

Abstract
Background
Health care systems have become increasingly more reliant on patients’ ability to navigate the digital world. However, little research has been conducted on why some communities are less able or less likely to successfully engage with digital health technologies (DHTs), particularly among culturally and linguistically diverse (CaLD) populations.
Objective
This systematic review aimed to determine the barriers to and facilitators of interacting with DHTs from the perspectives of CaLD population groups, including racial or ethnic minority groups, immigrants and refugees, and Indigenous or First Nations people.
Methods
A systematic review and thematic synthesis of qualitative studies was conducted. Peer-reviewed literature published between January 2011 and June 2022 was searched across 3 electronic databases. Terms for digital health were combined with terms for cultural or linguistic diversity, ethnic minority groups, or Indigenous and First Nations people and terms related to barriers to accessing digital technologies. A qualitative thematic synthesis was conducted to identify descriptive and analytical themes of barriers to and facilitators of interacting with DHTs. Quality appraisal was performed using the Mixed Methods Appraisal Tool.
Results
Of the 1418 studies identified in the electronic search, a total of 34 (2.4%) were included in this review. Half of the included studies (17/34, 50%) were conducted in the United States. There was considerable variation in terms of the CaLD backgrounds of the participants. In total, 26% (9/34) of the studies focused on Indigenous or First Nations communities, 41% (14/34) were conducted among ethnic minority populations, 15% (5/34) of the studies were conducted among immigrants, and 18% (6/34) were conducted in refugee communities. Of the 34 studies, 21 (62%) described the development or evaluation of a digital health intervention, whereas 13 (38%) studies did not include an intervention but instead focused on elucidating participants’ views and behaviors in relation to digital health. From the 34 studies analyzed, 18 descriptive themes were identified, each describing barriers to and facilitators of interacting with DHTs, which were grouped into 7 overarching analytical themes: using technology, design components, language, culture, health and medical, trustworthiness, and interaction with others.
Conclusions
This study identified several analytic and descriptive themes influencing access to and uptake of DHTs among CaLD populations, including Indigenous and First Nations groups. We found that cultural factors affected all identified themes to some degree and that cultural and linguistic perspectives should be considered in the design and delivery of DHTs, with this best served through the inclusion of the target communities at all stages of development. This may improve the potential of DHTs to be more acceptable, appropriate, and accessible to population groups currently at risk of not obtaining the full benefits of digital health.
Keywords: culturally and linguistically diverse, ethnicity, indigenous, digital health, technology, eHealth, qualitative, mobile phone
Introduction
Background
Over the past decade, the health care system has increasingly relied on digital technologies to educate, organize, and support people in managing their health [1]. Digital health can be described as “the field of knowledge and practice associated with the development and use of digital technologies to improve health” [2]. Patient-facing technologies such as telehealth systems, web-based services, or smartphone apps are now widely used to support the prevention, diagnosis, treatment, and self-management of health [3]. There is a large body of evidence demonstrating the effectiveness of digital health technologies (DHTs) for the treatment and prevention of various health conditions across multiple settings, including communities, primary care, and hospitals [4-6]. Furthermore, the use of DHTs has been shown to address other barriers that patients commonly experience with the health care system, such as poor access to health care providers and increased costs [7].
Despite substantial investment and an increasing number of DHTs available to health care consumers, their uptake has been limited among some population groups [8]. These include lower–socioeconomic-level groups and people from culturally and linguistically diverse (CaLD) communities, with the latter including racial or ethnic minority groups, immigrants and refugees, and First Nations people [8-15]. Studies have repeatedly reported that CaLD populations have lower uptake and use of DHTs than non-CaLD populations [8,16,17]. For example, US-based studies have found that African American and Latino people are less likely to use digital technologies for health care than White Americans [12,18], whereas other studies have shown less acceptability of DHTs among immigrants [12,13]. Indigenous and First Nations people are also less likely to use DHTs because of difficulties in access and low cultural appropriateness of the technology [19]. As such, DHTs may widen the existing inequalities within our health care system by creating a digital divide that affects the effective and equitable delivery of care [10].
This lower uptake of DHTs may, in part, be owing to a failure to meet the cultural, linguistic, or health literacy needs of these diverse population groups [20]. When designing DHTs, it is important to gain an understanding of the perspectives of the end users themselves (eg, consumers, patients, and carers) on the factors influencing their use of digital health [17]. Qualitative research approaches offer the opportunity to explore these perspectives in depth, with studies conducted among CaLD populations identifying several barriers to and facilitators of the uptake of digital health, including technical literacy, access to the internet, and acceptance of services [17]. Although this evidence is important for understanding barriers and facilitators from a consumer’s perspective, these qualitative studies are often small or focused on a single digital health intervention and, as such, may not provide representative data [21]. Furthermore, although existing qualitative reviews have explored barriers to and facilitators of the uptake of DHTs, few have explored the reasons influencing their use among CaLD populations [19,22-24].
Objectives
This study aimed to review and synthesize qualitative literature to determine the barriers to and facilitators of interacting with DHTs from the perspectives of CaLD population groups. In this review, CaLD populations were defined as those who were (1) born in countries where the official language differs from that of their current country of residence or their language spoken at home is not the official language of the country where they reside, (2) First Nations or Indigenous populations (who may or may not speak English), or (3) populations who were described in studies as “ethnically/racially diverse” or “ethnic/racial minority” [11]. We acknowledge the considerable heterogeneity among these groups; however, our intention was to capture population groups that are generally underserved in the health sector based on their cultural, linguistic, or ethnic background to identify the appropriateness of digital health for these groups and highlight areas for improvement [19]. We also acknowledge a recent recommendation that First Nations or Indigenous populations be reported separately from CaLD findings in research projects [11]. However, the small sample size of many studies with First Nations or Indigenous people indicates a need for caution when drawing community-wide conclusions, as recommended in other studies [25,26]. Therefore, for the purposes of assessing this review, we grouped these populations as we hypothesized that they may share many of the same concerns in terms of barriers and facilitators regarding DHTs.
Methods
Study Design
A systematic review and thematic synthesis of qualitative studies were conducted following the guidance of the Enhanced Transparency of Reporting the Synthesis of Qualitative Research framework and reporting guidelines [27].
Inclusion Criteria
Inclusion criteria were defined according to the Population, Intervention, Comparison, Outcome, and Study Type framework (Textbox 1). Additional inclusion criteria included publication in a peer-reviewed scientific journal in English and being accessible in full text. Protocols for research studies, book chapters, systematic reviews, and theses were excluded.
Study inclusion criteria according to the Population, Intervention, Comparison, Outcome, and Study Type framework.
-
Population
Studies on participants who were identified as patients, health consumers, or carers from culturally and linguistically diverse (CaLD) backgrounds or where CaLD groups were a subgroup of participants with results reported separately were included. To include studies from countries that do not share a common definition of CaLD communities, the following parameters were used to define CaLD: (1) those who were born in countries where the official language is not the same as that of their current country of residence or their main language spoken at home is not the official language of their current country of residence or (2) those described in the studies as “minority,” “ethnically/racially diverse,” and “ethnic/racial minority.” These studies may include Black and African American populations, as well as First Nations and Indigenous peoples in Canada, United States, New Zealand, and Australia.
-
Intervention
An intervention was included if it was delivered using a digital method (eg, smartphone) and directed at prevention, diagnosis, treatment, or self-management of health. Studies with no intervention were also included if participants discussed their perspectives on digital health more broadly as long as it was relevant to our aim. Studies conducted in any setting were included. Studies that focused only on telephone calls with no other digital health component were excluded.
-
Outcomes
Studies were included where findings were reported as participants’ perspectives on the barriers to and facilitators of access to and use of digital health or digital health technologies. Studies that reported clinician perspectives only were excluded.
-
Study design
Primary research studies were included if they used qualitative methods for data collection (eg, focus groups or interviews and open-ended survey questions) and data analysis (eg, thematic analysis). Studies using other designs (eg, mixed methods or cross-sectional) were included as long as there was a component of qualitative data collection and analysis that was reported separately from the quantitative component.
Search Strategy
An electronic search using 3 web-based databases (Ovid MEDLINE, Embase, and CINAHL) was performed to find studies published between January 2011 and June 2022. Terms for digital health were combined with terms for cultural or linguistic diversity, ethnic minority groups, or Indigenous or First Nations people and terms related to barriers to accessing digital technologies. Ovid MEDLINE search terms are shown in Multimedia Appendix 1. Reference lists from eligible studies and systematic reviews were also searched. The results were imported into the Covidence systematic review software (Veritas Health Innovation), where each title and abstract was independently screened by 2 researchers, with discrepancies resolved by consulting a third researcher. Full texts of potentially relevant articles were then inspected for inclusion by 2 researchers based on the aforementioned inclusion criteria.
Data Extraction
Data were extracted within Covidence using the following headings: study description (country of study and study design), participant description (percentage of female participants, mean age, and CaLD group), the type of digital health or DHT discussed and a brief description (if relevant), and results (extracted as relevant quotes from study participants and as text from the results section of each paper where authors identified barriers to and facilitators of interacting with DHT).
Data Synthesis
We conducted a qualitative thematic synthesis as described by Thomas and Harden [28]. A thematic synthesis treats qualitative findings as data for analysis [28]; these data include both direct quotes from participants and summaries and interpretation of findings from study authors. We used an inductive approach, whereby themes related to interacting with digital health were identified from within the data. We followed the three thematic synthesis steps by Thomas and Harden [28]: (1) free line-by-line coding, (2) organization of these codes to construct descriptive themes, and (3) development of analytical themes. In step 1, quotes and text were coded (“named”) according to their meaning and content. One author (LW) coded all studies individually. New codes were added as necessary as the researcher continued re-examining the data. Two authors (LW and AB) discussed the codes and revised the coding schema as needed. In step 2, similar codes were grouped together to create descriptive themes related to barriers and enablers; at this point, the synthesis still followed the original findings of the included studies. The frequency of the themes was recorded as the number of times the theme was mentioned across the included articles. In step 3, these descriptive themes were interpreted to develop inferences about barriers and enablers and implications for future research (“analytical themes”). To examine the hypothesis that First Nations or Indigenous populations share many of the same barriers and facilitators regarding DHTs as other CaLD populations, we performed a subgroup analysis using the aforementioned data synthesis approach.
