

Abstract
Objectives
The purpose of this study was to assess the effects of habitual chewing of khat (Catha edulis) on blood pressure, body mass index, and physiological aspects of sexuality among residents of an Ethiopian town.
Methods
A statistically determined and randomly selected sample of khat-chewing individuals in the town of Hosanna in Southern Ethiopia were included in the study. We used physical measurements and a self-administered questionnaire to collect the data, which was statistically analyzed.
Results
The participants comprised a total of 420 with mean age = 28.7±5.7 years; 336 (80.0%) were male. Nearly half (201; 47.9%) were in the age-group 30–34 years. The adverse effects of khat use were assessed from the median score of each outcome, namely, physical problems, abuse potential, and social effects. Having a score above the median on each of the three target outcomes was equated with the presence of adverse effects. Adverse effects were reported among 341 of 420 (81.2%) participants, of whom 277 of 341 (81.2%) were male and 64 of 341 (18.8%) were female. The reported adverse effects were significantly higher among those who co-used tobacco, coffee, or tea with khat, with adjusted odds ratio = 4.8; CI: 2.86–8.22.
Conclusions
Khat chewing was found to have a significant adverse effect on the health of individuals who indulged in it. This finding implies the need for urgent intervention from health authorities.
Keywords: Catha edulis, Khat, Mairungi, Miraa, Substance Abuse, Ethiopia
Introduction
Consumption of various plant-based psychotropic substances has been prevalent among humans since ancient times.1-4 Catha edulis is an evergreen shrub with mildly psychoactive properties, growing wild or cultivated in parts of Eastern Africa and the Arabian Peninsula. The plant is known by several regional names, such as khat (Ethiopia), qat (Yemen), qaad/jaad (Somalia), miraa (Kenya), mairungi (Uganda), muhulo (Tanzania), and hagigat (Hebrew).5,6 The tender leaves and young buds are chewed to attain states of mild euphoria and stimulation [Figure 1].6 Fresh leaves and stems are the favored parts of the plant. When chewed, it emits a characteristic odor and produces mild cocaine or amphetamine-like euphoria.6 The harvested leaves are usually packaged in plastic bags or wrapped in banana leaves to retain their moisture and freshness.
Figure 1.

Leaves of the khat plant (Catha edulis) and coconsumed substances (such as coffee and cigarettes) are seen arranged for consumption in a ‘khat-chewing room’ in the town of Hosanna, Southern Ethiopia.
Khat is estimated to be chewed daily by over 10 million people in the Arabian Peninsula and East Africa.7 The habit is deeply rooted in the socio-cultural traditions of these regions and is particularly widespread in Kenya, Yemen, Djibouti, and Ethiopia.7-9 In Ethiopia, 32.5–42.0% of the adult population are reported to consume khat daily.10 Khat-chewing habit is reportedly spreading overseas also, especially in the USA, Europe, and Australia.11
Among the numerous chemicals found in the leaves of Catha edulis are alkaloids, glycosides, tannins, and amino acids such as tryptophan, glutamic acid, alanine, glycine, and threonine. The leaves also contain vitamins such as ascorbic acid, thiamine, riboflavin, niacin, and carotene; minerals including calcium, iron, manganese, zinc, copper, and toxic metals lead, and cadmium.6,12 Cathinone, with mild amphetamine-like properties, is the plant’s principal psychoactive ingredient.6,12
Concerning the adverse effects of khat-chewing, contradicting opinions are documented. Wold Health Organization (WHO) has positionedkhat as the least harmful substance in a group of psychoactive substances evaluated by a panel of experts with low abuse potential.13 At the same time, several potentially harmful effects of khat—physical, physiological, public health, and social—have been documented.5,8-10
Traditionally, khat leaves have been used to treat depression and for social and academic purposes. The adverse consequences of khat-chewing range from mild emotional instability and irritability to more severe ones such as impaired cognitive functioning, chronic gastritis, constipation, anorexia, weight loss, cirrhosis, urinary retention, impotence, tachycardia, arrhythmia, hypertension, vasoconstriction, and myocardial infarction.9,14-16 It is also claimed to be associated with impotence in men and increased sexual desire in women.17 However, the reported adverse effects cover a vast spectrum of medical issues and may not be amenable to focused intervention [Figure 2]. Therefore, further research is called to verify and summarize the presumed adverse effects and settle the controversies. This study was therefore planned to identify the major adverse effects of khat-use and its associated factors.
Figure 2.
