

African relevance
-
•
Chest injuries represent one of the most common diagnoses in severely injured patients. Chest imaging plays a prominent role in the assessment of patients with blunt trauma. A reliable, economic, bedside, and rapidly accomplished screening test can be pivotal.
-
•
We aimed to compare the accuracy of E-FAST to that of the NEXUS chest algorithm in detecting blunt chest injuries.
-
•
Our study concluded that E-FAST is highly specific for the detection of hemothorax, pneumothorax, and chest injuries compared with the NEXUS chest algorithm, which demonstrated the lowest specificity. However, the NEXUS chest algorithm showed a higher sensitivity than E-FAST and hence can be used effectively to rule out thoracic injury.
-
•
The African Journal of Emergency Medicine is the official journal of the African Federation for Emergency Medicine. It is an international, peer-reviewed journal aimed in particular at supporting emergency care across Africa I understand the objectives of the journal and have formatted the manuscript to fit the style and needs of the journal.
Keywords: Pneumothorax, Hemothorax, E-FAST, NEXUS, Blunt chest trauma
Abstract
Introduction
Chest imaging plays a prominent role in the assessment of patients with blunt trauma. Selection of the right approach at the right time is fundamental in the management of patients with blunt chest trauma.[1] A reliable, economic, bedside, and rapidly accomplished screening test can be pivotal. [2]
Objective
The aim of this study was to compare the accuracy of extended- focused assessment with sonography for trauma (E-FAST) to that of the National Emergency X-Radiography Utilisation Study (NEXUS) chest algorithm in detecting blunt chest injuries.
Methods
This descriptive cross-sectional study included 50 polytrauma patients with blunt chest trauma from the emergency centre of Suez Canal University Hospital. E-FAST and computed tomography (CT) were conducted, followed by reporting of NEXUS criteria for all patients. Blinding of the E-FAST performer and CT reporter were confirmed. The results of both the NEXUS algorithm and E-FAST were compared with CT chest results.
Results
The NEXUS algorithm had 100% sensitivity and 15.3% specificity, and E-FAST had 70% sensitivity and 96.7% specificity, in the detection of pneumothorax.
In the detection of hemothorax, the sensitivity and specificity of the NEXUS algorithm were 90% and 7.5%, respectively, whereas E-FAST had a lower sensitivity of 80% and a higher specificity of 97.5%.
Conclusion
E-FAST is highly specific for the detection of hemothorax, pneumothorax, and chest injuries compared with the NEXUS chest algorithm, which demonstrated the lowest specificity. However, the NEXUS chest algorithm showed a higher sensitivity than E-FAST and hence can be used effectively to rule out thoracic injury.
Introduction
Trauma is one of the leading causes of death worldwide.[3] It has been reported that each year more than 45 million people have significant disability due to trauma [1].
Major trauma contributes ominously to high morbidity, mortality and long-term disabilities globally [2]. In developing countries, injuries are generally increasing due to the increase in motorization, civil violence, urbanization, and criminal and war activities. Major trauma remains one of the primary causes of hospitalization in these countries [3].
Chest trauma is one of the major burdens in polytrauma patients. Chest injuries account for 25% of deaths in people aged <40 years [4]. The majority of chest injuries are caused by blunt trauma; however, penetrating trauma constitutes only around 10% of these injuries [5]. In the majority of cases, severe thoracic trauma is associated with concomitant injuries. Therefore, chest injuries represent one of the most common diagnoses in severely injured patients [6].
The golden hour for chest injury is still extremely significant during which precise management is generally required to preclude fatality.[6] Approximately 15%–30% of penetrating thoracic injuries and <10% of blunt thoracic injuries necessitate surgical intervention.[4] The majority of thoracic injuries can be treated via conservative management [7].
Chest imaging plays a prominent role in the assessment of patients with blunt trauma; however, the inability to select the right tool in the right patient and in the right time is expensive, may result in delaying of care, and unnecessarily exposes patients to possibly harmful radiation [8]. It has been reported that supine chest radiography had a sensitivity of only 20.9% in the diagnosis of pneumothorax when compared with computed tomography (CT), which is the current gold standard in this setting [7].
Thoracic ultrasound (US) has been established to be a capable tool and a bedside technique [5]. It has numerous advantages compared with traditional radiographic imaging of pleura, including the ability to perform dynamic imaging, absence of radiation, real-time imaging, and better portability [6]. In patients with major trauma, the initial US examination is generally performed using a FAST protocol that is capable of defining an intraperitoneal free fluid collection, which is an indirect sign of injury of a solid organ and necessitates crucial surgical exploration. After conducting the preliminary FAST examination, the US examination could be extended to the chest to exclude hemothorax and pneumothorax, and when extended to the thorax, this examination is recognized as E-FAST [7].
