Abstract
Objective To compare the clinical results between conservative (CS) and surgical treatment (CXS) of A3 and A4 fractures without neurological deficit.
Methods Prospective observational study of patients with thoracolumbar fractures type A3 and A4. These patients were separated between the surgical and conservative groups, and evaluated sequentially through the numeric rating scale (NRS), Roland-Morris disability questionnaire (RMDQ), EuroQol-5D (EQ-5D) quality of life questionnaire, and Denis work scale (DWS) up to 2.5 years of follow-up.
Results Both groups showed significant improvement, with no statistical difference in pain questionnaires (NRS: CXS 2.4 ± 2.6; CS 3.5 ± 2.6; p > 0.05), functionality (RMDQ: CS 7 ± 6.4; CXS 5.5 ± 5.2; p > 0.05), quality of life (EQ-5D), and return to work (DWS).
Conclusion Both treatments are viable options with equivalent clinical results. There is a tendency toward better results in the surgical treatment of A4 fractures.
Keywords: internal fixation fracture, spinal fractures, treatment outcome, conservative treatment
Introduction
Thoracolumbar fractures (T11–L3) correspond to 90% of spinal fractures, 1 2 and about 2/3 of these fractures involve compression of the vertebral body without ligament injury or dislocation, classified as AOSpine type A, according to the classification described and previously validated for spinal fractures. 3 4 5 6
Compression fractures with comminution of the vertebral body and displacement of fragments towards the vertebral canal correspond to 20% of all fractures, 1 7 8 9 being characterized by the involvement of the posterior wall and one (AOSpine type A3) or both (AOSpine type A4) vertebral plateaus. 10 11 This involvement of the posterior wall leads to a retropulsion of the bone fragment in the vertebral canal, which may generate neurological deficit in about 15% of the cases. 5 12 13
Considering the group of less severe fractures, such as AOSpine type A0, A1, and A2, there is consensus on the best risk/benefit with conservative treatment, and similarly with surgical treatment for more severe type B and C fractures, and fractures with neurological deficit. 5 7 10
Despite its high incidence, the ideal treatment for A3/A4 fractures without neurological deficit remains controversial, and the extensive report of this topic in the literature was not able to demonstrate the superiority of either treatment method. 10 11 14 15
The main objectives of A3/A4 fractures management are to prevent and limit neurological deficit, allow early pain-free mobility, stabilize the spine, and correct and/or avoid kyphotic deformity. 9 12
Surgical treatment offers immediate stabilization, correction of deformity, early ambulation, and less dependence on orthotics, 8 but presents complications such as implant failure, pseudoarthrosis, infection, among others. 4
Historically, conservative treatment presented high morbidity rates for the long period of absolute rest, between 6 and 8 weeks. Currently, this rest period is restricted to a maximum of 6 days, followed by mobility and use of several orthotics for 3 months, 9 14 demonstrating good functional results, low progression of deformity, and low incidence of neurological deterioration. 12 16 17
The aim of this study was to compare the clinical results of patients with thoracolumbar A3 or A4 fractures, without neurological deficit, treated surgically and conservatively.
Materials and Methods
This prospective observational cohort study was accepted by the ethics committee of the two participating centers (CAAE: 02583312.4.2001.0066). All patients with thoracolumbar spine fractures from August 2016 to August 2017 were evaluated.
The inclusion criteria of the study were: traumatic fractures of the spine between T10 and L3, AOSpine type A3 or A4, absence of neurological deficit, patients over 18-years-old and under 65-years-old, with time elapsed between trauma and the proposed treatment of no more than 10 days. Furthermore, all patients allocated in the respective study groups, conservative or surgical, were required to present the exact same treatment conduction, regardless of the group to which they belonged, with details below.
Patients with pathological fracture, clinically evident osteoporosis, severe systemic disease, AOSpine type B or C fractures, pregnant women, injuries to other organs, and/or firearm injuries were excluded from the study.
Cases at risk of deformity progression or neurological risk were excluded from the study. The criteria used for exclusion were kyphosis of the fractured segment greater than 30 degrees, loss of height greater than 50% of the vertebral body, and involvement of more than 50% of the vertebral canal by bone fragment.
