

Abstract
Background
Verrucous carcinoma is a low-grade variant of squamous cell carcinoma with specific morphologic, cytokinetic and clinical features. Despite low mitotic activity and slow growth, it can infiltrate adjacent tissues in advanced stages but does not metastasize. The most frequently affected site is the oral cavity. The following article provides latest updates in the etiology, clinical presentation, diagnostics and treatment options in oral verrucous carcinoma and discusses the existing dilemmas linked to this unique malignancy.
Conclusions
Oral verrucous carcinoma must be differentiated from conventional squamous cell carcinoma due to its less aggressive behaviour with a more favourable prognosis. Close communication between clinician and pathologist is mandatory for making a correct diagnosis. Primary surgery with negative surgical margins seems to be the most successful treatment. However, management recommendations are not uniform since they are mostly based on case reports and small retrospective case series. Prospective and pooled multi-institutional studies are therefore needed.
Key words: verrucous carcinoma, oral verrucous carcinoma, squamous cell carcinoma, diagnostics; differential diagnosis, treatment
Introduction
Head and neck cancer is the world’s seventh most common cancer with over 870,000 new cases in 2020. Lip and oral cavity malignancies accounted for almost half of them.1 More than 90% of oral cavity cancers arises from squamous epithelium.2 Verrucous carcinoma is a low-grade variant of squamous cell carcinoma (SCC) with specific morphologic, cytokinetic and clinical features.3 It is a locally aggressive tumour and does not metastasize to regional lymph nodes or to distant sites.4 In 1941, Friedell and Rosenthal first reported verrucous papillary lesions on the buccal mucosa in eight tobacco chewers.5 Seven years later, Ackerman described histopathologic and clinical features of this neoplasm. He defined it as a distinct clinicopathologic entity and introduced a term »verrucous carcinoma«.6
Verrucous carcinoma most often arises on mucous membranes of the head and neck region with the oral cavity most commonly involved, particularly buccal mucosa, gum and tongue.3 Oral verrucous carcinoma accounts for 0.57-16.08% of oral squamous cell carcinoma (SCC)7, 8, 9 and is predominantly seen in males with the reported mean age at diagnosis between 49 and 69.5 years.9, 10, 11 In a study by Koch et al., glottic larynx was the most frequently affected nonoral site.3 Other reported locations in the head and neck region affected by verrucous carcinoma are nasal cavity, paranasal sinuses, nasopharynx, oesophagus and temporal bone.12, 13, 14 Verrucous carcinoma on the skin and mucosa of the anogenital region and extremities are described in the literature as well.15,16
Etiology
The etiopathogenesis of oral verrucous carcinoma is not completely understood. As in conventional oral SCC, there is a strong association with alcohol consumption and inhaled as well as chewing tobacco use. Other irritants to the oral mucosa such as betel nut chewing, poor oral hygiene, a poorly fitting dental prosthesis and earlier mucosal injuries or scars have also been described as risk factors in the development of oral verrucous carcinoma.9,17, 18, 19 There is growing evidence that oral microbiota and its imbalances may play a role in the etiology of oral cancers through activation of smoking and alcohol related carcinogens locally and chronic inflammation systemically.20 Human papillomaviruses (HPVs) have been considered as a possible etiologic factor in verrucous carcinoma, with the reported prevalence of HPV in verrucous carcinoma ranging from 0% to 100%.21, 22, 23 However, using highly sensitive and specific molecular methods, it has been shown that HPVs are not associated with the etiopathogenesis of verrucous carcinoma of the head and neck. Furthermore, no evidence of transcriptionally active high-risk α-HPV was found in verrucous carcinoma by real-time polymerase chain reaction (RT-PCR) for HPV E6/E7 messenger ribonucleic acid (mRNA). It appears that verrucous carcinoma of the head and neck is not associated with infection with HPV.4,24, 25
Clinical presentation
Verrucous carcinoma is characterized by low mitotic activity reflecting in slow growth7; hence it can take several years to reach the size that causes symptoms. Patients may report oral discomfort, difficulty chewing or swallowing, and bad breath. Pain usually indicates tumour invasion into the surrounding structures.26,27
Oral verrucous carcinoma typically appears as an exophytic broad-based lesion with a cauliflower-like warty surface28 as presented in Figure 1. Despite its slow growth, it can reach a significant size and infiltrate adjacent tissues such as muscles and bone.3 However, even when locally advanced, oral verrucous carcinoma has no tendency to metastasize to regional lymph nodes and distant sites.4 Cervical lymphadenopathy is commonly seen at initial clinical or radiological examination and is mostly considered reactive secondary to inflammation at the tumour-stromal interface.3
Figure 1.
