 |
| Employment status, % | ||||||
| Employed | 43.5 | 55.8 | 13.5 | 47.7 | 43.3 | 36.3 |
| Unemployed | 7.4 | 7.7 | 3.7 | 8.0 | 6.3 | 6.2 |
| Not in labor force | 49.1 | 36.5 | 82.8 | 44.3 | 50.4 | 57.5 |
| Region, % | ||||||
| Northeast | 14.2 | 14.2 | 15.4 | 13.5 | 14.5 | 7.9 |
| Midwest | 21.0 | 20.8 | 18.4 | 15.8 | 21.6 | 26.0 |
| South | 43.6 | 42.4 | 45.9 | 47.0 | 43.6 | 51.3 |
| West | 21.2 | 22.6 | 20.3 | 23.7 | 20.3 | 14.8 |
| Food security status, % | ||||||
| Low | 59.2 | 68.3 | 57.0 | 63.1 | 60.1 | 57.7 |
| Very low | 40.8 | 31.7 | 43.0 | 36.9 | 39.9 | 42.3 |
| Free or Reduced Lunch participant, % | ||||||
| No | 73.3 | 47.7 | 93.0 | 69.2 | 68.7 | 73.6 |
| Yes | 26.7 | 52.3 | 7.0 | 30.8 | 31.3 | 26.4 |
| WIC† participant, % | ||||||
| No | 91.3 | 83.2 | 98.9 | 89.1 | 90.7 | 91.9 |
| Yes | 8.7 | 16.8 | 1.1 | 10.9 | 9.3 | 8.1 |
| SNAP‡ participant, % | ||||||
| No | 50.7 | 44.4 | 53.9 | 49.0 | 46.6 | 51.6 |
| Yes | 49.3 | 55.6 | 46.1 | 51.0 | 53.4 | 48.4 |
AI/AN, Asian, NHPI, American Indian/Alaskan Native, Asian, Native Hawaiian and other Pacific Islander
WIC, Special Supplemental Nutrition Program for Women, Infants, and Children
SNAP, Supplemental Nutrition Assistance Program
Trends in use of the emergency food system between 2015 and 2020
Between 2015 and 2020, approximately 34% (95% confidence interval: 32.7%−35.1%) of low-income, food insecure households received emergency food (See Supplemental Table 1 for unadjusted and adjusted probabilities of using the EFS with 95% confidence intervals for each year and subpopulation between 2015 and 2020). Figure 1 shows the predicted probability of using the EFS for each year adjusting for demographic characteristics and reveals some differences in trends over time for subpopulation groups in 2020. From 2015 to 2019, there were no increases in EFS use overall or for any subpopulation. In 2020, use of emergency food services increased in the overall sample and in households with children, non-White or Hispanic led households, and female led households. However, in older adult led and non-metropolitan households, the predicted probability of using the emergency food system in 2020 were similar to previous years.
Figure 1.
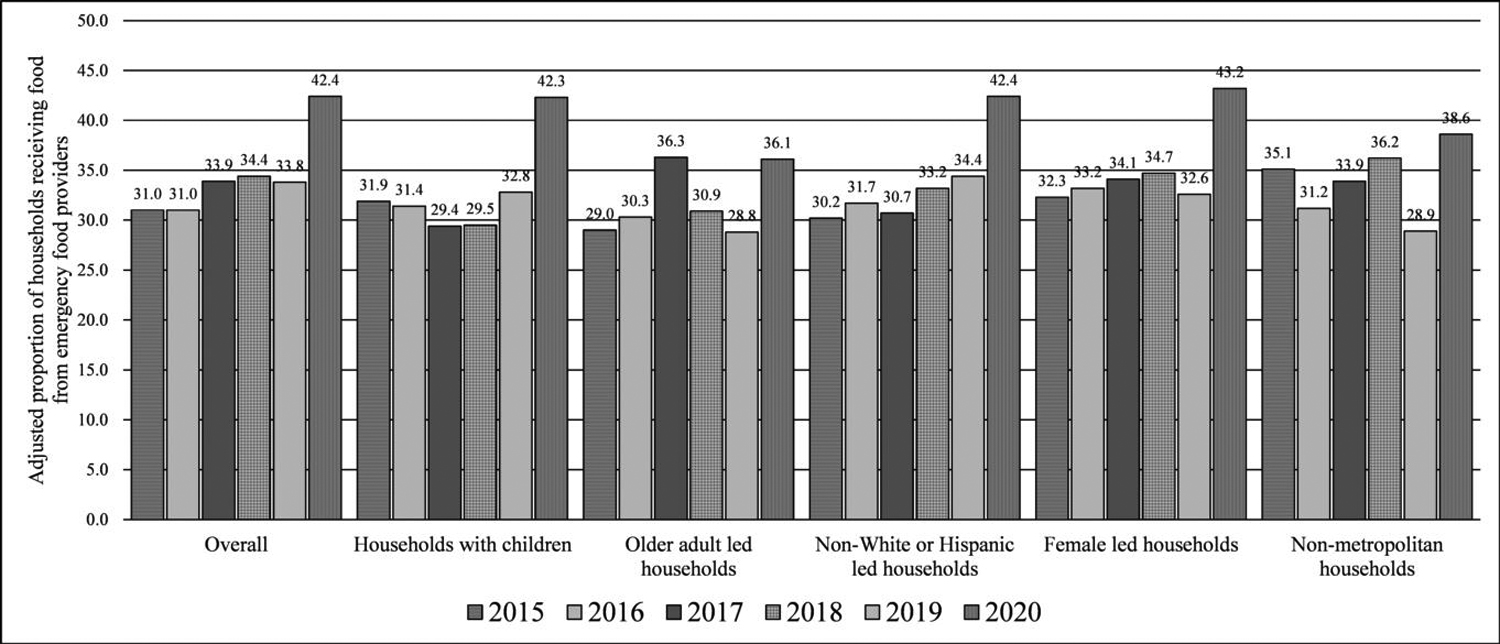
