

Abstract
There is growing recognition that engaging men in maternal, infant and young child nutrition (MIYCN) interventions can benefit child health and disrupt harmful gender norms. We conducted a cluster‐randomized controlled trial in Tanzania, which engaged men and women in behaviour change via mobile messaging (short message service [SMS]) and traditional interpersonal communication (IPC), separately and in combination. Here, we evaluate intervention effects on individual‐level men's MIYCN knowledge and discuss barriers to male engagement. Eligible clusters were dispensary catchment areas with >3000 residents. Forty clusters were stratified by population size and randomly allocated to the four study arms, with 10 clusters per arm. Data on knowledge and intervention exposure were collected from 1394 men through baseline and endline surveys (March–April 2018 and July–September 2019). A process evaluation conducted partway through the 15–18‐month intervention period included focus group discussions and interviews. Data were analysed for key trends and themes using Stata and ATLAS.ti software. Male participants in the short message service + interpersonal communication (SMS + IPC) group reported higher exposure to IPC discussions than IPC‐only men (43.8% and 21.9%, respectively). Knowledge scores increased significantly across all three intervention groups, with the greatest impact in the SMS + IPC group. Qualitative findings indicated that the main barriers to male participation were a lack of interest in health/nutrition and perceptions that these topics were a woman's responsibility. Other challenges included meeting logistics, prioritizing income‐earning activities and insufficient efforts to engage men. The use of a combined approach fusing IPC with SMS is promising, yet countering gender norms and encouraging stronger male engagement may require additional strategies.
Keywords: behaviour, health promotion, infant and child nutrition, International Child Health Nutrition, low‐income countries, qualitative methods
We conducted a cluster‐randomized controlled trial in rural Tanzania with four study arms, which received the following maternal, infant and young child nutrition (MIYCN) behaviour change interventions: a short message service text messaging intervention, traditional interpersonal communication, a combination of both interventions and a control arm; both men and women were recruited. Baseline and endline surveys demonstrated that male participants had moderate exposure to the interventions and that men's MIYCN knowledge increased significantly across all three arms, with the greatest impact in the combined intervention group. Qualitative data collected during a mid‐point process evaluation revealed that the main barriers to male participation were a lack of interest in health/nutrition, perceptions that such topics were a woman's responsibility and prioritization of income‐earning activities.
Key messages
Men's nutrition knowledge improved significantly more among those enrolled in a combined intervention strategy leveraging both traditional interpersonal communication (IPC) and a short message service text‐messaging intervention, as compared with those receiving either strategy alone.
Concurrent enrollment in a low‐intensity intervention leveraging technology may heighten men's motivation to engage in activities surrounding maternal and child nutrition.
The greatest barriers to male participation in IPC activities were perceptions that health and nutrition topics were a woman's responsibility and men's prioritization of income‐generating work over attending group discussions.
Gender‐transformative approaches that actively seek to shift social norms may enable greater male engagement in targeted nutrition interventions.
1. INTRODUCTION
Despite considerable progress, parts of Africa remain off course to reach targets for reducing child malnutrition—including stunting, wasting and overweight (Development Initiatives, 2020). This persistent burden is particularly troublesome because childhood undernutrition can be prevented with well‐known actions, such as exclusive breastfeeding and improved complementary feeding (Bhutta et al., 2013; Keats et al., 2021). Such actions have long been promoted by development interventions and health services, with interventions such as health worker visits and community support groups shown to be effective at improving children's diet quality and growth (Janmohamed et al., 2020).
These interventions are based on the understanding that women's knowledge and behaviour are essential for improving child nutrition and that women's empowerment plays a potentially important (although not always straightforward) role in influencing nutrition practices and outcomes (Malapit & Quisumbing, 2015; Malapit et al., 2015; Pratley, 2016; Quisumbing, Sproule, et al., 2021; Santoso et al., 2019; Shroff et al., 2011). Mothers and mothers‐to‐be are thus their main target. Recognition is growing, however, that engaging mothers alone is insufficient—both to improve nutrition and to support women's empowerment and gender role transformation (Ambikapathi et al., 2021; USAID Advancing Nutrition, 2020). Men currently often play a limited direct role in childcare and feeding—generally seen as a woman's responsibility—particularly in low‐ and middle‐income countries (LMICs). However, it has been well documented that fathers influence household nutrition and infant and young child feeding (IYCF) practices, such as breastfeeding (Bar‐Yam & Darby, 1997; Mukuria et al., 2016; Ochieng et al., 2017; Pelto & Armar‐Klemesu, 2015). Men's nutrition knowledge is associated with children's dietary outcomes (Ambikapathi et al., 2021; Bilal et al., 2016), and men often play a large role in shaping decision‐making, food choices and time availability within a household (Kuyper & Dewey, 2012). Moreover, women's large work burden and reduced leisure time, due to having near‐full responsibility for childcare and feeding, can be considered aspects of disempowerment (Alkire et al., 2013). Women's empowerment cannot be achieved without men's equitable contributions, especially in their roles as fathers (Engle, 1997).
Engaging men in child nutrition interventions could thus have many benefits, such as improving knowledge and skills of both caregivers, potentially reducing women's burden of care work, increasing women's social support within the household and improving men's ability to bond with and support their child and partner (Kuyper & Dewey, 2012). It could also have larger social benefits by helping question and dispel gender norms about masculinity and men's and women's roles in childcare—whereas programmes that engage only with women risk inadvertently reinforcing gender norms of child feeding and nutrition being ‘women's work’ (Muraya et al., 2017). Recent global recommendations thus argue for including fathers and other key family members in maternal, infant and young child nutrition (MIYCN) programmes (World Health Organization, 2018).
Currently, there is limited evidence of specific intervention approaches that can reach men with child nutrition programming and of the barriers to and enablers of men's participation. For example, a 2019 review of women's empowerment and child nutrition found that a few of the 62 identified studies even included indicators for men's engagement in childcare and nutrition (Santoso et al., 2019). A 2020 systematic review of behavioural interventions to engage family members in MIYCN in LMICs identified just 25 studies, of which most were focused on fathers and on breastfeeding (Martin et al., 2020). While these mainly reported positive results on topics such as knowledge and practices, the review also concluded that many studies had weak research designs, such as nonrandomization. Moreover, most approaches studied are ‘traditional’ community‐based interventions, such as discussion groups and home visits. There has been less focus on engaging men through more novel means that may be better aligned with their behaviours and preferences, like through mobile phones. In the review by Martin et al. (2020), for example, only one study included mobile messaging (Ke et al., 2018). Yet, there is growing interest in increasing the coverage and inclusiveness of nutrition interventions more broadly through mobile phone‐based approaches (Cole‐Lewis & Kershaw, 2010; Free et al., 2013; Heidkamp et al., 2021; Higgs et al., 2014). These might hold particular promise for men, who in East Africa are more likely than women to have access to high‐quality mobile phones (GSMA, 2021) and have been found receptive to such approaches for related topics, such as family planning (Harrington et al., 2019).
This paper adds to this small but growing literature with evidence of the potential of an intervention combining mobile messaging with interpersonal communication approaches with the aim of improving men's knowledge of MIYCN in rural Tanzania. We combine quantitative data from a cluster‐randomized controlled study (cRCT) with qualitative data to discuss not only the results but also the barriers to uptake and lessons learned from implementation, drawing implications for future interventions.
2. METHODS
2.1. Study design and setting
This study draws on data collected during a trial to compare the effectiveness of two nutrition behaviour change interventions, separately and in combination, on MIYCN knowledge and practices. The study design has been described previously (Rothstein et al., 2021). The 2 × 2 factorial, cRCT had four study arms that received the following interventions: (i) interpersonal communication (referred to as ‘IPC arm’); (ii) SMS text messaging (SMS); (iii) a combination of both interventions (SMS + IPC); and (iv) usual care without any special intervention (Control). In this setting, men are encouraged to attend antenatal care visits at public health dispensaries with their pregnant partners, yet usual care does not involve any MIYCN messaging addressed to men. Primary participants were pregnant women and mothers of children <12 months at enrollment; male household members were also enrolled when possible.