Quality Appraisal
Quality appraisal was undertaken using the 2018 version of the Mixed Methods Appraisal Tool developed for use in systematic reviews of mixed methods studies [29]. This tool is designed for the appraisal stage of reviews that include qualitative, quantitative, and mixed methods studies and applies 5 specific quality criteria to each study design, with results presented as a percentage score for each study indicating the proportion of criteria met. For quantitative studies, quality criteria included randomization (if appropriate), representativeness of participants, completeness of outcome data, bias, confounding, and statistical analysis. For qualitative studies, quality criteria included appropriateness of the approach used; data collection and analysis methods; and coherence between data sources, analysis, and interpretation. For mixed methods studies, criteria were related to both the aforementioned quantitative and qualitative aspects plus the rationale for using a mixed methods design and adequate integration of the qualitative and quantitative phases of the study.
Results
A total of 1418 studies were identified through database searches, with 1 additional study identified through reference list searches. Of these 1419 studies, 148 (10.43%) full-text articles were assessed for eligibility, with 34 (2.4%) studies included in this review (Figure 1).
Figure 1.
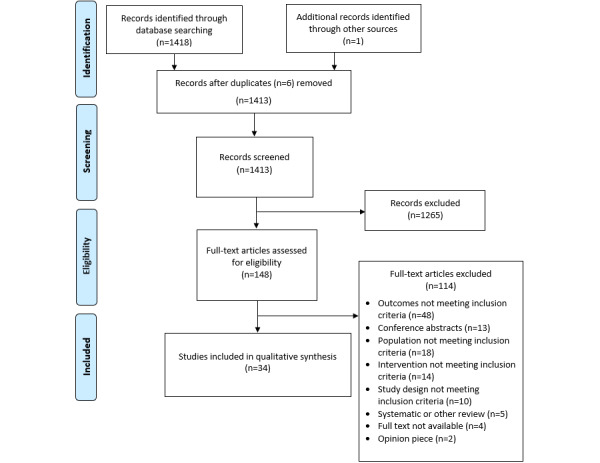
Prisma Flow Diagram.
Study Characteristics
Table 1 describes study and participant characteristics for all studies. Most of the included studies were conducted in the United States (17/34, 50%), Australia (6/34, 18%), and Canada (4/34, 12%), with 32% (11/34) of the studies using a mixed methods design and 6% (2/34) being randomized controlled trials, the latter including interviews with intervention participants to explore the cultural acceptability of the tool [30] and barriers to and enablers of the use of the app [31]. Nearly all studies (32/34, 94%) were conducted in the community, with 6% (2/34) conducted in primary care or outpatient clinics [32,33].
Table 1.
Study and participant characteristics (N=34).
| First author, year | Study design | Country and setting | Participant characteristics | Health condition | Quality rating | ||||
|
|
|
|
CaLDa background | Sample size, N | Age (years) |
|
|
||
| Aguilera et al [34], 2014 | Qualitative | United States; community | Latino, African American, and Euro-American | 20 | Mean 56 | Depression | 60% | ||
| Bagchi et al [35], 2018 | Mixed methods | United States; community | African American | 10 | Mean 59.9 | None | 60% | ||
| Blackwell et al [36], 2020 | Mixed methods | United States; community | African American, Hispanic, and Caribbean West Indian | 56 | FGb: range 20-45; T4Bc: mean 28 | Pregnancy | 100% | ||
| Brown et al [37], 2014 | Qualitative | United States; community | African American and Hispanic | 5 | Mean 18.2 (SD 0.8) | Postpartum depression | 80% | ||
| Burchert et al [38], 2019 | Qualitative | Egypt, Germany, and Sweden; community | Syrian refugees | 128 | Id: mean 33 (SD 11); KIIe: mean 33.8 (SD 10.9); FG: NRf | Mental health | 100% | ||
| Claudel et al [39], 2020 | Mixed methods | United States; community | African American | 16 | Mean 62.1 (SD 6.6) | Overweight or obesity | 80% | ||
| Filippi et al [40], 2012 | Qualitative | United States; community | American Indians | 108 | NR | Smoking cessation | 100% | ||
| Garner et al [41], 2021 | Mixed methods | Hong Kong; community | Asian Indian immigrants | 46 | Range 18-≥60; 54%, 15-59 | Hypertension and diabetes | 80% | ||
| Gesser-Edelsburg et al [20], 2017 | Qualitative | Israel; community | Former Soviet Union immigrants | 18 | Range 24-58 | Nutrition and diet | 80% | ||
| Goodall et al [42], 2014 | Qualitative | Australia; community | Greek and Italian immigrants | 54 | Mean 74.1 | None | 100% | ||
| Hiratsuka et al [32], 2013 | Qualitative | United States; primary care clinic | Alaska and Hawaiian Native | 17 | NR | Diabetes | 80% | ||
| Hyman et al [43], 2022 | Qualitative | Canada; community | Asian Indian immigrants | 46 | Mean 65.4 (SD 12.1) | Chronic disease | 100% | ||
| Hynie et al [44], 2022 | Qualitative | Canada; community | Syrian, Iranian, Eritrean, Somali, and Ethiopian refugees | 197 | Mean 35.4 (SD 9.8) | Mental health | 80% | ||
| Im et al [45], 2021 | Qualitative | United States; community | Korean American | 17 | NR | Breast cancer | 80% | ||
| Johnson-Turbes et al [46], 2015 | Mixed methods | United States; community | African American | 180 | NR | Breast cancer | 80% | ||
| Jongbloed et al [47], 2020 | Mixed methods | Canada; community | First Nations, Inuit, and Métis | 131 | Mean 33 (range 30-36) | Illicit drug use | 100% | ||
| Kurth et al [30], 2016 | RCTg | United States; community | Hispanic or Latino | 61 | Mean 48 (SD 12) | HIV | 20% | ||
| Lindegaard et al [48], 2021 | Qualitative | Sweden; community | Arabic-speaking immigrants and refugees | 10 | Mean 33.4 (SD 9.1) | Mental health | 80% | ||
| Lindegaard et al [49], 2022 | Mixed methods | Sweden; community | Dari or Farsi refugees and immigrants | 7 | Mean 22.3 (SD 2.35) | Mental health | 60% | ||
| Lyles et al [50], 2016 | Qualitative | United States; community | African American and Hispanic or Latino | 87 | Range 24-69 | Chronic disease | 100% | ||
| Maertens et al [51], 2017 | Qualitative | United States; community | Hispanic or Latino | 47 | NR | HPVh | 60% | ||
| McAra-Couper et al [52], 2020 | Qualitative | New Zealand; community | Mäori and Pacific Islanders | 24 | Range 16-40 | Pregnancy and reproductive health | 100% | ||
| Merculieff et al [53], 2020 | Mixed methods | United States; community | Alaska Native | 30 | Mean 45 (SD 12) | Smoking cessation | 40% | ||
| Ospina-Pinillos et al [54], 2019 | Qualitative | Australia; community | Colombian, Chilean, Argentinian, Spanish, and Venezuelan immigrants | 17 | Co-design: mean 24 (range 17-29); think-aloud: mean 26 (range 19-30) | Mental health | 60% | ||
| Pasipanodya et al [55], 2020 | Qualitative | United States; community | African American and Hispanic | 13 | Mean 46 (range 38-53) | HIV | 100% | ||
| Peiris et al [31], 2019 | RCT | Australia; community | Aboriginal and Torres Strait Islanders | 49 | Mean 42 (SD 14) | Smoking | 60% | ||
| Povey et al [56], 2016 | Qualitative | Australia; community | Aboriginal and Torres Strait Islanders | 9 | Mean 33 (SD 17) | Mental health | 100% | ||
| Rempel et al [57], 2016 | Qualitative | Canada; community | First Nations, Inuit, and Métis | 8 | Mean 23 | None | 80% | ||
| Spanhel et al [58], 2019 | Qualitative | Germany; community | Syrian, Iranian, Eritrean, Algerian, and Iraqi refugees | 6 | Mean 38 (SD 11.8) | Sleeping issues | 80% | ||
| Tappen et al [59], 2021 | Mixed methods | United States; community | African American, Hispanic, and European American | 49 | Mean 73 (SD 10) | None | 80% | ||
| Tighe et al [60], 2020 | Mixed methods | Australia; community | Aboriginal and Torres Strait Islanders | 13 | Mean 24.2 (SD 4.7) | Mental health | 60% | ||
| Wan et al [61], 2018 | Qualitative | United States; community | Tongan American | 36 | Mean 50 | Physical activity | 60% | ||
| Willey et al [33], 2020 | Qualitative | Australia; primary care | Afghan, Burmese, Indian, and Vietnamese refugees | 22 | NR | Mental health | 100% | ||
| Ye et al [62], 2012 | Mixed methods | United States; community | Korean immigrants | 16 | Mean 45.1 (SD 8.2) | Mental health | 20% | ||
aCaLD: culturally and linguistically diverse.
bFG: focus group.
cT4B: Text4Baby.
dI: interview.
eKII: key informant interview.
fNR: not reported.
gRCT: randomized controlled trial.
hHPV: human papillomavirus.
