

Abstract
Background
Widespread application of pulmonary rehabilitation (also known as respiratory rehabilitation) in chronic obstructive pulmonary disease (COPD) should be preceded by demonstrable improvements in function (health‐related quality of life, functional and maximal exercise capacity) attributable to the programmes. This review updates the review reported in 2006.
Objectives
To compare the effects of pulmonary rehabilitation versus usual care on health‐related quality of life and functional and maximal exercise capacity in persons with COPD.
Search methods
We identified additional randomised controlled trials (RCTs) from the Cochrane Airways Group Specialised Register. Searches were current as of March 2014.
Selection criteria
We selected RCTs of pulmonary rehabilitation in patients with COPD in which health‐related quality of life (HRQoL) and/or functional (FEC) or maximal (MEC) exercise capacity were measured. We defined 'pulmonary rehabilitation' as exercise training for at least four weeks with or without education and/or psychological support. We defined 'usual care' as conventional care in which the control group was not given education or any form of additional intervention. We considered participants in the following situations to be in receipt of usual care: only verbal advice was given without additional education; and medication was altered or optimised to what was considered best practice at the start of the trial for all participants.
Data collection and analysis
We calculated mean differences (MDs) using a random‐effects model. We requested missing data from the authors of the primary study. We used standard methods as recommended by The Cochrane Collaboration.
Main results
Along with the 31 RCTs included in the previous version (2006), we included 34 additional RCTs in this update, resulting in a total of 65 RCTs involving 3822 participants for inclusion in the meta‐analysis.
We noted no significant demographic differences at baseline between members of the intervention group and those who received usual care. For the pulmonary rehabilitation group, the mean forced expiratory volume at one second (FEV1) was 39.2% predicted, and for the usual care group 36.4%; mean age was 62.4 years and 62.5 years, respectively. The gender mix in both groups was around two males for each female. A total of 41 of the pulmonary rehabilitation programmes were hospital based (inpatient or outpatient), 23 were community based (at community centres or in individual homes) and one study had both a hospital component and a community component. Most programmes were of 12 weeks' or eight weeks' duration with an overall range of four weeks to 52 weeks.
The nature of the intervention made it impossible for investigators to blind participants or those delivering the programme. In addition, it was unclear from most early studies whether allocation concealment was undertaken; along with the high attrition rates reported by several studies, this impacted the overall risk of bias.
We found statistically significant improvement for all included outcomes. In four important domains of quality of life (QoL) (Chronic Respiratory Questionnaire (CRQ) scores for dyspnoea, fatigue, emotional function and mastery), the effect was larger than the minimal clinically important difference (MCID) of 0.5 units (dyspnoea: MD 0.79, 95% confidence interval (CI) 0.56 to 1.03; N = 1283; studies = 19; moderate‐quality evidence; fatigue: MD 0.68, 95% CI 0.45 to 0.92; N = 1291; studies = 19; low‐quality evidence; emotional function: MD 0.56, 95% CI 0.34 to 0.78; N = 1291; studies = 19; mastery: MD 0.71, 95% CI 0.47 to 0.95; N = 1212; studies = 19; low‐quality evidence). Statistically significant improvements were noted in all domains of the St. George's Respiratory Questionnaire (SGRQ), and improvement in total score was better than 4 units (MD ‐6.89, 95% CI ‐9.26 to ‐4.52; N = 1146; studies = 19; low‐quality evidence). Sensitivity analysis using the trials at lower risk of bias yielded a similar estimate of the treatment effect (MD ‐5.15, 95% CI ‐7.95 to ‐2.36; N = 572; studies = 7).
Both functional exercise and maximal exercise showed statistically significant improvement. Researchers reported an increase in maximal exercise capacity (mean Wmax (W)) in participants allocated to pulmonary rehabilitation compared with usual care (MD 6.77, 95% CI 1.89 to 11.65; N = 779; studies = 16). The common effect size exceeded the MCID (4 watts) proposed by Puhan 2011(b). In relation to functional exercise capacity, the six‐minute walk distance mean treatment effect was greater than the threshold of clinical significance (MD 43.93, 95% CI 32.64 to 55.21; participants = 1879; studies = 38).
The subgroup analysis, which compared hospital‐based programmes versus community‐based programmes, provided evidence of a significant difference in treatment effect between subgroups for all domains of the CRQ, with higher mean values, on average, in the hospital‐based pulmonary rehabilitation group than in the community‐based group. The SGRQ did not reveal this difference. Subgroup analysis performed to look at the complexity of the pulmonary rehabilitation programme provided no evidence of a significant difference in treatment effect between subgroups that received exercise only and those that received exercise combined with more complex interventions. However, both subgroup analyses could be confounded and should be interpreted with caution.
Authors' conclusions
Pulmonary rehabilitation relieves dyspnoea and fatigue, improves emotional function and enhances the sense of control that individuals have over their condition. These improvements are moderately large and clinically significant. Rehabilitation serves as an important component of the management of COPD and is beneficial in improving health‐related quality of life and exercise capacity. It is our opinion that additional RCTs comparing pulmonary rehabilitation and conventional care in COPD are not warranted. Future research studies should focus on identifying which components of pulmonary rehabilitation are essential, its ideal length and location, the degree of supervision and intensity of training required and how long treatment effects persist. This endeavour is important in the light of the new subgroup analysis, which showed a difference in treatment effect on the CRQ between hospital‐based and community‐based programmes but no difference between exercise only and more complex pulmonary rehabilitation programmes.
Plain language summary
Pulmonary rehabilitation for chronic obstructive pulmonary disease
Chronic obstructive pulmonary disease (COPD) describes a chronic lung condition that prevents the air supply from getting to the lungs. Symptoms include breathlessness, coughing, tiredness and frequent chest infection. Worldwide, COPD is a major cause of ill health.
Pulmonary rehabilitation programmes include exercise as a key component; some programmes contain other interventions such as assessment, education, psychological support and dietary advice. Pulmonary rehabilitation is one of the key recommended approaches in the treatment of COPD. This review compared the impact of pulmonary rehabilitation versus usual care on the health‐related quality of life of people with COPD. We included 65 studies involving 3822 participants. Participants were randomly assigned to receive pulmonary rehabilitation or usual care. The quality of the studies was generally good.
This review highlights that pulmonary rehabilitation improves the health‐related quality of life of people with COPD. Results strongly support inclusion of pulmonary rehabilitation as part of the management and treatment of patients with COPD.
Future studies should concentrate on identifying the most important components of pulmonary rehabilitation, the ideal length of a programme, the intensity of training required and how long the benefits of the programme last.
Summary of findings
Summary of findings for the main comparison. Rehabilitation versus usual care for chronic obstructive pulmonary disease.
| Rehabilitation versus usual care for chronic obstructive pulmonary disease | |||||
| Patient or population: patients with chronic obstructive pulmonary disease Settings: hospital and community Intervention: rehabilitation versus usual care | |||||
| Outcomes | Illustrative comparative effects* (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Response on control | Treatment effect | ||||
| Usual care | Rehabilitation versus usual care | ||||
|
QoL ‐ Change in CRQ (dyspnoea)
CRQ Questionnaire. Scale from 1 to 7 (Higher is better and 0.5 unit is an important difference) Follow‐up: median 12 weeks |
Median change = 0 units | Mean QoL ‐ change in CRQ (Dyspnoea) in the intervention groups was 0.79 units higher (0.56 to 1.03 higher) | 1283 (19 studies) | ⊕⊕⊕⊝ Moderate1,2,3 | Sensitivity analysis from studies at lower risk of bias was similar (MD 0.99, 95% CI 0.64 to 1.34; participants = 384; studies = 5; I2 = 34%) |
|
QoL ‐ Change in SGRQ (total)
Scale from 0 to 100 (Lower is better and 4 units is an important difference) Follow‐up: median 12 weeks |
Median change = 0.42 units | Mean QOL ‐ change in SGRQ (total) in the intervention groups was 6.89 units lower (9.26 to 4.52 lower) | 1146 (19 studies) | ⊕⊕⊕⊝ Moderate2,3,4 | Sensitivity analysis from studies at lower risk of bias was similar (MD ‐5.15, 95% CI ‐7.95 to ‐2.36; participants = 572; studies = 7; I2 = 51%) |
| Change in maximal exercise (Incremental Shuttle walk test (ISWT)) Distance metres Follow‐up: median 12 weeks | Median change = 1 metre | Mean maximal exercise (incremental shuttle walk test) in the intervention groups was 39.77 metres higher (22.38 to 57.15 higher) | 694 (8 studies) | ⊕⊕⊕⊝ Moderate2,3,5 | |
| Change in functional exercise capacity (6MWT)) Distance metres Follow‐up: median 12 weeks | Median change = 3.4 metres | Mean functional exercise capacity (6MWT)) in the intervention groups was 43.93 metres higher (32.64 to 55.21 higher) | 1879 (38 studies) | ⊕⊝⊝⊝ Very low2,3,6,7 | |
| Change in maximal exercise capacity (cycle ergometer) Workmax (watt) Follow‐up: median 12 weeks | Median change = ‐0.05 watts | Mean maximal exercise capacity (cycle ergometer) in the intervention groups was 6.77 watts higher (1.89 to 11.65 higher) | 779 (16 studies) | ⊕⊕⊝⊝ Low2,3,8,9 | |
| *The basis for the response on control is the median control group response across studies. CI: confidence interval; MD: mean difference. | |||||
| GRADE Working Group grades of evidence. High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | |||||
117 studies reported random sequence generation (1 unclear), 12 reported allocation concealment 2 did not have allocation concealment and it is unclear in 5 studies. 4 studies did not blind assessors, 11 blinded assessors and 4 were unclear as to assessor blinding. 6 studies had attrition bias greater than 20%. 2Downgraded as there is a high level of heterogeneity within the results. Several factors may impact heterogeneity, including content of the intervention programme, setting of the programme and severity of COPD. 3Greater than optimal Information size (OIS). 95% confidence interval does not includes "no effect," nor does the confidence limit cross the MID, so no need to downgrade. 418 studies reported random sequence generation (2 unclear), 10 reported allocation concealment, 2 did not have allocation concealment and it is unclear in 7 studies. 3 studies did not blind assessors, 9 blinded assessors and 7 were unclear as to assessor blinding. 7 studies had attrition bias greater than 20%. 5All 8 studies reported random sequence generation, 5 reported allocation concealment and it is unclear in 3 studies. 5 studies had blind assessors with 1 not blinded, and 2 were unclear as to assessor blinding. 4 studies had attrition bias greater than 20%. 634 studies reported random sequence generation, 4 were unclear, 20 reported allocation concealment, 3 did not have allocation concealment and it is unclear in 15 studies. 5 studies did not blind assessors, 19 blinded assessors and 13 were unclear as to assessor blinding. 13 studies had attrition bias greater than 20% and 2 were unclear. 7Downgraded as bias indicated for 6‐minute walk test: Egger: bias = 1.24304 (95% CI = 0.183967 to 2.302131; P value 0.0227). Begg‐Mazumdar: Kendall's tau = 0.16074 (P value 0.1601). 8All 16 studies reported random sequence generation, 6 reported allocation concealment, 3 did not have allocation concealment and it is unclear in 7 studies. 2 studies did not blind assessors, 10 blinded assessors and 4 were unclear as to assessor blinding. 4 studies had attrition bias greater than 20%. 9Downgraded as bias indicated for cycle ergometer test: Egger: bias = 1.57164 (95% CI = 0.6053 to 2.337984; P value 0.0036). Begg‐Mazumdar: Kendall's tau = ‐0.2666667 (P value 0.139).
Background
Description of the condition
Chronic obstructive pulmonary disease (COPD) is a multi‐factorial progressive chronic lung disease that causes obstruction in airflow. This obstruction results in persistent and progressive breathlessness, productive coughing, fatigue and recurrent chest infection (GOLD 2014). COPD is also associated with extrapulmonary effects such as muscle wasting, osteopaenia (reduction in protein and mineral content of bone tissue), cardiovascular disease and depression and therefore is now best understood as a systemic disease (Agusti 2003; Agusti 2005). Worldwide, COPD is a major cause of morbidity. It is estimated that 210 million people are living with COPD (Franchi 2009), and it is projected that by the year 2030, COPD will be the third most frequent cause of death globally (WHO 2008). At this time, COPD is an incurable condition that is associated with significant economic costs due to progressive disease severity and frequent hospital admissions and readmissions (GOLD 2014; Guarascio 2013).
Risk factors for COPD are numerous and include genetics, recurrent respiratory infection, low socioeconomic status, exposure to air pollutants, poor nutrition and asthma (Eisner 2010; GOLD 2014). However smoking is recognised as a major cause of COPD, and the more a person smokes, the more likely he or she is to develop this condition (Forey 2011).
COPD is a heterogeneous condition with marked variation in progression between individuals (Casanova 2011; Nishimura 2013). The initial underlying pathology of COPD is confined to the lungs, and a clinical diagnosis is based on presenting symptoms and confirmation of airflow obstruction with a postbronchodilator spirometry forced expiratory volume in one second/forced vital capacity ratio (FEV1/FVC) < 0.70 (GOLD 2014). The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines are usually used to grade the severity of airflow limitations as mild (FEV1 ≥ 80% predicted: GOLD 1), moderate (50% ≤ FEV1 < 80% predicted: GOLD 2), severe (30% ≤ FEV1 50% predicted: GOLD 3) or very severe (FEV1 < 30% predicted: GOLD 4) (GOLD 2014).
The symptoms of COPD make engagement in physical activity unpleasant as the result of air trapping and increased hyperinflation in the lungs, which result in increased breathlessness due to subsequent inefficient breathing (O' Donnell 2007). Increased breathlessness provokes anxiety, which inevitably leads to further breathlessness, exacerbation of COPD symptoms and panic. This causes a vicious circle whereby any activities that involve physical exertion are avoided, causing muscle de‐conditioning, which further reduces capacity to engage in physical activity (Bourbeau 2007). Physical inactivity is therefore a key predictor of mortality in people with COPD (Garcia‐Aymerich 2006; Spruit 2013; Waschki 2011). Consequently, the joint American Thoracic Society and European Respiratory Society (ATS/ERS) (Spruit 2013) guidelines highlight the importance of exercise in the treatment and management of COPD.
Description of the intervention
Treatment interventions for COPD include smoking cessation, pharmacological and non‐pharmacological therapies and, in specific circumstances, supplemental oxygen, ventilatory support, surgical treatment and palliative care (GOLD 2014). However, best evidence and all current international guidelines ratify the central role of pulmonary rehabilitation in the treatment of people with COPD (GOLD 2014; NICE 2010; Nici 2006; Ries 2007; Spruit 2013).
Pulmonary rehabilitation (PR), which was first defined by the American College of Chest Physicians Committee in 1974, is a proactive approach to minimising COPD symptoms, improving health‐related quality of life (HRQoL) and increasing physical and emotional involvement in everyday life (GOLD 2014; Nici 2006; Ries 2007). The ATS in conjunction with the ERS has published numerous comprehensive statements on PR, with the most recent update in 2013. In the latest update, pulmonary rehabilitation was defined newly as a "…comprehensive intervention based on a thorough patient assessment followed by patient tailored therapies that include, but are not limited to, exercise training, education, and behaviour change, designed to improve the physical and psychological condition of people with chronic respiratory disease and to promote the long‐term adherence to health‐enhancing behaviours" (Spruit 2013). This new definition differs from the previous one (2006) in that it focuses on the interdisciplinary and therefore more holistic approach to PR rather than on the previous multi‐disciplinary approach; highlights the importance of behaviour change; and places PR firmly within the concept of integrated care (Spruit 2013).
Depending on culture, healthcare systems and resources, the structure, personnel, content and settings of PR programmes may vary (Nici 2006;Spruit 2013). However, individually tailored exercise training is considered the cornerstone of PR (Nici 2006;Ries 2007;Spruit 2013). In particular, strength, low‐ and high‐intensity training, exercise endurance and upper and lower extremity training are recommended (Nici 2006;Ries 2007, Spruit 2013). In addition to exercise, the typical comprehensive PR programme includes patient assessment, education, psychosocial support and nutritional counselling (ATS 1999; GOLD 2014; Spruit 2013). Pulmonary rehabilitation is typically delivered to groups of patients (rather than to individuals), but no evidence suggests the optimal size of the exercise group. However, the American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR 2011) recommends a staff‐to‐participant ratio of 1:4, and the British Thoracic Society (British Thoracic Society 2001) a ratio of 1:8. The setting for PR programmes varies; both community‐based (Cambach 1997; Casey 2013; Wijkstra 1994a) and home‐based programmes (Maltais 2008; Viera 2010) are available. However, traditionally, most PR programmes have been hospital based (Bourbeau 2010), with participants attending as in‐patients or on an out‐patient basis.
The optimal duration of programmes, number of sessions offered per week and type of staff required to deliver PR programmes are unclear. Beauchamp 2011 concludes, following a systematic review, that available evidence is insufficient to show the optimal duration of PR programmes for people with COPD. However, a programme duration of at least eight weeks is recommended to attain a substantial effect (Beauchamp 2011). Likewise the number of times per week that programmes are offered differs; typically hospital‐based out‐patient programmes are offered two or three days per week, and in‐patient programmes are offered over five days (Spruit 2013). The optimal number of sessions required remains unclear. However, the 2006 ATS/ERS guidelines specify three sessions per week or a twice‐weekly supervised and one unsupervised home session (Nici 2006). Finally, key requirements for staff delivering the programme are that they are clinically competent, having the required skills and knowledge and maintain patient safety (Spruit 2013).
How the intervention might work
Pulmonary rehabilitation seeks to reduce COPD symptoms, reestablish and improve functional ability, enhance participation in everyday life, promote autonomy and improve HRQoL (Spruit 2013). It does this by focusing on the systemic aspects of the disease that are common among patients with COPD (AACVPR 2011). The exercise component of PR increases inspiratory volume and reduces dynamic hyperinflation, both of which reduce dyspnoea when the person is performing tasks (Casaburi 2009). Exercise also increases muscle function, delaying fatigue and resulting in increased exercise tolerance. Meanwhile, the educational component of PR focuses on collaborative self‐management and behaviour change (Spruit 2013). It encompasses providing information and knowledge regarding COPD; building skills such as goal setting, problem solving and decision making; and developing action plans that allow individuals to better recognise and manage the disease (Spruit 2013). The behaviour change element focuses on modifying nutritional intake and smoking patterns; adhering to medication and regular exercise; and utilising effective breathing techniques and energy‐saving strategies (Spruit 2013).
Why it is important to do this review
Review authors undertook the original version of this Cochrane review in 2001 in response to worldwide endorsement of PR as integral to the management of COPD and lack of clear evidence as to the impact of these programmes on HRQoL and exercise tolerance (Lacasse 2001). The review included 23 randomised controlled trials (RCTs), and review authors concluded that PR (exercise training for a minimum of four weeks with or without education and/or psychological support) resulted in statistically significant improvement in HRQoL and modest improvement in exercise capacity (Lacasse 2001). This review was updated in 2006, included 31 RCTs and again reported statistically significant improvement in HRQoL. However, results for both functional and maximal exercise capacity were below the threshold of clinical significance. Lacasse 2006 concluded that further RCTs comparing PR versus usual care for patients with COPD were not needed. Despite this, a large number of RCTs published since 2006 have endorsed the need for this current update. Furthermore, recent RCTs tend to use disease‐specific quality of life indices as primary outcome measures,, combined with more refined maximal and functional exercise capacity measurement tools (Curtis 2003;de Torres 2002;Gross 2004; Jones 2003). Consequently in the current review, we will take a more focused approach to assessment of primary and secondary outcomes. In recent years, wide variation has been noted in the follow‐up assessment times utilised within studies, and this may have an impact on study outcomes. Therefore in the current review, we will include only assessments completed up to and within three months of completion of the intervention. Also, risk of bias requirements for Cochrane reviews have been altered since the last update; review authors of this current update will ensure that these new requirements are met. Finally, as a separate systematic review examining the effects of PR following exacerbations of COPD has been undertaken (Puhan 2011(a)), we will exclude from this review studies that commenced within four weeks of an acute exacerbation of COPD.
Objectives
To compare the effects of pulmonary rehabilitation versus usual care on health‐related quality of life and functional and maximal exercise capacity in persons with COPD.
Methods
Criteria for considering studies for this review
Types of studies
All RCTs in which participants are randomly assigned at the individual or cluster level and in which researchers compare the effects of PR versus those of usual care.
Types of participants
We included RCTs in which more than 90% of participants had COPD defined as:
a clinical diagnosis of COPD; and
best recorded forced expiratory volume after one second (FEV1)/forced vital capacity (FVC) (FEV1/FVC) ratio of individual participants < 0.7.
We included RCTs in which:
any or all participants were on continuous oxygen.
We excluded RCTs that focused on participants:
who were mechanically ventilated; or
who had an acute exacerbation within four weeks before commencement of the intervention.
Types of interventions
Pulmonary rehabilitation
Any in‐patient, out‐patient, community‐based or home‐based rehabilitation programme of at least four weeks' duration that included exercise therapy with or without any form of education and/or psychological support delivered to patients with exercise limitation attributable to COPD.
We included any exercise therapy that included physical activity considered to be aerobically demanding.
We excluded:
interventions in which the physical activity component was considered to be not aerobically demanding (e.g. respiratory muscle training, breathing exercises, Tai Chi, yoga) (the degree of aerobic demand was assessed for each individual intervention by examining the detailed description of the intervention in identified studies); and
programmes of less than 4 weeks' duration.
Usual care
For the purpose of this review, usual care was defined as conventional care. We excluded trials in which the control group was given education or any form of additional intervention. Participants in the following situations were considered to be in receipt of usual care.
Only verbal advice was given. If the advice was accompanied by additional education provided in any way, for example, by video or by diary, then the study was excluded.
Medication was altered or optimised to what was considered best practice at the start of the trial for all participants.
Types of outcome measures
We considered disease‐specific HRQoL and/or maximal or functional exercise capacity (up to and including three months after the end of the intervention). We defined 'maximal exercise capacity' as the peak capacity measured by an incremental cycle ergometry test. 'Functional exercise capacity' was defined according to the results of timed walk tests (Holland 2014).
Primary outcomes
Disease‐specific health‐related quality of life (HRQoL)
Chronic Respiratory Disease Questionnaire (CRQ).
St. George's Respiratory Questionnaire (SGRQ).
Secondary outcomes
Exercise testing
The classification of exercise testing is divided into functional and maximal exercise groups, which include the following (Holland 2014).
Functional exercise capacity assessments.
Six‐minute walk test/distance (6MWT/6MWD).
Incremental shuttle walk test (ISWT).
Endurance shuttle walk test (ESWT).
Maximal exercise tests.
Incremental cycle ergometry.
Search methods for identification of studies
Electronic searches
We have detailed in Appendix 1 the search methods used in the previous version of this review. The previously published version included searches up to July 2004. The search period for this update is July 2004 to March 2014.
For the current update, we identified trials from the Cochrane Airways Group Specialised Register (CAGR), which is maintained by the Trials Search Co‐ordinator for the Group. The Register contains trial reports identified through systematic searches of bibliographic databases including the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, EMBASE, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), the Allied and Complementary Medicine Database (AMED) and PsycINFO, and by handsearching of respiratory journals and meeting abstracts (please see Appendix 2 for further details). We searched all records in the CAGR using the search strategy described in Appendix 3.
We also conducted a search of ClinicalTrials.gov (www.ClinicalTrials.gov) and the World Health Organization (WHO) trials portal (www.who.int/ictrp/en/). We searched all databases from their inception to the present, with no restriction on the language of publication. We completed the latest searches in March 2014.
Searching other resources
We reviewed the reference lists of relevant articles and retrieved any potential additional citations. We contacted the authors of studies included in the meta‐analysis and experts in the field of pulmonary rehabilitation to uncover unpublished material. We also included the papers suggested by the study authors contacted.
Data collection and analysis
The methods used in this review were designed in accordance with recommendations provided in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Selection of studies
Two review authors (BMC, DC) independently tested the inclusion criteria and sought clarification on all areas of concern with the wider review team, which included the original author of the review (YL). When the review authors were confident of the clarity of the criteria and their skills, they assessed studies with respect to the identified criteria. The two review authors then independently assessed all citation titles and abstracts. Review authors electronically collated initial decisions with the use of Distiller SR and later with Early Reviewing Software (EROS); they coded each citation as:
included to proceed;
more information needed before inclusion decision;
important article but not to be included in the review; or
excluded (Appendix 4; Appendix 5).
Review authors held a meeting after every 100 reviewed citations during which they resolved disagreements by consensus. They used quadratic weighted Kappa statistics to measure agreement between coders (Kramer 1981). When consensus could not be reached, a third review author (DD) adjudicated. Review authors then retrieved full‐text papers of all potentially eligible studies. Review authors maintained records on all studies that did not meet the inclusion criteria and provided the rationale for their exclusion.
Data extraction and management
The lead review author (BMC) extracted data from all original papers identified for inclusion in the meta‐analysis using a developed data extraction form. The other members of the review group (DC, KM, DD, EM) independently extracted data from an equal share of the same studies. Extracted information included the following.
Background characteristics of the research reports.
Characteristics of participants in the study.
The number and distribution of participants who dropped‐out or withdrew from the study.
A full description of the pulmonary rehabilitation programmes (setting, components and duration).
Health‐related quality of life measurement instruments and associated results.
Exercise capacity measure outcomes and corresponding results.
The lead review author and co‐review authors resolved discrepancies during the data extraction process through discussion; they consulted a third review author when unresolved issues remained. Review authors requested missing data from the authors of the primary studies. They asked these authors to provide additional information by filling in tables similar to the ones used by the review authors during the data extraction process. Two review authors (BMC, EM) entered all data into the Review Manager software (RevMan 2011) and checked them for accuracy.
If a study reported multiple group comparisons (e.g. exercise therapy with inspiratory muscle training compared with exercise therapy alone or with conventional community care), treatment groups considered relevant to PR were combined as if one intervention group,.and this group was compared with the group receiving conventional community care. Studies in which multiple group comparisons included interventions that were not considered relevant to PR such as acupuncture were not combined.
Assessment of risk of bias in included studies
The lead review author (BMC) assessed the risk of bias for all included studies. A second review author (DC, EM or KM) independently assessed the risk of bias for each study. The review authors followed the criteria for assessing risk of bias provided by The Cochrane Collaboration in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011) and contained in RevMan (RevMan 2011). We assessed risk of bias according to the following domains (Appendix 6).
Random sequence generation.
Allocation concealment.
Blinding of participants and personnel.
Blinding of outcome assessment.
Incomplete outcome data.
Selective outcome reporting.
Other bias.
We considered several important potential sources of bias that have proved to be major determinants of the magnitude of the effect size in clinical trials: unconcealed randomisation, unblinded study personnel, incomplete outcome data and attrition of more than 20% of those randomly assigned. The first of these has been associated with an overestimation of treatment effect by up to 40% (Schulz 1995), and the second may result in differential encouragement during performance testing, with the potential for distortion of the results (up to 30.5 metres in a six‐minute walk test) (Guyatt 1984). Schulz 1995 argued that loss to follow‐up of 20% or greater should be a matter of concern as it relates to the possibility of bias.
Review authors resolved disagreements by consensus. If details pertaining to randomisation, masking, drop‐out and withdrawal were not specified or were unclear in the original trial publication, we contacted the study authors to clarify the issue.
Measures of treatment effect
Continuous data
Different measures of HRQoL and exercise capacity have been reported in the primary studies. Both primary outcomes (HRQoL) and secondary outcomes (exercise capacity) are continuous outcomes. For these continuous variables, we recorded mean change from baseline or mean postintervention values and standard deviation (SD) for each group for outcomes measured using the same metrics. When 95% confidence intervals (CIs) and standard errors (SEs) were reported, we calculated SDs as guided by the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). When SDs were missing from studies and it was not possible to obtain the results from study authors, we used a mean value for the SD of the other studies that reported that outcome. All outcomes were reported independently, so standardised mean differences (SMDs) for outcomes were not required. Mean differences (MDs) with 95% CIs were calculated for each study by using a random‐effects model.
Dichotomous data
We did not plan to analyse dichotomous outcomes.
Unit of analysis issues
Cluster‐randomised trials
We included cluster‐randomised trials in the analysis for the current review alongside individually randomised trials. We made an adjustment to the sample size in these studies for each intervention based on the method described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). This method utilised the intracluster correlation co‐efficient (ICC) as calculated from trial results.
Multi‐armed trials
We included multi‐armed trials in this review. To overcome potential issues due to multiple, correlated comparisons, we analysed multi‐armed trials using methods described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). When feasible, we combined multiple comparison groups to create one relevant intervention group and one relevant comparison group.
Dealing with missing data
For included studies, we noted the level of attrition; any study with greater than 20% attrition was considered at high risk of attrition bias. When standard deviations (SDs) of the change were missing from studies, and it was not possible to obtain the result from study authors, we used the mean value for the SD of other included studies that reported that outcome. We excluded from the analysis studies in which only medians and percentiles were available and study authors reported no other means of calculating mean change scores.
Assessment of heterogeneity
We assessed heterogeneity visually through inspection of forest plots, and statistical heterogeneity in each meta‐analysis using Tau², I² and Chi² statistics. We regarded heterogeneity as substantial when Tau² was greater than zero and I² was greater than 30% or a low P value (< 0.10) was reported for the Chi² test for heterogeneity.
Assessment of reporting biases
When 10 or more studies were included in the meta‐analysis, we investigated reporting biases (such as publication bias) by using funnel plots. When asymmetry was suggested on visual assessment, we undertook exploratory analyses to investigate asymmetry using the test proposed by Egger 1997 (see Table 2).
1. Publication bias: results of Egger and Begg‐Mazumdar Kendall's tests.
| CRQ Fatigue |
Bias indicators Begg‐Mazumdar: Kendall's tau = 0.22807; P value 0.1863 Egger: bias = 1.61189 (95% CI = ‐0.194745 to 3.418525); P value 0.077 |
| CRQ Emotional |
Bias indicators Begg‐Mazumdar: Kendall's tau = 0.204678; P value 0.2378 Egger: bias = 0.997332 (95% CI = ‐0.618039 to 2.612702); P value 0.2101 |
| CRQ Mastery |
Bias indicators Begg‐Mazumdar: Kendall's tau = 0.146199; P value 0.4063 Egger: bias = 1.531134 (95% CI = ‐0.268167 to 3.330434); P value 0.0904 |
|
CRQ Dyspnoea (see Figure 1 for funnel plot) |
Bias indicators Begg‐Mazumdar: Kendall's tau = 0.274854; P value 0.1082 Egger: bias = 1.275427 (95% CI = ‐0.761574 to 3.312427); P value 0.204 |
|
SGRQ Total (see Figure 2 for funnel plot) |
Bias indicators Begg‐Mazumdar: Kendall's tau = ‐0.052632; P value 0.73 Egger: bias = ‐0.459813 (95% CI = ‐2.086751 to 1.167125); P value 0.5588 |
| SGRQ Symptoms |
Bias indicators Begg‐Mazumdar: Kendall's tau = 0.017544; P value 0.945 Egger: bias = 0.076734 (95% CI = ‐1.241745 to 1.395213); P value 0.9037 |
| SQRQ Activity |
Bias indicators Begg‐Mazumdar: Kendall's tau = ‐0.052632; P value 0.73 Egger: bias = ‐0.336937 (95% CI = ‐2.10096 to 1.427086); P value 0.692 |
| 6MWT |
Bias indicators Begg‐Mazumdar: Kendall's tau = 0.16074; P value 0.1601 Egger: bias = 1.24304 (95% CI = 0.183967 to 2.302131); P value 0.0227 |
| Incremental Shuttle Walk Test |
Bias indicators Begg‐Mazumdar: Kendall's tau = 0.0776906; P value 0.846 Egger: bias = ‐0.21 2523 (95% CI = ‐2.7776 to 2.351859); P value 0.846 |
| Cycle Ergometer |
Bias indicators Begg‐Mazumdar: Kendall's tau = ‐0.2666667; P value 0.139 Egger: bias = 1.57164 (95% CI = 0.6053 to 2.337984); P value 0.0036 |
Data synthesis
Review authors undertook statistical analysis by using Review Manager software (RevMan 2011). Throughout the analysis, we used mean differences (MDs) as determined (to take into account pre‐experiment group differences) from the differences between preintervention and postintervention changes in treatment and control groups. We combined MDs according to random‐effects analyses (Shadish 1994) and presented the results as average treatment effects with 95% CIs and estimates of Tau² and I². In the case of cross‐over trials, we considered only the first study period and excluded from the analysis data obtained during the second study period. We explored heterogeneity through a priori specified subgroup analyses. When possible, for each outcome, we discussed the summary effect estimate in the context of its minimal clinically important difference (MCID). The MCID is defined as the smallest difference in score corresponding to the smallest difference perceived by the average patient that would mandate, in the absence of troublesome side effects and excessive costs, a change in management of a patient's condition (Jaeschke 1989).
Subgroup analysis and investigation of heterogeneity
To explain anticipated heterogeneity among study results, we defined a set of three a priori hypotheses on which sensitivity analyses were to be based. We identified potential sources of heterogeneity in relation to the outcomes of exercise capacity and HRQoL. We then classified these hypotheses into subcategories as follows.
Interventions
The contribution of each of the components of PR programmes to patient improvement in exercise capacity and HRQoL is not known. We hypothesised that the more comprehensive the rehabilitation programme, the larger would be the effect size in improving exercise capacity and HRQoL. We also hypothesised that a difference in intervention effect may be noted between hospital only‐based and community/home‐based interventions. Therefore, we performed a subgroup analysis of:
pulmonary rehabilitation and exercise only interventions versus PR plus a more comprehensive intervention within which education was included; and
hospital only‐based versus community/home‐based programmes.
Methodological quality
We hypothesised that the results of trials would be influenced by their methodological quality. For the purpose of this subgroup analysis, we defined high‐quality trials as those at low risk of bias for:
allocation concealment; or
incomplete outcome data (i.e. loss to follow‐up ≥ 20%).
We assessed for subgroup differences by using interaction tests available within RevMan (RevMan 2011). We reported the results of subgroup analyses by quoting the statistic and the P value, and the interaction test by providing the I² value.
Sensitivity analysis
We performed sensitivity analyses on the basis of trial quality by repeating our analysis among only those trials judged to be of 'high quality.' For the purposes of this review, 'high‐quality' trials are defined as trials with low risk of bias due to allocation concealment or low risk of bias due to incomplete outcome data. We limited sensitivity analyses to primary outcomes (see Types of outcome measures).
Results
Description of studies
See Characteristics of included studies and Characteristics of excluded studies as well as baseline characteristics (Table 3) and study design (Table 4).
2. Baseline characteristics.
| Study | Rehab sample size | Male | Female | Mean age (SD) | FEV1 (SD) | Control sample size | Male | Female | Mean age (SD) | FEV1 (SD) |
| Barakat 2008 | 35 | na | na | 63.7 | 41.9 | 36 | na | na | 65.9 | 43.3 |
| Baumann 2012 | 37 | na | na | 65 | 45 | 44 | na | na | 63 | 47 |
| Behnke 2000a | 23 | 12 | 3 | 64.0 (1) | 34.1 (7.4) | 23 | 11 | 4 | 68.0 (2.2) | 37.5 (6.6) |
| Bendstrup 1997 | 27 | 7 | 9 | 64 (3) | 1.02 L/min (0.06) | 20 | 7 | 9 | 65 (2) | 1.04 L/min (0.07) |
| Booker 1984 | 32 | na | na | 66 (8) | 0.85 L (0.29) | 37 | na | na | 65 (7) | 0.97 L (0.37) |
| Borghi‐Silva 2009 | 20 | 13 | 7 | 67 (10) | 33 (9) | 14 | 12 | 8 | 67(10) | 35 (11) |
| Boxall 2005 | 23 | 11 | 12 | 77.6 (7.6) | 40.5 (15.9) | 23 | 15 | 8 | 75.8 (8.1) | 37.7 (15.0) |
| Busch 1988 | 7 | 5 | 2 | 65 (16) | 26% (9) | 7 | 6 | 1 | 66 (16) | 27% (11) |
| Cambach 1997 | 15 | 7 | 8 | 62 (5) | 59% (16) | 8 | 6 | 2 | 62 (9) | 60% (23) |
| Casaburi 2004 | 12 | 12 | 0 | 69 (10) | 36% (9) | 12 | 12 | 0 | 68 (9) | 39% (12) |
| Casey 2013 | 178 | 117 | 61 | 68.8 (10.2) | 57.6 (14.3) | 172 | 106 | 66 | 68.4 (10.3) | 59.7 (13.8) |
| Cebollero 2012 | 28 | 28 | 0 | 68 (7) | 47.8 (5) | 8 | 8 | 0 | 69(5) | 38.7 (5) |
| Chan 2011 | 69 | 61 | 8 | 73.6 (7.5) | 91 (0.39) | 67 | 58 | 9 | 73.6 (7.4) | 89 (0.39) |
| Chlumsky 2001 | 13 | 12 | 1 | 63 (11) | 43% (21) | 6 | 5 | 1 | 65 (13) | 51% (17) |
| Clark 1996 | 32 | na | na | 58 (8) | 1.72 L (0.83) | 16 | na | na | 55 (8) | 1.44 L (0.59) |
| Cochrane 2006 | 74 | 32 | 42 | na | na | 50 | 18 | 32 | na | na |
| Cockcroft 1981 | 18 | 18 | 0 | 61 (5) | 1.53 L (0.70) | 16 | 16 | 0 | 60 (5) | 1.32 L (0.44) |
| De Souto Araujo 2012 | 21 | 12 | 9 | 59 | 39.2 (11.4) /43.9 (10.3) |
11 | 8 | 3 | 71.1 | 45.1 (12.6) |
| Deering 2011 | 25 | 11 | 14 | 67.7 (5.3) | 77.0 (19) | 19 | 8 | 8 | 68.6 (5.5) | 45.8 (18.3) |
| Elci 2008 | 39 | 33 | 6 | 59.67 (8.6) | 47.7 | 39 | 33 | 6 | 58.08 (11.45) | 46.28 |
| Emery 1998 | 25 | 15 | 14 | 65 (6) | 1.29 L (0.63) | 25 | 12 | 13 | 67 (7) | 1.02 L (0.37) |
| Engström 1999 | 26 | 14 | 12 | 66 (5) | 31% (11) | 24 | 12 | 12 | 67 (5) | 34% (10) |
| Faager 2004 | 10 | 3 | 7 | 72 (9) | 26 (7) | 10 | 3 | 7 | 70 (8) | 28 (6) |
| Faulkner 2010 | 10 | na | na | na | na | 10 | na | na | na | na |
| Fernandez 2009 | 30 | 29 | 1 | 66 (8) | 33 (10) | 20 | 20 | 0 | 70 (5) | 38 (12) |
| Finnerty 2001 | 36 | 25 | 11 | 70 (8) | 41% (19) | 29 | 19 | 10 | 68 (10) | 41% (16) |
| Gohl 2006 | 17 | 6 | 4 | 62.5 (7) | 53.4 (10.7) | 17 | 7 | 2 | 53.7 (5.8) | 63.2 (8.5) |
| Goldstein 1994 | 38 | 21 | 17 | 66 (7) | 35% (15) | 40 | 17 | 23 | 65 (8) | 35% (12) |
| Gosselink 2000 | 37 | 31 | 6 | 60 (9) | 41% (16) | 33 | 30 | 3 | 63 (7) | 43% (12) |
| Gottlieb 2011 | 35 | 7 | 15 | 74.1 (66–82) | 64.27 (7.9) | 26 | 7 | 13 | 73.2 (67–88) | 67.05 (8.8) |
| Griffiths 2000 | 93 | 57 | 37 | 68 (8) | 40% (16) | 91 | 54 | 37 | 68 (8) | 39% (16) |
| Gurgun 2013 | 30 | 28 | 28 | 64.0 (10.8) | 41.9 (10.8) | 16 | 15 | 1 | 67.8 (6.6) | 39.3 (9.3) |
| Güell 1995 | 30 | 30 | 30 | 64 (7) | 31% (12) | 30 | 30 | 0 | 66 (6) | 39% (14) |
| Güell 1998 | 18 | 16 | 2 | 68 (8) | 32% (11) | 17 | 17 | 0 | 66 (8) | 38% (15) |
| Hernandez 2000 | 20 | 20 | 0 | 64 (8) | 71.1 (18.9) | 17 | 17 | 0 | 63 (7) | 74.7 (14.7) |
| Hoff 2007 | 6 | 4 | 2 | 62.8 (1.4) | 49.9 (4.6) | 6 | 4 | 2 | 60.6 (3.0) | 45.2 (6.0) |
| Jones 1985 | 8 | 6 | 2 | 64 (6) | 0.78 L (0.27) | 6 | 1 | 5 | 63 (8) | 0.68 L (0.12) |
| Karapolat 2007 | 26 | 21 | 5 | 64.81 (9.4) | 55.50% | 19 | 18 | 1 | 67.21 (6.72) | 58% |
| Lake 1990 | 7 | 6 | 1 | 66.3 (6.8) | 0.83 L (0.25) | 7 | 4 | 3 | 65.7 (3.5) | 0.97 L (0.29) |
| Lindsay 2005 | 25 | 20 | 5 | 69.5 (9.3) | 0.9 L (0.3) | 25 | 18 | 7 | 69.8 (10.3) | 0.8 L (0.4) |
| Liu 2012 | 36 | 26 | 10 | 61.34 (8.3) | 61.27 (5.86) | 36 | 29 | 7 | 62.2 (6.34) | 61.43 (6.17) |
| McGavin 1977 | 12 | 12 | 0 | 61 (6) | 0.97 L (0.33) | 12 | 12 | 0 | 57 (8) | 1.15 L (0.72) |
| McNamara 2013 | 38 | 18 | 15 | 72 (10) | 60 (10) | 15 | 8 | 7 | 70 (9) | 55 (20) |
| Mehri 2007 | 20 | 11 | 9 | 52.1 (10.7) | na | 18 | 7 | 11 | 52.17 (11.6) | na |
| Mendes De Oliveira 2010 | 56 | 46 | 10 | 66.4/71.3 | 47.5/ 51.5 | 29 | 19 | 10 | 70.8 | 41.4 |
| Nalbant 2011 | 14 | 11 | 3 | 73.5 | 58.5 (48‐65) | 15 | 13 | 2 | 68 | 57 (44‐66) |
| O'Shea 2007 | 27 | na | na | 66.9 (7) | 49 | 27 | na | na | 68.4 (9.9) | 52 |
| Ozdemir 2010 | 25 | 25 | 0 | 60.9 (8.8) | 54.5 (15.6) | 25 | 25 | 0 | 64.1 (8.9) | 54.1 (20.2) |
| Paz‐Diaz 2007 | 10 | 6 | 4 | 67 (5) | 34 (11) | 14 | 12 | 2 | 62 (7) | 30 (9) |
| Petty 2006 | 149 | 80 | 69 | 68.8 (9.2) | na | 73 | 40 | 33 | 66.8 (9.9) | na |
| Reardon 1994 | 10 | 5 | 5 | 66 (8) | 35% (10) | 10 | 5 | 5 | 66 (7) | 33% (15) |
| Ringbaek 2000 | 24 | 1 | 23 | 62 (7) | 50% (17) | 21 | 6 | 15 | 65 (8) | 44% (14) |
| Gomez 2006 | 64 | 39 | 9 | 64.1/64.9 | 74 (66.5‐81.5) | 33 | 19 | 4 | 63.4 | 60.1 (55.6‐64.4) |
| Simpson 1992 | 14 | 5 | 9 | 73 (5) | 40% (19) | 14 | 10 | 4 | 70 (6) | 39% (21) |
| Singh 2003 | 20 | na | na | na | 28 (7.5) | 20 | na | na | na | 26 (7.1) |
| Sridhar 2008 | 61 | 30 | 31 | 69.9 (9.6) | 42.9 (15.5) | 61 | 30 | 31 | 69.68 (10.4) | 48.9 (18.69) |
| Strijbos 1996 | 15 | 14 | 1 | 61 (6) | 40% (20) | 15 | 12 | 3 | 63 (5) | 43% (9) |
| Theander 2009 | 15 | 3 | 9 | 66 | 35.1 (7.6) | 15 | 10 | 4 | 64 | 32.3 (9.5) |
| Vallet 1994 | 10 | 7 | 3 | 60 (9) | 57.2 | 10 | 8 | 2 | 58 (6) | 55.7 |
| Van Wetering 2010 | 102 | 72 | 30 | 65.9 (8.8) | 58 (17) | 97 | 69 | 28 | 67.2 (8.9) | 60 (15) |
| Vijayan 2010 | 16 | na | na | na | na | 15 | na | na | na | na |
| Weiner 1992 | 12 | 6 | 6 | 67 (9) | 32.8 (3) | 12 | 5 | 7 | 61 (9) | 39.2 (2.8) |
| Wen 2008 | 32 | 31 | 1 | 67 (7)/68 (7) | 46 (10)/50 (14) | 9 | 9 | 0 | 66(10) | 52 (14) |
| Wijkstra 1994 | 28 | 23 | 5 | 64 (5) | 44% (11) | 15 | 14 | 1 | 62 (5) | 45% (9) |
| Xie 2003 | 25 | 22 | 3 | 54 (6) | 42% (16) | 25 | 21 | 4 | 54 (6) | 40% (17) |
na: not available.