All patients included signed the free and informed consent form and were then selected for the conservative treatment or surgical treatment groups, according to the experience and personal decision of the head surgeon. The selection occurred randomly, without specified factors, and, once there was exclusion according to specified criteria, the personal decision option and the therapeutic proposal defined by the attending physician predominated. Considering the characteristics of retrospective selection of cases, a random and unequal sample was obtained between the groups. Since, to date, the therapeutic decision for such cases of A3 and A4 fracture without neurological deficit remains plausible for both options, surgical or conservative, the indication of treatment is defined according to subjective and contextual criteria identified by the attending physician.
Patients allocated in conservative treatment were instructed to follow an initial rest period of up to 3 days, followed by the use of orthosis (Jewett vest) for 6 to 12 weeks. Patients in the surgical group were submitted to indirect reduction of the kyphotic deformity through lordotic positioning with the aid of the Hall support, and short fixation of the fracture with the Depuy-Synthes Universal Spine System (USS), corresponding to the reduction and instrumentation with pedicular screws in vertebrae above and below the fracture, in this case series, without the need for additional screws in the fractured level, using the applied principle of fracture fixation concept, without arthrodesis. All patients received the same care guidelines, such as avoiding heavy activities and sports for 3 months, according to the established protocol. 18
The patients were followed up for two years and were evaluated with thoracolumbar spine radiographs, numeric rating scale (NRS) for pain, 19 the Roland Morris disability questionnaire (RMDQ) 20 , quality of life with the EuroQol-5d (EQ-5D) 21 22 , and return to work with the Denis work scale (DWS) 23 questionnaires in pre-op, 6 weeks, 3 months, 6 months, 1 year, and 2 years of treatment. A smaller group of patients (n = 16) completed 2 years and 6 months of treatment.
The quantitative variables evaluated in the study were described by means, medians, minimum values, maximum values, and standard deviations. For categorical variables, frequencies and percentages were presented. For the comparison of the groups defined by the treatment (CSX or CS), regarding quantitative variables, either the Student t-test was used for independent samples or the Mann-Whitney nonparametric test were used, depending on the normality condition of the variables. This condition was assessed by the Kolmogorov-Smirnov test. Regarding categorical variables, the correlations were made considering the Fisher exact test. Values of p < 0.05 indicated statistical significance. The data were analyzed with the Statistical Package Social Sciences (SPSS, IBM Corp. Armonk, NY, USA) version 20.4 software.
Results
Demographic
A total of 59 patients completed the follow-up period and were included in the statistical analysis. Based on demographic characteristics ( Table 1 ), in terms of gender, 20 patients were female and 39 were male. According to the proposed treatment, 23 patients comprised the conservative group (CS), and 36 the surgical group (CSX). The most frequent site of fractures was L1 (n = 31), followed by T12 (n = 13), and the other levels presented similar distribution between T10, T11, L2, and L3.
Table 1. Patient demographics.
| Treatment | ||
|---|---|---|
| Gender | CS (n = 23) | CSX (n = 36) |
| Female | 10 (43.5%) | 10 (27.8%) |
| Male | 13 (56.5%) | 26 (72.2%) |
| Location | ||
| L1 | 11 (47.8%) | 20 (55.6%) |
| L2 | 2 (8.7%) | 5 (13.9%) |
| L3 | 3 (13%) | 3 (8.3%) |
| T10 | 1 (4.3%) | 0 (0%) |
| T11 | 0 (0%) | 1 (2.8%) |
| T12 | 6 (26.1%) | 7 (19.4%) |
| Rating (A) | ||
| 3 | 17 (73.9%) | 10 (27.8%) |
| 4 | 6 (26.1%) | 26 (72.2%) |
Abbreviations: CS, conservative treatment; CSX, surgical treatment.
Regarding the AOSpine classification, 27 cases were classified as A3 (46%), and 32 as A4 (54%). A significant difference was found ( p = 0.001) when comparing treatment options within each classification, A3 presented more conservative cases (CS: 17 vs CSX: 10) in relation to A4 fracture (CS: 6 vs CSX: 26).
Considering this case series, no grade-worthy complications were identified, considering the possibility of its interference in the functional results measured, both for the conservative group and for the surgical group, while the follow-up was proposed and performed.
Roland-Morris Disability Questionnaire (RMDQ)
A comparative analysis showed similar results in the initial conservative (RMDQ 18 ± 4.9) and surgical (RMDQ 18.1 ± 5.3) treatment scores. There was also no statistical difference between the RMDQ scores in the final evaluation (CS 7 ± 6.4; CXS 5.5 ± 5.2; p > 0.05). Using the period pretreatment as a comparison reference, both groups showed significant improvement in the RMDQ score from 3 months on, but in the final evaluation, with two and a half years of follow-up, the surgical group showed a tendency toward better results ( Table 2 ).