A cRCT (as opposed to an RCT) was chosen as certain IPC interventions were implemented at the community, as opposed to individual, level. Randomization took place at the level of public health dispensary catchment areas (DCAs); of all 53 public DCAs in the two study districts (ranging in population size from 987 to 21,264), DCAs with <3000 residents (n = 11) were excluded to maximize data collection efficiency. One DCA was also excluded because it contained a large health centre, unrepresentative of normal health service access. From the remaining DCAs, one was randomly selected and excluded to produce 10 DCAs per study arm (40 total DCAs). These DCAs were stratified by population size into >10,000, 4800–10,000 and <4800. Within each stratum, DCAs were randomly allocated to one of four study arms using random number generation by the study PI. Thus, each study arm contained two large‐, three small‐ and five medium‐sized DCAs. All DCAs within each study arm received the same set of interventions, described below, and all were included in the analysis.
Data were collected during three periods. Baseline questionnaires were administered following participant recruitment, before intervention implementation (March–April 2018), and endline questionnaires were administered following the intervention (July–September 2019); these data were used for the quantitative impact evaluation. The intervention period ranged from 15 to 18 months depending on the exact timing of recruitment and data collection for each participating household. In addition, partway through the intervention period (April 2019), a qualitative process evaluation, which included focus group discussions (FGDs) and in‐depth interviews (IDIs), was conducted among a subsample of participants to explore factors affecting implementation.
The study took place in Mtwara, a rural, agricultural region in southern Tanzania that has historically lacked access to health and nutrition projects. Regional young child nutrition indicators are worse than national averages; for example, only 19.9% of children 6–23 months in Mtwara consume the minimal meal frequency, as compared with 39.9% countrywide, and stunting among children under five is 37.7% in Mtwara versus 34.4% nationally (Ministry of Health, 2016). Two districts, Newala and Tandahimba, were selected in Mtwara as they were most representative of rural Tanzania and had no prior exposure to MIYCN interventions.
2.2. Participants and sample selection
The sample size (2400 total, with 600 per arm) was based on the study's primary outcomes (minimum dietary diversity of women and children), aiming to discern a 10% or greater difference based on a baseline prevalence of 50%, accepting a Type 1 (α) error and power (1 − b) of 80%, a design effect of 1.3 for cluster randomization (with an average cluster size of 60) and a 10% loss to follow‐up.
Study participants were recruited through door‐to‐door screening, with a complete enrollment of eligible persons. The husband/male partner of each eligible woman (pregnant woman or mother of a child <12 months) was enrolled if they were available and consented. If the head of the household was a man other than the woman's partner, this person was eligible to serve as the male participant if the partner was not available. Upon study enrollment, male participants were asked to consent to be enrolled in the free Wazazi Nipendeni service (SMS/SMS + IPC arms) or be contacted by a community health worker (CHW; IPC/SMS + IPC arms). For consenting participants in SMS arms, study personnel registered participants’ and other household members’ phones, as allowed, with the Wazazi Nipendeni service immediately after data collection; SMS were expected to begin soon thereafter. For participants assigned to the IPC intervention, activities were initiated within 3 months of baseline.
Study households were revisited during endline data collection, and male participants were interviewed if available. In addition, men who were not assessed at baseline but were identified as the partner of a female participant and/or head of household at endline were also eligible to be interviewed at endline; this was done to increase the sample size of men available for analysis. This was the only change to the study design made after trial commencement. Study recruitment and baseline occurred from March to April 2018, and the endline was completed from July to September 2019.
Full details on the process evaluation methods are provided elsewhere (Rothstein et al., 2021). Briefly, for IDIs, participants were recruited from villages in SMS and SMS + IPC arms, as the primary objective of IDIs was to understand participants’ experiences of receiving SMS. Men were eligible to participate if they owned a registered phone and had received at least one Wazazi Nipendeni SMS. IDI participants were randomly selected from a list of participants surveyed during the process evaluation. For the FGDs, three villages were identified that had relatively high rates of male participation in IPC meetings (‘active’ villages) and three villages with relatively low male participation rates (‘inactive’ villages), based on monitoring data; this sampling frame was used because the primary objective of the FGDs was to explore barriers to men's participation in the IPC intervention. Men residing within those villages were eligible to participate in FGDs if they had enrolled in the study and provided consent to be visited by a CHW.
2.3. Intervention design
The IPC intervention consisted of regular group discussions (cluster level) and home visits (individual level) by CHWs to educate participants on MIYCN using the government‐sponsored Mkoba wa Siku 1000 (‘1000 Days Initiative’) programme. During monthly meetings, CHWs played recorded messages and discussed recommended health and nutrition practices using a radio and counselling cards; all messages were targeted to a specific life stage. The original goal was to hold separate women's and men's groups, led by the same CHWs. During implementation, the make‐up of the groups differed across communities based on participation levels: five villages had separate men's groups, 12 villages had mixed‐gender groups and in seven villages, men did not participate at all. Individualized home visits, which happened once every 2 months, were intended to identify and address barriers to recommended practices, reinforce adoption and identify high‐risk women and children.
The project drew on existing female and male CHWs, with additional CHWs selected where needed. CHWs underwent 2 weeks of training before implementation, received monthly supervision thereafter and participated in quarterly meetings with all project CHWs to share experiences. They received job aids, such as bicycles and rainboots, as incentives but were not paid.
Among households assigned to the SMS and SMS + IPC arms, male and female participants’ mobile phones that were successfully enrolled in the Wazazi Nipendeni service received SMS free of charge with health and nutrition information and life stage‐timed reminders, from pregnancy through the child's fifth year. Registrants could identify themselves as pregnant women, new mothers or supporters (family, friends). Messages covered nutrition, such as breastfeeding and incorporating protein into child diets, and other health topics like child vaccinations. Message frequency varied by month and declined over time, from an average of 4.9 messages/month during pregnancy and the child's first year of life to an average of 1.25 messages/month sent during the child's fifth year.
2.4. Data collection
2.4.1. Baseline and endline surveys
Surveys were conducted in Swahili by a team of trained and experienced data collectors. Data were recorded on tablets and stored on an online server. Upon study enrollment, a survey was completed with the household head or most senior member available to collect sociodemographic, asset, infrastructure and dietary data using questions adapted from Tanzania's Demographic Health Survey and Malaria Indicatory Survey and an International Food Policy Research Institute (IFPRI) study of the same SMS programme in Tanzania (IFPRI, 2020; Ministry of Health, 2016). Food insecurity was assessed through USAID's Household Food Insecurity Access Scale (Coates et al., 2007). A separate survey was administered to the male participant to assess intervention exposure, IYCF knowledge (through 18 multiple‐choice questions) and mobile phone usage; these questions were developed by the research team. These same questions were administered to men at endline, along with a module exploring men's perceptions of the intervention(s).
2.4.2. FGDs (process evaluation)
FGDs were facilitated by two local interns familiar with Mkoba wa Siku 1000 and loosely structured by a discussion guide. FGDs explored men's level of interest in child health and nutrition topics, barriers to participation in IPC activities and suggestions for how to better engage men. Those who had attended meetings and/or interacted with a CHW during the study period were asked to describe their reactions to the content and impressions of the CHW. FGDs were held in a neutral community location and audio‐recorded.
2.4.3. IDIs (process evaluation)
Issues surrounding male participation in IPC activities were explored through IDIs to ascertain individuals’ perspectives outside of a group context and in more villages. IDIs were conducted by data collectors using semistructured guides that included questions similar to those of the FGDs, took place in a private location and were audio‐recorded.
2.5. Data analysis
From the cRCT data, our outcome of interest was individual‐level men's nutrition and health knowledge; this was a secondary outcome of the study, for which the primary outcomes were maternal and child dietary diversity. From the qualitative data, we sought to understand barriers and facilitators to engaging men in behaviour change communication on nutrition topics.