The usage of CT for the evaluation of adult patients with blunt trauma has significantly increased in the past two decades, and several trauma centers have accepted routine head-to-pelvis CT protocols (pan-scan) that rely on chest CT for victims of major trauma [9]. Nevertheless, several investigators have concluded that this intensification in CT use is concomitant with quantifiable and clear cancer risks [10]. Consequently, numerous organizations of major specialty have called for appraisal of the prevalent CT use in trauma, and in 2014, the American College of Surgeons enumerated the avoidance of routine whole body trauma CT as one of its five Choosing Judiciously recommendations [11].
The NEXUS chest algorithm has demonstrated high sensitivity for detecting thoracic injury on a multicenter, prospective cohort validation study at 9 US level I trauma centers from December 2009 to January 2012. In which they enrolled patients using the following inclusion criteria: [1] older than 14 years, [2] blunt trauma occurring within 24 hours of emergency centre (EC) presentation, and [3] receiving chest imaging (CXR or chest CT) in the EC as part of blunt trauma evaluation. It is generally performed in patients with blunt trauma aged >14 years. It includes the assessment of the patient, and when one or more of certain criteria are present, intrathoracic injury cannot be excluded and then a CT examination is necessary. When all criteria are absent in trauma patient, the risk of intrathoracic injury is very low and chest imaging is not indicated; these criteria include [1] age >60 years, [2] rapid deceleration mechanism, [3] chest pain, [4] intoxication, [5] abnormal alertness/mental status, [6] distracting painful injury, and [7] tenderness to chest wall palpation(12).
In an attempt to reduce the costs, radiation risks of unnecessary polytrauma trauma imaging, and transportation of unstable patients, we conducted the present study to improve the management process of polytrauma patients by evaluating the accuracy of the NEXUS chest algorithm compared with E-FAST in detecting blunt chest injuries in Suez Canal University Hospital.
Methods
Study design and setting
This research was a descriptive cross-sectional study. One day of the week was randomly selected. Of the polytrauma patients admitted to the emergency centre of Suez Canal University Hospital, 50 patients with blunt chest trauma who fulfilled our inclusion criteria were randomly selected using the Excel software and enrolled in the study. The selection was done at all hours of the day, and randomization was performed using table of random numbers.
Study objectives
Primary objectives: To compare between diagnostic accuracy of E-FAST and Nexus chest algorism in detection of blunt chest injury in polytrauma patients.
Secondary objectives: To determine the possibility of reducing the unnecessarily exposure of the patients to potentially harmful ionizing radiation especially in case of imaging contraindication (e.g. unstable patients).
Inclusion and exclusion criteria
Inclusion criteria were as follows: age >18 years, blunt trauma occurring within 24 hours of presentation, and patients undergoing chest CT examination as clinically indicated. The exclusion criteria were patients transferred from other hospitals, discharged on their demand or transferred to other hospitals, and undergoing any radiological investigation before presentation to the hospital.
Clinical evaluation
Clinical evaluations of the patients were conducted on arrival to the emergency centre, which included initial assessment of ABCDE (airway and cervical spine control, breathing, circulation, dysfunction of the central nervous system, GCS, and exposure). Then, a careful chest examination was performed to identify the type of chest injuries as follows:
-
•
Physicians recorded the presence of the NEXUS chest clinical criteria.
-
•
Then, all patients underwent a chest X-ray examination as a part of routine primary survey.
-
•
For saving time, E-FAST was performed immediately after routine FAST by a fixed staff radiologist.
-
•
E-FAST involved examination of third intercostal spaces to down at mid-clavicular lines and all intercostal spaces at parasternal lines and midaxillar lines for the detection of pneumothorax signs.
-
•
Presence of any one of the following findings was considered as positive for pneumothorax:
-
1.
Absence of pleural (lung) sliding.
-
2.
Absence of comet-tail artifacts, also referred to as B-lines.
-
3.
Absence of a lung pulse.
-
4.Presence of one or more lung points.
-
○This was followed by examination of the costophrenic angle on either side for the detection of hemothorax.
-
○The entire procedure took <60 s for each side and did not interfere with the resuscitation process.
-
○Then, all patients underwent a chest CT scan ordered by their physician as a part of the required investigation (which was considered as the gold standard).
-
○The ultrasound equipment used to examine the patients was Phillips HD11EXm. A linear probe with frequency ranging from 3.5 to 7.5 MHz was used. The CT equipment was ALEXION Toshiba Multidetector 16 slice.
-
○A radiologist reviewed the chest CT images and documented the findings of each patient.
-
○The E-FAST performer and CT reporter were blinded to the study. Immediately after the E-FAST and clinical evaluations, the results were placed in a closed envelope to ensure blinding from the CT scan results.
-
○Next, the results of both the NEXUS algorithm and E-FAST were compared with chest CT findings.