Table 2. Comparison of RMDQ between pre-treatment and follow-up of each group.
| Comparative evaluation | P- value | |
|---|---|---|
| CS | CXS | |
| Pre-treatment vs 6 weeks | 0.170 | 0.090 |
| Pre-treatment vs 3 months | 0.004 | 0.040 |
| Pre-treatment vs 6 months | 0.001 | 0.001 |
| Pre-treatment vs 1 year | 0.002 | < 0.001 |
| Pre-treatment vs 2.5 years | 0.144 | 0.004 |
Abbreviations: CS, conservative treatment; CSX, surgical treatment; RMDQ, Roland-Morris disability questionnaire.
EuroQol-5D (EQ-5D)
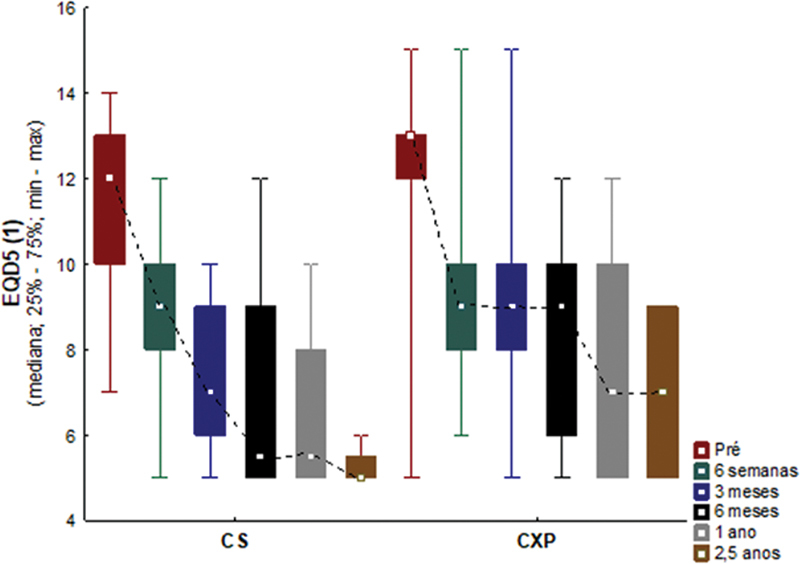
Considering the answers of the EQ-5D questionnaire, in terms of surgical versus conservative treatment, both showed similar improvement in the 6 weeks evaluation ( p > 0.05). At 3 months, the conservative group presented better results (CS 7.2 ± 5.9; CXS 8.8 ± 7; p < 0.05), but this difference did not continue from six months until the end of the follow-up, when both groups presented good results ( p > 0.05) ( Fig. 1 ). In the comparative evaluation of pretreatment with follow-up periods, both treatments improved significantly ( p < 0.05). In the group that reached 2 years and 6 months of follow-up (n = 16), the conservative group did not keep the results improved ( Table 3 ). Considering the second section of the EQ-5D, after 6 weeks both groups showed progressive improvement in quality of life until the end of follow-up ( Fig. 2 ).
Fig. 1.

EQD5 score of proposed treatments.
Table 3. Comparison of EQ-5D between pre-treatment and follow-up of each group.
| Comparative evaluation | P- value | |
|---|---|---|
| CS | CXS | |
| Pre-treatment vs 6 weeks | 0.001 | < 0.001 |
| Pre-treatment vs 3 months | < 0.001 | < 0.001 |
| Pre-treatment vs 6 months | < 0.001 | < 0.001 |
| Pre-treatment vs 1 year | 0.001 | < 0.001 |
| Pre-treatment vs 2.5 years | 0.068 | 0.003 |
Abbreviations: CS: conservative treatment; CXS surgical treatment; EQ-5D: EuroQol-5D.
Fig. 2.

EQ-D5 quality of life score.
