

ABSTRACT
There is currently no validated tool to measure the quality of life (QOL) in the Mongolian language. This study aimed to validate the Mongolian version of the World Health Organization Quality of Life – Brief (WHOQOL-BREF) questionnaire for the general population of Mongolia. The subjects were 301 adults aged 18–65 years selected randomly by a computer from 30 centers in 8 districts of Ulaanbaatar, Mongolia, in 2020. Reliability was measured using Cronbach’s α and intraclass correlation coefficients. Convergent, discriminant, and construct validities were examined using exploratory and confirmatory factor analyses for a four-domain factor structure. Among the participants, 56.1% were women, 32.9% held a bachelor’s degree or higher, 48.8% were employed, and 61.8% were married. The overall Cronbach’s α coefficient of the WHOQOL-BREF questionnaire was 0.804. Correlations between the component scores of the WHOQOL-BREF ranged from 0.581–0.822. All items showed higher item-total correlations with their corresponding domains than with other domains, except the mobility item from the physical domain. Discriminative validity was evident in physical and psychological domains. Exploratory and confirmatory factor analyses revealed a four-factorial structure consisting of 24 items that provided an acceptable fit to the data (RMSEA=0.084; CFI=0.860). In conclusion, the Mongolian version of the WHOQOL-BREF demonstrated evidence of good reliability and validity for assessing QOL in the general population of Mongolia. These findings indicate that it allows the comparison of QOL of adults in Mongolia with those in other countries.
Key Words: quality of life, WHOQOL-BREF, validation study, population-based, Mongolia
INTRODUCTION
The burden of disease has been changing globally over the past few decades. The incidence of non-communicable chronic diseases has increased in the last 30 years, influencing economic and healthcare conditions in many countries.1 In Mongolia, the disease burden has shifted from communicable diseases to non-communicable diseases. According to reports from the Institute for Health Metrics and Evaluation at the University of Washington, the share of the global burdens for non-communicable diseases, including mental and neurological disorders, increased by 19.8% between 1990 and 2017, whereas that for communicable diseases including diarrhea and neonatal infectious diseases decreased by 34.2% during the corresponding period.2 To meet the shift in disease burden, Mongolia has to establish appropriate policies to improve the efficacy of healthcare services by monitoring the quality of life (QOL) nationwide. This rapid shift in disease burden may be more influential for younger people in developing countries including Mongolia, than for those in developed countries.3
To evaluate the effectiveness of preventive, diagnostic, and treatment measures, the usage of a QOL assessment instrument is generally recommended.4 An important requirement for this is the establishment of its validity and reliability in the target population. Several generic QOL assessment instruments that have been examined in terms of validity and reliability across different cultures, such as the Short-Form Health Survey (SF-36), EuroQOL (EQ-5D), and World Health Organization Quality of Life (WHOQOL-100). Among them, WHOQOL-100 was developed by WHO experts by the simultaneous consideration of the context of the cultural aspects in 15 international field centers. Its abbreviated version, WHOQOL-BREF, is a concise self-report questionnaire that assesses health-related QOL both in general and clinical populations. It consists of 24 Likert scale items that represent four latent domains: physical health, psychological health, social relationship, and environmental health. There are two additional exclusive questions from the measurement model, which estimate the subject’s satisfaction with their life and general health. WHOQOL-BREF has been translated into more than 100 languages including Mongolian over 20 years.5 Concerning the Mongolian version, the evaluation has not been well documented to date. The source of the translation is not indicated, and the WHO claims no responsibility for the translation’s content or accuracy. Furthermore, it contains several misleading interpretations of the content of the original English version. Therefore, there was an urgent need to translate the WHOQOL-BREF into Mongolian based on the guidelines of cross-cultural adaptation.
Of note, no studies have assessed the QOL of the general Mongolian population. In particular, the political transition from communism to democracy, rapid urbanization, air pollution, changes in lifestyle, the shift in disease burden, and economic turbulence over the past three decades should have largely impacted the QOL of Mongolian people. Including but not limited to these factors, the subjective perception of QOL among Mongolian people may deviate from international standards. However, before establishing the normative data of the Mongolian people, it is mandatory to determine the psychometric properties of the Mongolian version of the WHOQOL-BREF to ensure its validity and reliability. In other countries, the instrument’s validity and reliability are satisfactory and appropriate for both general and clinical populations, although the poor reliability of a single domain has been reported in some countries.6,7
This study aimed to evaluate the psychometric properties of the Mongolian version of the WHOLQOL-BREF in a general population derived from a population-based cohort study in Mongolian. Confirmation of the validity of the WHOQOL-BREF in the general population could further promote the usage of QOL as an indicator in healthcare services and clinical research. With instrumental validation, it will be possible to establish the normative data for the Mongolian population for cross-cultural studies.