Adjusted probability of receiving emergency food for food insecure households in the United States with incomes less than 185% of the federal poverty level between 2015 and 2020 overall (n=8,617) and for households with children (n=3,945), households with a household respondent over age 60 (n=2,446), households with a non-White or Hispanic household respondent (n=3,805), households with a female household respondent (n=5,471), and households in non-metropolitan areas (n=2,144) from 2015–2020 Current Population Survey Food Security Supplement data
Demographic characteristics associated with receiving of emergency food
The estimated predicted probability of using the emergency food system for selected demographic characteristics from multivariable adjusted models are shown in Table 2. The estimated predicted probability of using the EFS for each demographic characteristics from multivariable adjusted models are shown in Supplemental Table 2. In the overall analysis, households led by respondents in the 35 to 59 age group (37.5%) were more likely to use emergency food services than those in the 34 or under group (31.8%) or 60 or older group (29.4%) that had other similar demographic characteristics. There were few differences in use of the emergency food system by age group in the subpopulation analyses. Some differences in use of emergency food services by race and ethnicity were found. Among older adults, Black led households (38.7%) were more likely to use emergency food services versus White led households (29.0%) that had other similar demographic characteristics. In contrast, after adjustment for other demographic factors, among non-metropolitan households, Black led households (26.9%) were less likely to use emergency food services versus White led households (34.2%). Multiracial led household were consistently more likely to use the emergency food system compared to White led households with other similar demographics. Receipt of emergency food was lower in Hispanic-led households (30.3%) versus non-Hispanic households adjusting for other demographics characteristics overall (35.0%), in households with children (28.2% versus 34.7%), and in female led households (30.5% versus 35.9%).
Table 2.