Pain Scale (NRS)
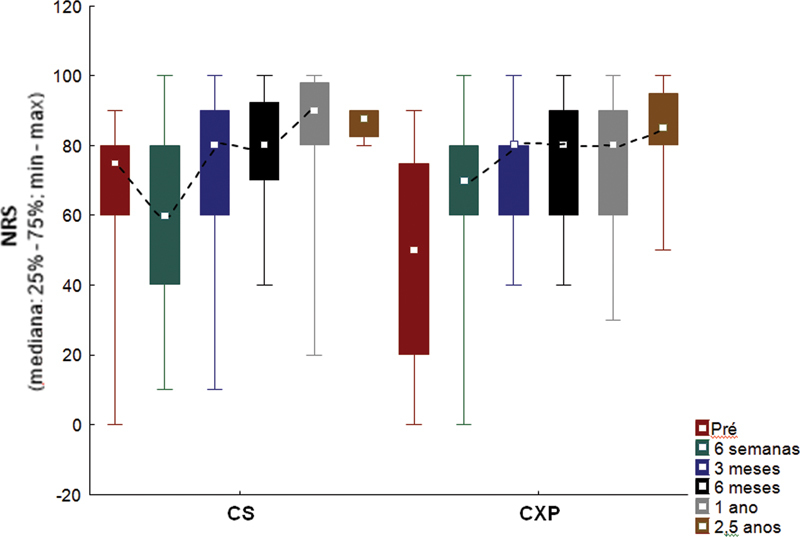
Comparing both treatment groups, an important improvement in the pain scale was seen until the final follow-up, but with no statistical difference between the proposed groups (CXS 2.4 ± 2.6; CS 3.5 ± 2.6; p > 0.05) ( Fig. 3 ). Comparing the evaluation of pain in pre-treatment (CXS 7.6 ± 2.2; CS 7 ± 2.6) with the follow-ups, CS group showed significant improvement up to 1 year of follow-up (NRS 2.5 ± 2.7; p < 0.05), unlike CSX group, which showed a significant improvement in pain up to the final evaluation (NRS 2.4. ± 2.6; p < 0.05).
Fig. 3.

NRS score of proposed treatments.
Denis Scale (DWS)
Considering that few patients were considered active in relation to work and excluding other reasons for impediment not related to spinal conditions, 19 patients were evaluated for the DWS at different times. After a comparative analysis, both groups showed improvement of the score, with significant improvement of the conservative group at 6 months ( p < 0.005), but this superiority was not maintained at the end of the follow-up ( Fig. 4 ).
Fig. 4.

Comparison of DWS scale for proposed treatments.
Discussion
The concept of explosion fracture has changed a lot since its definition by Denis, undergoing several changes and achieving greater agreement and reliability with the AOSpine classification of thoracolumbar fractures. 12 23 24 Many of the fractures considered by the old classifications as “unstable explosions” and grouped together with other fractures by explosion of the vertebral body have associated ligament injuries, increasing the potential for failure of conservative treatment. This factor may have directed some studies in favor of surgical treatment. 4 14
In the current classification, these lesions would be considered type B and their surgical treatment would be mandatory. Division between A3 and A4 fractures was subsequent to the beginning of the selection of patients for this study and was then reclassified by a new analysis of computed tomography imaging.
Wood et al. 1 demonstrated, in their randomized controlled study, that the 47 patients evaluated and separated in surgical and conservative treatment did not present significant difference in the questionnaires of functionality and pain after 2 years of follow-up. In the long-term reassessment (on average 18 years), both pain and functionality evaluations presented favorable results to the conservative group. 1 8 The surgical methods used in this study precede the use of pedicular fixation, generating an interpretation bias and making it difficult to compare them with current studies.
The final comparative analysis of this study demonstrated good results of both treatments, with no statistical difference in the evaluated items; however, in statistical tests applied individually between each of the groups (conservative and surgical), there was a tendency toward better results in favor of surgical treatment. In contrast to these results, Siebenga et al. 4 demonstrated that the surgical group presented better radiological and functional results (VAS and RMDQ-24) compared to the conservative group ones. An important point to be mentioned was the inclusion, in both groups, of patients with other types of type A fracture besides A3 and A4, and this heterogeneity of the sample may have generated a bias in the interpretation of the results.
In his study, Shen et al. 14 demonstrated that operated patients presented better pain control up to three months, but from the sixth month both groups showed improvement in functionality scores without statistical difference at the end of the follow-up, a result similar to that of the current study.
As in this study, Pehlivanoglu et al. 7 could not find significant difference in the evaluation of functionality and return to work between the groups. However, the surgical group presented better radiographic results in the short and long term. In the present study, radiographic worsening greater than five degrees did not occur in any case, and radiographic measurements will be the subject of future analysis.