MATERIALS AND METHODS
Study population
This study was part of a nationwide multicenter, interdisciplinary, prospective, population-based cohort study that investigated brain-related disorders in the general population of Mongolia by the Brain Science Institute at the Mongolian National University of Medical Sciences. According to the latest United Nations data, Mongolia’s population was estimated as 3,358,000, of which 1,597,000 individuals lived in Ulaanbaatar, the capital city, and the remaining lived in 4 rural regions. The cohort was derived from 64 sampling centers, including 30 primary health centers of 8 districts in Ulaanbaatar and 34 primary health centers of 4 rural regions in Mongolia. Primary health centers provide healthcare services to all individuals within specific geopolitical units, where the entire population is registered by name, age, sex, education, employment, and household income.
In this cross-sectional study, the sampling size was calculated to be 385 using a confidence level (CI) of 95%, margin of error of 5%, design effect of 1.50, and population size of 1,024,000 individuals aged older than 18 years in Ulaanbaatar. To select a representative sample that matches age and sex distribution of the population of Ulaanbaatar, we created 6 age-sex groups as follows: 18–39 years (52.3%), 40–59 years (36.3%), ≥60 years (11.4%) for men (46.1%) and women (53.9%). Considering a response rate of 60%, 616 individuals were invited to participate in the survey. The participants were randomly sampled using a computer program (randbetween function of Excel). Depending on the population density, 3 or 4 individuals for each age-sex group from 30 sampling centers of the 8 districts of Ulaanbaatar out of 9 districts were selected. The uninvolved district, Bagakhangai, has a small population and is located geographically apart from other districts. Mongolian citizens who lived in the units for at least 6 months were considered to meet inclusion criteria. Among the invited individuals, 297 did not come up at the sampling center. A total of 319 participants were approached to complete the validity study, and 18 of those approached either refused to take the study or had missing data. The remaining 301 participants were included in the final analysis.
Written informed consent was obtained from all participants. The Institutional Review Board and Ethics Committee of the Mongolian National University of Medical Sciences (MNUMS) approved the study protocol and procedures for obtaining informed consent (number: 2020/03-05).
Data collection
The data collection started on September 7 and the preliminary dataset was extracted on October 25, 2020. The study was conducted in the official language (Mongolian). All participants completed paper questionnaires addressing their demographics and WHOQOL-BREF questionnaire. A total of 154 participants completed the WHOQOL-BREF questionnaire again within 2 weeks of the initial administration to assess test-retest reliability. All field study members completed a data collection training program prior to the study.
Measures
The WHOQOL-BREF, one of the most commonly used generic QOL questionnaires, was developed by the WHOQOL group in 1996.5 The WHOQOL-BREF is open-source and accessible for non-commercial use, and has been translated into more than 40 different languages. It is suitable for large sample surveys and clinical trials. It contains one item from each of the 24 facets from the WHOQOL-100, the original version of the questionnaire. Two more single items on the overall perception of the QOL and general health were added in this study. This questionnaire determines QOL with four domain scores: physical, psychological, social relationship and, environmental QOL. Each item is measured on a five-point Likert scale. The score of each domain consists of a mean score of items multiplied by four, in which a higher score indicates a better QOL of that aspect. It converts each domain score to a 0–100 scale.
We translated the WHOQOL-BREF into Mongolian based on the guidelines of cross-cultural adaptation via the following steps: initial translation of the items into Mongolian was performed independently by three translators (one holding a PhD degree in medicine, another holding a PhD degree in neuroscience), and the translation was combined into one version with focus on sentence structure, word choice, and best fit to the original version.8 A subsequent pilot test examined the understanding of items, the ability to answer, and the meaningfulness of the scale as a whole. Back-translation was performed independently by two translators unfamiliar with the original WHOQOL-BREF and revealed no meaningful disagreement with the original version. Finally, the expert committee re-evaluated item translation based on the pilot test and reviewed the back-translation process before administering the Mongolian version of WHOQOL-BREF to study participants.