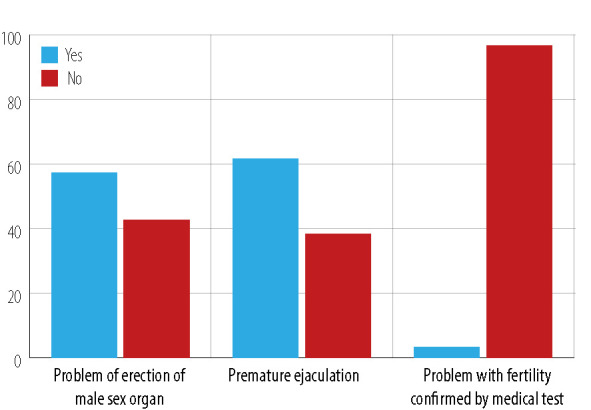
Harmful effects on male sexual behavior attributed to the khat-chewing.
Methods
We used a cross-sectional design to conduct this study, which was carried out among the townspeople in Hosanna, southern Ethiopia, many of whom habitually chew the leaves of Catha edulis.18 The sample size was estimated by taking the prevalence of adverse effects attributed to khat use at an estimated 50% (due to absence of published data), 95% CI, 5% margin of error, and 10% non-response rate. Consequently, the required sample size was estimated at 424. We used a single population proportion formula that would be used for calculating the adequate sample size in prevalence study.19,20
| n = (Z α2/2 p (1-p))/d2 |
Here, n is the sample size, Z is the statistic corresponding to the level of confidence, p is the expected proportion, and d is the precision (corresponding to the effect size).
| n = [(1.96)2 0.5 (1-0.5)]/ (0.05)2 = = 385 + (10% × 385) = 424 |
This study was conducted between June and September 2016 and approved by the institutional review committee of Hosanna College of Health Sciences (Ref No. HHSC 56/2016/013). Informed oral consent was obtained from all participants before data collection after explaining the objectives of the research.
During our initial screening visits, potential participants were contacted, informed, and asked for their consent to participate in the main study. Subjects who were willing to participate were assigned a code number (for use as a sampling frame) and asked when and where they could be contacted (mobile phone number and public khat chewing place) later for data collection. They were assured that their contact details would be used only for research purposes. We excluded pregnant women from the study due to the possible confounding effect of pregnancy on weight and blood pressure (BP). We used randomly generated numbers to select each sub-unit from the created sampling frame.
WHO mental health and substance abuse questionnaires were translated and modified for the local population and used for data collection. The composite questionnaire comprised three sections. The first section sought demographic data such as age, sex, marital status, level of education, occupation, and religion. The second section had questions on the participant’s khat-use practices. The third section consisted of questions that sought perceptions of participants regarding the adverse health effects attributed to khat-chewing. The fourth section comprised physical measurement data and the fifth section had questions to assess the abuse potential of khat. The English version of the questionnaire was translated into Amharic, the official language of the region, by a team of language experts. The Amharic language version of the questionnaire was used to collect data. The original English version of the questionnaire is attached as supporting information in Appendix.
The weight, height, and BP of all participants were taken after they completed the self-administered questionnaire. The WHO STEPS procedure was followed to measure BP.21 A mercury sphygmomanometer with best-fit cuff size was used to measure BP. Two consecutive measurements were taken after the subject had rested for at least 3–5 minutes before and after a khat-chewing session. Most participants would start chewing at noon and stop around 6 PM. The measurements were taken while the participant remained seated, from the right arm with the arm placed at the heart level. We used the difference in levels of BP recorded before and after a khat-chewing session to evaluate the influence of khat use on BP. We measured the height using a fixed-height measuring instrument with the participants standing upright with their heel, back, and buttocks in contact with the wall. Weight was measured using a calibrated weighing scale on which the participant stood barefoot and wearing light clothing.
We analyzed the consistency of the data collection tool using a reliability scale test, and the tool was found to be internally consistent (Cronbach’s Alpha = 0.83).22 Data was entered into Epi-Info version 3.5.2 and exported to STATA software (StataCorp. 2007. Stata Statistical Software: Release 10. College Station, TX: StataCorp LP.). A p-value of < 0.050 was considered statistically significant. We used frequencies and proportions to describe the data. Bivariate and multivariate analyses were conducted using logistic regression to examine the association between the adverse effects of khat use and selected sociodemographic and behavioral correlates. The multivariate logistic regression model was derived through simultaneous entry analysis. Odds ratio (OR) was used to estimate the strength of associations. Microsoft Excel 2007 was used to create tables and figures.
For the physical harm, we asked the participants to respond to questions designed to assess the physical harms of khat-use. Each item had ‘Yes’ or ‘No’ responses. ‘Yes’ scored 1 and ‘No’ scored 0. The physical harm score was dichotomized to physical harm present (score ≥ the median score) or not present (score < the median score). Participants who scored above the median score of items were taken as ‘exposed to physical harm from khat use’.