3. Study design.
| Study | Follow‐up |
Duration (weeks) |
Setting |
Programme type |
| Barakat 2008 | 14 weeks | 14 | Outpatient | Exercise + other |
| Baumann 2012 | 6 months | 8 | Community | Exercise + other |
| Behnke 2000a | 3, 6 months | 24 | Inpatient | Exercise + other |
| Bendstrup 1997 | 12, 24 weeks | 12 | Outpatient | Exercise |
| Booker 1984 | 3, 6, 12 months | 9 | Home | Exercise + other |
| Borghi‐Silva 2009 | 6 weeks | 6 | Outpatient | Exercise |
| Boxall 2005 | 12 weeks | 12 | Home | Exercise + other |
| Busch 1988 | 18 weeks | 18 | Home | Exercise |
| Cambach 1997 | 3 months | 12 | Community | Exercise + other |
| Casaburi 2004 | 10 weeks | 10 | Outpatient | Exercise + other |
| Casey 2013 | 12 weeks | 8 | Community | Exercise + other |
| Cebollero 2012 | 12 weeks | 12 | Outpatient | Exercise |
| Chan 2011 | 3 months | 12 | Community | Exercise |
| Chlumsky 2001 | 8 weeks | 8 | Outpatient | Exercise |
| Clark 1996 | 12 weeks | 12 | Home | Exercise |
| Cochrane 2006 | 6 weeks, 6 months, 12 months | 6 | Outpatient | Exercise + other |
| Cockcroft 1981 | 2, 6 months | 6 | Outpatient | Exercise |
| De Souto Araujo 2012 | 8 weeks | 8 | Community | Exercise |
| Deering 2011 | 8 weeks | 7 | Outpatient | Exercise + other |
| Elci 2008 | 1, 3 months | 12 | Community /Home |
Exercise + other |
| Emery 1998 | 10 weeks | 10 | Outpatient | Exercise + other |
| Engström 1999 | 12 months | 52 | Outpatient /Home |
Exercise + other |
| Faager 2004 | 8 weeks, 6 months | 8 | Inpatient /Home |
Exercise + other |
| Faulkner 2010 | week 9 | 8 | Community | Exercise + other |
| Fernandez 2009 | 1 year | 52 | Home | Exercise + other |
| Finnerty 2001 | 12, 24 weeks | 6 | Outpatient | Exercise + other |
| Gohl 2006 | 12 months | 52 | Community | Exercise |
| Goldstein 1994 | 24 weeks | 8 | Inpatient | Exercise + other |
| Gosselink 2000 | 6, 18 months | 24 | Outpatient | Exercise |
| Gottlieb 2011 | 6 months | 7 | Community | Exercise + other |
| Griffiths 2000 | 1 year | 6 | Outpatients /Home |
Exercise + other |
| Gomez 2006 | 3, 6 months | 12 | Community | Exercise + other |
| Güell 1995 | 3, 6, 9, 12, 18, 24 months | 12 | Outpatient /Home |
Exercise |
| Güell 1998 | 8 weeks | 8 | Outpatient | Exercise |
| Gurgun 2013 | 8 weeks, 6 months | 8 | Outpatient | Exercise + other |
| Hernandez 2000 | 12 weeks | 12 | Home | Exercise |
| Hoff 2007 | 8 weeks | 8 | Outpatient | Exercise |
| Jones 1985 | 10 weeks | 10 | Home | Exercise |
| Karapolat 2007 | 8, 12 weeks | 8 | Outpatient | Exercise + other |
| Lake 1990 | 8 weeks | 8 | Outpatient | Exercise |
| Lindsay 2005 | 6 weeks, 3 months | 6 | Community | Exercise + other |
| Liu 2012 | 6 months | 24 | Inpatient /Home |
Exercise |
| McGavin 1977 | 14 weeks | ?12 | Home | Exercise |
| McNamara 2013 | 8 weeks | 8 | Outpatient | Exercise |
| Mehri 2007 | 4 weeks | 4 | Outpatient | Exercise |
| Mendes De Oliveira 2010 | 12 weeks | 12 | Outpatient /Home |
Exercise + other |
| Nalbant 2011 | 3, 6 months | 24 | Nursing home | Exercise + other |
| O'Shea 2007 | 3, 6 months | 12 | Outpatient /Home |
Exercise |
| Ozdemir 2010 | 1 month | 4 | Outpatient | Exercise |
| Paz‐Diaz 2007 | 8 weeks | 8 | Outpatient | Exercise |
| Petty 2006 | 8 weeks | 8 | Home | Exercise + other |
| Reardon 1994 | 6 weeks | 6 | Outpatient | Exercise + other |
| Ringbaek 2000 | 8 weeks | 8 | Outpatient | Exercise + other |
| Simpson 1992 | 8 weeks | 8 | Outpatient | Exercise |
| Singh 2003 | 4 weeks | 4 | Home | Exercise |
| Sridhar 2008 | 6 months | 6 | Outpatients /Home |
Exercise + other |
| Strijbos 1996 | 3, 6, 12, 18 months | 12 | Outpatient | Exercise + other |
| Theander 2009 | 12 weeks | 12 | Outpatient /Home |
Exercise + other |
| Vallet 1994 | 8 weeks | 8 | Inpatient | Exercise |
| Van Wetering 2010 | 4 months | 12 | Community | Exercise + other |
| Vijayan 2010 | Unclear | 6 | Unclear | Exercise |
| Weiner 1992 | 6 months | 24 | Outpatient | Exercise |
| Wen 2008 | 12 weeks | 12 | Outpatient | Exercise |
| Wijkstra 1994 | 12 weeks | 12 | Outpatient /Home |
Exercise + other |
| Xie 2003 | 12 weeks | 12 | Home | Exercise |
Results of the search
Our search yielded 1284 citations with potential for inclusion (see Figure 3). We excluded 1132 citations during the initial screening of titles and abstracts and assessed 98 studies (152 citations) on the basis of a full‐text review. Of these, 51 studies (68 citations) failed to meet the inclusion criteria. A further five studies (eight citations) provided insufficient detail to allow a decision and are still awaiting classification (see Characteristics of studies awaiting classification). Of these, we conducted a teleconference with the author of two studies (Meshcheryakova 2010; Meshcheryakova 2012) and are awaiting additional unpublished information. We were not able to establish contact with the authors of the other three studies (Aksu 2006; D'Amico 2010; Ren 2011). Three studies were ongoing at the time of this review, and results were not yet published; the study authors wished to withhold results until after publication (Chang 2008; Gurgun 2011; Sathyapala 2008) (see Characteristics of ongoing studies). In addition, eight citations were related to five studies that were already included in the previous version of this review. Thus, 34 studies (65 citations) were included for the first time in this review, in addition to the 31 studies (65 citations) already included in the previous version of the review. We have provided details of the literature search for the previous version of the review in Appendix 1.
3.
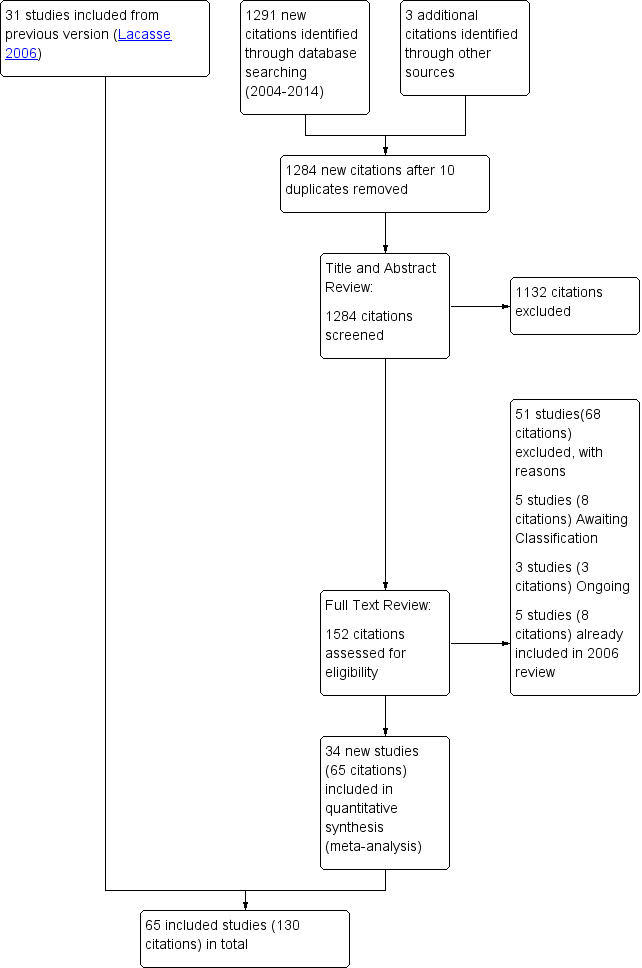
Study flow diagram.
Included studies
We included the 31 RCTs from the 2006 version of the Cochrane review (Lacasse 2006). A total of 65 studies (represented by 130 citations) contributed to this meta‐analysis, including 34 new studies (Barakat 2008; Baumann 2012; Borghi‐Silva 2009; Casey 2013; Cebollero 2012; Chan 2011; Cochrane 2006; De Souto Araujo 2012; Deering 2011; Elci 2008; Faager 2004; Faulkner 2010; Fernandez 2009; Gohl 2006; Gomez 2006; Gottlieb 2011; Gurgun 2013; Hoff 2007; Karapolat 2007; Lindsay 2005; Liu 2012; McNamara 2013; Mehri 2007; Mendes De Oliveira 2010; Nalbant 2011; O'Shea 2007; Ozdemir 2010; Paz‐Diaz 2007; Petty 2006; Sridhar 2008; Theander 2009; Van Wetering 2010; Vijayan 2010; Wen 2008), in addition to the 31 studies included in the original review (Behnke 2000a; Bendstrup 1997; Booker 1984; Boxall 2005; Busch 1988; Cambach 1997; Casaburi 2004; Chlumsky 2001; Clark 1996; Cockcroft 1981; Emery 1998; Engström 1999; Finnerty 2001; Goldstein 1994; Gosselink 2000; Griffiths 2000; Güell 1995; Güell 1998; Hernandez 2000; Jones 1985; Lake 1990; McGavin 1977; Reardon 1994; Ringbaek 2000; Simpson 1992; Singh 2003; Strijbos 1996; Vallet 1994; Weiner 1992; Wijkstra 1994; Xie 2003). We provided descriptions of these individual studies in the Characteristics of included studies table.
These studies involved 3822 participants, 2090 of whom were randomly allocated to some form of exercise rehabilitation for a minimum duration of four weeks, and 1732 individuals who were randomly assigned to usual care. For a detailed account of the criteria required for inclusion, see Criteria for considering studies for this review. The sample size in the included studies ranged from 12 participants (Hoff 2007) to 350 participants (Casey 2013) with a median of 45 participants (interquartile range (IQR) 29.5 to 67). We noted a large gender imbalance across all studies, with 69% of participants being male and with 10 studies including no female participants.
Only six studies reported patient‐based programmes, three of which were combined with a home‐based follow‐up component. Thirty‐seven studies were hospital out‐patient based; eight of these included a home‐based element. In all, 21 programmes were community based, 11 of which were entirely home based, and one programme combined community‐ and home‐based components. The venue for the programme run by Vijayan 2010 was unclear from the reports. The duration of the programmes ranged from four weeks (three studies) to one year (three studies). Eight‐ and 12‐week programmes (18 studies of each) were most common. Timelines for assessment of participants followed a pattern identical to that of programme duration.
All but two trials that met the inclusion criteria used a standard parallel‐group design. Casey 2013 utilised cluster samples from general practices, whereas Cambach 1997 conducted a cross‐over trial. Most studies (48 trials) randomly assigned participants to two groups (i.e. rehabilitation and usual care), and three trials randomly assigned participants to three intervention groups, in addition to the usual care group (Casaburi 2004; Cochrane 2006; Lake 1990). The remaining 14 trials utilised two intervention groups and a usual care group (Cebollero 2012; De Souto Araujo 2012; Deering 2011; Emery 1998; Gomez 2006; Gurgun 2013; Jones 1985; Liu 2012; McNamara 2013; Mendes De Oliveira 2010; Petty 2006; Strijbos 1996; Weiner 1992; Wen 2008)
Excluded studies
We excluded 51 studies from the current update during the full‐text screening process.The Characteristics of excluded studies table provides full details of the excluded studies.
Risk of bias in included studies
As a result of the nature of the intervention, it was expected that blinding of participants and of professionals who delivered the interventions was not possible. Consequently, risk of performance bias in all studies was high. Risk of bias for other bias domains varied across included studies, and insufficient detail was provided to inform judgement in several included studies (see Figure 4, Risk of bias summary table, and Figure 5, Risk of bias graph, for an overview).
4.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
5.
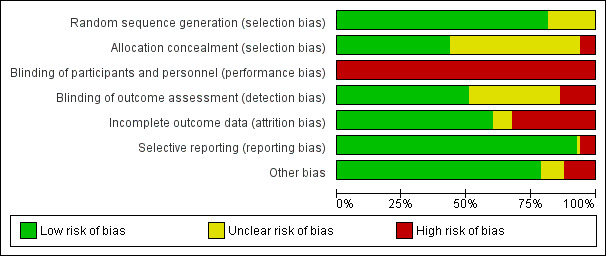
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Allocation
We judged 53 included studies as having low risk of bias in random sequence generation. Information was insufficient to permit a decision in relation to 12 trials (Bendstrup 1997; Borghi‐Silva 2009; Clark 1996; Faager 2004; Fernandez 2009; Hoff 2007; Lindsay 2005; Mehri 2007; Nalbant 2011; Paz‐Diaz 2007; Vijayan 2010; Wen 2008). With regard to allocation concealment, we judged 28 studies as having low risk of bias (Behnke 2000a; Booker 1984; Boxall 2005; Busch 1988; Cambach 1997; Casaburi 2004; Casey 2013; Cebollero 2012; Cochrane 2006; Cockcroft 1981; De Souto Araujo 2012; Emery 1998; Engström 1999; Faulkner 2010; Finnerty 2001; Goldstein 1994; Gomez 2006; Gosselink 2000; Gottlieb 2011; Griffiths 2000; Gurgun 2013; Karapolat 2007; Liu 2012; McNamara 2013; Mendes De Oliveira 2010; O'Shea 2007; Theander 2009; Van Wetering 2010) and four studies as having high risk of bias (Baumann 2012; Güell 1995; Güell 1998; Jones 1985); the remaining 33 studies provided insufficient information to inform judgements.
Blinding
Performance bias
As a result of the nature of the intervention, it was not possible to blind participants or professionals who delivered the interventions. Consequently, we judged all studies as having high risk of performance bias.
Detection bias
Across studies, the level of reporting of whether outcome assessment was blinded was relatively poor. We judged 32 studies as having low risk of detection bias ( Barakat 2008; Booker 1984; Busch 1988; Casaburi 2004; Casey 2013; Cebollero 2012; Chan 2011; Cochrane 2006; De Souto Araujo 2012; Deering 2011; Elci 2008; Emery 1998; Engström 1999; Finnerty 2001; Goldstein 1994; Gomez 2006; Griffiths 2000; Güell 1995; Güell 1998; Hernandez 2000; Jones 1985; Lake 1990; Liu 2012; McNamara 2013; O'Shea 2007; Petty 2006; Reardon 1994; Ringbaek 2000; Simpson 1992; Strijbos 1996; Van Wetering 2010; Weiner 1992). In two of these studies (Engström 1999; Simpson 1992), the primary outcome assessment (quality of life) was blinded but the secondary outcome assessment (exercise capacity) was not. In Lake 1990, the cycle ergometer test was blinded, but the six‐minute walk test was not. In Busch 1988, the cycle ergometer test was not blinded and the 12‐minute walk test was blinded. Among studies that reported blinding of outcome assessment, nine studies were judged as having high risk of detection bias (Boxall 2005; Cambach 1997; Faulkner 2010; Gosselink 2000; Gottlieb 2011; McGavin 1977; Theander 2009; Vallet 1994; Wijkstra 1994), and the remaining 23 studies provided insufficient information to inform judgements.
Incomplete outcome data
We judged 39 studies as having low risk of attrition bias (Barakat 2008; Borghi‐Silva 2009; Boxall 2005; Cambach 1997; Casaburi 2004; Chlumsky 2001; Cockcroft 1981; Emery 1998; Engström 1999; Fernandez 2009; Goldstein 1994; Griffiths 2000; Güell 1995; Güell 1998; Gurgun 2013; Hoff 2007; Karapolat 2007; Lake 1990; Lindsay 2005; Liu 2012; McGavin 1977; McNamara 2013; Mehri 2007; O'Shea 2007; Ozdemir 2010; Paz‐Diaz 2007; Petty 2006; Reardon 1994; Ringbaek 2000; Simpson 1992; Singh 2003; Strijbos 1996; Theander 2009; Vallet 1994; Van Wetering 2010; Vijayan 2010; Weiner 1992; Wijkstra 1994; Xie 2003) and 22 as having high risk (Baumann 2012 24% of people dropped out; Behnke 2000a 35%; Bendstrup 1997 24%; Booker 1984 27%; Busch 1988 30%; Casey 2013 24%; Chan 2011 23%, Cochrane 2006 43%; De Souto Araujo 2012 24%; Deering 2011 42%; Faager 2004 30%; Faulkner 2010 30%; Finnerty 2001 43%; Gohl 2006 44%; Gomez 2006 48%; Gosselink 2000 62%; Gottlieb 2011 32%; Hernandez 2000 38%; Jones 1985 26%; Mendes De Oliveira 2010 27%; Nalbant 2011 28%; Wen 2008 24%). Information was insufficient to inform judgements in five studies (Cambach 1997; Cebollero 2012; Clark 1996; Elci 2008; Vijayan 2010).
Selective reporting
We found no trial registration protocol for most studies to check whether all prespecified outcomes were reported in the articles. However, outcomes listed in the methods section of the included studies were reported in the results section, with the exception of four studies that were judged to have high risk of reporting bias (i.e. Ozdemir 2010, whose results for the CRQ are incomplete; Paz‐Diaz 2007, who did not provide results for the rehabilitation group for CRQ; Petty 2006, in which results of the six‐minute walk test and Short Form (SF)‐36 are not presented; and Weiner 1992, in which results of the SGRQ are not available ). In relation to publication bias, we visually reviewed the funnel plots (Figure 3; Figure 1; Figure 2) and followed this by performing the Egger test (Egger 1997) (Table 2). Egger test results showed no significant publication bias across the studies included in the current meta‐analysis.
1.
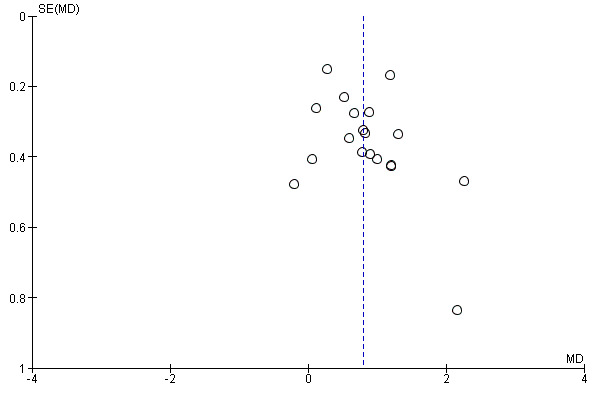
Funnel plot of comparison: 1 Rehabilitation versus usual care, outcome: 1.4 QoL ‐ Change in CRQ (Dyspnoea) (see Table 2 for Egger and Begg‐Mazumdar: Kendall's test results).
2.
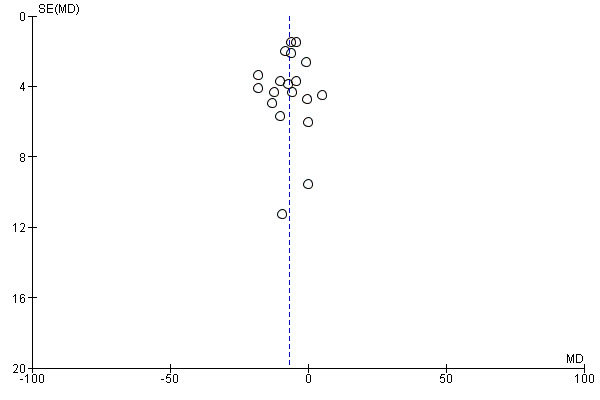
Funnel plot of comparison: 1 Rehabilitation versus usual care, outcome: 1.5 QoL ‐ Change in SGRQ (Total) (see Table 2 for Egger and Begg‐Mazumdar: Kendall's test results).
Other potential sources of bias
We found no other source of bias, with the exception of a tendency toward increased proportions of male participants, as was highlighted earlier.
Effects of interventions
See: Table 1
Pulmonary rehabilitation versus usual care
For this comparison, we included all participants who were randomly assigned in the included studies and received PR (defined as exercise training for at least four weeks with or without educational and/or psychological support) and those allocated to usual care (see Characteristics of included studies for details). We also undertook subgroup analysis as discussed in the Subgroup analysis and investigation of heterogeneity section. All outcomes results utilised in the analyses were based on baseline assessment measurements and the earliest follow‐up assessment up to three months after completion of the intervention.
Primary outcomes
Health‐related quality of life
Among the 65 trials that met the inclusion criteria of the meta‐analysis, 44 made an attempt to measure HRQoL using eight different strategies. Only three of these strategies ‐ the Transitional Dyspnoea Index (TDI; Mahler 1984), the Chronic Respiratory Disease Questionnaire (CRQ; Guyatt 1987a) and the St. Georges Respiratory Questionnaire (SGRQ; Jones 1992) ‐ have been demonstrated to be valid and responsive. Of these, the CRG and the SGRQ have become the recognised standard of assessment of HRQoL amongst patients with COPD and are reported here. We analysed the CRQ and the SGRQ separately. Not all subscales were fully completed by all participants, so the numbers of participants per outcome and per subscale varied.
Chronic Respiratory Disease Questionnaire (CRQ)
Scores for the CRQ are reported on a 7‐point scale. Although 23 studies utilised the CRQ to assess HRQoL, only 19 studies (1291 participants) provided results suitable for analysis.
Participants allocated to rehabilitation programmes had, on average, significantly greater changes in HRQoL CRQ scores across all subscales when compared with participants allocated to control groups (Fatigue: MD 0.68, 95% CI 0.45 to 0.92; 19 trials; 1291 participants; Tau² = 0.15; I² = 64%; Analysis 1.1; Emotional function: MD 0.56, 95% CI 0.34 to 0.78; 19 trials; 1291 participants; Tau² = 0.12; I² = 58%; Analysis 1.2; Mastery: MD 0.71, 95% CI 0.47 to 0.95; 19 trials; 1212 participants; Tau² = 0.16; I² = 63%; Analysis 1.3; Dyspnoea: MD 0.79, 95% CI 0.56 to 1.03; 19 trials; 1283 participants; Tau² = 0.15; I² = 63%; Analysis 1.4).
1.1. Analysis.
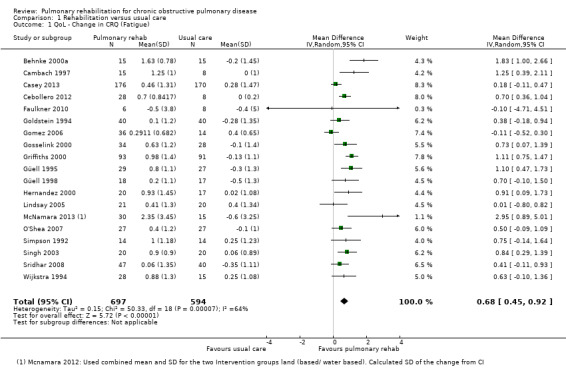
Comparison 1 Rehabilitation versus usual care, Outcome 1 QoL ‐ Change in CRQ (Fatigue).
1.2. Analysis.
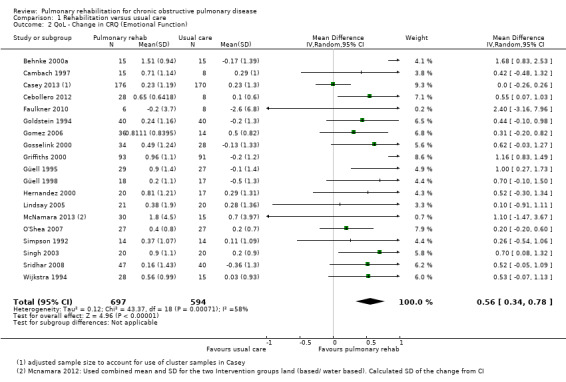
Comparison 1 Rehabilitation versus usual care, Outcome 2 QoL ‐ Change in CRQ (Emotional Function).
1.3. Analysis.
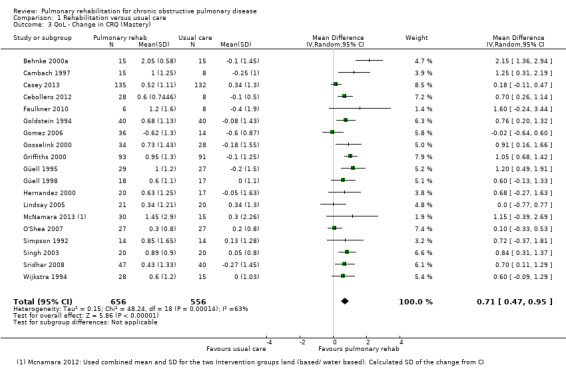
Comparison 1 Rehabilitation versus usual care, Outcome 3 QoL ‐ Change in CRQ (Mastery).
1.4. Analysis.
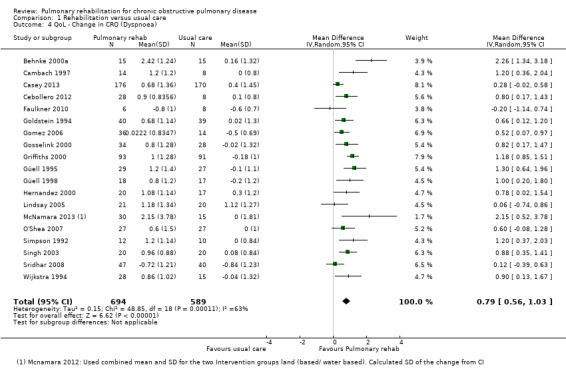
Comparison 1 Rehabilitation versus usual care, Outcome 4 QoL ‐ Change in CRQ (Dyspnoea).
For each of the CRQ domains (dyspnoea, fatigue, emotional function and mastery), the common effect size exceeded the 'minimal clinically important difference' (MCID) (0.5 points on the 7‐point scale) (Jaeschke 1989). The lower limit of the confidence interval around the common treatment effect of the dyspnoea domains (Analysis 1.4) exceeded the MCID, indicating not only statistical significance but also clinical significance in the effect of PR. The lower limits of the remaining domains were slightly below the MCID (Analysis 1.1; Analysis 1.2; Analysis 1.3).
Heterogeneity identified across all domains of the CRQ was substantial, as Tau² was greater than zero, and in all cases, I² was greater than 30% and the P value for the Chi² test was less than 0.10. We undertook subgroup and sensitivity analyses to try to explore heterogeneity; although findings are presented later, they did not explain the high level of heterogeneity.
St. George's Respiratory Questionnaire (SGRQ)
Scores for the SGRQ are reported on a 100‐point scale. Twenty trials utilised the SGRQ to assess the HRQoL of participants. Results were available in a usable format from 19 trials (a maximum of 1153 participants) for inclusion in the meta‐analysis. Barakat 2008 was not included in the analysis, as clarification regarding the SD of the change is needed from the study authors.
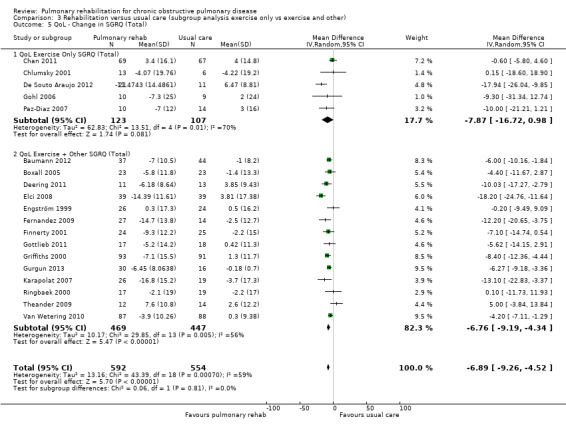
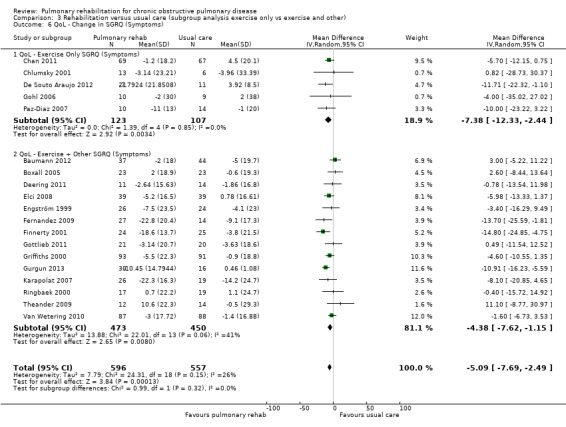
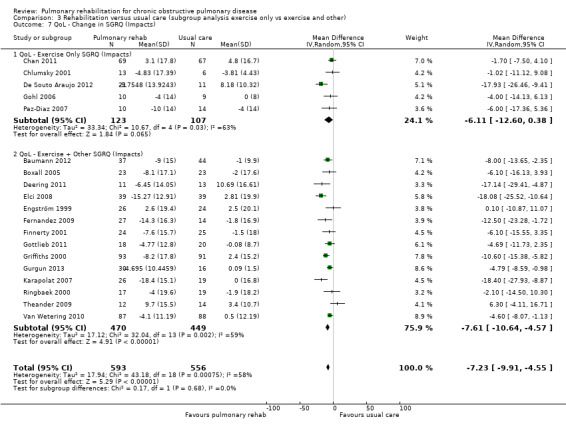
Similar to the CRQ, participants allocated to PR programmes had, on average, significantly greater changes in SGRQ scores across all subscales when compared with participants allocated to control groups (SGRQ total: MD ‐6.89, 95% CI ‐9.26 to ‐4.52; 19 trials; 1146 participants; Tau² = 13.17; I² = 59%; Analysis 1.5; SGRQ symptoms: MD ‐5.09, 95% CI ‐7.69 to ‐2.49; 19 trials; 1153 participants; Tau² = 7.79; I² = 26%; Analysis 1.6; SGRQ impact: MD ‐7.23, 95% CI ‐9.91 to ‐4.55; 19 trials; 1149 participants; Tau² = 17.94; I² = 58%; Analysis 1.7; SGRQ activity: MD ‐6.08, 95% CI ‐9.28 to ‐2.88; 19 trials; 1148 participants; Tau² = 27.01; I² = 64%; Analysis 1.8).
1.5. Analysis.
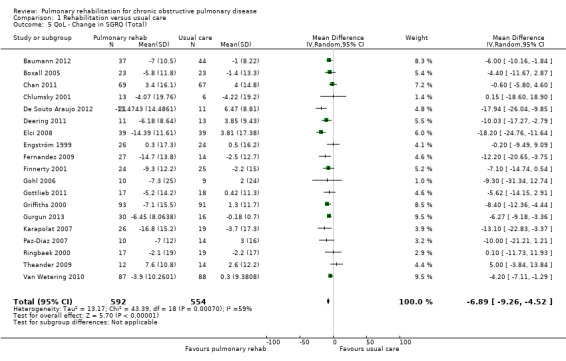
Comparison 1 Rehabilitation versus usual care, Outcome 5 QoL ‐ Change in SGRQ (Total).
1.6. Analysis.
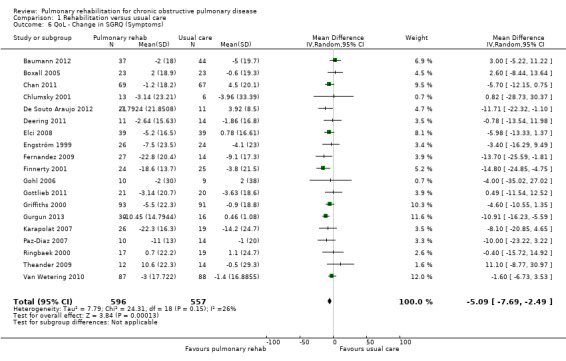
Comparison 1 Rehabilitation versus usual care, Outcome 6 QoL ‐ Change in SGRQ (Symptoms).
1.7. Analysis.
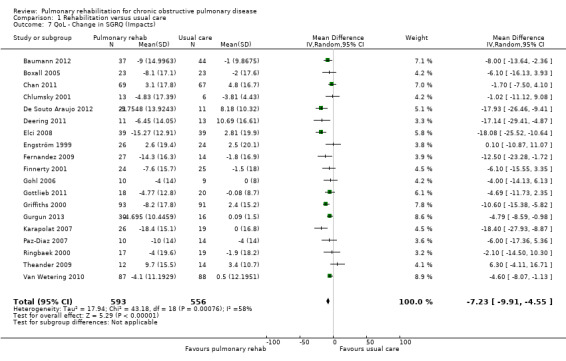
Comparison 1 Rehabilitation versus usual care, Outcome 7 QoL ‐ Change in SGRQ (Impacts).
1.8. Analysis.
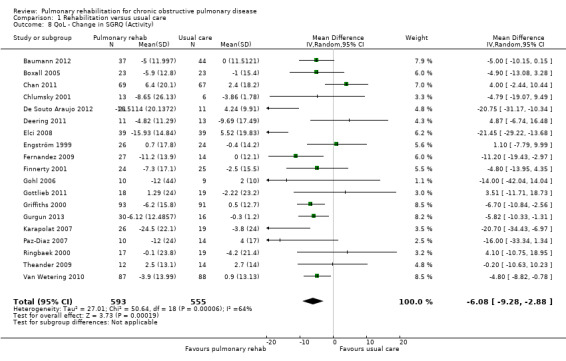
Comparison 1 Rehabilitation versus usual care, Outcome 8 QoL ‐ Change in SGRQ (Activity).
For each of the SGRQ domains (as well as the total SGRQ score), the common effect size exceeded the MCID of four (Jones 1991; Quirk 1991) (Analysis 1.5; Analysis 1.6; Analysis 1.7; Analysis 1.8). All results of the analysis for all domains of the SGRQ were statistically significant. However, the extent of the 95% CI around the pooled treatment effect exceeds the MCID only for the SGRQ total and SGRQ impact domains of the SGRQ, demonstrating unequivocal clinical and statistical significance in these domains.
Heterogeneity in results obtained from the total and all subscales of the SGRQ was substantial, with the exception of the symptoms subscale (Analysis 1.6).
Secondary outcomes
Maximal exercise capacity
A total of 34 trials measured maximal exercise capacity. We limited the meta‐analysis to the 16 trials that used the incremental cycle ergometer test.
Investigators in 16 studies (779 participants) used the incremental cycle ergometer test. On average, a statistically significant increase in mean Wmax (W) was reported among participants allocated to PR compared with those allocated to usual care (MD 6.77, 95% CI 1.89 to 11.65; Tau² = 40.97; I² = 74%; Analysis 1.10). The common effect size exceeded the MCID (4 watts) proposed by Puhan 2011(b). The maximal exercise test showed substantial heterogeneity in the results obtained.
1.10. Analysis.

Comparison 1 Rehabilitation versus usual care, Outcome 10 Maximal Exercise Capacity (cycle ergometer).
Functional exercise capacity
Of the included studies, 43 trials used the six‐minute walk test as an outcome. Of these, 38 (1879 participants: 1012 actively treated, 867 controls) presented the results in a format that could be used for the meta‐analysis (see Analysis 1.11). Investigators reported a statistically significant increase, on average, in the mean difference in metres walked associated with PR (MD 43.93 m, 95% CI 32.64 to 55.21; Tau² = 713.49; I² = 74%; Analysis 1.11). Both the common effect and the lower limit of its confidence interval exceeded the MCID for the 6WMD of 30 metres, as recommended by Holland 2014, indicating the clinical significance of the effect of PR. .
1.11. Analysis.

Comparison 1 Rehabilitation versus usual care, Outcome 11 Functional Exercise Capacity (6MWT)).
Eight trials (694 participants) reported data on the incremental shuttle walk test (ISWT). These test results were analysed independently from those of the 6MWT. On average, a statistically significant increase in mean metres walked was noted among participants allocated to PR compared with those allocated to usual care (MD 39.77, 95% CI 22.38 to 57.15; Tau² = 181.56; I² = 32%). This result is slightly below the MCID of 47.5 m (Singh 2008; Singh 2014) to make this a finding of clinical significance.
Similar to previous outcomes on maximal exercise, both the six‐minute walk test and the analyses demonstrated substantial heterogeneity.
Several other outcome measures were used to measure functional capacity, but because of the limited numbers of trials providing data for these other outcomes (endurance shuttle walk test: two trials; 12‐minute walk test: four trials); four‐minute walk test: one trial)), these findings were not included in the meta‐analysis.
Subgroup and sensitivity analyses
Rehabilitation versus usual care (subgroup analysis hospital‐ versus community‐based pulmonary rehabilitation)
In total, 39 included studies were considered to have a hospital‐based PR intervention delivered on an in‐patient or out‐patient basis. A total of 25 studies focused on programmes that were delivered in the community at community centres or in individuals' homes. One study had both a community‐based and an out‐patient‐based intervention group, so it was excluded from the subgroup analysis (Mendes De Oliveira 2010).
In the subgroup analysis for the CRQ domain outcomes, the 'community' subgroup included nine studies (Cambach 1997; Casey 2013; Faulkner 2010; Gomez 2006; Hernandez 2000; Lindsay 2005; O'Shea 2007; Singh 2003; Wijkstra 1994) and the 'hospital group' included 10 studies (Behnke 2000a; Cebollero 2012; Goldstein 1994; Gosselink 2000; Griffiths 2000; Güell 1995; Güell 1998; McNamara 2013; Simpson 1992; Sridhar 2008; ). For SGRQ outcomes, the community subgroup included nine studies (Baumann 2012; Boxall 2005; Chan 2011; De Souto Araujo 2012; Elci 2008; Fernandez 2009; Gohl 2006; Gottlieb 2011; Van Wetering 2010) and the hospital subgroup included 10 studies (Chlumsky 2001; Deering 2011; Engström 1999; Finnerty 2001; Griffiths 2000; Gurgun 2013; Karapolat 2007; Paz‐Diaz 2007; Ringbaek 2000; Theander 2009).
Evidence suggested a significant difference in treatment effect between subgroups for all domains of the CRQ, with higher mean values, on average, in the PR group in hospital than in the community‐based group (Analysis 2.1; Analysis 2.2; Analysis 2.3; Analysis 2.4). No subgroup differences were reported for any of the SGRQ domains (Analysis 2.5; Analysis 2.6; Analysis 2.7; Analysis 2.8).
2.1. Analysis.
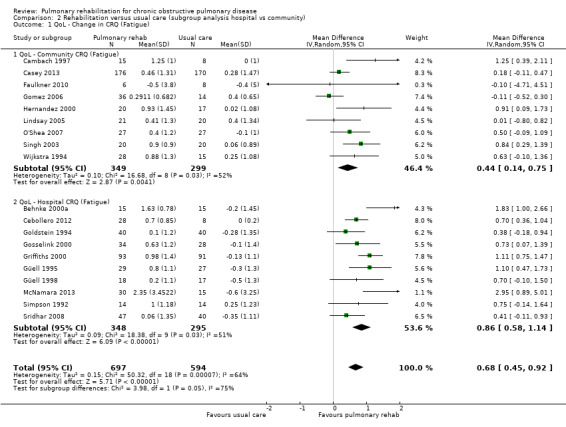
Comparison 2 Rehabilitation versus usual care (subgroup analysis hospital vs community), Outcome 1 QoL ‐ Change in CRQ (Fatigue).
2.2. Analysis.
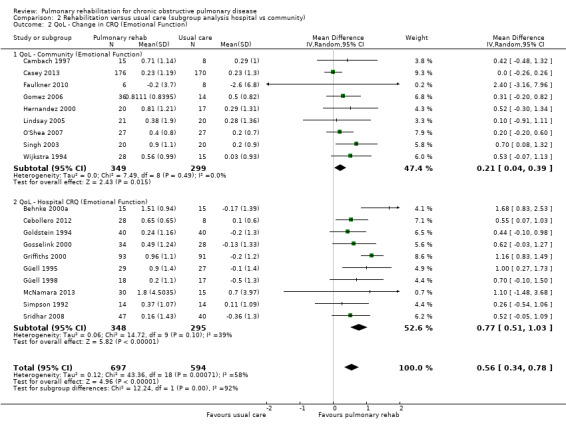
Comparison 2 Rehabilitation versus usual care (subgroup analysis hospital vs community), Outcome 2 QoL ‐ Change in CRQ (Emotional Function).
2.3. Analysis.
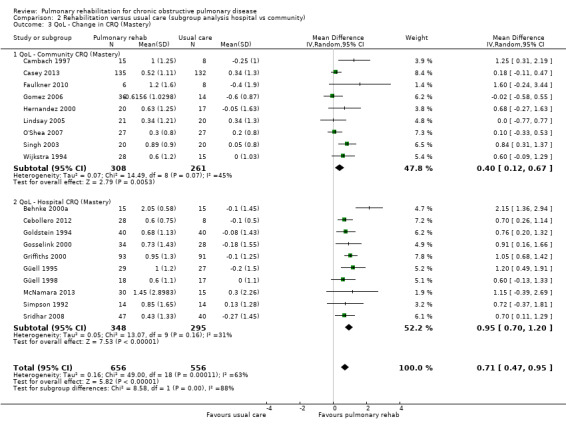
Comparison 2 Rehabilitation versus usual care (subgroup analysis hospital vs community), Outcome 3 QoL ‐ Change in CRQ (Mastery).
2.4. Analysis.
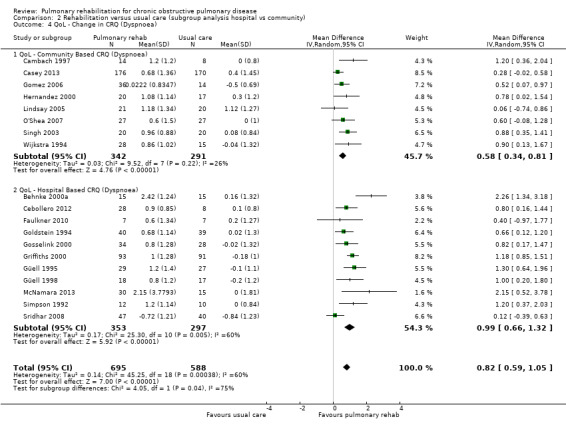
Comparison 2 Rehabilitation versus usual care (subgroup analysis hospital vs community), Outcome 4 QoL ‐ Change in CRQ (Dyspnoea).
2.5. Analysis.
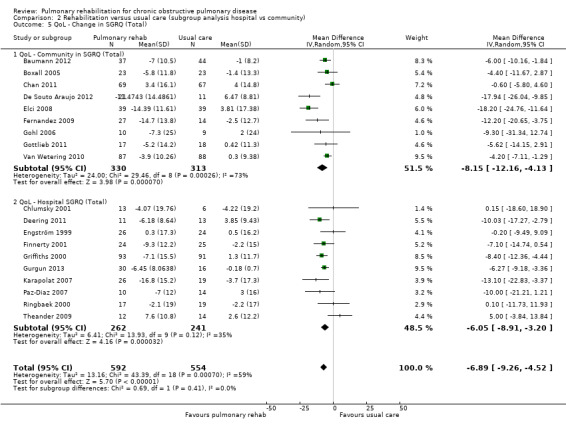
Comparison 2 Rehabilitation versus usual care (subgroup analysis hospital vs community), Outcome 5 QoL ‐ Change in SGRQ (Total).
2.6. Analysis.
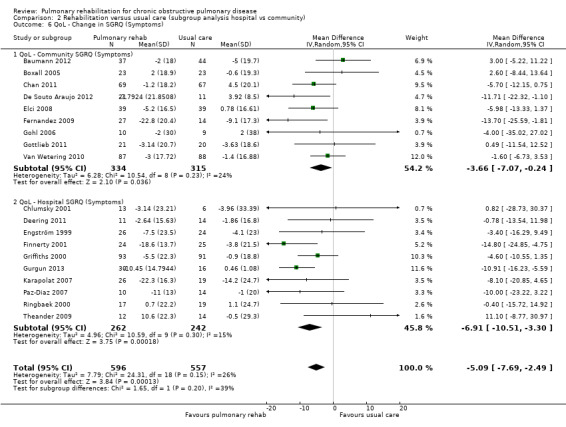
Comparison 2 Rehabilitation versus usual care (subgroup analysis hospital vs community), Outcome 6 QoL ‐ Change in SGRQ (Symptoms).
2.7. Analysis.
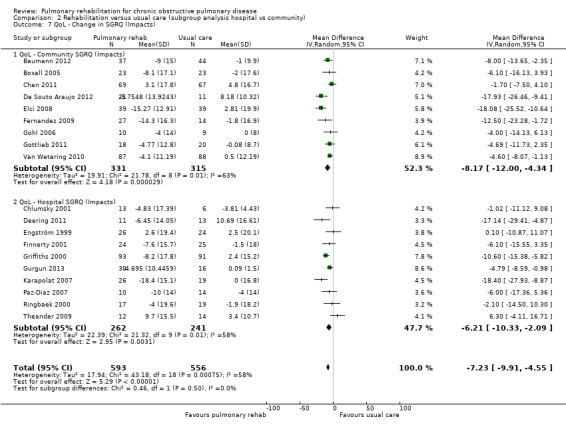
Comparison 2 Rehabilitation versus usual care (subgroup analysis hospital vs community), Outcome 7 QoL ‐ Change in SGRQ (Impacts).
2.8. Analysis.
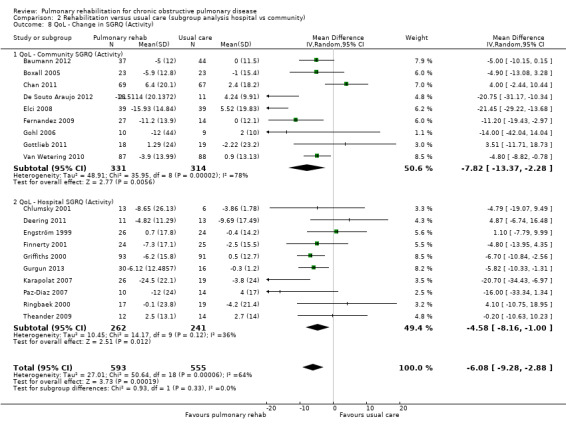
Comparison 2 Rehabilitation versus usual care (subgroup analysis hospital vs community), Outcome 8 QoL ‐ Change in SGRQ (Activity).
Rehabilitation versus usual care (subgroup analysis 'exercise only' vs 'exercise plus more comprehensive components')
A total of 31 trials were included in the 'exercise only' subgroup, and 34 trials in the 'exercise plus more comprehensive components' subgroup, of which 10 trials in the 'exercise only' subgroup (Cebollero 2012; Gosselink 2000; Güell 1995; Güell 1998; Hernandez 2000; McNamara 2013; O'Shea 2007; Simpson 1992; Singh 2003; Sridhar 2008), and nine in the more comprehensive subgroup (Behnke 2000a; Cambach 1997; Casey 2013; Faulkner 2010; Goldstein 1994; Gomez 2006; Griffiths 2000; Lindsay 2005; Wijkstra 1994) reported CRQ data.
For the SGRQ, five trials were included in the 'exercise only' subgroup (Chan 2011; Chlumsky 2001; De Souto Araujo 2012; Gohl 2006; Paz‐Diaz 2007) and 14 trials in the more comprehensive subgroup (Baumann 2012; Boxall 2005; Deering 2011; Elci 2008; Engström 1999; Fernandez 2009; Finnerty 2001; Gottlieb 2011; Griffiths 2000; Gurgun 2013; Karapolat 2007; Ringbaek 2000; Theander 2009; Van Wetering 2010).
No evidence was found of a significant treatment effect between subgroups for all domains of the CRQ (Analysis 3.1; Analysis 3.2; Analysis 3.3; Analysis 3.4) and the SGRQ (Analysis 3.5; Analysis 3.6; Analysis 3.7; Analysis 3.8).
3.1. Analysis.
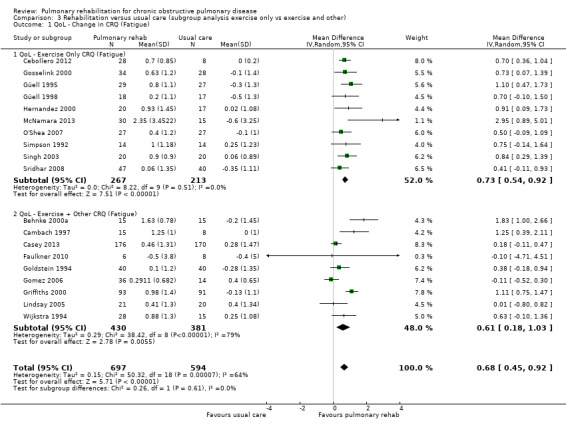
Comparison 3 Rehabilitation versus usual care (subgroup analysis exercise only vs exercise and other), Outcome 1 QoL ‐ Change in CRQ (Fatigue).