The sample sizes ranged from 5 to 197 (median 23), with an age range of 16 to 74 years. Most of the health topics considered were related to mental health (11/34, 32%), chronic health conditions (8/34, 24%), or lifestyle factors such as smoking or obesity and nutrition. In total, 12% (4/34) of the studies did not relate to any health topic. There was considerable variation in terms of the CaLD backgrounds of the participants. A total of 26% (9/34) of the studies focused on Indigenous or First Nations communities from the United States [32,40,53], Australia [31,56,60], Canada [47,57], and New Zealand [52]. Of the remaining 14 US studies, 3 (21%) were conducted solely in African American communities [35,39,46]; 2 (14%) were conducted among Hispanic or Latino groups only [30,51]; and 6 (43%) were conducted in mixed communities such as Latino, African American, and Euro-American communities [34,36,37,50,55,59]. Of the 17 US studies, 1 (6%) was conducted among Tongan American communities [61], and 2 (12%) were conducted among Korean immigrants or Korean American individuals [45,62]. Immigrants were also represented in 15% (5/34) of the studies from other countries, including Israel [20], Australia [42,54], Canada [43], and Hong Kong [41]. Refugees were represented in 6 studies: 2 (33%) from Sweden [48,49]; 1 (17%) each from Australia [33], Germany [58], and Canada [44]; and 1 (17%) conducted across Egypt, Germany, and Sweden [38].
Study Quality
The quality rating for each study is shown in Table 1. A total of 65% (22/34) of the studies had a rating of ≥80%, indicating that they met at least 4 of the 5 criteria for that study design. Of the studies that met fewer criteria, reasons included limited description of the qualitative approach and methodology used by the qualitative designs. For quantitative designs, reasons included small or nonrepresentative samples and limited description of the tools used to assess outcomes.
Description of Interventions
A total of 62% (21/34) of the included studies described a DHT (Table 2). Of these 21 interventions, 4 (19%) were classified as SMS text messaging services, including cognitive behavioral therapy for depression [34], health-promotion messages to new mothers [36,37], and checking participants’ use of illicit drugs [47]. In total, 29% (6/21) of the studies were classified as internet-based interventions; these included 67% (4/6) of mental health interventions [38,49,54,58], a series of skill-building videos for participants with HIV [30], and a multimedia intervention to improve sleep [58]. A total of 24% (5/21) of the interventions were classified as Android or iOS apps, including 20% (1/5) of the studies that evaluated 2 apps: a mental health intervention based on motivational intervention and a suicide prevention app [56]. A further study evaluated an app for improving mental health [60], and apps were also used to support smoking cessation [31] and teach hypertension and diabetes management [41]. One intervention was classified as a digital health survey offering screening and feedback for mental health issues before meeting with a midwife [33]. A total of 10% (2/21) of the interventions were classified as videoconference consultations; these included a telepsychiatry consultation [62] and a remote nursing assessment [35]. Other interventions included a web-based portal where patients could access their medical history and message their health care provider [50]. A total of 6% (2/34) of the studies used websites as their technology: one providing learning modules on breast cancer [46] and one tailored to users’ beliefs in relation to vaccination for human papillomavirus [51]. In total, 38% (13/34) of the studies did not include an intervention (data not shown). Instead, participants were asked for their views on mobile technology and health apps [39,61]; their web-based health information–seeking behavior and needs [40,42,52,57,59]; their use and intentions regarding telehealth [32]; their attitudes toward the use of apps in health-related research [55]; their views on health technology more broadly [43]; and their perspectives on internet-based mental health [44], social media postings [53], and technology-based cancer support programs [45].
Table 2.
Description of each digital health intervention (N=21).
| First author, year | Type of digital intervention and mode of delivery | Intervention description | Frequency |
| Aguilera et al [34], 2014 | SMS text messaging service; mobile phone | SMS text messages as part of cognitive behavioral therapy for depression; patients received SMS text messages to aid in “homework,” consisting of monitoring of mood, thoughts, social interactions, and healthy activities | Four 4-week modules (16 weeks total) |
| Bagchi et al [35], 2018 | Videoconference consultation; computer | A research nurse transported a laptop to a housing development to collect and transmit clinical information to a nurse practitioner off-site who could review clinical data and speak with patients and the nurse via live video stream | One 6-hour consult |
| Blackwell et al [36], 2020 | SMS text messaging service; mobile phone | Text4baby—a mental health SMS text messaging service from the US Centers for Disease Control and Prevention that sends free SMS text messages to pregnant women or those with children aged <1 year providing information and reminders to improve health | 4 weeks |
| Brown et al [37], 2014 | SMS text messaging service; mobile phone | Health-promotion information in the form of text blasts or pictures sent to mothers during the first 6 months postpartum; topics included promotion of breastfeeding, information about infant immunizations, and reminders about infant and maternal follow-up and well-being | 6 months (weekly) |
| Burchert et al [38], 2019 | Internet-based intervention; computer or smartphone | SbSa—an e–mental health intervention for depression with 3 tailored components: the content (educative narratives and exercises), the guidance model (contact with a trained nonspecialist), and the delivery system (web or app) | NRb |
| Garner et al [41], 2021 | Android or iOS app; smartphone or tablet | 3D animation to teach hypertension and diabetes prevention and management; culturally tailored animated videos, short pre- and posttests, and brief educational games that included voice-over and icons | Once |
| Gesser-Edelsburg et al [20], 2017 | Web-based forum; computer | Interviews to explore attitudes about the internet as a tool for nutritional therapy interventions; all participants were members of a web-based nutrition forum receiving nutritional consultation and long-term treatment via the internet | NR |
| Johnson-Turbes et al [46], 2015 | Self-navigated website; computer | Self-navigated web-only interface with information about breast cancer grouped into an 8-section workbook presented on the site and downloadable in full or by section | NR |
| Jongbloed et al [47], 2020 | SMS text messaging service; mobile phone | Weekly SMS text messages “checking-in” for young Indigenous people who have used drugs, with follow-up support from a case manager for participants reporting a problem | NR |
| Kurth et al [30], 2016 | Internet-based intervention; computer | A computer-based counseling tool that includes audio narrated risk assessment, tailored feedback through skill-building videos, and a risk-reduction plan; on completion, participants received a printout of their tailored feedback and health-promotion plan to share with their health care provider | 45-60 minutes |
| Lindegaard et al [48], 2021 | Internet-based intervention; computer or smartphone | Individually tailored, guided ICBTc treatment that was culturally adapted for the target audience: a total of 9 treatment modules and weekly feedback on homework, modules tailored based on participants’ responses, and email contact with therapists | 8 weeks |
| Lindegaard et al [49], 2022 | Internet-based intervention; computer or smartphone | An adapted version of a previously developed ICBT intervention for adult Arabic-speaking immigrants and refugees (see Lindegaard et al [48]); this adaptation included translating all treatment materials into Dari and Farsi, simplifying the language used to make it more suitable for a young population, and adding an extra module regarding prolonged grief and separation anxiety | 8 weeks |
| Lyles et al [50], 2016 | Web-based portal; computer or smartphone | The portal allows patients access to several features: (1) viewing medical history, including visit summaries and immunizations; (2) viewing laboratory results; (3) refilling medications; (4) making appointments; and (5) sending a secure message to a health care provider | NR |
| Maertens et al [51], 2017 | Customized website; computer | Participants complete a survey, after which they are directed to customized web pages, including photographs to match demographics; prioritizing vaccine information that matches participants’ beliefs; referencing characteristics such as first name, age, and gender throughout the web pages; and using statements to reiterate participants’ stated opinions | NR |
| Ospina-Pinillos et al [54], 2019 | Internet-based intervention; computer | MHeCd for young people experiencing mental health problems; a total of 5 main elements: a home page with a triage system, a web-based physical and mental health self-report assessment, a results dashboard, a videoconferencing system, and a personalized well-being plan | NR |
| Peiris et al [31], 2019 | Android or iOS app; smartphone or tablet | Multifaceted smoking cessation app comprising a personalized profile and quit plan, motivational in-app and SMS text messages, and a challenge feature allowing users to compete with others | 3 times per user (average) |
| Povey et al [56], 2016 | Android or iOS app; smartphone or tablet | Therapist-supported mental health intervention integrating motivational interviewing and cognitive behavioral therapy techniques; the app uses colorful graphics, audio, and animation with limited text; care plans can be saved, emailed, printed, and reaccessed as an ongoing monitoring tool | NR |
| Povey et al [56], 2016 | Android or iOS app; smartphone or tablet | The i-bobbly suicide prevention app includes 3 modules; self-assessment modules ask the user if they are experiencing intrusive thoughts or thoughts of suicide; if so, they are directed to seek urgent help; activity modules use activities, stories, and videos to help users manage upsetting thoughts and emotions and set small, realistic goals | NR |
| Spanhel et al [58], 2019 | Internet-based intervention; computer or smartphone | The eSano Sleep-e intervention—3 web-based modules using text and multimedia components (images, audios, and videos) as well as reports from role models and elements such as quizzes, a sleeping diary, and homework | 3 modules (45 minutes each) |
| Tighe et al [60], 2020 | Android or iOS app; smartphone or tablet | Used the i-bobbly suicide prevention app (see Povey et al [56]) | 3 modules over 6 weeks |
| Willey et al [33], 2020 | Web-based screening survey; tablet | At the first antenatal visit, women were provided with an iPad and asked to complete the Edinburgh Postnatal Depression Scale and a psychosocial assessment; a report was sent to the women via email with their scores and links to further information; scores and reports were also available to the midwife for the consultation | One-time survey |
| Ye et al [62], 2012 | Videoconference consultation; computer | A telepsychiatrist-conducted assessment and consultation via videoconference during which a facilitator remained in the waiting room in case patients needed assistance; when the telepsychiatry session ended, the facilitator re-entered the room and received the treatment plan and instructions on medication prescribed, future appointments, and any recommended referrals or resources | Weekly (over 20 weeks) |
aSbS: step-by-step.
bNR: not reported.
cICBT: internet-based cognitive behavioral therapy.
dMHeC: mental health e-clinic.
Thematic Analysis Results
Overview
From the 34 studies analyzed, 20 descriptive themes related to barriers and facilitators were identified. From these, 7 overarching analytical themes were developed (Table 3). These were (1) using technology, (2) design components, (3) language, (4) culture, (5) health and medical, (6) trustworthiness, and (7) interaction with others. The subgroup analysis of studies conducted with First Nations or Indigenous populations identified the same descriptive and analytical themes, although the proportion of studies within each theme varied. As such, findings for all CaLD groups were combined for reporting purposes, with any differences observed for First Nations or Indigenous populations highlighted in the text.
