

Abstract
Background:
Couples’ emotions and physiology change across interactions and based on behaviors. Aging couples’ emotions and physiology may be closely related as they spend more time together and rely on each other for support. We examined aging couples’ emotional and physiological associations across multiple indices and marital interactions; we also assessed how couples’ capitalization and responsive behaviors during the first discussion were protective in subsequent emotional conversations.
Methods:
Married couples (n=107 couples, 214 individuals) engaged in positive event, social support, and conflict discussions. Emotional and physiological assessments across discussions included: positive and negative emotion, electrodermal activity, systolic and diastolic blood pressure, heart rate, and heart rate variability. We coded partners’ capitalization and responsive behaviors during the first discussion.
Results:
There were ties in spouses’ positive emotion, negative emotion, electrodermal activity, systolic blood pressure, heart rate, and heart rate variability during positive, supportive, and conflictual discussions. Emotional and physiological associations reflecting shared stress (negative emotion, electrodermal activity, systolic blood pressure) were stronger in couples who were less capitalizing or responsive earlier that day; associations reflecting physiological adaptation (heart rate variability) were stronger for more capitalizing and responsive couples.
Conclusion:
Aging couples’ emotions and physiology tracked together during discussions central to maintaining relationships, and their past behaviors carried over into future interactions and across contexts. Enthusiastic, caring, and understanding behaviors may protect partners from shared emotional and physiological stress; lacking such behaviors may increase emotional and physiological vulnerability. This research identifies behavioral, emotional, and physiological pathways connecting relationships to health in adulthood.
Keywords: Marriage, stress, conflict, capitalization, health, responsiveness, relationships
1. Introduction
Couples’ shared experiences have substantial health implications, particularly in aging couples who prioritize spending meaningful time together. Indeed, partners mutually influence each other’s emotions and physiology, and their emotional and physical health converge over time (Kiecolt-Glaser & Wilson, 2017; Palumbo et al., 2017). For example, one partner may feel stressed when the other partner is stressed. However, as their daily lives become increasingly intertwined, some aging couples may adapt better to different interactions, producing varying health effects. Couples’ heightened emotional and physiological stress across interactions may threaten multiple regulatory systems, hastening morbidity and mortality (Chrousos, 2009; Epel et al., 2018; Pauly et al., 2021). Aging amplifies these health implications as older couples not only spend more time together but depend more on each other for support (Carstensen, 1995; Hoppmann & Gerstorf, 2014). In this study, we examined how various factors—including the type of interaction, behavior, and gender—influence aging couples’ emotional and physiological linkages across multiple measures and contexts. Addressing these effects across contexts provides insight into how and under what conditions spouses influence each other’s health in adulthood.
Dyadic stress and developmental-contextual frameworks suggest that changes in partners’ emotions and physiology are context-dependent (Pauly et al., 2021; Randall & Schoebi, 2018). For instance, partners reacted differently depending on the type of discussion and its intensity, tone, and outcome (Schoebi & Randall, 2015). During conflict, partners had heighted blood pressure (BP) and heart rate (HR) reactivity when they were more hostile relative to less hostile (Robles et al., 2014; Robles & Kiecolt-Glaser, 2003). Across different marital tasks, women’s resting heart rate variability (HRV) decreased more after a negative task than a positive or neutral task (Smith et al., 2011). Likewise, spouses showed greater increases in systolic BP (SBP) and HR during negative relative to positive and neutral marital interactions (Nealey-Moore et al., 2007). Additionally, spouses’ negative emotion increased more after conflict than a support discussion (Kiecolt-Glaser et al., 2005). These findings suggest that spouses experience greater emotional and physiological stress during negative relative to positive interactions.
Partners also mutually influence each other’s emotions and physiology during marital interactions (Pauly et al., 2021; Shrout, 2021). Partners may coregulate each other’s emotions and physiology when interacting, often without conscious effort or awareness (Saxbe & Repetti, 2010). For example, spouses’ HRV tracked together during a lab-based conflict discussion (Wilson et al., 2018). Across contexts, couples showed stronger associations in physiology—measured using an index of interbeat intervals, HR, pulse transmission time, movement, and electrodermal activity (EDA)—during conflict compared to a neutral conversation. Other studies have shown partners’ EDA increased together during both positive and negative emotional event disclosures (Chatel-Goldman et al., 2014; Coutinho et al., 2019). In daily diary studies, partners’ cortisol declined at similar rates across the day (Liu et al., 2013), and their positive and negative emotion tracked together on a daily basis (Butner et al., 2007). Thus, heightened emotional and physiological states across contexts may not only signal a person’s own stress but also a couple’s shared stress. Although these findings demonstrate associations in partners’ emotions and physiology, additional work is needed to understand in which measures and contexts these associations are strongest.
Importantly, couples’ behaviors may impact their emotional and physiological linkage (Pauly et al., 2021; Shrout, 2021). During a health behavior discussion, partners influenced each other’s BP, and their behaviors played a key role in this association: BP was similarly high among couples who used more negative behaviors, but not in couples using fewer negative behaviors (Reed et al., 2013). During conflict, dissatisfied partners’ physiology (interbeat intervals, HR, pulse transmission time, movement, and EDA) was higher and more similar compared to that of their satisfied peers (Levenson & Gottman, 1983). Thus, negative marital perceptions and behaviors may strengthen couples’ emotional and physiological associations. Though research has focused more on negative behavioral effects, positive behaviors have also predicted stronger physiological linkage. Indeed, greater dyadic empathy strengthened links in partners’ EDA when discussing a positive event (Chatel-Goldman et al., 2014; Coutinho et al., 2019).
Two positive behaviors that are not only key to maintaining happy and fulfilling relationships, but also to enhanced health, are capitalization and responsiveness (Donato et al., 2014; Gable et al., 2004; Reis et al., 2017). Capitalization, or showing joy, enthusiasm, or pride in response to partners’ positive disclosures, along with responsiveness, or showing validation, understanding and care, are associated with individual and relational benefits (Pagani et al., 2020; Reis et al., 2017). In contrast, lower capitalization and responsiveness—showing disinterest, minimization, or invalidation—are associated with poorer individual and relational well-being (Gable et al., 2004; Reis et al., 2017). Both enacting and receiving capitalization and responsive behavior is beneficial concurrently and longitudinally. Indeed, more capitalizing and responsive couples had greater well-being the same day and over time compared to less capitalizing and responsive couples (Donato et al., 2014; Pagani et al., 2020). Likewise, capitalizing partners showed increased positive emotion and decreased SBP and diastolic BP (DBP) during positive event discussions (Kaczmarek et al., 2022).
Despite work showing that capitalization and responsiveness are related to lower emotional and physiological responses, protective effects on emotional and physiological linkage have not been examined. Investigating such effects would help identify how positive marital dynamics influence biorhythms and health. Moreover, although research has primarily focused on how negativity and stress spillover to influence later interactions, recent evidence suggests that capitalization and responsive behaviors are protective in subsequent interactions (Kaczmarek et al., 2022; Peters, Reis, & Jamieson, 2018). Identifying how couples reduce shared emotional and physiological stress across marital interactions is important because shared stress is linked with poor health outcomes, including heightened inflammation and cholesterol (Pauly et al., 2020; Wilson et al., 2018). These marriage-related health risks contribute to clinical health endpoints, such as disease development and premature mortality, especially as people age and their relationships become more central to health (Chrousos, 2009; Epel et al., 2018; Pauly et al., 2021). Addressing these effects across contexts provides insight into how and under what conditions spouses influence each other’s health in adulthood.
Lastly, marital interactions have stronger health effects on women than men (Kiecolt-Glaser & Newton, 2001; Wanic & Kulik, 2011). As discussed in gendered socialization and inequality hypotheses, women are more attuned to their partners and monitor their relationships more often than men (Cross & Madson, 1997; Orbuch et al., 2013). Women also are more likely to include their relationships in their identities, whereas men’s self-perceptions are more independent and less relationship-oriented. Yet, compared to women, men’s health benefits more from marriage (Kiecolt-Glaser & Newton, 2001; Wanic & Kulik, 2011), perhaps because men rely more on their spouses for support (Antonucci, 2001). Accordingly, spouses’ emotional and physiological influence may be more pronounced in men or women.
The present study examined aging couples’ emotional and physiological associations and changes across positive event, social support, and conflict discussions. During an in-person lab visit, we assessed EDA, HR, and HRV during each discussion; SBP, DBP, and positive and negative emotion were measured after each discussion. We expected that partners’ emotions and physiology would change across discussions, with greater negative responses during and after conflict relative to positive and support discussions. Specifically, we hypothesized that partners’ HRV and positive emotion would be lower, and EDA, SBP, DBP, HR, and negative emotion would be highest during conflict. Next, we expected that spouses’ emotions and physiology would be positively associated, and that the strength of their emotional and physiological associations would change across discussions. Specifically, we hypothesized that associations in partners’ emotions and physiology would be stronger during conflict relative to the positive event and social support discussions. Third, we expected that each partner’s capitalization and responsive behaviors during the first positive discussion would influence the strength of partners’ emotional and physiological associations across discussions (Peters et al., 2018; Pietromonaco & Collins, 2017). Last, we modeled trajectories separately for women and men to examine gender differences in these effects.
2. Method
2.1. Participants
Couples (n=107 couples, 214 participants) were recruited for a parent study on molecular aging. Interested couples completed online and in-person screens to determine eligibility. Couples were excluded if they were together fewer than three years, not living together, younger than 40 years old, and had sensory impairments that would interfere with study completion. To reduce bias in physiological data, couples were also excluded if either partner had chronic health problems, smoked, abused substances, or used prescription medications other than statins (n=30) and antidepressants (n=49), given their widespread use. Nine participants also used beta-blockers, which served as a covariate in the current study. A total of 576 interested individuals were excluded or did not participate because they or their partner did not meet the stringent health criteria (n=412), their partner was not interested (n=48), they cancelled their visit (n=22), or never enrolled (n=94). All couples were different-sex, married, and cohabiting with an average relationship duration of 28.62 years (SD=14.06, range=3–63). Participants’ average age was 56.52 years (SD=11.22, range=40–86), and the majority of participants were white (92.5%), had graduate or professional training (49.1%), worked full time (57%), and had household incomes over $100,000 (57.5%).