3.2. Analysis.
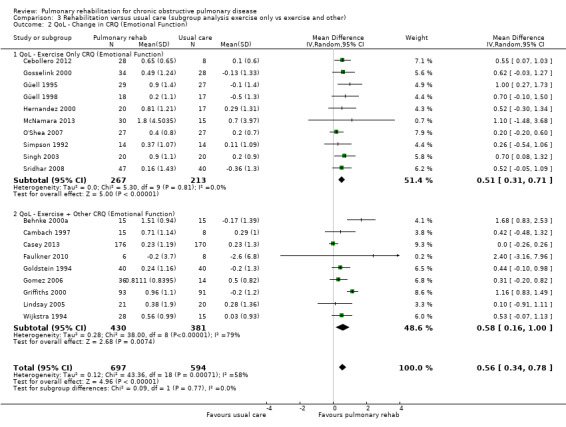
Comparison 3 Rehabilitation versus usual care (subgroup analysis exercise only vs exercise and other), Outcome 2 QoL ‐ Change in CRQ (Emotional Function).
3.3. Analysis.
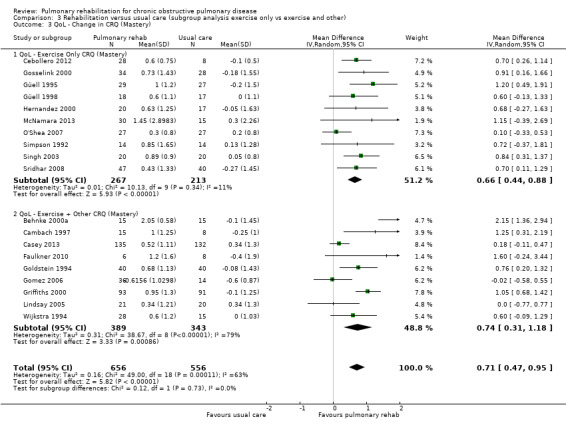
Comparison 3 Rehabilitation versus usual care (subgroup analysis exercise only vs exercise and other), Outcome 3 QoL ‐ Change in CRQ (Mastery).
3.4. Analysis.
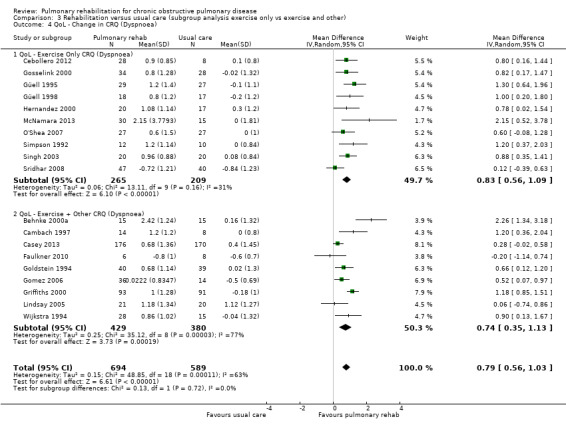
Comparison 3 Rehabilitation versus usual care (subgroup analysis exercise only vs exercise and other), Outcome 4 QoL ‐ Change in CRQ (Dyspnoea).
3.5. Analysis.
Comparison 3 Rehabilitation versus usual care (subgroup analysis exercise only vs exercise and other), Outcome 5 QoL ‐ Change in SGRQ (Total).
3.6. Analysis.
Comparison 3 Rehabilitation versus usual care (subgroup analysis exercise only vs exercise and other), Outcome 6 QoL ‐ Change in SGRQ (Symptoms).
3.7. Analysis.
Comparison 3 Rehabilitation versus usual care (subgroup analysis exercise only vs exercise and other), Outcome 7 QoL ‐ Change in SGRQ (Impacts).
3.8. Analysis.
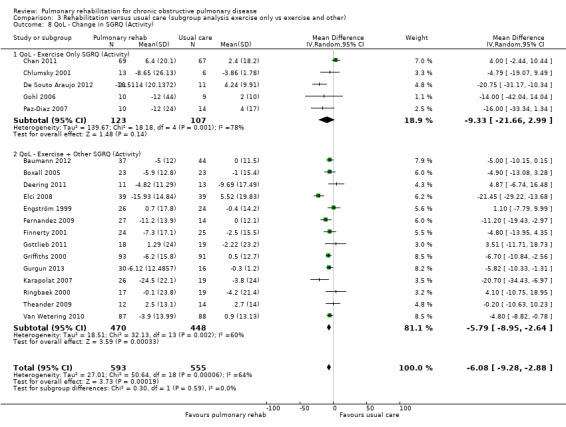
Comparison 3 Rehabilitation versus usual care (subgroup analysis exercise only vs exercise and other), Outcome 8 QoL ‐ Change in SGRQ (Activity).
Please see Table 5 for a summary of results of the subgroup analysis.
4. Summary of subgroup analysis.
| Pulmonary rehabilitation versus usual care. Subgroup: community versus hospital‐delivered programme | |||||
| Outcome | Subscale | Subgroups | Heterogeneity | MD [95% CI] | Test for subgroup differences |
| CRQ | Fatigue | Community | Tau² = 0.10; I² = 52% | 0.44 [0.14, 0.75] | Chi² = 3.98, df = 1 (P value 0.05), I² = 74.9% |
| Hospital | Tau² = 0.09; I² = 51% | 0.86 [0.58, 1.14] | |||
| CRQ | Emotional Function | Community | Tau² = 0.00; I² = 0% | 0.21 [0.04, 0.39] | Chi² = 12.24, df = 1 (P value 0.0005), I² = 91.8% |
| Hospital | Tau² = 0.06; I² = 39% | 0.77 [0.51, 1.03] | |||
| CRQ | Mastery | Community | Tau² = 0.07; I² = 45% | 0.40 [0.12, 0.67] | Chi² = 8.58, df = 1 (P value 0.003), I² = 88.3% |
| Hospital | Tau² = 0.05; I² = 31% | 0.95 [0.70, 1.20] | |||
| CRQ | Dyspnoea | Community | Tau² = 0.03; I² = 26% | 0.58 [0.34, 0.81] | Chi² = 4.05, df = 1 (P value 0.04), I² = 75.3% |
| Hospital | Tau² = 0.17; I² = 60% | 0.99 [0.66, 1.32] | |||
| SGRQ | Total | Community | Tau² = 24.00; I² = 73% | ‐8.15 [‐12.16, ‐4.13] | Chi² = 0.69, df = 1 (P value 0.41), I² = 0% |
| Hospital | Tau² = 6.41; I² = 35% | ‐6.05 [‐8.91, ‐3.20] | |||
| SGRQ | Symptoms | Community | Tau² = 6.28; I² = 24% | ‐3.66 [‐7.07, ‐0.24] | Chi² = 1.65, df = 1 (P value 0.20), I² = 39.2% |
| Hospital | Tau² = 4.96; I² = 15% | ‐6.91 [‐10.51, ‐3.30] | |||
| SGRQ | Impact | Community | Tau² = 19.91; I² = 63% | ‐8.17 [‐12.00, ‐4.34] | Chi² = 0.46, df = 1 (P value 0.50), I² = 0% |
| Hospital | Tau² = 22.39; I² = 58% | ‐6.21 [‐10.33, ‐2.09] | |||
| SGRQ | Activity | Community | Tau² = 48.91; I² = 78% | ‐7.82 [‐13.37, ‐2.28] | Chi² = 0.93, df = 1 (P value 0.33), I² = 0% |
| Hospital | Tau² = 10.45; I² = 36% | ‐4.58 [‐8.16, ‐1.00] | |||
| Pulmonary rehabilitation versus usual care. Subgroup: exercise only programme versus exercise plus additional elements in programme | |||||
| Outcome | Subscale | Subgroups | Heterogeneity | MD [95% CI] | Test for subgroup differences |
| CRQ | Fatigue | Exercise only | Tau² = 0.00; I² = 0% | 0.73 [0.54, 0.92] | Chi² = 0.26, df = 1 (P value 0.61), I² = 0% |
| Exercise + other | Tau² = 0.29; I² = 79% | 0.61 [0.18, 1.03] | |||
| CRQ | Emotional Function | Exercise only | Tau² = 0.00; I² = 0% | 0.51 [0.31, 0.71] | Chi² = 0.09, df = 1 (P value 0.77), I² = 0% |
| Exercise + other | Tau² = 0.28; I² = 79% | 0.58 [0.16, 1.00] | |||
| CRQ | Mastery | Exercise only | Tau² = 0.01; I² = 11% | 0.66 [0.44, 0.88] | Chi² = 0.12, df = 1 (P value 0.73), I² = 0% |
| Exercise + other | Tau² = 0.31; I² = 79% | 0.74 [0.31, 1.18] | |||
| CRQ | Dyspnoea | Exercise only | Tau² = 0.06; I² = 31% | 0.83 [0.56, 1.10] | Chi² = 0.13, df = 1 (P value 0.72), I² = 0% |
| Exercise + other | Tau² = 0.25; I² = 77% | 0.74 [0.35, 1.13] | |||
| SGRQ | Total | Exercise only | Tau² = 62.83; I² = 70% | ‐7.87 [‐16.72, 0.98] | |
| Exercise + other | Tau² = 10.17; I² = 56% | ‐6.76 [‐9.19, ‐4.34] | Chi² = 0.06, df = 1 (P value 0.81), I² = 0% | ||
| SGRQ | Symptoms | Exercise only | Tau² = 0.00; I² = 0% | ‐7.38 [‐12.33, ‐2.44] | |
| Exercise + other | Tau² = 13.88; I² = 41% | ‐4.38 [‐7.62, ‐1.15] | Chi² = 0.99, df = 1 (P value 0.32), I² = 0% | ||
| SGRQ | Impact | Exercise only | Tau² = 33.34; I² = 63% | ‐6.11 [‐12.60, 0.38] | |
| Exercise + other | Tau² = 17.12; I² = 59% | ‐7.61 [‐10.64, ‐4.57] | Chi² = 0.17, df = 1 (P value 0.68), I² = 0% | ||
| SGRQ | Activity | Exercise only | Tau² = 139.67; I² = 78% | ‐9.33 [‐21.66, 2.99] | Chi² = 0.30, df = 1 (P value 0.59), I² = 0% |
| Exercise + other | Tau² = 18.51; I² = 60% | ‐5.79 [‐8.95, ‐2.64] | |||
CRQ: Chronic Respiratory Disease Questionnaire; MD: mean difference; SGRQ: St. George's Respiratory Questionnaire.
Sensitivity analysis
A sensitivity analysis included only studies of high quality (studies for which both allocation concealment and Incomplete outcome data were rated as low risk) (see risk of bias table in Figure 4). Thirteen studies met the criteria for high quality (Boxall 2005; Cambach 1997; Cockcroft 1981; Emery 1998; Engström 1999; Goldstein 1994; Griffiths 2000; Karapolat 2007; Liu 2012; McNamara 2013; O'Shea 2007; Theander 2009; Van Wetering 2010). Effect estimates were consistent with overall summary effect estimates for the two primary outcomes when contributing data were restricted to high‐quality studies, with the exception of one domain, for which the confidence interval widened enough to include the possibility of no difference between rehabilitation and control. All domains for both the CRQ and the SGRQ continued to be statistically significant when restricted to studies of high quality, with the exception of the SGRQ symptoms domain, which was no longer statistically significant (MD ‐4.12, 95% CI ‐8.42 to 0.21;, seven trials; 572 participants; Tau² = 13.82; I² = 46%).
Neither subgroup analyses nor the sensitivity analysis based on quality had any impact on reducing or explaining high levels of heterogeneity.
Discussion
This review summarised 65 studies involving 3822 participants with chronic obstructive pulmonary disease (COPD), 2090 of whom were randomly allocated to some form of exercise rehabilitation for a minimum duration of four weeks, and 1732 individuals randomly assigned to usual care. This is the second update of this review, which was last updated in 2006 (Lacasse 2006). Pulmonary rehabilitation is now accepted within the scientific community as an essential strategy in the ongoing management of people with COPD (GOLD 2014). Development of objective health‐related quality of life (HRQoL) outcome measures (Kirshner 1985) and demonstration of a physiological rationale for exercise training in people with COPD (Casaburi 1991; Maltais 1996) have facilitated this acceptance. Results of the previous version of this meta‐analysis strongly supported pulmonary rehabilitation (PR) in the management of COPD, and results of this current update reconfirm these findings.
Three aspects of the meta‐analysis warrant comment. First, we examined the short‐term effects of PR in COPD, that is, the benefits of rehabilitation found at the completion of a programme. When the original review was undertaken, few investigators were examining the long‐term benefits of rehabilitation (Guell 2000; Ries 1995; Troosters 2000; Wijkstra 1995). More recently, focus on this aspect of PR has increased and exploration of strategies to maintain early benefits continues (Brooks 2002; Foglio 2001; Ries 2003). This review does not attempt to examine these issues. Second, we have been conservative in concluding clear benefit only when the 95% confidence interval (CI) representing the smallest treatment effect was still greater than the minimal clinically important difference (MCID). Third, we excluded a number of well‐conducted studies that have contributed to our understanding of PR, but in which control participants received interventions beyond what was considered conventional care. An example of this is Ries 1995, which was excluded on the grounds that control participants had been given an educational programme. Similarly, several studies in which an intervention such as inspiratory muscle training, psychosocial support or breathing exercises was compared with exercise training were excluded. Only studies in which usual care was directly compared with exercise rehabilitation were included for analysis.
As the care of patients with COPD is largely concerned with treating symptoms (Pauwels 2001), we believe that HRQoL should be considered as the primary outcome in PR. The present meta‐analysis reconfirms the findings of the previous version that PR is effective in relieving dyspnoea and fatigue, and in improving patients' emotional function and control over the disease. The magnitude of the improvement lies beyond the MCID.
In most trials, investigators measured HRQoL by using either the Chronic Respiratory Disease Questionnaire (CRQ) or the St. George's Respiratory Questionnaire (SGRQ). Head‐to‐head comparisons of these questionnaires have been published (Harper 1997; Rutten‐van Mölken 1999). In both studies, analyses of reliability, validity and responsiveness did not clearly favour one instrument above the other. Rutten‐van Mölken and colleagues (Rutten‐van Mölken 1999) suggested that the choice between the CRQ and the SGRQ should be based on other considerations, such as the required sample size. Only one trial included in the meta‐analysis reported results from both the CRQ and the SGRQ (Griffiths 2000), with no clear indication that one questionnaire is more sensitive to change than the other. Therefore, comparisons from this meta‐analysis are only indirect. We found wider 95% CIs around the pooled treatment effect from the SGRQ ‐ a situation that may be explained by the smaller number of participants contributing to this analysis.
Pulmonary rehabilitation programmes included in the meta‐analysis differed in several aspects, including clinical setting, duration and composition. This we believe is responsible for the substantial heterogeneity observed in the results obtained and is in keeping with a recent study by Spruit 2014 and supported by Rochester 2014, who also identified this as an issue requiring further investigation. For instance, the contributions of educational activities and psychological support to exercise training remain uncertain. This information would be of outmost importance to physicians and allied healthcare professionals who prescribe rehabilitation and to those who allocate the resources. We addressed this issue in a systematic overview of the literature (Lacasse 1997). Since the time this review was published, further evidence from randomised controlled trials (RCTs) has been published to better define the type and intensity of exercise (Bernard 1999), as well as the influence of programme components, including patient education and self‐management (Bourbeau 2003), nutritional support (Steiner 2003) and respiratory muscle training (Watson 1997). Sometimes, evidence even took the form of systematic reviews (Ferreira 2012; Lotters 2002; Taylor 2005). Such questions were too specific to be directly addressed in this meta‐analysis, which aimed to investigate the overall effect of rehabilitation in COPD (not the effects of its components). Nevertheless, homogeneity among study results suggested that less sophisticated rehabilitation programmes may also be effective in improving HRQoL, although the between‐study comparison from which this conclusion follows is relatively weak.
Investigators have identified an increase in exercise tolerance and functional activities such as walking as other relevant outcomes of rehabilitation (Fishman 1994; Pauwels 2001). Our current interpretation of the results of the six‐minute walk test (6MWT) analysis differs from that of the previous version of the meta‐analysis (Lacasse 2006). In 2006, results of the meta‐analysis were compared with an MCID of 54 metres (95% CI 37 to 71 metres; Redelmeier 1997). From this comparison, the clinical significance of results obtained from the 2006 meta‐analysis was interpreted as uncertain. Since 2006, several studies have further investigated the issue of the MCID in field walk tests in chronic respiratory disease. Results of these studies have recently been summarised in an important systematic review, which was supported by the European Respiratory and American Thoracic Societies (Holland 2014; Singh 2014). Although variability across studies and methods used to determine the MCID is evident, available evidence suggests that the MCID for the 6MWT lies between 25 and 33 metres (median estimate 30 metres). Results of our meta‐analysis (i.e. MD of 43.93 metres with 95% CI between 36.24 and 55.21 metres) indicate the clinical significance of the effects of PR.
When compared with the treatment effects of other important modalities of care for patients with COPD, such as long‐acting inhaled therapy or oral theophylline and its new derivatives (Kew 2014;Ram 2005), rehabilitation resulted in greater improvement in important domains of HRQoL and functional exercise capacity.
The importance of measures of maximal exercise capacity remains to be defined. An initial test may be useful in assisting with the prescription of an appropriate level of training. Retesting may provide physiological evidence that a training response has occurred and may be useful in adjustment of intensity levels during the programme (Jones 1988). As the results of maximal exercise tests correlate poorly with those of HRQoL measures (Guyatt 1985; Wijkstra 1994a), maximal exercise testing cannot serve as a substitute for such measures when the outcome of a rehabilitation programme is evaluated.
Authors' conclusions
Implications for practice.
Results of this meta‐analysis strongly support pulmonary rehabilitation, including at least four weeks of exercise training, as part of the spectrum of treatment for patients with COPD. We found clinically and statistically significant improvements in important domains of health‐related quality of life, including dyspnoea, fatigue, emotional function and mastery, in addition to the six‐minute walk/distance test ‐ a measure of functional exercise.
Pulmonary rehabilitation has long been underused in patients with COPD (Brooks 2007; Puhan 2011(a); Yohannes 2004). With the support of current international statements or clinical practice guidelines targeting respiratory rehabilitation in COPD (Bolton 2013; Nici 2006; Spruit 2013), we hope that the results of this meta‐analysis will encourage the implementation of new programmes.
Implications for research.
Overall, the conclusions of this meta‐analysis are in agreement with those of prior meta‐analyses published in 1996 and in 2001 (Lacasse 1996; Lacasse 2001). The addition of 34 RCTs since the 2006 update resulted, as expected, in narrowing of the CIs around the common effects of rehabilitation in the outcomes examined. This update continues to support the strong argument that PR is beneficial in improving HRQoL. It also reiterates the view presented in the 2006 update that additional RCTs comparing PR and conventional care in COPD are no longer warranted. However findings of the subgroup analysis undertaken as part of this update do stimulate new questions in relation to PR. The subgroup analysis finding that identified a difference in treatment effect between hospital‐based programmes and community‐based programmes suggests that further research should be undertaken to compare these two approaches. Similarly, the fact that the subgroup analysis identified no differences between basic exercise PR programmes and those that provided more complex interventions suggests the need to examine and identify the most essential components of PR programmes for achieving the best patient outcomes. Other factors that remain uncertain include the degree of supervision, the intensity of the training and how long the treatment effect persists. Recent recommendations provided by current guidelines from the ATS or ACSM that at least three weekly sessions are necessary for a treatment effect raise issues that require consideration beyond this current review. These specific issues demand further elucidation through RCTs and further meta‐analysis.
What's new
| Date | Event | Description |
|---|---|---|
| 21 April 2015 | Amended | Typo in CI for functional exercise capacity in results corrected. |
History
Protocol first published: Issue 1, 1998 Review first published: Issue 1, 2003
| Date | Event | Description |
|---|---|---|
| 26 March 2014 | New citation required and conclusions have changed | New author team Abstract, plain language summary and results redrafted. Inclusion criteria modified and outcomes defined. Methods brought up to date, including use of current Cochrane risk of bias tool. Summary of findings table added Conclusions strengthened through the addition of 35 new studies, and recommendations for future research modified Only assessments completed up to and within 3 months of completion of the intervention included in the analysis Studies that commenced within 4 weeks of an acute exacerbation of COPD excluded, as a separate systematic review examined the effects of pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease (Puhan 2011) Additional subgroup analysis undertaken |
| 26 March 2014 | New search has been performed | New literature search run |
| 20 August 2008 | Amended | Converted to new review format |
| 16 June 2006 | New citation required and conclusions have changed | Substantive amendments made |
Acknowledgements
We acknowledge the authors of the primary studies included in the meta‐analysis, who have kindly provided additional data and information regarding their previous work. We acknowledge the contributions of Eric Wong, Roger Goldstein and Gordon Guyatt, who co‐authored the initial version of this review. We would also like to thank Elizabeth Stovold (CAG Information Specialist) for conducting electronic literature searches, Emma Jackson for assisting with locating papers and Emma Welsh for providing assistance during the editorial process.
Yves Lacasse acknowledges Merck Frosst Canada, who funded a co‐author, Sylvie Martin, to work on a previously published version of the review. At the time, the Cochrane Airways Group did not believe that this funding presented a threat to the validity of the Reviews' findings. Merck Frosst Canada was not otherwise involved in the design or conduct of this meta‐analysis. We also acknowledge Nederlands Astma Fonds, Netherlands for funding for an earlier version of this review. No authors received funding for the 2015 update of the review.
John White was the Editor for this review and commented critically on the review.
The methods section of this review is based on a standard template used by the Cochrane Airways Group.
Appendices
Appendix 1. Archive of previous search methods and results
Search strategy used for review versions published up to 2004
We searched all records in the Cochrane Airways Group Register coded as 'COPD' for original articles published in any language using the following strategy: rehabilitat* or fitness* or exercis* or physical* or train*
In the first version of this review (Lacasse 1996), 522 publications were retrieved from the computerised search. The review authors reduced this list to 68 potentially eligible papers (quadratic weighted Kappa 0.53, 95% CI 0.45 to 0.61) that were assessed in detail. From this study list, 47 were excluded as the result of wrong population studies (n = 4), intervention not meeting the definition of rehabilitation (n = 7), control group not receiving conventional community care (n = 29), trials not randomised (n = 7). Both primary review authors agreed to include 17 papers in the meta‐analysis (quadratic Kappa 0.89, 95% CI 0.65 to 1.00). Six of the 14 RCTs included in the original meta‐analysis (Lacasse 1996) were not uncovered by this literature search. Therefore, a total of 23 randomised controlled trials were included. This represents an addition of nine RCTs to the meta‐analysis published in 1996 (Lacasse 1996). We contacted the authors of these trials for any additional information required; response rate was 91% (21/23).
An updated search for the review was undertaken in October 2004, which identified an additional 998 references. These were filtered to a list of 139 references, which were considered in the update of the review. Of these, 93 studies failed to meet the inclusion criteria. The original version of the review as previously indicated had included 23 trials. From the updated search (2004), eight additional RCTs (represented by 17 references) met the inclusion criteria of the review (Behnke 2000a; Boxall 2005; Casaburi 2004; Chlumsky 2001; Finnerty 2001; Güell 1998; Singh 2003; Xie 2003). Six papers were awaiting assessment (Corrado 1995: published as conference abstract; Fernández 1998: paper not available; Shu 1998: published as conference abstract; Tregonning 2000: published as conference abstract; Ward 1999: published as conference abstract; Wright 2002: unclear study methods). One trial was ongoing (Whiteford 2004). As an outcome of the update in 2004, a total of 31 RCTs (represented by 65 references) contributed to the meta‐analysis.
Appendix 2. Sources and search methods for the Cochrane Airways Group Specialised Register (CAGR)
Electronic searches: core databases
| Database | Frequency of search |
| CENTRAL | Monthly |
| MEDLINE (Ovid) | Weekly |
| EMBASE (Ovid) | Weekly |
| PsycINFO (Ovid) | Monthly |
| CINAHL (EBSCO) | Monthly |
| AMED (EBSCO) | Monthly |
Handsearches: core respiratory conference abstracts
| Conference | Years searched |
| American Academy of Allergy, Asthma and Immunology (AAAAI) | 2001 onwards |
| American Thoracic Society (ATS) | 2001 onwards |
| Asia Pacific Society of Respirology (APSR) | 2004 onwards |
| British Thoracic Society Winter Meeting (BTS) | 2000 onwards |
| Chest Meeting | 2003 onwards |
| European Respiratory Society (ERS) | 1992, 1994, 2000 onwards |
| International Primary Care Respiratory Group Congress (IPCRG) | 2002 onwards |
| Thoracic Society of Australia and New Zealand (TSANZ) | 1999 onwards |
MEDLINE search strategy used to identify trials for the CAGR
COPD search
1. Lung Diseases, Obstructive/
2. exp Pulmonary Disease, Chronic Obstructive/
3. emphysema$.mp.
4. (chronic$ adj3 bronchiti$).mp.
5. (obstruct$ adj3 (pulmonary or lung$ or airway$ or airflow$ or bronch$ or respirat$)).mp.
6. COPD.mp.
7. COAD.mp.
8. COBD.mp.
9. AECB.mp.
10. or/1‐9
Filter to identify RCTs
1. exp "clinical trial [publication type]"/
2. (randomised or randomised).ab,ti.
3. placebo.ab,ti.
4. dt.fs.
5. randomly.ab,ti.
6. trial.ab,ti.
7. groups.ab,ti.
8. or/1‐7
9. Animals/
10. Humans/
11. 9 not (9 and 10)
12. 8 not 11
The MEDLINE strategy and RCT filter are adapted to identify trials in other electronic databases
Appendix 3. Search strategy to identify relevant trials from the CAGR
#1 MeSH DESCRIPTOR Pulmonary Disease, Chronic Obstructive Explode All
#2 MeSH DESCRIPTOR Bronchitis, Chronic
#3 (obstruct*) near3 (pulmonary or lung* or airway* or airflow* or bronch* or respirat*)
#4 COPD:MISC1
#5 (COPD OR COAD OR COBD):TI,AB,KW
#6 #1 OR #2 OR #3 OR #4 OR #5
#7 MeSH DESCRIPTOR Rehabilitation
#8 MeSH DESCRIPTOR Respiratory Therapy
#9 rehabilitat*
#10 fitness*
#11 exercis*
#12 train*
#13 #7 or #8 or #9 or #10 or #11 or #12
#14 #6 and #13
[Note: in search line #4, MISC1 denotes the field in which the reference has been coded for condition, in this case, COPD]
Appendix 4. Exclusion criteria used to sort and categorise references
| Exclusion criteria |
| Less than 90% of participants have a diagnosis of COPD |
| Not a programme, or programme does NOT contain any exercise component |
| Has an exercise component but is NOT aerobically demanding |
| Programme of less than 4 weeks' duration |
| Control received more than conventional care |
| Includes ventilated patients (hospital ventilated) |
| Within 4 weeks post exacerbation |
| This citation linked to main study paper already being screened |
| Duplicate citation (identical to a citation previously included) |
| The intervention is a medication |
Appendix 5. Eligibility classification allocated to studies
| Classification | Action |
| Excluded | Study excluded |
| Important article but not to be included in review | Study excluded |
| Included but needs translation | Study included and proceeds to next stage |
| Included | Study included and proceeds to next stage |
| More information needed before inclusion decision | Awaiting additional information before study proceeds |
Appendix 6. Risk of bias domains and judgements
Sequence generation (possible selection bias)
A detailed description of the methods used to generate the allocation sequence was developed for each study to facilitate an assessment of whether it should produce comparable groups.
Risk of bias for sequence generation was graded based on the following:
low risk (any truly random process, e.g. random number table; computer random number generator);
high risk (any non‐random process, e.g. odd or even date of birth; hospital or clinic record number); or
unclear risk.
Allocation concealment (possible selection bias)
A description of the methods used to conceal the allocation sequence for each study was presented, and this determined whether the intervention allocation might have been anticipated in advance of, or during, recruitment, or changed after assignment.
Risk of bias associated with allocation concealment was graded as follows:
low risk (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes);
high risk (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth); or
unclear risk.
Blinding of participants and personnel (possible performance bias)
The nature of the interventions involved in pulmonary rehabilitation would make it highly unlikely or impossible to blind participants or personnel delivering the interventions.
However, it would be possible to blind outcome assessors. Therefore, we assessed the risk of bias for blinding of outcome assessors as:
high risk;
low risk; or
unclear risk.
Blinding of outcome assessment (checking for possible detection bias)
We will describe for each included study the methods used, if any, to blind outcome assessors from knowledge
of which intervention participants received. We will assess the risk of bias for blinding of outcome assessment as:
low risk;
high risk; or
unclear risk.
Incomplete outcome data (possible attrition bias associated with withdrawals, drop‐outs, deviations from original protocol)
A description of completeness of data for each outcome at all stages of the study was presented. This included examining attrition and exclusions from the analysis. Each study was examined to identify whether attrition and exclusions were reported (comparing the numbers presented at each stage with the total number of randomised participants). The studies were also examined for rationale and justifications explaining any attrition or exclusions. In instances where enough information could be identified or was obtained from the trial authors, we re‐included missing data in the analyses. We assessed the risk of bias for completeness of data as follows:
low risk (20% or less missing data);
high risk (more than 20% missing data); or
unclear risk.
Selective reporting bias
Studies were examined for selective outcome reporting bias by cross‐checking that all outcomes identified in the methods section of the results publication were reported in the results section of the trial publication(s).
The risk of bias for selective reporting was graded as follows:
high risk (where not all of the study’s prespecified outcomes had been reported; one or more reported primary outcomes were not prespecified; outcomes of interest were reported incompletely and so cannot be used; study failed to include results of a key outcome that would have been expected to have been reported);
low risk (where it was clear that all of the study’s prespecified outcomes and all expected outcomes of interest to the review have been reported); or
unclear risk.
Other sources of bias (bias due to problems not covered by the items above)
If the review authors believed that any other possible sources of bias were matters of concern, these were recorded.
The level at which studies were seen to be free of other problems that could put them at risk of bias was graded as:
low risk;
high risk; or
unclear risk.
Overall risk of bias
An overall judgement was made in relation to whether studies were at high risk of bias, according to the criteria given in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011) and identified above. The magnitude of the overall bias, along with the degree to which the bias was likely to have impacted the findings, was assessed for each study using the following grades:
low risk;
high risk; or
unclear risk.
Data and analyses
Comparison 1. Rehabilitation versus usual care.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 QoL ‐ Change in CRQ (Fatigue) | 19 | 1291 | Mean Difference (IV, Random, 95% CI) | 0.68 [0.45, 0.92] |
| 2 QoL ‐ Change in CRQ (Emotional Function) | 19 | 1291 | Mean Difference (IV, Random, 95% CI) | 0.56 [0.34, 0.78] |
| 3 QoL ‐ Change in CRQ (Mastery) | 19 | 1212 | Mean Difference (IV, Random, 95% CI) | 0.71 [0.47, 0.95] |
| 4 QoL ‐ Change in CRQ (Dyspnoea) | 19 | 1283 | Mean Difference (IV, Random, 95% CI) | 0.79 [0.56, 1.03] |
| 5 QoL ‐ Change in SGRQ (Total) | 19 | 1146 | Mean Difference (IV, Random, 95% CI) | ‐6.89 [‐9.26, ‐4.52] |
| 6 QoL ‐ Change in SGRQ (Symptoms) | 19 | 1153 | Mean Difference (IV, Random, 95% CI) | ‐5.09 [‐7.69, ‐2.49] |
| 7 QoL ‐ Change in SGRQ (Impacts) | 19 | 1149 | Mean Difference (IV, Random, 95% CI) | ‐7.23 [‐9.91, ‐4.55] |
| 8 QoL ‐ Change in SGRQ (Activity) | 19 | 1148 | Mean Difference (IV, Random, 95% CI) | ‐6.08 [‐9.28, ‐2.88] |
| 9 Maximal Exercise (Incremental shuttle walk test) | 8 | 694 | Mean Difference (IV, Random, 95% CI) | 39.77 [22.38, 57.15] |
| 10 Maximal Exercise Capacity (cycle ergometer) | 16 | 779 | Mean Difference (IV, Random, 95% CI) | 6.77 [1.89, 11.65] |
| 11 Functional Exercise Capacity (6MWT)) | 38 | 1879 | Mean Difference (IV, Random, 95% CI) | 43.93 [32.64, 55.21] |
1.9. Analysis.
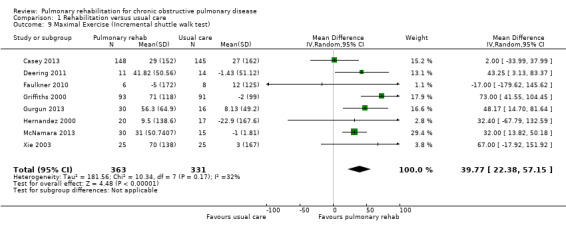
Comparison 1 Rehabilitation versus usual care, Outcome 9 Maximal Exercise (Incremental shuttle walk test).
Comparison 2. Rehabilitation versus usual care (subgroup analysis hospital vs community).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 QoL ‐ Change in CRQ (Fatigue) | 19 | 1291 | Mean Difference (IV, Random, 95% CI) | 0.68 [0.45, 0.92] |
| 1.1 QoL ‐ Community CRQ (Fatigue) | 9 | 648 | Mean Difference (IV, Random, 95% CI) | 0.44 [0.14, 0.75] |
| 1.2 QoL ‐ Hospital CRQ (Fatigue) | 10 | 643 | Mean Difference (IV, Random, 95% CI) | 0.86 [0.58, 1.14] |
| 2 QoL ‐ Change in CRQ (Emotional Function) | 19 | 1291 | Mean Difference (IV, Random, 95% CI) | 0.56 [0.34, 0.78] |
| 2.1 QoL ‐ Community (Emotional Function) | 9 | 648 | Mean Difference (IV, Random, 95% CI) | 0.21 [0.04, 0.39] |
| 2.2 QoL ‐ Hospital CRQ (Emotional Function) | 10 | 643 | Mean Difference (IV, Random, 95% CI) | 0.77 [0.51, 1.03] |
| 3 QoL ‐ Change in CRQ (Mastery) | 19 | 1212 | Mean Difference (IV, Random, 95% CI) | 0.71 [0.47, 0.95] |
| 3.1 QoL ‐ Community CRQ (Mastery) | 9 | 569 | Mean Difference (IV, Random, 95% CI) | 0.40 [0.12, 0.67] |
| 3.2 QoL ‐ Hospital CRQ (Mastery) | 10 | 643 | Mean Difference (IV, Random, 95% CI) | 0.95 [0.70, 1.20] |
| 4 QoL ‐ Change in CRQ (Dyspnoea) | 19 | 1283 | Mean Difference (IV, Random, 95% CI) | 0.82 [0.59, 1.05] |
| 4.1 QoL ‐ Community Based CRQ (Dyspnoea) | 8 | 633 | Mean Difference (IV, Random, 95% CI) | 0.58 [0.34, 0.81] |
| 4.2 QoL ‐ Hospital Based CRQ (Dyspnoea) | 11 | 650 | Mean Difference (IV, Random, 95% CI) | 0.99 [0.66, 1.32] |
| 5 QoL ‐ Change in SGRQ (Total) | 19 | 1146 | Mean Difference (IV, Random, 95% CI) | ‐6.89 [‐9.26, ‐4.52] |
| 5.1 QoL ‐ Community in SGRQ (Total) | 9 | 643 | Mean Difference (IV, Random, 95% CI) | ‐8.15 [‐12.16, ‐4.13] |
| 5.2 QoL ‐ Hospital SGRQ (Total) | 10 | 503 | Mean Difference (IV, Random, 95% CI) | ‐6.05 [‐8.91, ‐3.20] |
| 6 QoL ‐ Change in SGRQ (Symptoms) | 19 | 1153 | Mean Difference (IV, Random, 95% CI) | ‐5.09 [‐7.69, ‐2.49] |
| 6.1 QoL ‐ Community SGRQ (Symptoms) | 9 | 649 | Mean Difference (IV, Random, 95% CI) | ‐3.66 [‐7.07, ‐0.24] |
| 6.2 QoL ‐ Hospital SGRQ (Symptoms) | 10 | 504 | Mean Difference (IV, Random, 95% CI) | ‐6.91 [‐10.51, ‐3.30] |
| 7 QoL ‐ Change in SGRQ (Impacts) | 19 | 1149 | Mean Difference (IV, Random, 95% CI) | ‐7.23 [‐9.91, ‐4.55] |
| 7.1 QoL ‐ Community SGRQ (Impacts) | 9 | 646 | Mean Difference (IV, Random, 95% CI) | ‐8.17 [‐10.00, ‐4.34] |
| 7.2 QoL ‐ Hospital SGRQ (Impacts) | 10 | 503 | Mean Difference (IV, Random, 95% CI) | ‐6.21 [‐10.33, ‐2.09] |
| 8 QoL ‐ Change in SGRQ (Activity) | 19 | 1148 | Mean Difference (IV, Random, 95% CI) | ‐6.08 [‐9.28, ‐2.88] |
| 8.1 QoL ‐ Community SGRQ (Activity) | 9 | 645 | Mean Difference (IV, Random, 95% CI) | ‐7.82 [‐13.37, ‐2.28] |
| 8.2 QoL ‐ Hospital SGRQ (Activity) | 10 | 503 | Mean Difference (IV, Random, 95% CI) | ‐4.58 [‐8.16, 1.00] |
Comparison 3. Rehabilitation versus usual care (subgroup analysis exercise only vs exercise and other).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 QoL ‐ Change in CRQ (Fatigue) | 19 | 1291 | Mean Difference (IV, Random, 95% CI) | 0.68 [0.45, 0.92] |
| 1.1 QoL ‐ Exercise Only CRQ (Fatigue) | 10 | 480 | Mean Difference (IV, Random, 95% CI) | 0.73 [0.54, 0.92] |
| 1.2 QoL ‐ Exercise + Other CRQ (Fatigue) | 9 | 811 | Mean Difference (IV, Random, 95% CI) | 0.61 [0.18, 1.03] |
| 2 QoL ‐ Change in CRQ (Emotional Function) | 19 | 1291 | Mean Difference (IV, Random, 95% CI) | 0.56 [0.34, 0.78] |
| 2.1 QoL ‐ Exercise Only CRQ (Emotional Function) | 10 | 480 | Mean Difference (IV, Random, 95% CI) | 0.51 [0.31, 0.71] |
| 2.2 QoL ‐ Exercise + Other CRQ (Emotional Function) | 9 | 811 | Mean Difference (IV, Random, 95% CI) | 0.58 [0.16, 1.00] |
| 3 QoL ‐ Change in CRQ (Mastery) | 19 | 1212 | Mean Difference (IV, Random, 95% CI) | 0.71 [0.47, 0.95] |
| 3.1 QoL ‐ Exercise Only CRQ (Mastery) | 10 | 480 | Mean Difference (IV, Random, 95% CI) | 0.66 [0.44, 0.88] |
| 3.2 QoL ‐ Exercise + Other CRQ (Mastery) | 9 | 732 | Mean Difference (IV, Random, 95% CI) | 0.74 [0.31, 1.18] |
| 4 QoL ‐ Change in CRQ (Dyspnoea) | 19 | 1283 | Mean Difference (IV, Random, 95% CI) | 0.79 [0.56, 1.03] |
| 4.1 QoL ‐ Exercise Only CRQ (Dyspnoea) | 10 | 474 | Mean Difference (IV, Random, 95% CI) | 0.83 [0.56, 1.09] |
| 4.2 QoL ‐ Exercise + Other CRQ (Dyspnoea) | 9 | 809 | Mean Difference (IV, Random, 95% CI) | 0.74 [0.35, 1.13] |
| 5 QoL ‐ Change in SGRQ (Total) | 19 | 1146 | Mean Difference (IV, Random, 95% CI) | ‐6.89 [‐9.26, ‐4.52] |
| 5.1 QoL Exercise Only SGRQ (Total) | 5 | 230 | Mean Difference (IV, Random, 95% CI) | ‐7.87 [‐16.72, 0.98] |
| 5.2 QoL Exercise + Other SGRQ (Total) | 14 | 916 | Mean Difference (IV, Random, 95% CI) | ‐6.76 [‐9.19, ‐4.34] |
| 6 QoL ‐ Change in SGRQ (Symptoms) | 19 | 1153 | Mean Difference (IV, Random, 95% CI) | ‐5.09 [‐7.69, ‐2.49] |
| 6.1 QoL ‐ Exercise Only SGRQ (Symptoms) | 5 | 230 | Mean Difference (IV, Random, 95% CI) | ‐7.38 [‐12.33, ‐2.44] |
| 6.2 QoL ‐ Exercise + Other SGRQ (Symptoms) | 14 | 923 | Mean Difference (IV, Random, 95% CI) | ‐4.38 [‐7.62, ‐1.15] |
| 7 QoL ‐ Change in SGRQ (Impacts) | 19 | 1149 | Mean Difference (IV, Random, 95% CI) | ‐7.23 [‐9.91, ‐4.55] |
| 7.1 QoL ‐ Exercise Only SGRQ (Impacts) | 5 | 230 | Mean Difference (IV, Random, 95% CI) | ‐6.11 [‐12.60, 0.38] |
| 7.2 QoL ‐ Exercise + Other SGRQ (Impacts) | 14 | 919 | Mean Difference (IV, Random, 95% CI) | ‐7.61 [‐10.64, ‐4.57] |
| 8 QoL ‐ Change in SGRQ (Activity) | 19 | 1148 | Mean Difference (IV, Random, 95% CI) | ‐6.08 [‐9.28, ‐2.88] |
| 8.1 QoL ‐ Exercise Only SGRQ (Activity) | 5 | 230 | Mean Difference (IV, Random, 95% CI) | ‐9.33 [‐21.66, 2.99] |
| 8.2 QoL ‐ Exercise + Other SGRQ (Activity) | 14 | 918 | Mean Difference (IV, Random, 95% CI) | ‐5.79 [‐8.95, ‐2.64] |
Comparison 4. Rehabilitation versus usual care (sensitivity analysis by allocation concealment and incomplete outcome).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 QoL ‐ Change in CRQ (Dyspnoea) | 5 | 384 | Mean Difference (IV, Random, 95% CI) | 0.99 [0.64, 1.34] |
| 1.1 QoL ‐ Low Risk CRQ (Dyspnoea) | 5 | 384 | Mean Difference (IV, Random, 95% CI) | 0.99 [0.64, 1.34] |
| 2 QoL ‐ Change in CRQ (Emotional Function) | 5 | 386 | Mean Difference (IV, Random, 95% CI) | 0.60 [0.09, 1.11] |
| 2.1 QoL ‐ Low Risk (Emotional Function) | 5 | 386 | Mean Difference (IV, Random, 95% CI) | 0.60 [0.09, 1.11] |
| 3 QoL ‐ Low Risk CRQ (Fatigue) | 5 | 386 | Mean Difference (IV, Random, 95% CI) | 0.90 [0.41, 1.39] |
| 4 QoL ‐ Low Risk CRQ (Mastery) | 5 | 386 | Mean Difference (IV, Random, 95% CI) | 0.77 [0.28, 1.26] |
| 5 QoL ‐ Low Risk SGRQ (Total) | 7 | 572 | Mean Difference (IV, Random, 95% CI) | ‐5.15 [‐7.95, ‐2.36] |
| 6 QoL ‐ Low Risk SGRQ (Symptoms) | 7 | 572 | Mean Difference (IV, Random, 95% CI) | ‐4.12 [‐8.45, 0.21] |
| 7 QoL ‐ Low Risk SGRQ (Impacts) | 7 | 572 | Mean Difference (IV, Random, 95% CI) | ‐5.92 [‐10.01, ‐1.82] |
| 8 QoL ‐ Low Risk SGRQ (Activity) | 7 | 572 | Mean Difference (IV, Random, 95% CI) | ‐5.33 [‐8.10, ‐2.57] |
4.1. Analysis.
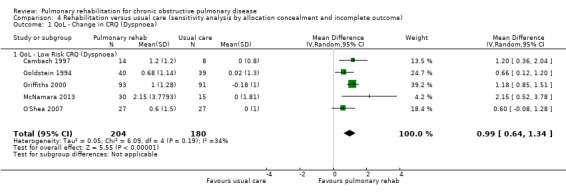
Comparison 4 Rehabilitation versus usual care (sensitivity analysis by allocation concealment and incomplete outcome), Outcome 1 QoL ‐ Change in CRQ (Dyspnoea).
4.2. Analysis.
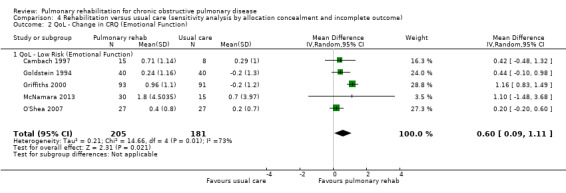
Comparison 4 Rehabilitation versus usual care (sensitivity analysis by allocation concealment and incomplete outcome), Outcome 2 QoL ‐ Change in CRQ (Emotional Function).
4.3. Analysis.
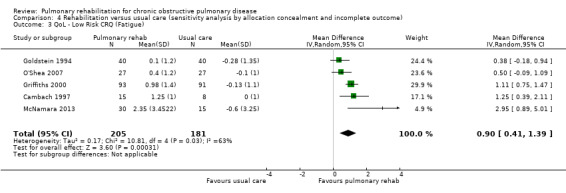
Comparison 4 Rehabilitation versus usual care (sensitivity analysis by allocation concealment and incomplete outcome), Outcome 3 QoL ‐ Low Risk CRQ (Fatigue).
4.4. Analysis.

Comparison 4 Rehabilitation versus usual care (sensitivity analysis by allocation concealment and incomplete outcome), Outcome 4 QoL ‐ Low Risk CRQ (Mastery).
4.5. Analysis.
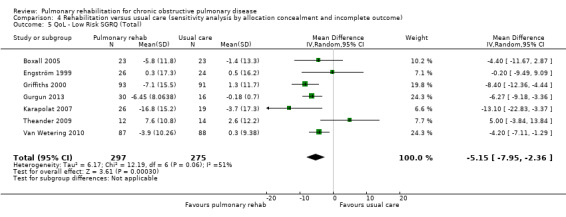
Comparison 4 Rehabilitation versus usual care (sensitivity analysis by allocation concealment and incomplete outcome), Outcome 5 QoL ‐ Low Risk SGRQ (Total).