Table 3.
Analytic and descriptive themes.
| Analytic and descriptive theme | Barriers (number of studies) | Facilitators (number of studies) | |
| Using technology | |||
|
|
Digital literacy |
|
|
|
|
Accessibility |
|
|
|
|
Interaction with digital systems | —a |
|
| Design components | |||
|
|
Content |
|
|
|
|
Delivery of information |
|
|
|
|
End-user input |
|
|
| Language | |||
|
|
Literacy in the English language |
|
|
|
|
Literacy in first language |
|
|
|
|
Preference for own language |
|
|
| Culture | |||
|
|
Cultural representation |
|
|
|
|
Cultural appropriateness |
|
|
| Health and medical | |||
|
|
Standard of care |
|
|
|
|
Health information |
|
|
|
|
Psychosocial aspects |
|
|
| Trustworthiness | |||
|
|
Privacy and confidentiality |
|
|
|
|
Information reliability |
|
|
| Interaction with others | |||
|
|
Interaction with health care providers |
|
— |
|
|
Social connectedness | — |
|
aNo barriers and facilitators for that particular theme.
Using Technology
In total, 3 descriptive themes influenced the way in which people used technology for health.
Digital Literacy
Digital literacy is defined as the skills necessary for technology use and problem-solving [63]. Core digital skills such as the ability to open an app, use SMS text messaging, or manually enter data proved challenging for many participants and, in some cases, created a reliance on others for help [39,43]. This finding was observed across all cultural groups and ages and in 38% (13/34) of the studies [30,31,34,35,38,39,42,43,50,55-57,59,61,62,64]. Other digital literacy barriers included a fear that technology is dangerous or intimidating reported by older Greek and Italian immigrants [42], Indigenous people [47], and Asian Indian immigrants [43]. Challenges with searching for credible and understandable web-based information were noted, including a self-reported lack of skills and confidence and feeling overwhelmed by the complexity of the information available [20,43,52,57].
Conversely, 9% (3/34) of the studies reported that familiarity with the use of mobile phones facilitated digital literacy [36,37,62]. Education was also mentioned as a facilitator for addressing low digital literacy, including attending classes held by ethno-specific service providers. This suggestion was reported among older African American, Hispanic, and European American individuals in the United States [39,59]; older Greek and Italian migrants in Australia [42]; younger Indigenous people in Canada [57]; and older Asian Indian immigrants in Canada [43], although the effort and cost associated with learning new skills were highlighted among the latter group.
Accessibility
Poor functionality of digital services was described as a barrier in 29% (10/34) of the studies across a range of cultural groups [30-32,35,38,39,48,49,59,62]. Specific barriers included issues with connectivity and reliability of the internet, often resulting in frustration on the part of the user. No facilitators were identified for functionality.
The cost of purchasing phones and data was also reported as a barrier to access across a range of cultural groups and ages [38,42,44,47,52,55,56,59], although 6% (2/34) of the studies identified that this could be partly outweighed by using public internet services such as those available in community libraries [40,52]. For American Indian individuals, lack of internet on reservations was also highlighted [40], and for Aboriginal Australians, DHTs were thought to be not always appropriate for people living in remote communities [56]. The cost savings associated with DHTs were seen as facilitators across most cultural groups, including fewer health care costs and less need for travel [20,32,35,38,39,44,45,47,60,62,64]. Other accessibility-related barriers reported across various cultural groups included limited user-friendly technology for older people [38,42,56] and the use of small screens or text [34,39,47]. Gender-related factors were also noted, such as domestic priorities for Asian Indian women [43] and inequities in access to technology for women refugees [44]. A total of 9% (3/34) of the studies on participants across a wide age range identified that mobile apps were more accessible than websites because of convenience and the fact that they use their phones “all day, every day” [39,50,54]. In total, 6% (2/34) of the studies noted that digital technologies could improve access to limited resources (eg, first-language therapists) [44], including for rural populations [49].
Interaction With Digital Systems
Some participants identified that talking with a computer was easier than talking to a person face to face, reporting that apps or computers are not judgmental. These studies were conducted with Aboriginal and Torres Strait Islanders [56], Mäori and Pacific Islanders [52], refugees [33], and South American migrant communities [54]. All these studies discussed user perspectives on mental health interventions. There were no reported barriers for this descriptive theme.
Design Components
Content
The importance of having engaging content was highlighted in 32% (11/34) of the studies. DHTs that were repetitive or had low visual appeal or limited interactivity were seen as frustrating or boring in 21% (7/34) of the studies that spanned all ages and cultural groups [31,33,38,41,46,59,60]. Across a range of cultural groups, participants suggested that apps could be made more engaging by incorporating games, challenges, and social elements [31,41,46,53,61], with the latter thought to also increase social connectedness among Aboriginal and Torres Strait Islanders [31]. In total, 9% (3/34) of the studies reported that the use of plain language, bullet points, and graphics would help users stay engaged with a website [40,41,53]. Incorporating a purposeful and culturally relevant storyline where individuals were virtually supported through a journey was also highlighted as important to Indigenous people in Australia [56] and the United States [53].
Having a large amount of content to read was also seen as a barrier to engagement with DHTs by younger refugees [38,58], African American individuals [46], and Asian Indian immigrants [41].
Delivery of Information
Studies among African American, Hispanic, and Latino participants identified that not being able to control the delivery of information could be frustrating, including poor timing of SMS text messages [34,55] and having little control over the amount of information provided at any one time [51]. Conversely, some participants reported the timeliness of messages as a facilitator, either as a reminder for managing health or as a motivating factor [31,34,46]. Delivery of health care or information via digital means was also thought to enable quick access, including immediate access to information and care and reducing the need to make appointments. This finding was observed across a range of cultural groups [20,35,52,56,60,64]. Convenience was also a facilitator of the uptake of DHTs, with many participants reporting less time spent in clinics and flexibility of access at a time and location to suit the end user [35-38,43,47,48].
End-User Input
Lack of end-user contribution to the design of a smoking cessation app was seen as a barrier to engagement in 3% (1/34) of the studies [31], whereas community involvement in app development was highlighted as a potential facilitator [56]. Both of these studies were conducted within Aboriginal and Torres Strait Islander communities.
Language
Literacy in the English Language
A common problem reported across many cultural groups, including refugees, was that of limited English literacy [33,36,42,46,52,54,56,57,59]. This was made more challenging by an overwhelming amount of text [38,51] and the use of complex medical terminology in some applications [30,39,48,52], including government health websites, as reported by Native American individuals [40]. Recommendations to support users with low literacy included the increased use of pictures, videos, and explanations and greater use of plain language, as reported by refugees [38,58], Indigenous people [40,56], and Asian Indian immigrants [41].
Literacy in the First Language
A total of 9% (3/34) of the studies reported that illiteracy in their own language was an issue for refugee groups [33,38,58] and Asian Indian immigrants [41]. The use of audio versions was suggested by refugees as a way of supporting access to information for people with limited ability to read in their native language [33].
Preference for Own Language
Numerous studies (10/34, 29%) across a wide range of cultural groups reported a strong preference for digital applications to be accessible in the first language of the participants [20,30,33,38,43,45,48,54,56,62] rather than in English or other dominant languages. A study on refugee Syrian women noted their praise for the use of their vernacular form of Levantine Arabic rather than formal Arabic in a mental health support app [38]. Having a clinician who spoke the patients’ own language during telehealth appointments was also thought to improve interaction with health care providers among Asian American individuals and Korean immigrants [62] and immigrants from the former Soviet Union [20]. Overall, perceptions were that this would support greater usability, including for Aboriginal and Torres Strait Islanders, who noted that this would increase their engagement with a mental health intervention [56].
Culture
Cultural Representation
Of the 34 studies, 2 (6%) conducted among refugees [38,58] and 2 (6%) conducted among Indigenous people [40,53] reported that seeing familiar, “contemporary” examples of their culture represented visually, with sensitivity and accuracy, was extremely important and influenced their desire to engage with the technology. This included using narrators from the same culture and background [38,53].
Cultural Appropriateness
Lack of recognition of cultural concerns was reported as a barrier to the use of DHTs in 15% (5/34) of the studies [30,39,45,51,58]. Of these 5 studies, 2 (40%) were conducted among Hispanic and Latino participants, and barriers included not identifying the issues faced by the community [51] and the use of culturally inappropriate questions [30]. American Indian individuals emphasized the importance of avoiding stereotyping or inaccurate portrayals of modern native people as this was seen as disrespectful [40]. The need to be aware of underlying community issues was also raised by African American participants [39]. Facilitators for cultural appropriateness included ensuring that the content and approach are relevant to the cultural community, such as using stories that reflect their experience, or ensuring that any health care providers are of the same cultural background [20,38,39,53,56,61,62]. Among refugees, the importance of avoiding the triggering of past traumas through inappropriate images (such as boats) within a DHT was highlighted, as well as understanding the restrictions of their current circumstances in being able to engage fully with an intervention [58]. A study also reported concerns about the acceptability of certain topics for refugees [48]. Cultural norms regarding electronic versus face-to-face communication were also highlighted in studies on Asian Indian immigrants [43] and Indian refugees [44], with both cultural groups noted to have a strong oral tradition.
Health and Medical
Standard of Care
There was a perception among some participants in the United States and Canada that delivery of health care via digital means led to a lower standard of care, including no opportunity for a physical assessment [32,35,44]. Conversely, several studies (4/34, 12%) across a range of cultural groups reported that the use of digital technologies allowed for an improved standard of care that was more personalized and up-to-date [45,55,56,59]. Among Alaska and Hawaiian Native participants, telehealth was thought to be improved if supported by an initial face-to-face visit with the clinician to allow for a thorough clinical assessment [32].
Health Information
Perceptions of information-based resources such as those used to promote vaccinations included an overfocus on medical information, with some African American and Hispanic and Latino participants wanting a greater focus on health and wellness [51,55] and others wanting more personalized information [39]. Both Indian-Asian migrants [43] and Korean American individuals [45] reported that web-based health information could lead to improved health.