Predicated probability of receiving emergency food for food insecure households in the United States with incomes less than 185% of the federal poverty level for selected demographic characteristics between 2015 and 2020 from 2015–2020 Current Population Survey Food Security Supplement data
| Characteristic | Overall (n=8,617) | Household with children (n=3,945) | Older adult led household (n=2,446) | Non-White or Hispanic led household (n=3,805) | Female led household (n=5,471) | Non- metropolitan household (n=2,144) |
|---|---|---|---|---|---|---|
| Age, % | ||||||
| 34 or under | 31.8 [29.2, 34.5] | 29.8 [26.8, 32.9] | N/A | 31.7 [28.0, 35.4] | 33.7 [30.3, 37.1] | 28.1 [22.3, 33.8] |
| 35 to 59 | 37.5 [35.8, 39.2] | 34.5 [32.2, 36.9] | N/A | 36.0 [33.5, 38.6] | 39.0 [36.8, 41.2] | 37.6 [34.0, 41.1] |
| 60 or over | 29.4 [27.1, 31.8] | 33.7 [28.1, 39.3] | N/A | 31.1 [27.2, 35.0] | 28.0 [25.1, 31.0] | 32.4 [27.6, 37.3] |
| Race, % | ||||||
| White | 32.6 [31.2, 33.9] | 32.7 [30.7, 34.7] | 29.0 [26.6, 31.5] | 30.8 [25.3, 36.2] | 33.3 [31.6, 35.1] | 34.2 [31.4, 37.0] |
| Black | 35.9 [33.2, 38.7] | 31.5 [27.6, 35.5] | 38.7 [33.6, 43.9] | 34.6 [30.3, 38.8] | 36.2 [32.8, 39.6] | 26.9 [20.7, 33.0] |
| AI/AN, Asian, NHPI* | 32.3 [27.1, 37.5] | 30.8 [23.3, 38.4] | 27.5 [15.8, 39.1] | 31.2 [25.7, 36.7] | 34.4 [27.4, 41.4] | 43.0 [30.3, 55.6] |
| Multiracial | 49.4 [42.4, 56.4] | 51.0 [39.7, 62.3] | 44.7 [30.3, 59.1] | 47.1 [39.6, 54.6] | 52.7 [43.8, 61.7] | 56.0 [41.0, 70.9] |
| Hispanic ethnicity, % | ||||||
| No | 35.0 [33.6, 36.3] | 34.7 [32.6, 36.8] | 32.0 [29.7, 34.4] | 34.6 [30.8, 38.4] | 35.9 [34.2, 37.6] | 34.2 [31.6, 36.7] |
| Yes | 30.3 [27.6, 33.0] | 28.2 [24.9, 31.5] | 30.3 [24.0, 36.6] | 32.2 [26.9, 37.4] | 30.5 [27.2, 33.9] | 30.9 [22.4, 39.5] |
| Employment status, % | ||||||
| Employed | 29.4 [27.5, 31.3] | 29.6 [27.3, 32.0] | 27.6 [21.4, 33.8] | 28.7 [26.0, 31.4] | 30.8 [28.4, 33.3] | 30.7 [26.4, 35.1] |
| Unemployed | 36.5 [32.1, 40.9] | 37.1 [30.7, 43.6] | 32.2 [20.5, 43.9] | 38.2 [31.8, 44.6] | 38.0 [32.0, 44.1] | 39.0 [29.1, 48.9] |
| Not in labor force | 37.3 [35.5, 39.1] | 36.2 [33.2, 39.1] | 32.4 [30.0, 34.7] | 37.6 [34.8, 40.4] | 37.5 [35.3, 39.8] | 35.2 [31.8, 38.6] |
| Region, % | ||||||
| South | 29.8 [28.1, 31.4] | 28.0 [25.6, 30.5] | 29.0 [25.9, 32.0] | 29.1 [26.7, 31.5] | 30.4 [28.3, 32.5] | 30.2 [26.8, 33.7] |
| Northeast | 32.5 [29.3, 35.6] | 33.1 [28.4, 37.8] | 28.7 [23.1, 34.3] | 33.4 [28.3, 38.4] | 33.8 [29.8, 37.8] | 32.2 [23.7, 40.8] |
| Midwest | 38.7 [36.1, 41.4] | 39.2 [35.3, 43.2] | 35.2 [30.2, 40.3] | 40.5 [35.8, 45.2] | 40.1 [36.7, 43.4] | 39.0 [34.0, 44.0] |
| West | 38.9 [36.2, 41.5] | 35.6 [31.9, 39.2] | 37.8 [32.6, 42.9] | 38.2 [34.3, 42.1] | 39.4 [35.9, 42.9] | 38.8 [32.6, 45.0] |
| Food security status, % | ||||||
| Low | 29.0 [31.6, 34.6] | 28.4 [26.3, 30.4] | 28.4 [25.6, 31.2] | 29.1 [26.9, 31.2] | 30.8 [28.9, 32.6] | 29.0 [26.0, 32.1] |
| Very low | 40.8 [38.9, 42.7] | 41.8 [38.6, 45.0] | 36.1 [32.8, 39.5] | 41.1 [38.1, 44.1] | 40.6 [38.2, 43.0] | 40.3 [36.5, 44.1] |
| SNAP‡ participant, % | ||||||
| No | 25.4 [23.8, 27.0] | 24.4 [21.8, 26.9] | 23.8 [21.0, 26.6] | 26.1 [23.6, 28.5] | 26.0 [23.8, 28.1] | 24.9 [21.7, 28.2] |
| Yes | 42.2 [40.4, 44.0] | 39.0 [36.5, 41.5] | 40.8 [37.3, 44.3] | 40.4 [37.8, 43.0] | 42.1 [39.9, 44.3] | 43.1 [39.2, 46.9] |
AI/AN, Asian, NHPI, American Indian/Alaskan Native, Asian, Native Hawaiian and other Pacific Islander
SNAP, Supplemental Nutrition Assistance Program
Predicted probabilities were calculated from multivariable logistic regression models predicting use of the emergency food system as a function of age, marital status, race, Hispanic ethnicity, employment status, participation in governmental food assistance programs, food security status, household income, household size, geographic region, and year. All models were weighted to account for the survey design and non-response.