4.6. Analysis.
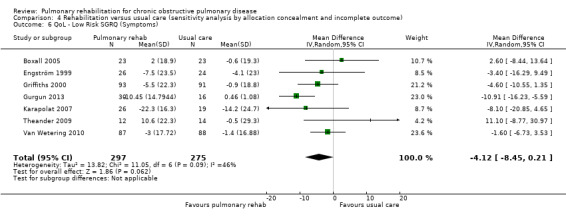
Comparison 4 Rehabilitation versus usual care (sensitivity analysis by allocation concealment and incomplete outcome), Outcome 6 QoL ‐ Low Risk SGRQ (Symptoms).
4.7. Analysis.
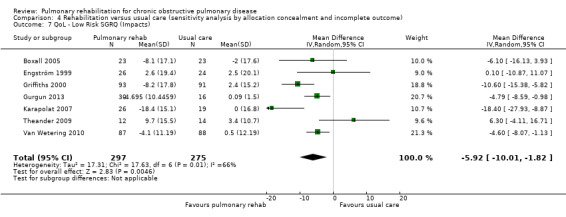
Comparison 4 Rehabilitation versus usual care (sensitivity analysis by allocation concealment and incomplete outcome), Outcome 7 QoL ‐ Low Risk SGRQ (Impacts).
4.8. Analysis.
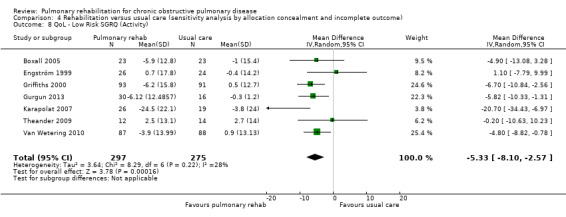
Comparison 4 Rehabilitation versus usual care (sensitivity analysis by allocation concealment and incomplete outcome), Outcome 8 QoL ‐ Low Risk SGRQ (Activity).
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Barakat 2008.
| Methods |
Study design: RCT "Randomization was in blocks of 10, using random numbers" (pg 157) |
|
| Participants |
Setting: out‐patients in France Inclusion criteria:
Exclusion criteria:
Participant status: Age, years: RG: 63.7; CG: 65.9 Gender (M/F): 67/13 FEV1 % predicted: RG: 41.9; CG: 43.3 Participants randomly assigned: Randomised: 80 Analysed Rehab: 35 Control: 36 |
|
| Interventions |
Pulmonary rehabilitation: Out‐patient‐based rehabilitation ULE, LLE, Edu Duration: 14‐Week programme |
|
| Outcomes |
Assessed: baseline and 14 weeks Spirometry, SGRQ, 6MWT, Bode Index |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomization was in blocks of 10, using random numbers" (pg 157) |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | The nature of the intervention made it impossible to blind participants to their allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "All tests including SGRQ outcome assessment [were] blinded" (pg 150) "All of these tests were supervised by a blinded observer, who subsequently repeated this assessment before the study and at the end of the study (0 and 14 weeks)" (pg 156) |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Commenced: 80; completed: 71; attrition: 11.25% |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None noted |
Baumann 2012.
| Methods | Study design: prospective, randomised, controlled, interventional, multi‐centre trial | |
| Participants |
Setting: Hamburg metropolitan area, multi‐centre trial Inclusion criteria:
Exclusion criteria:
Participant status: Age, years: RG: 65; CG: 63 Gender (M/F): 47/34 FEV1 % predicted: RG: 45; CG:47 Participants randomly assigned: Randomised: 100 Analysed Rehab: 37 Control: 44 |
|
| Interventions |
Pulmonary rehabilitation: Out‐patient (hospital based) Aerobic exercise, ULE, LLE Edu, peer support Duration: 8 sessions of 20 minutes and 18 sessions of 60 minutes Usual care: Standard care consisted of referral back to the participant’s pulmonologist following baseline assessments. The control group did not take part in any components of the rehabilitation programme |
|
| Outcomes |
Assessed: baseline and 6 months 6‐Minute walk test (6MWT) Cycle ergometry Short Form‐12 (SF‐12), SGRQ |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomisation was performed using a computer‐generated list of random numbers to assign participants to either training or standard care" (pg 3) |
| Allocation concealment (selection bias) | High risk | "Consecutive patients with COPD according to accepted criteria [5] were recruited" (pg 3) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | "Due to the nature of the intervention it was not possible to blind subjects to their allocation (pg 2) |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Those supervising the 6MWT were not blinded, whereas those supervising cycle ergometry were blinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Commenced: 42; completed: 32; attrition: 10 (24%) |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None noted |
Behnke 2000a.
| Methods | Study design: RCT | |
| Participants |
Setting: work undertaken in Germany Inclusion criteria:
Exclusion criteria:
Participant status: Age, (years± SD): RG: 64.0 ± 1.9; CG: 68.0 ± 2.2 Gender (M/F): RG: 12/3; CG: 11/4 FEV1 % predicted (± SD): RG: 34.1 ± 7.4; 37.5 ± 6.6 Participants randomly assigned: In‐patient and home‐based Randomised: 46 Analysed Rehab: 15 Control: 15 |
|
| Interventions |
Pulmonary rehabilitation: acute hospital admission followed by home exercise programme for 6 months LLE, Edu, Psy Duration: 24 weeks Usual care: Control participants were advised to perform exercise but without special instructions |
|
| Outcomes |
Assessment: baseline and 3, 6 months 6MWT, CRQ |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was in blocks of 10, using random numbers (from study authors) |
| Allocation concealment (selection bias) | Low risk | Randomisation process: sealed envelopes (from study authors) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the programme knew the allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Does not provide information on blinding of assessors, other than that main researcher undertook assessments "the questionnaire was administered as a structured interview, and all interviews were performed by the same investigator (M.B.)" (pg 11867) |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Commenced :46; completed: 30; attrition:16 (35%) |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None reported |
Bendstrup 1997.
| Methods | Study design: RCT | |
| Participants |
Setting: Patients came for out‐patient rehabilitation to a hospital in Denmark Inclusion criteria:
Exclusion criteria:
Participant status: Age, (years ± SD): RG: 64 ± 3; CG: 65 ± 2 Gender (M/F): RG: 7/9; CG: 7/9 Participants randomly assigned: Randomised: 42 Analysed Rehab: 16 Control: 16 |
|
| Interventions |
Pulmonary rehabilitation: out‐patient LLE, ULE, IMT Duration: 12 weeks Control: Stated that care was provided by primary physician |
|
| Outcomes |
Assessment: baseline and 12 weeks 6MWT, CRQ, activities of daily living, York QLQ |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided other than this: "The patients were randomly allocated to either an intervention or a control group" |
| Allocation concealment (selection bias) | Unclear risk | Information not available |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the programme knew the allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No information was provided in relation to blinding of those carrying out outcome assessments |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Commenced: 42; completed: 32; attrition: 10 (24%) |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None noted |
Booker 1984.
| Methods | Study design: RCT | |
| Participants |
Setting: home‐based UK study in London Inclusion criteria:
Exclusion criteria:
Participant status: Age, (years±SD) : RG: 66± 8; CG: 65 ± 7 Gender: not available Participants randomly assigned: Randomised: 69 Analysed Rehab: 32 Control: 37 |
|
| Interventions |
Pulmonary rehabilitation: LLE, BE, PD, Edu, Psy Duration: 9 weeks |
|
| Outcomes |
Assessment: baseline and 3, 6, 12 months 6MWT, DSSI/SAD, daily activity questionnaire |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: coin toss |
| Allocation concealment (selection bias) | Low risk | Study investigators unaware as to order of treatment group assignment |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the programme knew the allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All assessments were carried out by independent assessors who were unaware of the treatment received by each participant ‐ "double‐blind" (pg 258) |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Commenced: 128; completed: 94 (73%); attrition: 27% |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None noted |
Borghi‐Silva 2009.
| Methods | Study design: prospective randomised controlled trial | |
| Participants |
Setting: Brazil Inclusion criteria:
Exclusion criteria:
Participant status: Age (years): RG: 67 ±10; CG: 67 ± 10 Gender (M/F): RG: 13/7; CG: 12/8 FEV1 % predicted (± SD): RG: 64 ± 16; CG: 64 ± 18 Participants randomly assigned: Randomised: 40 Analysed: Rehab: 20 Control: 20 |
|
| Interventions |
Pulmonary rehabilitation: Out‐patient (hospital‐based) supervised training programme Aerobic exercise, ULE, LLE Duration: 6‐week programme Usual care |
|
| Outcomes |
Assessed: baseline and 6 weeks 6‐Minute walk ReR intervals |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information available |
| Allocation concealment (selection bias) | Unclear risk | No information available |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Unable to blind because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No information available |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Commenced: 40; completed: 34; attrition: 6 (15%) |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Unclear risk | None noted |
Boxall 2005.
| Methods | Study design: RCT | |
| Participants |
Setting: home‐based PR programme in Australia Inclusion criteria:
Exclusion criteria:
Participant status: Gender (M/F): RG: 11/12; CG: 15/8 Age (years±SD): RG: 77.6 ±7.6; CG: 75.8 ±8.1 FEV1 % predicted (± SD): RG: 40.5 ±15.9; CG: 37.7 ±15.0 FEV1/FVC % predicted (± SD): RG: 74.4 ± 21.3; CG: 70.4 ± 19.2 Participants randomly assigned: Randomised: 60 Analysed: Rehab: 23 Control: 23 |
|
| Interventions |
Pulmonary rehabilitation: supervised home‐based ULE, LLE, Edu Duration: 12 weeks Usual care: Control phase: Participants received no treatment in addition to usual medical care |
|
| Outcomes |
Assessed: baseline and 12 weeks 6MWT, SGRQ, dyspnoea |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "computer‐generated random numbers that were coded into opaque envelopes by a person independent from the study, they retained the envelopes until initial assessment was completed" (pg 380) |
| Allocation concealment (selection bias) | Low risk | Study investigators unaware as to order of treatment group: "computer‐generated random numbers that were coded into opaque envelopes by a person independent from the study, they retained the envelopes until initial assessment was completed" (pg 380) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | "Neither assessors nor participants were blinded to group assignment in this study" (pg 380) |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | "Neither assessors nor participants were blinded to group assignment in this study" (pg 380) |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Commenced: 60; completed: 46 (76.7%); attrition: 23.3% |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | High risk | "Had to live locally might bias the sample selection and be motivated to exercised daily" (pg 379) |
Busch 1988.
| Methods | Study design: RCT stratified in a random manner | |
| Participants |
Setting: home‐based; Saskatchewan, Canada Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 65 ±16; CG: 66 ±16 Gender (M/F): RG: 5/2; CG: 6/1 FEV1 (± SD): RG: 26% ± 9; CG: 27% ±11 Participants randomly assigned: Randomised: 14 Analysed: Rehab: 6 Control: 6 |
|
| Interventions |
Pulmonary rehabilitation: LLE, BE Duration: 18 weeks Usual care: Control group visited but did not follow the exercise programme |
|
| Outcomes |
Assessment: baseline and at 18 weeks CRQ (dyspnoea only), ICET, multi‐step stage test |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Letter received from study author: used a table of random numbers |
| Allocation concealment (selection bias) | Low risk | Study investigators unaware as to order of treatment group assignment |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Both participants and those delivering the intervention were aware of those allocated to the intervention group |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | “The testers did not know whether the patients were assigned to the Exercise Group or the Control Group" (pg 470) |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Commenced: 20; completed: 14; attrition: 6 (30%) |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Unclear risk | None noted |
Cambach 1997.
| Methods | Study design: RCT | |
| Participants |
Setting: 8 community‐based local physiotherapy practices in The Netherlands Inclusion criteria:
Exclusion criteria:
Participant status: Age, (years± SD): RG: 62 ± 5; CG: 62 ± 9 Gender (M/F): RG: 7/8; CG: 6/2 FEV1 % predicted (± SD): RG: 59% ± 16; CG: 60% ± 23 Participants randomly assigned: Randomised: 99 Analysed: Rehab: 15 Control: 8 |
|
| Interventions |
Pulmonary rehabilitation: community based LLE, ULE, Edu, IMT Duration: 12 weeks. (3 days a week for 90 minutes) Usual care: medication management only |
|
| Outcomes |
Assessment: baseline, 3 months 6MWT, CRQ, ICET |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Within each physiotherapy practice, four out of eight patients were randomly allocated to group RC, and four patients to group CR (block randomisation procedure; four closed envelopes for condition RC and four closed envelopes for condition CR) Baseline assessments were carried out prior to randomisation" (pg 105) |
| Allocation concealment (selection bias) | Low risk | Study investigators unaware as to order of treatment group assignment "four closed envelopes for condition RC and four closed envelopes for condition CR" (pg 105) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Both participants and those delivering the intervention were aware of those allocated to the intervention group |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcome assessments: not blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No information available |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None identified |
Casaburi 2004.
| Methods | Study design: RCT into 4 groups | |
| Participants |
Setting: out‐patient, Los Angeles Inclusion criteria:
Exclusion criteria:
Participant status: Age (years± SD): RG: 69 (10); CG: 68 (9) Gender (M/F):RG: 12/0; CG: 12/0 FEV1 % predicted: RG: 36% (9); CG: 39% (12) Participants randomly assigned: Randomised: 26 Analysed: Rehab: 12 Control: 12 |
|
| Interventions |
Pulmonary rehabilitation: out‐patient (hospital) LLE, nutritional instruction provided Duration: 10 weeks (3 sessions/wk) Usual care: Placebo injections and no training |
|
| Outcomes |
Assessment: baseline and 10 weeks Peak work rate |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Subjects were randomly assigned to treatment groups based on randomisation tables; randomisation was stratified for age < or ≥ 67 years and FEV1 < or ≥ 40% predicted" (supplement) |
| Allocation concealment (selection bias) | Low risk | Study investigators unaware as to order of treatment group assignment (from study author) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, it was not possible to blind participants to their allocation of exercise or to blind those delivering the exercise |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Investigators and study coordinators were blinded as to whether subjects received testosterone or placebo" (supplement) |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Commenced: 53; completed: 47 (88.7%); attrition: 6 (11.3%) |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None identified |
Casey 2013.
| Methods | Study design: 2‐Arm, cluster‐randomised controlled trial | |
| Participants |
Setting: community based, West of Ireland Inclusion criteria:
Exclusion criteria:
Participant status: Age (years± SD): RG: 68.8 ±10.2; CG: 68.4 ± 10.3 Gender (M/F): RG: 117/61; CG: 106/66 FEV1 % (pred ± SD): RG: 57.6 ±14.3 ; CG: 59.7 ±13.8 Participants randomly assigned: Randomised: 350 (16 clusters in control and 16 clusters in intervention) (participants: 178 intervention; 172 control) Analysed: Rehab: 178 Control: 172 |
|
| Interventions |
Pulmonary rehabilitation: community based, structured, nurse‐led and delivered in the primary healthcare setting Aerobic exercise, ULE, LLE, Edu, phone support, respiratory muscle training Duration: 8 weeks, 2 hours per week Usual care: routine GP care |
|
| Outcomes |
Assessment: baseline and 12 weeks Incremental shuttle walking test, CRQ, Self‐Efficacy for Managing Chronic Disease 6‐item scale EuroQol EQ‐5D, utilisation of healthcare service |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Random allocation using computerised random sequence generation" (Casey 2013, pg 3) |
| Allocation concealment (selection bias) | Low risk | "Group allocation concealment was achieved by giving responsibility for computerised allocation sequence generation and group allocation to a researcher independent of the research team and blinded to baseline outcome data" (Casey 2013, pg 3) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, unable to blind participants |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Research assistants trained in outcome assessment, blinded to group allocation" (Casey 2013, pg 3) |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Commenced: 350; completed: 277 (79%); attrition: 73 (21%) |
| Selective reporting (reporting bias) | Low risk | Outcomes reported matched the protocol |
| Other bias | Low risk | None identified |
Cebollero 2012.
| Methods | Study design: RCT; randomisation into 3 groups | |
| Participants |
Setting: 2 centres in Spain Inclusion criteria:
Exclusion criteria:
Participant status: Age (years): PG: 68 (7); CG: 69 (5) Gender (M/F): all male FEV1 % (pred): RG: 47.8 (5); REG: 44.3 (11.9); CG: 38.7 (5) Participants randomly assigned: Randomised: 36 Combined resistance and endurance group: 14 Resistance alone group: 14 Control: 8 Did not include anyone who did not finish the intervention |
|
| Interventions |
Pulmonary rehabilitation: out‐patient programme (hospital‐based PR); 3 groups: resistance training alone (n = 14); combined resistance and endurance training (n = 14); and control group (n = 8) Duration: 12 weeks. (twice a week 45‐60 minutes) Usual care |
|
| Outcomes |
Assessment: baseline and 12 weeks CRQ, 6MWT |
|
| Notes | Combined group of REG/RG used in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "For each subject included in the study, a researcher picked closed ticket with a number inside (from 1 to 3). The number corresponded to one of the three study groups" (additional information from study author) |
| Allocation concealment (selection bias) | Low risk | Allocation: closed ticket with a number inside (additional information from study author) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, it is not possible to blind participants |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Yes, according to the study authors |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Did not include anyone who did not finish the intervention; unclear as to attrition |
| Selective reporting (reporting bias) | Low risk | Provided summary of all outcomes |
| Other bias | Low risk | |
Chan 2011.
| Methods |
Study design: single‐blind, randomised controlled trial Randomly assigned to 1 of 3 groups (TCQ group, exercise, control) |
|
| Participants |
Setting: 5 general outpatient clinics in Hong Kong Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 73.6±7.5; CG: 73.6 ±7.4 Gender (M/F): RG: 61/8; CG: 58/9 FEV1 % (pred ± SD ): RG: 91 ±.39; CG: 89 ±.39 Participants randomly assigned: Randomised: 206 (TCQ 70, exercise 69, control 67) Analysed: (only exercise group) Rehab:69 Control: 67 |
|
| Interventions |
Pulmonary rehabilitation: community (primary care setting) ULE, LLE, respiratory muscle training (Tai chi Qigong + exercise) Duration: completed 60 minutes twice a week for 3 months Usual care: instructed to maintain usual activities |
|
| Outcomes |
Assessment: baseline and 3 months Spirometry results, 6MWD, SGRQ, multi‐dimensional scale of perceived social support (MSPSS) Secondary outcomes Number of exacerbations, hospital admissions, Borg scale, SaO2 |
|
| Notes | TCQ group not included in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Random allocation was done using a randomizer software" (pg 5) |
| Allocation concealment (selection bias) | Unclear risk | Not informed |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, unable to blind participants and those delivering the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Research assistants (RAs) for data collection were blind to the study in order to minimize researcher bias" (pg 6) |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Commenced: 206; completed: 158 (76.7%); attrition: 48 (23.3%) |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported between Chan 2010 and Chan 2011 articles and protocol paper |
| Other bias | Low risk | None noted |
Chlumsky 2001.
| Methods | Study design: RCT into 2 groups | |
| Participants |
Setting: out‐patient Inclusion criteria:
Exclusion criteria: Participant status: Age (years ± SD): RG: 63 ±11 ; CG: 65 ±13 Gender (M/F): RG: 12/1; CG: 5/1 FEV1 % (pred ± SD): RG: 43% ±21; CG: 51% ±17 Participants randomly assigned: Randomised: 19 Analysed: Rehab: 13 Control: 6 |
|
| Interventions |
Pulmonary rehabilitation: outpatient hospital LLE, BE Duration: 8 weeks (60 minutes a week) Usual care: conventional care |
|
| Outcomes |
Assessment: baseline and 8 weeks ICET, SGRQ, 6MWT |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomized using specific PC program taking into consideration severity of bronchial obstruction and aimed at desired ratio 2:1" (letter from study author) |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Both participants and those delivering the intervention had to be aware of those who were in the intervention group |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No information provided |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No information provided in relation to attrition, and no indication in results that any participants did not complete the second assessment |
| Selective reporting (reporting bias) | Low risk | No trial registration protocol was found at http://www.controlled‐trials.com/mrct/ or www.who.int/trialsearch (searched for author names and parts of title of paper or intervention) |
| Other bias | Low risk | None noted |
Clark 1996.
| Methods | Study design: RCT | |
| Participants |
Setting: hospital in Glasgow recruited from a hospital chest clinic; recruited for home‐based exercise Inclusion criteria:
Exclusion criteria: Participant status: Age (years± SD): RG: 58 ± 8 ; CG: 55 ± 8 Gender (M/F): N/A FEV1 ± SD : RG: 1.72 L ± 0.83; CG: 1.44 L ±0.59 Participants randomly assigned: Randomised: 48 Analysed: Rehab: 32 Control: 16 |
|
| Interventions |
Pulmonary rehabilitation: home exercise LLE, ULE Duration: 12 weeks once a week Usual care: Control group asked to continue with their usual daily routine |
|
| Outcomes |
Assessment: baseline and 12 weeks ICET, ITT QoL: not measured |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Information not available "The 48 patients were randomly allocated into training (n=32) or control (n=16) groups, with a 2:1 training versus control ratio" (pg 2591) |
| Allocation concealment (selection bias) | Unclear risk | Information not available |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants undertaking the exercise had to be aware that they were receiving same |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned whether assessors were blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No account provided of any attrition after allocation; difficult to interpret from the graphs and tables how many completed |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None noted |
Cochrane 2006.
| Methods | Study design: RCT, randomly assigned to 1 of 4 interventions | |
| Participants |
Setting: North Tyneside and South Northumberland from primary and secondary care Inclusion criteria:
Exclusion criteria:
Participant status: Age (years± SD ): 68.9 ± 7.3 across all groups Gender: male 113 (44.1%): combined 32, exercise 32, CBSM 31, cont 18 Female 143 (55.9%): combined 42, exercise 35, CBSM 33, cont 32 FEV1 % (pred± SD): 52.4% ± 15.7 across all groups Participants randomly assigned: Commenced: 256 Group 1: allocated combined: 74 Group 2: allocated exercise: 67 Group 3: allocated CBMS: 65 Group 4: allocated control: 50 |
|
| Interventions |
Pulmonary rehabilitation: out‐patient programme (hospital‐based PR) Aerobic, ULE, LLE, cognitive behavioural self‐management Duration: 6 weeks (twice weekly, sessions lasting 2 hours) Usual care: This group of participants received no intervention, except standard care |
|
| Outcomes |
Assessment: baseline and 6 weeks, 6, 12 months CRQ, Short Form‐12 (SF‐12), Psychological State Hospital Anxiety and Depression Scale, COPD Self‐Efficacy Scale (COPD‐SES) |
|
| Notes | Incomplete results available for analysis of CRQ (reported as medians) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "The random allocation sequence was generated using cards numbered one to four, which were picked at random. Randomisation was stratified according to site and cohort. There were different sequences for each site (Northumberland and North Tyneside) and a new sequence was started for each of the five cohorts" (pg 34) |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes: "Letters detailing the group the subject had been randomised to and details of the intervention were then placed in envelopes. Only the patient ID number was visible on the outside of the envelopes" (pg 34) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | "Study participants and the practitioners running the interventions could not be blinded to which intervention they were receiving" (pg 34) |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "However, both the subjects and the researchers were blinded to the results of previous assessments (they were not allowed to see previous answers to questionnaires for example)" (pg 34) |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Commenced: 256; completed: 46 (57%); attrition: 43% |
| Selective reporting (reporting bias) | Low risk | Appeared to report what had been identified for reporting |
| Other bias | Low risk | None reported |
Cockcroft 1981.
| Methods |
Study design: RCT The first 20 were allocated entirely randomly, and the remaining 19 by a method known as "minimisation," which ensured an even spread of certain variables between groups Randomisation process: sealed envelopes Outcome assessments: blinded |
|
| Participants |
Setting: in‐patient graduated exercise Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 61± 5; CG: 60 ± 5 Gender (M/F): RG: 18/0; CG: 16/0 FEV1 ± SD: RG: 1.53 L ±0.70; CG: 1.32 L ± 0.44 Participants randomly assigned: Randomised: 39 Analysed: Rehab: 18 Control: 16 |
|
| Interventions |
Pulmonary rehabilitation: out‐patient rehabilitation centre LLE, ULE Duration: 6 weeks Usual care: given no special advice to exercise |
|
| Outcomes |
Assessment: baseline and 2, 4 months 12‐Minute WT, ITT Interviews, POMS, Eysenck |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: sealed envelopes (letter from study author) |
| Allocation concealment (selection bias) | Low risk | Study investigators unaware as to order of treatment group assignment (Cochrane Grade A) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As participants had to undertake exercise, they were aware of the group allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No information on blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Commenced: 39; 3completed: 4; attrition: 12% |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | Gender selection: male only |
De Souto Araujo 2012.
| Methods |
Study design: RCT; participants were allocated to 3 experimental groups: control group (CG), floor group (FG) and aquatic group (AG) The randomisation process was conducted by a researcher who was not involved in data collection, through the use of opaque envelopes sealed and numbered consecutively in the ratio 1:1:1 and containing study group assignment |
|
| Participants |
Setting: Brazil Inclusion criteria:
Exclusion criteria:
Participant status: Age (years): RG: [FG: 56.9; AG: 62.4]; CG: 71.1 Gender (M/F): RG:[ FG: 8/5; AG: 4/4]; CG: 8/3 FEV1 % (pred± SD): RG:[ FG: 39.2 ± 11.4; AG: 43.9 ± 10.3]; CG: 45.1 ± 12.6 Participants randomly assigned: 32 participants were randomly assigned Analysed: Floor group (FG): 13 Aquatic group (AG): 8 Control group (CG): 11 |
|
| Interventions |
Pulmonary rehabilitation: Low‐intensity water and floor exercises on COPD Duration: 8 weeks (3 times: Each session lasted 1 hour and 30 minutes) Usual care |
|
| Outcomes |
Assessment: baseline and 8 weeks (6MWT), BODE Index, SGRQ |
|
| Notes | Combined 2 intervention groups for analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The randomisation process was conducted by a researcher not involved in data collection (contact with study authors) |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes (contact with study authors) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Unable to blind participants because of the nature of the condition |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All evaluations (initial and final) were performed by a single investigator, who did not know to which group participants were allocated |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 42 participants randomly assigned; losses: 10 Attrition: 24% |
| Selective reporting (reporting bias) | Low risk | It was reported that all said they would |
| Other bias | Low risk | None noted |
Deering 2011.
| Methods |
Study design: RCT; randomly assigned to 3 groups: controls, PR and acupuncture and PR Randomisation occurred with the use of a random numbers table |
|
| Participants |
Setting: Dublin (identified via referral from the respiratory service) Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD ): RG: [PR only 67.7 ± 5.3, PR + Acu 65.1 ±9.7]; CG: 68.6 ± 5.5 Gender (M/F): RG: [PR only 11/14, PR + Acu 8/8]; CG: 12/7 FEV1 % (pred ± SD): RG: [PR only 77.0 ±19 , PR + Acu 80.7 ± 24.2]; CG: 45.8 ± 1 8.3 Smokers, packs per year: RG: [PR only 51, PR + Acu 846.5]; CG: 46.2 Participants randomly assigned: 60 randomised (control 19, PR 25, 19 PR + Acu) Analysed: 14 control 11 PR |
|
| Interventions |
Pulmonary rehabilitation: out‐patient programme (hospital‐based PR) Aerobic, ULE, LLE, respiratory muscle training, Edu Duration: 7 weeks, 14 PR sessions Usual care: no specific intervention |
|
| Outcomes |
Assessment: Baseline, end of PR and 3‐month follow‐up St. George’s Questionnaire Incremental shuttle walk test FEV1, Pi Max Feree Living Physical Activity, EQ5D |
|
| Notes | Only the PR group was reported on in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation occurred with use of a random numbers table |
| Allocation concealment (selection bias) | Unclear risk | No information available |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, it is not possible to blind participants or those delivering the programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Assessors and the medical team analysing the blood samples were blinded to the treatments received |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Commenced: 44 in control and PR groups; assessed: 25 Attrition: 19 (42%) |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Unclear risk | None identified |
Elci 2008.
| Methods |
Study design: RCT; 2 groups Participants were randomly allocated to control or experimental groups with the use of number tables. Concealed until after allocation; once allocated, both participants and those delivering the intervention were aware of those in the intervention group |
|
| Participants |
Setting:
Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 59.67 ± 8.6; CG: 58.08 ± 11.45 Gender (M/F): RG: 33/6; CG: 33/6 FEV1 % (pred): RG: 47.7; CG: 46.28 FEV1/FVC (± SD): RG: 55.46 ± 8.79; CG: 55.10 ± 7.17 Smokers %: RG: 33.3; CG: 20.5 Participants randomly assigned: 78 participants with COPD randomised: Analysed: 39 experimental group 39 control group |
|
| Interventions |
Pulmonary rehabilitation: combined home/community/out‐patient Duration: 3 months; exercises twice a day for 10 minutes, 5 days a week, at home under the supervision of a relative All participants performed 24 sessions Aoribic, ULE, LLE, Edu Usual care: Control group received standard medical care |
|
| Outcomes |
Assessment: baseline,1 month, 3 months St. George’s Questionnaire SF‐36, HADS Hospital Anxiety and Depression, 6MWT, MMRC |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomly allocated to control or experimental groups with the use of number tables |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, participants had to be aware of their allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | However, the nurse was blinded to the results of the SF‐36, SGRQ, HADS and MMRC |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No account of attrition provided |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | High risk | Gender imbalance noted |
Emery 1998.
| Methods |
Study design: RCT (3 groups: exercise, education and stress management (EXESM); education and stress management (control) Randomisation process: random numbers table Outcome assessments: blinded |
|
| Participants |
Setting: out‐patient Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 65 ± 6; CG: 67 ± 7 Gender (M/F): RG: 15:15; CG: 12/13 FEV1 (±SD): RG: 1.29 L ± 0.63; CG: 1.02 L ± 0.37 Participants randomly assigned: Randomised: 79 Analysed: Rehab: 25 Control: 25 |
|
| Interventions |
Pulmonary rehabilitation: 3 groups: floor group (FG), aquatic group (AG) and control group (out‐patient) LLE, ULE, Edu, Psy Duration: 10 weeks (for 4 hours per day) Usual care: asked not to alter activities significantly during the 10‐week study |
|
| Outcomes |
Assessment: baseline and after the 10‐week intervention period ICET, SIP |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | From a random number schedule, printed on a piece of paper |
| Allocation concealment (selection bias) | Low risk | Study investigators unaware as to order of treatment group assignment (Cochrane Grade A) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Concealed until after allocation; once allocated, both participants and those delivering the intervention were aware of those in the intervention group |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Technical staff conducting the assessments were not aware of group assignments |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Overall loss: 6 Attrition: 7.6% |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None noted |
Engström 1999.
| Methods | Study design: RCT (2 groups) | |
| Participants |
Setting: out‐patients and home patients recruited from Pulmonary Medicine Department in Goteborg, Sweden Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 66 ± 5; CG: 67 ± 5 Gender (M/F): RG: 14/12; CG: 12/12 FEV1 % (pred): RG: 30.7; CG: 34.1 Smokers: RG: 6; CG: 4 Participants randomly assigned: Randomised: 55 Analysed: Rehab: 26 Control: 24 |
|
| Interventions |
Pulmonary rehabilitation: out‐patient and home based LLE, ULE, Edu, IMT Duration: 52 weeks (training at the physio department twice weekly for 6 weeks followed by once weekly for 6 weeks and every second week for 6 weeks, then monthly for the remainder of the year. Each session lasted 45 minutes Usual care: Control received usual out‐patient care |
|
| Outcomes |
Assessment: baseline to 12 months 6‐Minute WT, ICET SIP, SGRQ |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer random number tables |
| Allocation concealment (selection bias) | Low risk | Study investigators unaware as to order of treatment group assignment (Cochrane Grade A) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Those receiving the programme had to be aware that they were receiving the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessments: blinded for HRQoL, not blinded for WT |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 50 out of 55 completed (90.9%) Attrition rate: 9.1% |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None identified |
Faager 2004.
| Methods | Study design: RCT (2 groups); 2 weeks after onset of oxygen therapy, 20 participants were randomly assigned to rehabilitation | |
| Participants |
Setting: in‐patient/home Department of Pulmonary Medicine of the Karolinska Hospital: over 2 years Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 72 ± 9; CG: 70 ± 8 Gender (M/F): RG: 3/7; CG: 3/7 FEV1 % (pred ± SD): RG: 26 ± 7 ; CG: 28 ± 6 Participants randomly assigned: Randomised: 20 (RG: 10; CG: 10) Analysed: Rehab: 7 Control: 7 |
|
| Interventions |
Pulmonary rehabilitation: in‐patient and home based Aerobic, ULE, LLE, Edu Duration: 8‐Week programme with 1 training session a week; training took 90 to 120 minutes Usual care |
|
| Outcomes |
Assessment: baseline and 8 weeks, 6 months CRQ, 6‐Minute WT, spirometry, blood gas analyses, pulse oximetry, Hospital Anxiety and Depression Scale (HADS) Stanford Health |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No clear statement on random sequence generation |
| Allocation concealment (selection bias) | Unclear risk | No detail re allocation concealment or how randomisation was done |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Both participants and those delivering the programme were aware of those included in the intervention group |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No information provided |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Commenced overall: 20; finished week 8: 14 Attrition: 30% |
| Selective reporting (reporting bias) | Low risk | No protocol paper was registered, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None noted |
Faulkner 2010.
| Methods | Study design: RCT (2 groups) | |
| Participants |
Setting: recruited from primary care; 16 GP practices in Exeter Inclusion criteria:
Exclusion criteria:
Participant status: Age: not provided Gender (M/F): not provided FEV1 % (pred): not provided Smokers: all current non‐smokers Participants randomly assigned: Randomised: 20 (RG: 10; CG: 10) Analysed: Rehab:6 Control:8 |
|
| Interventions |
Pulmonary rehabilitation: community (primary care setting) Exercise programme run in an exercise facility at a university Aerobic, ULE, LLE, Edu Duration: 8 weeks once‐weekly 90‐minute supervised exercise and education sessions delivered by a qualified exercise and healthcare practitioner Usual care: Control group received usual care. All were given tiotropium |
|
| Outcomes |
Assessment: baseline, 1 week post intervention CRQ, ISWT, lung information needs questionnaire (LINQ), HADS, 7‐day physical activity recall questionnaire, physical self‐perception profile (PSPP) |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation sequence, stratified for smoking status, computer generated by a statistician who was independent of the trial |
| Allocation concealment (selection bias) | Low risk | Group allocation was kept concealed by means of sealed envelopes, which were opened in sequence by the trial researcher following baseline assessment |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | It was not possible to blind participants or GPs to group allocation |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcome assessors not blinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 20 randomly assigned; attrition: overall 6 (30%) |
| Selective reporting (reporting bias) | Low risk | All outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None noted |
Fernandez 2009.
| Methods | Study design: RCT (2 groups) performed in a 300‐bed district hospital and involving patients with very severe COPD who received oxygen treatment | |
| Participants |
Setting: Spanish study; 300‐bed district hospital Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 66 ± 8; CG: 70 ± 5 Gender (M/F): 1 woman, as the rest were men FEV1 % (pred ± SD): RG: 33 ± 10; CG: 38 ± 12 FEV1/FVC (± SD): RG: 42 ± 10; CG: 42 ± 11 Participants randomly assigned: Randomised: 50 (RG: 30; CG: 20) Analysed: Rehab:27 Control:14 |
|
| Interventions |
Pulmonary rehabilitation: home based Aerobic exercise, ULE, LLE, educational material, home physio visits Duration: received 2 one‐hour sessions in the hospital. A minimum of 1 hour of exercise per day was indicated, for a minimum of 5 days per week Usual care |
|
| Outcomes |
Assessment: baseline and Imediately post intervention (1 year) 6MWT, SGRQ |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not informed of process: only "randomly divided into 2 groups" |
| Allocation concealment (selection bias) | Unclear risk | Not informed |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, unable to blind participants or those delivering the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not informed |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | After 1 year, 41 participants completed (83.7%) Attrition: 16.3% |
| Selective reporting (reporting bias) | Low risk | No protocol paper was found, but all outcomes listed in the paper appear to have been reported |
| Other bias | High risk | All men; 1 woman excluded from analysis |
Finnerty 2001.
| Methods | Study design: RCT (2 groups) | |
| Participants |
Setting: recruited from an out‐patient clinical at the Chester Hospital NHS Trust, UK Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± Sd ): RG: 70.4 ± 8.0; CG: 68.4 ± 10.4 Gender (M/F): RG: 25/11; CG: 19/10 FEV1 % (pred ± SD): RG: 41.2 ± 19.2; CG: 41.2 ± 16.2 Smoking NO: RG: 2; CG: 6 Participants randomly assigned: Randomised: 100 (27 did not attend initial assessment) Analysed: Rehab:36 Control: 29 |
|
| Interventions |
Pulmonary rehabilitation: 6‐Week out‐patient‐based rehabilitation programme ULE, LLE, Edu Duration: 6‐Week out‐patient‐based rehabilitation programme; 2 visits per week: 2‐hour education visit and 1‐hour exercise visit Usual care: Control group reviewed routinely as medical out‐patients |
|
| Outcomes |
Assessment: baseline, 12 weeks and 24 weeks 6‐Minute WT, SGRQ |
|
| Notes | Jadad's score = 3 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was in blocks of 10, using random numbers |
| Allocation concealment (selection bias) | Low risk | Study investigators unaware as to order of treatment group assignment (Cochrane Grade A) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the exercise programme, unable to blind allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Both tests were supervised by a blinded observer who subsequently repeated these assessments" |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 100 randomly assigned; 55 completed (55%) Only 73 attended for initial assessment 45% attrition |
| Selective reporting (reporting bias) | Low risk | No protocol paper was found, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None identified |
Gohl 2006.
| Methods | Study design: RCT (2 groups) | |
| Participants |
Setting: out‐patient community, training in sports hall; Germany Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 62.5 ± 7; CG: 63.2 ± 8.5 Gender (M/F): RG: 6/4; CG: 7/2 FEV1 % (pred ± SD): RG: 53.4 ± 10.7; CG: 53.7 ± 5.8 Participants randomly assigned: Randomised: 34 (RG: 17; CG 17) Analysed: Rehab:10 Control: 9 |
|
| Interventions |
Pulmonary rehabilitation: community, complex long‐term training programme Aerobic exercise, ULE, LLE (escalating levels of activity over time) Duration: 12‐month training programme Usual care: Control group did not receive therapy |
|
| Outcomes |
Assessment: Baseline and 12 months (end of intervention) 6MWT, St. George’s Questionnaire, SF‐36, muscle force |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Assigned to training group or control group at random (chosen by lot) |
| Allocation concealment (selection bias) | Unclear risk | Not provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, it is not possible to blind participants or those delivering the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not provided |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Commenced: 34; completed: 19; lost: 15 Attrition: 44% |
| Selective reporting (reporting bias) | Low risk | No protocol paper was found, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None noted |
Goldstein 1994.
| Methods |
Study design: RCT (2 groups) Randomisation process: random numbers table Outcome assessments: blinded |
|
| Participants |
Setting: in‐patient/out‐patient; Canada Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 66 ± 7; CG: 65 ± 8 Gender (M/F): RG: 21/17; CG: 17/23 FEV1 % (pred ± SD): RG: 34.8 ±14.5; CG: 34.6 ± 11.8 FEV1 /FVC: RG: 36.8 ± 9.5; CG: 38.8 ± 12.4 Smoking packs (± SD): RG: 58 ± 24; CG: 51 ± 26 per year Participants randomly assigned: Randomised: 89 Analysed: Rehab: 38 Control: 40 |
|
| Interventions |
Pulmonary rehabilitation: in‐patient/home based Aerobics, LLE, ULE, BE, Edu, Psy Duration: 2 months of in‐patient rehabilitation followed by 4 months of out‐patient care Usual care: Control group received conventional care from general practitioner and respiratory specialist |
|
| Outcomes |
Assessment: baseline and 24 weeks 6‐Minute WT, ICET, SSCET, CRQ, BDI/TDI |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Used random tables for allocation |
| Allocation concealment (selection bias) | Low risk | Study investigators unaware as to order of treatment group assignment (Cochrane Grade A) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Both participants and those delivering the intervention were aware of the allocation of participants |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Investigator carrying out outcome assessments blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 89 randomised and 78 completed Attrition: 11 (12%) |
| Selective reporting (reporting bias) | Low risk | No protocol paper was found, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None noted |
Gomez 2006.
| Methods |
Study design: RCT (3 groups); PR for 3 months and rehabilitation maintenance for 12 months (RHBM group). Second group received PR for 3 months only (RHB group) and the third was the control |
|
| Participants |
Setting: recruited by family physicians from 7 primary care practices in Palma de Mallorca, Spain Inclusion criteria:
Exclusion criteria:
Participant status: Age (years): RG (RHB: 64.1; RHBM: 64.9); CG: 63.4 Gender (M/F): RG: 39/9; CG: 19/4 FEV1 % (pred): RG: 74 (Range 66.5‐81.5); CG: 60.1 (Range 55.6‐64.4) FEV1/FVC: RG: 61.2; CG: 59.1 Participants randomly assigned: Randomised: 97 (33 RHB group and 32 RHBM; control 32) Analysed: Rehab:36 Control: 14 |
|
| Interventions |
Pulmonary rehabilitation: community (primary care setting) Aerobic exercise, ULE, LLE, educational material Duration: 3 months; rehabilitation maintenance for 12 months Usual care: Group received routine care without rehabilitation |
|
| Outcomes |
Assessment: Baseline, 3 months and 12 months CRQ, pulmonary function tests, 6MWT |
|
| Notes | Analyses completed on 3‐month results for combined RHB and RHBM groups | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Centrally administered, computer‐generated block randomisation scheme using blocks of 6 with EPIDAT, stratified according to participating site |
| Allocation concealment (selection bias) | Low risk | See above |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, unable to blind participants and those delivering the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Health staff members involved in follow‐up (a psychologist and a nurse) were blinded to participant assignment |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Out of 97, only 50 at 3‐month evaluation Attrition: 47 (48%) |
| Selective reporting (reporting bias) | Low risk | Trial registration (ISRCTN94514482); all outcomes stated in the study appear to have been measured |
| Other bias | Low risk | None noted |
Gosselink 2000.
| Methods | Study design: RCT (2 groups) | |
| Participants |
Setting: out‐patient: referred from an outpatient department in Leuven, Belgium Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 60 ± 9; CG: 63 ± 7 Gender (M/F): RG: 31/6; CG: 30/3 FEV1 % (pred ± SD): 41 ±16; RG: CG: 43 ±12 Participants randomly assigned: Randomised: 100 Analysed: Rehab: 34 Control: 28 |
|
| Interventions |
Pulmonary rehabilitation: outpatient sessions; cycling, treadmill walking, stair climbing and peripheral muscle training LLE, ULE Duration: 24 weeks: 3 times a week in the first 3 months; during subsequent 3 months, training frequency was reduced to twice weekly. Each session had a duration of 1.5 hours Usual care: usual medical care |
|
| Outcomes |
Assessment: baseline and at 6 months and 18 months 6‐Minute WT, ICET, CRQ Isometric quadriceps strength, inspiratory and expiratory muscle strength |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: sealed envelopes |
| Allocation concealment (selection bias) | Low risk | Study investigators unaware as to order of treatment group assignment (Cochrane Grade A) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Both participants and those delivering the intervention were aware of the allocation of participants |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcome assessments: not blinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Commenced: 100; 6 months: 62; remaining: 62% Attrition: 38% |
| Selective reporting (reporting bias) | Low risk | No protocol paper was found, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None noted |
Gottlieb 2011.
| Methods |
Study design: RCT (2 groups) Single‐centre, randomised, placebo‐controlled, unblinded clinical trial |
|
| Participants |
Setting: patients listed with 56 GPs in Copenhagen, Denmark Inclusion criteria:
Exclusion criteria:
Participant status: Age (years, Range): RG: 74.1 (66–82); CG: 73.2 (67–88) Gender (M/F): RG: 7/15; CG: 7/13 FEV1 % (pred ± SD): RG: 64.27 ± 7.9; CG: 67.05 ± 8.8 FEV1 /FVC (± SD): RG: 0.54 ± 0.07; CG: 0.6 ± 0.1 Smokers: RG: 11; CG: 9 Participants randomly assigned: Randomised: 61 (RG: 35; GG: 26) Analysed: Rehab: 22 Control: 20 |
|
| Interventions |
Pulmonary rehabilitation: community Aerobic exercise, ULE, LLE, Edu, follow‐up call Duration: 7 weeks; two 90‐minute sessions a week Usual care: standard COPD care received from GP |
|
| Outcomes |
Assessment: baseline and 6 months 6MWT, MRC, SGRQ |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was performed using sealed opaque envelopes randomly assigned to participants |
| Allocation concealment (selection bias) | Low risk | |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Both participants and those delivering the intervention were aware of the allocation of participants |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded clinical trial |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 61 randomly assigned, 42 completed (68%) Attrition: 32% |
| Selective reporting (reporting bias) | Low risk | Study authors appear to have reported what they said they would at the beginning of the article |
| Other bias | Low risk | None identified |
Griffiths 2000.
| Methods |
Study design: RCT (2 groups) |
|
| Participants |
Setting: recruited from local hospitals and local general practices to participate; Wales Out‐patient + Home‐based follow‐up Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 68.2 ± 8.2; CG: 68.3 ± 8.1 Gender (M/F): RG: 57/36; CG: 54/37 FEV1 % (pred ± SD): RG: 39.7 ±16.2; CG: 39.4 ±16.4 FEV1 /FVC (± SD): RG: 0.49 ± 0.13; CG: 0.49 ± 0.13 Smoking, packs per year: RG: 43.5 (31.1); CG: 45.7 (21.9) Participants randomly assigned: Randomised: 200 Analysed: Rehab: 93 Control: 91 |
|
| Interventions |
Pulmonary rehabilitation: multi‐disciplinary, out‐patient/home based LLE, ULE, Edu, Psy, NS, SmC Duration: 6 weeks, 3 half‐days per week; session 2 hours long; in addition encouraged to follow a home exercise routine Usual care: continued with usual out‐patient or primary care follow‐up |
|
| Outcomes |
Assessment: baseline and follow‐up for 1 year Shuttle WT, CRQ, SF‐36, SGRQ, HADS |
|
| Notes | Jadad's score = 2 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: sealed envelopes |
| Allocation concealment (selection bias) | Low risk | Study investigators unaware as to order of treatment group assignment (Cochrane Grade A) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, it is not possible to blind participants or those delivering the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessments: blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 200 commenced; 180 completed Attrition: 10% |
| Selective reporting (reporting bias) | Low risk | No protocol paper was found, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None noted |
Gurgun 2013.