The sample size was calculated from the following equation:
Where:m = sample size; Zα and Zβ are normal deviates at the significance level of 0.05 and power of 90%
Zα = 1.96 and Zβ = 1.28
Φ is allocation ratio = 1
π1 is the proportion sensitivity of NEXUS-chest algorithm, which was 99.2% = 0.992 [13]
π2 is the proportion sensitivity of E-FAST, in the diagnosis of chest injuries, which was 77% = 0.77 [13]
π = (π1 + π2) /2 = 0.881
δ = π1 - π2 = 0.222
So, m = 42.5
In addition, expected drop out of 15% was added, so there were about 50 patients.Fig. 1.
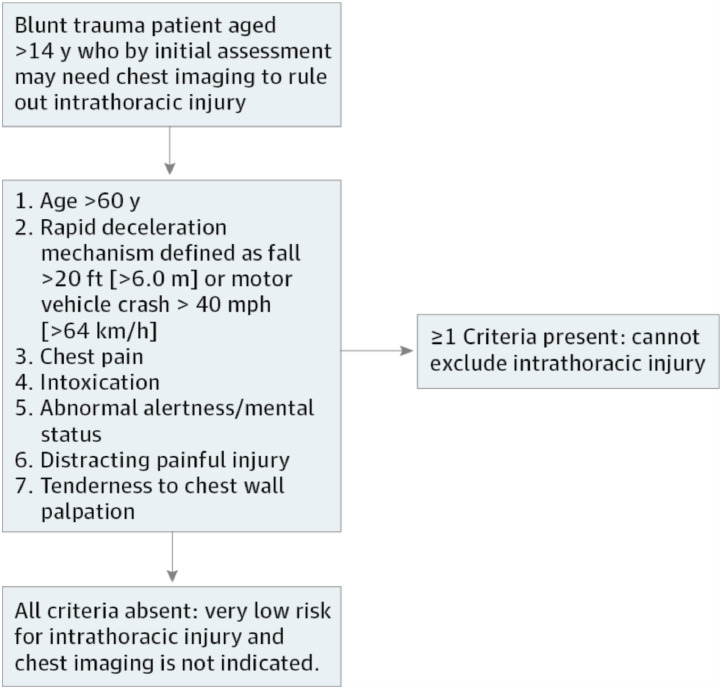 NEXUS Chest Decision Instrument Implementation [12]
NEXUS Chest Decision Instrument Implementation [12] -
○

Ethics approval
The institutional review board (IRB) of Suez Canal University and the University of Maryland, Baltimore, approved the protocol before study initiation.
Statistical methods
The collected data were coded, tabulated, and statistically analyzed using IBM SPSS statistics (Statistical Package for Social Sciences) software version 22.0, IBM Corp., Chicago, USA, 2013. Qualitative data described as number and percentage and their agreements tested using Kappa test. The level of significance was taken at P value < 0.050 was significant, otherwise was non-significant.
Diagnostic characteristics were calculated as follows:
-
-
Sensitivity = (True positive test / Total positive golden) x 100
-
-
Specificity = (True negative test / Total negative golden) x 100
-
-
Diagnostic accuracy =
([True positive test + True negative test] / Total cases) x 100
-
-
Youden's index = sensitivity + specificity – 1
-
-
Predictive positive value = (True positive test / Total positive test) x 100
-
-
Predictive negative value = (True negative test / Total negative test) x 100
-
-
LR+ = (sensitivity/ 1-specificity)
-
-
LR- = (1- sensitivity / specificity)
-
-
LR= LR+/ LR-
Kappa=Observed agreement–chance agreement / 1–chance agreement
Results
This descriptive cross-sectional study, which was conducted in Suez Canal University Hospital, included 50 polytrauma patients with blunt chest trauma, who presented within 24 h from the time of trauma to the emergency centre, from November 1, 2018, to May 1, 2019, and underwent chest CT examination as a part of clinical practice. The mean age of the study patients was 37.7 ± 14.6 years, with the majority of them (46%) being aged 30–39 years. Most of the patients were men (82%), and motor vehicle accidents were the major mechanism of injury (46%) (Table 1).
Table 2.
Diagnostic findings among the studied cases
| Variables | N | % | |
|---|---|---|---|
| NEXUS | Intoxication | 6 | 12.0 |
| Age >60 | 10 | 20.0 | |
| Altered mental status | 14 | 28.0 | |
| Deceleration | 16 | 32.0 | |
| Chest pain | 19 | 38.0 | |
| Chest tenderness | 19 | 38.0 | |
| Distraction injury | 18 | 36.0 | |
| Pneumothorax/Hemothorax | 46 | 92.0 | |
| X-Ray | Pneumothorax | 5 | 10.0 |
| Hemothorax | 8 | 16.0 | |
| Pneumothorax/Hemothorax | 13 | 26.0 | |
| E-FAST | Pneumothorax | 15 | 30.0 |
| Hemothorax | 9 | 18.0 | |
| Pneumothorax/Hemothorax | 24 | 48.0 | |
| CT | Pneumothorax | 20 | 40.0 |
| Hemothorax | 10 | 20.0 | |
| Pneumothorax/Hemothorax | 30 | 60.0 | |
Total = 50
Table 1.