Psychosocial Aspects
Among refugee communities, psychosocial barriers to the uptake of DHTs included existing psychological distress [38] or fatigue [58]. The risk of adverse psychological outcomes from using a DHT was also a potential barrier across several cultural groups, including becoming distressed [55,60] and feeling demotivated after receiving negative feedback from the DHT, such as automated comments appearing after failing a quiz [31,58]. Several studies (3/34, 9%) identified positive psychosocial outcomes from the use of DHTs, such as greater personal and psychological support [20,38] and increased awareness of mental health issues [54].
Trustworthiness
Privacy and Confidentiality
Privacy was both a barrier to and enabler of the use of DHTs for many cultural groups. Privacy from others when using computers or mobile phones was reported as a barrier in 15% (5/34) of the studies [33,35,44,50,55], including the need to remain private to avoid judgment from others [55]. Of note, 60% (3/5) of these studies were conducted among African American participants [35,50,55], with one author identifying that privacy is an important issue for this population [50]. Loss of privacy when using interpreters to help translate digital health information was noted to potentially lead to loss of truthfulness and avoidance of culturally taboo subjects among refugees [33]. Other participants, primarily those from Indigenous, refugee, or African American communities, felt that DHTs improved their sense of privacy and valued the anonymity they provided [30,35,47-49,52,55,56,60]. For example, Aboriginal participants in Australia expressed the idea of culturally based “shame” when addressing mental health issues inside their communities and noted the privacy that the digital app afforded [60]. Safety of personal information was also a frequently cited barrier across many cultural groups, with concerns about the trustworthiness of the technology, the risk of websites being “hacked,” and not being able to verify who is at the other end [38,39,47,52,55].
Information Reliability
Several studies (3/34, 9%) reported a lack of trust in web-based information, including in its currency and reliability [38,40,43,57]. In terms of believability, Aboriginal participants felt that a suicide prevention app’s claim of its impact was overstated [56]. A study among Hispanic and Latino participants reported that a digital health intervention to promote the uptake of the human papillomavirus vaccine provided reliable information and was similar to having access to another physician [30]. Among Korean American participants, confidence in critical appraisal skills was reported as important for judging information reliability [45].
Interaction With Others
Interaction With Health Care Providers
Across a number of cultural groups, DHTs were considered to adversely affect participant-provider interaction as they were described as being impersonal in nature, affecting communication, motivation, and understanding [35,38,44,48-50]. The DHTs discussed included videoconference consultation, mental health interventions, and a patient portal. The limited personal connection inherent in most DHTs was considered to negatively affect the ability to build good relationships with providers in 9% (3/34) of the studies [32,50,62].
Social Connectedness
This descriptive theme included 3 facilitators of the uptake of DHTs observed across a range of cultural groups. These were an increased sense of social support through web-based social interactions such as chat rooms [36,37,45]; the ability to learn from others who were experiencing the same issue [36]; and the ability to build social connections with other users [30,34,37,47,55,59,61], including through being able to reach out to others more easily, noted among First Nations, Inuit, and Métis participants [47].
Discussion
Principal Findings and Comparison With Other Studies
This study identified several analytic and descriptive themes influencing access to and uptake of DHTs among CaLD populations, including Indigenous groups. We found that cultural factors affected all the identified themes to some degree and that cultural and linguistic perspectives should be considered in the design and delivery of all DHTs, with this best served through the inclusion of the target communities at all stages of development.
The dominant analytic theme identified in this review was “Using Technology,” with accessibility and digital literacy (the skills required for technology use) being the most common barriers observed across most cultural groups. Although both factors are also noted as barriers to the uptake of DHTs among the wider population [21], this review suggests several mitigation strategies for culturally diverse populations. These include the delivery of DHTs via socially normative and familiar technologies (eg, mobile phones) and the provision of culturally tailored education programs. Improving access to free internet in public spaces (eg, community libraries) may also be a useful strategy. This access should address concerns about privacy noted among some population groups such as African American individuals [65] and also the irregular availability of public internet services [10,66]. The second most frequent analytic theme was “Language,” and for many participants across a range of cultural groups, lower literacy in English or in their own language was a barrier to the use of DHTs. This finding has also been observed in other systematic reviews [21]. The use of good health literacy principles when designing DHTs, such as plain language, limited text, clear layout, and use of appropriate images, would go some way toward addressing these language issues [24]. The delivery of content through multiple modes (audio, video, and text) could also enable users to understand basic messages without language or literacy barriers [22]. The use of vernacular languages within DHTs could also be considered as this may be more understandable to many users [67]. The theme of “Culture” identified the importance of ensuring that community sensitivities are considered and highlighted the value of seeing one’s own culture accurately represented. Although this analytic theme was less frequent than others, cultural-specific factors were noted within many other themes, such as fear of technology among Greek or Italian migrants and Indigenous people, triggering of past traumas through culturally inappropriate images for refugees, and the importance of co-design with Indigenous people. Finally, trustworthiness was also a common theme, including distrust of web-based information. There is limited literature on cultural or linguistic factors influencing trust in web-based information even in relation to the COVID-19 pandemic. Some comparative studies have suggested that cultural theories may underpin differences in trust between different populations (eg, individual vs collective societies) [68,69], whereas others report that an underlying mistrust of the medical system may also influence attitudes toward web-based health information [70,71]. This is an area requiring further research, including whether DHTs that are linguistically or culturally appropriate are seen as more trustworthy and also whether alternative strategies such as having community leaders champion the use of DHTs may be effective at enhancing cultural relevance [72].
Implications for Future Research Directions
Overall, there are considerable gaps in the evidence base for factors influencing interaction with DHTs among CaLD populations, including from the perspectives of community members [8,23,73]. This is surprising given the substantial investment in digital health in recent years [8]. These gaps include lack of evidence on health literacy and digital health literacy in CaLD populations, both of which are prerequisites for the effective use of DHTs. CaLD populations have been shown to have relatively low health literacy [74,75], whereas digital health literacy is rarely reported [23,76], although some European studies suggest it is lower among migrants and non–native language speakers [77,78]. Inadequate digital health literacy is compounded by barriers related to internet access, cultural and linguistic factors, self-efficacy in using digital technology, and concerns about privacy, all of which were factors identified in this review. Disparities in digital health literacy may lead to further widening of existing health inequalities, and there is a need to ensure that digital technologies are accessible and usable by all [10,65]. Therefore, a greater understanding of the digital health literacy needs of CaLD groups is required [23].
There are also few studies demonstrating the input of CaLD community members themselves during the development of DHTs. Participatory-based approaches such as co-design may be warranted to ensure that DHTs meet the needs of CaLD groups [79]. Co-design is a process in which targeted end users, stakeholders, and researchers work together on all aspects of intervention development, from needs assessment to content development and pilot-testing. In a recent meta-analysis, co-designed interventions were shown to have positive effects on health behaviors across multiple health conditions [80]. However, co-design of health technologies with culturally diverse groups is an emerging area [39,54,81,82], and there is little evidence on involving CaLD communities in the co-design of DHTs. A systematic review of eHealth interventions targeted at socially disadvantaged groups (including ethnic minority groups) identified that most interventions did not involve members of these communities in their development [76].
A further area for future research is understanding the factors influencing the digital divide. People from CaLD and First Nations or Indigenous communities are more likely to experience socioeconomic disadvantage [11], which will only compound many of the challenges associated with the use of DHTs identified in this review and further exacerbate the digital divide [17]. However, it is noteworthy that 15% (5/34) of the included studies highlighted participants’ motivation to engage with DHTs, including a stated willingness to improve their digital literacy skills [43]. Studies also highlighted the widespread use of mobile phones. Therefore, it is important that efforts to reduce the digital divide for CaLD populations do not just focus on access to technologies or assume a lack of motivation to adopt them. Rather, a greater focus on appropriate tailoring through understanding the cultural needs and assets within communities and then co-designing solutions is warranted [17].
Finally, it would be valuable to explore potential interactions between themes to enhance the value and effectiveness of DHTs. As noted previously, culture was a factor that influenced many of the themes identified in this study; however, the findings also suggested other interactions, such as using design elements to improve both social connectedness and engagement with content and the importance of a common language in creating positive interactions with clinicians during telehealth appointments.
Strengths and Limitations
This is the first qualitative systematic review to focus on the perspectives of CaLD populations. We used a comprehensive search strategy and a systematic, widely used method for synthesizing qualitative data. However, the limitations of this review must also be discussed. There was no consistent definition of CaLD populations in each of the reviewed articles, which might limit the generalizability and comparison of the findings [11]. The review included a broad range of cultural, linguistic, ethnic, and Indigenous groups that are heterogeneous with respect to multiple factors. Where possible, findings were reported separately to highlight barriers and facilitators unique to each population group and those that were common across several groups. Search terms for facilitators were not included. In addition, we were unable to contact the authors of the 12% (4/34) of the studies where full text was not available. As such, we may have missed some evidence in this review.
Conclusions
The combination of a health system that relies heavily on a patient’s skills in navigating the largely English-based digital system, with substantial proportions of the population for whom English is not their native language, leaves a potential gap in the ability of policy makers and health care providers to deliver health care in an equitable and effective manner. As technological innovations continue to become inseparable from health care, a greater understanding of the needs of CaLD populations will identify how digital health can be tailored to support improved health outcomes in these disadvantaged groups. The inclusion of CaLD community members in the design and development of DHTs may help ensure that cultural, linguistic, and other factors are considered and addressed from the outset. In turn, this may improve the potential of DHTs to be more acceptable, appropriate, and accessible to population groups currently at risk of not obtaining the full benefits offered by digital health.
Abbreviations
- CaLD
culturally and linguistically diverse
- DHT
digital health technology
Search terms.
Footnotes
Authors' Contributions: LW and AB conceived the study. All authors designed the study (the study protocol is available upon request). LW and AB conducted the literature searches. All authors contributed to study selection and data extraction. AB and JT conducted the quality assessments. LW and AB conducted the thematic synthesis and drafted the manuscript. All authors critically revised the manuscript and approved the final version.