2.5.1. Statistical analyses
Quantitative data were analysed using Stata SE15 (StataCorp). Percentages and mean/standard deviation were generated for categorical and continuous variables, respectively. Baseline characteristics of households and men were compared across arms using one‐way analysis of variance for continuous variables and χ 2 tests for categorical variables. Variables with significant differences (p ≤ 0.05) across arms were adjusted for in multivariate models assessing programme effects.
Exposure to the IPC intervention was measured by participation in a group meeting and receipt of a home visit by a CHW for nutrition counselling over the previous 12 months and frequency of these activities over prior 12‐ and 3‐month periods. Exposure to the SMS intervention was assessed through Wazazi Nipendeni enrollment, ever receiving a Wazazi Nipendeni SMS or SMS with health and nutrition information, and the number of SMS received in the prior 30 days.
Analysis of impact measures only considered observations with data from both baseline and endline. Men's nutrition knowledge scores were based on 14 questions after four of the original survey questions were excluded from analysis due to uncertain validity. The remaining questions were categorized into three areas—breastfeeding, child feeding and micronutrients, and hygiene (Supporting Information: Table 1). Participants received one point for each correct response, resulting in three area scores, and a total score was calculated as a sum of these scores (range: 0–14); these scores were then normalized (to 0–1 each) for further analysis.
The effect size for men's knowledge was estimated using mixed‐effects linear regression models. Using baseline and endline data, changes in knowledge scores within a given study arm were examined and compared with the control group change in the intervention period. In mixed‐effects models, the random‐effect component included indicators to control for clustering at individual and village levels. The fixed component included the study arm, time of survey (baseline = 0; endline = 1) and an arm–time interaction term. Clustering at the village level was adjusted for; the adjusted models included four variables that differed across groups at baseline (religion, drinking water source, type of toilet facility and garden ownership). The treatment effect and associated p value were derived using contrasts of average marginal effect.
2.5.2. Qualitative data analyses
Audio recordings from the FGDs were used to complement the detailed notes taken during each discussion, which were then translated into English. IDI recordings were transcribed verbatim by native Swahili speakers and simultaneously translated into English. Deductive and inductive codes were then applied to the transcripts using ATLAS.ti qualitative management software (Scientific Software Development) by the first author.
Following procedures for content analysis developed by Hsieh and Shannon (2005), codes were organized into categories, subthemes and then broader themes (Hsieh & Shannon, 2005). The first author sought feedback on initial interpretations from the data collectors, strengthening the trustworthiness of the findings.
2.6. Ethical approval
Ethical approval was obtained from Tanzania's National Institute for Medical Research (NIMR/HQ/R.8a/Vol.IX/2684). Written informed consent was obtained from all male and female participants before enrolment, with separate consent for audio recording where relevant. The cRCT was registered on ClinicalTrials.gov (NCT03297190).
3. RESULTS
3.1. Intervention impact
Baseline characteristics are given in Table 1. A total of 1442 men completed the baseline survey; of these, 394 were not included at endline (primarily due to moving, travel or not being located) and 347 men who were not assessed at baseline but were a father of an index child or household leader at endline were included (Figure 1). The total sample size was thus 1394. There were no notable sociodemographic differences among the three groups of men (data not shown).
Table 1.
Characteristics of households and men at baseline
| Characteristics | Total | Control | SMS only | IPC only | SMS+ IPC | p Valuea |
|---|---|---|---|---|---|---|
| Maximum n | N = 1442 | N = 373 | N = 346 | N = 378 | N = 345 | |
| Household size, mean (SD) | 4.4 (1.7) | 4.3 (1.7) | 4.4 (1.8) | 4.5 (1.8) | 4.6 (1.7) | 0.20 |
| Religion, n (%) | ||||||
| Muslim | 1403 (97.4) | 351 (94.1) | 341 (98.6) | 367 (97.4) | 344 (99.7) | 0.001 |
| Christian | 38 (2.6) | 22 (5.9) | 5 (1.5) | 10 (2.6) | 1 (0.3) | |
| Education of household head, n (%) | ||||||
| No education | 177 (12.3) | 44 (11.8) | 44 (12.7) | 50 (13.3) | 39 (11.3) | 0.99 |
| Primary school incomplete | 125 (8.7) | 31 (8.3) | 34 (9.8) | 33 (8.8) | 27 (78) | |
| Primary school complete | 996 (69.1) | 262 (70.2) | 233 (67.3) | 259 (68.7) | 242 (70.1) | |
| Secondary school complete or higher | 143 (9.9) | 36 (9.7) | 35 (10.1) | 35 (9.3) | 37 (10.7) | |
| Source of drinking water, n (%) | ||||||
| Unimproved | 772 (53.6) | 207 (55.5) | 167 (48.3) | 215 (57.0) | 183 (53.0) | 0.097 |
| Improved | 669 (46.4) | 166 (44.5) | 179 (51.7) | 162 (43.0) | 162 (47.0) | |
| Sanitation facilities, n (%) | ||||||
| Unimproved | 1197 (83.1) | 322 (86.3) | 276 (79.8) | 306 (81.2) | 293 (84.9) | 0.063 |
| Improved | 244 (16.9) | 51 (13.7) | 70 (20.2) | 71 (18.8) | 52 (15.1) | |
| Wealth, n (%) | ||||||
| Lowest quintile | 239 (16.9) | 80 (21.8) | 46 (13.7) | 65 (17.5) | 48 (14.1) | 0.017 |
| Second quintile | 199 (14.1) | 52 (14.2) | 54 (16.1) | 55 (14.8) | 38 (11.1) | |
| Third quintile | 487 (34.4) | 112 (30.5) | 116 (34.6) | 119 (32.1) | 140 (41.1) | |
| Fourth quintile | 449 (31.8) | 112 (30.5) | 111 (33.1) | 116 (31.3) | 110 (32.3) | |
| Fifth quintile | 40 (2.8) | 11 (3.0) | 8 (2.4) | 16 (4.3) | 5 (1.5) | |
| Electricity, n (%) | ||||||
| Yes | 1207 (83.8) | 310 (83.1) | 295 (85.3) | 316 (83.8) | 286 (82.9) | 0.83 |
| No | 234 (16.2) | 63 (16.9) | 51 (14.7) | 61 (16.2) | 59 (17.1) | |
| Owned/had access to the home garden, n (%) | 888 (61.6) | 235 (63.0) | 215 (62.1) | 242 (64.2) | 196 (56.8) | 0.19 |
| Owned land where vegetables or fruit is grown in the past 12 months, n (%) | 771 (53.5) | 194 (52.0) | 184 (53.2) | 199 (52.8) | 194 (56.2) | 0.69 |
| Access to cow or goat in the past 12 months, n (%) | 169 (11.7) | 47 9 (12.6) | 27 (7.8) | 58 (15.4) | 37 (10.8) | 0.014 |
| Household Food Insecurity Access Scale, n (%) | ||||||
| Food secure | 827 (57.4) | 203 (54.4) | 211 (61.0) | 202 (53.4) | 211 (61.2) | 0.003 |
| Mildly food insecure | 112 (7.8) | 34 (9.1) | 28 (8.1) | 40 (10.6) | 10 (2.9) | |
| Moderately food insecure | 311 (21.6) | 80 (21.4) | 73 (21.1) | 77 (20.4) | 81 (23.5) | |
| Severely food insecure | 192 (13.3) | 56 (15.0) | 34 (9.8) | 59 (15.6) | 43 (12.5) |
Abbreviations: IPC, interpersonal communication; SMS, short message service.
Comparability across groups was tested by one‐way analysis of variance for continuous variables and by χ 2 test for categorical variables. p < 0.05.
Figure 1.