For abuse potential, we adopted the WHO definition of substance dependence, as a cluster of physiological, behavioral, and cognitive phenomena in which the use of a substance or a class of substances takes on a much higher priority for a given individual than another behavior that once had greater priority. We used four items to measure the abuse potential of khat use. Here too, each item had ‘Yes’ or ‘No’ responses with ‘Yes’ scoring 1 and ‘No’ scoring 0. We dichotomized and defined the final average score into two categories. Category 0: participants with ‘low abuse potential’ (scored < the cohort’s median score), and Category 1: those with ‘high abuse potential’ (score ≥ the median score).
For adverse effects of khat-use, we used physical influences, social influences, and abuse potential of khat. The final score of these three constructs was dichotomized into adverse effects of ‘khat use present’ (score ≥ the median score) and adverse effects of ‘khat use absent’ (score < the median score).
Results
Of the 424 filled questionnaires received, those from N = 420 participants were valid and were chosen for the study. The selected participants comprised 336 (80.0%) male and 84 (20.0%) female. Their mean age was 28.7±5.6 years, with an overall age range of 17–55 years. Nearly half (201 of 420; 47.9%) were in the age group 30–34 years; 201 (47.9%; CI: 43.1–52.9) participants had completed higher education. A quarter (110; 26.2%) spent most of their lives with their siblings (not parents), 25.2% (n = 106) spent most of their life with their mothers only, while 65 (15.5%) participants spent most of their life with both parents [Tables 1 and 2].
Table 1. Sociodemographic characteristics of the study participants.
| Variables | All cohort | Male | Female | |||
|---|---|---|---|---|---|---|
| Number | % of N = 420 | Number | % of n = 336 | Number | % of n = 84 | |
| Age group | ||||||
| 15–19 | 6 | 1.4 | 2 | 0.6 | 4 | 4.8 |
| 20–24 | 115 | 27.4 | 60 | 17.9 | 55 | 65.5 |
| 25–29 | 58 | 13.8 | 52 | 15.5 | 6 | 7.1 |
| 30–34 | 201 | 47.9 | 187 | 55.7 | 14 | 16.7 |
| 35–39 | 37 | 8.8 | 32 | 9.5 | 5 | 6.0 |
| 40–44 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| 45–49 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| 50–54 | 2 | 0.5 | 2 | 0.6 | 0 | 0.0 |
| 55–59 | 1 | 0.2 | 1 | 0.3 | 0 | 0.0 |
| Total | 420 | 100 | 336 | 100 | 84 | 100 |
| Marital status | ||||||
| Single | 63 | 15.0 | 48 | 14.3 | 15 | 17.9 |
| Married | 128 | 30.5 | 116 | 34.5 | 12 | 14.3 |
| Divorced | 139 | 33.1 | 100 | 29.8 | 39 | 46.4 |
| Widowed | 90 | 21.4 | 72 | 21.4 | 18 | 21.4 |
| Total | 420 | 100 | 336 | 100 | 84 | 100 |
Table 2. Characteristics related to the participants’ family history, occupation, and education.
| Variables | All cohort (N = 420) | Male (n = 336) | Female (n = 84) | |||
|---|---|---|---|---|---|---|
| Number | % | Number | % | Number | % | |
| Grew up with | ||||||
| Both parents | 65 | 15.5 | 58 | 17.3 | 7 | 8.3 |
| Only with mother | 106 | 25.2 | 86 | 25.6 | 20 | 23.8 |
| Only with father | 32 | 7.6 | 23 | 6.8 | 9 | 10.7 |
| Siblings | 52 | 12.4 | 47 | 14.0 | 5 | 6.0 |
| Sister only | 110 | 26.2 | 85 | 25.3 | 25 | 29.8 |
| Other | 55 | 13.1 | 37 | 11.0 | 18 | 21.4 |
| Occupation | ||||||
| No job | 127 | 30.2 | 117 | 34.8 | 10 | 11.9 |
| Government employee | 130 | 31.0 | 125 | 37.2 | 5 | 6.0 |
| Student | 37 | 8.8 | 22 | 6.5 | 15 | 17.9 |
| Daily laborer | 27 | 6.4 | 14 | 4.2 | 13 | 15.5 |
| Merchant | 56 | 13.3 | 42 | 12.5 | 14 | 16.7 |
| Commercial sex worker | 25 | 6.0 | 0 | 0.0 | 25 | 29.8 |
| Others | 18 | 4.3 | 16 | 4.8 | 2 | 2.4 |
| Education | ||||||
| Primary | 37 | 8.8 | 12 | 3.6 | 25 | 29.8 |
| Secondary | 182 | 43.3 | 142 | 42.3 | 40 | 47.6 |
| Higher education | 201 | 47.9 | 182 | 54.2 | 19 | 22.6 |
Nearly half (46.9%) of the participants (42.9% of male and 63.1% of female) had been chewing khat for 4–10 years (median = 9.2 years). The majority (70.2%) of male and (57.1%) of female chewed khat daily. Most participants (78.2%) were in the habit of chewing khat for three hours in a single session (median = 3.2±0.8 hours).