Demographic and clinical characteristics among the studied cases
| Variables | N | % | |
|---|---|---|---|
| Demographic characteristics | |||
| Age categories | <30.0 | 10 | 20.0 |
| 30.0− | 23 | 46.0 | |
| 40.0− | 4 | 8.0 | |
| 50.0− | 3 | 6.0 | |
| ≥60.0 | 10 | 20.0 | |
| Sex | Male | 41 | 82.0 |
| Female | 9 | 18.0 | |
| Mechanism of trauma | MCV | 23 | 46.0 |
| Falls | 11 | 22.0 | |
| Pedestrian | 7 | 14.0 | |
| Accident | 9 | 18.0 | |
| Clinical characteristics | |||
| Heart rate ≥100 beat/minute | 16 | 32.0 | |
| Systolic blood pressure <90.0 mmHg | 3 | 6.0 | |
| Respiratory rate ≥24 cycle/minute | 7 | 14.0 | |
| Oxygen saturation ≤94 % | 6 | 12.0 | |
Total = 50
When applying on NEXUS criteria we found that chest pain and chest tenderness were the most common features (38%). In total, 30 patients (60%) had chest injuries detected by CT, E-FAST showed 24 (48%) positive results, and chest X-ray showed 13 (26%) positive results, whereas the NEXUS algorithm showed only 4 (8%) negative results (Table 2).
In diagnosing pneumothorax, only E-FAST had significant moderate agreement with CT (golden) findings. NEXUS had highest sensitivity and NPV but had also the lowest specificity and PPV. E-FAST had highest specificity, PPV, diagnostic accuracy and Youden's index (Table 3).
Table 3.
Diagnostic characteristics of NEXUS, X-Ray and E-FAST in diagnosing pneumothorax
| Characters | Value | 95% CI | Value | 95% CI | Value | 95% CI |
|---|---|---|---|---|---|---|
| NEXUS | X-RAY | E-FAST | ||||
| Sensitivity | 100.0% | 83.2%–100.0% | 15.0% | 3.2%–37.9% | 70.0% | 45.7%–88.1% |
| Specificity | 13.3% | 3.8%–30.7% | 93.3% | 77.9%–99.2% | 96.7% | 82.8%–99.9% |
| DA | 48.0% | 33.7%–62.6% | 62.0% | 47.2%–75.3% | 86.0% | 73.3%–94.2% |
| YI | 13.3% | 1.2%–25.5% | 8.3% | -9.7%–26.3% | 66.7% | 45.6%–87.8% |
| PPV | 43.5% | 28.9%–58.9% | 60.0% | 14.7%–94.7% | 93.3% | 68.1%–99.8% |
| NPV | 100.0% | 39.8%–100.0% | 62.2% | 46.5%–76.2% | 82.9% | 66.4%–93.4% |
| LR+ | 1.15 | 1.00–1.33 | 2.25 | 0.41–12.28 | 21.00 | 2.99–147.35 |
| LR- | 0.00 | 0.00–0.00 | 0.91 | 0.74–1.12 | 0.31 | 0.16–0.61 |
| LR | Infinity | Infinity–Infinity | 2.47 | 0.37–16.32 | 67.67 | 7.42–617.45 |
| Kappa | 0.110 | 0.002–0.218 | 0.095 | -0.110–0.300 | 0.696 | 0.492–0.899 |
| ^P-value | 0.089 | 0.336 | <0.001* | |||
^Kappa test.
Significant (<0.050)
CI, Confidence interval, DA, Diagnostic accuracy, YI, Youden's Index, PPV, Positive Predictive value, NPV, Negative Predictive value, LR+, Positive likelihood ratio, LR-, Negative likelihood ratio, LR, Diagnostic odds ratio
In diagnosing hemothorax, X-Ray and E-FAST respectively had significant moderate and high agreements with CT (golden) findings. NEXUS had highest sensitivity and NPV but had also the lowest specificity and PPV. E-FAST had highest specificity, PPV, diagnostic accuracy and Youden's index (Table 4).
Table 4.