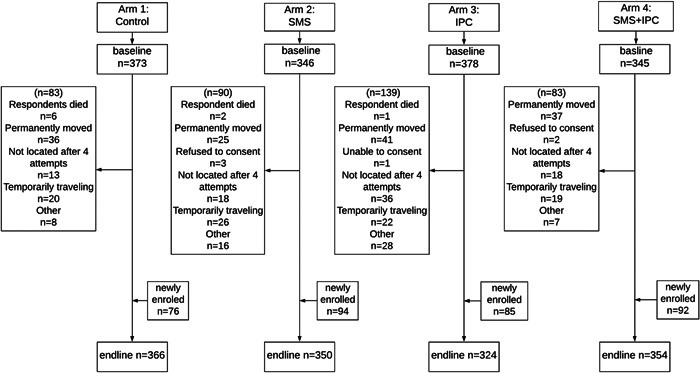
Study flow of male participants in the quantitative survey. IPC, interpersonal communication; SMS, short message service.
Table 2 summarizes intervention exposure. Among the 82.4%–91.1% of men with access to a mobile phone, the proportion receiving health/nutrition text messages in the past 2 years was 43.4% in the SMS and 35.9% in the SMS + IPC groups, versus 12.8% in the control and 13.3% in IPC group. Rates were similar for Wazazi Nipendeni, specifically. About 21% in SMS groups (vs. <5% in non‐SMS groups) had received at least one message in the past month. Overall, SMS exposure was similar between SMS and SMS + IPC groups.
Table 2.
Intervention exposures among men (n = 1394)
| Characteristics | Control | SMS only | IPC only | SMS + IPC | p Valuea |
|---|---|---|---|---|---|
| Maximum n | n = 366 | n = 350 | n = 324 | n = 354 | |
| Mobile phone and SMS exposure | |||||
| Has access to a working mobile phone (including own phone) | 313 (85.5) | 319 (91.1) | 267 (82.4) | 307 (86.7) | 0.010 |
| Received phone messages with information about health and nutrition in the past 2 years (among men who had access to working phones) | 47 (12.8) | 152 (43.4) | 43 (13.3) | 127 (35.9) | <0.001 |
| Enrolled in the WN programme | 38 (10.4) | 133 (38.0) | 33 (10.2) | 115 (32.5) | <0.001 |
| Received WN messages in the past 2 years | 36 (9.8) | 130 (37.1) | 32 (9.9) | 115 (32.5) | <0.001 |
| Number of WN messages received in the past 30 days | |||||
| None | 351 (95.0) | 271 (77.4) | 311 (96.0) | 284 (80.2) | <0.001 |
| 1 or 2 messages | 4 (1.1) | 16 (4.6) | 4 (1.2) | 15 (4.2) | |
| 3–10 messages | 9 (2.5) | 42 (12.0) | 9 (2.8) | 31 (8.8) | |
| >10 messages | 1 (0.3) | 14 (4.0) | 0 (0.0) | 22 (6.2) | |
| Don't know | 1 (0.3) | 7 (2.0) | 0 (0.0) | 2 (0.6) |
| IPC | |||||
|---|---|---|---|---|---|
| In the past 12 months, have you participated in any group discussions, trainings or meetings on a topic related to the nutrition or health of you or your child? | 1 (0.3) | 5 (1.4) | 71 (21.9) | 155 (43.8) | <0.001 |
| Participated in IPC meeting in the past 12 months | 0 (0.0) | 0 (0.0) | 71 (21.9) | 146 (41.2) | <0.001 |
| Last time participated in the IPC meeting | |||||
|---|---|---|---|---|---|
| Within the past month | 0 | 0 | 9 (2.8) | 17 (4.8) | <0.001 |
| In the prior month | 0 | 0 | 14 (4.3) | 30 (8.5) | |
| About 3 months ago | 0 | 0 | 13 (4.0) | 26 (7.3) | |
| 4–5 months ago | 0 | 0 | 7 (2.2) | 18 (5.1) | |
| More than 5 months ago | 0 | 0 | 23 (7.1) | 44 (12.4) | |
| Don't know | 0 | 0 | 5 (1.5) | 11 (3.1) | |
| Never | 366 (100) | 350 (99.8) | 253 (78.1) | 208 (58.8) | |
| In the past 12 months, has anyone come by your house to discuss with you a topic related to the nutrition or health of you or your child? | 0 | 0 | 134 (41.4) | 198 (55.9) | <0.001 |
| How many times in the past 12 months has this happened? | |||||
| Never | 366 (100.0) | 350 (100.0) | 190 (58.6) | 156 (44.1) | <0.001 |
| 1–5 times | 0 (0.0) | 0 (0.0) | 88 (27.2) | 99 (28.0) | |
| 6 or more times | 0 (0.0) | 0 (0.0) | 34 (10.5) | 78 (22.0) | |
| Don't know | 0 (0.0) | 0 (0.0) | 12 (3.7) | 21 (5.9) | |
| Person who conducted a home visit | |||||
| CHW | 0 (0.0) | 0 (0.0) | 132 (40.7) | 191 (54.0) | <0.001 |
| Others | 0 (0.0) | 0 (0.0) | 1 (0.3) | 5 (1.4) | |
| Never | 366 (100) | 350 (100) | 191 (59.0) | 158 (44.6) | |
Abbreviation: CHW, community health worker; IPC, interpersonal communication; SMS, short message service; WN, wazazi nipendeni.
Comparability across groups was tested by one‐way analysis of variance for continuous variables and by χ 2 test for categorical variables.
Regarding IPC, the proportion of men participating in any group discussions or meetings on nutrition or health in the previous 12 months was 21.9% in the IPC group and 43.8% in the SMS + IPC group, with similar results when asked specifically about Mkoba wa Siku. This was significantly lower than for women, who showed participation rates of 84.1%–94.1%. Nutrition‐related home visits in the past 12 months were reported by 41.4% of men in the IPC group and 55.9% in the SMS + IPC group. No men in the control or SMS‐only groups reported participation in meetings or home visits. Overall, IPC exposure was stronger in the SMS + IPC group than in the IPC group.
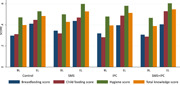
At baseline, average scores for breastfeeding, child feeding/micronutrients, hygiene and total knowledge were comparable across the four groups (p > 0.05) (Supporting Information: Table 2). Each knowledge score showed an increasing trend from baseline to endline across all groups (Table 3 and Supporting Information: Figure 1). None of the three intervention groups showed a significant difference in the breastfeeding knowledge score compared with the control group (all p > 0.05), but differences were found for all other scores. The child feeding/micronutrient scores were 0.048 and 0.090 points higher in the IPC and SMS + IPC groups, respectively, compared with the control group (p < 0.05). The hygiene score was 0.052, 0.065 and 0.073 points higher in the SMS, IPC and SMS + IPC groups, respectively, compared with the control group (p < 0.05). Likewise, the total knowledge score was 0.030, 0.039 and 0.066 points higher in the SMS, IPC and SMS + IPC groups, respectively, compared with the control group (p < 0.05).
Table 3.
Programme effect on men's nutrition knowledge score, using endline data only
| Characteristics | Control | SMS | IPC | SMS + IPC |
|---|---|---|---|---|
| Maximum n | 366 | 350 | 324 | 354 |
| Breastfeeding score, mean (SD) | 0.41 (0.20) | 0.43 (0.22) | 0.39 (0.21) | 0.40 (0.21) |
| Unadjusted β | – | 0.02 | −0.02 | −0.01 |
| p Value | – | 0.21 | 0.30 | 0.50 |
| Adjusted β a | 0.02 | −0.01 | −0.01 | |
| p Valueb | – | 0.17 | 0.61 | 0.64 |
| Child feeding and micronutrient score, mean (SD) | 0.44 (0.22) | 0.45 (0.21) | 0.49 (0.24) | 0.53 (0.22) |
| Unadjusted β | – | 0.01 | 0.05 | 0.09 |
| p Value | – | 0.69 | 0.02 | <0.001 |
| Adjusted β | – | 0.01 | 0.05 | 0.09 |
| p Value | – | 0.58 | 0.03 | <0.001 |
| Hygiene score, mean (SD) | 0.52 (0.28) | 0.57 (0.28) | 0.58 (0.27) | 0.59 (0.27) |
| Unadjusted β | – | 0.05 | 0.07 | 0.07 |
| p Value | – | 0.03 | 0.001 | <0.001 |
| Adjusted β | – | 0.05 | 0.07 | 0.07 |
| p Value | – | 0.02 | 0.001 | <0.001 |
| Total knowledge score, mean (SD) | 0.48 (0.19) | 0.50 (0.21) | 0.51 (0.20) | 0.54 (0.19) |
| Unadjusted β | – | 0.03 | 0.04 | 0.06 |
| p Value | 0.05 | 0.04 | <0.001 | |
| Adjusted β | 0.03 | 0.04 | 0.07 | |
| p Value | – | 0.02 | 0.04 | <0.001 |
Abbreviations: CI, confidence interval; IPC, interpersonal communication; SMS, short message service.