The participants gave various reasons for their khat habit including: ‘for relaxation purposes’ (n = 154; 36.7%) and ‘social purposes’ (n = 25; 6.0%). Most (64.8%) subjects knew of the harms associated with chewing khat. While 171 (40.7%) participants (42.0% of males, 35.7% of females) used public khat-chewing rooms (Mekamiya Bet in local language), 90 (21.4%) preferred hotels [Tables 3 and 4].
Table 3. History and patterns of khat use among male and female participants.
| Characteristics | Male | Female | Total | ||||
|---|---|---|---|---|---|---|---|
| Frequency | Percent | Frequency | Percent | Frequency | Percent | ||
| Duration of khat habit, year | |||||||
| < 1 | 35 | 10.4 | 5 | 6.0 | 40 | 9.5 | |
| 1–3 | 87 | 25.9 | 6 | 7.1 | 93 | 22.1 | |
| 4–10 | 144 | 42.9 | 53 | 63.1 | 197 | 46.9 | |
| > 10 | 70 | 20.8 | 20 | 23.8 | 90 | 21.5 | |
| Usual place for chewing khat | |||||||
| Public khat-chewing rooms | 141 | 42.0 | 30 | 35.7 | 171 | 40.7 | |
| Hotels | 65 | 19.3 | 25 | 29.8 | 90 | 21.4 | |
| Home | 58 | 17.3 | 11 | 13.1 | 69 | 16.5 | |
| Elsewhere | 72 | 21.4 | 18 | 21.4 | 90 | 21.4 | |
| Frequency of khat use | |||||||
| Daily | 236 | 70.2 | 48 | 57.2 | 284 | 67.7 | |
| Weekly | 76 | 22.6 | 30 | 35.7 | 106 | 25.2 | |
| Occasionally | 24 | 7.2 | 6 | 7.1 | 30 | 7.1 | |
| Consumption of other substances† while chewing | |||||||
| Yes | 265 | 78.9 | 0 | 0 | 265 | 63.1 | |
| No | 71 | 21.1 | 84 | 20.0 | 155 | 36.9 | |
†Tobacco, coffee, tea, etc.
Table 4. Participants’ reasons of using khat and their awareness of its harmful potential (N = 420).
| Characteristics | Male | Female | Total | |||
|---|---|---|---|---|---|---|
| Frequency | Percent | Frequency | Percent | Frequency | Percent | |
| Reason for khat use | ||||||
| To concentrate on studies (academic purposes) | 40 | 11.9 | 15 | 17.9 | 55 | 13.1 |
| For better work performance | 37 | 11.1 | 9 | 10.7 | 46 | 11.0 |
| For relaxation | 123 | 36.6 | 31 | 36.9 | 154 | 36.7 |
| For socializing with friends/family | 22 | 6.5 | 3 | 3.5 | 25 | 6.0 |
| Uncertain reason | 114 | 33.9 | 26 | 31.0 | 140 | 33.2 |
| Knows harm of khat use | ||||||
| Yes | 220 | 65.5 | 52 | 61.9 | 272 | 64.8 |
| No | 116 | 34.5 | 32 | 38.1 | 148 | 35.2 |
Most (265; 63.1%) participants reported that they used other substances while chewing khat. Only male participants (295 of 336; 87.9%) used tobacco products while chewing khat. Most men (269; 80.1%) also revealed consuming alcohol after chewing khat.
Overall, 81.4% of khat chewers reported experiencing adverse effects of its use. Nearly half of participants (187; 44.5%) reported social problems, 102 (24.3%) acknowledged dependency, and 53 (12.6%) reported physical harm related to khat use. Evaluation of the overall score suggests that with a score of ≥ 4 in 275 (65.5%) of the participants, khat has a high potential of abuse [Table 5].
Table 5. Adverse effects on behavioral and physical health attributed to khat use (N = 420).
| Characteristics | Participants, n | Percent, % |
|---|---|---|
| Whether the participant experienced adverse effects of khat use | ||
| Yes | 342 | 81.4 |
| No | 78 | 18.6 |
| Whether the participant committed any illegal activity† associated with khat use | ||
| Yes | 54 | 12.9 |
| No | 366 | 87.1 |
| Computed degree of khat abuse | ||
| Low abuse | 144 | 34.3 |
| High abuse | 275 | 65.5 |
| Major adverse effects associated with khat use | ||
| Physical | 53 | 12.6 |
| Social | 187 | 44.5 |
| Dependence | 102 | 24.3 |
| None | 78 | 18.6 |
† Committed at least one of the following: theft, disturbing peace, disorderly behavior, and interpersonal conflict.