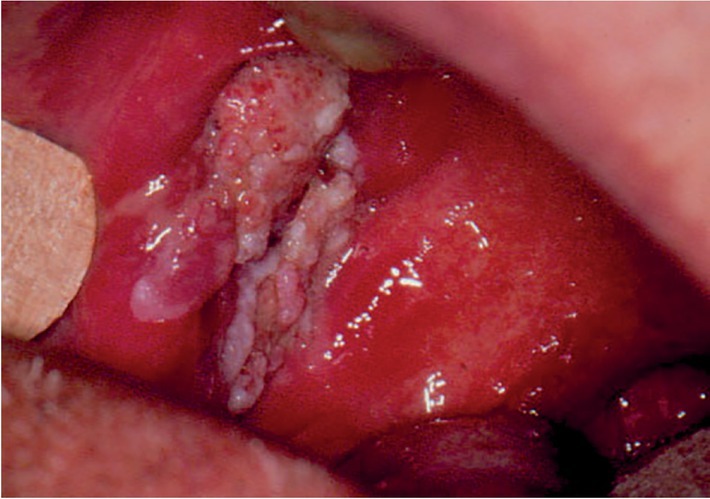
Verrucous carcinoma of the right buccal mucosa (clinical stage T2N0M0) in an 81-year-old male patient. He presented with a whitish exophytic tumour mass of the inner side of the right cheek and without suspicious lymph nodes on the neck. The lesion was noticed by the patient a month before initial examination, and it occasionally hurt, but he had no problems feeding. Due to associated diseases, he was treated with radiotherapy (55 Gy, 2.2 Gy/fraction) and concurrent intravenous chemotherapy (vinblastine 2 mg, day 1; methotrexate 50 mg, day 2; bleomycin 15 mg, days 2 and 3). The patient died of injury 5.5 years after completion of treatment for verrucous carcinoma with no evidence of malignant disease in oral cavity.
Initial reports of neck metastasis in verrucous carcinoma were later attributed to incorrect pathologic diagnosis or to a presence of foci of conventional SCC of varying degree of differentiation within a verrucous carcinoma. The so-called hybrid verrucous carcinoma was first described by Batsakis et al. in 1982 in three verrucous lesions of the larynx.29 Medina et al. later reported coexistence of verrucous carcinoma and conventional SCC in 20% of 104 patients with oral verrucous carcinoma.30 In contrast to the classic, histologically uniform verrucous carcinoma, a hybrid verrucous carcinoma is capable of metastasizing and must therefore be managed as a more common and aggressive conventional SCC.31 However, it is not possible to differentiate these lesions at clinical examination due to similar appearance. Moreover, examination of small tumour samples obtained with biopsy could be misleading as an invasive component is often missed at sampling.32 Gokavarapu et al. reported that 51% of cases preoperatively diagnosed as oral verrucous carcinoma or its benign precursors were actually hybrid lesions.33 Although multiple biopsies from different areas of the tumour might be helpful to identify invasive component, surgical excision and histopathological examination of whole resection specimen is needed for definitive diagnosis.32 If hybrid verrucous carcinoma is recognized, the pathologist should quantitate each component of the tumour, define the degree of differentiation of the conventional SCC component and comment on depth of the tumour invasion, potential presence of lymphatic or perineural invasion and the adequacy of the resection margins. These features help the clinicians to decide about adjuvant treatment options.31
Various mucosal abnormalities including verrucous hyperplasia and dysplasia are frequently found adjacent to the oral verrucous carcinoma supporting the view that verrucous carcinoma develops from precursor lesions.28 Patients with oral verrucous carcinoma are also at high risk of developing metachronous second primary tumours. This can be explained with the concept of »field cancerization« proposed by Slaughter et al. who postulated that prolonged exposure of the upper aerodigestive tract to carcinogens leads to genomic instability even beyond the area of clinically and histopathologically evident mucosal changes.34
Diagnostics and differential diagnosis
Diagnosis of oral verrucous carcinoma is based on a patient’s history, clinical manifestation and histopathologic features of the lesion. However, establishing the correct diagnosis is often difficult due to other oral lesions with often similar verrucous presentation and/or insufficient biopsy specimen as well.9 Medical history should include information on the duration of the growth of the lesion and potential etiologic factors (smoking, alcohol abuse). Computed tomography (CT) and/or magnetic resonance imaging (MRI) is helpful to determine local extent of the lesion with potential invasion to surrounding structures and to exclude tumour spread to regional lymph nodes.35
The clinician’s impression of a malignant lesion frequently does not match its benign nature described in the histopathology report. Therefore, biopsies are often repeated, which can significantly delay the start of a treatment.10,36 Close communication between the clinician and the pathologist is therefore of the utmost importance.33
Microscopically, verrucous carcinoma consists of filiform projections lined by thick, well-differentiated keratinized squamous epithelium, composed of one to a few layers of basal cells, and multiplied, voluminous spinous cells lacking cytological atypia. It invades the underlying stroma with a well-defined, pushing margin.37 When oral verrucous carcinoma is highly suspicious by clinical appearance, it is recommended that the lesion is surgically excised if not too extensive.38
Lesions in oral cavity with a verrucous appearance may belong to a broad spectrum, extending from verrucous hyperplasia, proliferative verrucous leukoplakia, oral squamous papilloma, oral verrucous carcinoma, hybrid oral verrucous carcinoma to conventional oral SCC with an exophytic growth pattern (Figure 2). It is difficult to distinguish them clinically from each other; they may also coexist.39
Figure 2.