Mixed‐effects models included a fixed part (intervention group, time of survey visit, interaction term between intervention group and time of survey visit) and a random part (village and individual clustering), adjusted by religion, type of drinking water sources, type of toilet facilities and garden ownership.
Treatment effect (95% CI) and p value of treatment effect derived using contrasts of average marginal effect.
The interventions thus significantly increased men's knowledge, with the largest impact seen for the SMS + IPC group. The effect magnitude corresponds to men in the SMS + IPC group responding correctly to about one additional question, relative to the control group. As a robustness check, we undertook a similar analysis using the longitudinal sample of 1033 men assessed at both baseline and endline (Supporting Information: Table 3); while this rendered some effects for the SMS‐ and IPC‐only groups insignificant, there were few qualitative differences.
3.2. Men's impressions of the IPC intervention
Men who participated in meetings and home visits generally viewed them positively. Of the 217 men who reported having participated in meetings at endline (71 from IPC arm, 146 from SMS + IPC arm), the most widely cited reasons for attendance were an interest in learning about child health and nutrition (78.3%), wanting their child to be healthy (28.1%) and having been told to attend (24.4%) (Supporting Information: Table 4). The overwhelming majority of attendees viewed the meetings as useful, relevant, clear and a source of new information (Supporting Information: Table 4).
The IDIs and FGDs shed light on the types of knowledge acquired through the meetings. Participants mentioned learning specific skills, such as using peanuts to create nutritious porridge and constructing homemade hand‐washing stations. In addition, participants recalled learning general guidelines, such as the importance of helping their spouses with domestic work and seeking antenatal care. Although not all information was novel, the IPC meetings served to underscore the messages’ relevance.
This issue of breastfeeding a baby for six months—we have been hearing that [since a] long time ago, but we didn't know its importance before attending these classes. Formerly we took it for granted. (28‐year‐old male participant)
Participants also expressed appreciation for opportunities to learn from others during meetings, and a few mentioned noticing changes in their children's health and alertness since the intervention began.
Nearly all endline survey participants who attended meetings reported approving of their CHW's facilitation style (Supporting Information: Table 4). These perceptions were reflected in the qualitative data, as IDI and FGD participants spoke of the CHWs’ expertise and credibility. One 27‐year‐old man commented, ‘I always like it because these people are well informed. They have been educated, so when they come and tell me, they open my mind’.
Attendees’ main critiques of the IPC intervention involved the meetings’ length—more than one‐third agreed they were too long—and the fact that recommended practices were not always feasible to implement (23.0%), largely due to financial constraints and the lack of affordability of certain recommended foods, including animal products (Table 4). Some men preferred home visits over group meetings as the visits offered a private setting for asking questions and receiving personalized guidance.
3.3. Barriers to male engagement
Several factors contributed to poor engagement among the 461 men from IPC and SMS + IPC arms who reported having never attended a meeting. The main reason cited was a lack of interest in the topics discussed (44.0%) (Supporting Information: Table 5). Qualitative data suggested that this disinterest was related to the perception that child health and nutrition did not pertain to men. For example, one interview participant who had previously attended meetings explained,
I think those men lack adequate education and understanding of what needs to be done… Some men may question, ‘why should I attend those meetings?’ Some say, ‘what for?’… Some men say a woman is the one who is supposed to attend because she is a mother of a child. (37‐year‐old male participant)
Logistical issues also played a role in limiting men's participation: 42.1% and 16.5% of nonattendees reported the meeting location and timing, respectively, were inconvenient. Men's economic responsibilities were an additional limiting factor, as 14.1% of nonattendees reported they were unable to attend meetings due to farming or other work responsibilities. These economic concerns affected the value some men saw in the meetings.
The financial situation has been difficult. So, if you tell a man to go and attend the meeting, he thinks he is wasting his time… So, if the chance presented itself, someone will say, ‘Let me go and work to earn some income. Therefore…at least I can buy some maize flour, which will be prepared for my children to eat.’ (42‐year‐old male participant)
Finally, several men cited issues related to information dissemination from CHWs. Some FGD participants in ‘inactive’ villages explained feeling as though health and nutrition information from CHWs was directed towards women, which made them ‘feel inferior’. Others perceived that CHWs gave IPC meeting invitations exclusively to women.
3.4. Recommendations for increasing male engagement
FGD and IDI participants shared several ideas for encouraging their attendance at meetings. Participants requested more practical lessons such as cooking demonstrations—for example, how to incorporate all food groups into children's meals—in place of broader conceptual learning. Some men also suggested using more props such as cards and boards to make topics easier to understand and remember, rather than relying solely on the Mkoba wa Siku radio. In several FGDs, men agreed that incorporating other topics would make the meetings more appealing; they frequently mentioned an interest in learning about agricultural issues, managing money and ways to improve living standards.
Regarding logistical issues, several participants said they would be more likely to attend meetings if they occurred at a different time. One IDI participant suggested the meetings be held on Friday mornings before mosque, as men are certain to be home at that time. Several IDI participants suggested using rewards or gifts, such as clothing or hats, to motivate attendance.
I suggest if there is a possibility of impressing people, even for a small extent…. if they know something will be provided as a reward for the attendees, they will attend and the message you intended will be conveyed to them. (30‐year‐old male participant)
Finally, participants made several recommendations surrounding how to publicize the meetings. FGD participants from two villages suggested that CHWs intensify their efforts to recruit men directly, rather than simply focusing on women. One suggestion was for CHWs to discuss the meetings with men during social gatherings, such as when they are drinking coffee or playing games in the village centre. Men also recommended that CHWs work with local leaders and other respected individuals like village elders to make public announcements about meeting times and purpose. Several participants suggested village leaders attend meetings themselves to demonstrate their importance.
4. DISCUSSION
In this study, we employed mixed methods to evaluate the impact of two intervention strategies on men's MIYCN knowledge, while also describing lessons learned through efforts to engage men in intervention programming. By comparing baseline and endline measures, we demonstrated that IPC and SMS behaviour change interventions, alone and in combination, led to significant improvements in men's health/nutrition knowledge, among all intervention groups as compared with the control group. In each knowledge domain, the combined SMS + IPC group exhibited the greatest increases in knowledge, followed by the IPC group, supporting an initial hypothesis that intervention impact would be related to increasing intervention intensity. Given that nutrition‐ and health‐related knowledge are widely viewed as fundamental for behaviour change, and that men's roles in supporting MIYCN are increasingly recognized as essential, the results suggest engaging men in behaviour change communication can be an important step in improving MIYCN.