A recent meta-analysis by Rometsch et al. analyzed 12 articles that compared conservative and surgical treatment of A3 and A4 fractures with no neurological deficit and found no statistical difference in pain and functionality scores. An important point indicated by the authors is that most studies do not differentiate A3 and A4 fractures, failing to detect potential differences in results between these two types of fractures. 10
Rabb et al., 15 through their systematic review, evaluated 6 level 2 studies of evidence and, despite the relatively high quality, the studies produced conflicting conclusions, so that both surgery and conservative treatment remained viable options for compression fractures.
This study has as limitation the absence of standardization of conservative treatment, in which some patients used orthosis, while others, for various reasons, did not use any type of immobilization.
Conclusion
Both conservative and surgical treatments showed good clinical results at the end of the study, being viable options for type A3 and A4 fractures without neurological deficit. In cases of A4 fracture, from the individualized analysis of results, a statistical trend to better results obtained by surgical treatment stands out.
Agradecimentos
Agradecemos aos Doutores Letícia Cardoso Ern e Wellington Ueda pela colaboração na coleta de dados. Agradecemos também a AOSpine Knowledge Forum on Trauma, pelo apoio logístico.
Acknowledgment
We thank Doctors Letícia Cardoso Ern and Wellington Ueda for their collaboration in data collection. We also thank AOSpine Knowledge Forum on Trauma, for the logistical support.
Conflito de Interesses Os autores declaram não haver conflito de interesses.
Suporte Financeiro
Este estudo teve suporte financeiro e logístico da AOSpine Latin America.
Financial Support
This study had financial and logistical support from AOSpine Latin America.
Trabalho multicêntrico desenvolvido no Hospital Universitário Cajuru, Pontifícia Universidade Católica do Paraná (PUCPR), Curitiba, PR e no Hospital Cristo Redentor, Porto Alegre, RS, Brasil.
Multicenter work developed at the Hospital Universitário Cajuru, Pontifícia Universidade Católica do Paraná (PUCPR), Curitiba, PR and the Hospital Cristo Redentor, Porto Alegre, RS, Brazil.
Referências
- 1.Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003;85(05):773–781. doi: 10.2106/00004623-200305000-00001. [DOI] [PubMed] [Google Scholar]
- 2.Jansson K A, Blomqvist P, Svedmark P et al. Thoracolumbar vertebral fractures in Sweden: an analysis of 13,496 patients admitted to hospital. Eur J Epidemiol. 2010;25(06):431–437. doi: 10.1007/s10654-010-9461-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.AOSpine Spinal Cord Injury & Trauma Knowledge Forum . Vaccaro A R, Oner C, Kepler C K et al. AOSpine thoracolumbar spine injury classification system: fracture description, neurological status, and key modifiers. Spine. 2013;38(23):2028–2037. doi: 10.1097/BRS.0b013e3182a8a381. [DOI] [PubMed] [Google Scholar]
- 4.Siebenga J, Leferink V J, Segers M J et al. Treatment of traumatic thoracolumbar spine fractures: a multicenter prospective randomized study of operative versus nonsurgical treatment. Spine. 2006;31(25):2881–2890. doi: 10.1097/01.brs.0000247804.91869.1e. [DOI] [PubMed] [Google Scholar]
- 5.Post R B, van der Sluis C K, Leferink V J, Dijkstra P U, ten Duis H J. Nonoperatively treated type A spinal fractures: mid-term versus long-term functional outcome. Int Orthop. 2009;33(04):1055–1060. doi: 10.1007/s00264-008-0593-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Vorlat P, Leirs G, Tajdar F, Hulsmans H, De Boeck H, Vaes P. Predictors of Recovery After Conservative Treatment of AO-Type A Thoracolumbar Spine Fractures Without Neurological Deficit. Spine. 2018;43(02):141–147. doi: 10.1097/BRS.0b013e3181cdb5fc. [DOI] [PubMed] [Google Scholar]
- 7.Pehlivanoglu T, Akgul T, Bayram S et al. Conservative Versus Operative Treatment of Stable Thoracolumbar Burst Fractures in Neurologically Intact Patients: Is There Any Difference Regarding the Clinical and Radiographic Outcomes? Spine. 2020;45(07):452–458. doi: 10.1097/BRS.0000000000003295. [DOI] [PubMed] [Google Scholar]