The influence of khat habit on participants’ nutritional status was assessed through self-reported data and measurement of body mass index (BMI). Most subjects (300; 71.4%) reported the habit had a negative influence on their food intake. This was supported by the fact that 220 (52.4%) participants had BMIs below the WHO minimum of 16 kg/m2. The overall mean BMI was 16.0±2.0 kg/m2 (range = 12–28 kg/m2).
A typical khat-chewing session was associated with a significant increase in the chewer’s BP. The mean systolic BP before khat-chewing was 112.0 mm Hg which rose to 130.5 mm Hg at the end of the chewing session, representing a mean rise of 30.5±6.0 mm Hg (range = 20–50 mm Hg). Mean diastolic BP also rose from 74.4 to 95.8 mm Hg after chewing and increase of 20.5±6.8 mm Hg (range = 10–40 mmHg). Out of the 336 male participants, 193 (57.4%) reported erectile problems.
Selected sociodemographic characteristics and behavioral correlates were tested for association with adverse effects of khat use. Use of other substances (p < 0.001), duration (p = 0.040), and frequency (p = 0.020) of khat use were significantly associated with adverse effects. The misuse potential of khat also significantly varied across sex (p = 0.060), religion (p = 0.002), duration of khat habit (p = 0.001), cited reasons for khat use (p = 0.007), and place commonly used to chew khat (p = 0.007).
The adverse effects were significantly higher among individuals who used other substances (tobacco, coffee, tea) while chewing khat (AOR = 4.80; CI: 2.86–8.22) than those who used khat only with water. The likelihood of adverse effects was significantly higher in individuals who used khat daily (AOR = 2.50; CI: 1.10–5.73) than in occasional users. The odds of harmful influences of khat use were significantly lower in individuals who were chewing khat for < 1 year (AOR = 0.50; CI: 0.26–0.97) than in those who had the habit for more than 10 years [Table 6].
Table 6. Regression analysis findings of factors associated with adverse effects of khat use.
| Variables | Experiencing adverse effects | Adjusted OR (95% CI) | p-value | |
|---|---|---|---|---|
| Yes (%) | No (%) | |||
| Sex | ||||
| Male | 275 (81.8) | 61 (18.2) | 1.10 (0.62–2.05) | 0.060 |
| Female | 67 (79.8) | 17 (20.2) | 1.00 | |
| Use other substances* | ||||
| Yes | 286 (87.7) | 40 (12.3) | 4.80 (2.86–8.22) | < 0.001† |
| No | 56 (59.6) | 38 (40.4) | 1.00 | |
| Duration of khat use, year | ||||
| < 1 | 32 (80.0) | 8 (20.0) | 0.50 (0.26–0.97) | 0.040† |
| 1–3 | 70 (75.3) | 23 (24.7) | 0.94 (0.37–2.40) | |
| 4–10 | 171 (86.8) | 26 (13.2) | 1.18 (0.59–2.37) | |
| > 10 | 69 (76.7) | 21 (23.3) | 1.00 | |
| Frequency of khat use | ||||
| Daily | 237 (83.5) | 47 (16.5) | 2.50 (1.10–5.73) | 0.020† |
| Weekly | 85 (80.2) | 21 (19.8) | 1.20 (0.70–2.20) | |
| Occasionally | 20 (66.7) | 10 (33.3) | 1.00 | |
*tobacco, coffee, tea; †p < 0.050; 1: Reference; OR: odds ratio.
Discussion
This study examined the adverse effects of chewing khat among users in the town of Hosanna. The vast majority (81.4%) experienced adverse effects. Being the first study to compute the adverse effects of khat use using constructs in different dimensions, there is a dearth of comparative data.
Our results suggest significant adverse effects on habitual and long-term khat users. The habit was more prevalent among our male participants, a finding consistent with reports on different populations in eastern Kenya.23 The frequency distribution of marital status of our participants suggested a higher prevalence of khat use in those who were divorced and single, albeit lacking statistical significance. It is possible that khat use is associated with social, marital, and productivity issues. The majority of our subjects were well-educated and knew of the harms of the habit. However, the adverse effects experienced were not significantly affected by the user’s educational level or knowledge.
A substantial proportion of our participants were in the habit of consuming other substances (tobacco, coffee, tea) while chewing khat. This finding is supported by a similar study in another Ethiopian town, Jimma, which reported cigarette smoking and alcohol use to be significantly associated with khat chewing.24,25 Taking of other substances (cigarettes, shisha, coffee, tea) with khat was significantly associated with harmful influences of khat use in the current study. There is no published data on the influence of the concomitant use of other substances with khat. These substances seem to facilitate increased consumption of khat, which in turn might increase khat’s adverse effects. It is also possible that the co used substances by themselves contribute to the adverse effects.