2.2. Procedure
Participants completed a full day visit at the Clinical Research Center (CRC), a hospital research unit. Couples were told to avoid alcohol and strenuous physical activity two days before the study visit. They began a 12-hour fast at 7:30 p.m. the evening before the visit and then couples arrived at 7:30 a.m. Each person was fitted with a wristband on the non-dominant hand to obtain EDA and a heart rate (HR) monitor to obtain HR and HRV throughout the visit. After a 5-minute resting baseline period to assess resting/baseline emotions and physiology, couples ate a standardized breakfast and then completed three interactions together in the following order: a positive event discussion, a support seeking discussion, and a conflict discussion, with 15 to 20 minutes between each for pre- and post-discussion measures and a brief rest. The research team remained out of sight while videorecording each discussion. On average, couples finished the marital interactions by 12–12:30 p.m. Spouses then completed psychological interviews and cognitive testing in separate rooms, and finished study procedures by 2:30–3 p.m.; these assessments are not pertinent to this study and thus are not described here. Study procedures were approved by the Ohio State University Institutional Review Board; participants provided written informed consent before participating.
2.2.1. Positive Event Discussion
In accordance with previous studies (Gable et al., 2006), couples completed a 10-minute positive event (i.e., capitalization) discussion where each partner shared 1–2 events that evoke positive emotions from their personal, individual life rather than something involving both of them. Before the discussions, each partner identified their events. The other partner was instructed to listen and respond as they normally would as if they were at home, and to stay focused on their partner’s topic. Partner order was randomized, and they reversed roles after five minutes.
2.2.2. Social Support Discussion
Couples completed a 10-minute social support discussion in which each partner either solicited or offered social support (Kiecolt-Glaser et al., 2005; Pasch & Bradbury, 1998). Prior to the discussions, both partners identified an important personal characteristic, problem, or issue they wished to change; the issue could not be a source of marital dissension. The other partner was instructed to be involved and respond as they normality would as if they were at home. Partner order was randomized, and they reversed roles after five minutes.
2.2.3. Conflict Discussion
Couples engaged in a 20-minute marital problem discussion to resolve one or more of their marital issues. To initiate the discussions, an experimenter first conducted a 10- to 20-minute interview to identify the most contentious topics within the marriage for both spouses (Kiecolt-Glaser et al., 2005; Kiecolt-Glaser & Newton, 2001). These topics were selected from an inventory each spouse completed about their relationship problems (Kiecolt-Glaser et al., 1993; Knox, 1971). Couples were then asked to discuss and try to resolve one or more marital issues that the experimenter judged to be the most conflict-producing (e.g., money, communication, or in-laws).
2.2.4. Discussion Manipulation Check
As a manipulation test of the various discussions, we assessed spouses’ momentary closeness, how often they talked about the various topics, and each topic’s level of importance. For momentary closeness, we added the two 6-point scale items: “Right now, I feel emotionally distant from my partner” (reverse coded) and “Right now, I feel close to my partner” with scores ranging from 0 to 16. Multilevel models showed spouses felt closer after the positive event (M=10.78, SD=0.20) and social support (M=10.76, SE=0.20) discussions than the conflict discussion (M=9.65, SE=0.20, ps<.00, F(2, 208)=20.59, p<.001); there were no differences in momentary closeness after the positive event and support discussions (p=.906). Spouses also rated the topic’s importance, ranging from 1 (not very important) to 7 (extremely important). Spouses rated the topic discussed during conflict as the most important (M=6.09, SE=0.08, ps<.038, F(2, 212)=16.22, p<.001) followed by the social support topic (M=5.89, SE=0.08, ps<.038), and then the positive event topic (M=5.54, SE=0.08, ps<.001). Last, spouses rated how often they talked about the topic, ranging from 0 (never) to 3 (frequently). Spouses indicated that the topic during conflict was most frequently discussed (M=2.64, SE=0.06, ps<.001, F(2, 210)=37.53, p<.001) followed by the social support topic (M=2.17, SE=0.06, ps<.013), and then the positive event topic (M=1.96, SE=0.06, ps<.013). Thus, compared to positive event and support discussions, spouses felt the least close after conflict and also rated the conflict topic as most frequently discussed and important. These findings are in line with expectations regarding the three discussions’ relative relational effects, importance, and frequency.
2.3. Measures and Materials
2.3.1. Coded Behavior During the Positive Event Discussion
Each partner’s behavior in the responder role was coded for how responsive and active they were while listening to their partners share positive events during the couples’ first discussion of the day. In line with prior research (Gable et al., 2006, 2012; Gable & Reis, 2010), undergraduate and graduate student coders received extensive coding training across two separate variables—responsiveness and capitalization. The three components of responsiveness (understanding, validation, and caring) were coded separately and then averaged to a create a composite index of partner (listener) responsiveness (Reis et al., 2004). The two components of capitalization (active responses and constructive responses) were coded and then averaged to create a composite index of partner (listener) capitalization (Gable et al., 2004). Each discussion was coded by at least six independent coders. Interrater reliabilities were good for responsiveness (.88) and capitalization (.84).
2.3.2. Positive and Negative Emotion
At baseline and immediately after each discussion, participants rated how they felt right now across six emotions scaled 0 (not at all) to 100 (extremely); positive emotions included “happy” and “at ease”, while negative emotions included “sad or blue”, “gloomy”, “angry or irritable”, and “upset.” These items were selected given their reliability and sensitivity to an emotional video (Richter et al., 2011; Richter & Kunzmann, 2011). Cronbach’s α ranged from .75 to .85 for positive emotion and .87 to .89 for negative emotion across baseline and the discussions in the present study.
2.3.3. EDA
Each participant was fitted with an Empatica E4 (Milan, Italy) wristband on the non-dominant hand to measure EDA during each discussion; EDA were recorded at 4 Hz and measured in units of microsiemens (μS). This device has shown accuracy for measuring participants’ continuous EDA levels in the field (Kim & Fesenmaier, 2015; Shoval et al., 2018; van Lier et al., 2020). Visual checks were performed to identify failed measurements, and signal drops (i.e., values less than .1) were excluded to avoid downwardly biasing averages (van Lier et al., 2020). Five-minute segments of EDA during each discussion were used to match the 5-minute window of the rest period. Within each discussion, the 5-minute segments were averaged to represent average EDA during the discussion.
2.3.4. SBP and DBP
SBP and DBP were assessed at baseline during rest and immediately after each discussion using an automated system, the Dinamap/Critikon 1846SX/P (GE Healthcare, Milwaukee, WI.). SBP and DBP were measured in millimeters of mercury (mmHg)
2.3.5. HR and HRV
HR and HRV data were obtained with the Firstbeat Bodyguard 2 (Firstbeat Technologies Ltd, Jyväskylä, Finland), a lightweight heart monitor with electrodes placed under the right clavicle and on the left side of the ribcage below the heart (Bogdány et al., 2016). The device produces reliable and easily extractable HR and HRV data (Bogdány et al., 2016; Hinde et al., 2021). Visual artifact correction was performed on the raw interbeat interval data using Kubios HRV software (Tarvainen et al., 2014). HR was measured in beats per minute. For HRV, we extracted the interbeat interval series and calculated a standard time-domain measure of HRV, the root mean square of successive differences (RMSSD) using Kubios software (Laborde et al., 2017). As discussed by Laborde and colleagues (2017), RMSSD is meant to capture vagal activity, tracks with high-frequency HRV over short time periods, and is relatively unaffected by respiration. We used 5-minute segments of each discussion to match the 5-minute window of the rest period; these segments are standard for short-term HRV recording and track closely with high-frequency HRV in similar time intervals (Laborde et al., 2017). Within each discussion, we then averaged the 5-minute segments to represent average HR and HRV during the discussion. HRV measurements were natural log transformed to better approximate normality of residuals. HRV data in Tables 1 and 2 and Figure 1 represent back transformed geometric numbers to enhance interpretability.
Table 1.
Correlations of Study Variables and Summary Statistics
| 1. NE | 2. PE | 3. EDA | 4. DBP | 5. SBP | 6. HR | 7. HRV | 8. Cap. behavior | 9. Resp. behavior | 10. Age | 11. Gender | 12.SAD | 13. Beta blocker | 14. CSI | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. NE | – | |||||||||||||
| 2. PE | −.53*** | – | ||||||||||||
| 3. EDA | .08* | .06 | – | |||||||||||
| 4. DBP | .02 | .12 | .15* | – | ||||||||||
| 5. SBP | .00 | .18* | .16* | .72*** | – | |||||||||
| 6. HR | .26*** | −.14* | .09 | .24*** | .17* | – | ||||||||
| 7. HRV | −.06 | .14* | .06 | −.12 | −.10 | −.47*** | – | |||||||
| 8. Cap. | −.05 | −.09 | .10 | .01 | −.03 | .07 | −.14 | – | ||||||
| 9. Resp | −.07 | −.03 | .10 | .02 | .00 | .06 | −.11 | .89*** | – | |||||
| 10. Age | −.07 | .07 | .05 | −.04 | .20** | −.13* | −.15* | −.14* | −.16* | – | ||||
| 11. Gen der | .01 | −.13 | .20** | .28*** | .22** | .08 | .01 | .10 | .10 | −.06 | – | |||
| 12. SAD | .04 | .10 | .17* | .35*** | .43 *** | .21** | −.20** | .01 | .03 | .03 | −.38*** | – | ||
| 13. BB | −.06 | 03 | .05 | .03 | .06 | −.18** | .01 | −.02 | .00 | .16* | −.07 | .03 | – | |
| 14. CSI | −.24*** | .25** | .05 | .01 | .03 | −.02 | −.13 | .15* | .23*** | .01 | −.10 | .01 | .02 | – |
| Mean | 5.67 | 79.46 | 1.06 | 71.76 | 124.35 | 62.45 | 31.22 | 10.10 | 13.06 | 56.30 | 0.00 | 22.04 | 0.04 | 128.35 |
| SD | 9.24 | 12.53 | 1.77 | 10.39 | 18.58 | 9.89 | 21.57 | 1.61 | 3.00 | 10.81 | 1.00 | 3.42 | 0.20 | 26.50 |
Note.
p <0.05;
p <0.01;
p <0.001.