Histopathology images of oral verrucous lesions. Squamous cell papilloma (A) exophytic lesion, composed of finger-like projections, lined by non-keratinizing stratified squamous epithelium and a central connective tissue core. Verrucous hyperplasia (B) exophytic lesion, composed of hyperplastic keratinizing squamous epithelium with no invasion into the underlying stroma. Verrucous carcinoma (C) exophytic tumour, resembling verrucous hyperplasia, but with invasive growth, consisting of broad epithelial islands and processes, with no atypia, exhibiting a pushing-border into the underlying stroma.
Oral verrucous hyperplasia resembles oral verrucous carcinoma both clinically and histopathologically. It presents as a white elevated mucosal plaque or mass with exophytic verrucous surface. In oral verrucous hyperplasia and oral verrucous carcinoma, hyperplastic epithelium is superficial to adjacent normal mucosa, but in oral verrucous carcinoma, broad epithelial processes also extend deeper, exhibiting a pushing-border invasion into the underlying connective tissue but the basement membrane remains intact.40 Therefore, it was suggested that oral verrucous carcinoma can be best differentiated from oral verrucous hyperplasia with biopsies taken from the deep portion and the margin of the tumour where adjacent normal mucosa is evident to compare.33 Oral verrucous hyperplasia is an irreversible precancerous lesion that may transform into oral verrucous carcinoma. Wang et al. reported a 10% of malignant transformation rate in their series of 60 oral verrucous hyperplasia cases. Thus, once diagnosed, oral verrucous hyperplasia should be treated as oral verrucous carcinoma.41
Proliferative verrucous leukoplakia is an aggressive form of nonhomogeneous multifocal oral leukoplakia characterized by a progressive clinical course with changing clinical and histopathologic features. It is more commonly seen among elderly women. Although etiology of proliferative verrucous leukoplakia remains unclear, it seems that consumption of tobacco and alcohol does not play a role.42 Proliferative verrucous leukoplakia usually begins as a single white mucosal plaque that eventually becomes multifocal with exophytic, verrucous or erythematous appearance. Its description includes a histopathological continuum ranging from benign hyperkeratosis to lesions with increasing degree of dysplasia. Therefore, proliferative verrucous leukoplakia has no specific histological features and microscopic findings depend on the histopathologic stage of proliferative verrucous leukoplakia.43 According to the World Health Organization, proliferative verrucous leukoplakia is a potentially malignant disorder with the highest rate of malignant transformation either to oral verrucous carcinoma or conventional oral SCC.42 In addition, several authors proposed different clinical and histopathological criteria for diagnosing proliferative verrucous leukoplakia.44,45 In the meta-analysis by Palaia et al. which included 22 studies with a total of 699 proliferative verrucous leukoplakia patients, a malignant transformation rate of proliferative verrucous leukoplakia was 45.8%.46 Thus, once proliferative verrucous leukoplakia is confirmed, active therapy should be undertaken, such as surgery, laser ablation, photodynamic therapy or radiotherapy.47 However, proliferative verrucous leukoplakia responds poorly to various treatment modalities and its recurrence rate is high, even after surgical removal.48
Squamous cell papilloma (SCP) in the oral cavity appears as a pink to white mucosal exophytic lesion with a warty or granular surface. It is most commonly caused by HPV type 6 and type 11, tends to progress slowly and has a very low risk of becoming malignant. SCP is possible to differentiate from oral verrucous carcinoma microscopically. In contrast to oral verrucous carcinoma which shows epithelial processes with downgrowth into the underlying connective tissue, SCP presents with long, thin and finger-like projections, extending above the mucosal surface. Each of these projections is lined by stratified squamous epithelium and contains a central connective tissue core.49