Statistical analysis
The normality of the data was evaluated using the Kolmogorov-Smirnoff test. Differences in continuous or categorical variables were tested by the Mann-Whitney or Kruskal-Wallis test as appropriate. The reliability of the questionnaire was assessed for internal consistency using Cronbach’s α (good, ≥0.8; acceptable, ≥0.7; marginally acceptable, ≥0.6) and for external reliability using the intraclass correlation coefficient (ICC). A test-retest procedure was performed at a 2-week interval. ICC values of <0.5, <0.75, <0.9, and >0.9 were considered to have poor, moderate, good, and excellent test-retest reliability, respectively, according to Koo et al.9
Further, questionnaire validity was evaluated by exploratory factor analysis (EFA) using principal component analysis with equamax rotation and confirmatory factor analysis (CFA) to supplement EFA. Factor analysis suitability was examined by the Bartlett test of sphericity (p<0.001) and Kaiser-Meye-Olkin (KMO) test of sampling adequacy (p>0.65), followed by determining the number of relevant factors via eigenvalue analysis.10 The factors with eigenvalues >1 was assumed to be meaningful and retained for rotation. A threshold factor loading of 0.4 was chosen as a good indicator of sample-to-population pattern fit. The CFA was carried out for the Mongolian version of the WHOQOL-BREF using AMOS statistical software (Amos 26; SPSS Inc). The overall model fit was assessed using the chi-square test, and alternative fit indices with the following cut-offs for acceptable fit as follows: <0.08 for the root mean squared error of approximation (RMSEA), ≥0.8 for the comparative fit index (CFI), and ≥0.40 for the factor loading.11
A receiver operating characteristic (ROC) curve and area under curve (AUC) with a 95% CI were constructed to evaluate the diagnostic capacity of different cut-off points for the QOL in all domains to predict good QOL or poor QOL for each participant. We adopted the statistical analysis described in a previous study.12 Briefly, the single questions including perception of QOL and perception of general health, were used to establish good QOL/general health and poor QOL/general health. We used a cut-off point of 60 for the overall perception of QOL to create an ROC curve and the best cut-off point for each domain. Statistical significance was set at p<0.05, and all tests were two-tailed. Data are presented as means ± standard deviation with 95% CI. Data were analyzed using SPSS v26.0.
Ethics approval and consent to participate
All procedures performed in this study were done so in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments. The design and methods were reviewed and approved by the ethics committee at the Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia (number: MNUMS 20/03-05). This study was not a trial and did not require registration. Written informed consent was obtained from all participants.
RESULTS
Demographic characteristics
This study comprised 301 participants aged 18–65 years with a mean age and standard deviation of 40.1±15.5 years. Among them, 56.1% were women, 32.9% held a bachelor’s degree or higher, 48.8% were employed, and 61.8% were married. The mean age and sex were relatively close to the general population of Ulaanbaatar: 56.1% of the study subjects vs. 53.9% of the general population for women; 45.8% for 18–39 years, 41.2% for 40–59 years, and 13.0% for 60 years or older in the study subjects vs 52.3%, 36.3%, and 11.4% in the general population, respectively. As presented in Table 1, there were no significant differences in mean age, age group, marital status, education, and employment (p=0.629, 0.731, 0.413, 0.507, and 0.140, respectively).
Table 1.
Demographic characteristics of the study subjects (n=301)
| Characteristics | Total (%) | Male (%) | Female (%) | |
| Number | 301 (100) | 132 (100) | 169 (100) | |
| Age (years) | Mean±SD | 40.1±15.5 | 39.6±15.4 | 40.5±15.6 |
| Age-group | 18–39 | 138 (45.8) | 61 (46.2) | 77 (45.6) |
| 40–59 | 124 (41.2) | 56 (42.4) | 68 (40.2) | |
| ≥60 | 39 (13.0) | 15 (11.4) | 24 (14.2) | |
| Marital status | Married | 186 (61.8) | 83 (62.9) | 103 (60.9) |
| Never-married | 74 (24.6) | 37 (28.0) | 37 (21.9) | |
| Others* | 41 (13.6) | 12 (9.1) | 29 (17.2) | |
| Education | ≤ Middle school | 130 (43.2) | 63 (47.7) | 67 (39.6) |
| Associate’s degree | 72 (23.9) | 25 (18.9) | 47 (27.8) | |
| Bachelor’s degree | 85 (28.2) | 36 (27.3) | 49 (29.0) | |
| ≥ Master’s degree | 14 (4.7) | 8 (6.1) | 6 (3.6) | |
| Employment | Student | 43 (14.3) | 20 (15.2) | 23 (13.6) |
| Pensioner | 70 (23.3) | 26 (19.7) | 44 (26.0) | |
| Unemployed | 41 (13.6) | 12 (9.1) | 29 (17.2) | |
| Employed | 147 (48.8) | 74 (56.1) | 73 (43.2) | |
SD: standard deviation
*re-married, co-habiting, separated, divorced, and widowed.
Reliability
Item analyses included inspecting means, medians, standard deviations, item-to-total correlations, and Cronbach’s α to determine internal consistency (Table 2).
Table 2.
Cronbach’s α of the Mongolian version of WHOQOL-BREF (n=301)
| Components |
Mean ± standard
deviation |
Corrected item-total
correlation |
Cronbach’s α |
| Perception on quality of life | 3.9±0.8 | 0.626 | 0.920 |
| Perception on general health | 3.7±0.9 | 0.581 | 0.921 |
| Domain 1: Physical* | 60.9±17.1 | 0.666 | 0.871 |
| Domain 2: Psychological* | 73.1±16.1 | 0.810 | 0.816 |
| Domain 3: Social* | 69.9±17.7 | 0.662 | 0.874 |
| Domain 4: Environment* | 68.9±16.1 | 0.822 | 0.811 |
| WHOQOL-BREF (overall) | 0.804 |
*Score ranges from 0 to 100
The Cronbach’s α coefficients of the Mongolian version of the WHOQOL-BREF questionnaire were as follows: perception on quality of life, 0.920; perception on general health, 0.921; physical domain, 0.871; psychological domain, 0.816; social relationship domain, 0.874; and environmental domain, 0.811. The overall Cronbach’s α coefficient of the WHOQOL-BREF questionnaire was 0.804. The component scores were significantly correlated with the WHOQOL-BREF score, which was 0.581–0.822.