Use of the EFS was not substantially different between households with different levels of educational attainment and income among food insecure, low-income households (Supplemental Table 2). Households where the household respondent was unemployed or not in the labor force had higher use of the EFS when compared to being employed in the overall sample and in most subpopulations after adjusting for demographic characteristics. Some differences in emergency food use by region were found overall and within some subpopulations. To summarize, use was higher among households with similar demographics in the overall sample in the Midwest (38.7%) and West (38.9%) versus the Northeast (32.5%) or South (29.8%) and this was reflected in the subpopulation results. Use of the emergency food system was consistently higher among households experiencing very low food security versus low food security.
Use of the emergency food system was not higher among FRL and WIC participants overall, but use was higher for FRL participants compared to demographically similar non-participants in households with children (35.8% versus 29.4%; Supplemental Table 2). Overall (42.2% versus 25.4%) and in all subpopulations, use of the emergency food system was higher among households that participate in SNAP compared to non-participants after adjusting for demographic characteristics.
Discussion
In the CPS, emergency food use was relatively stable between 2015 and 2019 but increased substantially in 2020. Certain demographic characteristics such as age, racial identity, Hispanic ethnicity, employment status, and geographic region were associated with receipt of emergency food. These results should be used to inform outreach efforts and investigations into systemic factors that could be acting as barriers for some populations. While there are concerns related to the need for households to chronically utilize these services and how best to address unmet food needs in the United States,(29, 30) it is also imperative to ensure that the emergency food system has the capacity and resources to meet the food requirements of in-need households now and moving forward.
Previous research showed increasing trends in use of the emergency food system for food insecure households starting from the Great Recession starting in 2007, peaking in 2015, remaining relatively between 2015 and 2019, and increasing in 2020.(33–35) This is consistent with what was observed in our adjusted analyses where there were no increases between 2015–2019 and then a substantial increase in 2020. The large increase in 2020 may indicate success in increasing the availability and accessibility of the emergency food system along with meeting increasing demand in response to the COVID-19 pandemic.(48, 49) Emergency food providers responded to the pandemic in several ways to increase accessibility and keep up with rising demand, such as having drive-up or curbside collection, expanding home delivery, and having mobile, pop-up distribution events.(48, 49) These changes should be evaluated and, if feasible and effective in improving access to healthy foods, funded and sustained in order to increase accessibility of the emergency food system in the future.
Despite the increase in emergency food use in 2020, the majority of low-income, food insecure households did not use these resources in any year, which may be an indication that previously identified barriers, such as stigma and lack of accessibility,(36–39) are likely still present. Future studies using qualitative methods could explore the emergence of new barriers and facilitators to accessing emergency food resources and the persistence of established barriers and facilitators within the context of COVID-19 and the emergency food system’s response. Furthermore, because use of the emergency food system is a function of both need and accessibility, research should examine how changes in the delivery of emergency food persists following the pandemic and the extent to which observed increases in use are sustained.