Conventional oral SCC most commonly presents as an ulcerated mucosal lesion with necrotic central area, surrounded by irregular raised and indurated borders. However, an exophytic growth with a smooth, ulcerated or verrucous surface may also be seen.50,51 In comparison to oral verrucous carcinoma, conventional oral SCC is histopathologically marked by a greater degree of atypia and mitotic activity of the tumour cells and invasion beyond the basement membrane.31 It grows more rapidly, frequently metastasizes to the regional and distant sites and has a worse prognosis.8 Oral verrucous carcinoma with foci of conventional SCC can be found at histopathological examination, which dictates treatment choices and prognosis.31
Molecular biomarkers
The development of oral verrucous carcinoma is modulated by genetic predisposition and environmental influences resulting in a wide range of genetic and epigenetic alterations that can be detected by various tumour markers. Molecular mechanisms of oral verrucous carcinoma are therefore increasingly being investigated. Although many different molecules associated with diagnosis, tumour progression and prognosis of oral verrucous carcinoma have been proposed, a reliable and effective biomarker has still not been identified.35
Genetic studies have shown that several genes are differently expressed between oral verrucous carcinoma and oral SCC.52 Most investigated markers in carcinogenesis of oral verrucous carcinoma are p5353,54, Ki-6753,55,56, cyclin-B156,57 and cyclin-D1.58 Except for Ki-67, their expression levels were significantly higher in conventional oral SCC than in oral verrucous carcinoma. Tumour suppression markers p21 and p27 may not be of much diagnostic use in distinguishing oral verrucous carcinoma from oral verrucous hyperplasia 59 and oral SCC.54,60 Components of extracellular matrix and basement membrane play an important role in tumour invasion and metastasis. Oral verrucous carcinoma is associated with lower expression of matrix metal-loproteinase 9 (MMP-9)53 and higher expression of laminin61 in comparison to oral SCC. Laminin and type IV collagen are good markers for basement membrane integrity and their discontinuity is more evident in severe oral epithelial dysplasia than in verrucous carcinoma.61 Among cell surface proteins, high level of expression of glucose transporter 1 (GLUT-1) in both oral SCC and oral verrucous carcinoma could differentiate them from oral epithelial dysplasia.62 Oral SCC could be distinguished from oral verrucous carcinoma based on a higher density of CD68 (marking tumour associated macrophages) and CD31 (marking microvessel density) found in immunohistochemical studies.63 Regarding cytoskeletal proteins, CK20 is highly expressed in oral verrucous carcinoma and oral SCC but not in benign squamous lesions64, and CD34 along with α-smooth muscle actin (α-SMA) seem to be helpful in the diagnosis of oral verrucous hyperplasia.65 Different expression of desmosomal proteins (up-regulation of plakophilin 1, desmoglein 2, desmoglein 3, desmoplakin), microRNA (miRNA) molecules (up-regulation of miRNA-203, down-regulation of miRNA-125a-5p, miRNA-125b) and proteins (down-regulation of p63) in verrucous carcinoma is useful in differentiation from conventional SCC and detecting foci of SCC in hybrid verrucous carcinoma as well.37,66
Treatment
Due to the rarity of oral verrucous carcinoma, treatment recommendations found in the literature is mostly based on case reports and small retrospective case series, and are consequently not uniform. The treatment modalities available include surgery, radiotherapy, chemotherapy, or combinations thereof.