ICC was calculated using a two-factor mixed-effects model with a 95% CI to determine external reliability (Table 3).
Table 3.
Intraclass correlation coefficients (ICC) of the Mongolian version of WHOQOL-BREF (n=154)
| Domains | Mean ± standard deviation | ICC | |
| Test | Retest | ||
| Perception on quality of life | 3.8±0.8 | 3.9±0.7 | 0.602 |
| Perception on general health | 3.7±1.0 | 3.8±0.9 | 0.723 |
| Domain 1: Physical | 61.4±13.5 | 55.1±13.4 | 0.356 |
| Domain 2: Psychological | 63.5±17.2 | 66.3±14.9 | 0.669 |
| Domain 3: Social | 63.6±21.2 | 64.3±20.8 | 0.674 |
| Domain 4: Environment | 63.5±15.3 | 63.9±15.4 | 0.722 |
A total of 154 participants completed the WHOQOL-BREF questionnaire within 2 weeks of initial administration to assess test-retest reliability. Results from ICC analyses showed that the overall result of the domains was 0.602–0.723, which indicates moderate reliability, but the physical domain (0.356) showed poor reliability.
Validity
EFA using the equamax rotation and maximum likelihood extraction method for 24 items of data identified five components with eigenvalue greater than 1, as presented by the scree plot in Fig. 1.
Fig. 1.
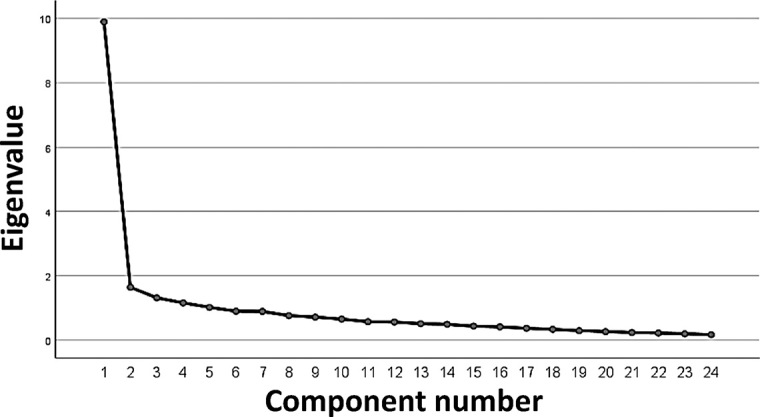
Scree plot for 24 items of the Mongolian version of WHOQOL-BREF (n=301)
Meanwhile, the results of EFA indicated a four-factor solution (Table 4). Items with factor loadings ≥0.40 on the dimensions were retained, as well as Question 15 “Mobility” (0.294) of factor 4 to keep the high Cronbach’s α. Together, these factors accounted for 41.2% of the total variance. KMO and Bartletts test results were 0.91 and p<0.001, respectively. The WHOQOL-BREF was invariant across sex, education level, and marital status. However, scalar invariance could not be established for age and employment in the physical health domain. RMSEA was 0.08, and CFI was 0.86 for the overall model fit.
Table 4.
Exploratory factor analysis of the Mongolian version of WHOQOL-BREF (n=301)
| Components | Factor loadings | |||
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | |
| Question 3: Pain | 0.074 | 0.099 | 0.047 | 0.874 |
| Question 4: Medication | 0.013 | 0.012 | 0.066 | 0.884 |
| Question 5: Positive | 0.575 | 0.394 | 0.280 | 0.173 |
| Question 6: Spiritual | 0.649 | 0.208 | 0.363 | 0.159 |
| Question 7: Think | 0.517 | 0.332 | 0.146 | 0.295 |
| Question 8: Safety | 0.484 | 0.439 | 0.302 | 0.190 |
| Question 9: Environment | 0.405 | 0.417 | 0.314 | 0.157 |
| Question 10: Energy | 0.327 | 0.603 | 0.268 | 0.359 |
| Question 11: Body | 0.580 | 0.199 | 0.297 | 0.231 |
| Question 12: Finance | 0.254 | 0.630 | 0.380 | 0.092 |
| Question 13: Information | 0.274 | 0.614 | 0.433 | 0.018 |
| Question 14: Leisure | 0.188 | 0.540 | 0.473 | 0.143 |
| Question 15: Mobility | –0.500 | 0.229 | 0.294 | –0.243 |
| Question 16: Sleep | 0.184 | 0.521 | 0.305 | 0.418 |
| Question 17: Activity | 0.421 | 0.458 | 0.456 | 0.254 |
| Question 18: Work | 0.458 | 0.319 | 0.422 | 0.212 |
| Question 19: Esteem | 0.555 | 0.174 | 0.518 | 0.225 |
| Question 20: Relationship | 0.663 | 0.199 | 0.390 | 0.152 |
| Question 21: Sex | 0.473 | 0.370 | –0.074 | 0.001 |
| Question 22: Support | 0.080 | 0.344 | 0.521 | –0.011 |
| Question 23: Home | 0.587 | 0.319 | 0.478 | 0.139 |
| Question 24: Service | 0.027 | 0.166 | 0.717 | 0.247 |
| Question 25: Transport | 0.210 | –0.089 | 0.669 | 0.164 |
| Question 26: Negative | 0.013 | 0.703 | –0.137 | 0.271 |
We applied a four-dimensional measurement model to evaluate how well the four domains were combined to identify the underlying latent construct of QOL. Figure 2 presents the factor correlations and loading of the Mongolian version of the WHOQOL-BREF.