Resting baseline emotion and physiology were used for correlations and summary statistics. HRV was natural-log-transformed; HRV mean and SD represent back transformed geometric numbers. Gender coded −1 = men, 1 = women. Beta blocker use coded 0 = no, 1 = yes. NE = negative emotion, PE = positive emotion. EDA = electrodermal activity, DBP = diastolic blood pressure, SBP = systolic blood pressure, HR = heart rate variability, HRV = heart rate variability, Cap. = capitalization, Resp. = responsiveness, BB = beta blocker, CSI = couples satisfaction inventory-32.
Table 2.
Estimated Marginal Means and Standard Errors of Emotional and Physiological Variables Across Couples’ Discussions
| Resting baseline | Positive event | Social support | Conflict | F | M (SE) by gender | |||
|---|---|---|---|---|---|---|---|---|
| Women | Men | P | ||||||
| NE | 5.68 (0.92)a | 3.26 (0.92)b | 7.78 (0.92)a | 11.84 (0.92)c | F(3, 318)=18.78, p<0.001 | 7.12 (0.69) | 7.16 (0.68) | .890 |
| PE | 79.46 (1.37)a | 82.83 (1.37)b | 75.49 (1.37)c | 66.14 (1.37)d | F(3, 318)=37.74, p<0.001 | 74.96 (1.08) | 77.00 (1.08) | .040 |
| EDA | 1.03 (0.12)a,b | 0.96 (0.12)a | 0.89 (0.12)a | 1.19 (0.12)b | F(3, 275)=2.95, p<0.001 | 0.78 (0.11) | 1.24 (0.12) | <.001 |
| DBP | 70.62 (1.19)a | 68.45 (1.19)b | 67.90 (1.19)b | 72.04 (1.19)c | F(3, 314)=29.80, p<0.001 | 67.01 (1.24) | 72.48 (1.21) | <.001 |
| SBP | 123.12 (2.00)a | 126.07 (2.00)b | 124.52 (2.00)a,b | 127.90 (2.00)c | F(3, 314)=9.43, p<0.001 | 121.67 (2.05) | 129.11 (1.99) | <.001 |
| HR | 62.51 (0.77)a | 69.10 (0.77)b | 70.08 (0.77)b | 64.47 (0.77)c | F(3, 313)=166.70, p<0.001 | 63.61 (1.24) | 59.98 (1.23) | <.001 |
| HRV | 25.48 (1.04)a | 24.05 (1.04)b | 22.87 (1.04)c | 23.24 (1.04)b,c | F(3, 289)=9.81, p<0.001 | 23.10 (1.05) | 24.78 (1.05) | 0.10 |
Note. Within each row, means that do not share the same superscript differ at p<.05. Discussion order = (1) positive event discussion, (2) social support, and (3) conflict. NE = negative emotion, PE = positive emotion, EDA = electrodermal activity, DBP = diastolic blood pressure, SBP = systolic blood pressure, HR = heart rate variability, HRV = heart rate variability. HRV data represent back transformed geometric numbers. The average means and standard errors across all discussions are reported for women and men given that there were no gender differences by discussion type.
Figure 1.
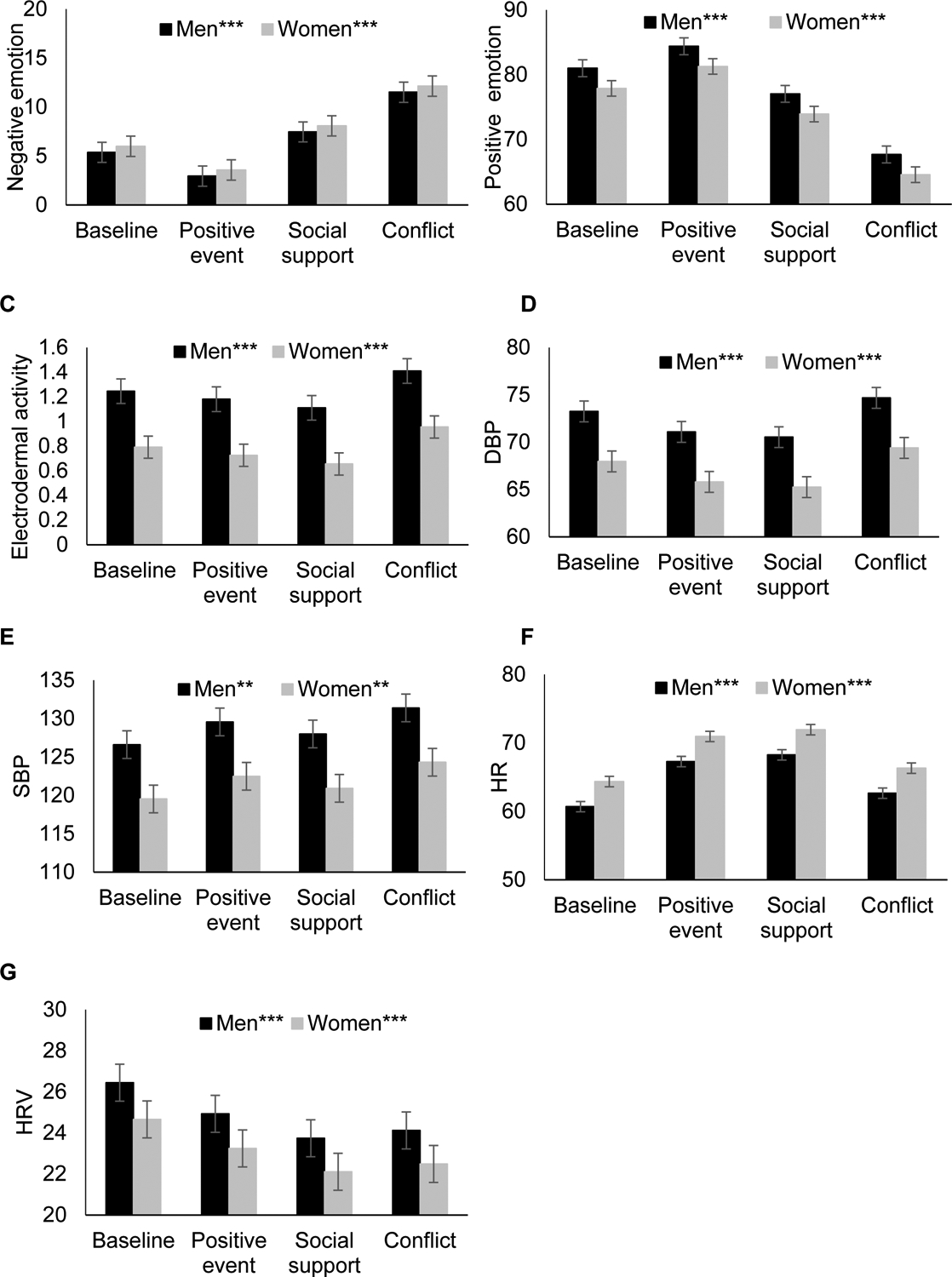
Spouses’ (A) negative emotion, (B) positive emotion, (C) electrodermal activity, (D) diastolic blood pressure, (E) systolic blood pressure, (F) heart rate, and (G) heart rate variability trajectories across discussions by gender. HRV data represent back transformed geometric numbers. Error bars are ±1 standard error. +p<0.10; *p<0.05; **p<0.01; ***p<0.001
2.3.6. Covariates
Analyses controlled for age and relationship satisfaction (Couples Satisfaction Inventory-32; Funk & Rogge, 2007; α=.98), given their association with study variables. Models predicting physiological variables also adjusted for sagittal abdominal diameter, given its association with psychophysiological responsiveness. Models predicting SBP, DBP, HR, and HRV also adjusted for beta-blocker use (n=9).
2.4. Analysis Plan
Prior to the main analyses, we examined correlations among study variables and used paired samples t-tests to assess gender differences. We also examined variables for outliers and invalid values using visual and statistical inspections, meeting distributional assumptions of the analyses, and missing values. HRV measurements were natural log transformed to better approximate normality of residuals. For EDA, signal drops (i.e., values less than .1) were excluded to avoid downwardly biasing averages; two multivariate outliers were also trimmed in EDA models due to influential data identified from residual diagnostics. There were no outlier and/or influential data points for the other models. Missing data were minimal; there were no missing data for positive and negative emotion, one missing data point for HR, DBP, and SBP (0.12%), 59 missing data points for HRV (7%), and 91 missing data points for EDA (10%). All analyses used multilevel modeling which accounted for missing data by maximizing the use of existing data and including all participants in the analyses, regardless of missing data points (Brauer & Curtin, 2018). In the primary analyses, unstandardized betas were used as the point estimate in the models, and standardized betas were also provided. Continuous predictors and covariates (responsive behaviors, capitalization behaviors, baseline emotion/physiology, age, relationship satisfaction, and sagittal abdominal diameter) were grand mean centered to improve the interpretability of the intercepts. Models corrected for multiple comparisons, and all analyses were done using SPSS version 26 (IBM Corp., Armonk, NY). Data and code for this study are available upon request to the first author.
To address study hypotheses that spouses’ emotions and physiology would change across discussions and be more negative during and after conflict, we assessed emotional and physiological trajectories across baseline and the three discussions using dyadic multilevel models; couples’ discussion type was treated as a categorical variable due to the varying nonlinear trajectories. We examined expected gender differences in trajectories using two-way interactions between gender and discussion type.
We then used multilevel models to test hypotheses regarding associations in couples’ emotions and physiology (Butner et al., 2007); we controlled for baseline emotions/physiology to adjust for initial levels. In this framework, each model estimated separate regression equations for men and women simultaneously (i.e., separate intercepts and slopes for men and women in the same model) with spouses denoted by dummy variables that were used to calculate intercepts; these separate estimates also allowed us to test how effects differed for women and men (Butner et al., 2007; Laurenceau & Bolger, 2005). Models included random intercepts for men and women using a variance components covariance structure. We attempted to estimate random effects for the focal predictors and discussion type, but the models did not converge. Separate models were run for each emotional and physiological variable. In this modeling approach, couples’ associations were tested by predicting people’s own emotion or physiology from their partners’ emotion or physiology at the same time point (Butner et al., 2007). Thus, couples’ associations were captured by the main effect of the partner emotional/physiological variable. Each partner emotional/physiological predictor variable was within-person centered to reflect deviations from the person’s individual means (Butner et al., 2007). Accordingly, the partner predictor variables reflected how much higher or lower a person’s emotions and physiology were during each discussion relative to their average across discussions.