This study also examined the influence of khat use on the nutritional status of participants. Participant responses and BMI data suggest that khat-use was negatively influencing their nutritional status, which is consistent with existing understanding.26 We also identified that during the course of a khat-chewing session, the BP of the individual was likely to rise significantly, which also is consistent with other Ethiopian studies.15
The current study also identified khat use had adverse effects on the sexual and reproductive health of male subjects. Erectile problems, premature ejaculation, and failure to make penetrative sexual intercourse were the identified sexual problems associated with khat use.27,28 The self-reported findings from this study showed that 2.6% of participants experienced infertility. Previous studies have also shown similar findings.29,30 According to previous research, high-dose khat consumption may decrease sperm quality.29,30 While such a distressing outcome requires attention, the mechanisms by which khat may affect the male reproductive physiology have not been fully elucidated and warrant further study.
This study also tried to examine the misuse potential of khat. Unlike a previous report which attributed to khat only mild to moderate psychological dependence,31 the current study has detected a high potential of abuse. The contradicting opinions on the abuse potential of khat-use warrant further study. Furthermore, this study identified social influence, dependency, and physical harm as the priority harmful influences of khat use. This is consistent with other studies from the Horn of Africa and the Arabian Peninsula.7 Similarly, we identified that habitual khat-chewing worsened stroke and mental illness, which again is supported by previous studies.6,17
The present study has limitations. One is related to the cross-sectional design of the study due to which the temporal relationships between predictor variables and the outcomes could not be established. Moreover, the sample was confined to a single population which limited the power of the study. In addition, since the data was taken from one group and collected at one point in time, the extent to which the problems could be attributed to khat use alone. We recommend an exhaustive longitudinal exploration of the factors associated with the adverse effects of khat chewing behavior among different segments of the Ethiopian population.
Conclusion
This study suggests that habitual khat-chewing has high abuse potential and causes adverse health effects, which contradicts some previous assumptions. The duration and frequency of khat-chewing and co use of other substances were the major predictors of the habit’s adverse effects. Khat-use negatively influences nutrition intake, sexual and reproductive health, and BP. We also recommend a re-evaluation of khat’s potential as a substance of abuse by global drug abuse policymakers including WHO.
Appendix
| Part 1: Background characteristics | |||||
|---|---|---|---|---|---|
| 1. Sex | Male o | ||||
| Female o | |||||
| 2. Age | ______(years old) | ||||
| 3. Educational status | No formal education o | ||||
| Primary o | |||||
| Secondary o | |||||
| Higher o | |||||
| 4. Marital status | Single o | ||||
| Married o | |||||
| Divorced o | |||||
| Widowed o | |||||
| 5. Religion | Orthodox o | ||||
| Protestant o | |||||
| Muslim o | |||||
| Other ____________ | |||||
| 6. Ethnicity | Hadiya o | ||||
| Gurage o | |||||
| Silte o | |||||
| Amhara o | |||||
| Other ______________ | |||||
| 7. Monthly income | _______ Ethiopian Birr (ETB) | ||||
| 8. Employment status | No job o | ||||
| Government o | |||||
| Student o | |||||
| Daily laborer o | |||||
| Merchant o | |||||
| Commercial sex worker o | |||||
| Others ______________ | |||||
| 9. Grew up with and spent most of life with | Both parents o | ||||
| Mother only o | |||||
| Father only o | |||||
| Siblings o | |||||
| Sisters only o | |||||
| Others________________ | |||||
| 10. Educational status of parents | No formal education o | ||||
| Primary education o | |||||
| Higher education o | |||||
| 11. Parents or family monthly income | ________________ ETB | ||||
| Part 2: Khat-use profile of participants | |||||
| 12. Parents use khat | Yes o | ||||
| No o | |||||
| 13. Who influenced you to start khat-use? | Family o | ||||
| Friends o | |||||
| Unknown reason o | |||||
| Others ______________ | |||||
| 14. How often do you use khat? | Daily o | ||||
| Weekly o | |||||
| Occasionally o | |||||
| 15. Duration of khat-use | < 1 year o | ||||
| 1-3 yeasrs o | |||||
| 4-10 years o | |||||
| > 10 years o | |||||
| 16. Reasons for Khat-use | Accademic | ||||