Conflicts of Interest: None declared.
References
- 1.Meskó B, Drobni Z, Bényei É, Gergely B, Győrffy Z. Digital health is a cultural transformation of traditional healthcare. Mhealth. 2017;3:38. doi: 10.21037/mhealth.2017.08.07. https://europepmc.org/abstract/MED/29184890 .mh-03-2017.08.07 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Global strategy on digital health 2020-2025. World Health Organization. [2023-11-03]. https://apps.who.int/iris/handle/10665/344249 .
- 3.Kowatsch T, Otto L, Harperink S, Cotti A, Schlieter H. A design and evaluation framework for digital health interventions. Inform Technol. 2019;61(5-6):253–63. doi: 10.1515/itit-2019-0019. [DOI] [Google Scholar]
- 4.Hewitt S, Sephton R, Yeowell G. The effectiveness of digital health interventions in the management of musculoskeletal conditions: systematic literature review. J Med Internet Res. 2020 Jun 05;22(6):e15617. doi: 10.2196/15617. https://www.jmir.org/2020/6/e15617/ v22i6e15617 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Finucane AM, O'Donnell H, Lugton J, Gibson-Watt T, Swenson C, Pagliari C. Digital health interventions in palliative care: a systematic meta-review. NPJ Digit Med. 2021 Apr 06;4(1):64. doi: 10.1038/s41746-021-00430-7. doi: 10.1038/s41746-021-00430-7.10.1038/s41746-021-00430-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sasseville M, LeBlanc A, Boucher M, Dugas M, Mbemba G, Tchuente J, Chouinard M, Beaulieu M, Beaudet N, Skidmore B, Cholette P, Aspiros C, Larouche A, Chabot G, Gagnon M. Digital health interventions for the management of mental health in people with chronic diseases: a rapid review. BMJ Open. 2021 Apr 05;11(4):e044437. doi: 10.1136/bmjopen-2020-044437. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=33820786 .bmjopen-2020-044437 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jiang X, Ming W, You JH. The cost-effectiveness of digital health interventions on the management of cardiovascular diseases: systematic review. J Med Internet Res. 2019 Jun 17;21(6):e13166. doi: 10.2196/13166. https://www.jmir.org/2019/6/e13166/ v21i6e13166 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nouri S, Adler-Milstein J, Thao C, Acharya P, Barr-Walker J, Sarkar U, Lyles C. Patient characteristics associated with objective measures of digital health tool use in the United States: a literature review. J Am Med Inform Assoc. 2020 May 01;27(5):834–41. doi: 10.1093/jamia/ocaa024. https://europepmc.org/abstract/MED/32364238 .5828196 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lyles CR, Harris LT, Jordan L, Grothaus L, Wehnes L, Reid RJ, Ralston JD. Patient race/ethnicity and shared medical record use among diabetes patients. Med Care. 2012 May;50(5):434–40. doi: 10.1097/MLR.0b013e318249d81b. [DOI] [PubMed] [Google Scholar]
- 10.Veinot TC, Mitchell H, Ancker JS. Good intentions are not enough: how informatics interventions can worsen inequality. J Am Med Inform Assoc. 2018 Aug 01;25(8):1080–8. doi: 10.1093/jamia/ocy052. https://europepmc.org/abstract/MED/29788380 .4996916 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Pham TT, Berecki-Gisolf J, Clapperton A, O'Brien KS, Liu S, Gibson K. Definitions of culturally and linguistically diverse (CALD): a literature review of epidemiological research in Australia. Int J Environ Res Public Health. 2021 Jan 16;18(2):737. doi: 10.3390/ijerph18020737. https://www.mdpi.com/resolver?pii=ijerph18020737 .ijerph18020737 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mitchell UA, Chebli PG, Ruggiero L, Muramatsu N. The digital divide in health-related technology use: the significance of race/ethnicity. Gerontologist. 2019 Jan 09;59(1):6–14. doi: 10.1093/geront/gny138.5185649 [DOI] [PubMed] [Google Scholar]
- 13.Wang Y, Do DP, Wilson FA. Immigrants' use of eHealth services in the United States, national health interview survey, 2011-2015. Public Health Rep. 2018 Nov 17;133(6):677–84. doi: 10.1177/0033354918795888. https://europepmc.org/abstract/MED/30223716 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kouvonen A, Kemppainen T, Taipale S, Olakivi A, Wrede S, Kemppainen L. Health and self-perceived barriers to internet use among older migrants: a population-based study. BMC Public Health. 2022 Mar 23;22(1):574. doi: 10.1186/s12889-022-12874-x. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-022-12874-x .10.1186/s12889-022-12874-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Blackstone SR, Hauck FR. Telemedicine use in refugee primary care: implications for care beyond the COVID-19 pandemic. J Immigr Minor Health. 2022 Dec 04;24(6):1480–8. doi: 10.1007/s10903-022-01360-6. https://europepmc.org/abstract/MED/35378695 .10.1007/s10903-022-01360-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Nguyen A, Mosadeghi S, Almario CV. Persistent digital divide in access to and use of the Internet as a resource for health information: results from a California population-based study. Int J Med Inform. 2017 Jul;103:49–54. doi: 10.1016/j.ijmedinf.2017.04.008.S1386-5056(17)30086-2 [DOI] [PubMed] [Google Scholar]
- 17.Huh J, Koola J, Contreras A, Castillo AK, Ruiz M, Tedone KG, Yakuta M, Schiaffino MK. Consumer health informatics adoption among underserved populations: thinking beyond the digital divide. Yearb Med Inform. 2018 Aug;27(1):146–55. doi: 10.1055/s-0038-1641217. http://www.thieme-connect.com/DOI/DOI?10.1055/s-0038-1641217 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gordon NP, Hornbrook MC. Differences in access to and preferences for using patient portals and other eHealth technologies based on race, ethnicity, and age: a database and survey study of seniors in a large health plan. J Med Internet Res. 2016 Mar 04;18(3):e50. doi: 10.2196/jmir.5105. https://www.jmir.org/2016/3/e50/ v18i3e50 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cardona M, Fien S, Myooran J, Hunter C, Dillon A, Lewis E, Browning M, Lewis L, Ní Chróinín D. Clinical and cost-effectiveness of telehealth for Indigenous and culturally and linguistically diverse (CALD) people: a scoping review. Ethn Health. 2023 Jan;28(1):114–35. doi: 10.1080/13557858.2021.2023111. [DOI] [PubMed] [Google Scholar]
- 20.Gesser-Edelsburg A, Shalayeva S. Internet as a source of long-term and real-time professional, psychological, and nutritional treatment: a qualitative case study among former Israeli Soviet Union immigrants. J Med Internet Res. 2017 Feb 03;19(2):e33. doi: 10.2196/jmir.7130. https://www.jmir.org/2017/2/e33/ v19i2e33 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.O'Connor S, Hanlon P, O'Donnell CA, Garcia S, Glanville J, Mair FS. Understanding factors affecting patient and public engagement and recruitment to digital health interventions: a systematic review of qualitative studies. BMC Med Inform Decis Mak. 2016 Sep 15;16(1):120. doi: 10.1186/s12911-016-0359-3. https://bmcmedinformdecismak.biomedcentral.com/articles/10.1186/s12911-016-0359-3 .10.1186/s12911-016-0359-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Arsenijevic J, Tummers L, Bosma N. Adherence to electronic health tools among vulnerable groups: systematic literature review and meta-analysis. J Med Internet Res. 2020 Feb 06;22(2):e11613. doi: 10.2196/11613. https://www.jmir.org/2020/2/e11613/ v22i2e11613 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Parker S, Prince A, Thomas L, Song H, Milosevic D, Harris MF, IMPACT Study Group Electronic, mobile and telehealth tools for vulnerable patients with chronic disease: a systematic review and realist synthesis. BMJ Open. 2018 Aug 29;8(8):e019192. doi: 10.1136/bmjopen-2017-019192. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=30158214 .bmjopen-2017-019192 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Carter DD, Robinson K, Forbes J, Hayes S. Experiences of mobile health in promoting physical activity: a qualitative systematic review and meta-ethnography. PLoS One. 2018;13(12):e0208759. doi: 10.1371/journal.pone.0208759. https://dx.plos.org/10.1371/journal.pone.0208759 .PONE-D-18-20417 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Griffiths K, Coleman C, Al-Yaman F, Cunningham J, Garvey G, Whop L, Pulver LJ, Ring I, Madden R. The identification of Aboriginal and Torres Strait Islander people in official statistics and other data: critical issues of international significance. Stat J IAOS. 2019 Mar 19;35(1):91–106. doi: 10.3233/sji-180491. [DOI] [Google Scholar]
- 26.Korngiebel DM, Taualii M, Forquera R, Harris R, Buchwald D. Addressing the challenges of research with small populations. Am J Public Health. 2015 Sep;105(9):1744–7. doi: 10.2105/AJPH.2015.302783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Tong A, Flemming K, McInnes E, Oliver S, Craig J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med Res Methodol. 2012 Nov 27;12:181. doi: 10.1186/1471-2288-12-181. https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/1471-2288-12-181 .1471-2288-12-181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008 Jul 10;8:45. doi: 10.1186/1471-2288-8-45. https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/1471-2288-8-45 .1471-2288-8-45 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hong QN, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, Gagnon M, Griffiths F, Nicolau B, O'Cathain A, Rousseau M, Vedel I. Improving the content validity of the mixed methods appraisal tool: a modified e-Delphi study. J Clin Epidemiol. 2019 Jul;111:49–59.e1. doi: 10.1016/j.jclinepi.2019.03.008. https://linkinghub.elsevier.com/retrieve/pii/S0895-4356(18)30082-9 .S0895-4356(18)30082-9 [DOI] [PubMed] [Google Scholar]