Diagnostic characteristics of NEXUS, X-Ray and E-FAST in diagnosing hemothorax
| Characters | Value | 95% CI | Value | 95% CI | Value | 95% CI |
|---|---|---|---|---|---|---|
| NEXUS | X-RAY | E-FAST | ||||
| Sensitivity | 90.0% | 55.5%–99.7% | 60.0% | 26.2%–87.8% | 80.0% | 44.4%–97.5% |
| Specificity | 7.5% | 1.6%–20.4% | 95.0% | 83.1%–99.4% | 97.5% | 86.8%–99.9% |
| DA | 24.0% | 13.1%–38.2% | 88.0% | 75.7%–95.5% | 94.0% | 83.5%–98.7% |
| YI | -2.5% | -22.8%–17.8% | 55.0% | 23.9%–86.1% | 77.5% | 52.2%–102.8% |
| PPV | 19.6% | 9.4%–33.9% | 75.0% | 34.9%–96.8% | 88.9% | 51.8%–99.7% |
| NPV | 75.0% | 19.4%–99.4% | 90.5% | 77.4%–97.3% | 95.1% | 83.5%–99.4% |
| LR+ | 0.97 | 0.78–1.22 | 12.00 | 2.84–50.77 | 32.00 | 4.51–227.17 |
| LR- | 1.33 | 0.15–11.50 | 0.42 | 0.20–0.90 | 0.21 | 0.06–0.71 |
| LR | 0.73 | 0.07–7.87 | 28.50 | 4.25–191.17 | 156.00 | 12.58–1935.20 |
| Kappa | -0.011 | -0.097–0.076 | 0.595 | 0.304–0.886 | 0.805 | 0.593–1.017 |
| ^P-value | 0.749 | <0.001* | <0.001* | |||
CI, Confidence interval, DA, Diagnostic accuracy, PPV, Positive Predictive value, NPV, Negative Predictive value, LR+, Positive likelihood ratio, LR-, Negative likelihood ratio, LR, Diagnostic odds ratio
In diagnosing pneumothorax/ hemothorax, only E-FAST had significant moderate agreement with CT (golden) findings. NEXUS had highest sensitivity and NPV but had also the lowest specificity and PPV. E-FAST had highest specificity, PPV, diagnostic accuracy and Youden's index (Table 5).
Table 5.
Diagnostic characteristics of NEXUS, X-Ray and E-FAST in diagnosing pneumothorax/ hemothorax
| Characters | Value | 95% CI | Value | 95% CI | Value | 95% CI |
|---|---|---|---|---|---|---|
| NEXUS | X-RAY | E-FAST | ||||
| Sensitivity | 96.7% | 82.8%–99.9% | 30.0% | 14.7%–49.4% | 73.3% | 54.1%–87.7% |
| Specificity | 15.0% | 3.2%–37.9% | 80.0% | 56.3%–94.3% | 90.0% | 68.3%–98.8% |
| DA | 64.0% | 49.2%–77.1% | 50.0% | 35.5%–64.5% | 80.0% | 66.3%–90.0% |
| YI | 11.7% | -5.2%–28.6% | 10.0% | -14.0%–34.0% | 63.3% | 42.8%–83.9% |
| PPV | 63.0% | 47.5%–76.8% | 69.2% | 38.6%–90.9% | 91.7% | 73.0%–99.0% |
| NPV | 75.0% | 19.4%–99.4% | 43.2% | 27.1%–60.5% | 69.2% | 48.2%–85.7% |
| LR+ | 1.14 | 0.94–1.38 | 1.50 | 0.53–4.21 | 7.33 | 1.93–27.79 |
| LR- | 0.22 | 0.02–1.99 | 0.88 | 0.63–1.21 | 0.30 | 0.16–0.55 |
| LR | 5.12 | 0.49–53.18 | 1.71 | 0.45–6.58 | 24.75 | 4.66–131.48 |
| Kappa | 0.135 | -0.059–0.328 | 0.088 | -0.124–0.299 | 0.603 | 0.389–0.817 |
| ^P-value | 0.136 | 0.430 | <0.001* | |||
CI, Confidence interval, DA, Diagnostic accuracy, PPV, Positive Predictive value, NPV, Negative Predictive value, LR+, Positive likelihood ratio, LR-, Negative likelihood ratio, LR, Diagnostic odds ratio
Discussion
To the best of our knowledge, this is a unique study that evaluated the diagnostic accuracy of the NEXUS chest algorithm in detecting both hemothorax and pneumothorax individually and compared the diagnostic accuracy of both E-FAST and NEXUS criteria in detecting blunt chest injuries.
The mean age of our study patients was 37.7 ± 14.6 years, with the major age group being 30–40 years. This finding indicates that the majority of patients were in the economically productive age group in Egypt. This result is consistent with a study performed by Kozaci N, et al., which was conducted at Antalya Education and Research Hospital in Turkey from June 2015 to March 2018, wherein the mean age of the study population was 38 ± 20 years [6]. This might be because the middle-aged group of individuals used motor vehicles more often than others [14].
Several studies have reported a specific relationship between the male gender and increased trauma, possibly due to the more active behavior of men than women [15]. Even in eastern societies, men predominate in practicing several activities that are restricted to women, such as sports and motor cycling, which increases the risk of trauma. This is consistent with our study, in which 82% of the study patients were men. Our results are also comparable with those of another cross-sectional study, which was conducted at the emergency centre of Sina Hospital from March 2011 to March 2012, in which 84% were men [16].