Therefore, to test hypotheses that spouses’ emotions and physiology would be related, and that couples’ associations would change across discussions, we specified models that included two-way interactions between the partner predictor (e.g., negative emotion) and couple discussion type, along with their main effects. Then, we tested hypotheses that individuals’ own and their partners’ capitalization and responsive behaviors during the first positive event discussion would alter associations across discussions. Thus, we added three-way interactions between the partner predictor (e.g., negative emotion), couple discussion type, and own/partner capitalization/responsive behavior, along with all lower-order interaction terms and main effects; responsive behaviors and capitalization behaviors were tested in separate models. Nonsignificant higher order interactions were removed when interpreting lower order interactions or main effects. Significant interacting effects were probed at one standard deviation above and below the means for each continuous interacting variable (Aiken & West, 1991).
3. Results
Table 1 shows means, standards deviations, and correlations among study variables; resting baseline emotion and physiology variables were used for correlations and summary statistics. For the emotion variables, baseline negative emotion was correlated with lower positive emotion and higher resting HR; baseline positive emotion was related to lower resting HR, as well as higher resting SBP and HRV. Among the physiological variables, resting EDA, DBP, and SBP were all positively correlated. Resting DBP and SBP also were related to higher HR. Resting HR and HRV were negatively correlated. In addition, capitalization and responsive behaviors during the first positive event discussion were positively correlated with each other. For gender differences, men had higher resting EDA, SBP, and DBP (EDA: Mmen=1.41, SD=2.20, Mwomen=0.69, SD=1.05, t(141)=2.88, p=0.002; SBP: Mmen=128.46, SD=16.13, Mwomen=120.24, SD=19.98, t(212)=3.31, p<0.001; DBP: Mmen=74.70, SD=10.20, Mwomen=68.82, SD=9.78, t(212)=4.30, p<0.001).
3.1. Emotional and Physiological Changes Across Couples’ Discussions
The dyadic multilevel models showed that couples’ emotions and physiology changed across baseline and the three discussions (ps<.001); see Table 2 and Figure 1 for means and standard errors. When comparing emotion across baseline and the three discussions, negative emotion was highest (ps<.001 to .042), while positive emotion was lowest (ps<.001 to .043), after conflict, followed by social support and baseline, and then the positive event discussion. For physiological markers during discussions, EDA (ps=.005 to .030) and DBP (ps<.001) were higher during conflict compared to the positive event and social support discussions; SBP was higher during conflict than social support (p<.001); HR was higher during the positive event and social support discussions compared to the conflict discussion (ps<.001); and HRV was higher during the positive event discussion than the social support discussion (p=.020). Compared to the discussions, HR (ps<.001) was lower at baseline, while HRV (ps<.007) was higher at baseline. Compared to women, men had lower HR and higher positive emotion, EDA, DBP, and SBP (see Table 2 for means and standard errors). Emotional and physiological trajectories did not differ by gender (ps>.084).
For covariates, on average, more satisfied spouses had lower negative emotion (b=−0.12, β=−.25, SE=0.02, p<.001) and SBP (b=−0.07, SE=0.03, p=.037), as well as higher positive emotion (b=0.20, β=.27, SE=0.03, p<.001). Individuals with greater sagittal abdominal diameters had lower HRV (b=−0.04, β=−.20, SE=0.01 p<.001), as well as higher EDA (b=0.06, β=.10, SE=0.02, p=.012), DBP (b=1.00, β=.30, SE=0.14, p<.001), SBP (b=2.31, β=.41, SE=0.24, p<.001), and HR (b=0.75, SE=0.14, p<.001). Older spouses also had higher SBP (b=0.19, β=.11, SE=0.09, p=0.042) and lower HRV (b=−0.02, β=−.29, SE=0.004, p<.001). Those using beta blockers had a lower average HR (b=−10.38, β=−.94, SE=2.01, p<.001).
3.2. Associations in Couples’ Emotional and Physiological Changes Across Discussions
Table 3 shows coefficients for associations in couples’ emotional and physiological changes across discussions, controlling for baseline emotions/physiology. The results demonstrated significant associations for each emotional and physiological marker across discussions except DBP (ps>.541); thus, as one spouse’s emotion/physiology increased, so did the other spouse’s. Specifically, there were significant associations in couples’ negative emotion (pwomen=.001; pmen=.003), positive emotion (pwomen and men <.001), EDA (pwomen=.048; pmen=.038), SBP (pwomen=.005; pmen=.012), and HR (pwomen=.043; pmen=.007). For HRV, men’s HRV increased with their wives’ higher HRV (pmen=.023), but women’s HRV was unrelated to that of their husbands (pwomen=.318).
Table 3.
Multilevel Model Coefficients for Associations in Couples’ Emotional and Physiological Changes Across Discussions
| Model 1a: b, β (SE) or F | Model 1b: b (SE) or F | |||
|---|---|---|---|---|
| Women | Men | Women | Men | |
| NE | ||||
| Partner NE | 0.20, .16 (0.06)** | 0.15 (0.06)** | 0.19, .15 (0.09)* | 0.28, .23 (0.10)** |
| Discussion type | F(2, 421)=7.35*** | F(2, 420)=9.67*** | F(2, 466)=5.53** | F(2, 468)=8.39*** |
| Partner NE*Discussion type | F(2, 480)=0.13 | F(2, 90)=1.03 | ||
| PE | ||||
| Partner PE | 0.34, .26 (0.07)*** | 0.27, .20 (0.06)*** | 0.50, .38 (0.10)*** | 0.50, .38 (0.10)*** |
| Discussion type | F(2, 424)=6.42* | F(2, 421)=18.34*** | F(2, 465)=6.66 * | F(2, 467)=19.40*** |
| Partner PE*Discussion type | F(2, 510)=1.84 | F(2, 463)=5.10* | ||
| EDA | ||||
| Partner EDA | 0.13, .07 (0.07)* | 0.18, .09 (0.09)* | 0.33, .16 (0.12)** | 0.18, .09 (0.15) |
| Discussion type | F(2, 333)=11.73*** | F(2, 332)=0.65 | F(2, 330)=10.83*** | F(2, 330)=0.42 |
| Partner EDA*Discussion type | F(2, 394)=1.93 | F(2, 374)=0.03 | ||
| DBP | ||||
| Partner DBP | −0.04, −.02 (0.07) | −0.03, −.01 (0.07) | 0.11, .05 (0.13) | 0.02, .01 (0.12) |
| Discussion type | F(2, 417)=12.88*** | F(2, 416)=27.79*** | F(2, 426)=10.07*** | F(2, 424)=27.38*** |
| Partner DBP*Discussion type | F(2, 499)=1.02 | F(2, 507)=0.16 | ||
| SBP | ||||
| Partner SBP | 0.18, .07 (0.07)** | 0.17, .07 (0.06)* | 0.20, .08 (0.11)+ | 0.30, .12 (0.12)* |
| Discussion type | F(2, 415)=3.50* | F(2, 415)=1.81 | F(2, 411)=3.12* | F(2, 418)=1.46 |
| Partner SBP*Discussion type | F(2, 506)=1.07 | F(2, 504)=2.52+ | ||
| HR | ||||
| Partner HR | 0.13, .05 (0.06)* | 0.20, .07 (0.07)** | 0.04, .02 (0.10) | 0.19, .07 (0.14) |
| Discussion type | F(2, 421)=29.37*** | F(2, 419)=27.93*** | F(2, 438)=29.47*** | F(2, 440)=24.37*** |
| Partner HR*Discussion type | F(2, 486)=0.72 | F(2, 502)=0.23 | ||
| HRV | ||||
| Partner HRV | 0.11, .04 (0.10) | 0.22, .08 (0.10)* | 0.13, .05 (0.21) | −0.03, −.01 (0.19) |
| Discussion type | F(2, 208)=12.22*** | F(2, 215)=3.31* | F(2, 209)=11.96*** | F(2, 216)=3.99* |
| Partner HRV*Discussion type | F(2, 274)=0.41 | F(2, 240)=0.31 | ||
Note. Discussion order = (1) positive event discussion, (2) social support, and (3) conflict. NE = negative emotion, PE = positive emotion, EDA = electrodermal activity, DBP = diastolic blood pressure, SBP = systolic blood pressure, HR = heart rate variability, HRV = heart rate variability.
p<0.10;
p<0.05;
p<0.01;
p<0.001
Across discussions, the strength of associations in couples’ negative emotion, EDA, HR, SBP, and HRV did not change (ps>.082). However, changes were shown for men’s positive emotion: Men reported greater positive emotion when their wives did too during conflict (b=0.50, β=.37 SE=.10, p<.001) but not during the positive event or social support discussions (ps>.092).
3.3. Associations in Couples’ Emotional and Physiological Changes Based on Coded Capitalization and Responsive Behavior1
Capitalization and responsive behaviors during the positive event discussion (the first discussion) were associated with or moderated associations in couples’ negative emotion, DBP, SBP, EDA, and HRV across discussions, but not their positive emotion (ps>.105) or HR (ps>.202). Table 4 provides significant interaction effects, standard errors, and p-values.
Table 4.
Multilevel Model Coefficients for Significant Moderating Effects of Coded Behavior on Couples’ Emotional and Physiological Associations Across Discussions
| Men | b, β(SE) or F | p |
|---|---|---|
| NE | ||
| Partner NE*Partner capitalization behavior | −0.11, −.14 (0.04) | .009 |
| SBP | ||
| Partner SBP*Own capitalization behavior*Discussion type | F(2, 476)=5.17 | .006 |
| Partner SBP*Own responsive behavior*Discussion type | F(2, 477)=4.19 | .016 |
| Women | b (SE) or F | |
| EDA | ||
| Partner EDA*Own responsive behaviora | 0.06, .09 (0.03) | .032 |
| Partner EDA*Partner responsive behaviora | −0.05, −.08 (0.03) | .048 |
| HRV | ||
| Partner HRV*Partner capitalization behavior*Discussion type | F(2, 236)=3.50 | .032 |
| Partner HRV*Partner responsive behavior*Discussion type | F(2, 244)=4.30 | .015 |
Note.