Surgery
Wide surgical excision is usually considered the treatment of choice because of the wide spectrum of reconstruction possibilities of the resulting tissue defect in the oral cavity with good functional results, and encouraging locoregional control and survival rates.17,38,67 However, there is ongoing debate about the optimal width of surgical margins and the need for elective neck dissection (END). Similar to conventional oral SCC, clinical surgical margin of 10–15 mm and histological margin of at least 5 mm are still generally considered sufficient to not increase the risk of local recurrence of oral verrucous carcinoma68, 69, 70, although no worse outcomes were reported in patients with close histological margins (i.e. less than 5 mm) who did not receive adjuvant radiotherapy.10 Since histologically pure oral verrucous carcinoma does not metastasize, END is usually not performed during primary surgery but is indicated in hybrid oral verrucous carcinoma and when microvascular flap is used for reconstruction of tumour defect.10,67,68 Some authors advocate a selective supraomohyoid neck dissection (neck levels I–III) also in patients with advanced primary tumour stages (cT3–4) and/or clinically overt lymphadenopathy. However, in several studies, no patient with END had histologically proven nodal metastasis.10,17,38,71
Radiotherapy
Oral verrucous carcinoma is thought to be less sensitive to radiotherapy than conventional oral SCC.72,73 Radiotherapy targets DNA in rapidly dividing cells, whereas studies on cytokinetic characteristics of verrucous carcinoma have shown that only low proportion of tumour cells are in S-phase compartment of the cell cycle during which DNA is synthesized, corresponding to a low mitotic activity of this tumour and reduced susceptibility to irradiation.29 Mohan et al. demonstrated that patients with oral verrucous carcinoma who received postoperative radiotherapy trended toward worse disease-specific survival (DSS) than those with oral SCC, suggesting relative radioresistance of oral verrucous carcinoma.7
Studies reporting local control rate and survival rate for upfront surgery and primary radiotherapy are summarized in Table 1 and Table 2.
Table 1.
Primary surgery in the treatment of oral verrucous carcinoma - review of the literature series
| Authors and study year | Number patients of | Local control (%) | Survival | Follow-up time |
|---|---|---|---|---|
| Kraus 196674 and Perezmesa, | 64 | 55 (85.9) | N.S. | N.S. |
| Medina 198430 et al, | 90 | 74 (82.2) | N.S. | At least 2 years |
| Jyothirmayi 19978 et al, | 11 | N.S. | 5-year DFS 68% | Median (range 56 7months –110) |
| Koch 20013 et al, | 484 | N.S. | 5-year RSR 85.7% | N.S. |
| Kang 200338 et al, | 38 | 38 (100) at 3 years | 3-year OSR 94.7% | Median 37.5 13months –76) (range |
| Walvekar 200917 et al, | 101 | 80 (79.2) | 5-year DFS 77.6% | Median (range 4.61 0.5–years 14.3) |
| Huang et al, 200967 | 39 | 38 (97.4) | 5-year CSS 89.1% | Median 90 months (range, 13–171) |
| Candau-Alvarez et al, 201468 | 13 | 12 (92.3) | OSR 92.9% for a mean follow-up of 2 years | Mean 24.8 months (range 6–53) |
| Franklyn et al, 201710 | 22 | 21 (95.5) (recurrence in a patient with hybrid OVC) | N.S. | Median 24 months |
CSS = cancer specific survival; DFS = disease free survival; N.S. = not specified; OSR = overall survival rate; OVC = oral verrucous carcinoma; RSR = relative survival rate
Table 2.
Primary radiotherapy in the treatment of oral verrucous carcinoma - review of the literature series
| Authors and study year | Number of patients | Local control rate with primary radiotherapy (%) | Surgical salvage | Local control rate with primary radiotherapy and salvage surgery (%) | Survival | Follow-up time |
|---|---|---|---|---|---|---|
| Kraus 196674 and Perezmesa, | 13 | 0 (0) | 8/13 | 7 (53.8) | N.S. | N.S. |
| Memula 198075 et al, | 32 | 19 (59.4) | 6/13 | 25 (78.1) | 5-year 31% DFS | N.S. |
| Medina 198430 et al, | 12 | 7 (58.3) | 3/5 | 10 (83.3) | N.S. | At least 2 years |
| Nair 1988et 76 al, | 50 | 22 (44) at 3 years | 4/28 | N.S. | 3-year 44% DFS | At least 3 years |
| Vidysagar et al, 199236 | 107 | 55 (51.4) (residual disease in 19 patients, recurrence in 33 patients) | 20/52 | N.S. | 5-year DFS 49% | Range 6–60 months |
| Jyothirmayi et al, 19978 | 42 | 16 (38.1) (residual disease in 10 patients, recurrence in 16 patients) | 9/26 | N.S. | 5-year DFS 66% | Median 56 months (range 7–110) |
| Koch 20013 et al, | 33 | N.S. | N.S. | N.S. | 5-year 41.8% RSR | N.S. |
DFS = disease free survival; N.S. = not specified; OVC = oral verrucous carcinoma; RSR = relative survival rate
However, a fair comparison between oncological results of surgery and radiotherapy is difficult to make due to obvious lack of well-designed prospective studies or even comparisons. In most series, patients were recruited over a longer time period which resulted in suboptimal treatments in at least part of these patients. Thus, local control and survival rates of irradiated patients must be interpreted with caution and understanding that irradiation techniques and fractionation schemes used in the past changed significantly over time. Nevertheless, radiotherapy is an acceptable alternative to surgery for patients who refuse proposed operation or are medically unfit for major surgery as well as in whom surgery would cause an important functional and/or cosmetic impairment.77 In cases of radiotherapy failure, surgical salvage remains an option.78