- 8.Wood K B, Buttermann G R, Phukan R et al. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: a prospective randomized study with follow-up at sixteen to twenty-two years. J Bone Joint Surg Am. 2015;97(01):3–9. doi: 10.2106/JBJS.N.00226. [DOI] [PubMed] [Google Scholar]
- 9.Yi L, Jingping B, Gele J, Baoleri X, Taixiang W. Operative versus non-operative treatment for thoracolumbar burst fractures without neurological deficit. Cochrane Database Syst Rev. 2006;(04):CD005079. doi: 10.1002/14651858.CD005079.pub2. [DOI] [PubMed] [Google Scholar]
- 10.Rometsch E, Spruit M, Härtl R et al. Does Operative or Nonoperative Treatment Achieve Better Results in A3 and A4 Spinal Fractures Without Neurological Deficit?: Systematic Literature Review With Meta-Analysis. Global Spine J. 2017;7(04):350–372. doi: 10.1177/2192568217699202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Butler J S, Walsh A, O'Byrne J. Functional outcome of burst fractures of the first lumbar vertebra managed surgically and conservatively. Int Orthop. 2005;29(01):51–54. doi: 10.1007/s00264-004-0602-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rajasekaran S. Thoracolumbar burst fractures without neurological deficit: the role for conservative treatment. Eur Spine J. 2010;19 01:S40–S47. doi: 10.1007/s00586-009-1122-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Aebi M. Classification of thoracolumbar fractures and dislocations. Eur Spine J. 2010;19 01:S2–S7. doi: 10.1007/s00586-009-1114-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Shen W J, Liu T J, Shen Y S. Nonoperative treatment versus posterior fixation for thoracolumbar junction burst fractures without neurologic deficit. Spine. 2001;26(09):1038–1045. doi: 10.1097/00007632-200105010-00010. [DOI] [PubMed] [Google Scholar]
- 15.Rabb C H, Hoh D J, Anderson P A et al. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines on the Evaluation and Treatment of Patients with Thoracolumbar Spine Trauma: Operative Versus Nonoperative Treatment. Neurosurgery. 2019;84(01):E50–E52. doi: 10.1093/neuros/nyy361. [DOI] [PubMed] [Google Scholar]
- 16.Cantor J B, Lebwohl N H, Garvey T, Eismont F J. Nonoperative management of stable thoracolumbar burst fractures with early ambulation and bracing. Spine. 1993;18(08):971–976. doi: 10.1097/00007632-199306150-00004. [DOI] [PubMed] [Google Scholar]
- 17.Bailey C S, Dvorak M F, Thomas K C et al. Comparison of thoracolumbosacral orthosis and no orthosis for the treatment of thoracolumbar burst fractures: interim analysis of a multicenter randomized clinical equivalence trial. J Neurosurg Spine. 2009;11(03):295–303. doi: 10.3171/2009.3.SPINE08312. [DOI] [PubMed] [Google Scholar]
- 18.Bailey C S, Urquhart J C, Dvorak M F et al. Orthosis versus no orthosis for the treatment of thoracolumbar burst fractures without neurologic injury: a multicenter prospective randomized equivalence trial. Spine J. 2014;14(11):2557–2564. doi: 10.1016/j.spinee.2013.10.017. [DOI] [PubMed] [Google Scholar]
- 19.Breivik H, Borchgrevink P C, Allen S M et al. Assessment of pain. Br J Anaesth. 2008;101(01):17–24. doi: 10.1093/bja/aen103. [DOI] [PubMed] [Google Scholar]
- 20.Roland M, Morris R. A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain. Spine. 1983;8(02):141–144. doi: 10.1097/00007632-198303000-00004. [DOI] [PubMed] [Google Scholar]
- 21.EuroQol Group . EuroQol–a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(03):199–208. doi: 10.1016/0168-8510(90)90421-9. [DOI] [PubMed] [Google Scholar]
- 22.Haywood K L, Garratt A M, Fitzpatrick R. Quality of life in older people: a structured review of generic self-assessed health instruments. Qual Life Res. 2005;14(07):1651–1668. doi: 10.1007/s11136-005-1743-0. [DOI] [PubMed] [Google Scholar]
- 23.Denis F, Armstrong G W, Searls K, Matta L. Acute thoracolumbar burst fractures in the absence of neurologic deficit. A comparison between operative and nonoperative treatment. Clin Orthop Relat Res. 1984;(189):142–149. [PubMed] [Google Scholar]
- 24.Sadatsune D A, Costa P P, Caffaro M F, Umeta R S, Meves R, Avanzi O. Thoracolumbar burst fracture: correlation between kyphosis and function after surgical treatment. Rev Bras Ortop. 2015;47(04):474–478. doi: 10.1016/S2255-4971(15)30131-2. [DOI] [PMC free article] [PubMed] [Google Scholar]