| Methods | Study design: RCT (3 groups) | |
| Participants |
Setting: patients from Ege University Hospital Turkey outpatient clinic admitted to the PR unit between January 2010 and November 2010 Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: [PRNS: 64.0 ± 10.8; PR: 66.8 ± 9.6]; CG: 67.8 ± 6.6 Gender (M/F): RG: [PRNS 13/2; PR: 15/0]; CG: 16/0 FEV1 % (pred ± SD): RG:[ PRNS: 41.9 ± 10.8; PR: 41.9 ± 13.2]; CG: 39.3 ± 9.3 FEV1 /FVC (± SD): RG: [PRNS: 53.4 ± 15.8; PR: 49.0 ± 6.7]; CG: 46.7 ± 7.2 Participants randomly assigned: Randomised: 46 Analysed: Rehab: PRNS: 15; PR: 15 Control: 16 |
|
| Interventions |
Pulmonary rehabilitation: out‐patient programme (hospital based). Pulmonary rehabilitation and nutritional support (Pr Alone (PR) or PR and nutritional support (PRNS)) Aerobic exercise, ULE, LLE, educational material, nutritional support Duration: 8 weeks Usual care: usual medical standard care |
|
| Outcomes |
Assessment: baseline and following 8 weeks of PR MRC, 6MWT, ISWT, ESWT, SGRQ, HADS |
|
| Notes | Reported results using combined group PR + PRNS | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Eligible patients were randomly assigned in a 1:1:1 ratio with the use of sealed envelopes |
| Allocation concealment (selection bias) | Low risk | As above |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, unable to blind participants or those delivering the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not stated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No attrition reported |
| Selective reporting (reporting bias) | Low risk | No protocol paper was found, but all outcomes listed in the paper appear to have been reported |
| Other bias | High risk | All men; 15 in PR group, 15 in control. 2 women in PRNS |
Güell 1995.
| Methods |
Study design: RCT (2 groups) Randomisation process: random numbers table Outcome assessments: blinded |
|
| Participants |
Setting: out‐patient: secondary care respiratory clinic in Barcelona Inclusion criteria:
Exclusion criteria:
Participant status: Age (years): RG: 66 (7); CG: 65 (6) Gender (M/F): all men FEV1 % (pred): RG: 31 (12); CG: 39 (14) Participants randomly assigned: Randomised: 60 Analysed: Rehab: 29 Control: 27 |
|
| Interventions |
Pulmonary rehabilitation (out‐patient and home based; 3 months of outpatient breathing retraining and chest physiotherapy; 3 months of daily supervised exercise) LLE, BE, PD Duration: 6 months (3 months of PR; participants were included in two 30‐minute sessions each week (breathing retraining) combined with home exercise programme). Second 3‐month period (exercise training): five 30‐minute sessions weekly on a stationary cycle ergometer Usual care: Control group received standard care |
|
| Outcomes |
Assessment: baseline and 3, 6, 9, 12, 18 and 24 months 6MWT, ICET, CRQ |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Used random number tables; letter sent to LaCasse |
| Allocation concealment (selection bias) | High risk | No concealment |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Unable to blind both participants and those delivering the intervention because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Technicians who collected data for outcome measures at every visit, as explained below, were blinded to participants' allocation to PR or control groups |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All 60 participants completed 6 months of follow‐up |
| Selective reporting (reporting bias) | Low risk | No protocol paper was found, but all outcomes listed in the paper appear to have been reported |
| Other bias | High risk | All men only |
Güell 1998.
| Methods | Study design: RCT (2 groups) | |
| Participants |
Setting: out‐patient Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): 68 ± 8; CG: 66 ± 8 Gender (M/F): RG: 16/2; CG: 17/0 FEV1 % (pred ± SD): RG: 32% ±11; CG: 38% ±15 Participants randomly assigned: Randomised: 40 Analysed: Rehab: 18 Control: 17 |
|
| Interventions |
Pulmonary rehabilitation: 2 months of chest physio and 2 months of muscle training LLE, IMT Duration: 8 weeks Usual care |
|
| Outcomes |
Assessment: baseline and post intervention (8 weeks) CRQ, 6MWT, dyspnoea, maximal workload |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random numbers table |
| Allocation concealment (selection bias) | High risk | Randomisation was not concealed, but the likelihood of bias introduced by unconcealed randomisation was reduced by recruitment of consecutive patients |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Unable to blind both participants and those delivering the intervention because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Technicians who collected data were blinded to participant allocation to the PRG or the CG, as were data analysts, until the analysis was deemed complete |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Commenced: 40; attrition: 5 (12%) |
| Selective reporting (reporting bias) | Low risk | No protocol paper was found, but all outcomes listed in the paper appear to have been reported |
| Other bias | Low risk | None noted |
Hernandez 2000.
| Methods |
Study design: RCT (2 groups) Randomisation process: random numbers table Outcome assessments: blinded |
|
| Participants |
Setting: home‐based; Seville, Spain Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 64.3 ± 8.3 ; CG: 63.1 ± 6.9 Gender (M/F): RG: 20/0; CG: 17/0 FEV1 % (pred ± SD): RG: 71.1 ± 18.9; CG: 74.7 ± 14.7 FEV1 /FVC (SD): RG: 47 ± 9.9; CG: 42.3 ±12 Participants randomly assigned: Randomised: 60 Analysed: Rehab: 20 Control: 17 |
|
| Interventions |
Pulmonary rehabilitation: home rehabilitation programme; training intensity was determined individually LLE Duration: 12 weeks Usual care: Control group participants (standard medical treatment alone; also made visits to the hospital every 2 weeks for a clinical checkup and for supervision of treatment) |
|
| Outcomes |
Assessment: baseline and 12 weeks ICET, Shuttle WT, CRQ, BDI/TDI |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random numbers table used |
| Allocation concealment (selection bias) | Unclear risk | No details provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Unable to blind both participants and those delivering the intervention because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Investigators were blinded (letter from study author) |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 60 randomly assigned; 37 completed (61.6%) Attrition: 38.3% |
| Selective reporting (reporting bias) | Low risk | It appears that all outcomes stated at the outset of the article were reported in the findings |
| Other bias | Low risk | Participants who were excluded because they did not meet the criteria appear to have been excluded after randomisation |
Hoff 2007.
| Methods | Study design: RCT (2 groups) | |
| Participants |
Setting: Norway Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 62.8 ± 1.4; CG: 60.6 ± 3.0 Gender (M/F): RG: 4/2; CG: 4/2 FEV1/FVC (± SD): RG: 49.9 ± 4.6; CG: 45.2 ± 6.0 Participants randomly assigned: Randomised: Analysed: 12 Rehab: 6 Control: 6 |
|
| Interventions |
Pulmonary rehabilitation: lab‐based maximal strength training (seated horizontal leg press apparatus) LLE Duration: 8 weeks Usual care: Control group continued normal daily living with modest regular activity, as recommended by pulmonary physician |
|
| Outcomes |
Assessment: baseline and week 8 Incremental cycle ergometry |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient information provided |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, unable to blind both participants and those delivering the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information provided |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants completed the study protocol with no adverse effects, and the MST group completed 100% of the planned training |
| Selective reporting (reporting bias) | Low risk | No protocol was identified. All outcomes identified in the methods section of the paper were reported in the results |
| Other bias | Low risk | None noted |
Jones 1985.
| Methods | Study design: RCT (3 groups: exercise, resistive breathing, control) | |
| Participants |
Setting: home based; recruited from a chest clinic in Dunedin, New Zealand Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD ): RG: 63.8 ± 6.09; CG: 62.7 ± 8.36 Gender (M/F): RG: 6/2; CG: 1/5 FEV1 % (pred ± SD): RG: 0.78 ± 0.27; CG: 0.68 ± 0.12 Smoking: RG: 8; CG: 5 Participants randomly assigned: Randomised: 30 (exercise 11, breathing 11, control 8) Analysed: Rehab: exercise: 8, breathing: 7 Control: 6 |
|
| Interventions |
Pulmonary rehabilitation: Simple physical exercises at home under the supervision of a physiotherapist and every 2 weeks in the gymnasium LLE, ULE Duration: 10 weeks Usual care: placebo respiratory device and usual care |
|
| Outcomes |
Assessment: baseline and 10 weeks 12‐Minute WT, ICET, SSCET, daily diary, Lubin Affectometer |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: drawing lots |
| Allocation concealment (selection bias) | High risk | No concealment apparent |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, unable to blind both participants and those delivering the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessments: not blinded for ICET, blinded for the others |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Commenced: 19; completed: 14 (73.7%) Attrition: 26.3% |
| Selective reporting (reporting bias) | Low risk | No protocol was identified. All outcomes identified in the methods section of the paper are reported in the results |
| Other bias | High risk | Control received a placebo respiratory device, which may have an impact |
Karapolat 2007.
| Methods | Study design: RCT (2 groups) | |
| Participants |
Setting: Dept Chest Medicinein Izmir, Turkey Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 64.81 ± 9.4; CG: 67.21 ± 6.72 Gender (M/F): RG: 21/5; CG: 18/1 FEV1 %: RG: 55.50%; CG: 58% Participants randomly assigned: Randomised: 54 Analysed: Rehab: 26 Control: 19 |
|
| Interventions |
Pulmonary rehabilitation: out‐patient programme Aerobic exercise, ULE, LLE, breathing exercises, educational material Duration: 8 weeks Education component: 16 sessions of discussion (1 hour/wk) Exercise component: 3 times a week Usual care |
|
| Outcomes |
Assessment: baseline, week 8 and week 12 6MWT, SGRQ |
|
| Notes | Week 8 data used for analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants were randomly assigned in a 1:1 ratio with the use of sealed envelopes |
| Allocation concealment (selection bias) | Low risk | |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, unable to blind both participants and those delivering the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not informed |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Commenced: 49; completed: 45 Attrition: 18.17% |
| Selective reporting (reporting bias) | Low risk | No protocol was identified. All outcomes identified in the methods section of the paper are reported in the results |
| Other bias | Low risk | Participants who were excluded because they did not meet the criteria appear to have been excluded after randomisation |
Lake 1990.
| Methods | Study design: RCT (4 groups); participants were randomly assigned to a control group and to 3 actively trained groups | |
| Participants |
Setting: intervention delivered in outpatient hospital setting; Perth, Western Australia Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD ): RG: 66.3 ± 6.8; CG: 65.7 ± 3.5 Gender (M/F): RG: 6/1; CG: 4/3 FEV1 % (pred ± Sd): RG: 0.97 ± 0.29; CG: 0.83 ± 0.25 Participants randomly assigned: Randomised: 28 Analysed: Rehab: 7 Control: 7 |
|
| Interventions |
Pulmonary rehabilitation: out‐patient hospital based: 4 groups (combined exercise: 7; upper limb: 6; lower limb: 7; control) LLE or ULE or both Duration: 8 weeks (1 hour 3 times per week) Usual care |
|
| Outcomes |
Assessment: baseline and immediately after the 8 weeks 6MWT, ICET, IAET Bandura Scale of Well‐being |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: randomisation chart |
| Allocation concealment (selection bias) | Unclear risk | No allocation concealment discussed |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, unable to blind participants and those delivering the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessments: blinded for ICET, not blinded for 6MWT |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Commenced: 28; finished: 26 (92.9%) Attrition: 7.1% |
| Selective reporting (reporting bias) | Low risk | No protocol was identified. All outcomes identified in the methods section of the paper were reported in the results |
| Other bias | Unclear risk | None noted |
Lindsay 2005.
| Methods | Study design: RCT (2 groups) | |
| Participants |
Setting: Lek Yuen Family Medicine Teaching Clinic, Hong Kong, and the Family Medicine Training Centre of the Prince of Wales Hospital Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 69.5 ± 9.3; CG: 69.8 ± 10.3 Gender (M/F): RG: 20/5; CG: 18/7 FEV1 % (pred ± SD): RG: 0.9 ± 0.3; CG: 0.8 ± 0.4 Current smoker: RG 3 (12%); CG: 7 (28) Participants randomly assigned: Randomised: 50 (25 each group) Analysed: Rehab: 21 Control: 20 |
|
| Interventions |
Pulmonary rehabilitation: community (primary care setting) Aerobic exercise, ULE, LLE, educational material, home physio visits Duration: 6 weekly sessions of psychoeducation, each lasting for 2 hours Usual care: given tiotropium, which is considered standard usual care |
|
| Outcomes |
Assessment: baseline, start of PRP, end of PRP and 3 months 6MWD, spirometry, CRQ |
|
| Notes | For analysis, used mean and standard deviation of all other studies, as did not provide SD | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not provided |
| Allocation concealment (selection bias) | Unclear risk | Not provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, unable to blind participants and those delivering the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not provided |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 50 randomly assigned; drop‐out: 9 Attrition: 18% |
| Selective reporting (reporting bias) | Low risk | No protocol was identified. All outcomes identified in the methods section of the paper were reported in the results |
| Other bias | Low risk | None noted |
Liu 2012.
| Methods |
Study design: RCT (3 groups) Single‐blind |
|
| Participants |
Setting: conducted in Hong Kong, in the care of respiratory specialists of Jiangs Province Hospitals from October 2008 to October 2010 Inclusion criteria: COPD severity level at GOLD stages I and II Exclusion criteria: no serious co‐morbidities (e.g. pulmonary tuberculosis, emphysema, congestive heart failure) Participant status: Age (years± SD):RG:[ HQG: 61.82 ± 7.69; PRG: 61.34 ± 8.3]; CG: 62.2 ± 6.34 Gender (M/F): RG:[HQG: 78%/22%; RG: 72%/28%]; CG: 80%/20% FEV1 % (pred ± SD ): [HQG: 74.43 ± 12.93; PRP: 75.31 ± 12.84;] FEV1 /FVC (± SD): RG[HQG: 60.73 ± 6.18; PRP: 61.27± 5.86]; control: 61.43 ± 6.17 Never smoked: HQG: 37.3%; PRP: 43.8%; control: 34.3% Participants randomly assigned: Randomised: 132 (PR: 36; Qiqong: 60; control: 36) Analysed: Rehab: 32 Control: 35 |
|
| Interventions |
Pulmonary rehabilitation: combined in‐patient and/or home/community/out‐patient
Aerobic exercise, ULE, LLE, peer support Duration: 6 months; then encouraged to participate in peer‐led weekly walking and ball game activities thrice a week, 1 hour each time, for 6 months Usual care: received health education and was advised to continue exercising alone |
|
| Outcomes |
Assessment: baseline and 6 months 6MWD, Zhongshan COPD Questionnaire for QoL, immune cell factor, hospital admissions |
|
| Notes | Used only exercise group for analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participant allocation list was drawn on the basis of random order of the block ("H‐H‐H‐P‐P‐C‐C") for 20 times, until a list of 140 individuals in a specific order was obtained |
| Allocation concealment (selection bias) | Low risk | Not provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, participants and those delivering the programme could be randomly assigned |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All outcome assessors were blinded to each participant’s allocated group, as well as to the objectives of the study, to minimise bias |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Randomised: 132 (control: 36; PR: 36; Qigong: 60) 118 included in the final analysis (control: 35; PR: 32; Qigong: 51) So lost 14 overall (89%) participated; attrition: 11% |
| Selective reporting (reporting bias) | Low risk | No protocol was identified, but all results re stated outcomes seem to have been included |
| Other bias | Low risk | None noted |
McGavin 1977.
| Methods |
Study design: RCT (2 groups) |
|
| Participants |
Setting: home based; New Delhi, India Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD ): RG: 61.4 ± 5.6, CG: 57.2 ± 7.9 Gender (M/F): RG: 12/0; CG: 12/0 FEV1 % (pred ± SD ): RG: 0.97 L ± 0.33; CG: 1.15 L ± 0.72 FEV1 /FVC: RG:CG Participants randomly assigned: Randomised: 28 Analysed: Rehab: 12 Control: 12 |
|
| Interventions |
Pulmonary rehabilitation: home‐based training programme consisting of graded stair‐climbing exercises tailored to suit the ability of the individual LLE Duration: continuous, once a day, at least 5 days a week Usual care: Control group did not receive exercise instructions or an out‐patient check at 2 weeks |
|
| Outcomes |
Assessment: baseline and mean 14 weeks control; mean 19 weeks intervention 12‐Minute WT, ICET Interviews |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Used random numbers tables |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, participants and those delivering the programme could be randomly assigned |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcome assessments: not blinded (letter from study authors) |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 28 started; 24 finished (85.7%) Attrition: 14.28% |
| Selective reporting (reporting bias) | Low risk | No protocol was identified, but all stated results re outcomes seem to have been included |
| Other bias | Low risk | None identified |
McNamara 2013.
| Methods |
Study design: RCT (3 groups, land based, water based, control) |
|
| Participants |
Setting: patients referred to outpatient pulmonary rehabilitation at an Australian tertiary public hospital Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG:[ water: 72 ± 10; land: 73 ± 7]; CG: 70 ± 9 Gender (M/F): RG: 15/23; CG: 7/8 FEV1 % (pred ± SD): RG: [WB: 60 ± 10; LB: 62 ± 15]; CG: 55 ± 20 FEV1 /FVC: RG: [WB: 59 ± 9; LB: 58 ± 9]; CG: 53 ± 13 Current smokers: RG: [WB: 3; LB: 1]; CG: 2 Participants randomly assigned: Randomised: 53 (control: 15; land based: 20; water based: 18) Analysed: Rehab: land based: 15; water based: 15 Control: 15 |
|
| Interventions |
Pulmonary rehabilitation: out‐patient programme: hospital gymnasium; participants walked at an intensity of 80% of the average 6MWT speed over ground or on a treadmill. Water‐based exercise training group exercised in a hospital hydrotherapy pool Aerobic exercise, ULE, LLE Duration: 8 weeks; three 60‐minute sessions a week of supervised exercise led by the same experienced physiotherapist Usual care: Control group participants received usual medical care and no exercise training. They were asked not to alter their exercise level over the study period |
|
| Outcomes |
Assessment: baseline and 8 weeks CRDQ, 6MWT, ISWT, ESWT |
|
| Notes | Please note: Combined intervention groups of land and water used for analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomly assigned by an investigator external to the study using a Web‐based computer‐generated sequence |
| Allocation concealment (selection bias) | Low risk | Concealed allocation achieved with the use of opaque envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the exercise interventions, it was not possible to blind therapists or participants to allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Assessor blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Commenced: 53; analysed: 55 Attrition: 8 (15%) |
| Selective reporting (reporting bias) | Low risk | Registered on www.anzctr.org.au (ACTRN0126000408583) Primary outcomes and all planned secondary outcomes appear to have been reported |
| Other bias | Low risk | None noted |
Mehri 2007.
| Methods | Study design: RCT (2 groups) | |
| Participants |
Setting: Iran Inclusion criteria:
Exclusion criteria: Participant status: Age (years ± SD): RG: 52.1 ± 10.7; CG: 52.17 ± 11.6 Gender (M/F): RG: 11/9; CG: 7/11 FEV1 % (pred): RG:CG: not available FEV1 /FVC: RG:CG: not available Participants randomly assigned: Randomised: 38 (RG: 20, CG: 18) Analysed: Rehab: 20 Control: 18 |
|
| Interventions |
Pulmonary rehabilitation: outpatient clinic, exercised on a treadmill Aerobic exercise, ULE, LLE Duration: 4 weeks, 2 times a week Usual care: Control group completed no treadmill exercise training |
|
| Outcomes |
Assessment: baseline and 4 weeks VO2 peak, based on the Rockport formula |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the exercise interventions, it was not possible to blind therapists or participants to allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No information provided |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No attrition reported |
| Selective reporting (reporting bias) | Low risk | No protocol was identified, but all stated results re outcomes appear to have been included |
| Other bias | Low risk | None noted |
Mendes De Oliveira 2010.
| Methods |
Study design: RCT (3 groups); outpatient group that performed all activities at the clinic, home‐based group that performed activities at home and control group |
|
| Participants |
Setting: private pulmonology clinic in Cascavel (southern Brazil) Inclusion criteria:
Exclusion criteria:
Participant status: Age (years): RG: [home: 66.4; outpatients: 71.3]; CG: 70.8 Gender (M/F): RG:[ home: 27/6; outpatients: 19/4]: CG: 19/10 FEV1 % (pred): RG:[ home 47.5 ; outpatient 51.5 ]; CG: 41.4 Participants randomly assigned: Randomised: 117 Analysed: Rehab: home: 33; outpatient: 23 Control: 29 |
|
| Interventions |
Pulmonary rehabilitation: outpatient clinic or home based Aerobic exercise, ULE, LLE, education Duration: 12 weeks, 3 times a week Usual care: Control group performed no PR |
|
| Outcomes |
Assessment: baseline and 12 weeks MRC, BODE Index, 6MWT |
|
| Notes | Combined 2 intervention groups for the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomly assigned electronically by a computer to 3 groups |
| Allocation concealment (selection bias) | Low risk | Not provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, unable to blind participants and those delivering intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | 2 duly trained healthcare professionals were responsible for the evaluations, which were performed by the same evaluators for all participants |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Loss: 32; attrition: 27% |
| Selective reporting (reporting bias) | Low risk | No protocol was identified, but all stated results re outcomes appear to have been included |
| Other bias | Low risk | None noted |
Nalbant 2011.
| Methods |
Study design: RCT (2 groups) |
|
| Participants |
Setting: nursing home residents in Turkey Inclusion criteria:
Exclusion criteria:
Participant status: Age (years): RG: 73.5; CG: 68 Gender (M/F): RG: 11/3; CG: 13/2 FEV1/FVC (Range): RG: 58.5 (48‐65); CG: 57 (44‐66) Participants randomly assigned: Randomised: 29 (RG: 14, CG: 15) Analysed: Rehab: 10 Control: 11 |
|
| Interventions |
Pulmonary rehabilitation: Aerobic exercise, ULE, LLE, educational material Duration: 6 months, 3 days a week for 1.5 hours Usual care |
|
| Outcomes |
Assessment: baseline, 3 months and 6 months 6MWT, lower extremity strength test |
|
| Notes | Note: Only medians and ranges provided, so cannot be used in analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not provided |
| Allocation concealment (selection bias) | Unclear risk | Not provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, unable to blind participants and those providing intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not provided |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 29 people were randomly assigned 21 completed; loss of 8 people Attrition: 28% |
| Selective reporting (reporting bias) | Low risk | No protocol was identified, but seems to have included all results re outcomes stated |
| Other bias | Low risk | None noted |
O'Shea 2007.
| Methods |
Study design: RCT (2 groups); single‐ blind randomised trial |
|
| Participants |
Setting: 4 sites including 3 regional health services and 1 large metropolitan hospital; Australia Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 66.9 ± 7: CG: 68.4 ± 9.9 Gender (M/F): RG:CG FEV1 % (pred): RG: 49; CG: 52 FEV1/FVC: RG: 50; CG: 49 Hx smoking per day: RG: 40; CG: 26.5 Participants randomly assigned: Randomised: 54 (27 to each group) Analysed: Rehab: 20 Control: 24 |
|
| Interventions |
Pulmonary rehabilitation: outpatient clinic and home based: under the supervision of an experienced physiotherapist; progressive resistance exercise programme ULE, LLE Duration: 12 weeks: 1 session per week facilitated, 2 sessions performed independently at home Usual care: Control group received no intervention |
|
| Outcomes |
Assessment: baseline and 3 months and 6 months CRDQ, 6MWT, Timed Up and Go Test, Grocery Shelving Test, Patient‐Specific Functional Scale, participation restrictions: London Handicap Scale, hand‐held dynamometry |
|
| Notes | Utilised data at 3 months for analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Generated by member of the research team not involved in participant recruitment |
| Allocation concealment (selection bias) | Low risk | Concealed allocation |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants and those delivering the intervention were aware of which individuals were included in the intervention group |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Assessor blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Commenced: 54; loss: 44 Attrition: 19% |
| Selective reporting (reporting bias) | Low risk | No protocol was identified, but all results re stated outcomes appear to have been included |
| Other bias | High risk | All male |
Ozdemir 2010.
| Methods |
Study design: RCT (2 groups): water based exercise (WE) and control |
|
| Participants |
Setting: Chest Diseases Outpatient Clinic between April 2006 and November 2006; Turkey Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 60.9 ± 8.8; CG: 64.1 ± 8.9 Gender (M/F): all male FEV1 % (pred ± SD): RG: 54.5 ± 15.6; CG: 54.1 ± 20.2 FEV1/FVC (± SD) : RG: 56.0 ± 10.5; CG: 54.6 ± 9.1 Smoker: RG: 5 (20%); CG: 6 (24%) Participants randomly assigned: Randomised: 50 (25 in each) Analysed: Rehab: 25 Control: 25 |
|
| Interventions |
Pulmonary rehabilitation: out‐patient; water‐based exercise (WE) Aerobic exercise, ULE, LLE Duration: 4‐Week water‐based pulmonary rehabilitation for 35 minutes 3 times a week Usual care: received only medical therapy |
|
| Outcomes |
Assessment: baseline and 1 month Spirometry, 6MWT, CRDQ, HAD Scale, arterial blood gas examination |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | According to "tables of random numbers" |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention were aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No information provided |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No attrition reported |
| Selective reporting (reporting bias) | High risk | No protocol was identified, but results for CRQ of rehabilitation group were not provided |
| Other bias | Low risk | None noted |
Paz‐Diaz 2007.
| Methods | Study design: RCT (2 groups) | |
| Participants |
Setting: recruited from the pulmonary clinic at the University Hospital of Caracas Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 67 ± 5; CG: 62 ± 7 Gender (M/F): RG: 6/4; CG: 12/2 FEV1 % (pred ± SD): RG: 34 ± 11; CG: 30 ± 9 FEV1/FVC (± SD): RG: 39 ± 7; CG: 30 ± 9 Participants randomly assigned: Randomised: 24 (PG: 10; CG: 14) Analysed: 24 Rehab: 10 Control: 14 |
|
| Interventions |
Pulmonary rehabilitation: out‐patient programme (hospital‐based PR) Aerobic exercise, ULE, LLE Duration: 8‐Week programme 3 days per week in groups of 2 or 3 Usual care: Control group received optimal care, as suggested by the American Thoracic Society |
|
| Outcomes |
Assessment: baseline and Immediately after PR (8 weeks) Spirometry, Beck Depression Inventory, State Trait Anxiety Inventory, MRC Scale, SGRQ |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not informed |
| Allocation concealment (selection bias) | Unclear risk | Not informed |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention were aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not informed |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Commenced: 24 (control: 14; intervention: 10) No loss reported |
| Selective reporting (reporting bias) | High risk | No protocol was identified, but results for the rehabilitation group for CR were not provided |
| Other bias | Low risk | None noted |
Petty 2006.
| Methods | Study design: RCT (3 groups): randomised tailored videotape, standard videotape, control | |
| Participants |
Setting: physician referrals from private offices, the Denver office of Kaiser Permanente and the Denver Veterans Affairs Medical Center Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: [customised video: 68.8 ± 9.2; standard video: 68.4 ± 9.0]; CG: 66.8 ± 9.9 Gender (M): RG:[customised video: 39 (54.2%); standard video: 41 (59.4%)]; CG: 40 (54.8%) Current smoker: RG:[ customised video: 10 ± 14.3%); standard video: 18 ± 26.5%]; CG: 22 ±30.1% Participants randomly assigned: Randomised: 214 (customised video: 72; standard video: 69; control: 73) Analysed: Rehab: customised video: 52; standard video: 62 Control: 61 |
|
| Interventions |
Pulmonary rehabilitation: home‐based programme (in home): a tailored videotape (Group A) and a standard videotape (Group B) Aerobic exercise, ULE, LLE, educational material, home physio visits Duration: 8 weeks Usual care |
|
| Outcomes |
Assessment: baseline and 8 weeks Fatigue Impact Scale (FIS), Seattle Obstructive Lung Questionnaire (SOLQ), SF‐36, 6MWD |
|
| Notes | Data could not be analysed, as full results were not available | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomly assigned to 1 of 3 groups in a blocked fashion to achieve balance |
| Allocation concealment (selection bias) | Unclear risk | Not known |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention were aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Self‐completion by participants |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Randomly assigned: 214; completed: 174 Attrition: 40 (19%) |
| Selective reporting (reporting bias) | High risk | No protocol was identified Results of the 6‐minute walk test and SF‐36 not presented |
| Other bias | Unclear risk | None noted |
Reardon 1994.
| Methods | Study design: RCT (2 groups) | |
| Participants |
Setting: out‐patient; Connecticut Inclusion criteria:
Exclusion criteria:
Participant status: Age (yearsn): RG: 66.3; CG: 66.1 Gender (M/F): RG: 5/5; CG: 5/5 FEV1 % (pred ± SD): RG: 35% ± 10; CG: 33% ± 15 Participants randomly assigned: Randomised: 20 Analysed: Rehab: 10 Control: 10 |
|
| Interventions |
Pulmonary rehabilitation: outpatient LLE, ULE, BE, Edu, Psy Duration: 6 weeks (12 three‐hour sessions) Usual care: session with the OPR nurse clinician for optimisation of pulmonary therapy |
|
| Outcomes |
Assessment: baseline and 6 weeks ITT, BDI/TDI, 12MWD |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: random numbers table |
| Allocation concealment (selection bias) | Unclear risk | Not informed |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention were aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessments: blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No participant loss after allocation |
| Selective reporting (reporting bias) | Low risk | No trial registration protocol was found at www.controlled‐trials.com/mrct/ or www.who.int/trialsearch (searched for author names and parts of title of paper or intervention). However it would seem that all outcomes stated in the study were measured |
| Other bias | Low risk | None noted |
Ringbaek 2000.
| Methods |
Study design: RCT (2 groups) Randomisation process: sealed envelopes Outcome assessments: blinded |
|
| Participants |
Setting: delivered as an outpatient programme in Denmark Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 61.8 ± 6.8; CG: 64.6 ± 7.7 Gender (M/F): RG: 1/23; CG: 6/15 FEV1 % (pred ± SD): RG: 49.5 ± 17.4; CG: 44.3 ± 3.7 Current smoking: RG: 16; CG: 7 Participants randomly assigned: Randomised: 45 (RG: 24; control: 21) Analysed: Rehab: 17 Control: 19 (130 approached; 45 randomised) |
|
| Interventions |
Pulmonary rehabilitation: out‐patient (hospital) Aerobic, LLE, ULE, education, nutritional support Duration: 8 weeks, 2 sessions a week of 2 hours Usual care: conventional community care |
|
| Outcomes |
Assessment: baseline and 8 weeks 6‐Minute WT, SGRQ, Psychological General Well‐being (PGWB), Borg Scale |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: sealed envelopes |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention were aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessments: blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Overall commenced: 45; finished: 36 (84.4%) Overall attrition: 7 (15.6%) |
| Selective reporting (reporting bias) | Low risk | No trial registration protocol was found at www.controlled‐trials.com/mrct/ or www.who.int/trialsearch (searched for author names and parts of title of paper or intervention). However it would seem that all outcomes stated in the study were measured |
| Other bias | Low risk | None noted |
Simpson 1992.
| Methods | Study design: RCT (2 groups), stratified | |
| Participants |
Setting: out‐patient Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD ): RG: 73 ± 4.8; CG: 70 ± 5.7 Gender (M/F): RG: 5/9; CG: 10/4 FEV1 % (pred ± SD): RG: 39.5 ±18.96; CG: 39.2 ± 21.39 FEV1/FVC: RG: 49.4 (12.95); CG: 47.8 (14.04) Participants randomly assigned: Randomised: 34 Analysed: Rehab: 14 Control: 14 |
|
| Interventions |
Pulmonary rehabilitation: Weight‐lifting programme training was prescribed for upper and lower limb muscles; resistance was increased progressively LLE, ULE Duration: 8 weeks 3 times a week Usual care: Control group attended only for testing |
|
| Outcomes |
Assessment: baseline and 8 weeks 6MWT, ICET, SSCET, CRQ |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: coin toss |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention were aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessments: blinded for CRQ, not blinded for the others |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 28/34 completed = 82.3% Attrition: 17.64% |
| Selective reporting (reporting bias) | Low risk | No trial registration protocol was found. However it would seem that all outcomes stated in the study were measured |
| Other bias | Low risk | None noted |
Singh 2003.
| Methods |
Study design: RCT (2 groups) |
|
| Participants |
Setting: home based, carried out by Department of Medicine, SMS Medical College and Hospital, Jaipur, India Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): 59.3 ± 6.4 Gender (M/F): male 32 (80%), female 8 (20%) FEV1 % (pred ± SD ): RG: 28 ± 7.5; CG: 26 ± 7.1 FEV1/FVC (±SD): RG: 44 ± 16; CG: 48 ± 10.4 Participants randomly assigned: Randomised: 40 Analysed: Rehab: 20 Control: 20 |
|
| Interventions |
Pulmonary rehabilitation: domiciliary pulmonary rehabilitation for 4 weeks; supervised weekly to ensure that participants were following the rehabilitation schedule properly and were taking regular treatment LLE, IMT Duration: 4 weeks 30 minutes twice a day Usual care: Control group participants were asked to continue their activities as usual |
|
| Outcomes |
Assessment: baseline and 4 weeks CRQ, 6MWT |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: random numbers table |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention were aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcome assessments: not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No attrition |
| Selective reporting (reporting bias) | Low risk | All outcomes appearing in the controlled trial registry (clinicaltrials.gov) seem to have been reported on in the paper |
| Other bias | Low risk | None reported |
Sridhar 2008.
| Methods |
Study design: RCT (2 groups) |
|
| Participants |
Setting: community and hospital care in West London Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD ): RG: 69.9 ± 9.6; CG: 69.68 ± 10.4 Gender (M/F): RG: 30/31; CG: 30/31 FEV1 % (pred ± SD): RG: 42.9 ±15.5; CG: 48.9 ± 18.69 FEV1/FVC: RG:CG Current smoker (Y/N): RG: 18/61; CG: 12/61 Participants randomly assigned: Randomised: 122 Analysed: Rehab: 47 Control: 40 |
|
| Interventions |
Pulmonary rehabilitation: outpatient followed by home package Aerobic exercise, ULE, LLE, educational material, home physio visits Duration: 4 weeks, 2 attendances per week (1 hour of education, 1 hour of physical training) followed by 3 monthly home visits Usual care: Control group received usual care from primary care physician |
|
| Outcomes |
Assessment: baseline and 6 months CRQ, hospital readmission rate |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomly assigned with the use of random numbers to intervention or control group |
| Allocation concealment (selection bias) | Unclear risk | Not informed |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention were aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcome assessments: not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Commenced: 122; outcome data for 104 Attrition: 18 (15%) |
| Selective reporting (reporting bias) | Low risk | No trial registration protocol was found. However it would seem that all outcomes stated in the study were measured |
| Other bias | Unclear risk | None reported |
Strijbos 1996.
| Methods |
Study design: RCT (3 groups) |
|
| Participants |
Setting: out‐patient Inclusion criteria: Exclusion criteria: Participant status: Age (years ± SD ): RG: 61 ± 6 ; CG: 63 ± 5 Gender (M/F): RG: 14/1; CG: 12/3 FEV1 % (pred ± SD): RG: 40.4 ±19.6; CG: 42.6 ± 8.8 Participants randomly assigned: Randomised: 32 Analysed: Rehab: 15 Control: 15 |
|
| Interventions |
Pulmonary rehabilitation: hospital‐based outpatient pulmonary rehabilitation programmes (HRPa) are compared with those of a 12‐week home care rehabilitation programme (HCRP) LLE, BE, PD, Edu, Psy Duration: 12 weeks twice a week for 1‐hour session Usual care: Control group received no rehabilitation therapy |
|
| Outcomes |
Assessment: baseline, 3 months, 6 months, 12 months and 18 months 4‐Minute WT, ICET, interviews |
|
| Notes | Utilised 3‐month results for analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Lottery procedure used to determine which group participants allocated to. |
| Allocation concealment (selection bias) | Unclear risk | No information related to allocation concealment provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention would be aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessments: blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Started 50; finished 45; attrition at 3 months: 5 (10%) |
| Selective reporting (reporting bias) | Low risk | No trial registration protocol was found. However it would seem that all outcomes stated in the study were measured |
| Other bias | Low risk | None noted |
Theander 2009.
| Methods |
Study design: RCT (2 groups) |
|
| Participants |
Setting: pulmonary out‐patient department in a central county district of Sweden Inclusion criteria:
Exclusion criteria:
Participant status: Age (years): RG: 66; CG: 64 Gender (M/F): RG: 3/9; CG: 10/4 FEV1 % (pred ± SD): RG: 35.1 ± 7.6; CG: 32.3 ± 9.5 Smokers: 3 in each group currently smoking Participants randomly assigned: Randomised: 30 Analysed: Rehab: 12 Control: 14 |
|
| Interventions |
Pulmonary rehabilitation: out‐patient programme (hospital based followed by home based), multi‐disciplinary; comprising a physiotherapist, a dietician, an occupational therapist and a nurse. After 1 month, individualised home exercise added Aerobic exercise, ULE, LLE, breathing exercises, educational material, nutrition Duration: 12 weeks 2 days per week,1 hour long Usual care: Control group received none of the multi‐disciplinary rehabilitation programmes and no care from multi‐disciplinary professionals |
|
| Outcomes |
Assessment: baseline and 12 weeks 6MWD, SQRQ, hand grip strength and health perception, fatigue, functional limitations due to fatigue, functional performance and satisfaction |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation procedures were performed by an independent person from the research group, who took a random envelope from the prepared box with sealed envelopes |
| Allocation concealment (selection bias) | Low risk | For this purpose, we prepared 80 sealed opaque envelopes with assignment information |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention would be aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Data collection was performed by members of the rehabilitation group. Data collected were not blinded to the data collector |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 26/30 complete data for analysis 4/30 lost to follow‐up = 13.33% |
| Selective reporting (reporting bias) | Low risk | No trial registration protocol was found. However it would seem that all outcomes stated in the study were measured |
| Other bias | Low risk | None noted |
Vallet 1994.
| Methods | Study design: RCT (2 groups) | |
| Participants |
Setting: in‐patient; France Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD ): RG: 59.6 ± 2.75; CG: 58.2 ± 1.8 Gender (M/F): RG: 7/3; CG: 8/2 FEV1/FVC: RG: 57.2; CG: 55.7 Participants randomly assigned: Randomised: 22 Analysed: Rehab: 10 Control: 10 |
|
| Interventions |
Pulmonary rehabilitation: in‐patient rehabilitation LLE, BE Duration: 8 weeks Usual care |
|
| Outcomes |
Assessment: baseline and 2 months ICET QoL: not measured |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: drawing lots Outcome assessments: not blinded |
| Allocation concealment (selection bias) | Unclear risk | No information related to allocation concealment provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention would be aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcome assessments: not blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 18/20 (90%) completed |
| Selective reporting (reporting bias) | Low risk | No trial registration protocol was found. However it would seem that all outcomes stated in the study were measured |
| Other bias | Low risk | None noted |
Van Wetering 2010.
| Methods |
Study design: RCT (2 groups) |
|
| Participants |
Setting: Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 65.9 ± 8.8; CG: 67.2 ± 8.9 Gender (M/F): 71% male in each group FEV1 % (pred ± SD): RG: 58 ±17; CG: 60 ±15 FEV1/FVC: RG: 49 ±11; CG: 36.1 ± 26.4 Current smokers (%): RG: 33%; CG: 24% Participants randomly assigned: Randomised: 199 Analysed: Rehab: 87 Control: 88 |
|
| Interventions |
Pulmonary rehabilitation: community (primary care setting) Standardised supervised rehabilitation phase and a 20‐month active maintenance phase Aerobic exercise, ULE, LLE, educational material Duration: Initally 4‐Month, followed by 20‐month active maintenance phase (twice a day during 30 minutes) Usual care: received pharmacotherapy according to accepted guidelines |
|
| Outcomes |
Assessment: baseline and 4 months (immediately after initial intervention) SGRQ, cycle endurance test (CET), 6MWD, muscle strength (handgrip force (HGF), isometric quadriceps peak torque (QPT), maximal inspiratory mouth pressure (Pimax)), 17 body composition (FFM) |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Care provided through a computerised procedure with concealed participant allocation |
| Allocation concealment (selection bias) | Low risk | Programme or usual care through a computerised procedure with concealed participant allocation |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention would be aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All measurements were assessed single‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Loss = 24 (12%) (intervention: 15 (4.7%); control: 9 (9.2%)) 88% completed, so 12% attrition |
| Selective reporting (reporting bias) | Low risk | From protocol paper (http://clinicaltrials.gov/ct2/show/NCT00840892), outcomes matched those in the protocol paper |
| Other bias | Low risk | None noted |
Vijayan 2010.
| Methods | Study design: RCT (2 groups) | |
| Participants |
Setting: India Inclusion criteria:
Exclusion criteria: Participant status: Age (years): not provided Gender: not provided FEV1 %: not provided FEV1/FVC: not provided Participants randomly assigned: Randomised: 31 (15 control; 16 intervention) Analysed: Rehab: 16 Control: 15 |
|
| Interventions |
Pulmonary rehabilitation: not informed of venue Aerobic exercise, ULE, LLE Duration: 8 weeks (5 days a week for 90 minutes) Usual care: Both groups had medication adjusted for 8 weeks |
|
| Outcomes |
Assessment: baseline 6‐Minute walk test (Only relevant test) |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No Information |
| Allocation concealment (selection bias) | Unclear risk | No details provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention would be aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details provided |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No attrition reported |
| Selective reporting (reporting bias) | Unclear risk | Insufficent details provided |
| Other bias | High risk | Very superficial information available in relation to the study, precluding good quality assessment |
Weiner 1992.
| Methods |
Study design: RCT (3 groups): SIMT group received threshold inspiratory muscle trainer and exercise programme, exercise training group and control randomly matched to 3 groups according to the following criteria: age; FEV1; and FEV1/FVC |
|
| Participants |
Setting: out‐patient; Isreal Inclusion criteria:
Exclusion criteria: Participant status: Age (years ± SD): RG: 64.4 ± 3; CG: 62.3 ± 2.4 Gender (M/F): RG: 6/6; CG: 5/7 FEV1 % (pred ± SD): RG: 32.8 ± 3; CG: 39.2 ± 2.8 Participants randomly assigned: Randomised: 24 Analysed: Rehab: 12 Control: 12 |
|
| Interventions |
Pulmonary rehabilitation: out‐patient (hospital) Performed under the supervision of a physiotherapist LLE, ULE, IMT, BE Duration: 6 months, 3 times a week, each session consisting of 1 hour of training Usual care: no additional treatment |
|
| Outcomes |
Assessment: baseline and 6 months 12‐Minute WT, ICET, SSCET QoL: not measured |
|
| Notes | 1 exercise only group used in the analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: random numbers table |
| Allocation concealment (selection bias) | Unclear risk | No information related to allocation concealment provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention would be aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessments: blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No loss to follow‐up |
| Selective reporting (reporting bias) | High risk | No trial registration protocol was found. Results of SGRQ not available |
| Other bias | Low risk | None noted |
Wen 2008.
| Methods |
Study design: RCT (3 groups) High‐intensity group Anaerobic threshold group Control group |
|
| Participants |
Setting: out‐patient clinic in China Inclusion criteria:
Exclusion criteria:
Participant status: Age (years± SD): RG: [ATG: 67 ± 7; HIG: 68 ± 7]; CG: 66 ± 10 Gender (M/F): all male with exception of 1 FEV1% (pred ± SD): RG:[ ATG: 46 ± 10; HIG: 50 ± 14;] CG: 52 ± 14 Participants randomly assigned: Randomised: 41 (high‐intensity group: 17; anaerobic threshold group: 15; control group: 9) Analysed: Rehab: High‐intensity group: 17; anaerobic threshold group: 15 Control: 9 |
|
| Interventions |
Pulmonary rehabilitation: bicycle exercise training Aerobic exercise, LLE Duration: 12 weeks, 2 days a week Usual care |
|
| Outcomes |
Assessment: baseline and 12 weeks SGRQ, Borg/Max Oxygen Intake |
|
| Notes | No results available for the SGRQ | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No Information |
| Allocation concealment (selection bias) | Unclear risk | No details provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention would be aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details provided |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 54 randomly assigned, 13 lost Attrition: 24% |
| Selective reporting (reporting bias) | Low risk | No trial registration protocol was found. However it would seem that all outcomes stated in the study were measured |
| Other bias | Low risk | None noted |
Wijkstra 1994.
| Methods | Study design: RCT (2 groups), stratified | |
| Participants |
Setting: home based Inclusion criteria:
Exclusion criteria:
Participant status: Age (years ± SD): RG: 64 ± 5; CG: 62 ± 5 Gender (M/F): RG: 23/5; CG: 14/1 FEV1% (pred ± SD): RG: 44 ± 11; CG: 45 ± 9 FEV1/FVC (± SD): RG: 39 ± 8; CG: 36 ± 7 Participants randomly assigned: Randomised: 45 (RG: 30; CG: 15) Analysed: Rehab: 28 Control: 15 |
|
| Interventions |
Pulmonary rehabilitation: out‐patient clinic and home based: progressive physiotherapy programme LLE, ULE, IMT, BE, Edu, Psy, nurse home visited Duration: 12 weeks, twice a week In addition, participants had to practice twice a day for half an hour at home Usual care: Control group did not follow the above mentioned protocol |
|
| Outcomes |
Assessment: baseline and 12 weeks 6‐Minute WT, ICET CRQ |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: stratified randomisation |
| Allocation concealment (selection bias) | Unclear risk | No details provided |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention would be aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Not blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 43/45 = 95.6% completed Attrition rate: 4.4% |
| Selective reporting (reporting bias) | Low risk | No trial registration protocol was found. However it would seem that all outcomes stated in the study were measured |
| Other bias | Low risk | None noted |
Xie 2003.