Indicates interactions were tested in the same model; all other interactions were tested in separate models. Only significant interactions are shown; all interaction effects are reported in text. Discussion order = (1) positive event discussion, (2) social support, and (3) conflict. NE = negative emotion, EDA = electrodermal activity, SBP = systolic blood pressure.
As shown in Figure 2, across discussions, couples’ capitalization and responsive behaviors were associated with men’s negative emotion and DBP, as well as wives’ EDA. In Figure 2A, men’s negative emotion increased with their wives’ negative emotion across discussions if their wives were less capitalizing (b=0.33, SE=0.09, p<.001), but not more capitalizing (p=.916), during the positive event discussion. In addition, men’s negative emotion was highest when their wives reported high negative emotion and used fewer capitalization behaviors (b=−2.85, SE=0.96, p=.003). Likewise, as depicted in Figure 2B, women’s EDA increased with their husbands’ EDA across discussions but only if women’s husbands were less responsive (b=0.38 SE=0.13, p=.004) but not more responsive (p=.383) during the earlier positive event discussion. In contrast, Figure 2C shows that women’s EDA increased with their husbands’ EDA if women more responsive (b=0.40, SE=0.13, p=.003) but not less responsive (p=.571) during the earlier positive event discussion.
Figure 2.
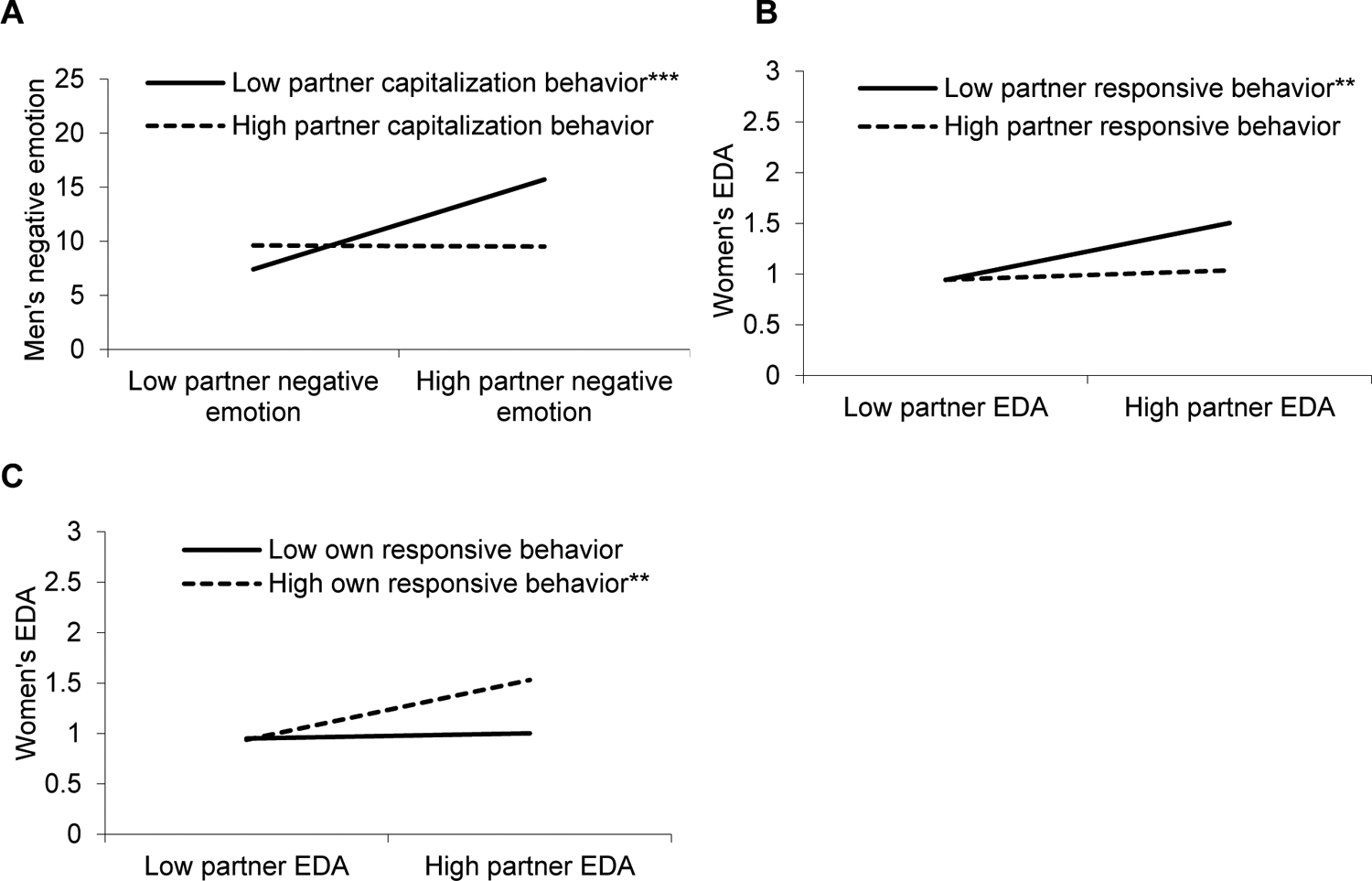
Visual depiction of significant interactions for (A) men’s average negative emotion predicted by their wives’ negative emotion and capitalization behavior, (B) women’s average EDA predicted by their husbands’ EDA and responsive behavior, and (C) women’s average EDA predicted by their husbands’ EDA and their own responsive behavior. Asterisks indicate significant simple slopes. +p<0.10; *p<0.05; **p<0.01; ***p<0.001
Interactions with discussion type showed that during conflict, couples’ earlier capitalization and responsive behaviors predicted men’s lower SBP and wives’ higher HRV; see Figure 3. Men’s SBP increased with that of their wives during conflict, but only among men who were less capitalizing (b=0.74, SE=0.17 p<.001; Figure 3A) or responsive (b=0.61, SE=0.16, p<.001; Figure 3B) during the positive event discussion earlier that day. Men’s SBP did not increase with their wives’ SBP if men were more capitalizing or responsive (ps>.182). Also, at low and high partner SBP, less capitalizing men had higher SBP during conflict than more capitalizing men (bs=−1.84 and −2.42, SEs=0.71 and 0.74, ps<.012). As shown in Figures 3C and 3D, women’s HRV increased with their husbands’ HRV during conflict if their husbands used more capitalization (b=0.72, SE=0.32 p=.025; Figure 3C) or responsive (b=0.86, SE=0.33 p=.009; Figure 3D) behaviors earlier that day. HRV in women with less capitalizing or responsive husbands did not change with their husbands’ HRV (ps>0.142).
Figure 3.
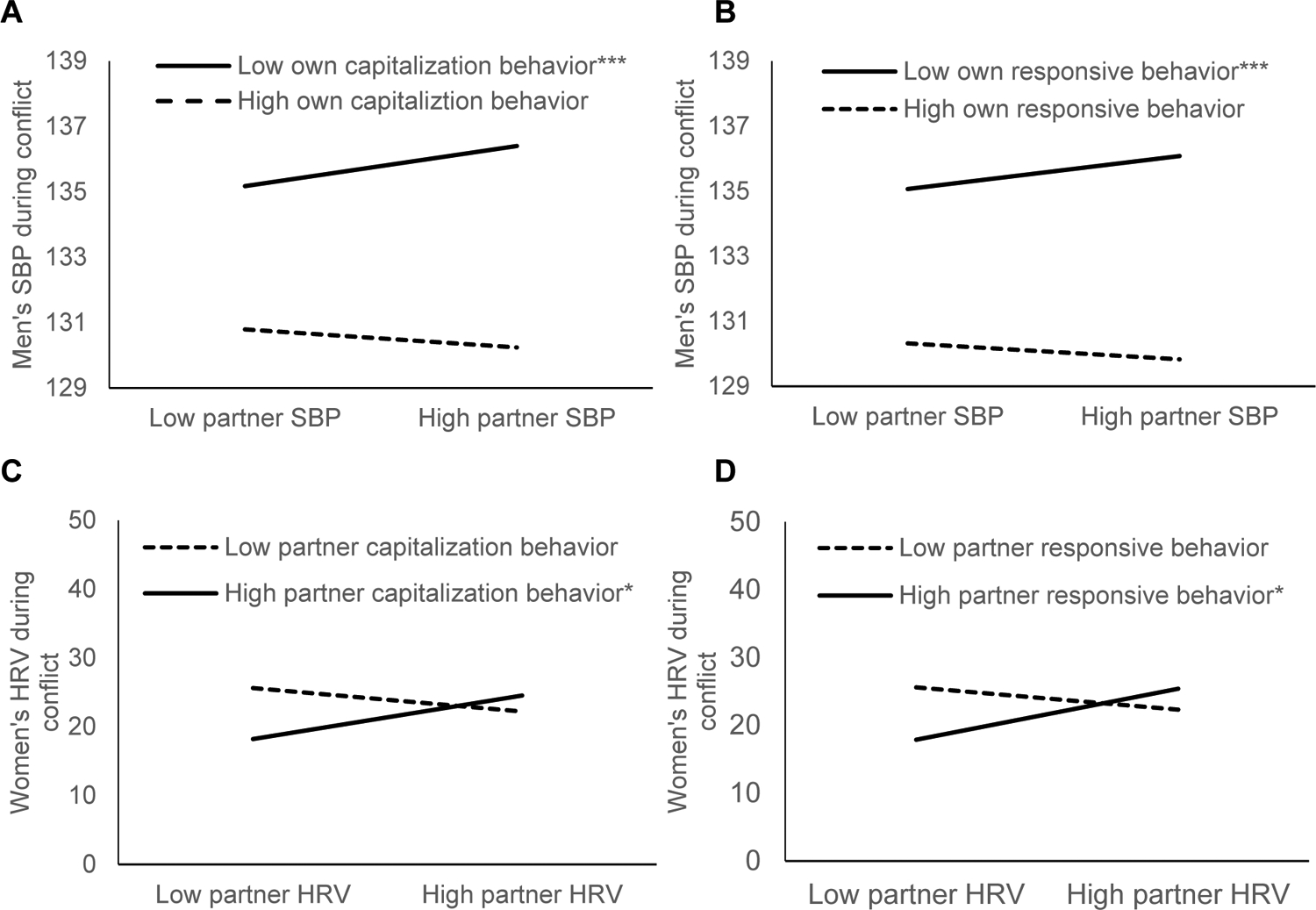
Visual depiction of significant interactions during conflict for (A) men’s SBP predicted by their wives’ SBP and their own capitalization behavior; (B) men’s SBP predicted by their wives’ SBP and their own responsive behavior; (C) women’s HRV predicted by their husbands’ HRV and capitalization behavior; and (D) women’s HRV predicted by their husbands’ HRV and responsive behavior. Asterisks indicate significant simple slopes. +p<0.10; *p<0.05; **p<0.01; ***p<0.001
In addition to moderating couples’ emotional and physiological associations, men’s capitalization (F(2, 406)=3.97, p=.020) and responsive F(2, 405)=5.59, p=.004) behaviors moderated their own DBP across discussions. Among men who were less capitalizing and responsive during the positive event discussion, DBP was higher during the conflict discussion compared to the positive event discussion (cap.: b=5.17, SE=0.84, p<.001; resp.: b=5.48, SE=0.93, p<.001) and social support discussion (cap.: b=6.51, SE=1.01, p<.001; resp.: b=6.93, SE=0.99, p<.001). Among men who were more capitalizing and responsive during the positive event discussion, DBP also was higher during conflict relative to the positive event discussion (cap.: b=3.65, SE=1.09 p=.003; resp.: b=3.11, SE=1.10 p=.014), but not during the social support discussion (ps>.098). There were no DBP differences in the positive event and social support discussions at low or high capitalization or responsiveness (ps>.249). In addition, men’s HRV was higher if their wives were more capitalizing (b=0.05, SE=0.02 p=.048) and responsive (b=0.02, SE=0.01 p=.047) during the positive event discussion.