Road traffic crashes are one of the world's largest preventable public health problems. According to the WHO, the number of road traffic deaths was 1.25 million in 2013, which has remained fairly constant since 2007, despite the increase in global motorization and population and the predicted rise in the number of deaths [11]. In our study, motor vehicle accidents were responsible for 46% of the total cases, followed by falls (22%). This result is in agreement with another study conducted by Yasser Abdulrahman et al. at a level I trauma center in Qatar between July 2011 and January 2013, in which motor vehicle crashes (46.6%) and falls from height (22.6%) were the most frequently associated injury mechanisms [2].
In a multicenter, prospective cohort study conducted at nine US level I trauma centers from December 2009 to January 2012, the NEXUS chest algorithm was derived and validated to decrease unnecessary thoracic imaging in patients with blunt trauma, and the sensitivity and specificity in detecting chest injuries in general were found to be 99.7% and 13.3%, respectively [17]. In our study, we focused only on its role in the detection of both hemothorax and pneumothorax in comparison with E-FAST. Our results demonstrated that the NEXUS chest algorithm had 100% sensitivity and 15% specificity in detecting pneumothorax and 90% sensitivity and 7.5% specificity in detecting hemothorax, whereas it had a sensitivity of 96.7% and a specificity of only 15% in detecting both pneumothorax and hemothorax together. Therefore, the NEXUS chest algorithm identifies a very low-risk population of patients with blunt trauma for whom chest imaging can be avoided. However, it requires that all the seven study chest criteria be absent [18].
As radiation exposure continues to increase in trauma patients, attempts are being made to provide more directed imaging to the chest. Consequently, the US imaging technique has improved, and its role continues to advance in the initial evaluation of a trauma patient [19]. In our study, the comparative analysis of pneumothorax detection using different diagnostic modalities revealed that E-FAST had a sensitivity of 70% and a specificity of 95%, with a statistically significant relationship. This result is consistent with the study conducted by Chitra Subramaniam, et al., which included patients admitted to Govt. Rajaji Hospital Trauma Care Center with blunt injury chest and reported that ultrasonography has a very good sensitivity of 72.41% and a specificity of 100% [20].
On the other hand, in our study, the comparative analysis of hemothorax detection using different diagnostic modalities revealed that E-FAST had a sensitivity of 80% and a specificity of 97.5%, with a statistically significant relationship. This result is in agreement with a retrospective cross-sectional study conducted by Ali Vafaei et al., which included patients with traumatic intrathoracic injuries, who were referred to the emergency centre from December 2013 to December 2014, in which the sensitivity and specificity of E-FAST for hemothorax detection were 75.9% and 95.9%, respectively [21]. In our study, the sensitivity and specificity of E-FAST in detecting both pneumothorax and hemothorax together were 73.3% and 90%, respectively.
The supine anteroposterior CXR has been the initial thoracic evaluation tool during a trauma examination. Its use is primarily to screen for pneumothorax, hemothorax, fractures, and aortic injuries. Unfortunately, studies continue to demonstrate that it has a low sensitivity in diagnosing several critical injuries, missing pneumothorax in 30%–40% of patients and 5%–15% of blunt thoracic aorta injuries.[16,[22], [23], [24]] In our study, the sensitivity of CXR was only 15% in detecting pneumothorax, which is consistent with the study of Yasser Abdulrahman et al. conducted at a level I trauma center in Qatar, in which the sensitivity of CXR was only 10.7% [2]. Another study conducted by Chitra Subramanian et al. reported a sensitivity of 17.24% [20].
On the other hand, our study demonstrated a sensitivity of 60% for CXR in detecting hemothorax, with a statistically significant relationship. This finding is consistent with the study conducted by Nejat A, et al. that evaluated the efficacy, sensitivity, and specificity of chest X-ray as a diagnostic imaging tool in the management of thorax traumas, in which the sensitivity of CXR in hemothorax detection was 62.5% [25].
Our study has some important limitations. First, for the elimination of bias due to the difference in personal skills and years of experience, there was a fixed radiologist for the examination of all cases. However, this led to the difficulty in obtaining some cases due to the unavailability of the fixed radiologist on certain occasions.
Second, due to the relatively small sample size, further studies with a greater number of patients would be helpful to provide more accurate results, which can be generalized.
Lung sliding seen in the anterior lung fields bilaterally effectively rules out large pneumothorax with a sensitivity of 95.3% and a negative predictive value of 100%. However, the absence of lung sliding does not always indicate the presence of pneumothorax (specificity <80%) ([26,27])
Conclusion
E-FAST is highly specific for the detection of hemothorax, pneumothorax, and chest injuries compared with the NEXUS chest algorithm, which showed the lowest specificity. However, the NEXUS chest algorithm had a higher sensitivity than E-FAST and hence can be used effectively to rule out thoracic injury.
E-FAST can be used as an efficient triaging tool in blunt chest trauma patients that could be performed simultaneously along with resuscitation in trauma room to explore life-threatening injuries without any delay or even interruption of resuscitation.