| Methods |
Study design: RCT (2 groups) |
|
| Participants |
Setting: home‐based affiliated central hospital of Jilin Medical College, China Inclusion criteria:
Exclusion criteria:
Participant status: Age (years± SD): RG: 54 ±6; CG: 54 ± 6 Gender (M/F): RG: 22/3; CG: 21/4 FEV1% (pred ± SD): RG: 41.8 ± 15; CG: 40 ± 16.5 FEV1/FVC(±SD): RG: 40.3 ± 9.3; CG: 42.3 ± 12.1 Participants randomly assigned: Randomised: 50 Analysed: Rehab: 25 Control: 25 |
|
| Interventions |
Pulmonary rehabilitation: 1 home rehabilitation walking programme; training intensity was individually determined LLE Duration: 12 weeks, 6 days a week, duration of 1 hour Usual care: Control group participants (medical treatment alone) also made visits to the hospital every 2 weeks for clinical checkup |
|
| Outcomes |
Assessment: baseline and 12 weeks ICE, SWT, dyspnoea, lung function, blood gas |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: random numbers table |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As a result of the nature of the intervention, both participants and those delivering the intervention would be aware of allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcome assessments: not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No mention of attrition |
| Selective reporting (reporting bias) | Low risk | No trial registration protocol was found. However it would seem that all outcomes stated in the study were measured |
| Other bias | Low risk | None noted |
6MWT: six‐minute walk test; BDI/TDI: baseline dyspnoea index/transition dyspnoea index; BE: breathing exercises; CRQ: Chronic Respiratory Disease Questionnaire; Edu: education; IAET: incremental arm ergometer test; ICET: incremental cycle ergometer test; IMT: inspiratory muscle training; ITT: incremental treadmill test; LLE: lower limb exercise; NEADL: Nottingham Extended Actvities of Daily Living scale; PD: postural drainage; POMS: profile of mood state; Psy: psychological support; QoL: quality of life; SGRQ: St. George's Respiratory Questionnaire; SIP: sickness impact profile; SSCET: steady‐state cycle ergometer test; SSTT: steady‐state treadmill test; ULE: upper limb exercise; WT: walk test; HADS: Hospital Anxiety Depression Scale.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Akinci 2011 | Not a randomised controlled trial |
| Ambrosino 1981 | Experimental group did not receive exercise training |
| Ambrosino 2006 | Control group does not receive 'usual care' |
| Amin 2011 | Control group does not receive 'usual care' |
| Arnadottir 2001 | Control group does not receive 'usual care' |
| Backer 2003 | Control group does not receive 'usual care' |
| Bauldoff 1996 | Control group does not receive 'usual care' |
| Bauldoff 2002 | Wrong aim |
| Behnke 2002 | No control group |
| Behnke 2002a | Control group does not receive 'usual care' |
| Behnke 2003 | No control group |
| Bernard 1999 | Control group does not receive 'usual care' |
| Berry 1996 | Control group does not receive 'usual care' |
| Bjerre‐Jepsen 1981 | No physical exercise component |
| Bourbeau 2000 | No physical exercise component |
| Bourjeily‐Habr 2002 | No physical exercise component |
| Breyer 2010 | Control group does not receive 'usual care' |
| Brooks 2000 | Control group does not receive 'usual care' |
| Böhning 1990 | Wrong comparison |
| Cai 2003 | No physical exercise component |
| Carrieri‐Kohlman 96 | Control group does not receive 'usual care' |
| Cegla 2002 | No physical exercise component |
| Chen 2011 | Control group does not receive 'usual care' |
| Ciric 2008 | Not a randomised controlled trial |
| Clark 2000 | FEV1 higher than 70% of predicted |
| Cockcroft 1985 | Control group does not receive 'usual care' |
| Coppoolse 1999 | Control group does not receive 'usual care' |
| Covey 2004 | Not a randomised controlled trial (review article) |
| Cox 1993 | Not a randomised controlled trial |
| de Blasio 2000 | Not a randomised controlled trial (editorial) |
| de Lucas Ramos 1998 | Experimental group does not receive exercise training |
| Dekhuijzen 1990 | Control group does not receive 'usual care' |
| Dekhuijzen 1991 | Control group does not receive 'usual care' |
| Demir‐Deriven 2001 | Control group does not receive 'usual care' |
| Demir‐Deriven 2002 | Wrong comparison (men compared with women) |
| Dewse 1998 | Not a randomised controlled trial (review article) |
| Di Marzo 2000 | No physical exercise component |
| Downes Vogel 2002 | No physical exercise component |
| Dushianthan 2009 | Not a randomised controlled trial (review article) |
| Egan 2012 | Not a randomised controlled trial |
| Ellum 2002 | Wrong comparison (effect of posture on dyspnoea) |
| Emtner 1998 | Not COPD |
| Epstein 1997 | Control group does not receive 'usual care' |
| Esteve 1996 | Control group does not receive 'usual care' |
| Fan 2008 | Control group does not receive 'usual care' |
| Foglio 2001 | Control group does not receive 'usual care' |
| Gadoury 2005 | Control group does not receive 'usual care' |
| Gale 2009 | Not a randomised controlled trial |
| Garuti 2010 | Not a randomised controlled trial (review article) |
| Gautier 1998 | Control group does not receive 'usual care' |
| Gautier 2002 | Control group does not receive 'usual care' |
| Ghanem 2010 | Participants not clearly 4 weeks post exacerbation |
| Gimenez 2000 | Control group does not receive 'usual care' Quasi‐randomisation |
| Girodo 1992 | Not COPD |
| Goldman 1997 | FEV1 is higher than 70% predicted |
| Gormley 1993 | Control group does not receive 'usual care' |
| Gosselink 1990 | Control group does not receive 'usual care' |
| Green 1999 | Control group does not receive 'usual care' |
| Griffiths 1996 | Control group does not receive 'usual care' |
| Grosbois 1999 | Control group does not receive 'usual care' |
| Gu 2011 | No physical exercise component |
| Guell 2006 | Control group does not receive 'usual care' |
| Harver 1989 | Experimental group did not receive exercise training |
| Hawkins 1999 | No physical exercise component |
| Hentschel 2002 | Control group does not receive 'usual care' |
| Holland 2003 | Control group does not receive 'usual care' |
| Hospes 2009 | No physical exercise component |
| Houchen 2011 | Control group does not receive 'usual care' |
| Innocenti 2000 | Control group does not receive 'usual care' |
| Jensen 1983 | No physical exercise component |
| Johnson 2000 | Control group does not receive 'usual care' |
| Jungblut 2007 | Not a randomised controlled trial |
| Kaplan 1990 | Control group does not receive 'usual care' |
| Katsura 2000 | Control group does not receive 'usual care' |
| Kurabayashi 1998 | Experimental group does not receive exercise training |
| Kurabayashi 2000 | Experimental group does not receive exercise training |
| Larson 1999 | Control group does not receive 'usual care' |
| Lathlean 2008 | Randomisation unclear |
| Laukandt 1998 | Control group does not receive 'usual care' |
| Levine 1986 | Wrong comparison |
| Lewczuk 1998 | Not a randomised controlled trial |
| Li 2002 | No physical exercise component |
| Liu 2002 | Randomisation unclear |
| Lotshaw 2003 | Control group does not receive 'usual care' |
| Ma 2002 | Control group does not receive 'usual care' |
| Mador 2002 | Healthy controls |
| Mador 2004 | Control group does not receive 'usual care' |
| Make 2000 | Non‐randomised comparison |
| Martinez 1993 | Control group does not receive 'usual care' |
| McKeogh 2012 | Control group does not receive 'usual care' |
| Morgan 1999 | Not a randomised controlled trial (review) |
| Moros Garcia 1996 | Not randomised |
| Morris 2003 | Control group does not receive 'usual care' |
| MTU 2003 | Systematic review |
| Murphy 2004 | Control group does not receive 'usual care' |
| Myers 2000 | Enhancement strategy |
| Na 2005 | Not a randomised controlled trial |
| Nasilowski 2011 | Not a randomised controlled trial |
| Nava 1998 | Unstable patients (wrong population) |
| Ndundu 2001 | Case series |
| Neder 2002 | Control group does not receive 'usual care' |
| Newall 2000 | Control group does not receive 'usual care' |
| Nguyen 2005 | Control group does not receive 'usual care' |
| Ninot 2011 | Outcomes measured longer than 3 months after the end of the intervention |
| Nosworthy 1992 | Control group does not receive 'usual care' |
| Nygren‐Bonnier 2002 | Control group does not receive 'usual care' |
| O'Hara 1987 | Not a randomised controlled trial |
| Ortega 2002 | Control group does not receive 'usual care' |
| Patessio 1994 | Control group does not receive 'usual care' |
| Petersen 2008 | Control group does not receive 'usual care' |
| Piantadosi 2000 | No randomised comparison between PR and control group |
| Pison 2001 | Not a randomised controlled trial (review article) |
| Pison 2008 | Control group does not receive 'usual care' |
| Pitta 2004 | Not a randomised controlled trial |
| Ponsioen 2010 | Not a randomised controlled trial (review article) |
| Prince 1989 | Control group does not receive 'usual care' |
| Probst 2003 | Acute effect of walking aid on exercise capacity |
| Proshchaev 2009 | Control group does not receive 'usual care' |
| Puente 1996 | 2 types of training compared |
| Raschke 1990 | Not randomised |
| Regiane Resqueti 2007 | Control group does not receive 'usual care' |
| Reilly 2000 | NETT trial does not meet entry criteria for the review |
| Riario‐Sforza 2009 | Randomisation unclear |
| Ries 1986 | Control group does not receive 'usual care' |
| Ries 1988 | Control group does not receive 'usual care' |
| Ries 1995 | Control group does not receive 'usual care' |
| Roberts 1999 | Control group does not receive 'usual care' |
| Rooyackers 1996 | Control group does not receive 'usual care' |
| Rudkin 1997 | Control group does not receive 'usual care' |
| Santiworakul 2009 | Randomisation unclear |
| Sassi‐Dambron 1995 | Experimental group does not receive exercise training |
| Saunders 1965 | No physical exercise component |
| Scherer 1998 | Control group does not receive 'usual care' |
| Scorsone 2010 | Control group does not receive 'usual care' |
| Semenyuk 2007 | No physical exercise component |
| Serres 1997 | Inadequate duration (shorter than 4 weeks) |
| Sewell 2005 | Control group does not receive 'usual care' |
| Sinclair 1980 | Not a randomised controlled trial |
| Sindhwani 2011 | Not a randomised controlled trial |
| Sivori 1998 | Control group does not receive 'usual care' |
| Solanes Garcia 2004 | Randomisation unclear |
| Sparrow 1997 | Control group does not receive 'usual care' |
| Spruit 2001 | Control group does not receive 'usual care' |
| Steele 2008 | Control group does not receive 'usual care' |
| Stellefson 2009 | Not an exercise programme |
| Sudo 1997 | Control group does not receive 'usual care' |
| Sugawara 2007 | Control group does not receive 'usual care' |
| Sun 2003 | No physical exercise component |
| Swerts 1990 | Control group does not receive 'usual care' |
| Taylor 2012 | Not an exercise programme |
| Toevs 1984 | Control group does not receive 'usual care' |
| Troosters 1999 | Not a randomised controlled trial (review article) |
| Tsang 2001 | Control group does not receive 'usual care' |
| Ubaidullayev 1990 | No physical exercise component |
| Vargas 1998 | No physical exercise component |
| Vogiatzis 1999 | Treatment allocation not randomised |
| Vogiatzis 2001 | Control group does not receive 'usual care' |
| Vogiatzis 2002 | Control group does not receive 'usual care' |
| Wadell 2005 | Not a randomised controlled trial |
| Wadell 2013 | Control group does not receive 'usual care' |
| Wanke 1994 | Control group does not receive 'usual care' |
| Wedzicha 1998 | Control group does not receive 'usual care' |
| Weiner 1992a | Not COPD |
| Wen 2004 | Participants not clearly 4 weeks post exacerbation and length of intervention unclear |
| White 2002 | Control group does not receive 'usual care' |
| Worth 1985 | Not randomised |
| Xu 2010 | Length of programme unclear |
| Yamanaka 2009 | Not a randomised controlled trial |
| Yan 1996 | Experimental group does not receive exercise training |
| Yosbauran 1996 | Control group does not receive 'usual care' |
| Zanini 2002 | Control group does not receive 'usual care' |
| Zhang 2008 | No physical exercise component |
COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in one second; NETT: National Emphysema Treatment Trial; PR: pulmonary rehabilitation.
Characteristics of studies awaiting assessment [ordered by study ID]
Aksu 2006.
| Methods | 3 groups |
| Participants | 58 participants |
| Interventions |
Pulmonary rehab: aerobic exercise group; aerobic exercise plus isotonic strengthening exercise group; control group with no exercise Duration: 3 times per week for 12 weeks Usual care: not known |
| Outcomes |
Assessment: baseline and 12 weeks Exercise performance (measured by Bruce exercise tolerance test), 6MWT, dyspnoea scores, SGRQ, SF‐36, BMI and pulmonary function |
| Notes | Not possible to establish contact with study authors |
D'Amico 2010.
| Methods | Not known |
| Participants | RCT (2 groups) |
| Interventions |
Pulmonary rehabilitation: indoor aerobic training Duration: 3 days per week, 60 minutes each time, for 6 months Usual care: not known |
| Outcomes | Spirometry, oxygen saturation, ambulatory blood pressure measurement, health‐related quality of life (SF‐12) |
| Notes | Not possible to establish contact with study authors |
Meshcheryakova 2010.
| Methods | RCT (4 groups) |
| Participants | 57 participants |
| Interventions |
Pulmonary rehabilitation: physical training Duration: not known Usual care: standardised medication |
| Outcomes | 6‐Minute walk test, respiratory muscle strength, health‐related quality of life (SF‐36), lung function |
| Notes | Contact information: m_natalia1967@inbox.ru |
Meshcheryakova 2012.
| Methods | RCT (3 groups) |
| Participants | 45 participants |
| Interventions |
Pulmonary rehabilitation: a physical exercise programme Duration: not known |
| Outcomes | BMI, pulmonary function, 6MWT, shortness of breath, health‐related quality of life (SF‐36), systemic inflammation blood indicators, blood testosterone, muscle power and depression |
| Notes | Contact information: m_natalia1967@inbox.ru |
Ren 2011.
| Methods | RCT (3 groups) |
| Participants | 89 patients with COPD, divided into groups according to severity of COPD |
| Interventions |
Pulmonary rehabilitation: 2 different programmes used for 20 weeks Usual care: not known |
| Outcomes |
Assessment: baseline and 20 weeks 6MWT, BODE Index, acute exacerbation frequency, Modified Medical Research Council Scale, BMI and pulmonary function (FEV1) |
| Notes | Not possible to establish contact with study authors |
6MWT: six‐minute walk test; BMI: body mass index; COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in one second; RCT: randomised controlled trial; SF: Short Form; SGRQ: St. George's Respiratory Questionnaire. Six studies were awaiting classification in the previous version of the review (Corrado 1995; Fernández 1998; Shu 1998; Tregonning 2000; Ward 1999; Wright 2002). The current search yielded no related publications since 2006 to allow us to clarify the status of these studies.
Characteristics of ongoing studies [ordered by study ID]
Chang 2008.
| Trial name or title | Pulmonary rehabilitation or self‐management (PRSM) for chronic obstructive pulmonary disease (COPD) |
| Methods | RCT (3 groups) Individual randomisation, blinded outcome assessment, 3‐monthly follow‐up assessments across a 12‐month period and concurrent economic evaluation |
| Participants | Target of 85 per group |
| Interventions | Stanford Chronic Disease Self‐Management programme vs multi‐factorial pulmonary rehabilitation group vs usual care provided by a GP |
| Outcomes | Primary outcome measure is St. George's Respiratory Disease Questionnaire Secondary outcome measures are measured by Frenchay Activities Index, International Physical Activity Questionnaire, the Hospital Anxiety and Depression Scale, the COPD Self‐Efficacy scale and 2 physiological measures (forced vital capacity in 1 second and an incremental shuttle walk) measured at baseline and at 3‐monthly intervals across 12 months. Also, spirometry and incremental shuttle walk at baseline and at 3 months |
| Starting date | April 2008 |
| Contact information | terrence.haines@monash.edu |
| Notes | Results not yet published |
Gurgun 2011.
| Trial name or title | Efficacy of an Eight‐Week Pulmonary Rehabilitation in COPD Patients: An Experience of a Single Center in Turkey |
| Methods | RCT (2 groups) |
| Participants | 152 stable patients with COPD |
| Interventions | 8‐Week pulmonary rehabilitation programme vs usual care |
| Outcomes |
Assessment: at 8 weeks Walking distance, perceived dyspnoea, health‐related quality of life, anxiety and depression |
| Starting date | Not known |
| Contact information | alev.gurgun@ege.edu.tr |
| Notes | Study still recruiting at the time of this review |
Sathyapala 2008.
| Trial name or title | Comparison of Repetitive Magnetic Stimulation (rMS) and Exercise Versus No Active Treatment on Quadriceps Function in Chronic Obstructive Pulmonary Disease (COPD) |
| Methods | RCT (3 groups) |
| Participants | 58 |
| Interventions |
Pulmonary rehabilitation: supervised 2‐hour resistance and endurance exercise programme twice a week for 8 weeks Repetitive magnetic stimulation of the intramuscular branches of the femoral nerve for 3 hours twice a week for 8 weeks Usual care: no intervention |
| Outcomes |
Assessment at 8 weeks Lung function, fat‐free mass, quadriceps strength, locomotion time and movement intensity over a 2‐day period |
| Starting date | 2007 |
| Contact information | m.polkey@imperial.ac.uk |
| Notes | Results not yet published |
One ongoing study in the previous version of the review (Whiteford 2004) remains unpublished.
Differences between protocol and review
In this current update, the following changes were made from the previous version.
-
We made the following changes to the inclusion and exclusion criteria.
-
We excluded randomised controlled trials that focused on participants:
who were ventilated; or
who had an acute exacerbation within four weeks before commencement of the intervention
We excluded interventions for which the physical activity component was considered to not be aerobically demanding (such as respiratory muscle training, breathing exercises, Tai Chi and yoga). The degree of aerobic demand was assessed for each individual intervention by examining the detailed description of the intervention in identified studies. We also excluded programmes of less than four weeks' duration.
-
We clarified what was considered usual care.
Contributions of authors
BMC and DC selected trials. BMC, DC, EM and KM extracted data. BMC, DC, EM, DD and KM assessed the methodological quality of trials. BMC was responsible for handling data in RevMan. BMC and DD designed the meta‐analysis. BMC and DD completed the clinical interpretation of results. YL provided support and guidance throughout the update and critically reviewed the final manuscript.
Declarations of interest
The review authors DC, BMC, KM and DD were involved in the PRINCE study conducted by Casey 2013, a cluster‐randomised trial that was included in this review. The risk of bias table for this study was therefore completed by two independent review authors, who were not involved in this trial but were experienced in conducting Cochrane systematic reviews. These were the review authors EM and Miriam Brennan, Lecturer at the School of Nursing & Midwifery, NUI Galway.
Edited (no change to conclusions)
References
References to studies included in this review
Barakat 2008 {published data only}
- Barakat S, Michele G, George P, Nicole V, Guy A. Outpatient pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. International Journal of COPD 2008;3(1):155‐62. [DOI] [PMC free article] [PubMed] [Google Scholar]
Baumann 2012 {published data only}
- Baumann HJ, Kluge S, Rummel K, Klose HF, Hennigs JK, Schmoller T, et al. Low intensity, long‐term outpatient rehabilitation in COPD: a randomised controlled trial. Respiratory Research 2012;13(1):86. [DOI] [PMC free article] [PubMed] [Google Scholar]
Behnke 2000a {published data only}
- Behnke M. The effects of a home‐based exercise training programme in patients with chronic obstructive lung disease [Die Wirkungen eines häuslichen Belastungstrainings bei Patienten mit chronisch‐obstruktiver Lungenerkrankung]. Pneumologie 1999;53:2‐3. [PubMed] [Google Scholar]
- Behnke M, Jörres RA, Kirsten D, Magnussen H. Clinical benefits of a combined hospital and home‐based exercise programme over 18 months in patients with severe COPD. Monaldi Archives for Chest Disease 2003;59(1):44‐51. [PubMed] [Google Scholar]
- Behnke M, Kirsten D, Jörres RA, Magnussen H. Home‐based exercise training in patients with severe COPD‐global effects. American Journal of Respiratory and Critical Care Medicine 2000;161(3 Suppl):A254. [Google Scholar]
- Behnke M, Kirsten D, Lehnigk B, Jörres RA, Magnussen H. The effects of home‐based exercise training on walking distance and quality of life in patients with severe COPD. European Respiratory Journal 1998;12(Suppl 38):3S. [Google Scholar]
- Behnke M, Taube C, Kirsten D, Jörres RA, Lehnigk B, Magnussen H. The long‐term effects of domestic walking training in patients with severe COPD [Die Langzeitwirkungen eines häuslichen Gehtrainings bei Patienten mit schwergradiger COPD]. Pneumologie 2000;54(S56):P77. [Google Scholar]
- Behnke M, Taube C, Kirsten D, Lehnigk B, Jörres RA, Magnussen H. Home‐based exercise is capable of preserving hospital‐based improvements in severe chronic obstructive pulmonary disease. Respiratory Medicine 2000;94:1184‐91. [DOI] [PubMed] [Google Scholar]
Bendstrup 1997 {published data only}
- Bendstrup KE, Ingemann Jensen J, Holm S, Bengtsson B. Out‐patient rehabilitation improves activities of daily living, quality of life and exercise tolerance in chronic obstructive pulmonary disease. European Respiratory Journal 1997;10:2801‐6. [DOI] [PubMed] [Google Scholar]
Booker 1984 {published data only}
- Booker HA. Exercise training and breathing control in patients with chronic airflow limitation. Physiotherapy 1984;70:258‐60. [PubMed] [Google Scholar]
Borghi‐Silva 2009 {published data only}
- Borghi‐Silva A, Arena R, Castello V, Simoes RP, Martins LE, Catai AM, et al. Aerobic exercise training improves autonomic nervous control in patients with COPD. Respiratory Medicine 2009;103(10):1503‐10. [DOI] [PubMed] [Google Scholar]
Boxall 2005 {published and unpublished data}
- Boxall A, Barclay L, Caplan G. A randomised controlled trial of home‐based pulmonary rehabilitation for elderly, housebound COPD patients. Proceedings of the Thoracic Society of Australia & New Zealand Annual Scientific Meeting; 2003 4‐9 April; Adelaide. 2003:P106.
- Boxall AM, Barclay L, Sayers A, Caplan GA. Managing chronic obstructive pulmonary disease in the community: a randomized controlled trial of home‐based pulmonary rehabilitation for elderly housebound patients. Journal of Cardiopulmonary Rehabilitation 2005;25(6):378‐85. [DOI] [PubMed] [Google Scholar]
Busch 1988 {published data only}
- Busch AJ, McClements JD. Effects of a supervised home exercise program on patients with severe chronic obstructive pulmonary disease. Physical Therapy 1988;68:469‐74. [DOI] [PubMed] [Google Scholar]
Cambach 1997 {published data only}
- Cambach W, Chadwick‐Straver RVM, Wagenaar RC. The effects of a community‐based pulmonary rehabilitation programme on exercise capacity and quality of life: a randomized controlled trial. European Respiratory Journal 1997;10(Suppl 25):394S. [DOI] [PubMed] [Google Scholar]
- Cambach W, Chadwick‐Straver RVM, Wagenaar RC, Keimpema ARJ. Efficacy of a rehabilitation programme in patients with asthma and chronic obstructive pulmonary disease (COPD) [Effectiviteit van een revalidatieprogramma voor patienten met astma en COPD uitgevoerd in de eerstelijnsgozondheidszorg]. Nederlands Tijdschrift Fysiotherapie 1998;108(2):26‐36. [Google Scholar]
- Cambach W, Chadwick‐Straver RVM, Wagenaar RC, Keimpema ARJ, Kemper HCG. The effects of a community‐based pulmonary rehabilitation programme on exercise tolerance and quality of life: a randomized controlled trial. European Respiratory Journal 1997;10:104‐13. [DOI] [PubMed] [Google Scholar]
Casaburi 2004 {published data only}
- Casaburi R, Bhasin S, Cosentino L, Porszasz J, Somfay A, Lewis MI, et al. Effects of testosterone and resistance training in men with chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine 2004;170:870‐8. [DOI] [PubMed] [Google Scholar]
- Casaburi R, Cosentino G, Bhasin S, Fournier M, Lewis M, Porszasz J, et al. A randomised trial of strength training and testosterone supplementation in men with chronic obstructive pulmonary disease. European Respiratory Journal 2001;18(Suppl 33):173S. [Google Scholar]
- Chavoshan B, Fournier M, Lewis MI, Porszasz J, Storer TW, Da X, et al. Testosterone and resistance training effects on muscle nitric oxide synthase isoforms in COPD men. Respiratory Medicine 2012;106(2):269‐75. [DOI] [PubMed] [Google Scholar]
Casey 2013 {published data only}
- Casey D, Murphy K, Devane D, Cooney A, McCarthy B, Mee L, et al. The effectiveness of a structured education pulmonary rehabilitation programme for improving the health status of people with moderate and severe chronic obstructive pulmonary disease in primary care: the PRINCE cluster randomised trial. Thorax 2013;68(10):922‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Casey, Murphy D, Cooney A, Mee L. Developing a structured education programme for clients with COPD. British Journal of Community Nursing 2011;16(5):231‐7. [DOI] [PubMed] [Google Scholar]
- Murphy K, Casey D, Devane D, Cooney A, McCarthy B, Mee L, et al. The effectiveness of a structured education pulmonary rehabilitation programme for improving the health status of people with chronic obstructive pulmonary disease (COPD): the PRINCE study [Abstract]. Irish Journal of Medical Science 2011;180(Suppl 12):S457. [Google Scholar]
- Murphy K, Casey D, Devane D, Cooney A, McCarthy, B, Mee L, et al. A cluster randomised controlled trial evaluating the effectiveness of a structured pulmonary rehabilitation education programme for improving the health status of people with chronic obstructive pulmonary disease (COPD): the PRINCE Study protocol. BMC Pulmonary Medicine 2011;11:4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cebollero 2012 {published and unpublished data}
- Cebollero P, Zambon F, Hernandez M, Gorostiaga E, Ibanez J, Hueto J, et al. Effects of exercise twice a week in the peripheral muscle dysfunction in COPD patients. American Journal of Respiratory and Critical Care Medicine [Abstract] 2012;185(Meeting Abstracts):A4854. [Google Scholar]
Chan 2011 {published data only}
- Chan AW, Lee, K, Suen A, Tam LKP, Tam WW. Tai chi Qigong improves lung functions and activity tolerance in COPD clients: a single blind, randomized controlled trial. Complementary Therapies in Medicine 2011;19(1):3‐11. [DOI] [PubMed] [Google Scholar]
Chlumsky 2001 {published data only}
- Chlumsky J, Sterbova L, Smolikova L, Matous M, Salajka F. The effect of pulmonary rehabilitation on exercise tolerance and quality of life in patients with COPD. Preliminary data. European Respiratory Journal 2001;18(Suppl):223S. [Google Scholar]
Clark 1996 {published data only}
- Clark CJ, Cochrane L, Mackay E. Low intensity peripheral muscle conditioning improves exercise tolerance and breathlessness in COPD. European Respiratory Journal 1996;9(12):2590‐6. [DOI] [PubMed] [Google Scholar]
Cochrane 2006 {published and unpublished data}
- Afolabi G, Watson B, Cochrane W, Dogan S, Heatley M. A study of the effectiveness of individual components of pulmonary rehabilitation when compared with the combined programme and standard treatment [Abstract]. European Respiratory Journal 2004;24(Suppl 48):209s. [Google Scholar]
- Cochrane WC, Watson B, Dogan S, Afolabi OA, McAlpine C, Heatley M. Exercise training leads to a broader reduction in community and hospital service utilisation, compared with other forms of rehabilitation, after 6‐months [Abstract]. American Thoracic Society 100th International Conference; 2004 May 21‐26; Orlando. 2004:D96 Poster 128.
- Cochrane WC, Watson B, Dogan S, Heatley M, McAlpine C, Dovey‐Pearce G, et al. A study of the effectiveness of individual components of pulmonary rehabilitation when compared with the combined programme and standard treatment. Final Report. Final Report Northumbria University and Northumbria Healthcare NHS Trust November 2006.
Cockcroft 1981 {published data only}
- Cockcroft A, Berry G, Brown EB, Exall C. Psychological changes during a controlled trial of rehabilitation in chronic respiratory disability. Thorax 1982;37:413‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cockcroft AE, Saunders MJ, Berry G. Randomised controlled trial of rehabilitation in chronic respiratory disability. Thorax 1981;36:200‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Deering 2011 {published and unpublished data}
- Deering BM, Fullen B, Egan C, McCormack N, Kelly E, Pender M, et al. Acupuncture as an adjunct to pulmonary rehabilitation. Journal of Cardiopulmonary Rehabilitation and Prevention 201;31(6):392‐99. [DOI] [PubMed] [Google Scholar]
De Souto Araujo 2012 {published and unpublished data}
- Souto Araujo ZT, Miranda Silva Nogueira PA, Cabral EE, Paula Dos Santos LD, Silva IS, Ferreira GM. Effectiveness of low‐intensity aquatic exercise on COPD: a randomized clinical trial. Respiratory Medicine 2012;106(11):1535‐43. [DOI] [PubMed] [Google Scholar]
Elci 2008 {published data only}
- Elci A, Borekci S, Ovayolu N, Elbek O. The efficacy and applicability of a pulmonary rehabilitation programme for patients with COPD in a secondary‐care community hospital. Respirology 2008;13(5):703‐7. [DOI] [PubMed] [Google Scholar]
Emery 1998 {published data only}
- Emery CF, Schein RL, Hauck ER, MacIntyre NR. Psychological and cognitive outcomes of a randomised trial of exercise among patients with chronic obstructive pulmonary disease. Health Psychology 1998;17:232‐40. [DOI] [PubMed] [Google Scholar]
Engström 1999 {published data only}
- Engström CP, Persson LO, Larsson S, Sullivan M. Long‐term effects of a pulmonary rehabilitation programme in outpatients with chronic obstructive pulmonary disease: a randomized controlled study. Scandinavian Journal of Rehabilitation Medicine 1999;31:207‐13. [DOI] [PubMed] [Google Scholar]
Faager 2004 {published data only}
- Faager G, Larsen FF. Performance changes for patients with chronic obstructive pulmonary disease on long‐term oxygen therapy after physiotherapy. Journal of Rehabilitation Medicine 2004;36(4):153‐8. [DOI] [PubMed] [Google Scholar]
Faulkner 2010 {published and unpublished data}
- Faulkner J, Walshaw E, Campbell J, Jones R, Taylor R, Price, et al. The feasibility of recruiting patients with early COPD to a pilot trial assessing the effects of a physical activity intervention. Primary Care Respiratory Journal 2010;19:124‐30. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fernandez 2009 {published data only}
- Fernandez AM, Pascual J, Ferrando C, Arnal A, Vergara I, Sevila V. Home‐based pulmonary rehabilitation in very severe COPD: is it safe and useful?. Journal of Cardiopulmonary Rehabilitation and Prevention 2009;29(5):325‐31. [DOI] [PubMed] [Google Scholar]
Finnerty 2001 {published data only}
- Finnerty JP, Keeping I, Bullough I, Jones J. The effectiveness of outpatient pulmonary rehabilitation in chronic lung disease. A randomized controlled trial. Chest 2001;119:1705‐10. [DOI] [PubMed] [Google Scholar]
Gohl 2006 {published data only}
- Gohl O, Linz H, Schonleben T, Otte B, Weineck J, Worth H. [Benefits of a multimodular outpatient training program for patients with COPD]. [German]. Pneumologie 2006;60(9):529‐36. [DOI] [PubMed] [Google Scholar]
Goldstein 1994 {published data only}
- Goldstein RS, Gort EH, Guyatt GH, Feeny D. Economic analysis of respiratory rehabilitation. Chest 1997;112(2):370‐9. [DOI] [PubMed] [Google Scholar]
- Goldstein RS, Gort EH, Stubbing D, Avendano MA, Guyatt GH. Randomised controlled trial of respiratory rehabilitation. Lancet 1994;344:1394‐7. [DOI] [PubMed] [Google Scholar]
- Gort EH, Goldstein R, Guyatt G, Stubbing D, Avendano M. Randomized controlled trial of respiratory rehabilitation. Canadian Journal of Rehabilition 1993;7(1):13‐4. [DOI] [PubMed] [Google Scholar]
- Guyatt GH, King DR, Feeny DH, Stubbing D, Goldstein RS. Generic and specific measurement of health‐related quality of life in a clinical trial of respiratory rehabilitation. Journal of Clinical Epidemiology 1999;52(3):187‐92. [DOI] [PubMed] [Google Scholar]
Gomez 2006 {published data only}
- Gomez A, Roman M, Larraz C, Esteva M, Mir I, Thomás V. Efficacy of respiratory rehabilitation on patients with moderate COPD in primary care and maintenance of benefits at 2 years. Aten Primaria 2006;38:230‐33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roman M, Concepcion L, Gomez A, Ripoll J, Mir I, Miranda EZ, et al. Efficacy of pulmonary rehabilitation in patients with moderate chronic obstructive pulmonary disease: a randomized controlled trial. http://www.biomedcentral.com/1471‐2296/14/21 (accessed 21 October 2014). [DOI] [PMC free article] [PubMed]
Gosselink 2000 {published data only}
- Gosselink R, Troosters T, Houtmeyers E, Decramer M. Adaptations in breathing pattern after exercise training in patients with COPD. American Journal of Respiratory and Critical Care Medicine 1998;157(Suppl 3):A257. [Google Scholar]
- Gosselink R, Troosters T, Rollier H, Decramer M. Improved exercise capacity after out‐patient pulmonary rehabilitation in COPD patients. European Respiratory Journal 1996;9(Suppl 23):383S. [Google Scholar]
- Gosselink R, Troosters T, Rollier H, Decramer M. Pulmonary rehabilitation improves exercise capacity in COPD: preliminary results. European Respiratory Journal 1995;8(Suppl 19):356S. [Google Scholar]
- Troosters T, Gosselink R, Decramer M. Short and long‐term effects of outpatient rehabilitation in patients with chronic obstructive pulmonary disease: a randomized trial. American Journal of Medicine 2000;109:207‐12. [DOI] [PubMed] [Google Scholar]
Gottlieb 2011 {published data only}
- Gottlieb V, Lyngsø AM, Nybo B, Frølich A, Backer V. Pulmonary rehabilitation for moderate COPD (GOLD 2) ‐ does it have an effect?. COPD 2011;8(5):380‐6. [DOI] [PubMed] [Google Scholar]
Griffiths 2000 {published data only}
- Griffiths TL, Burr ML, Campbell IA, Lewis‐Jenkins V, Mullins J, Shiels K, et al. Results at 1 year of outpatient multidisciplinary pulmonary rehabilitation: a randomised controlled trial. The Lancet 2000;355:362‐8. [DOI] [PubMed] [Google Scholar]
- Griffiths TL, Phillips CJ, Davies S, Burr ML, Campbell IA. Cost effectiveness of an outpatient multidisciplinary pulmonary rehabilitation programme. Thorax 2001;56(10):779‐84. [DOI] [PMC free article] [PubMed] [Google Scholar]
Güell 1995 {published and unpublished data}
- Güell R, Casan P, Belda J, Sangenis M, Morante F. Effect of maintenance techniques on outcomes in a respiratory rehabilitation programme in COPD patients. Archivos de Bronconeumología 1997;33(Suppl 1):6. [Google Scholar]
- Güell R, Casan P, Belda J, Sangenis M, Morante F, Guyatt GH, et al. Long‐term effects of outpatient rehabilitation of COPD: a randomized trial. Chest 2000;117(4):976‐83. [DOI] [PubMed] [Google Scholar]
- Güell R, Casan P, Belda J, Sangenis M, Morante F, Sanchis J. Effects of maintenance techniques on the results obtained in a respiratory rehabilitation programme for COPD patients. European Respiratory Journal 1997;10(Suppl 25):394S. [Google Scholar]
- Güell R, Casan P, Sangenis M, Morante F, Belda J, Guyatt GH. Quality of life in patients with chronic respiratory disease: the Spanish version of the Chronic Respiratory Questionnaire (CRQ). European Respiratory Journal 1998;11(1):55‐60. [DOI] [PubMed] [Google Scholar]
- Güell R, Morante F, Sangenis M, et al. Effects of respiratory rehabilitation on the effort capacity and on the health‐related quality of life of patients with chronic obstructive pulmonary disease. European Respiratory Journal 1995;8(Suppl):356. [Google Scholar]
- Güell R, Morante F, Sangenís M, Casan P. Effects of respiratory rehabilitation on quality of life of patients with chronic obstructive pulmonary disease. Annals de Medicina 1995;81(1):9. [Google Scholar]
Güell 1998 {unpublished data only}
- Guell R, Resqueti V, Sangenis M, Morante F, Martorell B, Casan P, et al. Impact of pulmonary rehabilitation on psychosocial morbidity in with severe COPD. Chest 2006;129(4):899‐904. [DOI] [PubMed] [Google Scholar]
- Güell R, Gonzalez Y, Gonzalez A, Sotomayor C, Sangenis M, Morante F, et al. Impact of respiratory rehabilitation on personality traits and characteristics of patients with COPD. Archivos de Bronconeumología 1998;34(Suppl 1):34. [DOI] [PubMed] [Google Scholar]
- Güell R, Gonzalez Y, Martorell B, Gonzalez A, Sotomayor C, Sangenis M, et al. Impact of pulmonary rehabilitation on personality traits and styles in COPD patients. European Respiratory Journal 1998;12(Suppl 28):228S. [Google Scholar]
Gurgun 2013 {published data only}
- Gurgun A, Deniz S, Argin M, Karapolat H. Effects of nutritional supplementation combined with conventional pulmonary rehabilitation in muscle‐wasted chronic obstructive pulmonary disease: a prospective, randomized and controlled study. Respirology 2013;18(3):495‐500. [DOI] [PubMed] [Google Scholar]
- Gurgun A, Deniz S, Argyn M, Karapolat H. The effects of nutritional supplementation added to pulmonary rehabilitation in muscle wasted chronic obstructive pulmonary disease: a randomised, controlled, prospective study [Abstract]. American Journal of Respiratory and Critical Care Medicine 2011;183(Meeting Abstracts):A3972. [Google Scholar]
Hernandez 2000 {published data only}
- Cejudo P, Elias T, Montemayor T, Ortega F, Sanchez H, Villagomez R. Results of a home‐based training program applied to patients with chronic obstructive pulmonary disease (COPD). European Respiratory Society 9th Annual Congress; 1999 Oct 9‐13; Madrid. 1999:210.
- Elias M, Ortega F, Toral J, Sanchez H, Cejudo P, Montemayor T. Improvement in exercise tolerance and quality of life in COPD patients following a home training programme. Archivos De Bronconeumologia 1998;34(Suppl 1):34. [Google Scholar]
- Elias M, Ortega F, Toral J, Tabernero E, Sanchez H, Montemayor T. Evaluation of a home training programme in patients with COPD (preliminary results). Archivos De Bronconeumologia 1997;33(Suppl 1):12. [Google Scholar]
- Elias MT, Ortega F, Toral J, Sanchez H, Cejudo P, Montemayor T. Results from a home‐based exercise training program in patients with COPD [Resultados de un programa domiciliario de entrenamiento al ejercicio en pacientes con EPOC]. Neumosur 1998;10(1):16‐7. [Google Scholar]
- Elías MT, Ortega F, Toral J, Sánchez H, Cejudo P, Montemayor T. Improvement in exercise tolerance and quality of life in COPD patients following a home training programme [Mejoria en la tolerancia al ejercico y en la calidad de vida en pacientes EPOC tras un programa de entrenamiento domiciliario]. Archivos de Bronconeumologìa 1998;34(Suppl 1):34. [Google Scholar]
- Elías MT, Ortega F, Toral J, Tabernero E, Sánchez H, Montemayor T. Evaluation of a home training programme in patients with COPD (preliminary results) [Evaluación de un programa de entremiento domiciliaro en pacientes con EPOC (resultados perliminares)]. 1997 Archivos de Bronconeumología;33(Suppl 1):12. [Google Scholar]
- Hernandez MT, Rubio TM, Ruiz FO, Riera HS, Gil RS, Gomez JC. Results of a home‐based training program for patients with COPD. Chest 2000;118:106‐14. [DOI] [PubMed] [Google Scholar]
Hoff 2007 {published data only}
- Hoff J, Tjonna AE, Steinshamn S, Hoydal M, Richardson RS, Helgerud J. Maximal strength training of the legs in COPD: a therapy for mechanical inefficiency. Medicine and Science in Sports and Exercise 2007;39(2):220‐6. [DOI] [PubMed] [Google Scholar]
Jones 1985 {published data only}
- Jones DT, Thomson RJ, Sears MR. Physical exercise and resistive breathing in severe chronic airways obstruction ‐ are they effective?. European Journal of Respiratory Diseases 1985;67:159‐66. [PubMed] [Google Scholar]
Karapolat 2007 {published data only}
- Karapolat H, Atasever A, Atamaz F, Kirazli J, Elmas F, Erdinc E. Do the benefits gained using a short‐term pulmonary rehabilitation program remain in COPD patients after participation?. Lung 2007;185:221‐5. [DOI] [PubMed] [Google Scholar]
Lake 1990 {published data only}
- Lake FR, Henderson K, Briffa T, Openshaw J, Musk AW. Upper‐limb and lower‐limb exercise training in patients with chronic airflow obstruction. Chest 1990;97:1077‐82. [DOI] [PubMed] [Google Scholar]
Lindsay 2005 {published data only (unpublished sought but not used)}
- Lindsay M, Lee A, Chan K, Poon P, Han LK, Wong WC, et al. Does pulmonary rehabilitation give additional benefit over tiotropium therapy in primary care management of chronic obstructive pulmonary disease? Randomized controlled clinical trial in Hong Kong Chinese. Journal of Clinical Pharmacy and Therapeutics 2005;30(6):567‐73. [DOI] [PubMed] [Google Scholar]
- Lindsay M, Lee A, Poon P, Han LK, Wong WC, Wong W, et al. Does pulmonary rehabilitation give additional benefits to primary care patients with chronic obstructive pulmonary disease? Results from randomized controlled clinical trial in Hong Kong [Abstract]. Respirology 2004;9(Suppl):A100. [Google Scholar]
Liu 2012 {published data only}
- Liu XD, Jin HZ, Ng Bh‐ P, Gu YH, Wu Y‐C, Lu G. Therapeutic effects of qigong in patients with COPD: a randomized controlled trial. Hong Kong Journal of Occupational Therapy 2012;22(1):38‐46. [Google Scholar]
McGavin 1977 {published data only}
- McGavin CR, Gupta SP, Lloyd EL, McHardy GJR. A controlled trial of self‐regulated physical training in chronic bronchitis. British Journal of Diseases of the Chest 1976;70(4):278. [Google Scholar]
- McGavin CR, Gupta SP, Lloyd EL, McHardy GJR. Physical rehabilitation for the chronic bronchitis: results of a controlled trial of exercises in the home. Thorax 1977;32:307‐11. [DOI] [PMC free article] [PubMed] [Google Scholar]
McNamara 2013 {published and unpublished data}
- McNamara RJ, Alison JA, McKenzie DK, McKeough ZJ. Water‐based exercise improves exercise capacity in people with COPD with physical co‐morbid conditions [Abstract]. Respirology 1010;15(Suppl 1):A24 [TO 056]. [Google Scholar]
- McNamara RJ, McKeough ZJ, McKenzie DK, Alison JA. Water‐based exercise in COPD with physical comorbidities: a randomised controlled trial. European Respiratory Journal 2013;6:1284‐91. [DOI] [PubMed] [Google Scholar]
- McNamara, RJ, Alison JA, McKenzie DK, McKeough ZJ. Water‐based exercise in people with COPD and physical co‐morbid conditions: a randomised controlled trial [Abstract]. European Respiratory Society 20th Annual Congress; 2010 Sep 18‐22; Barcelona. 2010:181.
Mehri 2007 {published data only}
- Mehri SN, Khoshnevis MA, Zarrehbinan F, Hafezi S, Ghasemi A, Ebadi A. Effect of treadmill exercise training on VO2 peak in chronic obstructive pulmonary disease. Tanaffos 2007;6(4):18‐24. [Google Scholar]
Mendes De Oliveira 2010 {published and unpublished data}
- Mendes De Oliveira JC, Studart Leitao Filho FS, Malosa Sampaio LM, Negrinho De Oliveira AC, Hirata RP, Costa D, et al. Outpatient vs. home‐based pulmonary rehabilitation in COPD: a randomized controlled trial. Multidisciplinary Respiratory Medicine 2010;5(6):401‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oliveira JCM, Filho FSL, Sampaio L, Oliveira AC, Hirata R, Costa D. Outpatient vs. home‐based pulmonary rehabilitation in COPD: A randomized controlled trial [Abstract]. European Respiratory Society 21st Annual Congress; 2011 Sep 24‐28; Amsterdam 2011;38(55):879s [P4805]. [Google Scholar]
Nalbant 2011 {published data only (unpublished sought but not used)}
- Nalbant O, Nur H, Ogus C, Toraman NF. Effects of long‐term aerobic exercise program in chronic obstructive pulmonary disease. Turkiye Fiziksel Tip ve Rehabilitasyon Dergisi 2011;57(1):8‐13. [Google Scholar]
O'Shea 2007 {published data only}
- O' Shea SD, Taylor NF, Paratz J. Peripheral strength training for people with chronic obstructive pulmonary disease [Abstract]. Respirology 2005;10(suppl):A58. [Google Scholar]
- O'Shea SD, Taylor NF, Paratz JD. A predominantly home‐based progressive resistance exercise program increases knee extensor strength in the short‐term in people with chronic obstructive pulmonary disease: a randomised controlled trial. Australian Journal of Physiotherapy 2007;53(4):229‐37. [DOI] [PubMed] [Google Scholar]
- O'Shea SD, Taylor NF, Paratz JD. Peripheral strength training for people with chronic obstructive pulmonary disease: a randomised controlled trial. [abstract]. Australian Journal of Physiotherapy 2006;52(2):s22. [DOI] [PubMed] [Google Scholar]
- O'Shea SD, Taylor NF, Paratz JD. Qualitative outcomes of progressive resistance exercise for people with COPD. Chronic Respiratory Disease 2007;4(3):135‐42. [DOI] [PubMed] [Google Scholar]
Ozdemir 2010 {published data only}
- Ozdemir EP, Solak O, Fidan F, Demirdal US, Evcik, D, Unlu M, et al. The effect of water‐based pulmonary rehabilitation on anxiety and quality of life in chronic pulmonary obstructive disease patients. Turkiye Klinikleri Journal of Medical Sciences 2010;30(1):880‐7. [Google Scholar]
Paz‐Diaz 2007 {published data only}
- Paz‐Diaz H, Montes de Oca M, Lopez JM, Celli BR. Pulmonary rehabilitation improves depression, anxiety, dyspnea and health status in patients with COPD. American Journal of Physical Medicine and Rehabilitation 2007;86(1):30‐6. [DOI] [PubMed] [Google Scholar]
Petty 2006 {published data only}
- Petty TL, Dempsey EC, Collins T, Pluss W, Lipkus I, Cutter GR, et al. Impact of customized videotape education on quality of life in patients with chronic obstructive pulmonary disease. Journal of Cardiopulmonary Rehabilitation 2006;26(2):112‐7. [DOI] [PubMed] [Google Scholar]
Reardon 1994 {published data only}
- Reardon J, Awad E, Normandin E, Vale F, Clark B, ZuWallack RL. The effect of comprehensive outpatient pulmonary rehabilitation on dyspnea. Chest 1994;105:1046‐52. [DOI] [PubMed] [Google Scholar]
Ringbaek 2000 {published data only}
- Broendum E, Lybeck K, Andersen C, Hemmingsen L, Nielsen D, Lange P, et al. Rehabilitation in patients with COPD ‐ the effect of a "twice‐a‐week‐programme". European Respiratory Society 9th Annual Congress; 1999 Oct 9‐13; Madrid. 1999:208.