Study findings also indicate the numerous challenges to motivating and sustaining men's participation in nutrition interventions and the importance of incorporating a gender‐sensitive or gender‐transformative approach in intervention content and delivery. Participants’ perceptions that child health and nutrition issues did not concern them were the greatest impediment to male engagement, echoing findings from elsewhere in East and West Africa (Flax et al., 2019; Isler et al., 2020; Muraya et al., 2017). The coinciding sociocultural norms of men's disinterest in nutrition and their control over household finances and decision‐making threaten to compromise the impact of nutrition interventions—particularly those which require shifts in finance‐related household decisions, such as purchasing or cultivating more nutrient‐dense foods for young children. In our study, results from ‘inactive’ villages suggested the CHWs’ communication may have unintentionally reinforced perceived gender norms, as men often thought they were not invited to meetings or that CHWs were only concerned with women. In other contexts, certain aspects of intervention design may also reinforce these norms. For example, in a project promoting the adoption of orange sweet potato crops in Uganda, nutrition trainings were targeted exclusively towards women; this may have limited programme effectiveness given the importance of joint decision‐making around uses of household land (Gilligan et al., 2020).
To counter such norms, it may be necessary to intensify involvement of (male) village leaders and other authority figures in publicizing intervention activities open to men. This strategy proved effective in the context of a reproductive, maternal, newborn and child health intervention in rural Kenya, which found that men responded more positively to messaging from church leaders, teachers and other respected individuals (Lusambili et al., 2021). Larger community events that bring together leaders, CHWs and community members may also play an important role in shifting perceptions that MIYCN is solely a woman's responsibility. In addition, deploying male CHWs to engage with men directly may prove to be a culturally acceptable approach to recruiting larger numbers of male participants for IPC interventions. While our study involved both male and female CHWs, we did not analyse rates of male engagement based on CHW gender or other characteristics; future research should explore such factors to better understand the potential benefits of recruiting and training male CHWs. Another strategy involves providing nutrition trainings to groups of husbands and wives together. In Bangladesh, Quisumbing, Ahmed et al. (2021) found that such trainings improved empowerment scores and gender attitudes among both men and women, suggesting that this model may help men recognize and value women's responsibilities. The authors posit that the trainings may have been particularly impactful for men if they were previously less involved in their children's health and nutrition (Quisumbing, Ahmed, et al., 2021).
Nevertheless, addressing the underlying norms that limit men's participation in MIYCN activities will likely require moving beyond gender‐sensitive approaches towards gender‐transformative approaches that actively seek to shift social norms (Gender Practitioners Collaborative, 2018). One approach for doing so is community champions: identifying men or couples who are particularly open‐minded about gender norms and engaging them to serve as role models and change agents for others (Nutrition International, 2019). In Senegal, for example, USAID's SPRING project provided potentially effective couples with training that involved deconstructing gender roles, discussing gender equity and advocacy (USAID, 2017). Other approaches (such as the one used in Bangladesh, above) use group‐based curricula directed at men and women throughout the community, integrating nutrition messaging alongside gender‐transformative content (HKI, 2015). By contributing to shifts in gender norms, such approaches may facilitate men's engagement in more targeted nutrition interventions.
Economic factors also impeded men's engagement in IPC activities, as many study participants prioritized income‐generating work over spending time in a meeting. This is consistent with other studies from the region demonstrating that contributing financially to one's family took precedent over attendance at scheduled activities (Lusambili et al., 2021). These findings suggest that intervention activities would be more appealing to men if associated with economic well‐being by, for example, emphasizing how the household's financial stability could improve if women and children are healthier.
The tension between men's economic responsibilities and meeting attendance underscores the importance of carefully timing IPC activities according to men's availability. In our study population, male attendance was affected by logistical challenges to a far greater extent than for women: in the endline survey, only 10.1% and 10.7% of women cited the meeting location and timing as a reason for nonattendance, respectively, as compared with 42.1% and 16.5% of men. Home visits may be more convenient than group discussions for men, as visits can be tailored to each individual's schedule and do not require travelling. Furthermore, home visits allow men to ask questions specifically related to their circumstances, while potentially avoiding the social stigma associated with being a man interested in ‘female’ topics like child nutrition. Formative research plays a critical role in designing gender‐sensitive interventions that consider such factors, yet it has been underutilized to date (Yourkavitch et al., 2017). Future efforts can aim to establish more inclusive procedures, such as easily accessible locations and convenient schedules, centred on engaging men in a sustainable way.
Study findings also suggest that one mechanism for increasing male attendance at CHW‐led meetings is concurrent enrollment in a low‐intensity intervention leveraging technology. While 21.9% of male participants enrolled in the IPC arm reported participating in IPC meetings, 43.8% of men in the SMS + IPC arm did. Exposure to Wazazi Nipendeni SMS seems to have heightened men's interest in health and nutrition, or made them view such topics as more relevant, and thus motivated them to attend meetings. This likely occurred because Wazazi Nipendeni leveraged a channel—the mobile phone—which men used widely and viewed positively, and because the SMS enabled more frequent communication.
Participants also suggested integrating topics related to men's economic interests and concerns, rather than focusing exclusively on health‐related issues. For example, nutrition messages could be presented alongside training in agriculture or other livelihoods. Several nongovernmental organizations have achieved this by integrating health education into farmers’ groups (Yourkavitch et al., 2017). Indeed, such combined messaging directed at women is common in nutrition‐sensitive agriculture interventions (Nordhagen et al., 2019; Ruel et al., 2018), and research in Bangladesh shows that integrated nutrition‐sensitive agriculture approaches that address men and women jointly can increase the empowerment of both men and women and have potentially positive effects on nutrition (Quisumbing, Ahmed, et al., 2021). Strategies like these would prove more sustainable than providing gifts to men to incentivize attendance.
4.1. Limitations
This study faced several limitations. It focused on only one region of rural Tanzania, and results should be generalized with caution. Second, we did not limit participation to phone owners, out of concerns for bias and equity, but the inclusion of nonphone owners may have limited the potential effect that could be achieved via SMS. Third, our outcome measures include only men's knowledge, not their behaviours. Fourth, qualitative data were collected cross‐sectionally mid‐intervention and thus may have been subject to recall bias or not captured factors that became relevant later in implementation. Nevertheless, triangulation across IDIs, FGDs and surveys allowed for a comprehensive understanding of the factors influencing male engagement and lends credibility to the analysis (Creswell et al., 2011). Fifth, we faced some attrition of men between baseline and endline and included a set of men at endline who were not assessed at baseline, which may have introduced bias. Similarly, due to attrition and nonavailability of men, as well as the relatively small number of clusters included, we were somewhat underpowered for detecting differences in outcomes. Finally, the qualitative methods used relatively small sample sizes, limiting their generalizability, but recruiting participants from ‘active’ and ‘inactive’ villages helped account for diverse perspectives.
5. CONCLUSIONS
Despite these limitations, this study provides evidence of the impact of a novel SMS + IPC intervention on men's nutrition knowledge, as well as key barriers and potential enablers to achieving men's full participation. With heightened global focus on male engagement in nutrition interventions, identifying which strategies are most effective remains a critical question. In‐depth evaluations of interventions that engage men are necessary to deepen understanding of how content, delivery mechanisms and intersectoral efforts translate to improved women's and children's dietary patterns and health. Our findings indicate that a combined strategy, fusing traditional IPC with text messaging, is promising but that additional interventions are likely needed to more directly address gender norms that constrain men's engagement in MIYCN.
AUTHOR CONTRIBUTIONS
Stella Nordhagen, Rolf D. W. Klemm, Erin Smith and Jessica D. Rothstein designed the study. Jessica D. Rothstein and Stella Nordhagen led the drafting of the manuscript. Jessica D. Rothstein oversaw data collection and qualitative data analysis. Yunhee Kang analysed the quantitative data. Debora Niyeha oversaw field implementation. All authors read and approved the final manuscript.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
Supporting information
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
ACKNOWLEDGEMENTS
We wish to acknowledge the Tanzania Ministry of Health Community Development Gender Elderly and Children, especially the Mtwara Regional office and Newala and Tandahimba District Offices, for their support during the intervention. The authors also acknowledge the staff at Tanzania Food and Nutrition Centre of the Ministry of Health Community Development Gender Elderly and Children, especially Sikitu Simon, for their collaboration on this study as well as the National Bureau of Statistics for their support. Special thanks to Dr. Jennifer Nielsen (Helen Keller International, New York) who led initial formative research to design the intervention, Tiransia Soo (Helen Keller International, Tanzania) who oversaw baseline and endline data collection, Joyceline Kaganda (Tanzania Food and Nutrition Center, Save the Children Tanzania) who served as an investigator on the RCT and Chytanya Kompala (Eleanor Crook Foundation) for guidance and feedback throughout the study. Finally, we wish to acknowledge the CHWs, mothers, fathers and children who participated in the study. This research was funded by the Eleanor Crook Foundation (grant number 66450).