E-FAST is cost-effective and repeatable, even when the clinical status of the patient changes. Therefore, more efforts are required to improve familiarity with thoracic US in critical care units and emergency centres.
NEXUS Chest algorithms can effectively rule out thoracic injury observed on chest imaging, when none of the 7 criteria are present. However, its specificity is low and consequently many uninjured patients will exhibit at least 1 of the 7 criteria.
Dissemination of results
Results of this study were presented locally at the emergency center scientific day with staff members at Suez Canal University.
Funding
This work was funded by the National Institutes of Health, Fogarty International Center, Bethesda, MD (grant number, 2D43TW007296).
Authors’ contribution
Authors contributed as follows to the conception or design of the work; the acquisition, analysis, or interpretation of data for the work; and drafting the work or revising it critically for important intellectual content: YZA contributed 65%; NMA contributed 5%; HME contributed 5%; GME contributed 5%; ME contributed 5%; JMH contributed 5%; AHE contributed 5% and ME contributed 5%. All authors approved the version to be published and agreed to be accountable for all aspects of the work.
Declaration of Competing Interests
This work was funded by the National Institutes of Health, Fogarty International Center, Bethesda, MD (grant number, 2D43TW007296). The authors declare that they have no other competing interests.
Footnotes
Supplementary material associated with this article can be found, in the online version, at doi:10.1016/j.afjem.2023.02.003.
Appendix. Supplementary materials
References
- 1.Daurat A, Millet I, Roustan J-P, Maury C, Taourel P, Jaber S, et al. Thoracic trauma severity score on admission allows to determine the risk of delayed ARDS in trauma patients with pulmonary contusion. Injury. 2016;47(1):147–153. doi: 10.1016/j.injury.2015.08.031. [DOI] [PubMed] [Google Scholar]
- 2.Abdulrahman Y, Musthafa S, Hakim SY, Nabir S, Qanbar A, Mahmood I, et al. Utility of extended FAST in blunt chest trauma: is it the time to be used in the ATLS algorithm? World J Surg. 2015;39(1):172–178. doi: 10.1007/s00268-014-2781-y. [DOI] [PubMed] [Google Scholar]
- 3.Alberdi F, Garcia I, Atutxa L, Zabarte M. Epidemiology of severe trauma. Medicina Intensiva. 2014;38(9):580–588. doi: 10.1016/j.medin.2014.06.012. [DOI] [PubMed] [Google Scholar]
- 4.Rossaint R, Bouillon B, Cerny V, Coats TJ, Duranteau J, Fernández-Mondéjar E, et al. Management of bleeding following major trauma: an updated European guideline. Critical Care. 2010;14(2):1–29. doi: 10.1186/cc8943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Battle C, Hayward S, Eggert S, Evans PA. Comparison of the use of lung ultrasound and chest radiography in the diagnosis of rib fractures: a systematic review. Emerg Med J. 2019;36(3):185–190. doi: 10.1136/emermed-2017-207416. [DOI] [PubMed] [Google Scholar]
- 6.Kozaci N, Avcı M, Ararat E, Pinarbasili T, Ozkaya M, Etli I, et al. Comparison of ultrasonography and computed tomography in the determination of traumatic thoracic injuries. Am J Emerg Med. 2019;37(5):864–868. doi: 10.1016/j.ajem.2018.08.002. [DOI] [PubMed] [Google Scholar]
- 7.Mojtaba C, Toktam H-G, Hesam A, Vafa R-M. Accuracy of chest radiography versus chest computed tomography in hemodynamically stable patients with blunt chest trauma. Chin J Traumatol. 2013;16(06):351–354. [PubMed] [Google Scholar]
- 8.Harvey J, West A. The right scan, for the right patient, at the right time: the reorganization of major trauma service provision in England and its implications for radiologists. Clin Radiol. 2013;68(9):871–886. doi: 10.1016/j.crad.2013.01.006. [DOI] [PubMed] [Google Scholar]
- 9.Murphy SP, Hawthorne N, Haase D, Chiku C, Wen J, Rodriguez RM. Low yield of clinically significant injury with Head-To-Pelvis computed tomography in blunt trauma evaluation. J Emerg Med. 2017;53(6):865–870. doi: 10.1016/j.jemermed.2017.08.036. [DOI] [PubMed] [Google Scholar]
- 10.Linder F, Mani K, Juhlin C, Eklöf H. Routine whole body CT of high energy trauma patients leads to excessive radiation exposure. SJTREM. 2016;24(1):1–7. doi: 10.1186/s13049-016-0199-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Organization WH. World Health Organization; 2015. Global status report on road safety 2015. [Google Scholar]