- 30.Kurth AE, Chhun N, Cleland CM, Crespo-Fierro M, Parés-Avila JA, Lizcano JA, Norman RG, Shedlin MG, Johnston BE, Sharp VL. Linguistic and cultural adaptation of a computer-based counseling program (CARE+ Spanish) to support HIV treatment adherence and risk reduction for people living with HIV/AIDS: a randomized controlled trial. J Med Internet Res. 2016 Jul 13;18(7):e195. doi: 10.2196/jmir.5830. https://www.jmir.org/2016/7/e195/ v18i7e195 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Peiris D, Wright L, News M, Rogers K, Redfern J, Chow C, Thomas D. A smartphone app to assist smoking cessation among aboriginal Australians: findings from a pilot randomized controlled trial. JMIR Mhealth Uhealth. 2019 Apr 02;7(4):e12745. doi: 10.2196/12745. https://mhealth.jmir.org/2019/4/e12745/ v7i4e12745 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hiratsuka V, Delafield R, Starks H, Ambrose AJ, Mau MM. Patient and provider perspectives on using telemedicine for chronic disease management among Native Hawaiian and Alaska Native people. Int J Circumpolar Health. 2013 Aug 05;72(1):21401. doi: 10.3402/ijch.v72i0.21401. https://europepmc.org/abstract/MED/23977642 .21401 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Willey SM, Blackmore RP, Gibson-Helm ME, Ali R, Boyd LM, McBride J, Boyle JA. "If you don't ask … you don't tell": refugee women's perspectives on perinatal mental health screening. Women Birth. 2020 Sep;33(5):e429–37. doi: 10.1016/j.wombi.2019.10.003.S1871-5192(19)30223-9 [DOI] [PubMed] [Google Scholar]
- 34.Aguilera A, Berridge C. Qualitative feedback from a text messaging intervention for depression: benefits, drawbacks, and cultural differences. JMIR Mhealth Uhealth. 2014 Nov 05;2(4):e46. doi: 10.2196/mhealth.3660. http://mhealth.jmir.org/2014/4/e46/ v2i4e46 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Bagchi A, Melamed B, Yeniyurt S, Holzemer W, Reyes D. Telemedicine delivery for urban seniors with low computer literacy: a pilot study. Online J Nurs Informatics. 2018;22(2) [Google Scholar]
- 36.Blackwell TM, Dill LJ, Hoepner LA, Geer LA. Using text messaging to improve access to prenatal health information in urban African American and Afro-Caribbean immigrant pregnant women: mixed methods analysis of Text4baby usage. JMIR Mhealth Uhealth. 2020 Feb 13;8(2):e14737. doi: 10.2196/14737. https://mhealth.jmir.org/2020/2/e14737/ v8i2e14737 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Brown S, Brage Hudson D, Campbell-Grossman C, Yates BC. Health promotion text blasts for minority adolescent mothers. MCN Am J Matern Child Nurs. 2014;39(6):357–62. doi: 10.1097/NMC.0000000000000081.00005721-201411000-00004 [DOI] [PubMed] [Google Scholar]
- 38.Burchert S, Alkneme MS, Bird M, Carswell K, Cuijpers P, Hansen P, Heim E, Harper Shehadeh M, Sijbrandij M, Van't Hof E, Knaevelsrud C. User-centered app adaptation of a low-intensity e-mental health intervention for Syrian refugees. Front Psychiatry. 2018;9:663. doi: 10.3389/fpsyt.2018.00663. https://europepmc.org/abstract/MED/30740065 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Claudel SE, Ceasar JN, Andrews MR, El-Toukhy S, Farmer N, Middleton KR, Sabado-Liwag M, Mitchell VM, Tamura K, Brooks AT, Wallen GR, Powell-Wiley TM. Time to listen: a mixed-method study examining community-based views of mobile technology for interventions to promote physical activity. BMJ Health Care Inform. 2020 Aug 23;27(3):e100140. doi: 10.1136/bmjhci-2020-100140. https://informatics.bmj.com/lookup/pmidlookup?view=long&pmid=32830106 .bmjhci-2020-100140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Filippi MK, McCloskey C, Williams C, Bull JW, Choi WS, Greiner KA, Daley CM. Perceptions, barriers, and suggestions for creation of a tobacco and health website among American Indian/Alaska Native college students. J Community Health. 2013 Jun 13;38(3):486–91. doi: 10.1007/s10900-012-9634-0. https://europepmc.org/abstract/MED/23149568 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Garner SL, Wong CL, Young P, Fendt M, Hitchcock J, George CE. Mobile health to improve hypertension and diabetes health literacy among Asian Indian migrants to Hong Kong. Comput Inform Nurs. 2021 Sep 10;40(4):269–77. doi: 10.1097/CIN.0000000000000807.00024665-202204000-00009 [DOI] [PubMed] [Google Scholar]
- 42.Goodall KT, Newman LA, Ward PR. Improving access to health information for older migrants by using grounded theory and social network analysis to understand their information behaviour and digital technology use. Eur J Cancer Care (Engl) 2014 Nov;23(6):728–38. doi: 10.1111/ecc.12241. [DOI] [PubMed] [Google Scholar]
- 43.Hyman A, Stacy E, Mohsin H, Atkinson K, Stewart K, Novak Lauscher H, Ho K. Barriers and facilitators to accessing digital health tools faced by South Asian Canadians in surrey, British Columbia: community-based participatory action exploration using photovoice. J Med Internet Res. 2022 Jan 13;24(1):e25863. doi: 10.2196/25863. https://www.jmir.org/2022/1/e25863/ v24i1e25863 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hynie M, Jaimes A, Oda A, Rivest-Beauregard M, Perez Gonzalez L, Ives N, Ahmad F, Kuo BC, Arya N, Bokore N, McKenzie K. Assessing virtual mental health access for refugees during the COVID-19 pandemic using the Levesque client-centered framework: what have we learned and how will we plan for the future? Int J Environ Res Public Health. 2022 Apr 20;19(9):5001. doi: 10.3390/ijerph19095001. https://www.mdpi.com/resolver?pii=ijerph19095001 .ijerph19095001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Im E, Kim S, Jang M, Chee W. Attitudes toward technology-based cancer support programs among Korean American breast cancer survivors. West J Nurs Res. 2021 Aug;43(8):732–41. doi: 10.1177/0193945920974028. https://europepmc.org/abstract/MED/33191877 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Johnson-Turbes A, Schlueter D, Moore AR, Buchanan ND, Fairley TL. Evaluation of a web-based program for African American young breast cancer survivors. Am J Prev Med. 2015 Dec;49(6 Suppl 5):S543–9. doi: 10.1016/j.amepre.2015.09.003. https://linkinghub.elsevier.com/retrieve/pii/S0749-3797(15)00526-7 .S0749-3797(15)00526-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Jongbloed K, Pearce ME, Thomas V, Sharma R, Pooyak S, Demerais L, Lester RT, Schechter MT, Spittal PM, Cedar Project Partnership The Cedar project - mobile phone use and acceptability of mobile health among young indigenous people who have used drugs in British Columbia, Canada: mixed methods exploratory study. JMIR Mhealth Uhealth. 2020 Jul 27;8(7):e16783. doi: 10.2196/16783. https://mhealth.jmir.org/2020/7/e16783/ v8i7e16783 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Lindegaard T, Kashoush F, Holm S, Halaj A, Berg M, Andersson G. Experiences of internet-based cognitive behavioural therapy for depression and anxiety among Arabic-speaking individuals in Sweden: a qualitative study. BMC Psychiatry. 2021 Jun 03;21(1):288. doi: 10.1186/s12888-021-03297-w. https://bmcpsychiatry.biomedcentral.com/articles/10.1186/s12888-021-03297-w .10.1186/s12888-021-03297-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Lindegaard T, Wasteson E, Demetry Y, Andersson G, Richards D, Shahnavaz S. Investigating the potential of a novel internet-based cognitive behavioural intervention for Dari and Farsi speaking refugee youth: a feasibility study. Internet Interv. 2022 Apr;28:100533. doi: 10.1016/j.invent.2022.100533. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(22)00040-9 .S2214-7829(22)00040-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Lyles CR, Allen JY, Poole D, Tieu L, Kanter MH, Garrido T. "I want to keep the personal relationship with my doctor": understanding barriers to portal use among african americans and latinos. J Med Internet Res. 2016 Oct 03;18(10):e263. doi: 10.2196/jmir.5910. https://www.jmir.org/2016/10/e263/ v18i10e263 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Maertens JA, Jimenez-Zambrano AM, Albright K, Dempsey AF. Using community engagement to develop a web-based intervention for Latinos about the HPV vaccine. J Health Commun. 2017 Apr;22(4):285–93. doi: 10.1080/10810730.2016.1275890. [DOI] [PubMed] [Google Scholar]
- 52.McAra-Couper J, Gilkison A, Clemons J, Payne D, Dann L, Benn C. “I’ve done a test, what now?” A focus group study exploring eHealth access for women. New Zealand College Midwives J. 2020 Dec 01;56:5–12. doi: 10.12784/nzcomjnl56.2020.1.5-12. [DOI] [Google Scholar]
- 53.Merculieff ZT, Koller KR, Sinicrope PS, Hughes CA, Bock MJ, Decker PA, Resnicow K, Flanagan CA, Meade CD, McConnell CR, Prochaska JJ, Thomas TK, Patten CA. Developing a social media intervention to connect Alaska native people who smoke with resources and support to quit smoking: the connecting alaska native quit study. Nicotine Tob Res. 2021 May 24;23(6):1002–9. doi: 10.1093/ntr/ntaa253. https://europepmc.org/abstract/MED/33674856 .6016149 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Ospina-Pinillos L, Davenport T, Mendoza Diaz A, Navarro-Mancilla A, Scott EM, Hickie IB. Using participatory design methodologies to co-design and culturally adapt the Spanish version of the mental health eClinic: qualitative study. J Med Internet Res. 2019 Aug 02;21(8):e14127. doi: 10.2196/14127. https://www.jmir.org/2019/8/e14127/ v21i8e14127 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Pasipanodya EC, Kohli M, Fisher CB, Moore DJ, Curtis B. Perceived risks and amelioration of harm in research using mobile technology to support antiretroviral therapy adherence in the context of methamphetamine use: a focus group study among minorities living with HIV. Harm Reduct J. 2020 Jun 11;17(1):41. doi: 10.1186/s12954-020-00384-1. https://harmreductionjournal.biomedcentral.com/articles/10.1186/s12954-020-00384-1 .10.1186/s12954-020-00384-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Povey J, Mills PP, Dingwall KM, Lowell A, Singer J, Rotumah D, Bennett-Levy J, Nagel T. Acceptability of mental health apps for Aboriginal and Torres Strait Islander Australians: a qualitative study. J Med Internet Res. 2016 Mar 11;18(3):e65. doi: 10.2196/jmir.5314. https://www.jmir.org/2016/3/e65/ v18i3e65 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Rempel E, Donelle L, Kothari A. Exploring the health literacy of First Nations young adult women. J Commun Healthcare. 2016 Jan 14;9(1):11–21. doi: 10.1080/17538068.2015.1122873. [DOI] [Google Scholar]