- Ringbaek TJ, Broendum E, Hemmingsen L, Lybeck K, Nielsen D, Andersen C, et al. Rehabilitation of patients with chronic obstructive pulmonary disease. Exercise twice a week is not sufficient!. Respiratory Medicine 2000;94(2):150‐4. [DOI] [PubMed] [Google Scholar]
Simpson 1992 {published data only}
- Simpson K, Killian K, McCartney N, Jones NL. Randomised controlled trial of weightlifting exercise in patients with chronic airflow limitation. Thorax 1992;47:70‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Singh 2003 {published data only}
- Singh V, Khandelwal DC, Khandelwal R, Abusaria S. Pulmonary rehabilitation in patients with chronic obstructive pulmonary diseases. Indian Journal of Chest Diseases and Allied Sciences 2003;45(1):13‐7. [PubMed] [Google Scholar]
Sridhar 2008 {published data only}
- Sridhar M, Taylor R, Dawson S, Roberts NJ, Partridge MR. A nurse led intermediate care package in patients who have been hospitalised with an acute exacerbation of chronic obstructive pulmonary disease. Thorax 2008;63(3):194‐200. [DOI] [PubMed] [Google Scholar]
Strijbos 1996 {published data only}
- Strijbos JH, Koëter GH, Meinesz AF. Home care rehabilitation and perception of dyspnea in chronic obstructive pulmonary disease. Chest 1990;97(Suppl):109‐10. [DOI] [PubMed] [Google Scholar]
- Strijbos JH, Postma DS, Altena R, et al. A comparison between an outpatient hospital‐based pulmonary rehabilitation program and a home‐care pulmonary rehabilitation program in patients with COPD. A follow‐up of 18 months. Chest 1996;109(2):366‐72. [DOI] [PubMed] [Google Scholar]
- Strijbos JH, Postma DS, Altena R, Gimeno F, Koeter GH. Feasibility and effects of a home‐care rehabilitation program in patients with chronic obstructive pulmonary disease. Journal of Cardiopulmonary Rehabilitation 1996;16(6):386‐93. [DOI] [PubMed] [Google Scholar]
- Strijbos JH, Wijkstra PJ, Postma DS, Koeter GH. Five year effects of rehabilitation at different settings in patients with chronic obstructive pulmonary disease. European Respiratory Society 9th Annual Conference; 1999; Oct 9‐13; Madrid. 1999:209.
Theander 2009 {published data only}
- Theander K, Jakobsson P, Jorgensen N, Unosson M. Effects of pulmonary rehabilitation on fatigue, functional status and health perceptions in patients with chronic obstructive pulmonary disease: a randomized controlled trial. Clinical Rehabilitation 2009;23(2):125‐36. [DOI] [PubMed] [Google Scholar]
Vallet 1994 {published data only}
- Vallet G, Varray A, Fontaine JL, Prefaut C. Interest of individualized training program at the ventilatory threshold in mild to moderate COPD patients [Intérêt du réentraînement à l'effort individualisé, au niveau du seuil ventilatoire, au cours de la bronchopneumopathie chronique obstructive de sévérité modérée]. Revue des Maladies Respiratoires 1994;11(5):493‐501. [PubMed] [Google Scholar]
Van Wetering 2010 {published data only}
- Hoogendoorn M, Wetering CR, Schols AM, Rutten‐van Molken MP. Is INTERdisciplinary Community‐based COPD management (INTERCOM) cost effective?. European Respiratory Journal 2010;35:79‐87. [DOI] [PubMed] [Google Scholar]
- Wetering CR, Hoogendoorn M, Munck DR, Rutten‐van Molken MP, Schols AM. Cost‐effectiveness of a 24 month INTERdisciplinary COMmunity ‐based COPD management program (INTERCOM) in patients with less advanced airflow obstruction [Abstract]. American Thoracic Society International Conference, May 15‐20, 2009, San Diego. 2009:A5373.
- Wetering CR, Hoogendoorn M, Mol SJ, Rutten‐Van Molken M, Schols AM. Short‐ and long‐term efficacy of a community‐based COPD management programme in less advanced COPD: a randomised controlled trial. Thorax 65;1:7‐13. [DOI] [PubMed] [Google Scholar]
- Wetering CR, Hoogendoorn M, Broekhuizen R, Geraerts‐Keeris GJ, Munck DR, Rutten‐van Mölken MP. Efficacy and costs of nutritional rehabilitation in muscle‐wasted patients with chronic obstructive pulmonary disease in a community‐based setting: a prespecified subgroup analysis of the INTERCOM trial. Journal of the American Medical Directors Association 2010;11(3):179‐87. [DOI] [PubMed] [Google Scholar]
- Wetering CR, Nooten FE, Mol, SJ, Hoogendoorn M, Rutten‐Van Molken MP, Schols AM. Systemic impairment in relation to disease burden in patients with moderate COPD eligible for a lifestyle program. Findings from the INTERCOM trial. International Journal of COPD 2008;3(3):443‐51. [DOI] [PMC free article] [PubMed] [Google Scholar]
Vijayan 2010 {published data only (unpublished sought but not used)}
- Vijayan VK, Senthil K, Menon B, Bansal V. Effect of pulmonary rehabilitation on markers of inflammation, muscle mass and exercise capacity in patients with chronic obstructive pulmonary disease (COPD) [Abstract]. 15th Congress of the Asian Pacific Society of Respirology; 2010 Nov 22‐25; Manila. 2010.
Weiner 1992 {published data only}
- Weiner P, Azgad Y, Ganam R. Inspiratory muscle training combined with general exercise reconditioning in patients with COPD. Chest 1992;102:1351‐6. [DOI] [PubMed] [Google Scholar]
Wen 2008 {published data only}
- Wen H, Gao Y, An JY. Comparison of high‐intensity and anaerobic threshold programs in rehabilitation for patients with moderate to severe chronic obstructive pulmonary disease. [Chinese]. Chung‐Hua Chieh Ho Ho Hu Hsi Tsa Chih Chinese Journal of Tuberculosis & Respiratory Diseases 2008;31(8):571‐6. [PubMed] [Google Scholar]
Wijkstra 1994 {published data only}
- Wijkstra PJ, Kraan J, Mark THW, Altena R, Postama DS, Koeter GH. Long‐term benefits of rehabilitation at home on inspiratory muscle function and dyspnoea in patients with chronic obstructive pulmonary disease (COPD). European Respiratory Journal 1994;7(Suppl 18):296S. [Google Scholar]
- Wijkstra PJ, Altena R, Kraan J, Otten V, Postma DS, Koëter GH. Quality of life in patients with chronic obstructive pulmonary disease improves after rehabilitation at home. European Respiratory Journal 1994;7:269‐73. [DOI] [PubMed] [Google Scholar]
- Wijkstra PJ, Mark TW, Kraan J, Altena R, Koeter GH, Postma DS. Long‐term effects of home rehabilitation on physical performance in chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine 1996;153(4 (pt 1)):1234‐41. [DOI] [PubMed] [Google Scholar]
Xie 2003 {published data only}
- Xie SL, Zhu MG, Cui HB, Liu HY. Influence of home‐based training program on patients with COPD. Zhonghua Linchuang Kangfu Zazhi 2003;7(18):2554‐5. [Google Scholar]
References to studies excluded from this review
Akinci 2011 {published and unpublished data}
- Akinci AC, Olgun N. The effectiveness of nurse‐led, home‐based pulmonary rehabilitation in patients with COPD in Turkey. Rehabilitation Nursing 2011;36(4):159‐65. [DOI] [PubMed] [Google Scholar]
Ambrosino 1981 {published data only}
- Ambrosino N, Paggiaro PL, Macchi M, Filieri M, Toma G, Lombardi FA, et al. A study of short‐term effect of rehabilitative therapy in chronic obstructive pulmonary disease. Respiration 1981;41(1):40‐4. [DOI] [PubMed] [Google Scholar]
Ambrosino 2006 {published data only}
- Ambrosino N, Angelis G, Pasqua P, Paggiaro A, Cogo G, Balzano K, et al. Physiological and symptom correlates of exercise tolerance in COPD patient. American Thoracic Society International Conference; 2006 May 19‐21; San Diego. 2006; Vol. A212 [Poster L78].
Amin 2011 {published and unpublished data}
- Amin S, Quinn M, Abrazado M, Forster R, Berenc M, Storer T. Controlled feasibility study of a community‐based exercise program In patients with moderate COPD. American Journal of Respiratory and Critical Care Medicine 2011;183(Meeting Abstracts):A5042. [Google Scholar]
Arnadottir 2001 {published data only}
- Arnardottir H, Larsson K, Ringqvist I, Sorensen S. Endurance training compared to non‐endurance training in chronic obstructive pulmonary disease (COPD). A randomized controlled trial. American Journal of Respiratory and Critical Care Medicine 2001;163(Suppl 5):A647. [Google Scholar]
- Arnrdottir H, Emtner M, Hedenstrom H, Larsson K, Boman G. Comparing interval and continuous endurance training in COPD. European Respiratory Journal 2005;26(Suppl 49):1694. [Google Scholar]
Backer 2003 {published data only}
- Backer V, Beyer N, Madsen MK, Jorgensen K, Larson L, Kjaer M. Resistance‐training improves muscle strength, functional level and self‐reported health in patients with chronic obstructive pulmonary disease [Abstract]. American Thoracic Society 99th International Conference; 2003 May 16‐21; Seattle. 2003:C042, Poster C33.
Bauldoff 1996 {published data only}
- Bauldoff GS, Hoffman LA, Sciurba F, Zullo TG. Home‐based, upper‐arm exercise training for patients with chronic obstructive pulmonary disease. Heart and Lung 1996;25:288‐94. [DOI] [PubMed] [Google Scholar]
Bauldoff 2002 {published data only}
- Bauldoff GS, Hoffman LA, Zullo TG, Sciurba FC. Exercise maintenance following pulmonary rehabilitation: effect of distractive stimuli. Chest 2002;122(3):948‐54. [DOI] [PubMed] [Google Scholar]
Behnke 2002 {published data only}
- Behnke M, Schwertfeger I, von Foreich, Robinson I, Jörres RA, Magnussen H. Monitoring home‐based exercise training in patients with stable COPD. American Journal of Respiratory and Critical Care Medicine 2002;165(Suppl 8):A16. [Google Scholar]
Behnke 2002a {published data only}
- Behnke M, Schwertfeger I, Froreich K, Robinson I, Jörres RA, Magnussen H. Combined exercise programs in patients with stable COPD: influence of psychological profile and monitoring. European Respiratory Journal 2002;20(Suppl 38):18S. [Google Scholar]
Behnke 2003 {published data only}
- Behnke M, Schwertfeger I, Froreich K, Robinson I, Kirsten D, Joerres RA, et al. Psychological profile but not monitoring predicts the outcome of exercise programs in COPD. American Thoracic Society 99th International Conference; 2003 May 16‐21; Seattle. 2003:C042, Poster C43.
Bernard 1999 {published data only}
- Bernard S, Whittom F, Leblanc P, Jobin J, Belleau R, Berube C, et al. Aerobic and strength training in patients with chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine 1999;159(3):896‐901. [DOI] [PubMed] [Google Scholar]
Berry 1996 {published data only}
- Berry MJ, Adair NE, Sevensky KS, Quinby A, Lever HM. Inspiratory muscle training and whole‐body reconditioning in chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine 1996;153(6 (Pt 1)):1812‐6. [DOI] [PubMed] [Google Scholar]
Bjerre‐Jepsen 1981 {published data only}
- Bjerre‐Jepsen K, Secher NH, Kok‐Jensen A. Inspiratory resistance training in severe chronic obstructive pulmonary disease. European Journal of Respiratory Diseases 1981;62(6):405‐11. [PubMed] [Google Scholar]
Böhning 1990 {published data only}
- Bohning W, Wettengel R. Physical exercise training in COPD during a 4‐week rehabilitation programme. European Respiratory Journal 1990;3(Suppl 10):212S. [Google Scholar]
Bourbeau 2000 {published data only}
- Bourbeau J, Collet JP, Schwartzman K, Beaupre A, Begin R, Maltais F, et al. Integrating rehabilitative elements into a COPD self‐management program reduces exacerbations and health service utilization: a randomized clinical trial. American Journal of Respiratory and Critical Care Medicine 2000;161(Suppl 3):A254. [Google Scholar]
- Bourbeau J, Julien M, Rouleau M, Maltais F, Beaupré A, Bégin R. Impact of an integrated rehabilitative self‐management program on health status of COPD patients: a multicentre randomised clinical trial. European Respiratory Journal 2000;16(Suppl 31):159S. [Google Scholar]
Bourjeily‐Habr 2002 {published data only}
- Bourjeily‐Habr G, Rochester CL, Palermo F, Snyder P, Mohsenin V. Randomised controlled trial of transcutaneous electrical muscle stimulation of the lower extremities in patients with chronic obstructive pulmonary disease. Thorax 2002;57(12):1045‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Breyer 2010 {published data only}
- Breyer MK, Breyer‐Kohansal R, Funk GC, Dornhofer N, Spruit MA, Wouters EF, et al. Nordic walking improves daily physical activities in COPD: a randomised controlled trial. Respiratory Research 2010;11:112. [DOI] [PMC free article] [PubMed] [Google Scholar]
Brooks 2000 {unpublished data only}
- Brooks D, Krip B, Mangovski Alzamora S, Avendano M, Goldstein R. The influence of post‐rehabilitation program on health related quality of life (HRQL) and functional exercise capacity in patients with chronic obstructive pulmonary disease (COPD). American Journal of Respiratory and Critical Care Medicine 2000;161(Suppl 3):A504. [Google Scholar]
Cai 2003 {published data only}
- Cai H. Rehabilitation effect of combination of respiration exercise, Jinshuibao capsule and external application in stable stage of chronic obstructive pulmonary diseases. Zhonghua Linchuang Kangfu Zazhi 2003;7(5):877. [Google Scholar]
Carrieri‐Kohlman 96 {published data only}
- Carrieri‐Kohlman V, Gormley JM, Douglas MK, Paul SM, Stulbarg MS. Exercise training decreases dyspnea and the distress and anxiety associated with it. Monitoring alone may be as effective as coaching. Chest 1996;110(6):1526‐35. [DOI] [PubMed] [Google Scholar]
Cegla 2002 {published data only}
- Cegla UH, Jost HJ, Harten A, Weber T, Wissmann S. Course of severe COPD with and without physiotherapy with the RC‐Cornet®: a randomized 2 years long‐term study. Pneumologie 2002;56(7):418‐24. [DOI] [PubMed] [Google Scholar]
Chen 2011 {published data only}
- Chen G, Zhou X, Hu X, Liu Y, Li Q. Effect of exercise on the quality of life and pulmonary function in patients with chronic obstructive pulmonary disease. Zhong Nan da Xue Xue Bao. Yi Xue Ban [Journal of Central South University. Medical Sciences] 2011;36(7):682‐6. [DOI] [PubMed] [Google Scholar]
Ciric 2008 {published data only}
- Ciric Z, Stankovic I, Rancic M, Pejcic T, Radovic M. Pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Vojnosanitetski Pregled 2008;65(7):533‐8. [DOI] [PubMed] [Google Scholar]
Clark 2000 {published data only}
- Clark CJ, Cochrane LM, Mackay E, Paton B. Skeletal muscle strength and endurance in patients with mild COPD and the effects of weight training. European Respiratory Journal 2000;15(1):92‐7. [DOI] [PubMed] [Google Scholar]
- Mackay EM, Clark CJ, Cochran LM, Bell F. The effect of a 12 week weight training programme in improving muscle endurance in patients with chronic obstructive pulmonary disease. 12th International Congress of the World Confederation of Physical Therapy; 1995; Washington DC. 1995; Vol. 30:430.
Cockcroft 1985 {published data only}
- Cockcroft A, Beaumont A, Guz A. Effect of exercise training on walking distance, exercise ventilation and breathlessness in patients with COAD. Clinical Science 1985;69(Suppl 12):7. [Google Scholar]
Coppoolse 1999 {published data only}
- Coppoolse R, Schols A, Baarends EM, Mostert R, Akkermans MA, Janssen PP, et al. Interval versus continuous training in patients with severe COPD: a randomized clinical trial. European Respiratory Journal 1999;14(2):258‐63. [DOI] [PubMed] [Google Scholar]
Covey 2004 {published data only}
- Covey MK, Larson JL. Exercise and COPD. American Journal of Nursing 2004;104(5):40‐3. [DOI] [PubMed] [Google Scholar]
Cox 1993 {published data only}
- Cox NJ, Hendricks JC, Binkhorst RA, Herwaarden CL. A pulmonary rehabilitation program for patients with asthma and mild chronic obstructive pulmonary diseases (COPD). Lung 1993;171(4):235‐44. [DOI] [PubMed] [Google Scholar]
de Blasio 2000 {published data only}
- Blasio F. A doubting Thomas dealing with pulmonary rehabilitation. Chest 2000;117(4):929‐31. [DOI] [PubMed] [Google Scholar]
Dekhuijzen 1990 {published data only}
- Dekhuijzen PNR, Beek MML, Folgering HTM, Herwaarden CLA. Psychological changes during pulmonary rehabilitation and target‐flow inspiratory muscle training in COPD patients with a ventilatory limitation during exercise. International Journal of Rehabilitation Research 1990;13:109‐17. [DOI] [PubMed] [Google Scholar]
Dekhuijzen 1991 {published data only}
- Dekhuijzen PN, Folgering HT, Herwaarden CL. Target‐flow inspiratory muscle training during pulmonary rehabilitation in patients with COPD. Chest 1991;99(1):128‐33. [DOI] [PubMed] [Google Scholar]
- Dekhuijzen PNR, Herwaarden van CLA, Folgering HThM. Target‐flow inspiratory muscle training (IMT) increases inspiratory muscle strength and endurance [Abstract]. European Respiratory Journal 1989;2(Suppl):389S. [Google Scholar]
de Lucas Ramos 1998 {published data only}
- Lucas Ramos P, Rodriguez Gonzalez‐Moro JM, Garcia de Pedro J, Santacruz Siminiani A, Tatay Marti E, Cubillo Marcos JM. Training of inspiratory muscles in chronic obstructive lung disease. Its impact on functional changes and exercise tolerance. Archivos de Bronconeumologia 1998;34(2):64‐70. [PubMed] [Google Scholar]
Demir‐Deriven 2001 {published data only}
- Demir‐Deviren S, Carrieri‐Kohlman V, Nguyen H, Neuhaus J, Eiser S, Stulbarg MS. Long term effect of exercise on dyspnea and exercise performance in COPD: how much training is enough?. American Journal of Respiratory and Critical Care Medicine 2001;163(Suppl 5):A13. [Google Scholar]
Demir‐Deriven 2002 {published data only}
- Demir‐Deviren S, Carrieri‐Kohlman V, Nguyen H, Paul SM, Stulbarg MS. Effects of gender on dyspnea with activities of daily living and health‐related quality of life after long term exercise training in patients with COPD. American Journal of Respiratory and Critical Care Medicine 2002;165(Suppl 8):A734. [Google Scholar]
Dewse 1998 {published data only}
- Dewse M. Improving pulmonary disease outcomes. Nursing New Zealand 1998;4(9):20‐2. [PubMed] [Google Scholar]
Di Marzo 2000 {published data only}
- Marzo A, Torrice M, Ciappi G. Inspiratory muscle training and relaxation therapy in advanced COPD patients. European Respiratory Journal 2000;16(Suppl 31):46S. [Google Scholar]
- Marzo A, Torrice M, Ciappi G. Inspiratory muscles training and relaxation in COPD patients. American Journal of Respiratory and Critical Care Medicine 2000;161(Suppl 3):A752. [Google Scholar]
Downes Vogel 2002 {published data only}
- Downes Vogel PJ. Effect of adding inspiratory muscle training to a pulmonary rehabilitation program for patients with COPD which includes upper extremity exercises. American Journal of Respiratory and Critical Care Medicine 2002;165(Suppl 8):A737. [Google Scholar]
Dushianthan 2009 {published data only}
- Dushianthan A. Safety and effectiveness of home‐based pulmonary rehabilitation in COPD. Thorax 2009;64(7):619. [Google Scholar]
Egan 2012 {published and unpublished data}
- Egan C, Costello R, Deering B, McCormack N, Blake C. Short term and long term effects of pulmonary rehabilitation on physical activity in COPD. Respiratory Medicine 2012;106:1671‐9. [DOI] [PubMed] [Google Scholar]
Ellum 2002 {published data only}
- Ellum SG, Rafferty GF, Nikoletou D, Moxham J. Effect of forward lean sitting on work of breathing and breathless scores in stable, severe COPD patients following exercise induced breathlessness. American Journal of Respiratory and Critical Care Medicine 2002;165(Suppl 8):A267. [Google Scholar]
Emtner 1998 {published data only}
- Emtner M, Finne M, Stalenheim G. High‐intensity physical training in adults with asthma. A comparison between training on land and in water. Scandinavian Journal of Rehabilitation Medicine 1998;30(4):201‐9. [DOI] [PubMed] [Google Scholar]
Epstein 1997 {published data only}
- Epstein SK, Celli BR, Martinez FJ, Couser JI, Roa J, Pollock M, et al. Arm training reduces the VO2 and VE cost of unsupported arm exercise and elevation in chronic obstructive pulmonary disease. Journal of Cardiopulmonary Rehabilitation 1997;17(3):171‐7. [DOI] [PubMed] [Google Scholar]
Esteve 1996 {published data only}
- Esteve F, Blanc‐Gras N, Gallego J, Benchetrit G. The effects of breathing pattern training on ventilatory function in patients with COPD. Biofeedback and Self Regulation 1996;21(4):311‐21. [DOI] [PubMed] [Google Scholar]
Fan 2008 {published data only}
- Fan VS, Giardino ND, Blough DK, Kaplan RM, Ramsey SD, Fishman AP, et al. Costs of pulmonary rehabilitation and predictors of adherence in the National Emphysema Treatment Trial. COPD 2008;5(2):105‐16. [DOI] [PubMed] [Google Scholar]
- Fan VS, Ramsey SD, Blough DK. Costs of pulmonary rehabilitation and predictors of adherence [Abstract]. Poster #608. American Thoracic Society International Conference; 2007 May 18‐23; San Francisco. 2007; Vol. Poster #608.
Foglio 2001 {published data only}
- Foglio K, Bianchi L, Ambrosino N. Is it really useful to repeat outpatient pulmonary rehabilitation programs in patients with chronic airway obstruction? A 2‐year controlled study. Chest 2001;119(6):1696‐704. [DOI] [PubMed] [Google Scholar]
Gadoury 2005 {published data only}
- Gadoury MA, Schwartzman K, Rouleau M, Maltais F, Julien M, Beaupre A, et al. Self‐management reduces both short‐ and long‐term hospitalisation in COPD. European Respiratory Journal 2005;26(5):853‐7. [DOI] [PubMed] [Google Scholar]
Gale 2009 {published data only}
- Gale NS, Duckers JM, Proud D, Lines T, Enright S, Cockcroft JR, et al. Pulmonary rehabilitation improves cardiovascular risk factors in patients with COPD. Thorax 2009;64(Suppl IV):A40 [S75]. [DOI] [PMC free article] [PubMed] [Google Scholar]
Garuti 2010 {published data only}
- Garuti G. Home rehabilitation and therapy. Rassegna di Patologia dell'Apparato Respiratorio 2010;25(2):76‐7. [Google Scholar]
Gautier 1998 {unpublished data only}
- Gautier V, Godard P, Serres I, Hayot M, Prefaut C. Respiratory rehabilitation in chronic obstructive pulmonary disease (COPD) outpatients under long term oxygen therapy. American Journal of Respiratory and Critical Care Medicine 1998;157(Suppl 3):A119. [Google Scholar]
Gautier 2002 {unpublished data only}
- Gautier V, Pison C, Fournial F, Benichou M, Tardif C, Veale D, et al. Home rehabilitation in COPD patients on long term oxygen therapy (LTOT): a multi‐centre randomized controlled study [abstract]. European Respiratory Society Annual Congress; 2002; September 14‐18; Stockholm. 2002:Abstract nr: P1520.
Ghanem 2010 {published data only}
- Ghanem ME, Laal EA, Mehany M, Tolba K. Home‐based pulmonary rehabilitation program: Effect on exercise tolerance and quality of life in chronic obstructive pulmonary disease patients. Annals of Thoracic Medicine 2010;5(1):18‐25. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gimenez 2000 {published data only}
- Gimenez M, Servera E, Vergara P, Bach JR, Polu JM. Endurance training in patients with chronic obstructive pulmonary disease: A comparison of high versus moderate intensity. Archives of Physical Medicine and Rehabilitation 2000;81(1):102‐9. [DOI] [PubMed] [Google Scholar]
Girodo 1992 {published data only}
- Girodo M, Ekstrand KA, Metivier GJ. Deep diaphragmatic breathing: rehabilitation exercises for the asthmatic patient. Archives of Physical Medicine and Rehabilitation 1992;73(8):717‐20. [PubMed] [Google Scholar]
Goldman 1997 {unpublished data only}
- Goldman J, Carr V, Dobson L, Jones S, Rowles R, Wallace L. A randomised controlled trial of pulmonary rehabilitation (PR) in a district general hospital. Thorax 1997;52(Suppl 6):A10. [Google Scholar]
- Goldman J, Carr V, Dobson L, Jones S, Rowles R, Wallace L. Does pulmonary rehabilitation produce a lasting benefit in patients with COPD?. Thorax 1997;52(Suppl 6):A10. [Google Scholar]
Gormley 1993 {published data only}
- Gormley JM, Carrieri‐Kohlman V, Douglas MK, Stulbarg MS. Treadmill self‐efficacy and walking performance in patients with COPD. Journal of Cardiopulmonary Rehabilitation 1993;13(6):424‐31. [Google Scholar]
Gosselink 1990 {unpublished data only}
- Gosselink H, Keimpema A, Wagenaar R, Chadwick Straver R. The relative efficacy of a rehabilitation‐programme in COPD patients. European Respiratory Journal 1990;10(Suppl 3):212S. [Google Scholar]
Green 1999 {published data only}
- Green RH, Singh SJ, Williams J, Morgan MDL. A randomised controlled trial of four weeks v seven weeks pulmonary rehabilitation in chronic obstructive pulmonary disease (COPD). Thorax 1999;54(Suppl 3):S63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green RH, Singh SJ, Williams J, Morgan MDL. A randomised controlled trial of four weeks versus seven weeks of pulmonary rehabilitation in chronic obstructive pulmonary disease. Thorax 2001;56(2):143‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Griffiths 1996 {unpublished data only}
- Griffiths TL, Gregory SE, Ward SA, Saunders KB, Whipp BJ. Effects of structured domicilliary exercise training programme on quality of life and walking tolerance in patients with severe COPD. European Respiratory Journal 1996;9(Suppl 23):145S. [Google Scholar]
Grosbois 1999 {published data only}
- Grosbois JM, Lamblin C, Lemaire B, Chekroud H, Dernis JM, Douay B, et al. Long‐term benefits of exercise maintenance after outpatient rehabilitation program in patients with chronic obstructive pulmonary disease. Journal of Cardiopulmonary Rehabilitation 1999;19(4):216‐25. [DOI] [PubMed] [Google Scholar]
Gu 2011 {published data only}
- Gu W, Chen R, Xi Y. The effect of pulmonary rehabilitation toward expiratory airflow limitation in patients with chronic obstructive pulmonary disease. European Respiratory Society 21st Annual Congress; 2011 Sep 24‐28; Amsterdam 2011;38(55):657s [p3654]. [Google Scholar]
Guell 2006 {published data only}
- Guell R, Lucas P, Galdiz JB, Montemayor T, Rodriguez Gonzalez‐Moro JM, Gorostiza A, et al. Home vs hospital‐based pulmonary rehabilitation for patients with chronic obstructive pulmonary disease: a Spanish multicenter trial. Archivos de Bronconeumologia 2008;44:512‐18. [PubMed] [Google Scholar]
Harver 1989 {published data only}
- Harver A, Mahler DA, Daubenspeck JA. Targeted inspiratory muscle training improves respiratory muscle function and reduces dyspnea in patients with chronic obstructive pulmonary disease. Annals of Internal Medicine 1989;111(2):117‐24. [DOI] [PubMed] [Google Scholar]
Hawkins 1999 {published data only}
- Hawkins P, Nikoletou D, Johnson LC, Moxham J. Increased exercise capacity in patients with severe COPD after cycle training with proportional assist ventilation (PAV). Thorax 1999;54(Suppl 3):A61 (P169). [Google Scholar]
- Hawkins P, Nikoletou D, Johnson LC, Moxham J. Physiological training in severe chronic obstructive pulmonary disease (COPD) is possible using proportional assist ventilation (PAV). Thorax 1999;54(Suppl 3):A61 (P170). [DOI] [PMC free article] [PubMed] [Google Scholar]
Hentschel 2002 {published data only}
- Hentschel M, Becker J, Lepthin HJ. Effects of a high intensity training program on patients with chronic obstructive airways disease (COAD) [Nutzen eines intensiven trainingsprogrammes bei patienten mit obstruktiver atemwegskrankheit]. Pneumologie 2002;56(4):240‐6. [DOI] [PubMed] [Google Scholar]
Holland 2003 {published data only}
- Holland A, Nehez E, Ntoumenopoulos. Unsupported upper limb exercise training in chronic obstructive pulmonary disease ‐ effect on endurance, symptoms and quality of life [Abstract]. Proceedings of the Thoracic Society of Australia & New Zealand, Annual Scientific Meeting; 2003 4‐9 April; Adelaide. 2003:P094.
Hospes 2009 {published data only}
- Hospes G, Bossenbroek L, Hacken NH, Hengel P, Greef MH. Enhancement of daily physical activity increases physical fitness of outclinic COPD patients: results of an exercise counselling program. Patient Education and Counseling 2009;75(2):274‐8. [DOI] [PubMed] [Google Scholar]
Houchen 2011 {published data only}
- Houchen L, Menon M, Harrison S, Sandland C, Morgan M, Singh S, et al. Does protein supplementation enhance the effects of resistance training in patients with COPD?. European Respiratory Society 21st Annual Congress; 2011 Sep 24‐28; Amsterdam 2011;38(55):325s [1888]. [Google Scholar]
Innocenti 2000 {published data only}
- Innocenti F, Fabbri A, Guerrini M, Fonseca D, Lippi P. Results of an outpatient pulmonary rehabilitation program in patients with COPD. European Respiratory Journal 2000;16(Suppl 31):46S. [Google Scholar]
Jensen 1983 {published data only}
- Jensen PS. Risk, protective factors, and supportive interventions in chronic airway obstruction. Archives of General Psychiatry 1983;40(11):1203‐7. [DOI] [PubMed] [Google Scholar]
Johnson 2000 {published data only}
- Johnson LC, Hawkins P, Polkey MI, Moxham J. The effects of pulmonary rehabilitation on inspiratory muscle loading in severe COPD. Thorax 2000;55(Suppl 3):A52. [Google Scholar]
Jungblut 2007 {published data only}
- Jungblut S, Frickmann H, Klingler J, Muller U, Bargon J. Improvement in expiratory peak flow (PEF) of COPD patients due to "lung" sport for 12 months [Verbesserung des exspiratorischen Spitzenflusses (PEF) von COPD‐Patienten durch Lungensport über 12 Monate]. Pneumologie 2007;61(2):83‐5. [DOI] [PubMed] [Google Scholar]
Kaplan 1990 {published data only}
- Kaplan RM. Randomized trial of rehabilitation in chronic obstructive pulmonary disease. Journal of Rehabilitation Research and Development 1991;28(1):268. [Google Scholar]
Katsura 2000 {published data only}
- Katsura H, Yamada K, Motegi T, Kida K. Effectiveness of a short‐course inpatient comprehensive pulmonary rehabilitation program managed by the critical path for COPD in the elderly. American Journal of Respiratory and Critical Care Medicine 2000;161(Suppl 3):A495. [Google Scholar]
Kurabayashi 1998 {published data only}
- Kurabayashi H, Machida I, Handa H, Akiba T, Kubota K. Comparison of three protocols for breathing exercises during immersion in 38 degrees C water for chronic obstructive pulmonary disease. American Journal of Physical Medicine and Rehabilitation 1998;77(2):145‐8. [PubMed] [Google Scholar]
Kurabayashi 2000 {published data only}
- Kurabayashi H, Machida I, Tamura K, Iwai F, Tamura J, Kubota K. Breathing out into water during subtotal immersion: a therapy for chronic pulmonary emphysema. American Journal of Physical Medicine and Rehabilitation 2000;79(2):150‐3. [DOI] [PubMed] [Google Scholar]
Larson 1999 {published data only}
- Larson JL, Covey MK, Wirtz SE, Berry JK, Alex CG, Langbein WE, et al. Cycle ergometer and inspiratory muscle training in chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine 1999;160(2):500‐7. [DOI] [PubMed] [Google Scholar]
Lathlean 2008 {published and unpublished data}
- Lathlean T, Cafarella P, Rowett D, Frith P, Lawrence J. Combining chronic condition self management and pulmonary rehabilitation for COPD patients. Respirology 2008;13(Suppl 5):A172 [P2‐114]. [Google Scholar]
Laukandt 1998 {published data only}
- Laukandt I, Kaspar P, Petro W. Patiententraining in der pneumologischen rehabiltation verbessert die lebensqulität bei patienten mit chronisch obstruktiven atemwegserkrankungen [Patient training in pneumological rehabilitation improves quality of life in patients with chronic obstructive pulmonary disease]. Pneumologie 1998;52(SH1):41S. [Google Scholar]
Levine 1986 {published data only}
- Levine S, Weiser P, Gillen J. Evaluation of a ventilatory muscle endurance training program in the rehabilitation of patients with chronic obstructive pulmonary disease. American Review of Respiratory Disease 1986;133(3):400‐6. [DOI] [PubMed] [Google Scholar]
Lewczuk 1998 {published data only}
- Lewczuk J, Piszko P, Kowalska‐Superlak M, Jagas J, Wojciak S, Wrabec K. Impact of 2‐year rehabilitation on exercise tolerance and transcutaneous oxygen saturation during exercise in patients with chronic obstructive pulmonary disease. Polskie Archiwum Medycyny Wewn¿trznej 1998;100:331‐6. [PubMed] [Google Scholar]
- Piszko P, Lewczuk J, Kowalska Superlak M, Wrabec K. Oxygen saturation at rest, on exercise and during sleep in patients with COPD undergoing pulmonary rehabilitation program. Two years, prospective, controlled study [Kontrolowane badanie przezskorne wysycenia tlenem krwi tetniczej w czasie dnia, w nocy oraz w czasie wysiiku u rehabilitowanych chorych na pochp]. Pneumonologia i Alergologia Polska 2002;70:11‐2. [PubMed] [Google Scholar]
Li 2002 {published data only}
- Li YL. Nutritional supplementation and respiratory gym in patients with chronic obstructive pulmonary disease. Zhongguo Linchuang Kangfu (Chinese Journal of Clinical Rehabilitation) 2002;6(9):1260‐2. [Google Scholar]
Liu 2002 {published data only}
- Liu YF. Effects of the comprehensive pulmonary rehabilitation programme on the quality of life of the patients with COPD in recovery period. Zhongguo Linchuang Kangfu (Chinese Journal of Clinical Rehabilitation) 2002;6(21):3170‐1. [Google Scholar]
Lotshaw 2003 {published data only}
- Lotshaw A, Duncan C, Hart M, Millard M. Land and water‐based pulmonary rehabilitation; a comparison of physical performance and quality of life in patients with COPD [Abstract]. National COPD Conference; 2003 November 14‐15; Arlington. 2003:Abstract no: 1143.
Ma 2002 {published data only}
- Ma HM, Chan WC, Chung PH, Tung SY, Dai LK, Sung JY. A randomised control study of 3‐week versus 4‐week pulmonary rehabilitation program (PRP) for moderate to severe geriatric COPDs in Hong Kong. Chest Meeting; 2002 2‐7 November 2002; San Diego. 2002:P195.
Mador 2002 {published data only}
- Mador MJ, Bozkanat E, Aggarwal A, Shaffer M, Kufel TJ. Does strength training alter quadriceps fatigability in patients with COPD. American Journal of Respiratory and Critical Care Medicine 2002;165(Suppl 8):A506. [Google Scholar]
Mador 2004 {published data only}
- Mador MJ, Bozkanat E, Aggarwal A, Shaffer M, Kufel TJ. Endurance and strength training in patients with COPD. Chest 2004;125(6):2036‐45. [DOI] [PubMed] [Google Scholar]
- Mador MJ, Deniz O, Aggarwal A, Shaffer M, Kufel TJ, Spender CM. Effect of respiratory muscle endurance training in patients with COPD undergoing pulmonary rehabilitation. Chest 2005;128(3):1216‐24. [DOI] [PubMed] [Google Scholar]
- Mador MJ, Deniz O, Aggarwal A, Shaffer M, Kufel TJ, Spengler CM. Effect of respiratory muscle endurance training in patients with COPD undergoing pulmonary rehabilitation [Abstract]. American Thoracic Society 99th International Conference; 2003 May 16‐21; Seattle. 2003:B046, Poster D8. [DOI] [PubMed]
Make 2000 {published data only}
- Make B, Tolliver R, Christensen P, Karla S, MacIntyre N, Ries A. Pulmonary rehabilitation improves exercise capacity and dyspnea in the national emphysema treatment trial (NETT). American Journal of Respiratory and Critical Care Medicine 2000;161(Suppl 3):A254. [Google Scholar]
Martinez 1993 {published data only}
- Martinez FJ, Vogel PD, Dupont DN, Stanopoulos I, Gray A, Beamis JF. Supported arm exercise vs unsupported arm exercise in the rehabilitation of patients with severe chronic airflow obstruction. Chest 1993;103(5):1397‐402. [DOI] [PubMed] [Google Scholar]
McKeogh 2012 {published data only}
- McKeough ZJ, Bye PTP, Alison JA. Arm exercise training in chronic obstructive pulmonary disease: a randomised controlled trial. Chronic Respiratory Disease 2012;9(3):153–62. [DOI] [PubMed] [Google Scholar]
Morgan 1999 {published data only}
- Morgan MDL. The prediction of benefit from pulmonary rehabilitation: setting, training intensity and the effect of selection by disability. Thorax 1999;54(Suppl 2):S3‐S7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Moros Garcia 1996 {published data only}
- Moros Garcia JSM, Cisneros Lanuza MT, Rubio Obanos MT, Samperiz Legarre AL, Escolar Castellon F, Moros Garcia MT. Rehabilitation of disability in COPD [Rehabilitacion de la discapacidad en la enfermedad pulmonar obstructiva cronica]. Rehabilitacion 1996;30:194‐200. [Google Scholar]
Morris 2003 {published data only}
- Morris N, Sabapathy S, Kingsley R, Schneider D, Adams L. Improved exercise tolerance with intermittent exercise in patients with moderate COPD [Abstract]. American Thoracic Society 99th International Conference; 2003 May 16‐21; Seattle. 2003:C042, Poster C34.
MTU 2003 {published data only}
- Medical Technology Unit‐Federal Social Insurance Office Switzerland. Effectiveness of Rehabilitation in Chronic Obstructive Pulmonary Disease. Bern, Switzerland: Swiss Federal Office of Public Health, 2003. [Google Scholar]
Murphy 2004 {published data only}
- Murphy M, Campbell M, Saunders J, Jackson B, Rangan N, Zimmerman F, et al. A randomised, controlled trial of pulmonary rehabilitation, weekly exercise and better health self‐management in COPD [Abstract]. Respirology 2004;9(Suppl 2):A48. [Google Scholar]
- Murphy MC, Berlowitz DJ, Saunders JE, Campbell M, Jackson B. A randomised trial to compare pulmonary rehabilitation (PRP) & the Stanford model chronic disease self management program (CDSMP) in COPD with 12 month follow‐up. Respirology 2005;10(Suppl):A61. [Google Scholar]
Myers 2000 {published data only}
- Myers R, Ries AL, Kaplan RM, Prewitt LM. Pulmonary rehabilitation: outcome measures and maintenance. American Journal of Respiratory and Critical Care Medicine 2000;161(Suppl 3):A254. [DOI] [PubMed] [Google Scholar]
Na 2005 {published data only}
- Na JO, Kim DS, Yoon SH, Jegal YJ, Kim WS, Kim ES, et al. A simple and easy home‐based pulmonary rehabilitation programme for patients with chronic lung diseases. Monaldi Archives for Chest Disease 2005;63(1):30‐6. [DOI] [PubMed] [Google Scholar]
Nasilowski 2011 {published and unpublished data}
- Nasilowski J, Przybylowski T, Zielinski J, Chazan R, Sliwinski P, Bielen P, et al. Stationary bicycle training at home in COPD patient on LTOT. Is it enough to improve quality of life and exercise capacity? A pilot study. European Respiratory Society 21st Annual Congress; 2011 Sep 24‐28; Amsterdam 2011;38(55):881s [P4813]. [Google Scholar]
Nava 1998 {published data only}
- Nava S. Rehabilitation of patients admitted to a respiratory intensive care unit. Archives of Physical Medicine and Rehabilitation 1998;79(7):849‐54. [DOI] [PubMed] [Google Scholar]
Ndundu 2001 {published data only}
- Muzembo Ndundu J, Nkakudulu Bikuku H, Frans A. Respiratory rehabilitation in patients with bronchial asthma and chronic obstructive pulmonary disease (COPD) in Kinshasa. Revue de Pneumologie Clinique 2001;57(3):209‐18. [PubMed] [Google Scholar]
Neder 2002 {published data only}
- Neder JA, Sword D, Cochrane LK, Mackay E, Ward SA, Clark CJ. A new rehabilitative strategy for severely‐disabled patients with advanced COPD: neuromuscular electrical stimulation. American Journal of Respiratory and Critical Care Medicine 2001;163(Suppl 5):A967. [Google Scholar]
- Neder JA, Sword D, Ward SA, Mackay E, Cochrane LM, Clark CJ. Home based neuromuscular electrical stimulation as a new rehabilitative strategy for severely disabled patients with chronic obstructive pulmonary disease (COPD). Thorax 2002;57(4):333‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Newall 2000 {published data only}
- Newall C, Richardson B, McConnell AK, Stockley RA, Hill SL. Inspiratory muscle training (IMT) as an adjunct to a pulmonary rehabilitation programme in COPD. American Journal of Respiratory and Critical Care Medicine 2000;161(Suppl 3):A753. [Google Scholar]
Nguyen 2005 {published data only}
- Nguyen HQ, Carrieri‐Kohlman V. Dyspnea self‐management in patients with chronic obstructive pulmonary disease: moderating effects of depressed mood. Psychosomatics 2005;46(5):402‐10. [DOI] [PubMed] [Google Scholar]
Ninot 2011 {published data only}
- Ninot G, Moullec G, Picot MC, Jaussent A, Hayot M, Desplan M, et al. Cost‐saving effect of supervised exercise associated to COPD self‐management education program. Respiratory Medicine 2011;105(3):377‐85. [DOI] [PubMed] [Google Scholar]
Nosworthy 1992 {published data only}
- Nosworthy J, Barter C, Thomas S, Flynn M. An evaluation of three elements of pulmonary rehabilitation. The Australian Journal of Physiotherapy 1992;38(3):189‐93. [DOI] [PubMed] [Google Scholar]
Nygren‐Bonnier 2002 {published data only}
- Nygren‐Bonnier M, Karlsson S, Klefbeck B. Effects of a home‐based training program and an outpatient hospital‐based training program on patients with chronic obstructive pulmonary disease (COPD) [Abstract]. European Respiratory Society 12th Annual Congress; 2002 Sep 14‐18; Stockholm. 2002:abstract nr: P1166.
O'Hara 1987 {published data only}
- O'Hara WJ, Lasachuk KE, Matheson PC, Renahan MC, Schlotter DG, Lilker ES. Weight training benefits in chronic obstructive pulmonary disease: a controlled crossover study. Respiratory Care 1987;32(8):660‐8. [Google Scholar]
Ortega 2002 {published data only}
- Cejudo P, Ortega F, Villagomez R, Hernandez A, Toral J, Sanchez H, et al. Effects of peripheral muscle training on dyspnea and leg pain in patients with chronic obstructive pulmonary disease. European Respiratory Journal 2001;18(Suppl 33):188S. [Google Scholar]
- Ortega F, Toral J, Cejudo P, Villagomez R, Sanchez H, Castillo J, et al. Comparison of effects of strength and endurance training in patients with chronic obstructive pulmonary disease. American Journal or Respiratory and Critical Care Medicine 2002;166(5):669‐74. [DOI] [PubMed] [Google Scholar]
- Toral Marìn J, Ortega F, Cejudo P, Elìas T, Sanchez H, Montemayor T. Effects of an exercise training programme on the quality of life of patients with COPD [Repercusiones en la calidad de vida de un programa de entrenamiento con ejercio en pacientes con EPOC]. Archivos de Bronconeumologìa 1998;34(Suppl 1):64. [Google Scholar]
- Toral Marìn J, Ortega F, Cejudo P, Elìas T, Sanchez H, Montemayor T. Physiological effects of an exercise training programme in patients with stable COPD [Repercusion fisiolgica de un programa de entrenamento con ejercio en pacientes con EPOC estable]. Archivos de Bronconeumologìa 1998;34(Suppl 1):33. [Google Scholar]
Patessio 1994 {published data only}
- Patessio A, Donner CF. Selection criteria for exercise training in patients with COPD. Z‐Kardiol 1994;83(Suppl 3):155‐8. [PubMed] [Google Scholar]
Petersen 2008 {published data only}
- Petersen AM, Mittendorfer B, Magkos F, Iversen M, Pedersen BK. Physical activity counteracts increased whole‐body protein breakdown in chronic obstructive pulmonary disease patients. Scandinavian Journal of Medicine and Science in Sports. 2008;18(5):557‐64. [DOI] [PubMed] [Google Scholar]
Piantadosi 2000 {published data only}
- Piantadosi S. A prospective randomized trial of lung volume reduction surgery. Journal of Cardiopulmonary Rehabilitation 2000;20(1):24‐36. [DOI] [PubMed] [Google Scholar]
Pison 2001 {published data only}
- Pison C. Exercise retraining in severe chronic obstructive bronchopneumopathy [Le Réentraînement a l'effort en pratique]. Revue Des Maladies Respiratoires 2001;18(2):S35‐6. [PubMed] [Google Scholar]
Pison 2008 {published data only}
- Pison CM, Cano NJ, Cherion C, Caron F, Antonini MT, Gonzalez‐Bermejo J, et al. Multimodal nutritional rehabilitation improves clinical outcomes of malnourished patients with chronic respiratory failure: a randomised controlled trial. Thorax 2011;66(11):953‐60. [DOI] [PubMed] [Google Scholar]
Pitta 2004 {unpublished data only}
- Pitta F, Brunetto AF, Padovani CR, Godoy I. Effects of isolated cycle ergometer training on patients with moderate‐to‐severe chronic obstructive pulmonary disease. Respiration 2004;71(5):477‐83. [DOI] [PubMed] [Google Scholar]
- Oliveira Pitta F, Brunetto AF, Probst VS, Padovani CR, Godoy I. Effects of isolated lower extremity training with cycle‐ergometer in moderate/severe COPD patients [Abstract]. European Respiratory Journal 2002;20(Suppl 38):18S. [Google Scholar]
Ponsioen 2010 {published data only}
- Ponsioen B. Temporary effect of physiotherapy for moderately severe COPD. Nederlands Tijdschrift voor Geneeskunde 2010;154(21):1021. [Google Scholar]
Prince 1989 {published data only}
- Prince KL, Helm M. Effectiveness of a rehabilitation programme in chronic bronchitis and emphysema. Clinical Rehabilitation 1989;3:211‐4. [Google Scholar]
Probst 2003 {published data only}
- Probst VS, Heyvaert H, Coosemans I, Pitta F, Spruit MA, Troosters T, et al. Effects of a rollator on exercise capacity, gas exchange and ventilation in COPD patients [Abstract]. American Thoracic Society 99thInternational Conference; 2003 May 16‐21; Seattle. 2003:C042, Poster C36.