Rothstein, J. D. , Klemm, R. D. W. , Kang, Y. , Niyeha, D. , Smith, E. , & Nordhagen, S. (2023). Engaging men in maternal, infant and young child nutrition in rural Tanzania: Outcomes from a cluster randomized control trial and qualitative study. Maternal & Child Nutrition, 19, e13460. 10.1111/mcn.13460
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Alkire, S. , Meinzen‐Dick, R. , Peterman, A. , Quisumbing, A. , Seymour, G. , & Vaz, A. (2013). The women's empowerment in agriculture index. World Development, 52, 71–91. 10.1016/j.worlddev.2013.06.007 [DOI] [Google Scholar]
- Ambikapathi, R. , Passarelli, S. , Madzorera, I. , Canavan, C. R. , Noor, R. A. , Abdelmenan, S. , Tewahido, D. , Tadesse, A. W. , Sibanda, L. , Sibanda, S. , Munthali, B. , Madzivhandila, T. , Berhane, Y. , Fawzi, W. , & Gunaratna, N. S. (2021). Men's nutrition knowledge is important for women's and children's nutrition in Ethiopia. Maternal & Child Nutrition, 17(1), e13062. 10.1111/mcn.13062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bar‐Yam, N. B. , & Darby, L. (1997). Fathers and breastfeeding: A review of the literature. Journal of Human Lactation, 13(1), 45–50. 10.1177/089033449701300116 [DOI] [PubMed] [Google Scholar]
- Bhutta, Z. A. , Das, J. K. , Rizvi, A. , Gaffey, M. F. , Walker, N. , Horton, S. , Lartey, A. , & Black, R. E. , The Maternal and Child Nutrition Study Group . (2013). Evidence‐based interventions for improvement of maternal and child nutrition: What can be done and at what cost. The Lancet, 382(9890), 452–477. 10.1016/S0140-6736(13)60996-4 [DOI] [PubMed] [Google Scholar]
- Bilal, S. M. , Dinant, G. , Blanco, R. , Crutzen, R. , Mulugeta, A. , & Spigt, M. (2016). The influence of father's child feeding knowledge and practices on children's dietary diversity: A study in urban and rural districts of Northern Ethiopia, 2013: Children's dietary diversity. Maternal & Child Nutrition, 12(3), 473–483. 10.1111/mcn.12157 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coates, J. , Swindale, A. , & Bilinsky, P. (2007). Household food insecurity access scale (HFIAS) for measurement of food access: Indicator guide (version 3). Food and Nutrition Technical Assistance Project, Academy for Educational Development. [Google Scholar]
- Cole‐Lewis, H. , & Kershaw, T. (2010). Text messaging as a tool for behavior change in disease prevention and management. Epidemiologic Reviews, 32, 56–69. 10.1093/epirev/mxq004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Creswell, J. W. , Klassen, A. C. , & Plano Clark, V. L. (2011). Best practices for mixed methods research in the health sciences. National Institutes of Health, Office of Behavioral and Social Sciences Research. [Google Scholar]
- Development Initiatives . (2020). 2020 Global Nutrition Report: Action on equity to end malnutrition. https://globalnutritionreport.org/reports/2020-global-nutrition-report/
- Engle, P. L. (1997). The role of men in families: Achieving gender equity and supporting children. Gender & Development, 5(2), 31–40. 10.1080/741922351 [DOI] [PubMed] [Google Scholar]
- Flax, V. L. , Chapola, J. , Mokiwa, L. , Mofolo, I. , Swira, H. , Hosseinipour, M. C. , & Maman, S. (2019). Infant and young child feeding learning sessions during savings groups are feasible and acceptable for HIV‐positive and HIV‐negative women in Malawi. Maternal & Child Nutrition, 15(3), e12765. 10.1111/mcn.12765 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Free, C. , Phillips, G. , Galli, L. , Watson, L. , Felix, L. , Edwards, P. , Patel, V. , & Haines, A. (2013). The effectiveness of mobile‐health technology‐based health behaviour change or disease management interventions for health care consumers: A systematic review. PLoS Medicine, 10(1), e1001362. 10.1371/journal.pmed.1001362 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gender Practitioners Collaborative . (2018). Minimum standards for mainstreaming gender equality. https://dldocs.mercycorps.org/MinimumStandardsMainstreamingGenderEquality.pdf.
- Gilligan, D. O. , Kumar, N. , McNiven, S. , Meenakshi, J. V. , & Quisumbing, A. (2020). Bargaining power, decision making, and biofortification: The role of gender in adoption of orange sweet potato in Uganda. Food Policy, 95, 101909. 10.1016/j.foodpol.2020.101909 [DOI] [PMC free article] [PubMed] [Google Scholar]
- GSMA . (2021). Connected women—The Mobile Gender Gap Report 2021. https://www.gsma.com/r/wp-content/uploads/2021/07/The-Mobile-Gender-Gap-Report-2021.pdf [Google Scholar]
- Harrington, E. K. , McCoy, E. E. , Drake, A. L. , Matemo, D. , John‐Stewart, G. , Kinuthia, J. , & Unger, J. A. (2019). Engaging men in an mHealth approach to support postpartum family planning among couples in Kenya: A qualitative study. Reproductive Health, 16(1), 17. 10.1186/s12978-019-0669-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heidkamp, R. A. , Piwoz, E. , Gillespie, S. , Keats, E. C. , D'Alimonte, M. R. , Menon, P. , Das, J. K. , Flory, A. , Clift, J. W. , Ruel, M. T. , Vosti, S. , Akuoku, J. K. , & Bhutta, Z. A. (2021). Mobilising evidence, data, and resources to achieve global maternal and child undernutrition targets and the sustainable development goals: An agenda for action. The Lancet, 397(10282), 1400–1418. 10.1016/S0140-6736(21)00568-7 [DOI] [PubMed] [Google Scholar]
- Helen Keller International (HKI) . (2015). Nurturing connections—Adapted for homestead food production and nutrition. https://fr.fsnnetwork.org/resource/nurturing-connections-adapted-homestead-food-production-and-nutrition [Google Scholar]
- Higgs, E. S. , Goldberg, A. B. , Labrique, A. B. , Cook, S. H. , Schmid, C. , Cole, C. F. , & Obregón, R. A. (2014). Understanding the role of mHealth and other media interventions for behavior change to enhance child survival and development in low‐ and middle‐income countries: An evidence review. Journal of Health Communication, 19(Suppl 1), 164–189. 10.1080/10810730.2014.929763 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hsieh, H. F. , & Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qualitative Health Research, 15(9), 1277–1288. 10.1177/1049732305276687 [DOI] [PubMed] [Google Scholar]
- International Food Policy Research Institute (IFPRI) . (2020). mNutrition Tanzania baseline study. https://www.ifpri.org/publication/mnutrition-tanzania-baseline-study [Google Scholar]
- Isler, J. , Sawadogo, N. H. , Harling, G. , Bärnighausen, T. , Adam, M. , Sié, A. , & McMahon, S. A. (2020). ‘If he sees it with his own eyes, he will understand’: How gender informed the content and delivery of a maternal nutrition intervention in Burkina Faso. Health Policy and Planning, 35(5), 536–545. 10.1093/heapol/czaa012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Janmohamed, A. , Sohani, N. , Lassi, Z. , & Bhutta, Z. (2020). The effects of community home visit and peer group nutrition intervention delivery platforms on nutrition outcomes in low and middle‐income countries: A systematic review and meta‐analysis. Nutrients, 12(2), 440. 10.3390/nu12020440 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ke, J. , Ouyang, Y. Q. , & Redding, S. R. (2018). Family‐centered breastfeeding education to promote primiparas' exclusive breastfeeding in China. Journal of Human Lactation, 34(2), 365–378. 10.1177/0890334417737293 [DOI] [PubMed] [Google Scholar]