- 58.Spanhel K, Schweizer JS, Wirsching D, Lehr D, Baumeister H, Bengel J, Sander L. Cultural adaptation of internet interventions for refugees: results from a user experience study in Germany. Internet Interv. 2019 Dec;18:100252. doi: 10.1016/j.invent.2019.100252. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(19)30012-0 .S2214-7829(19)30012-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Tappen RM, Cooley ME, Luckmann R, Panday S. Digital health information disparities in older adults: a mixed methods study. J Racial Ethn Health Disparities. 2022 Feb;9(1):82–92. doi: 10.1007/s40615-020-00931-3. https://europepmc.org/abstract/MED/33415705 .10.1007/s40615-020-00931-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Tighe J, Shand F, McKay K, Mcalister T, Mackinnon A, Christensen H. Usage and acceptability of the iBobbly app: pilot trial for suicide prevention in Aboriginal and Torres Strait Islander youth. JMIR Ment Health. 2020 Dec 01;7(12):e14296. doi: 10.2196/14296. https://mental.jmir.org/2020/12/e14296/ v7i12e14296 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Wan N, Wen M, Fan JX, Tavake-Pasi OF, McCormick S, Elliott K, Nicolosi E. Physical activity barriers and facilitators among US Pacific Islanders and the feasibility of using mobile technologies for intervention: a focus group study with Tongan Americans. J Phys Act Health. 2018 Apr 01;15(4):287–94. doi: 10.1123/jpah.2017-0014. [DOI] [PubMed] [Google Scholar]
- 62.Ye J, Shim R, Lukaszewski T, Yun K, Kim SH, Ruth G. Telepsychiatry services for Korean immigrants. Telemed J E Health. 2012 Dec;18(10):797–802. doi: 10.1089/tmj.2012.0041. https://europepmc.org/abstract/MED/23234426 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Norgaard O, Furstrand D, Klokker L, Karnoe KA, Batterham R, Kayser L. The e-health literacy framework: a conceptual framework for characterizing e-health users and their interaction with e-health systems. Knowl Manage E-learning. 2015;7(4):522–40. doi: 10.34105/j.kmel.2015.07.035. [DOI] [Google Scholar]
- 64.Ghaddar S, Vatcheva KP, Alvarado SG, Mykyta L. Understanding the intention to use telehealth services in underserved hispanic border communities: cross-sectional study. J Med Internet Res. 2020 Sep 03;22(9):e21012. doi: 10.2196/21012. https://www.jmir.org/2020/9/e21012/ v22i9e21012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Sieck CJ, Sheon A, Ancker JS, Castek J, Callahan B, Siefer A. Digital inclusion as a social determinant of health. NPJ Digit Med. 2021 Mar 17;4(1):52. doi: 10.1038/s41746-021-00413-8. doi: 10.1038/s41746-021-00413-8.10.1038/s41746-021-00413-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Medero K, Merrill K, Ross MQ. Modeling access across the digital divide for intersectional groups seeking web-based health information: national survey. J Med Internet Res. 2022 Mar 15;24(3):e32678. doi: 10.2196/32678. https://www.jmir.org/2022/3/e32678/ v24i3e32678 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Sibuyi I, de la Harpe R, Nyasulu P. A stakeholder-centered mHealth implementation inquiry within the digital health innovation ecosystem in South Africa: MomConnect as a demonstration case. JMIR Mhealth Uhealth. 2022 Jun 16;10(6):e18188. doi: 10.2196/18188. https://mhealth.jmir.org/2022/6/e18188/ v10i6e18188 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Song H, Omori K, Kim J, Tenzek KE, Morey Hawkins J, Lin W, Kim Y, Jung J. Trusting social media as a source of health information: online surveys comparing the United States, Korea, and Hong Kong. J Med Internet Res. 2016 Mar 14;18(3):e25. doi: 10.2196/jmir.4193. https://www.jmir.org/2016/3/e25/ v18i3e25 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Khosrowjerdi M. National culture and trust in online health information. J Librarianship Inform Sci. 2019 Mar 26;52(2):509–28. doi: 10.1177/0961000619836716. [DOI] [Google Scholar]
- 70.Harris M, Ekwonye A, Munala L, Buesseler H, Hearst MO. Exploring knowledge, prevention methods, and prevention barriers of COVID-19 among Somali, Karen, and Latinx community members in Minneapolis, Minnesota, USA. J Prim Care Community Health. 2021;12:21501327211056595. doi: 10.1177/21501327211056595. https://journals.sagepub.com/doi/abs/10.1177/21501327211056595?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Yashadhana A, Fields T, Blitner G, Stanley R, Zwi AB. Trust, culture and communication: determinants of eye health and care among Indigenous people with diabetes in Australia. BMJ Glob Health. 2020 Jan 09;5(1):e001999. doi: 10.1136/bmjgh-2019-001999. https://gh.bmj.com/lookup/pmidlookup?view=long&pmid=32133172 .bmjgh-2019-001999 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Community champions a rapid scoping review of community champion approaches for the pandemic response and recovery. Public Health England. [2022-11-03]. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1011854/A_rapid_scoping_review_of_community_champion_approaches_for_the_pandemic_response_and_recovery_V8.pdf .
- 73.Patel S, Akhtar A, Malins S, Wright N, Rowley E, Young E, Sampson S, Morriss R. The acceptability and usability of digital health interventions for adults with depression, anxiety, and somatoform disorders: qualitative systematic review and meta-synthesis. J Med Internet Res. 2020 Jul 06;22(7):e16228. doi: 10.2196/16228. https://www.jmir.org/2020/7/e16228/ v22i7e16228 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Rheault H, Coyer F, Jones L, Bonner A. Health literacy in Indigenous people with chronic disease living in remote Australia. BMC Health Serv Res. 2019 Jul 26;19(1):523. doi: 10.1186/s12913-019-4335-3. https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-019-4335-3 .10.1186/s12913-019-4335-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Beauchamp A, Buchbinder R, Dodson S, Batterham RW, Elsworth GR, McPhee C, Sparkes L, Hawkins M, Osborne RH. Distribution of health literacy strengths and weaknesses across socio-demographic groups: a cross-sectional survey using the Health Literacy Questionnaire (HLQ) BMC Public Health. 2015 Jul 21;15(1):678. doi: 10.1186/s12889-015-2056-z. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-015-2056-z .10.1186/s12889-015-2056-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Cheng C, Beauchamp A, Elsworth GR, Osborne RH. Applying the electronic health literacy lens: systematic review of electronic health interventions targeted at socially disadvantaged groups. J Med Internet Res. 2020 Aug 13;22(8):e18476. doi: 10.2196/18476. https://www.jmir.org/2020/8/e18476/ v22i8e18476 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Bergman L, Nilsson U, Dahlberg K, Jaensson M, Wångdahl J. Health literacy and e-health literacy among Arabic-speaking migrants in Sweden: a cross-sectional study. BMC Public Health. 2021 Nov 25;21(1):2165. doi: 10.1186/s12889-021-12187-5. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-021-12187-5 .10.1186/s12889-021-12187-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Villadsen SF, Hadi H, Ismail I, Osborne RH, Ekstrøm CT, Kayser L. ehealth literacy and health literacy among immigrants and their descendants compared with women of Danish origin: a cross-sectional study using a multidimensional approach among pregnant women. BMJ Open. 2020 May 07;10(5):e037076. doi: 10.1136/bmjopen-2020-037076. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=32385065 .bmjopen-2020-037076 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Peeters G, Barker AL, Talevski J, Ackerman I, Ayton DR, Reid C, Evans SM, Stoelwinder JU, McNeil JJ. Do patients have a say? A narrative review of the development of patient-reported outcome measures used in elective procedures for coronary revascularisation. Qual Life Res. 2018 May 29;27(5):1369–80. doi: 10.1007/s11136-018-1795-6.10.1007/s11136-018-1795-6 [DOI] [PubMed] [Google Scholar]
- 80.Halvorsrud K, Kucharska J, Adlington K, Rüdell K, Brown Hajdukova E, Nazroo J, Haarmans M, Rhodes J, Bhui K. Identifying evidence of effectiveness in the co-creation of research: a systematic review and meta-analysis of the international healthcare literature. J Public Health (Oxf) 2021 Apr 12;43(1):197–208. doi: 10.1093/pubmed/fdz126. https://europepmc.org/abstract/MED/31608396 .5585850 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Chauhan A, Leefe J, Shé ÉN, Harrison R. Optimising co-design with ethnic minority consumers. Int J Equity Health. 2021 Nov 04;20(1):240. doi: 10.1186/s12939-021-01579-z. https://equityhealthj.biomedcentral.com/articles/10.1186/s12939-021-01579-z .10.1186/s12939-021-01579-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.O'Brien J, Fossey E, Palmer V. A scoping review of the use of co-design methods with culturally and linguistically diverse communities to improve or adapt mental health services. Health Soc Care Community. 2021 Jan;29(1):1–17. doi: 10.1111/hsc.13105. doi: 10.1111/hsc.13105. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Search terms.