Increased use of emergency food assistance by food insecure households in 2020 were not seen in all subpopulations, with non-significant results for households led by an older adult and non-metropolitan households. This could be due to fears around exposure to the COVID-19 virus as well as existing barriers to receiving emergency food, such as transportation and geographic access,(37) more strongly impacting these households. Additionally, it could be due to a lack of awareness of available resources in these populations, unwillingness to utilize a stigmatized resource, or other factors discouraging use of the EFS. Further outreach should be done with older adults and in non-metropolitan communities to ensure they are aware of the resources available to them and to encourage use of these resources. Strategies that address these populations resources, capacity, and needs, such as home-delivery services and mobile food pantries, should continue to be implemented and evaluated.
When examining the demographic characteristics that were associated with receipt of emergency food, there were demographic differences and non-differences presented here with a variety of implications. Before discussing differences in EFS use by racial identity and Hispanic ethnicity among food insecure households, it should be noted that in households where the household respondent identifies as Black, non-Hispanic or Hispanic, food insecurity rates in the general population are substantially higher than in White households.9 While we only included food-insecure households in this analysis, this disparity is concerning, and this context should be kept in mind when considering these results and their implications on program and policy choices. In our analysis, there did not appear to be differences in emergency food system use between Black and White led households across subpopulations, except in older adult led households where use was higher among Black compared to White led households. In households led by an individual identifying as multiracial, the use was much higher. Concerningly, households led by an individual who identified as Hispanic were less likely to use the emergency food system in comparison to non-Hispanic led households. Both organizational (e.g., not having Spanish language resources available; lacking culturally appropriate food) and structural (e.g., fears related to use of public services, law enforcement, and immigration status) barriers to using the emergency food system by Hispanic population have been identified in previous research,(38) and may have been especially salient in the time period analyzed. Finally, use was lower in households in the South and Northeast compared to the Midwest and West. In practice, efforts should be made by policymakers and emergency food providers to ensure the emergency food system is accessible in the Northeastern and Southern United States and to reduce the disparity in use between Hispanic and non-Hispanic households.
Use of the emergency food system was consistently higher among SNAP participants. Furthermore, use of EFS was higher among FRL participants in households with children. These findings may be due to outreach efforts and interventions which aim to connect households with government programs and the emergency food system. These results may also reflect that the users of one form of assistance may be more likely to use another resource for a variety of reasons that we are not able to explore with this data. Interpreting these results is further complicated by the fact that not all households are eligible for government food assistance programs. Additional research is needed to understand the reasons for lower use of emergency food resources in food insecure households who do not participate in government food assistance. Special, targeted efforts are needed to ensure food insecure households not participating in government programs have access to and use emergency food assistance.
There are some limitations that should be considered when interpreting these results. We defined use of the emergency food system as receiving food from a food pantry, food bank, church, or meal site in the previous year, which does not necessarily capture every part of the emergency food system, for example, emergency food received in a non-traditional setting such as a hospital or school. Despite this, food pantries, food banks, churches, and meal sites are the predominant emergency food providers in the United States. This analysis excludes households with unmet food needs that do not meet USDA’s criteria of food insecurity, specifically those experiencing marginal food security. Further analysis with this population is warranted. Additionally, food insecurity is a multi-dimensional construct, and the USDA 18-item food security module does not capture all dimensions of food insecurity.50 Therefore households may be excluded from this analysis because they have limited accessibility due to factors not examined in the USDA module, such as geographic access to retailers that offer affordable, healthy foods. Incorporating measures of food insecurity (e.g., adding geographic measures of food availability alongside the USDA module) in research that better capture its multidimensional nature would provide valuable information in assessing use of governmental and emergency food assistance programs and services. Finally, while we examined non-metropolitan households as one of our subpopulations of interest, there are limitations of metropolitan status regarding understanding how the level of urbanity and rurality influences use of the emergency food system. There are differences between non-metropolitan communities relevant to use of the emergency food system which are not able to be assessed in this analysis, e.g., those residing in remote rural locations with no metropolitan area within reasonable driving distance may have different access to and use of emergency food assistance compared to those residing in small towns within driving distance to a metropolitan area. Further research using a more detailed measure of the urban-rural continuum is needed to examine the impact of urbanity and rurality on emergency food system use.