In the past, radiotherapy was burdened with the phenomenon of anaplastic transformation which assumed the possibility of conversion of verrucous carcinoma to a less-differentiated SCC after irradiation.79 In older literature, its incidence has been reported to be as high as 30%.80 Recently, different authors questioned the concept of this phenomenon and raised the possibility of hybrid lesions containing foci of conventional SCC that had been missed at the initial biopsy and not controlled by irradiation, resulting in tumour recurrence.3,79,81 This hypothesis is further justified by the reports of anaplastic transformation following primary surgery as well, probably due to the same reason as in the case of radiotherapy, i.e. an incorrect histopathologic diagnosis.73
Postoperative radiotherapy
The benefit of postoperative radiotherapy (PORT) in oral verrucous carcinoma is controversial. The decision about PORT usually follows recommendations for patients with conventional oral SCC (i.e. positive or close surgical margins, pT3–T4 primary tumour, perineural and lymphovascular invasion).67,82 Analysing the SEER database, however, Mohan et al. demonstrated a statistically significant improvement in DSS in patients solely operated compared to those receiving surgery and PORT.7 In a recent retrospective cohort study of the National Cancer Database (NCDB), Naik et al. showed that positive surgical margins were associated with significantly worse overall survival (OS) (hazard ratio [HR] 2.85, P = 0.006).82 However, in those patients the use of PORT showed no OS benefit (HR 3.12, P = 0.072). These findings suggest that the role of PORT is limited in oral verrucous carcinoma, favouring surgical re-resection, when feasible, over adjuvant radiotherapy in patients with adverse pathologic features or clinically overt residual tumour after surgery.82
Chemotherapy
Experiences with chemotherapy, alone or in combination with other modalities, in oral verrucous carcinoma are scarce.83 Chemotherapy can be implemented in a neo-adjuvant setting to reduce tumour size before subsequent surgery, which is expected to be less extensive and mutilating, resulting in better functional and cosmetic outcome.84 It can also be used as a salvage treatment for patients with recurrent disease and to palliate symptoms in advanced tumours not suitable for aggressive radical treatment.85,86 Although the data on the use of older chemotherapy drugs are available in the literature, there is no information on the use of modern drugs (targeted agents, check-point inhibitors) in oral verrucous carcinoma.
Encouraging results were reported by Wu et al. using intra-arterial methotrexate infusion as a primary therapy in 15 patients with oral verrucous carcinoma. Despite locally advanced T3–4 tumours in eight of these patients, a complete tumour remission was observed in all patients who were without disease recurrence at a mean follow-up of 42 months.83 Karkazoglou et al. reported on 12 oral verrucous carcinoma patients who had also been treated with methotrexate, given by various routes and in different doses, because of either the extent of the tumour or poor general condition of the patient. Only one patient failed to respond. Authors concluded that methotrexate reduced morbidity and improved quality of life with minimal and reversible toxicity.87 Preliminary observations in two elderly patients with locally advanced oral verrucous carcinoma showed that single cycle of oral fluoropyrimidine capecitabine induced rapid and clinically significant response with near complete resolution of oral lesions within 3 weeks of initiating therapy. A durable partial response was seen at 6 months and 1 year and was associated with significant improvement in life quality with acceptable toxicity profile.88
Chemoradiotherapy
In addition, chemotherapy can be given simultaneously with radiotherapy. In a group of 12 patients with previously untreated verrucous carcinoma of different head and neck mucosal sites, concurrent chemoradiotherapy with at least two cycles of intravenous vinblastine, methotrexate and bleomycin and radiotherapy dose of 44–70 Gy (median 65.2 Gy) resulted in local control (median follow-up of 3.4 years) in 11 patients, nine of whom had advanced T3–4 tumours.85 Authors concluded that concomitant chemotherapy seems to successfully compensate lower effectiveness of radiotherapy in verrucous carcinoma and even allows reduction of radiation dose bellow the standard 66–70 Gy, and, therefore, alleviates its toxicity and contributes to organ sparing.84 Promising results of chemoradiotherapy were also reported by Yoshimura et al. using 5-fluorouracil and its analogues.89
Non-surgical techniques
Non-surgical methods are well established treatment modalities in low risk nonmelanoma skin cancers and to some extent in oral benign and precancerous lesions but there are only a few case reports regarding their use in oral verrucous carcinoma.