Fig. 2.

Confirmatory factor analysis for the four domains of the Mongolian version of WHOQOL-BREF (n=301)
The arrows in Fig. 2 are the factor loadings, representing direct effects of the indicators on the latent QOL. The value ranged from 0.33–0.90 for the correlation coefficients between the domains and from 0.77–0.92 for the standardized regression weights. The squared multiple correlations were 0.59–0.85, whereas the measurement errors were represented from e1 to e24.
The ROC curve in Fig. 3 describes the sensitivity and specificity of the four domains in this study to predict QOL.
Fig. 3.
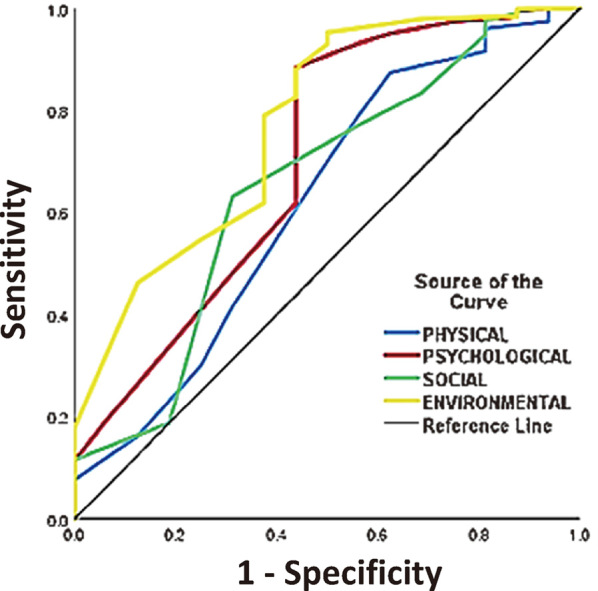
Receiver operating characteristic curves of the Mongolian version of WHOQOL-BREF according to domain (n=301)
AUC value for Domain 1 (physical) to Domain 4 (environmental) was 0.765 (95%CI, 0.590-0.940), 0.814 (95%CI, 0.642–0.986), 0.781 (95%CI, 0.598–0.964), and 0.785 (95%CI, 0.621–0.950), respectively. The cut-off points were 48, 60, 54, and 54, yielding a sensitivity of >80% (81.0%, 83.1%, 83.1%, and 82.8%) and a specificity >60% (81.8%, 81.8%, 72.7%, and 63.6%), respectively.
To determine convergent validity, we analyzed the correlation of each item with its corresponding domain (corrected item-total correlations) and inter-item correlations between the domains (Table 5).
Table 5.