| To do other work | |||||
| For enjoyment | |||||
| For social purpose | |||||
| Any combination ______ | |||||
| Other reason __________ | |||||
| 17. Do you know the harm of khat-use? | Yes o No o |
||||
| 18. Where do you usually use khat ? | Public khat-chewing rooms o |
||||
| Hotels o | |||||
| Home o | |||||
| Elsewhere o | |||||
| 19. Do you use other substances while chewing khat? | Yes o No o |
||||
| 20. Smoke cigarette when chewing khat | Yes o No o |
||||
| 21. Drink coffee when chewing khat | Yes o No o |
||||
| 22. Take alcohol after khat | Yes o No o |
||||
| Part 3: Harmful influences of khat-use | |||||
| 23. Cost for khat-use (daily) |
___________ ETB | ||||
| 24. Erectile problem of male sex organ after khat-use | Yes o No o |
||||
| Not applicable o | |||||
| 25. Problem of premature ejaculation | Yes o No o |
||||
| 26. Problem with birth | Yes o No o |
||||
| 27. Problem with pattern of feeding due to khat | Yes o No o |
||||
| 28. Performed illegal activity due to khat-use | Yes o No o |
||||
| 29. Plan to reduce or stop khat-use | Yes o No o |
||||
| Part 4: Physical measurements | |||||
| 30. Weight | __________Kg | ||||
| 31. Height | _________meters | ||||
| 32. Blood pressure (BP) | Diastolic BP | Before khat-use DBP 1:_________mmHg DBP 2:_________mmHg After khat-use DBP 1: _________mmHg DBP 2: _________mmHg |
|||
| Systolic BP | Before khat-use SBP 1:_________mmHg SBP 2:_________mmHg After khat-use SBP 1: _________mmHg SBP 2: _________mmHg |
||||
| Part 5: Abuse potential of khat | |||||
| 33. Ever felt you should stop khat-use? | Yes o No o |
||||
| 34. Do people irritate you for your khat-use? | Yes o No o |
||||
| 35. Ever felt guilty about your khat-use? | Yes o No o |
||||
| 36. Unable to perform activities without khat | Yes o No o |
||||
| Please rate the priority harmful influences of khat-use for you. 3 - Severe or the 1st rank 2 - Moderate 2nd rank 1 - Mild 3rd rank | |||||
| Harmful influences of khat-use | 1 | 2 | 3 | ||
| 37. Physical harm to you (your organ damage, illness, tooth decay, gastritis…) | |||||
| 38. Social harm (harm to your family, conflicts, unemployment, social value …) | |||||
| 39. Dependence (unable to perform activities in absence of khat, unable to stop khat-use…) | |||||
Disclosure
The author declared no conflicts of interest. Hosanna College of Health Sciences funded the study. The funder had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Acknowledgments
The author would like to thank Hosanna College of Health Sciences Research and Community Service. I am also grateful to Hosanna residents, data collectors, and the town health office for their cooperation during the process of data collection.
References
- 1.Sarvet AL, Hasin D. The natural history of substance use disorders. Curr Opin Psychiatry 2016. Jul;29(4):250-257. 10.1097/YCO.0000000000000257 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nathan PE, Conrad M, Skinstad AH. History of the concept of addiction. Annu Rev Clin Psychol 2016;12(12):29-51. 10.1146/annurev-clinpsy-021815-093546 [DOI] [PubMed] [Google Scholar]
- 3.Crocq MA. Historical and cultural aspects of man’s relationship with addictive drugs. Dialogues Clin Neurosci 2007;9(4):355-361. 10.31887/DCNS.2007.9.4/macrocq [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Saah T. The evolutionary origins and significance of drug addiction. Harm Reduct J 2005. Jun;2:8. 10.1186/1477-7517-2-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Abebe M, Kindie S, Adane K. Adverse health effects of khat: a review. Fam Med Med Sci Res 2015;4(1):1-5. [Google Scholar]
- 6.Wabe NT. Chemistry, pharmacology, and toxicology of khat (catha edulis forsk): a review. Addict Health 2011;3(3-4):137-149. [PMC free article] [PubMed] [Google Scholar]
- 7.Al-Juhaishi T, Al-Kindi S, Gehani A. Khat: A widely used drug of abuse in the Horn of Africa and the Arabian Peninsula: Review of literature. Qatar Med J 2013. Nov;2012(2):1-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Teklie H, Gonfa G, Getachew T, Defar A, Bekele A, Bekele A, et al. Prevalence of khat chewing and associated factors in Ethiopia: findings from the 2015 national non-communicable diseases STEPS survey. Ethiop J Health Dev 2017;31(1):320-330. [Google Scholar]
- 9.Ongeri L, Kirui F, Muniu E, Manduku V, Kirumbi L, Atwoli L, et al. Khat use and psychotic symptoms in a rural Khat growing population in Kenya: a household survey. BMC Psychiatry 2019. May;19(1):137. 10.1186/s12888-019-2118-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Teni FS, Surur AS, Hailemariam A, Aye A, Mitiku G, Gurmu AE, et al. Prevalence, reasons, and perceived effects of khat chewing among students of a college in Gondar town, Northwestern Ethiopia: a cross-sectional study. Ann Med Health Sci Res 2015;5(6):454-460. 10.4103/2141-9248.177992 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Thomas S, Williams T. Khat (Catha edulis): a systematic review of evidence and literature pertaining to its harms to UK users and society. Drug Sci Policy Law 2013;1:205032451349833 . 10.1177/2050324513498332 [DOI] [Google Scholar]