Conclusion
These results demonstrate the extent to which use of the emergency food system increased in food insecure households in 2020 and highlight demographic characteristics associated with use between 2015 and 2020. Increased use in 2020 may have been, at least partially, due to increased accessibility coming from organizational and policy responses to the COVID-19 pandemic. Importantly, increases in use of the emergency food system in 2020 among the subpopulations examined were similar with the exception of households led by older adults and non-metropolitan households where use remained consistent with previous years. Policymakers and emergency food providers need to ensure that the emergency food system has the resources and capacity to continue to meet needs of low-income food insecure households as well as expand its reach.
Supplementary Material
Acknowledgements:
PJB is supported by Award Number T32DK083250 from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). KMB is supported by Award Number F31HD107980 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). SV is supported by Award Number T32GM008244 from the National Institute of General Medical Sciences (NIGMS). Additionally, the authors gratefully acknowledge support from the Minnesota Population Center (P2C HD041023) and the use of the Integrated Public Use Microdata Series Current Population Survey (R01HD067258) both funded through grants from NICHD. The content is solely the responsibility of the authors and does not necessarily represent the official view of the NIDDK, NICHD, NIGMS, or National Institutes of Health.
Abbreviations:
- CPS
Current Population Survey
- EFS
Emergency Food System
- FPL
Federal Poverty Level
- FRL
Free or Reduced Lunch
- IPUMS
Integrated Public Use Microdata Series
- WIC
Special Supplemental Nutrition Program for Women, Infants, and Children
- SNAP
Supplemental Nutrition Assistance Program
- USDA
United States Department of Agriculture
Footnotes
Disclosure: The authors declare no conflicts of interest.
References
- 1.National Research Council. (2006). Food insecurity and hunger in the United States: an assessment of the measure. National Academies Press. [Google Scholar]
- 2.Gundersen C, & Ziliak JP (2015). Food insecurity and health outcomes. Health affairs, 34(11), 1830–1839. [DOI] [PubMed] [Google Scholar]
- 3.Johnson AD, & Markowitz AJ (2018). Food insecurity and family well-being outcomes among households with young children. The Journal of Pediatrics, 196, 275–282. [DOI] [PubMed] [Google Scholar]
- 4.Lombe M, Nebbitt VE, Sinha A, & Reynolds A (2016). Examining effects of food insecurity and food choices on health outcomes in households in poverty. Social work in health care, 55(6), 440–460. [DOI] [PubMed] [Google Scholar]
- 5.Berkowitz SA, Seligman HK, Meigs JB, & Basu S (2018). Food insecurity, healthcare utilization, and high cost: a longitudinal cohort study. The American journal of managed care, 24(9), 399. [PMC free article] [PubMed] [Google Scholar]
- 6.Garcia SP, Haddix A, & Barnett K (2018). Incremental Health Care Costs Associated with Food Insecurity and Chronic Conditions Among Older Adults. Preventing chronic disease, 15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Berkowitz SA, Basu S, Gundersen C, & Seligman HK (2019). State-Level and County-Level Estimates of Health Care Costs Associated with Food Insecurity. Preventing chronic disease, 16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Walker RE, Keane CR, & Burke JG (2010). Disparities and access to healthy food in the United States: A review of food deserts literature. Health & place, 16(5), 876–884. [DOI] [PubMed] [Google Scholar]
- 9.Odoms-Young AM (2018). Examining the impact of structural racism on food insecurity: implications for addressing racial/ethnic disparities. Family & community health, 41(Suppl 2 food insecurity and obesity), S3–S6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Vaccaro JA, & Huffman FG (2017). Sex and race/ethnic disparities in food security and chronic diseases in US older adults. Gerontology and geriatric medicine, 3, 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Byrd AS, Toth AT, & Stanford FC (2018). Racial disparities in obesity treatment. Current obesity reports, 7(2), 130–138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hernandez DC, Reesor LM, & Murillo R (2017). Food insecurity and adult overweight/obesity: gender and race/ethnic disparities. Appetite, 117, 373–378. [DOI] [PubMed] [Google Scholar]
- 13.Gundersen C, Kreider B, & Pepper JV (2017). Partial identification methods for evaluating food assistance programs: a case study of the causal impact of SNAP on food insecurity. American Journal of Agricultural Economics, 99(4), 875–893. [Google Scholar]
- 14.Nord M, & Golla AM (2009). Does SNAP decrease food insecurity? Untangling the self-selection effect. United States Department of Agriculture Economic Research Service: Washington, DC [Google Scholar]