Convergent validity of the Mongolian version of WHOQOL-BREF (n=301)
| Items / Domains | Domains, r | |||
| Physical | Psychological | Social | Environment | |
| Item convergence
(r ≥ 0.4) |
6/7 | 6/6 | 3/3 | 8/8 |
| Corrected item-total correlations | ||||
| Domain 1: Physical health | ||||
| Q3 Pain | 0.707*** | 0.362*** | 0.236*** | 0.282*** |
| Q4 Medication | 0.673*** | 0.327*** | 0.105 | 0.241*** |
| Q10 Energy | 0.742*** | 0.687*** | 0.472*** | 0.675*** |
| Q15 Mobility | 0.133* | –0.126* | –0.110 | –0.011 |
| Q16 Sleep | 0.761*** | 0.549*** | 0.480*** | 0.575*** |
| Q17 Activity | 0.723*** | 0.640*** | 0.619*** | 0.720*** |
| Q18 Work | 0.635*** | 0.617*** | 0.506*** | 0.617*** |
| Domain 2: Psychological health | ||||
| Q5 Positive | 0.549*** | 0.764*** | 0.480*** | 0.636*** |
| Q6 Spirit | 0.464*** | 0.755*** | 0.513*** | 0.640*** |
| Q7 Think | 0.487*** | 0.700*** | 0.403*** | 0.567*** |
| Q11 Body | 0.449*** | 0.766*** | 0.448*** | 0.557*** |
| Q19 Esteem | 0.545*** | 0.751*** | 0.633*** | 0.651*** |
| Q26 Negative | 0.348*** | 0.558*** | 0.300*** | 0.363*** |
| Domain 3: Social relationship | ||||
| Q20 Relationship | 0.491*** | 0.664*** | 0.724*** | 0.628*** |
| Q21 Sex | 0.251*** | 0.407*** | 0.699*** | 0.347*** |
| Q22 Support | 0.325*** | 0.360*** | 0.732*** | 0.490*** |
| Domain 4: Environmental health | ||||
| Q8 Safety | 0.532*** | 0.653*** | 0.468*** | 0.729*** |
| Q9 Environment | 0.455*** | 0.558*** | 0.457*** | 0.723*** |
| Q12 Finance | 0.503*** | 0.604*** | 0.511*** | 0.777*** |
| Q13 Information | 0.480*** | 0.610*** | 0.567*** | 0.767*** |
| Q14 Leisure | 0.532*** | 0.594*** | 0.459*** | 0.736*** |
| Q23 Home | 0.538*** | 0.711*** | 0.648*** | 0.771*** |
| Q24 Service | 0.429*** | 0.442*** | 0.369*** | 0.661*** |
| Q25 Transport | 0.309*** | 0.360*** | 0.329*** | 0.590*** |
| Inter-item correlations for domains | ||||
| Physical domain | 1 | |||
| Psychological domain | 0.659*** | 1 | ||
| Social domain | 0.479*** | 0.640*** | 1 | |
| Environment domain | 0.657*** | 0.787*** | 0.664*** | 1 |
*p<0.05
***p<0.001
p-values were calculated using Pearson’s correlations.
We expected each item to be more strongly correlated (r≥0.4) with its corresponding domain than with the other domains. In line with this, no items correlated more strongly with another domain than with its corresponding domain. However, the mobility item from the physical domain was the only item that showed a weak correlation with the corresponding domain (r<0.4). Therefore, 23 out of 24 items (95.8%) met the criterion for item convergence. These results support the existence of a four-domain structure.
An additional method (face validity) was adopted to provide further support for the instrument’s construct validity. According to the WHOQOL group, all domains should have strong and significant associations with the general facet items: perception on QOL, perception on general health, and the combined variable.6 Using a multiple linear regression for each general facet item, we analyzed their correlations (r) and associations (standardized β) with all four domains (Table 6).
Table 6.
Associations of domains with the general facet items (n=301)
| General facet | Domains, standardized Beta (r) | ||||
| Physical | Psychological | Social | Environment | R 2 | |
| Perception on quality of life | 0.101
(0.487) |
0.351***
(0.606) |
0.046
(0.452) |
0.202*
(0.575) |
0.398 |
| Perception on general health | 0.399***
(0.568) |
0.131
(0.497) |
0.066
(0.392) |
0.077
(0.487) |
0.355 |
| Both perceptions | 0.303***
(0.619) |
0.273***
(0.640) |
0.066
(0.491) |
0.158*
(0.616) |
0.492 |
*p<0.05
***p<0.001
p-values were analyzed using multiple linear regressions.
Perception on QOL and the combined variable were strongly associated with all four domains, which explained 39.8% and 49.2% of their variances, respectively. Perception of general health was predicted only by the physical and psychological domains.
To determine discriminant validity, we compared the domain scores between healthy and ill participants using an independent samples t-test (Table 7).
Table 7.
Discriminant validity of the Mongolian version of WHOQOL-BREF (n=286)
| Relation with illness | Domain scores (mean ± SD) | |||
| Physical | Psychological | Social | Environment | |
| Healthy participants (n=165) | 63.20±16.47 | 74.92±14.87 | 70.15±16.99 | 69.60±14.96 |
| Ill participants (n=121) | 56.08±16.26 | 69.93±16.53 | 69.21±17.77 | 66.27±16.47 |
| t-value | 3.632 | 2.671 | 0.452 | 1.243 |
| p-value | <0.001 | 0.008 | 0.652 | 0.215 |
p-values were analyzed with Student-t test.
The results revealed that discriminant validity was significant in the physical and psychological domains of the tested questionnaire. The ability of the other domains to discriminate between ill and healthy participants was insufficient.