- Probst VS, Troosters T, Coosemans I, Spruit MA, Pitta FDO, Decramer M, et al. Mechanisms of improvement in exercise capacity using a rollator in patients with COPD. Chest 2004;126(4):1102‐7. [DOI] [PubMed] [Google Scholar]
Proshchaev 2009 {published data only}
- Proshchaev KI, Il'nitskii AN, Medvedev DS, Altukhov AA, Aksenov DV, Sovenko GN, et al. The role of the short‐wave therapy in rehabilitation of elderly patents with chronic obstructive pulmonary disease. Uspekhi Gerontologii / Rossiiskaia Akademiia Nauk, Gerontologicheskoe Obshchestvo (Advances in Gerontology) 2009;22(2):368‐71. [PubMed] [Google Scholar]
Puente 1996 {published data only}
- Puente Maestu L, Sanz ML, Sanz P, Mayol P, Lucas P, Cubillo JM. Training effects of a partly supervised exercise program in COPD patients. European Respiratory Journal 1996;9(Suppl 23):380S. [Google Scholar]
Raschke 1990 {published data only}
- Raschke F, Schlenker E, Fischer J. Development of nocturnal oxygen desaturation, sleep disorders, and pulmonary function during rehabilitation in chronic obstructive bronchitis. European Respiratory Journal 1990;3(Suppl 10):326S. [Google Scholar]
Regiane Resqueti 2007 {published data only}
- Regiane Resqueti V, Gorostiza A, Galdiz JB, Lopez de Santa Maria E, Casan Clara P, Guell Rous R. Benefits of a home‐based pulmonary rehabilitation program for patients with severe chronic obstructive pulmonary disease. Archivos de Bronconeumologia 2007;43(11):599‐604. [DOI] [PubMed] [Google Scholar]
Reilly 2000 {published data only}
- Reilly J, Moy M, Kaplan R, Diaz P, Benditt J, Criner G, et al. Predictors of improved health‐related quality of life (QOL) following pulmonary rehabilitation in the national emphysema treatment trial (NETT). American Journal of Respiratory and Critical Care Medicine 2000;161(Suppl 3):A503. [Google Scholar]
Riario‐Sforza 2009 {published data only}
- Riario‐Sforza G, Gincorvaia C, Paterniti F, Pessina L, Caligiuri R, Pravettoni C, et al. Effects of pulmonary rehabilitation on exercise capacity in patients with COPD: a number needed to treat study. International Journal of COPD 2009;4:315‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ries 1986 {published data only}
- Ries AL, Moser KM. Comparison of isocapnic hyperventilation and walking exercise training at home in pulmonary rehabilitation. Chest 1986;90(2):285‐9. [DOI] [PubMed] [Google Scholar]
Ries 1988 {published data only}
- Ries AL, Ellis B, Hawkins RW. Upper extremity exercise training in chronic obstructive pulmonary disease. Chest 1988;93(4):688‐92. [DOI] [PubMed] [Google Scholar]
Ries 1995 {published data only}
- Ries AL, Kaplan RM, Limberg TM, Prewitt LM. Effects of pulmonary rehabilitation on physiologic and psychological outcomes in patients with chronic obstructive pulmonary disease. Annals of Internal Medicine 1995;122:823‐32. [DOI] [PubMed] [Google Scholar]
Roberts 1999 {published data only}
- Roberts E, Wallace L, Rowles R, Jones S, Dobson L, Goldman JM. Do the effects of pulmonary rehabilitation (PR) last for 1 year in patients with COPD?. Thorax 1999;54(Suppl 3):64S. [Google Scholar]
Rooyackers 1996 {published data only}
- Rooyackers JM, Dekhuijzen PN, Herwaarden CL, Folgering HT. Long‐term effects of training in patients with COPD and exercise hypoxaemia. European Respiratory Journal 1996;9(Suppl 23):145S. [Google Scholar]
Rudkin 1997 {published data only}
- Rudkin ST, Harrison S, Harvey I, White RJ. A randomised trial of hospital v home rehabilitation in severe chronic obstructive pulmonary disease (COPD). Thorax 1997;52(Suppl 6):41S. [Google Scholar]
Santiworakul 2009 {published data only}
- Santiworakul A, Jarungjitaree S, Jalayondeja W, Chantarothorn S, Supaibulpipat S. Effect of lower extremity exercise on muscle strength and physical capacity in COPD patients. Journal of the Medical Association of Thailand 2009;92(4):556‐63. [PubMed] [Google Scholar]
Sassi‐Dambron 1995 {published data only}
- Sassi‐Dambron DE, Eakin EG, Ries AL, Kaplan RM. Treatment of dyspnea in COPD. A controlled clinical trial of dyspnea management strategies. Chest 1995;107(3):724‐9. [DOI] [PubMed] [Google Scholar]
Saunders 1965 {published data only}
- Saunders KB, White JE. Controlled trial of breathing exercises. British Medical Journal 1965;5463:680‐2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Scherer 1998 {published data only}
- Scherer YK, Schmieder LE, Shimmel S. The effects of education alone and in combination with pulmonary rehabilitation on self‐efficacy in patients with COPD. Rehabilitation Nursing 1998;23(2):71‐7. [DOI] [PubMed] [Google Scholar]
Scorsone 2010 {published data only}
- Scorsone D, Bartolini S, Saporiti R, Braido F, Baroffio M, Pellegrino R, et al. Does a low‐density gas mixture or oxygen supplementation improve exercise training in COPD?. Chest 2010;138(5):1133‐9. [DOI] [PubMed] [Google Scholar]
Semenyuk 2007 {published data only}
- Semenyuk S, Belevskiy A. Influence of the education program for COPD patients on a health related quality of life. Chest 2007;132(4):534s. [Google Scholar]
Serres 1997 {published data only}
- Serres I, Varray A, Vallet G, Micallef JP, Prefaut C. Improved skeletal muscle performance after individualized exercise training in patients with chronic obstructive pulmonary disease. Journal of Cardiopulmonary Rehabilitation 1997;17(4):232‐8. [DOI] [PubMed] [Google Scholar]
Sewell 2005 {published data only}
- Sewell L, Singh SJ, Williams JE, Collier RJ, Morgan MDL. Goal directed pulmonary rehabilitation does not significantly improve health status and domestic function. European Respiratory Journal 2001;18(Suppl 33):187S. [Google Scholar]
- Sewell L, Singh SJ, Williams JEA, Collier R, Morgan MDL. Can individualized rehabilitation improve functional independence in elderly patients with COPD?. Chest 2005;128(3):1194‐200. [DOI] [PubMed] [Google Scholar]
Sinclair 1980 {published data only}
- Sinclai DJ, Ingram CG. Controlled trial of supervised exercise training in chronic bronchitis. British Medical Journal 1980;280(6213):519‐21. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sindhwani 2011 {published data only}
- Sindhwani G, Verma A, Biswas D, Srivastava M, Rawat J. A pilot study on domiciliary pulmonary rehabilitation programme in the management of severe chronic obstructive pulmonary disease. Singapore Medical Journal 2011;52(9):689‐93. [PubMed] [Google Scholar]
Sivori 1998 {published data only}
- Sivori M, Rhodius E, Kaplan P, Talarico M, Gorojod G, Carreras B, et al. Exercise training in chronic obstructive pulmonary disease. Medicina 1998;58:717‐27. [PubMed] [Google Scholar]
Solanes Garcia 2004 {published and unpublished data}
- Solanes Garcia I. Evaluate the effects of pulmonary rehabilitation on chronic obstructive pulmonary disease [PhD thesis]. Universitat Autonoma de Barcelona, 2004. [Google Scholar]
Sparrow 1997 {published data only}
- Sparrow D, Gottlieb D, Lieberman S, Garshick E, Schwartzstein R, Celli B. Randomized controlled trial of upper‐extremity exercise training in patients with COPD. Rehabiliation Rearch and Development Progress Reports 1997;July:106‐7. [Google Scholar]
Spruit 2001 {published data only}
- Spruit MA, Gosselink R, Troosters T, Paepe K, Decramer M. Exercise training in patients with COPD and muscle weakness. American Journal of Respiratory and Critical Care Medicine 2001;163(Suppl 5):A967. [Google Scholar]
- Spruit MA, Gosselink R, Troosters T, Decramer M. Rehabilitation of patients with moderate to severe COPD and muscle weakness. European Respiratory Journal 2001;18(Suppl 33):23S. [Google Scholar]
Steele 2008 {published data only}
- Steele BG, Belza B, Cain KC, Coppersmith J, Lakshminarayan S, Howard J, et al. A randomized clinical trial of an activity and exercise adherence intervention in chronic pulmonary disease. Archives of Physical Medicine and Rehabilitation 2008;89(3):404‐12. [DOI] [PubMed] [Google Scholar]
Stellefson 2009 {published data only}
- Stellefson ML. Efficacy of DVD technology in chronic obstructive pulmonary disease self‐management education of rural patients. Dissertation Abstracts International Section A: Humanities and Social Sciences 2009;70(2‐A):488. [Google Scholar]
Sudo 1997 {published data only}
- Sudo E, Ohga E, Matsuse T, Teramoto S, Nagase T, Katayama H, et al. The effects of pulmonary rehabilitation combined with inspiratory muscle training on pulmonary function and inspiratory muscle strength in elderly patients with chronic obstructive pulmonary disease. Japanese Journal of Geriatrics 1997;34:929‐34. [DOI] [PubMed] [Google Scholar]
Sugawara 2007 {published data only}
- Sugawara K, Takashi H, Kasai C, Kiyokawa N, Watanabe T, Fujii S, et al. Comprehensive pulmonary rehabilitation improves systemic inflation in patients with stable COPD. European Respiratory Journal 2007;30(Suppl 51):514s [E3082]. [Google Scholar]
Sun 2003 {published data only}
- Sun JX, Yin MX, Shao H, Li ZS, Li S W. Effect of respiratory muscle gymnastics on lung function and quality of life in the old patients with chronic obstructive pulmonary disease. Zhonghua Linchuang Kangfu Zazhi 2003;7(27):3698‐9. [Google Scholar]
Swerts 1990 {published data only}
- Swerts PM, Kretzers LM, Terpstra‐Lindeman E, Verstappen FT, Wouters EF. Exercise reconditioning in the rehabilitation of patients with chronic obstructive pulmonary disease: a short‐ and long‐term analysis. Archives of Physical Medicine and Rehabilitation 1990;71(8):570‐3. [PubMed] [Google Scholar]
Taylor 2012 {published data only}
- Taylor SJC, Sohanpal R, Bremner SA, Devine A, McDaid D, Fernandez JL, et al. Self‐management support for moderate‐to‐severe chronic obstructive pulmonary disease: a pilot randomised controlled trial. British Journal of General Practice 2012;62(603):e687‐95. [DOI] [PMC free article] [PubMed] [Google Scholar]
Toevs 1984 {published data only}
- Toevs CD, Kaplan RM, Atkins CJ. The costs and effects of behavioral programs in chronic obstructive pulmonary disease. Medical Care 1984;22(12):1088‐100. [DOI] [PubMed] [Google Scholar]
Troosters 1999 {published data only}
- Troosters T, Gosselink R, Decramer M. Pulmonary rehabilitation in patients with severe chronic obstructive pulmonary disease. Monaldi Archives for Chest Disease 1999;54(6):510‐3. [PubMed] [Google Scholar]
Tsang 2001 {published data only}
- Tsang AH, Carrieri‐Kohlman V, Janson S, Gold W, Stulbarg MS. Effectiveness of three strengths of education and exercise on self‐efficacy for walking in patients with COPD. American Journal of Respiratory and Critical Care Medicine 2001;163(Suppl 5):A968. [Google Scholar]
Ubaidullayev 1990 {published data only}
- Ubaidullayev AM. Rehabilitation of patients with chronic bronchitis. European Respiratory Journal 1990;3(Suppl 10):412S. [Google Scholar]
Vargas 1998 {published data only}
- Vargas R, Sanchez H, Castillo D, Cehudo P, Ortega F, Montemayor T. Repercusion del entrenamiento muscular ventilatorio sobre la disnea, ejercicio y calidad de vida en la EPOC. Neumosur 1998;10(1):18. [Google Scholar]
- Vargas R, Sánchez H, Castillo D, Cejudo P, Ortega F, Montemayor T. Impact of ventilatory muscle training on dyspnea, exercise and quality of life in COPD. Neumosur 1998;10(1):17. [Google Scholar]
Vogiatzis 1999 {published data only}
- Vogiatzis I, Sherman R, Williamson A, Miles J, Taylor I. Physiological effects of rehabilitative exercise training in patients with chronic obstructive pulmonary disease (COPD). Journal of Sports Sciences 1999;17:544‐5. [Google Scholar]
- Vogiatzis I, Williamson A, Miles J, Taylor I. Effects of a 12‐week supervised outpatient rehabilitation programme on physical performance in patients with COPD in the north east of England. Thorax 1997;52(Suppl 6):P24. [Google Scholar]
- Vogiatzis I, Williamson AF, Miles J, Taylor IK. Physiological response to moderate exercise workloads in a pulmonary rehabilitation program in patients with varying degrees of airflow obstruction. Chest 1999;116:1200‐7. [DOI] [PubMed] [Google Scholar]
- Williamson A, Vogiatzis I, Miles J, Taylor I. Effects of rehabilitation on exercise tolerance & quality of life in patients with chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine 1998;157(Suppl 3):A117. [Google Scholar]
Vogiatzis 2001 {published data only}
- Vogiatzis I, Sideri D, Pentaraki M, Komboti M, Nanas S, Roussos C. Interval versus continuous rehabilitative exercise training at the same time maintained intensity in patients with COPD: a randomised trial of the effects on exercise tolerance and quality of life. American Journal of Respiratory and Critical Care Medicine 2001;163(5 Suppl):A968. [Google Scholar]
Vogiatzis 2002 {published data only}
- Vogiatzis I, Nanas S, Roussos C. Interval training as an alternative modality to continuous exercise in patients with COPD. European Respiratory Journal 2002;20:12‐9. [DOI] [PubMed] [Google Scholar]
- Vogiatzis I, Nanas S, Sakelariou D, Kasiotis C, Papazahou O, Sideri D, et al. Interval training as an alternative rehabilitative modality to continuous exercise in patients with COPD: a randomised trial. European Respiratory Journal 2001;18(Suppl 33):187S. [Google Scholar]
- Vogiatzis I, Sideri D, Pentaraki M, Komboti M, Nanas S, Roussos C. Interval versus continuous rehabilitative exercise training at the same maintained intensity in patients with COPD: a randomised trial of the effects on exercise tolerance and quality of life. American Journal of Respiratory and Critical Care Medicine 2001;163(Suppl 5):A968. [Google Scholar]
- Vogiatzis I, Williamson AF, Miles J, Taylor IK. Long‐term benefits of supervised maintenance rehabilitation strategies in patients with COPD: a 12‐month randomised trial at an outpatient setting. European Respiratory Journal 2000;16(Suppl 31):159S. [Google Scholar]
- Williamson A, Vogiatzis L, Miles J, Taylor I. Long term benefits of pulmonary rehabilitation on exercise tolerance in patients with chronic obstructive pulmonary disease (COPD). European Respiratory Journal 1998;12(Suppl 28):405S. [Google Scholar]
Wadell 2005 {published data only}
- Wadell K. Physical training in patients with chronic obstructive pulmonary disease [Dissertation]. Umea University, 2004. [Google Scholar]
- Wadell K, Henriksson‐Larsen K, Lundgren R, Sundelin G. Group training in patients with COPD – Long‐term effects after decreased training frequency. Disability and Rehabilitation 2005;27(10):571‐81. [DOI] [PubMed] [Google Scholar]
- Wadell K, Lundgren R, Henriksson‐Larsen K, Sundelin G. Training in water and on land in patients with COPD ‐ short and long term perspective [Abstract]. European Respiratory Journal 2004;24(Suppl 48):666s. [Google Scholar]
- Wadell K, Sundelin G, Henriksson‐Larsén K, Lundgren R. High intensity physical group training in water ‐ An effective training modality for patients with COPD. Respiratory Medicine 2004;98(5):428‐38. [DOI] [PubMed] [Google Scholar]
- Wadell K, Sundelin G, Henriksson‐Larsén K, Lundgren R. Physical training in water is effective in patients with COPD ‐ A randomised controlled study. European Respiratory Journal 2002;20(Suppl 38):68s. [Google Scholar]
Wadell 2013 {published data only}
- Wadell K, Webb KA, Preston M, Amornputtisathaporn N, Samis L, Patelli J, et al. Impact of pulmonary rehabilitation on the major dimensions of dyspnea in COPD. Journal of Chronic Obstructive Pulmonary Disease 2013;10:1‐11. [DOI] [PubMed] [Google Scholar]
Wanke 1994 {published data only}
- Wanke T, Formanek D, Lahrmann H, Brath H, Wild M, Wagner C, et al. Effects of combined inspiratory muscle and cycle ergometer training on exercise performance in patients with COPD. European Respiratory Journal 1994;7(12):2205‐11. [DOI] [PubMed] [Google Scholar]
Wedzicha 1998 {published data only}
- Bestall JC, Garrod R, Garnham R, Paul EA, Jones PW, Wedzicha JA. Long term effects of pulmonary rehabilitation in patients with COPD. European Respiratory Journal 1998;12(Suppl 28):2S. [DOI] [PubMed] [Google Scholar]
- Bestall JC, Garrod R, Garnham R, Paul EA, Jones PW, Wedzicha JA. Prolonged effects of pulmonary rehabilitation in patients with COPD. Thorax 1997;52(Suppl 6):40S. [Google Scholar]
- Bestall JC, Garrod R, Garnham R, Paul EA, Jones PW, Wedzicha JA. Randomised controlled trial of pulmonary rehabilitation in house‐bound patients with severe COPD. European Respiratory Journal 1997;10(Suppl 25):393S. [DOI] [PubMed] [Google Scholar]
- Garrod R, Bestall JC, Garnham R, Paul EA, Jones PW, Wedzicha JA. Randomised controlled trial of pulmonary rehabilitation in moderate and severe COPD: prolonged benefits. American Journal of Respiratory and Critical Care Medicine 1998;157(Suppl 3):A257. [Google Scholar]
- Wedzicha JA, Bestall JC, Garrod R, Garnham R, Paul EA, Jones PW. Randomised controlled trial of pulmonary rehabilitation in severe chronic obstructive pulmonary disease patients, stratified with the MRC dyspnoea scale. European Respiratory Journal 1998;12(2):363‐9. [DOI] [PubMed] [Google Scholar]
Weiner 1992a {published data only}
- Weiner P, Azgad Y, Ganam R, Weiner M. Inspiratory muscle training in patients with bronchial asthma. Chest 1992;102(5):1357‐61. [DOI] [PubMed] [Google Scholar]
Wen 2004 {published data only}
- Wen YL, Huang DF, Huang M, Huang YP. Evaluation on the effect of systemic exercise rehabilitation intervention in patients with chronic obstructive pulmonary disease. Zhongguo Linchuang Kangfu 2004;8(12):2224‐5. [Google Scholar]
White 2002 {published data only}
- White RJ, Rudkin ST, Harrison ST, Day KL, Harvey IM. Pulmonary rehabilitation compared with brief advice given for severe chronic obstructive pulmonary disease. Journal of Cardiopulmonary Rehabilitation 2002;22(5):338‐44. [DOI] [PubMed] [Google Scholar]
Worth 1985 {published data only}
- Störiko H, Worth H, Goeckenjan G, Smidt U. Effects of physical training on respiratory muscle endurance in patients with chronic airflow obstruction [Ermüdbarkeit der Atemmuskeln bei Patienten mit obstruktiven]. Praxis und Klinik der Pneumologie 1985;39(Suppl 1):877‐8. [PubMed] [Google Scholar]
- Worth H, Storiko H, Goekenjan G, Smidt U. Effects of physical training on respiratory muscle endurance in patients with chronic airflow limitation [Zur Trainierbarkeit der Atemmuskeln bei Patienten mit obstruktiven Atemwegserkrankungen]. Praxis und Klinik der Pneumologie 1985;39(7):226‐32. [PubMed] [Google Scholar]
Xu 2010 {published data only}
- Xu YH, Wang JH, Li HF, Zhu XH, Wang G. Efficacy of integrative respiratory rehabilitation training in exercise ability and quality of life of patients with chronic obstructive pulmonary disease in stable phase: a randomized controlled trial. Journal of Chinese Integrative Medicine 2010;8(5):432‐7. [DOI] [PubMed] [Google Scholar]
Yamanaka 2009 {published data only}
- Yamanaka Y, Ishikawa A, Miyasaka T, Totsu Y, Urabe Y, Inui K. The effect of unsupervised home exercise program for patients with chronic obstructive pulmonary disease. Nippon Ronen Igakkai Zasshi ‐ Japanese Journal of Geriatrics 2009;46(2):154‐9. [DOI] [PubMed] [Google Scholar]
Yan 1996 {published data only}
- Yan Q, Sun Y. Quantitative research for improving respiratory muscle contraction by breathing exercise. Chinese Medical Journal 1996;109(10):771‐5. [PubMed] [Google Scholar]
Yosbauran 1996 {published data only}
- Yosbauran N, Cimrin A, Tureyen ZC, Elci OC, Kostek N, Ozsoz A, et al. Evaluation of the impact of group exercises on the quality of life in patients with chronic obstructive pulmonary disease. European Respiratory Journal 1996;9(Suppl 23):381S. [Google Scholar]
Zanini 2002 {published data only}
- Zanini A, Giorgetti G, Facchetti C, Mazzucchelli G, Conti S, Lucioni A, et al. Efficacy of a rehabilitation program based on circuit training in COPD subjects: a preliminary report. American Journal of Respiratory and Critical Care Medicine 2002;165(Suppl 8):A738. [Google Scholar]
Zhang 2008 {published data only}
- Zhang ZQ, Chen RC, Yang QK, Li P, Wang CZ, Zhang ZH. A randomized controlled trial study of pulmonary rehabilitation with respiratory physiology as the guide on prognosis in patients with chronic obstructive pulmonary disease. Chinese Critical Care Medicine 2008;20(10):607‐10. [PubMed] [Google Scholar]
References to studies awaiting assessment
Aksu 2006 {published data only}
- Aksu B, Inanir M, Basyigit I, Dursun N, Yildiz F. Comparison of two different exercise programs in chronic obstructive pulmonary disease [Abstract]. European Respiratory Journal 2006;28(Suppl 50)(5555c):3198. [Google Scholar]
D'Amico 2010 {published data only}
- D'Amico F, Grasso R, Chirafisi F. Adapted physical activity in elderly people with chronic obstructive bronchopneumopathy and hypertension.. High Blood Pressure and Cardiovascular Prevention 2010;17(3):131‐90. [Google Scholar]
Meshcheryakova 2010 {published data only}
- Meshcheryakova N, Belevskiy A, Cherniak A, Semashko O. The role of exercise and respiratory training on the depression level in COPD patients [Abstract]. European Respiratory Society 20th Annual Congress; 2010 Sep 18‐22; Barcelona 2010;18(22):632. [Google Scholar]
Meshcheryakova 2012 {published and unpublished data}
- Meshcheryakova N, Belevskiy A, Cherniak A. Physical training is a universal method of pulmonary rehabilitation of patients with chronic obstructive pulmonary disease]. [Russian]. Terapevticheskii Arkhiv 2012;3:17‐21. [PubMed] [Google Scholar]
Ren 2011 {published data only}
- Ren L, Li QY, Du JB, Zhou JM, Weng QL, Chen XH. Comparison of different strategies of pulmonary rehabilitation for patients with COPD of different severity. Journal of Shanghai Jiaotong University (Medical Science) 2011;31(5):620‐4. [Google Scholar]
References to ongoing studies
Chang 2008 {published data only}
- Chang AT, Haines T, Jackson C, Yang I, Nitz J. Rationale and design of the PRSM study: pulmonary rehabilitation or self management for chronic obstructive pulmonary disease (COPD), what is the best approach?. Contemporary Clinical Trials 2008;29(2):796‐800. [DOI] [PubMed] [Google Scholar]
Gurgun 2011 {published data only}
- Gurgun A, Tuncel S, Korkmaz Ekren P, Deniz PS, Karapolat H, Kayahan B. Efficacy of an eight‐week pulmonary rehabilitation in COPD patients: an experience of a single center In Turkey. American Journal of Respiratory and Critical Care Medicine 2011;183:A5049. [Google Scholar]
Sathyapala 2008 {published data only}
- Sathyapala SA, Marsh GS, Seymour JM, Moxham J, Polkey MI. Effect of repetitive magnetic stimulation training of the quadriceps, compared with exercise therapy, on quadriceps strength in patients with chronic obstructive pulmonary disease. Thorax 2008;63:A16‐A17. [Google Scholar]
Additional references
AACVPR 2011
- AACVPR. Guidelines for Pulmonary Rehabilitation Programs. 4th Edition. Chicago, IL: American Association of Cardiovascular and Pulmonary Rehabilitation, 2011. [Google Scholar]
Agusti 2003
- Agusti AGN, Noguera A, Sauleda E, Sala E, Pons J, Busquets X. Systemic effects of chronic obstructive pulmonary disease. European Respiratory Journal 2003;21:347‐60. [DOI] [PubMed] [Google Scholar]
Agusti 2005
- Agusti AGN. COPD, a multicomponent disease: implications for management. Respiratory Medicine 2005;99:670‐82. [DOI] [PubMed] [Google Scholar]
ATS 1999
- American Thoracic Society. Pulmonary rehabilitation. American Journal of Respiratory and Critical Care Medicine 1999;159:1666‐82. [DOI] [PubMed] [Google Scholar]
Beauchamp 2011
- Beauchamp MK, Janaudis‐Ferreira T, Goldstein RS, Brooks D. Optimal duration of pulmonary rehabilitation for individuals with chronic obstructive pulmonary disease ‐ a systematic review. Chronic Respiratory Disease 2011;8(2):129‐400. [DOI] [PubMed] [Google Scholar]
Bolton 2013
- Bolton CE, Bevan‐Smith EF, Blakey JD, et al. British Thoracic Society guideline on pulmonary rehabilitation in adults. Thorax 2013;68:ii1–ii30. [DOI] [PubMed] [Google Scholar]
Bourbeau 2003
- Bourbeau J, Julien M, Maltais F, Rouleau M, Beaupre A, Begin R, et al. Reduction of hospital utilization in patients with chronic obstructive pulmonary disease: a disease‐specific self‐management intervention. Archives of Internal Medicine 2003;163:585‐91. [DOI] [PubMed] [Google Scholar]
Bourbeau 2007
- Bourbeau J, Nault D. Self‐management strategies in chronic obstructive pulmonary disease. Clinics in Chest Medicine 2007;28(3):617‐28. [DOI] [PubMed] [Google Scholar]
Bourbeau 2010
- Bourbeau J. Making pulmonary rehabilitation a success in COPD. Swiss Medical Weekly 2010;140:w13067. [DOI] [PubMed] [Google Scholar]
British Thoracic Society 2001
- British Thoracic Society Standards of Care Committee. Pulmonary rehabilitation. British Thoracic Society Standards of Care Subcommittee on Pulmonary Rehabilitation. Thorax 2001;56:827‐34. [Google Scholar]
Brooks 2002
- Brooks D, Krip B, Mangovski‐Alzamora S, Goldstein RS. The effect of post‐rehabilitation programmes among individuals with chronic obstructive pulmonary disease. European Respiratory Journal 2002;20(1):20‐9. [DOI] [PubMed] [Google Scholar]
Brooks 2007
- Brooks D, Sottana R, Bell B, Hanna M, Laframboise L, Selvanayagarajah S, et al. Characterization of pulmonary rehabilitation programs in Canada in 2005. Canadian Respiratory Journal 2007;14(2):87‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
Casaburi 1991
- Casaburi R, Patessio A, Loli F, Zanaboni S, Donner CF, Wasserman K. Reductions in exercise lactic acidosis and ventilation as a result of exercise training in patients with obstructive lung disease. American Review of Respiratory Disease 1991;143:9‐18. [DOI] [PubMed] [Google Scholar]
Casaburi 2009
- Casaburi R, ZuWallack R. Pulmonary rehabilitation for management of chronic obstructive pulmonary disease. New England Journal of Medicine 2009;360(13):1329‐35. [DOI] [PubMed] [Google Scholar]
Casanova 2011
- Casanova C, Torres JP, Aguirre‐Jaíme A, Pinto‐Plata V, Marin JM, Cordoba E. The progression of chronic obstructive pulmonary disease is heterogeneous: the experience of the BODE cohort. American Journal of Respiratory and Critical Care Medicine 2011;184(9):1015‐21. [DOI] [PubMed] [Google Scholar]
Corrado 1995
- Corrado A, Gorini M, Paola E, Martorana P, Villella G, Augustynen A, et al. Effects of a short outpatient pulmonary rehabilitation program (PRP) in severe COPD patients with chronic respiratory insufficiency (CRI). European Respiratory Journal 1995;8(Suppl 19):126S. [Google Scholar]
Curtis 2003
- Curtis JR, Patrick DL. The assessment of health status among patients with COPD. European Respiratory Journal 2003;21:(Suppl. 41):36s–45s. [DOI] [PubMed] [Google Scholar]
de Torres 2002
- Torres JP, Pinto‐Plata V, Ingenito E, Bagley P, Gray A, Berger R, et al. Power of outcome measurements to detect clinically significant changes in pulmonary rehabilitation of patients with COPD. Chest 2002;121:1092‐8. [DOI] [PubMed] [Google Scholar]
Egger 1997
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple, graphical test. BMJ 1997;13(315):629‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Eisner 2010
- Eisner MD, Anthonisen N, Coultas D, Kuenzli N, Perez‐Padilla R, Postma D, et al. An official American Thoracic Society public policy statement. Novel risk factors and the global burden of chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine 2010;182(5):693‐718. [DOI] [PubMed] [Google Scholar]
Fernández 1998
- Fernández J, Martín M, Moreno LF. Evaluation of a home‐based rehabilitation program controlled with pulse‐meter in COPD. Neumosur 1998;10(1):54‐5. [Google Scholar]
Ferreira 2012
- Ferreira IM, Brooks D, White J, Goldstein R. Nutritional supplementation for stable chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews 2012, Issue 12. [DOI: 10.1002/14651858.CD000998.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Fishman 1994
- Fishman AP. Pulmonary rehabilitation research. American Journal of Respiratory and Critical Care Medicine 1994;149:825‐33. [DOI] [PubMed] [Google Scholar]
Forey 2011
- Forey BA, Thornton AJ, Lee PN. Systematic review with meta‐analysis of the epidemiological evidence relating smoking to COPD, chronic bronchitis and emphysema. BMC Pulmonary Medicine 2011;11:36. [DOI] [PMC free article] [PubMed] [Google Scholar]
Franchi 2009
- Franchi M. EFA book on chronic obstructive pulmonary disease in Europe: sharing and caring. Brussels: European Federation of Allergy and Airways Disease. http://www.efanet.org/documents/EFACOPDBook.pdf (accessed 23 October 2014).
Garcia‐Aymerich 2006
- Garcia‐Aymerich J, Lange P, Benet M, Schnohr P, Anto JM. Regular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: a population based cohort study. Thorax 2006;61(9):772‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
GOLD 2014
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and prevention of Chronic Obstructive Pulmonary Disease. http://www.goldcopd.org/uploads/users/files/GOLD_Report_2014_Jun11.pdf (accessed 24 October 2014).
Gross 2004
- Gross NJ. Outcome measures for COPD treatments; a critical evaluation. COPD 2004;1:41‐57. [DOI] [PubMed] [Google Scholar]
Guarascio 2013
- Guarascio AJ, Ray SM, Finch CK, Self TH. The clinical and economic burden of chronic obstructive pulmonary disease in the USA. Clinicoeconomics and Outcomes Research 2013;5:235–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
Guell 2000
- Guell R, Casan P, Belda J, Sangenis M, Morante F, Guyatt GH, et al. Long‐term effects of outpatient rehabilitation of COPD: a randomized trial. Chest 2000;117(4):976‐83. [DOI] [PubMed] [Google Scholar]
Guyatt 1984
- Guyatt GH, Pugsley SO, Sullivan MJ, Thompson PJ, Berman LB, Jones NL, et al. Effect of encouragement on walking test performance. Thorax 1984;39:818‐22. [DOI] [PMC free article] [PubMed] [Google Scholar]
Guyatt 1985
- Guyatt GH, Thompson PJ, Berman LB, Sullivan MJ, Townsend M, Jones NL, et al. How should we measure function in patients with chronic heart and lung disease?. Journal of Chronic Diseases 1985;38:517‐24. [DOI] [PubMed] [Google Scholar]
Guyatt 1987a
- Guyatt GH, Berman LB, Townsend M, Pugsley SO, Chambers LW. A measure of quality of life for clinical trials in chronic lung disease. Thorax 1987;42:773‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Harper 1997
- Harper R, Brazier JE, Waterhouse JC, Walters SJ, Jones NM, Howard P. Comparison of outcome measures for patients with chronic obstructive pulmonary disease (COPD) in an outpatient setting. Thorax 1997;52:879‐87. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. www.cochrane‐handbook.org.
Holland 2014
- Holland AE, Spruit MA, Troosters T, Puhan MA, Pepin V, et al. An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease. European Respiratory Journal 2014;44:1428–46. [DOI] [PubMed] [Google Scholar]
Jaeschke 1989
- Jaeschke R, Singer J, Guyatt GH. Measurement of health status: ascertaining the minimal clinically important difference. Controlled Clinical Trials 1989;10:407‐15. [DOI] [PubMed] [Google Scholar]
Jones 1988
- Jones NL. Approaches to clinical exercise testing. Clinical Exercise Testing. Philadelphia: WB Saunders, 1988:123‐34. [Google Scholar]
Jones 1991
- Jones PW, Quirk FH, Baveystock CM. The St George's Respiratory Questionnaire. Respiratory Medicine 1991;85(Suppl B):25‐31. [DOI] [PubMed] [Google Scholar]
Jones 1992
- Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self‐complete measure of health status for chronic airflow limitation. The St. George's Respiratory Questionnaire. American Review of Respiratory Disease 1992;145:1321‐7. [DOI] [PubMed] [Google Scholar]
Jones 2003
- Jones PW, Kaplan RM. Methodological issues in evaluating measures of health as outcomes for COPD. European Respiratory Journal 2003;21(Suppl 41):13s–18s. [PubMed] [Google Scholar]
Kew 2014
- Kew KM, Seniukovich A. Inhaled steroids and risk of pneumonia for chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews 2014, Issue 3. [DOI: 10.1002/14651858.CD010115.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kirshner 1985
- Kirshner B, Guyatt G. A methodological framework for assessing health indices. Journal of Chronic Diseases 1985;38:27‐36. [DOI] [PubMed] [Google Scholar]
Kramer 1981
- Kramer MS, Feinstein AR. Clinical biostatistics. LIV. The biostatistics of concordance. Clinical Pharmacology and Therapeutics 1981;29:111‐23. [DOI] [PubMed] [Google Scholar]
Lacasse 1997
- Lacasse YL, Wong E, Guyatt GH, Goldstein RS. Health‐status measure instruments in chronic obstructive pulmonary disease. Canadian Respiratory Journal 1997;4:152‐64. [Google Scholar]
Lotters 2002
- Lotters F, Tol B, Kwakkel G, Gosselink R. Effects of controlled inspiratory muscle training in patients with COPD: a meta‐analysis. European Respiratory Journal 2002;20:570‐6. [DOI] [PubMed] [Google Scholar]
Mahler 1984
- Mahler DA, Weinberg DH, Wells CK, Feinstein AR. The measurement of dyspnea. Contents, interobserver agreement, and physiologic correlates of two new clinical indexes. Chest 1984;85:751‐8. [DOI] [PubMed] [Google Scholar]
Maltais 1996
- Maltais F, LeBlanc P, Simard C, Jobin J, Berube C, Bruneau J, et al. Skeletal muscle adaptation to endurance training in patients with chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine 1996;154:442‐7. [DOI] [PubMed] [Google Scholar]
Maltais 2008
- Maltais F, Bourbeau J, Shapiro S, Lacasse Y, Perrault H, Baltzan M, et al. Effects of home‐based pulmonary rehabilitation in patients with chronic obstructive pulmonary disease: a randomized trial. Annals of Internal Medicine 2008;149(12):869‐78. [DOI] [PubMed] [Google Scholar]
NICE 2010
- National Clinical Guideline Centre. Chronic obstructive pulmonary disease: management of chronic obstructive pulmonary disease in adults in primary and secondary care. London: National Clinical Guideline Centre,. London: National Clinical Guideline Centre, 2010.
Nici 2006
- Nici L, Donner C, Wouters E, Zuwallack R, Ambrosino N, Bourbeau J. American Thoraic Society/European Respiratory Society statement on pulmonary rehabilitation. American Journal of Respiratory and Critical Care Medicine 2006;173:1390–413. [DOI] [PubMed] [Google Scholar]
Nishimura 2013
- Nishimura K, Mitsuma S, Kobayashi A, Yanagida M, Nakayasu K, Hasegawa Y, et al. COPD and disease‐specific health status in a working population. Respiratory Research 1013;14:61. [DOI] [PMC free article] [PubMed] [Google Scholar]
O' Donnell 2007
- O'Donnell DE, Aaron S, Bourbeau J, Hernandez P, Marciniuk DD, Balter M, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease ‐ 2007 update. Canadian Respiratory Journal 2007;14(Suppl B):5B‐32B. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pauwels 2001
- Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. American Journal of Respiratory and Critical Care Medicine 2001;163(5):1256‐76. [DOI] [PubMed] [Google Scholar]
Puhan 2011(a)
- Puhan MA, Gimeno‐Santos E, Scharplatz M, Troosters T, Walters EH, Steurer J. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews 2011, Issue 10. [DOI: 10.1002/14651858.CD005305.pub3] [DOI] [PubMed] [Google Scholar]
Puhan 2011(b)
- Puhan MA, Chandra D, Mosenifar z Reis A, Make B, Hansel NN, Wise RA, et al. The minimal important difference of exercise tests in severe COPD. European Respiratory Journal 2011;37(4):784‐90. [DOI] [PMC free article] [PubMed] [Google Scholar]
Quirk 1991
- Quirk FH, Baveystock CM, Wilson RC, Jones PW. Influence of demographic and disease related factors on the degree of distress associated with symptoms and restrictions on daily living due to asthma in six countries. European Respiratory Journal 1991;4:167‐71. [PubMed] [Google Scholar]
Ram 2005
- Ram FSF, Jardinb JR, Atallahc A, Castrod AA, Mazzinie R, Goldsteinf R, et al. Efficacy of theophylline in people with stable chronic obstructive pulmonary disease: a systematic review and meta‐analysis. Respiratory Medicine 2005;99:135‐44. [DOI] [PubMed] [Google Scholar]
Redelmeier 1997
- Redelmeier DA, Bayoumi AM, Goldstein RS, Guyatt GH. Interpreting small differences in functional status: the Six Minute Walk test in chronic lung disease patients. American Journal of Respiratory and Critical Care Medicine 1997;155:1278‐82. [DOI] [PubMed] [Google Scholar]
RevMan 2011 [Computer program]
- Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011. Review Manager (RevMan). Version 5.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011, 2011.
Ries 2003
- Ries AL, Kaplan RM, Myers R, Prewitt LM. Maintenance after pulmonary rehabilitation in chronic lung disease: a randomized trial. American Journal of Respiratory and Critical Care Medicine 2003;167(6):880‐8. [DOI] [PubMed] [Google Scholar]
Ries 2007
- Ries AL, Bauldoff GS, Carlin BW, Casaburi R, Emery CF, Mahler DA, et al. Pulmonary rehabilitation: joint ACCP/AACVPR evidence‐based clinical practice guidelines. Chest 2007;131(5 Suppl):4s‐42s. [DOI] [PubMed] [Google Scholar]
Rochester 2014
- Rochester CL, Spanevello A. Heterogeneity of pulmonary rehabilitation: like apples and oranges ‐ both healthy fruit. European Respiratory Journal 2014;43(5):1223‐6. [DOI] [PubMed] [Google Scholar]
Rutten‐van Mölken 1999
- Rutten‐van Mölken M, Roos B, Noord JA. An empirical comparison of the St‐George's Respiratory Questionnaire (SGRQ) and the Chronic Respiratory Disease Questionnaire (CRQ) in a clinical setting. Thorax 1999;54:995‐1003. [DOI] [PMC free article] [PubMed] [Google Scholar]
Schulz 1995
- Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias ‐ Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995;273:408‐12. [DOI] [PubMed] [Google Scholar]
Shadish 1994
- Shadish WR, Haddock CK. Combining estimates of effect size. In: Cooper H, Hedges LV editor(s). The Handbook of Research Synthesis. New York: Russel Sage Foundation, 1994:261‐81. [Google Scholar]
Shu 1998
- Shu MF, Kao CH, Kuo HP. Upper arm exercise improves exercise tolerance and dyspnea sensation in patients with chronic obstructive airway disease (COAD). European Respiratory Journal 1998;12(Suppl 28):406S. [Google Scholar]
Singh 2008
- Singh S J, Jones PW, Evans R, Morgan MDL. The minimum clinically important improvement for the incremental shuttle walking test. Thorax 2008;63(9):775‐7. [DOI] [PubMed] [Google Scholar]
Singh 2014
- Singh SJ, Puhan MA, Adrianopoulos V, Hernandes NA, Mitchell KE, Hill CJ, Lee AL, et al. An official systematic review of the European Respiratory Society/American Thoracic Society: measurement properties of field walking tests in chronic respiratory disease. European Respiratory Journal 2014;44:1447‐78. [DOI] [PubMed] [Google Scholar]
Spruit 2013
- Spruit MA, Singh SJ, Garvey C, ZuWallack R, Nici L, Rochester C. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. American Journal of Respiratory and Critical Care Medicine 2013;188(8):e13‐e64. [DOI] [PubMed] [Google Scholar]
Spruit 2014
- Spruit MA, Pitta F, Garvey C, ZuWallack RL, Roberts CM, Collins, EG, et al. Differences in content and organisational aspects of pulmonary rehabilitation programmes. European Respiratory Journal 2014;43(5):1326‐37. [DOI] [PubMed] [Google Scholar]
Stanton 1995
- Stanton M, Beauchamp C, Weinberger M. A randomized controlled trial of pulmonary rehabilitation in chronic obstructive airways disease. Journal of General Internal Medicine 1995;10(Suppl):50. [Google Scholar]
Steiner 2003
- Steiner MC, Barton RS, Singh SJ, Morgan MDL. Nutritional enhancement of exercise performance in chronic obstructive pulmonary disease: a randomised controlled trial. Thorax 2003;58(9):745‐51. [DOI] [PMC free article] [PubMed] [Google Scholar]
Taylor 2005
- Taylor SJ, Candy B, Bryar RM, Ramsay J, Vrijhoef HJ, Esmond G, et al. Effectiveness of innovations in nurse led chronic disease management for patients with chronic obstructive pulmonary disease: systematic review of evidence. BMJ 2005;331:485‐91. [DOI] [PMC free article] [PubMed] [Google Scholar]
Tregonning 2000
- Tregonning M, Roberts S, Langley C, Dawe C, Rossdale C, Harvey JE, et al. Randomised controlled trial of home exercise and education in chronic obstructive pulmonary disease (COPD). Thorax 2000;55(Suppl 3):A7. [Google Scholar]
Troosters 2000
- Troosters T, Gosselink R, Decramer M. Short‐and long‐term effects of outpatient rehabilitation in patients with chronic obstructive pulmonary disease: a randomized trial. American Journal of Medicine 2000;109(3):207‐12. [DOI] [PubMed] [Google Scholar]
Viera 2010
- Vieira DS, Maltais F, Bourbeau J. Home‐based pulmonary rehabilitation in chronic obstructive pulmonary disease patients. Current Opinion in Pulmonary Medicine 2010;16(2):134‐43. [DOI] [PubMed] [Google Scholar]
Ward 1999
- Ward H, Dunsmore J, Thomas K, Sourdin S, Norton K, Wilson C, et al. A randomised controlled trial of pulmonary rehabilitation in moderate to severe chronic airflow limitation (CAL). Respirology 1999;4:A4. [Google Scholar]
Waschki 2011
- Waschki B, Kirsten A, Holz O, Müller KC, Meyer T, Watz H, et al. Physical activity is the strongest predictor of all‐cause mortality in patients with COPD: a prospective cohort study. Chest 2011;140:331‐42. [DOI] [PubMed] [Google Scholar]
Watson 1997
- Watson PB, Town GI, Holbrook N, Dwan C, Toop LJ, Drennan CJ. Evaluation of a self‐management plan for chronic obstructive pulmonary disease. European Respiratory Journal 1997;10:1267‐71. [DOI] [PubMed] [Google Scholar]
Whiteford 2004
- Whiteford S. Evaluation of the effect of a home‐based, cognitive‐behavioural pulmonary rehabilitation programme on physiological and psychosocial outcomes in COPD patients [N0394118760]. National Research Register 2004.
WHO 2008
- World Health Organization. World Health Stastistics. 2008; Vol. http://www.who.int/gho/publications/world_health_statistics/EN_WHS08_Full.pdf?ua=1, issue accessed 17 November 2014.
Wijkstra 1994a
- Wijkstra PJ, Tenvergert EM, Mark TW, Postma DS, Altena R, Kraan J. Relation of lung function, maximal inspiratory pressure, dyspnoea, and quality of life with exercise capacity in patients with chronic obstructive pulmonary disease. Thorax 1994;49:468‐72. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wijkstra 1995
- Wijkstra PJ, Vergert EM, Altena R, Otten V, Kraan J, Postma DS. Long term benefits of rehabilitation at home quality of life and exercise tolerance in patients with chronic obstructive pulmonary disease. Thorax 1995;50:824‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wright 2002
- Wright PR, Heck H, Langenkamp H, Franz KH, Weber U. Effect of a resistance training on pulmonary function and performance measures in patients with COPD [Einfluß eines Krafttrainings auf Lungenfunktionsparameter und Größen der Leistungfähigkeit von COPD Patienten]. Pneumologie 2002;56:413‐7. [DOI] [PubMed] [Google Scholar]
Yohannes 2004
- Yohannes AM, Connolly MJ. Pulmonary rehabilitation programmes in the UK: a national representative survey. Clinical Rehabilitation 2004;18:444‐9. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Lacasse 1996
- Lacasse Y, Wong E, Guyatt GH, King D, Cook DJ, Goldstein RS. Meta‐analysis of respiratory rehabilitation in chronic obstructive pulmonary disease. The Lancet 1996;348:1115‐9. [DOI] [PubMed] [Google Scholar]
Lacasse 2001
- Lacasse Y, Brosseau L, Milne S, Martin S, Wong E, Guyatt GH, et al. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews 2001, Issue 4. [DOI: 10.1002/14651858.CD003793] [DOI] [PubMed] [Google Scholar]
Lacasse 2006
- Lacasse Y, Goldstein RS, Lasserson TJ, Sylvie M. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews 2006, Issue 3. [DOI: 10.1002/14651858.CD003793.pub2] [DOI] [PubMed] [Google Scholar]