Cryotherapy acts by freezing a lesion in situ which leads to disruption of cell membranes, damage of tumour vasculature, activation of cytotoxic immune mechanisms and finally cell necrosis.90 Yeh et al. reported clinically complete response to shave excision and subsequent cryotherapy with liquid nitrogen in 11 of 18 patients with oral verrucous hyperplasia and oral verrucous carcinoma. After a mean follow-up of 23 months, recurrence was found in three cases and all were successfully treated by the same technique.91
Photodynamic therapy (PDT) is based on topical or systemic administration of an exogenous photosensitiser which increases tumour tissue sensitiveness to light of a specific wavelength.92 It mediates tumour destruction by creating oxygen free radicals, damaging tumour vasculature and activating immune response against tumour cells. Chen et al. reported a complete clinical regression and no tumour recurrence at 6 months follow-up after 22 cycles of PDT using topical 5-aminole-vulinic acid followed by multiple fractionated irradiations with LED red light in a 56-year-old male with oral verrucous carcinoma extending from mouth angle to buccal mucosa.93 In order to better expose deeper part of the lesion under mucosal surface to cryotherapy or PDT and make a definitive histopathologic diagnosis, its exophytic part may initially be removed with debulking methods such as shave or laser excision.91
CO2 laser destructs a lesion with tissue vaporization and is therefore proposed for treatment of tumours involving cosmetically critical areas such as lips, where wide surgical excision may lead to unacceptable aesthetic and/or functional impairment.94 Several authors reported good clinical response with complete tumour removal and no recurrence in a follow-up from 15 to 48 months.94, 95, 96
Described procedures are non-invasive and can be safely carried out in a local anaesthesia in the outpatient clinic. Other reported advantages are short procedure duration, ability to treat multifocal lesions, limited pain and scarring, fast homeostasis and healing process, low risk of secondary infection and little or no side effects.91,93,95 However, their effect is limited by a depth of agent penetration, which therefore makes them suitable only for a treatment of superficial oral lesions.92 They also lack working precision since it is difficult to judge the final extent of tissue necrosis during a procedure. Moreover, tumour resolution can only be assessed clinically and not histopathologically.91 Large-scale clinical studies with longer follow-up are further necessary to evaluate their effectiveness in the management of oral verrucous carcinoma.
Conclusions
Oral verrucous carcinoma is a rare variant of oral SCC that must be differentiated from conventional SCC due to its locally invasive and non-metastasizing behaviour with a more favourable prognosis. For making a correct diagnosis, close communication between clinician and pathologist is mandatory. Primary surgery with negative surgical margins seems to be the optimal treatment for patients with oral verrucous carcinoma; whether to perform the END remains controversial. The concern about anaplastic transformation after irradiation should not affect the decision on treatment with radiotherapy which is usually proposed to patients with extensive tumours or patients in poor general condition. The role of systemic therapy, particularly immunotherapy and targeted therapy, and non-surgical treatment methods are yet to be defined. Due to rarity of the disease, pooled multi-institutional analyses are warranted to properly address opened questions.
Acknowledgments
This review was funded by the Slovenian Research Agency (ARRS), grant number P3-0307.
Disclosure
No potential conflicts of interest were disclosed.