DISCUSSION
The study suggested that the Mongolian version of the WHOQOL-BREF showed good validity and reliability for measuring QOL in Mongolian general populations. The results indicated that the Mongolian version of WHOQOL had good internal consistency and moderate test-retest reliability (external reliability), although a single domain was poor. Previous validation studies for general populations reported that Cronbach’s α were marginally acceptable for some domains. For example, the WHOQOL group reported good values for Cronbach’s α for the physical (0.82), psychological (0.81), and environmental domains (0.80), but a marginal value for the social relationship domain (0.68), based on results from 24 sampling centers across the world.6 Another validation study in Bangladesh reported relatively low values (0.57–0.69) for the social relationship and environmental domains.13 Similarly, the Cronbach’s α for the social relationship domain was only marginally acceptable in studies conducted in Iran and Japan.14,15 In contrast, in a China study, the physical domain (0.67) was marginal, whereas the psychological (0.76), social (0.72), and environmental domains (0.78), were acceptable.16 Compared with these studies’ results, our results showed a high level of reliability (≥0.8) in terms of internal consistency. However, the test-retest reliability of the physical domain was relatively weak, whereas that of the other domains were strong. The weak correlation in the test-retest was lower than the reliability results of the WHOQOL group, but similar to a previous report from the general population in Bangladesh.6,13 The correlation variation could be because of the mobility item that showed a very weak corrected item-total correlation with the physical domain in our study. Future studies should address this issue by carefully redesigning the items.
Convergent, discriminative, and construct validities were assessed. The results showed that all items had higher item-total correlations with their corresponding domains than with other domains, except for the mobility item from the physical domain. Discriminative validity was evident for the physical and psychological domains, whereas there was no discrimination capacity in the social and environmental domains. Healthy participants reported better QOL scores than ill participants in the physical and psychological domains, but not in the social and environmental domains. This finding is congruent with that of WHOQOL studies in Italy, Norway, Spain, and the UK.6 However, the status of participants, whether they were healthy or ill, as defined by self-report was not confirmed by health professionals using any diagnostic manual. All participants were considered to have non-patient status because of limited resources. Future studies should use a fully structured design and protocol to differentiate the sample populations based on physical and mental diseases.
Furthermore, CFA of the Mongolian version of the WHOQOL-BREF resulted in a four-factor structure, same as the original factorial structure of the instrument and supported the use of the instrument in diverse populations.6,17 The EFA suggested that a four-domain model was appropriate and potentially equivalent in terms of factor loadings and factor correlations among the study population, although a single question was not fit. The reason for the low component loadings on that question might be due to variations in culture and demographics. Our results displayed high loadings across several domains, indicating that QOL may be better represented by a single dimension. However, it suggested that one-dimensional factor structure had a rather acceptable fit to data in the clinical population than the general population.18 Moreover, using the cut-off criteria to estimate the prevalence of QOL, we found that the cut-of-points were set at relatively low levels compared to previous studies.16
The main limitations of this study were: (1) as the participants were recruited from only the capital city, the population surveyed did not represent the entire Mongolian population; (2) as a cross-sectional study, it did not provide information regarding the persistence of QOL over time; and (3) although convergent, discriminant, and construct validities were assessed, this study did not examine the incremental and criterion validity. Despite these limitations, this is the first study to evaluate the psychometric properties of the WHOQOL-BREF in the Mongolian language within the general population. To improve the validity of the instrument, future studies should compare the WHOQOL-BREF scores with other relevant measures. To further assess sensitivity and specificity of the instrument, the assessment needs to be conducted in both population-based and hospital-based settings using a longitudinal design.
Hence, this study validated the WHOQOL-BREF in Mongolia, and provided an assessment of the tool’s advantages and disadvantages for future work on QOL both in clinical and general populations. The current research supported the convergent, discriminant, and construct validities of the Mongolian version of the WHOQOL-BREF by providing evidence of acceptable internal consistency, external reliability, and four-factor structure. In conclusion, this study suggested that the Mongolian version of the WHOQOL-BREF is a valid and reliable instrument for determining QOL in the general population of Mongolia.
AUTHOR CONTRIBUTIONS
BL conceived and designed the study; EB, ET, GT, TJ, and BL performed and collected data; EB, GT, and BL analyzed the data; OJ and TJ contributed materials; EY, OT, NH, and BL reviewed and edited the paper; EB, NH, and BL wrote the paper.
AVAILABILITY OF DATA AND MATERIALS
The data are available in the Brain Science Institute at the Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia, and can be obtained upon request.
Data can be accessed by contacting:
Director, Brain Science Institute
+976-70161717
Zorig Street 3, Ulaanbaatar 14210, Mongolia
ACKNOWLEDGMENTS
We greatly appreciate those who participated in our study and 30 sampling center coordinators who supported collecting study data from Ulaanbaatar City.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
FUNDING
This study was supported by the International Brain Research Organization RHF-2014 to BL.
Abbreviations
- EFA
exploratory factor analysis
- QOL
quality of life
- WHO
World Health Organization
- WHOQOL-BREF
World Health Organization Quality of Life – Brief
REFERENCES
- 1.GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi: 10.1016/S0140-6736(20)30925-9. [DOI] [PMC free article] [PubMed]
- 2.Roser MR, Hannah. Burden of Disease 2016. https://ourworldindata.org/burden-of-disease. Published 2016. Accessed September 28, 2020.