- Keats, E. C. , Das, J. K. , Salam, R. A. , Lassi, Z. S. , Imdad, A. , Black, R. E. , & Bhutta, Z. A. (2021). Effective interventions to address maternal and child malnutrition: An update of the evidence. The Lancet Child & Adolescent Health, 5(5), 367–384. 10.1016/S2352-4642(20)30274-1 [DOI] [PubMed] [Google Scholar]
- Kuyper, E. M. , & Dewey, K. (2012). Literature review: Fathers support infant and young child feeding: Their contributions to better outcome. Alive & Thrive. https://www.aliveandthrive.org/sites/default/files/attachments/Literature-Reivew-Dads.pdf [Google Scholar]
- Lusambili, A. M. , Muriuki, P. , Wisofschi, S. , Shumba, C. S. , Mantel, M. , Obure, J. , Nyaga, L. , Mulama, K. , Ngugi, A. , Orwa, J. , Luchters, S. , & Temmerman, M. (2021). Male involvement in reproductive and maternal and new child health: An evaluative qualitative study on facilitators and barriers from rural Kenya. Frontiers in Public Health, 9, 644293. 10.3389/fpubh.2021.644293 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malapit, H. J. L. , Kadiyala, S. , Quisumbing, A. R. , Cunningham, K. , & Tyagi, P. (2015). Women's empowerment mitigates the negative effects of low production diversity on maternal and child nutrition in Nepal. The Journal of Development Studies, 51(8), 1097–1123. 10.1080/00220388.2015.1018904 [DOI] [Google Scholar]
- Malapit, H. J. L. , & Quisumbing, A. R. (2015). What dimensions of women's empowerment in agriculture matter for nutrition in Ghana? Food Policy, 52, 54–63. 10.1016/j.foodpol.2015.02.003 [DOI] [Google Scholar]
- Martin, S. L. , McCann, J. K. , Gascoigne, E. , Allotey, D. , Fundira, D. , & Dickin, K. L. (2020). Mixed‐methods systematic review of behavioral interventions in low‐ and middle‐income countries to increase family support for maternal, infant, and young child nutrition during the first 1000 days. Current Developments in Nutrition, 4(6), nzaa085. 10.1093/cdn/nzaa085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) [Tanzania Mainland], Ministry of Health (MoH) [Zanzibar], National Bureau of Statistics (NBS), Office of the Chief Government Statistician (OCGS), and ICF . (2016). Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS‐MIS) 2015–16. [Google Scholar]
- Mukuria, A. G. , Martin, S. L. , Egondi, T. , Bingham, A. , & Thuita, F. M. (2016). Role of social support in improving infant feeding practices in Western Kenya: A quasi‐experimental study. Global Health: Science and Practice, 4(1), 55–72. 10.9745/GHSP-D-15-00197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muraya, K. W. , Jones, C. , Berkley, J. A. , & Molyneux, S. (2017). “If it's issues to do with nutritionaI can decide…”: Gin rural coastal Kenya. Health Policy and Planning, 32(Suppl_5), v31–v39. 10.1093/heapol/czx032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nordhagen, S. , Nielsen, J. , van Mourik, T. , Smith, E. , & Klemm, R. (2019). Fostering CHANGE: Lessons from implementing a multi‐country, multi‐sector nutrition‐sensitive agriculture project. Evaluation and Program Planning, 77, 101695. 10.1016/j.evalprogplan.2019.101695 [DOI] [PubMed] [Google Scholar]
- Nutrition International . (2019). Engaging men and boys in gender equality and women's empowerment. https://www.nutritionintl.org/wp-content/uploads/2020/04/NI_Engaging-Men-and-Boys-in-Gender-Equality-and-Women%E2%80%99s-Empowerment.pdf [Google Scholar]
- Ochieng, J. , Afari‐Sefa, V. , Lukumay, P. J. , & Dubois, T. (2017). Determinants of dietary diversity and the potential role of men in improving household nutrition in Tanzania. PLoS One, 12(12), e0189022. 10.1371/journal.pone.0189022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pelto, G. H. , & Armar‐Klemesu, M. (2015). Identifying interventions to help rural Kenyan mothers cope with food insecurity: Results of a focused ethnographic study. Maternal & Child Nutrition, 11(Suppl 3), 21–38. 10.1111/mcn.12244 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pratley, P. (2016). Associations between quantitative measures of women's empowerment and access to care and health status for mothers and their children: A systematic review of evidence from the developing world. Social Science & Medicine, 169, 119–131. 10.1016/j.socscimed.2016.08.001 [DOI] [PubMed] [Google Scholar]
- Quisumbing, A. , Ahmed, A. , Hoddinott, J. , Pereira, A. , & Roy, S. (2021). Designing for empowerment impact in agricultural development projects: Experimental evidence from the Agriculture, Nutrition, and Gender Linkages (ANGeL) project in Bangladesh. World Development, 146, 105622. 10.1016/j.worlddev.2021.105622 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quisumbing, A. R. , Sproule, K. , Martinez, E. M. , & Malapit, H. (2021). Do tradeoffs among dimensions of women's empowerment and nutrition outcomes exist? Evidence from six countries in Africa and Asia. Food Policy, 100, 102001. 10.1016/j.foodpol.2020.102001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rothstein, J. D. , Klemm, R. , Niyeha, D. , Smith, E. , & Nordhagen, S. (2021). Assessing the challenges to women's access and implementation of text messages for nutrition behaviour change in rural Tanzania. Public Health Nutrition, 24(6), 1478–1491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruel, M. T. , Quisumbing, A. R. , & Balagamwala, M. (2018). Nutrition‐sensitive agriculture: What have we learned so far? Global Food Security, 17, 128–153. 10.1016/j.gfs.2018.01.002 [DOI] [Google Scholar]
- Santoso, M. V. , Kerr, R. B. , Hoddinott, J. , Garigipati, P. , Olmos, S. , & Young, S. L. (2019). Role of women's empowerment in child nutrition outcomes: A systematic review. Advances in Nutrition, 10(6), 1138–1151. 10.1093/advances/nmz056 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shroff, M. R. , Griffiths, P. L. , Suchindran, C. , Nagalla, B. , Vazir, S. , & Bentley, M. E. (2011). Does maternal autonomy influence feeding practices and infant growth in rural India. Social Science & Medicine, 73(3), 447–455. 10.1016/j.socscimed.2011.05.040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- USAID . (2017). Couples as champions for gender equity: Learning and Recommendations from SPRING in Senegal. https://www.spring-nutrition.org/sites/default/files/publications/briefs/spring_senegal_gender_brief_11-7-2017.pdf [Google Scholar]
- USAID Advancing Nutrition . (2020). Program guidance: Engaging family members in improving maternal and child nutrition. https://www.advancingnutrition.org/sites/default/files/2020-11/program_guidance_on_engaging_family_members.pdf [Google Scholar]
- World Health Organization, United Nations Children's Fund, & World Bank Group . (2018). Nurturing care for early childhood development: A framework for helping children survive and thrive to transform health and human potential. https://apps.who.int/iris/bitstream/handle/10665/272603/9789241514064-eng.pdf [Google Scholar]
- Yourkavitch, J. M. , Alvey, J. L. , Prosnitz, D. M. , & Thomas, J. C. (2017). Engaging men to promote and support exclusive breastfeeding: A descriptive review of 28 projects in 20 low‐ and middle‐income countries from 2003 to 2013. Journal of Health, Population, and Nutrition, 36(1), 43. 10.1186/s41043-017-0127-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.