4. Discussion
Consistent with dyadic stress and developmental-contextual theories, this study demonstrated couples’ emotional and physiological connections across multiple indices—negative and positive emotion, EDA, SBP, HR, and HRV—during positive event, social support, and conflict discussions. In addition, couples’ behaviors during the first positive event discussion had implications for their emotional and physiological associations across discussions; these findings suggest that couples’ behaviors may carry over into future interactions and different contexts. Interestingly, associations in spouses’ negative emotion, EDA, and SBP, each of which reflect shared stress, were stronger among couples who used fewer capitalization or responsive behaviors during the first positive discussion. In contrast, associations in spouses’ HRV, a measure reflecting physiological adaptation, were stronger in couples using greater capitalization or responsiveness earlier in the day. Couples’ capitalization and responsive behaviors may therefore alter how closely their emotions and physiology track together in subsequent interactions.
When examining each measure separately, couples showed significant ties in their positive emotion, negative emotion, EDA, SBP, and HR across discussions; men’s HRV was also related to their wives’ HRV across discussions. The strength of couples’ negative emotion, EDA, SBP, HR, and HRV associations did not change across discussions, suggesting that they tracked together across discussions at similar rates. Women’s emotional and physiological ties to their husbands were similar across the three discussions. For men, their positive emotion increased with their wives’ positive emotion during conflict, but not during the positive event or support discussions. These findings are consistent with previous research showing couples’ emotions and physiology were linked across the day and in different discussions (Chatel-Goldman et al., 2014; Coutinho et al., 2019; Liu et al., 2013); they also illuminate gender differences across emotional and physiological measures. Women may have experienced similar emotional and physiological associations across discussions because marital interactions have stronger effects on women’s health than that of men (Kiecolt-Glaser & Wilson, 2017). Men, however, rely more on their spouses compared to women, particularly as they age (Antonucci, 2001). Men may therefore be particularly sensitive to their spouses’ emotions during conflictual conversations.
In addition, couples’ emotional and physiological markers changed across baseline measurements and the discussions. Couples’ negative emotion was highest, while positive emotion was lowest, during conflict, followed by social support and baseline, and then the positive event discussion. For physiological markers during discussions, EDA, DBP, and SBP were highest during conflict, whereas HR and HRV were highest during the positive event or social support discussions. Compared to the discussions, HR was lower at baseline, while HRV was higher at baseline. These findings are consistent with expectations except those for HR; HR may have been highest during positive and supportive discussions because it has both parasympathetic and sympathetic influences (Laborde et al., 2017). During conflict, higher negative emotion, EDA, DBP, and SBP, as well as lower positive emotion and HRV, might reflect greater emotional and physiological stress while discussing a contentious marital issue compared to a positive or support discussion. Conflict, however, is common and central to maintaining intimate relationships. Sharing emotional and physiological stress during these conversations may increase each partner’s psychological, immune, and cardiovascular risks over time (Kiecolt-Glaser & Wilson, 2017).
Couples’ emotional and physiological associations also changed based on individuals’ own and their partners’ capitalization and responsiveness earlier that day. Men’s SBP tracked with their wives’ SBP during conflict but only in men who were less, but not more, capitalizing and responsive during the positive event discussion earlier in the day. Also, men’s negative emotion increased with that of their wives across discussions when wives were less capitalizing, but not more capitalizing, during the positive event discussion. For women, EDA increased with their husbands’ EDA across discussions when their husbands were less responsive, but not more responsive, during the positive event discussion. In contrast, women’s HRV increased with their husbands HRV during conflict but only if their husbands were more capitalizing and responsive during the earlier positive event discussion—suggesting greater autonomic flexibility and adaptation during stress. These findings are consistent with and extend past research showing emotional and physiological ties among more negative couples (Levenson & Gottman, 1983; Saxbe & Repetti, 2010). Capitalization promotes couples’ relationships, shared identities, well-being, and more positive events (Peters et al., 2018). Individuals’ own and their partners’ relationship-enhancing behaviors may have put them at ease and protected them from subsequent emotional and physiological stress. Notably, among women, their husbands’ earlier beneficial behaviors may have promoted physiological adaptation and regulation during a later conflictual discussion. In contrast, not capitalizing on positive interactions or showing care and understanding to one another may have promoted emotional and physiological vulnerability and interfered with autonomic regulation. These findings demonstrate the physiological benefits of capitalization and responsiveness during couples’ interactions (Gable et al., 2004; Reis et al., 2010).
Interestingly, women who were more responsive to their husbands’ positive events also experienced higher EDA with that of their husbands across discussions that day. Thus, women’s EDA tracked with their husbands’ EDA if their husbands were less responsive, and if women were more responsive, earlier that day. Women may have been shielded from husbands’ understanding, validating, and caring behaviors. Yet, women providing understanding and validation to their husbands might have strengthened their physiological connection. Responsiveness is key to maintaining strong relationships (Reis et al., 2017), and thus providing responsiveness may promote women’s physiological ties with their husbands.
These findings fit within and contribute to both dyadic stress and developmental-contextual theories. The Dyadic Biobehavioral Stress Model suggests partners influence each other’s emotions and physiology, and that each person’s behaviors provide health consequences (Shrout, 2021). The current results provide new evidence that spouses’ emotions and physiology change and are associated across positive, supportive, and conflictual discussions. This study also identified capitalization and responsiveness as key behaviors shaping couples’ emotional and physiological associations. These relationship-enhancing behaviors may have lasting effects on couple dynamics, and are important candidates for understanding how marital interactions connect to biorhythms and health.
The present study also has implications for aging theories and research on aging couples’ relationships and health. Couples’ relationship quality and interactions can promote or impair their health, and these effects become even stronger as spouses age and spend more time together (Kiecolt-Glaser & Wilson, 2017; Shrout, 2021). In accord with socioemotional selectivity theory, older couples’ daily experiences become increasingly interconnected as they shift focus toward their relationships and building stronger bonds (Hoppmann & Gerstorf, 2014). The current findings show aging couples’ emotional and physiological connections across multiple discussions, with particularly high emotional and physiological stress in those who were less positive or showed little validation and understanding toward one another in earlier discussions. Shared emotional and physiological stress threatens multiple regulatory systems that underlie morbidity and mortality. Indeed, heightened cortisol, inflammation, and cholesterol accompany partners’ shared stress (Pauly et al., 2020; Shrout et al., 2020; Wilson et al., 2018). As couples grow older and spend more time together, it may be even more beneficial for them to use capitalization and responsive behaviors when reflecting on the past and talking about their relationships. These positive behaviors might not only promote their relationships but also protect their health.
This study has several notable strengths. The dyadic approach allowed for examination of couples’ emotional and physiological associations during common conversations. Having both couple members also allowed us to address how each partner’s behaviors altered emotional and physiological ties. Capturing how a partner influences a person’s own emotions and physiology is key to understanding a relationship’s health impact (Pietromonaco & Collins, 2017; Shrout, 2021). Likewise, research has focused on how negative behaviors influence couples’ health, neglecting the role of positive relationship behaviors in protecting and promoting their health. This study addressed this gap and focused on how positive behaviors altered couples’ associations during discussions. Including multiple couple discussions allowed us to illustrate couples’ emotional and physiological relations across positive, supportive, and conflictual contexts, and uniquely situated this work to address how couples’ behavior in earlier discussions altered links in later discussions.
Additionally, we adjusted for important covariates, including relationship satisfaction, which demonstrated that couples’ capitalization and responsive behavior uniquely predicted couples’ emotional and physiological associations over and above their global relationship satisfaction. These findings support the notion that capitalization and responsiveness should be considered as a description of interpersonal processes within relationships, rather than a global characterization of that relationship (Peters et al., 2018; Reis et al., 2004). Likewise, findings showed later conflict behaviors did predict changes in couples’ emotional and physiological associations in earlier discussions. These results lend additional credence to the study’s hypothesis of earlier behaviors predicting later emotional and physiological linkage. We also provided evidence for emotional and physiological connections among aging couples, an understudied group whose relationships provide health risks and benefits (Hoppmann & Gerstorf, 2014; Kiecolt-Glaser & Wilson, 2017). Finally, the inclusion of multiple emotional and physiological measures allowed us to demonstrate couples’ associations across several important indices associated with the autonomic nervous system, highlighting a relationship’s far-reaching health effects.