- 3.Bollyky TJ, Templin T, Cohen M, Dieleman JL. Lower-income countries that face the most rapid shift in noncommunicable disease burden are also the least prepared. Health Aff(Millwood). 2017;36(11):1866–1875. doi: 10.1377/hlthaff.2017.0708. [DOI] [PMC free article] [PubMed]
- 4.Basch E. New frontiers in patient-reported outcomes: adverse event reporting, comparative effectiveness, and quality assessment. Annu Rev Med. 2014;65:307–317. doi: 10.1146/annurev-med-010713-141500. [DOI] [PubMed]
- 5.The Whoqol Group. The World Health Organization Quality of Life Assessment (WHOQOL): development and general psychometric properties. Soc Sci Med. 1998;46(12):1569–1585. doi: 10.1016/s0277-9536(98)00009-4. [DOI] [PubMed]
- 6.Skevington SM, Lotfy M, O’Connell KA, WHOQOL Group. The World Health Organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res. 2004;13(2):299–310. doi: 10.1023/B:QURE.0000018486.91360.00. [DOI] [PubMed]
- 7.Taylor WJ, Myers J, Simpson RT, McPherson KM, Weatherall M. Quality of life of people with rheumatoid arthritis as measured by the World Health Organization Quality of Life Instrument, short form (WHOQOL-BREF): score distributions and psychometric properties. Arthritis Rheum. 2004;51(3):350–357. doi: 10.1002/art.20398. [DOI] [PubMed]
- 8.Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine(Phila Pa 1976). 2000;25(24):3186–3191. doi: 10.1097/00007632-200012150-00014. [DOI] [PubMed]
- 9.Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi: 10.1016/j.jcm.2016.02.012. [DOI] [PMC free article] [PubMed]
- 10.Cattell RB. The scree test for the number of factors. Multivariate Behav Res. 1966;1(2):245–276. doi: 10.1207/s15327906mbr0102_10. [DOI] [PubMed]
- 11.Brown TA. Confirmatory factor analysis of the Penn State Worry Questionnaire: multiple factors or method effects? Behav Res Ther. 2003;41(12):1411–1426. doi: 10.1016/s0005-7967(03)00059-7. [DOI] [PubMed]
- 12.Silva PA, Soares SM, Santos JF, Silva LB. Cut-off point for WHOQOL-bref as a measure of quality of life of older adults[in English, Portuguese]. Rev Saude Publica. 2014;48(3):390–397. doi: 10.1590/s0034-8910.2014048004912. [DOI] [PMC free article] [PubMed]
- 13.Tsutsumi A, Izutsu T, Kato S, et al. Reliability and validity of the Bangla version of WHOQOL-BREF in an adult population in Dhaka, Bangladesh. Psychiatry Clin Neurosci. 2006;60(4):493–498. doi: 10.1111/j.1440-1819.2006.01537.x. [DOI] [PubMed]
- 14.Nedjat S, Montazeri A, Holakouie K, Mohammad K, Majdzadeh R. Psychometric properties of the Iranian interview-administered version of the World Health Organization’s Quality of Life Questionnaire (WHOQOL-BREF): a population-based study. BMC Health Serv Res. 2008;8:61. doi: 10.1186/1472-6963-8-61. [DOI] [PMC free article] [PubMed]
- 15.Yoshitake N, Sun Y, Sugawara M, et al. The psychometric properties of the WHOQOL-BREF in Japanese couples. Health Psychol Open. 2015;2(2):2055102915598089. doi: 10.1177/2055102915598089. [DOI] [PMC free article] [PubMed]
- 16.Xia P, Li N, Hau KT, Liu C, Lu Y. Quality of life of Chinese urban community residents: a psychometric study of the mainland Chinese version of the WHOQOL-BREF. BMC Med Res Methodol. 2012;12:37. doi: 10.1186/1471-2288-12-37. [DOI] [PMC free article] [PubMed]
- 17.Krägeloh CU, Kersten P, Rex Billington D, et al. Validation of the WHOQOL-BREF quality of life questionnaire for general use in New Zealand: confirmatory factor analysis and Rasch analysis. Qual Life Res. 2013;22(6):1451–1457. doi: 10.1007/s11136-012-0265-9. [DOI] [PubMed]
- 18.Kalfoss MH, Reidunsdatter RJ, Klöckner CA, Nilsen M. Validation of the WHOQOL-Bref: psychometric properties and normative data for the Norwegian general population. Health Qual Life Outcomes. 2021;19(1):13. doi: 10.1186/s12955-020-01656-x. [DOI] [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data are available in the Brain Science Institute at the Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia, and can be obtained upon request.
Data can be accessed by contacting:
Director, Brain Science Institute
+976-70161717
Zorig Street 3, Ulaanbaatar 14210, Mongolia