- 12.Getasetegn M. Chemical composition of Catha edulis (khat): a review. Phytochem Rev 2016;15(5):907-920 . 10.1007/s11101-015-9435-z [DOI] [Google Scholar]
- 13.Nutt D, King LA, Saulsbury W, Blakemore C. Development of a rational scale to assess the harm of drugs of potential misuse. Lancet 2007. Mar;369(9566):1047-1053. 10.1016/S0140-6736(07)60464-4 [DOI] [PubMed] [Google Scholar]
- 14.Al-Duais MA, Al-Awthan YS. Khat chewing and lipid profile in human and experimental animals. Biomed Res Int 2021;2021. [DOI] [PMC free article] [PubMed]
- 15.Geta TG, Woldeamanuel GG, Hailemariam BZ, Bedada DT. Association of chronic khat chewing with blood pressure and predictors of hypertension among adults in gurage zone, southern Ethiopia: a comparative study. Integr Blood Press Control 2019. Dec;12:33-42. 10.2147/IBPC.S234671 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Getahun W, Gedif T, Tesfaye F. Regular Khat (Catha edulis) chewing is associated with elevated diastolic blood pressure among adults in Butajira, Ethiopia: a comparative study. BMC Public Health 2010. Jul;10:390. 10.1186/1471-2458-10-390 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wedegaertner F, al-Warith H, Hillemacher T, te Wildt B, Schneider U, Bleich S, et al. Motives for khat use and abstinence in Yemen–a gender perspective. BMC Public Health 2010. Nov;10:735. 10.1186/1471-2458-10-735 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Balint EE, Falkay G, Balint GA. Khat - a controversial plant. Wien Klin Wochenschr 2009;121(19-20):604-614. 10.1007/s00508-009-1259-7 [DOI] [PubMed] [Google Scholar]
- 19.Pourhoseingholi MA, Vahedi M, Rahimzadeh M. Sample size calculation in medical studies. Gastroenterol Hepatol Bed Bench 2013;6(1):14-17. [PMC free article] [PubMed] [Google Scholar]
- 20.Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med 2013. Apr;35(2):121-126. 10.4103/0253-7176.116232 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ogedegbe G, Pickering T. Principles and techniques of blood pressure measurement. Cardiol Clin 2010. Nov;28(4):571-586. 10.1016/j.ccl.2010.07.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ 2011. Jun;2:53-55. 10.5116/ijme.4dfb.8dfd [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Aden A, Dimba E A O, Ndolo UM, Chindia ML. Socio-economic effects of khat chewing in north eastern Kenya. East Afr Med J 2006. Mar;83(3):69-73. [DOI] [PubMed] [Google Scholar]
- 24.Fiidow OA, Minhat HS, Zulkefli NA, Ahmad N. A systematic review on risk factors for khat chewing among adolescents in the African continent and Arabian Peninsula. PLoS One 2022. Feb;17(2):e0263372. 10.1371/journal.pone.0263372 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gebrehanna E, Berhane Y, Worku A. Prevalence and predictors of harmful khat use among university students in Ethiopia. Subst Abus Res Treat 2014;8:SART-14413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Legesse TG, Takle ZJ, Best MG. Effect of khat and associated factors on nutritional status among khat chewers at gulelle sub-city, addis. Int J Food Sci Nutr Eng 2017;7(1):11-18. [Google Scholar]
- 27.Abate A, Tareke M, Tirfie M, Semachew A, Amare D, Ayalew E. Chewing khat and risky sexual behavior among residents of Bahir Dar City administration, Northwest Ethiopia. Ann Gen Psychiatry 2018. Jun;17(1):26. 10.1186/s12991-018-0194-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Nassar OH, Aklan HM. Erectile dysfunction among Yemenis: does chewing khat play a role? Eurasian J Med 2014. Jun;46(2):69-73. 10.5152/eajm.2014.18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Mwenda JM, Arimi MM, Kyama MC, Langat DK. Effects of khat (Catha edulis) consumption on reproductive functions: a review. East Afr Med J 2003. Jun;80(6):318-323. [DOI] [PubMed] [Google Scholar]
- 30.Nyachieo A, Kiraithe MM, Spiessens C, Chai DC, Kiulia NM, D’Hooghe TM, et al. Short-term effects of high-dose khat on sperm parameters and reproductive hormonal levels in olive baboons (Papio anubis). Gynecol Obstet Invest 2013;75(2):109-114. 10.1159/000345308 [DOI] [PubMed] [Google Scholar]
- 31.El-Setouhy M, Alsanosy RM, Alsharqi A, Ismail AA. Khat dependency and psychophysical symptoms among chewers in Jazan Region, Kingdom of Saudi Arabia. Biomed Res Int 2016;2016. [DOI] [PMC free article] [PubMed]