A limitation of the study was that the sample was primarily white, highly educated, and included only heterosexual couples. Partners’ emotional and physiological relations should be addressed in more diverse samples, particularly given cultural differences in couples’ emotional connections (Randall et al., 2011). This study focused on how capitalization and responsive behaviors in a positive event discussion influenced associations in subsequent and more conflictual discussions; nevertheless, it is possible that the discussion order contributed to couples’ patterns across discussions. Future research comparing couples’ emotional and physiological associations across various discussion orders could help tease apart these effects.
This study also focused on emotional and physiological associations across multiple discussions and from topic to topic. Assessing moment-to-moment physiological changes within topics would be valuable, as would capturing physiological reactivity using change scores. Thus, examining autonomic arousal and change in shorter intervals may reveal meaningful effects within and between partners. Also, our findings demonstrated differences in couples’ emotional and physiological responses and associations to the various lab-based discussions, but these effects may differ if discussions were to occur spontaneously or in couples’ natural environments. Research suggests laboratory studies provide more conservative estimates of interpersonal behavior and processes (Heyman, 2001); the effects documented in this study may be stronger if captured in couples’ natural settings. Likewise, spouses’ speaking, turn taking, and task engagement may have influenced their emotions and physiology. Teasing apart these other factors’ effects and those related to the nature of the discussion may provide a clearer picture of how and under what conditions couples experience emotional and physiological linkage. Couples’ emotional and physiological relations during these different discussions may also look different on a daily basis. Examining how these associations change daily and over time may further our understanding on how relationships influence emotional and physical health.
This lab-based study demonstrated aging couples’ emotional and physiological associations across multiple indices and during common yet emotional conversations. On average, spouses’ positive emotion, negative emotion, EDA, SBP, HR, and HRV were associated with one another during positive, supportive, and conflictual conversations. Emotional and physiological associations reflecting shared stress (negative emotion, EDA, SBP) were stronger in couples who were less capitalizing or responsive early in the day, whereas associations reflecting physiological adaptation (HRV) were stronger for more capitalizing and responsive couples. This research identifies key behavioral, emotional, and physiological pathways through which relationships may influence health in adulthood.
Highlights.
Aging couples engaged in positive event, social support, and conflict discussions
Spouses’ positive emotion, negative emotion, EDA, SBP, HR, and HRV were associated with each other
Couples’ behaviors altered associations in subsequent interactions across the day
Ties reflecting shared stress were stronger in less capitalizing and responsive couples
We highlight pathways connecting marital interactions to biorhythms and health
Funding:
Work on this project was supported by an Ohio State University Presidential Postdoctoral Scholars Fellowship, and NIH grants KL2TR002530, UL1TR002529, R01 AG057032, T32 CA229114, and TL1TR002735. This research was also supported by the Clinical Research Center/Center for Clinical Research Management of The Ohio State University Wexner Medical Center and The Ohio State University College of Medicine in Columbus, Ohio.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declaration of Conflicting Interests: The author(s) declared that there were no conflicts of interest with respect to the authorship or the publication of this article.
To further test hypothesized spillover effects, we examined if later conflict behaviors predicted changes in couples’ emotional and physiological associations across discussions. Results showed negative conflict behaviors did not predict couples’ emotional or physiological linkage with one exception: Women’s HRV increased with their husbands’ HRV when they used fewer negative conflict behaviors but only during conflict (p=.036) but not the earlier positive event or support discussions. Thus, negative conflict behavior did not predict HRV in the earlier discussions. These results suggest later behavior did not predict couples’ earlier emotional or physiological linkage, lending credence to the study’s spillover hypothesis of earlier behaviors predicting later linkage.
References
- Aiken LS, & West SG (1991). Multiple regression: Testing and interpreting interactions. In Multiple regression: Testing and interpreting interactions. Sage Publications, Inc. [Google Scholar]
- Antonucci TC (2001). Social relations: An examination of social networks, social support, and sense of control. In Handbook of the psychology of aging, 5th ed. (pp. 427–453). Academic Press. [Google Scholar]
- Bogdány T, Boros S, Szemerszky R, & Köteles F (2016). Validation of the Firstbeat TeamBelt and BodyGuard2 systems Health tourism View project Nutrition as an intervention View project. October, 4–12. https://www.researchgate.net/publication/308809187
- Brauer M, & Curtin JJ (2018). Linear mixed-effects models and the analysis of nonindependent data: A unified framework to analyze categorical and continuous independent variables that vary within-subjects and/or within-items. Psychological Methods, 23(3), 389–411. 10.1037/met0000159 [DOI] [PubMed] [Google Scholar]
- Butler EA (2015). Interpersonal affect dynamics: It takes two (and time) to tango. Emotion Review, 7(4), 336–341. 10.1177/1754073915590622 [DOI] [Google Scholar]
- Butner J, Diamond LM, & Hicks AM (2007). Attachment style and two forms of affect coregulation between romantic partners. Personal Relationships, 14(3), 431–455. 10.1111/j.1475-6811.2007.00164.x [DOI] [Google Scholar]
- Carstensen LL (1995). Evidence for a life-span theory of socioemotional selectivity. Current Directions in Psychological Science, 4(5), 151–156. 10.1111/1467-8721.ep11512261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chatel-Goldman J, Congedo M, Jutten C, & Schwartz JL (2014). Touch increases autonomic coupling between romantic partners. Frontiers in Behavioral Neuroscience, 8(MAR), 1–12. 10.3389/fnbeh.2014.00095 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chrousos GP (2009). Stress and disorders of the stress system. Nature Reviews Endocrinology, 5(7), 374–381. 10.1038/nrendo.2009.106 [DOI] [PubMed] [Google Scholar]
- Coutinho J, Oliveira-Silva P, Fernandes E, Gonçalves OF, Correia D, Perrone Mc-Govern K, & Tschacher W (2019). Psychophysiological synchrony during verbal interaction in romantic relationships. Family Process, 58(3), 716–733. 10.1111/famp.12371 [DOI] [PubMed] [Google Scholar]
- Cross SE, & Madson L (1997). Models of the Self: Self-Construals and Gender. Psychological Bulletin, 122(1), 5–37. [DOI] [PubMed] [Google Scholar]
- Donato S, Pagani A, Parise M, Bertoni A, & Iafrate R (2014). The Capitalization Process in Stable Couple Relationships: Intrapersonal and Interpersonal Benefits. Procedia - Social and Behavioral Sciences, 140, 207–211. 10.1016/j.sbspro.2014.04.411 [DOI] [Google Scholar]
- Epel ES, Crosswell AD, Mayer SE, Prather AA, Slavich GM, Puterman E, & Mendes WB (2018). More than a feeling: A unified view of stress measurement for population science. Frontiers in Neuroendocrinology, 49(December 2017), 146–169. 10.1016/j.yfrne.2018.03.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Funk JL, & Rogge RD (2007). Testing the ruler with item response theory: Increasing precision of measurement for relationship satisfaction with the couples satisfaction index. Journal of Family Psychology, 21(4), 572–583. 10.1037/0893-3200.21.4.572 [DOI] [PubMed] [Google Scholar]
- Gable SL, Gonzaga GC, & Strachman A (2006). Will you be there for me when things go right? Supportive responses to positive event disclosures. Journal of Personality and Social Psychology, 91(5), 904–917. 10.1037/0022-3514.91.5.904 [DOI] [PubMed] [Google Scholar]
- Gable SL, Gosnell CL, Maisel NC, & Strachman A (2012). Safely testing the alarm: Close others’ responses to personal positive events. Journal of Personality and Social Psychology, 103(6), 963–981. 10.1037/a0029488 [DOI] [PubMed] [Google Scholar]
- Gable SL, Impett EA, Reis HT, & Asher ER (2004). What do you do when things go right? The intrapersonal and interpersonal benefits of sharing positive events. Journal of Personality and Social Psychology, 87(2), 228–245. 10.1037/0022-3514.87.2.228 [DOI] [PubMed] [Google Scholar]
- Gable SL, & Reis HT (2010). Chapter Four: Good news! capitalizing on positive events in an interpersonal context. In Advances in Experimental Social Psychology (1st ed., Vol. 42, Issue 10). Elsevier Inc. 10.1016/S0065-2601(10)42004-3 [DOI] [Google Scholar]
- Heyman RE (2001). Observation of couple conflicts: Clinical assessment applications, stubborn truths, and shaky foundations. Psychological Assessment, 13(1), 5–35. 10.1037//1040-3590.13.1.5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hinde K, White G, & Armstrong N (2021). Wearable devices suitable for monitoring twenty four hour heart rate variability in military populations. Sensors, 21(4), 1–20. 10.3390/s21041061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoppmann CA, & Gerstorf D (2014). Biobehavioral Pathways Underlying Spousal Health Dynamics: Its Nature, Correlates, and Consequences. Gerontology, 60(5), 458–465. 10.1159/000357671 [DOI] [PubMed] [Google Scholar]
- Kaczmarek LD, Kelso KC, Behnke M, Kashdan TB, Dziekan M, Matuła E, Kosakowski M, Enko J, & Guzik P (2022). Give and take: The role of reciprocity in capitalization. Journal of Positive Psychology, 17(4), 561–572. 10.1080/17439760.2021.1885054 [DOI] [Google Scholar]