- 12.Rodriguez RM, Anglin D, Langdorf MI, Baumann BM, Hendey GW, Bradley RN, et al. NEXUS chest: validation of a decision instrument for selective chest imaging in blunt trauma. JAMA Surg. 2013;148(10):940–946. doi: 10.1001/jamasurg.2013.2757. [DOI] [PubMed] [Google Scholar]
- 13.Ianniello S, Di Giacomo V, Sessa B, Miele V. First-line sonographic diagnosis of pneumothorax in major trauma: accuracy of e-FAST and comparison with multidetector computed tomography. Radiol Med (Torino) 2014;119(9):674–680. doi: 10.1007/s11547-014-0384-1. [DOI] [PubMed] [Google Scholar]
- 14.Zhang J, Fraser S, Lindsay J, Clarke K, Mao Y. Age-specific patterns of factors related to fatal motor vehicle traffic crashes: focus on young and elderly drivers. Public Health. 1998;112(5):289–295. doi: 10.1038/sj.ph.1900485. [DOI] [PubMed] [Google Scholar]
- 15.Martin CG, Cromer LD, DePrince AP, Freyd JJ. The role of cumulative trauma, betrayal, and appraisals in understanding trauma symptomatology. Psychol Trauma. 2013;5(2):110. doi: 10.1037/a0025686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Chardoli M, Hasan-Ghaliaee T, Akbari H. Rahimi-Movaghar V. Accuracy of chest radiography versus chest computed tomography in hemodynamically stable patients with blunt chest trauma. Chin J Traumatol. 2013;16(6):351–354. [PubMed] [Google Scholar]
- 17.Raja AS, Lanning J, Gower A, Langdorf MI, Nishijima DK, Baumann BM, et al. Prevalence of chest injury with the presence of NEXUS Chest criteria: Data to inform shared decisionmaking about imaging use. Ann Emerg Med. 2016;68(2):222–226. doi: 10.1016/j.annemergmed.2015.09.024. [DOI] [PubMed] [Google Scholar]
- 18.Rodriguez RM, Langdorf MI, Nishijima D, Baumann BM, Hendey GW, Medak AJ, et al. Derivation and validation of two decision instruments for selective chest CT in blunt trauma: a multicenter prospective observational study (NEXUS Chest CT) PLoS Med. 2015;12(10) doi: 10.1371/journal.pmed.1001883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Körner M, Krötz MM, Degenhart C, Pfeifer K-Jr, Reiser MF, Linsenmaier U. Current role of emergency US in patients with major trauma. Radiographics. 2008;28(1):225–242. doi: 10.1148/rg.281075047. [DOI] [PubMed] [Google Scholar]
- 20.Subramaniam C, Chakaravarthy DA. Utility of extended focused assessment with sonography in blunt chest trauma-its clinical implication and its sensitivity compared with chest x-ray and clinical examination. JEMDS. 2017;6(4):328–333. [Google Scholar]
- 21.Vafaei A, Hatamabadi HR, Heidary K, Alimohammadi H, Tarbiyat M. Diagnostic accuracy of ultrasonography and radiography in initial evaluation of chest trauma patients. Emergency. 2016;4(1):29. [PMC free article] [PubMed] [Google Scholar]
- 22.Kea B, Gamarallage R, Vairamuthu H, Fortman J, Lunney K, Hendey GW, et al. What is the clinical significance of chest CT when the chest x-ray result is normal in patients with blunt trauma? Am J Emerg Med. 2013;31(8):1268–1273. doi: 10.1016/j.ajem.2013.04.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Trupka A, Waydhas C, Hallfeldt K, Nast-Kolb D, Pfeifer K, Schweiberer L. Value of thoracic computed tomography in the first assessment of severely injured patients with blunt chest trauma: results of a prospective study. J Trauma Acute Care Surg. 1997;43(3):405–412. doi: 10.1097/00005373-199709000-00003. [DOI] [PubMed] [Google Scholar]
- 24.Deunk J, Brink M, Dekker HM, Kool DR, Blickman JG, van Vugt AB, et al. Routine versus selective multidetector-row computed tomography (MDCT) in blunt trauma patients: level of agreement on the influence of additional findings on management. J Trauma Acute Care Surg. 2009;67(5):1080–1086. doi: 10.1097/TA.0b013e318189371d. [DOI] [PubMed] [Google Scholar]
- 25.Cakmak M, Yuksel M, Kandemir MN. Characteristics of the patients undergoing surgical treatment for pneumothorax: a descriptive study. J Pak Med Assoc. 2016;66(5):554–558. [PubMed] [Google Scholar]
- 26.Chichra A, Makaryus M, Chaudhari P, Narasimhan M. Ultrasound for the pulmonary consultant. Clin Med Insights. 2016;10:1. doi: 10.4137/CCRPM.S33382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lichtenstein DA, Mezière G, Lascols N, Biderman P, Courret J-P, Gepner A, et al. Ultrasound diagnosis of occult pneumothorax. Crit Care Med. 2005;33(6):1231–1238. doi: 10.1097/01.ccm.0000164542.86954.b4. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.