- 15.Vigil A (2019). Trends in Supplemental Nutrition Assistance Program Participation Rates: Fiscal Year 2010 to Fiscal Year 2017. United States Department of Agriculture Food and Nutrition Service Office of Policy Support: Washington, DC. [Google Scholar]
- 16.Chiappone A, Parks CA, Calloway E, Fricke HE, Stern K, & Yaroch AL (2019). Perceptions and experiences with SNAP and potential policies: viewpoint from SNAP participants. Journal of Hunger & Environmental Nutrition, 14(1–2), 98–109. [Google Scholar]
- 17.Leung CW, Hoffnagle EE, Lindsay AC, Lofink HE, Hoffman VA, Turrell S, … & Blumenthal SJ (2013). A qualitative study of diverse experts’ views about barriers and strategies to improve the diets and health of Supplemental Nutrition Assistance Program (SNAP) beneficiaries. Journal of the Academy of Nutrition and Dietetics, 113(1), 70–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Waxman E, Gundersen C, & Thompson M (2018). How Far Do SNAP Benefits Fall Short of Covering the Cost of a Meal? Urban Institute: Washington DC. Retrieved from https://www.urban.org/research/publication/how-far-do-snap-benefits-fall-short-covering-cost-meal [Google Scholar]
- 19.Kaye L, Lee E, & Chen YY (2013). Barriers to Food Stamps in New York State: A perspective from the field. Journal of Poverty, 17(1), 13–28. [Google Scholar]
- 20.Gray C (2018, May 21). Why Leave Benefits on the Table? Evidence from SNAP. Upjohn Institute. Retrieved from 10.2139/ssrn.3203395 [DOI] [Google Scholar]
- 21.Fletcher JM, & Frisvold DE (2017). The relationship between the school breakfast program and food insecurity. Journal of Consumer Affairs, 51(3), 481–500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Holley CE, & Mason C (2019). A systematic review of the evaluation of interventions to tackle children’s food insecurity. Current nutrition reports, 8(1), 11–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kowlessar N, Robinson K, & Schur C (2015). Older Americans Benefit from Older Americans Act Nutrition Programs. Retrieved from https://acl.gov/programs/health-wellness/nutrition-services
- 24.Askelson NM, Golembiewski EH, Bobst A, Delger PJ, & Scheidel CA (2017). Understanding perceptions of school administrators related to school breakfast in a low school breakfast participation state. Journal of School Health, 87(6), 427–434. [DOI] [PubMed] [Google Scholar]
- 25.Gualtieri MC, Donley AM, Wright JD, & Vega SS (2018). Home delivered meals to older adults: a critical review of the literature. Home healthcare now, 36(3), 159–168. [DOI] [PubMed] [Google Scholar]
- 26.Lee JS, Sinnett S, Bengle R, Johnson MA, & Brown A (2011). Unmet needs for the Older Americans Act nutrition program. Journal of Applied Gerontology, 30(5), 587–606. [Google Scholar]
- 27.Lloyd JL, & Wellman NS (2015). Older Americans Act Nutrition Programs: A community-based nutrition program helping older adults remain at home. Journal of nutrition in gerontology and geriatrics, 34(2), 90–109. [DOI] [PubMed] [Google Scholar]
- 28.Bailey-Davis L, Virus A, McCoy TA, Wojtanowski A, Vander Veur SS, & Foster GD (2013). Middle school student and parent perceptions of government-sponsored free school breakfast and consumption: A qualitative inquiry in an urban setting. Journal of the Academy of Nutrition and Dietetics, 113(2), 251–257. [DOI] [PubMed] [Google Scholar]
- 29.Bazerghi C, McKay FH, & Dunn M (2016). The role of food banks in addressing food insecurity: a systematic review. Journal of Community Health, 41(4), 732–740. [DOI] [PubMed] [Google Scholar]
- 30.Poppendieck J (2014). Food assistance, hunger and the end of welfare in the USA. In First world hunger revisited (pp. 176–190). Palgrave Macmillan, London. [Google Scholar]
- 31.Feeding America. (2021). Together we are Feeding America: Annual Report 2020. Feeding America, Washington D.C. Retrieved from https://www.feedingamerica.org/about-us/financials [Google Scholar]
- 32.Cronquist Kathryn. (2021). Characteristics of Supplemental Nutrition Assistance Program Households: Fiscal Year 2019. U.S. Department of Agriculture, Food and Nutrition Service, Office of Policy Support, Alexandria, VA. Retrieved from https://www.fns.usda.gov/snap/characteristics-snap-households-fy-2019 [Google Scholar]
- 33.Coleman-Jensen A (2018). Food pantries provide emergency food to more than one-quarter of food-insecure households. Amber Waves: The Economics of Food, Farming, Natural Resources, and Rural America, (10). [Google Scholar]
- 34.Coleman-Jensen A, Rabbitt MP, Gregory CA, & Singh A (2020). Statistical Supplement to Household Food Security in the United States in 2019 (No. APN-084)
- 35.Coleman-Jensen A, Rabbitt MP, Gregory CA, & Singh A (2021). Statistical Supplement to Household Food Security in the United States in 2020 (No. 1962-2021-2625).