- Kiecolt-Glaser JK, Loving TJ, Stowell JR, Malarkey WB, Lemeshow S, Dickinson SL, & Glaser R (2005). Hostile marital interactions, proinflammatory cytokine production, and wound healing. Archives of General Psychiatry, 62(12), 1377–1384. 10.1001/archpsyc.62.12.1377 [DOI] [PubMed] [Google Scholar]
- Kiecolt-Glaser JK, Malarkey WB, Chee M, Newton T, Cacioppo JT, Mao - HY, Glaser R, & Ewart CK (1993). Negative behavior during marital conflict is associated with immunological down-regulation. Psychosomatic Medicine, 55(5), 395–412. 10.1097/00006842-199309000-00001 [DOI] [PubMed] [Google Scholar]
- Kiecolt-Glaser JK, & Newton TL (2001). Marriage and health: His and hers. Psychological Bulletin, 127(4), 472–503. 10.1037/0033-2909.127.4.472 [DOI] [PubMed] [Google Scholar]
- Kiecolt-Glaser JK, & Wilson S (2017). Lovesick: How couples’ relationships influence health. Annual Review of Clinical Psychology, 8(13), 421–443. 10.1146/annurev-clinpsy-032816-045111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim JJ, & Fesenmaier DR (2015). Measuring Emotions in Real Time: Implications for Tourism Experience Design. Journal of Travel Research, 54(4), 419–429. 10.1177/0047287514550100 [DOI] [Google Scholar]
- Knox D (1971). Marriage Happiness. Research Press. [Google Scholar]
- Laborde S, Mosley E, & Thayer JF (2017). Heart rate variability and cardiac vagal tone in psychophysiological research - Recommendations for experiment planning, data analysis, and data reporting. In Frontiers in Psychology (Vol. 8, Issue FEB). Frontiers Research Foundation. 10.3389/fpsyg.2017.00213 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laurenceau J-P, & Bolger N (2005). Using diary methods to study marital and family processes. Journal of Family Psychology, 19(1), 86–97. 10.1037/0893-3200.19.1.86 [DOI] [PubMed] [Google Scholar]
- Levenson RW, & Gottman JM (1983). Marital interaction: Physiological linkage and affective exchange. Journal of Personality and Social Psychology, 45(3), 587–597. 10.1037/0022-3514.45.3.587 [DOI] [PubMed] [Google Scholar]
- Liu S, Rovine MJ, Klein LC, & Almeida DM (2013). Synchrony of diurnal cortisol pattern in couples. Journal of Family Psychology, 27(4), 579–588. 10.1037/a0033735 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nealey-Moore JB, Smith TW, Uchino BN, Hawkins MW, & Olson-Cerny C (2007). Cardiovascular reactivity during positive and negative marital interactions. Journal of Behavioral Medicine, 30(6), 505–519. 10.1007/s10865-007-9124-5 [DOI] [PubMed] [Google Scholar]
- Orbuch TL, Bauermeister JA, Brown E, & Mckinley BD (2013). Early Family Ties and Marital Stability Over 16 Years: The Context of Race and Gender. Family Relations, 62(2), 255–268. 10.1111/fare.12005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pagani AF, Parise M, Donato S, Gable SL, & Schoebi D (2020). If You Shared My Happiness, You Are Part of Me: Capitalization and the Experience of Couple Identity. Personality and Social Psychology Bulletin, 46(2), 258–269. 10.1177/0146167219854449 [DOI] [PubMed] [Google Scholar]
- Palumbo R. v., Marraccini ME, Weyandt LL, Wilder-Smith O, McGee HA, Liu S, & Goodwin MS (2017). Interpersonal autonomic physiology: A systematic review of the literature. Personality and Social Psychology Review, 21(2), 99–141. 10.1177/1088868316628405 [DOI] [PubMed] [Google Scholar]
- Pasch LA, & Bradbury TN (1998). Social support, conflict, and the development of marital dysfunction. In Journal of Consulting and Clinical Psychology (Vol. 66, Issue 2, pp. 219–230). American Psychological Association. 10.1037/0022-006X.66.2.219 [DOI] [PubMed] [Google Scholar]
- Pauly T, Gerstorf D, Ashe MC, Madden KM, & Hoppmann CA (2020). You’re under my skin: Long-term relationship and health correlates of cortisol synchrony in older couples. Journal of Family Psychology. 10.1037/fam0000809 [DOI] [PubMed] [Google Scholar]
- Pauly T, Gerstorf D, Wahl HW, & Hoppmann CA (2021). A Developmental–Contextual Model of Couple Synchrony Across Adulthood and Old Age. Psychology and Aging. 10.1037/pag0000651 [DOI] [PubMed] [Google Scholar]
- Peters BJ, Reis HT, & Gable SL (2018). Making the good even better: A review and theoretical model of interpersonal capitalization. Social and Personality Psychology Compass, 12(7), 1–19. 10.1111/spc3.12407 [DOI] [Google Scholar]
- Peters BJ, Reis HT, & Jamieson JP (2018). Cardiovascular indexes of threat impair responsiveness in situations of conflicting interests. International Journal of Psychophysiology, 123, 1–7. 10.1016/J.IJPSYCHO.2017.12.005 [DOI] [PubMed] [Google Scholar]
- Pietromonaco PR, & Collins NL (2017). Interpersonal mechanisms linking close relationships to health. American Psychologist, 72(6), 531–542. 10.1037/amp0000129 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Randall AK, Corkery SA, Duggi D, Kamble S. v., & Butler EA (2011). ―We’re having a good (or bad) day‖: Differences in emotional synchrony in married couples in the United States and India. Family Science, 2(3), 203–211. 10.1080/19424620.2012.665378 [DOI] [Google Scholar]
- Randall AK, & Schoebi D (2018). Conceptual approaches to studying interpersonal emotion dynamics. In Interpersonal Emotion Dynamics in Close Relationships (pp. 7–26). Cambridge University Press. 10.1017/9781316822944.003 [DOI] [Google Scholar]
- Reed RG, Randall AK, Post JH, & Butler EA (2013). Partner influence and in-phase versus anti-phase physiological linkage in romantic couples. International Journal of Psychophysiology, 88(3), 309–316. 10.1016/j.ijpsycho.2012.08.009 [DOI] [PubMed] [Google Scholar]
- Reis HT, Clark MS, & Holmes JG (2004). Perceived Partner Responsiveness as an Organizing Construct in the Study of Intimacy and Closeness. In Handbook of closeness and intimacy. (pp. 201–225). Lawrence Erlbaum Associates Publishers. [Google Scholar]
- Reis HT, Lemay EP, & Finkenauer C (2017). Toward understanding understanding: The importance of feeling understood in relationships. Social and Personality Psychology Compass, 11(3), 1–22. 10.1111/spc3.12308 [DOI] [Google Scholar]
- Reis HT, Smith SM, Carmichael CL, Caprariello PA, Tsai FF, Rodrigues A, & Maniaci MR (2010). Are you happy for me? How sharing positive events with others provides personal and interpersonal benefits. Journal of Personality and Social Psychology, 99(2), 311–329. 10.1037/a0018344 [DOI] [PubMed] [Google Scholar]
- Richter D, Dietzel C, & Kunzmann U (2011). Age differences in emotion recognition: The task matters. Journals of Gerontology - Series B Psychological Sciences and Social Sciences, 66 B(1), 48–55. 10.1093/geronb/gbq068 [DOI] [PubMed] [Google Scholar]
- Richter D, & Kunzmann U (2011). Age Differences in Three Facets of Empathy: Performance-Based Evidence. Psychology and Aging, 26(1), 60–70. 10.1037/a0021138 [DOI] [PubMed] [Google Scholar]
- Robles TF, & Kiecolt-Glaser JK (2003). The physiology of marriage: Pathways to health. Physiology and Behavior, 79(3), 409–416. 10.1016/S0031-9384(03)00160-4 [DOI] [PubMed] [Google Scholar]
- Robles TF, Slatcher RB, Trombello JM, & McGinn MM (2014). Marital quality and health: A meta-analytic review. Psychological Bulletin, 140(1), 140–187. 10.1037/a0031859 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saxbe D, & Repetti RL (2010). For better or worse? Coregulation of couples’ cortisol levels and mood states. Journal of Personality and Social Psychology, 98(1), 92–103. 10.1037/a0016959 [DOI] [PubMed] [Google Scholar]
- Schoebi D, & Randall AK (2015). Emotional dynamics in intimate relationships. Emotion Review, 7(4), 342–348. 10.1177/1754073915590620 [DOI] [Google Scholar]
- Shoval N, Schvimer Y, & Tamir M (2018). Real-Time Measurement of Tourists’ Objective and Subjective Emotions in Time and Space. Journal of Travel Research, 57(1), 3–16. 10.1177/0047287517691155 [DOI] [Google Scholar]
- Shrout MR (2021). The Health Consequences of Stress in Couples: A Review and New Integrated Dyadic Biobehavioral Stress Model. Brain, Behavior, & Immunity - Health, 16. 10.1016/j.bbih.2021.100328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shrout MR, Brown RD, Orbuch TL, & Weigel DJ (2019). A multidimensional examination of marital conflict and subjective health over 16 years. Personal Relationships, 26(3), 490–506. 10.1111/pere.12292 [DOI] [Google Scholar]
- Shrout MR, Renna ME, Madison AA, Jaremka LM, Fagundes CP, Malarkey WB, & Kiecolt-glaser JK (2020). Cortisol slopes and conflict: A spouse’s perceived stress matters. Psychoneuroendocrinology, 121, 104839. 10.1016/j.psyneuen.2020.104839 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith TW, Cribbet MR, Nealey-Moore JB, Uchino BN, Williams PG, MacKenzie J, & Thayer JF (2011). Matters of the Variable Heart: Respiratory Sinus Arrhythmia Response to Marital Interaction and Associations With Marital Quality. Journal of Personality and Social Psychology, 100(1), 103–119. 10.1037/a0021136 [DOI] [PubMed] [Google Scholar]
- Tarvainen MP, Niskanen JP, Lipponen JA, Ranta-aho PO, & Karjalainen PA (2014). Kubios HRV - Heart rate variability analysis software. Computer Methods and Programs in Biomedicine, 113(1), 210–220. 10.1016/j.cmpb.2013.07.024 [DOI] [PubMed] [Google Scholar]
- van Lier HG, Pieterse ME, Garde A, Postel MG, de Haan HA, Vollenbroek-Hutten MMR, Schraagen JM, & Noordzij ML (2020). A standardized validity assessment protocol for physiological signals from wearable technology: Methodological underpinnings and an application to the E4 biosensor. Behavior Research Methods, 52(2), 607–629. 10.3758/s13428-019-01263-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wanic R, & Kulik J (2011). Toward an Understanding of Gender Differences in the Impact of Marital Conflict on Health. Sex Roles, 65(5), 297–312. 10.1007/s11199-011-9968-6 [DOI] [Google Scholar]
- Wilson SJ, Bailey BE, Jaremka LM, Fagundes CP, Andridge R, Malarkey WB, Gates KM, & Kiecolt-Glaser JK (2018). When couples’ hearts beat together: Synchrony in heart rate variability during conflict predicts heightened inflammation throughout the day. Psychoneuroendocrinology, 93(September 2017), 107–116. 10.1016/j.psyneuen.2018.04.017 [DOI] [PMC free article] [PubMed] [Google Scholar]