- 36.Bradley SE, & Vitous CA (2019). Using GIS to Explore Disparities between the Location of Food Deserts and Vulnerability to Food Insecurity. Journal of Hunger & Environmental Nutrition, 16(3), 406–422. [Google Scholar]
- 37.Fong K, Wright RA, & Wimer C (2016). The cost of free assistance: Why low-income individuals do not access food pantries. J. Soc. & Soc. Welfare, 43, 71. [Google Scholar]
- 38.Wright KE, Lucero J, & Crosbie E (2020). “It’s nice to have a little bit of home, even if it’s just on your plate”–perceived barriers for Latinos accessing food pantries. Journal of Hunger & Environmental Nutrition, 15(4), 496–513. [Google Scholar]
- 39.Kindle PA, Foust-Newton M, Reis M, & Gell M (2019). Food Pantries and Stigma: Users’ Concerns and Public Support. Contemporary Rural Social Work Journal, 11(1), 2. [Google Scholar]
- 40.Liu Y, Desmond NE, Wright BN, Bailey RL, Dong T, Craig BA, & Eicher-Miller HA (2021). Nutritional contributions of food pantries and other sources to the diets of rural, Midwestern food pantry users in the USA. British Journal of Nutrition, 125(8), 891–901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Simmet A, Depa J, Tinnemann P, & Stroebele-Benschop N (2017). The nutritional quality of food provided from food pantries: a systematic review of existing literature. Journal of the Academy of Nutrition and Dietetics, 117(4), 577–588 [DOI] [PubMed] [Google Scholar]
- 42.United States Census Bureau. (2019, October). Current Population Survey Design and Methodology Technical Paper 77. Retrieved from https://www.census.gov/programs-surveys/cps/technical-documentation/complete.html
- 43.Nord M, & Hopwood H (2007). Does interview mode matter for food security measurement? Telephone versus in-person interviews in the Current Population Survey Food Security Supplement. Public Health Nutrition, 10(12), 1474–1480. [DOI] [PubMed] [Google Scholar]
- 44.Flood S, King M, Rodgers R, Ruggles S, Warren JR, & Westberr M (2021). Integrated Public Use Microdata Series, Current Population Survey: Version 9.0 [dataset]. Minneapolis, MN: IPUMS. 10.18128/D030.V9.0 [DOI] [Google Scholar]
- 45.Jones CP (2000). Levels of racism: a theoretic framework and a gardener’s tale. American journal of public health, 90(8), 1212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Boyd RW, Lindo EG, Weeks LD, & McLemore MR (2020). On racism: a new standard for publishing on racial health inequities. Health Affairs Blog, 10(10.1377).
- 47.StataCorp. 2021. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC. [Google Scholar]
- 48.Lanier J, & Schumacher J (2021). The Action of Foodbanks and Food Pantries in Central Illinois During the COVID-19 Pandemic. Journal of Hunger & Environmental Nutrition, 1–9. [Google Scholar]
- 49.Hege A, McCormick N, Robinson P, Charles K, Jones J, & Aft E (2021). Perspectives from the front line. Journal of Agriculture, Food Systems, and Community Development, 10(2), 1–5. [Google Scholar]
- 50.Barrett CB (2010). Measuring food insecurity. Science, 327(5967), 825–828. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.