References
- 1.Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–49. doi: 10.3322/caac.21660. et al. doi. [DOI] [PubMed] [Google Scholar]
- 2.Van Dijk BAC, Brands MT, Geurts SME, Merkx MAW, Roodenburg JLN. Trends in oral cavity cancer incidence, mortality, survival and treatment in the Netherlands. Int J Cancer. 2016;139:574–83. doi: 10.1002/ijc.30107. doi. [DOI] [PubMed] [Google Scholar]
- 3.Koch BB, Trask DK, Hoffman HT, Karnell LH, Robinson RA, Zhen W. National survey of head and neck verrucous carcinoma: patterns of presentation, care, and outcome. Cancer. 2001;92:110–20. doi: 10.1002/1097-0142(20010701)92:1<110::AID-CNCR1298>3.0.CO;2-K. et al. doi. [DOI] [PubMed] [Google Scholar]
- 4.Patel KR, Chernock RD, Zhang TR, Wang X, El-Mofty SK, Lewis JSJ. Verrucous carcinomas of the head and neck, including those with associated squamous cell carcinoma, lack transcriptionally active high-risk human papillomavirus. Hum Pathol. 2013;44:2385–92. doi: 10.1016/j.humpath.2013.07.011. doi. [DOI] [PubMed] [Google Scholar]
- 5.Friedell HL, Rosenthal LM. The etiologic role of chewing tobacco in cancer of the mouth: report of eight cases treated with radiation. J Am Med Assoc. 1941;116:2130–5. doi: 10.1001/jama.1941.02820190006002. doi. [DOI] [Google Scholar]
- 6.Ackerman LV. Verrucous carcinoma of the oral cavity. Surgery. 1948;23:670–8. PMID: 18907508. [PubMed] [Google Scholar]
- 7.Mohan S, Pai SI, Bhattacharyya N. Adjuvant radiotherapy is not supported in patients with verrucous carcinoma of the oral cavity. Laryngoscope. 2017;127:1334–8. doi: 10.1002/lary.26443. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Jyothirmayi R, Sankaranarayanan R, Varghese C, Jacob R, Nair MK. Radiotherapy in the treatment of verrucous carcinoma of the oral cavity. Oral Oncol. 1997;33:124–8. doi: 10.1016/S0964-1955(96)00059-0. doi. [DOI] [PubMed] [Google Scholar]
- 9.Rekha KP, Angadi PV. Verrucous carcinoma of the oral cavity: a clinicopathologic appraisal of 133 cases in Indians. Oral Maxillofac Surg. 2010;14:211–8. doi: 10.1007/s10006-010-0222-0. doi. [DOI] [PubMed] [Google Scholar]
- 10.Franklyn J, Janakiraman R, Tirkey AJ, Thankachan C, Muthusami J. Oral verrucous carcinoma: ten year experience from a tertiary care hospital in India. Indian J Med Paediatr Oncol. 2017;38:452–5. doi: 10.4103/ijmpo.ijmpo_153_16. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Alonso JE, Kuan EC, Arshi A, St. John MA. A population-based analysis of verrucous carcinoma of the oral cavity. Laryngoscope. 2018;128:393–7. doi: 10.1002/lary.26745. doi. [DOI] [PubMed] [Google Scholar]
- 12.Alonso JE, Han AY, Kuan EC, Suh JD, John MAS. Epidemiology and survival outcomes of sinonasal verrucous carcinoma in the United States. Laryngoscope. 2018;128:651–6. doi: 10.1002/lary.26790. doi. [DOI] [PubMed] [Google Scholar]
- 13.Sweetser S, Jacobs NL, Wong Kee Song LM. Endoscopic diagnosis and treatment of esophageal verrucous squamous cell cancer. Dis Esophagus. 2014;27:452–6. doi: 10.1111/j.1442-2050.2012.01434.x. doi. [DOI] [PubMed] [Google Scholar]
- 14.Miller ME, Martin N, Juillard GF, Bhuta S, Ishiyama A. Temporal bone verrucous carcinoma: outcomes and treatment controversy. Eur Arch Oto-Rhino-Laryngology. 2010;267:1927–31. doi: 10.1007/s00405-010-1281-4. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Prince ADP, Harms PW, Harms KL, Kozlow JH. Verrucous carcinoma of the foot: a retrospective study of 19 cases and analysis of prognostic factors influencing recurrence. Cutis. 2022;109:E21–8. doi: 10.12788/cutis.0499. doi. [DOI] [PubMed] [Google Scholar]
- 16.Koch H, Kowatsch E, Hödl S, Smola MG, Radl R, Hofmann T. Verrucous carcinoma of the skin: long-term follow-up results following surgical therapy. Dermatol Surg. 2004;30:1124–30. doi: 10.1111/j.1524-4725.2004.30338.x. et al. doi. [DOI] [PubMed] [Google Scholar]
- 17.Walvekar RR, Chaukar DA, Deshpande MS, Pai PS, Chaturvedi P, Kakade A. Verrucous carcinoma of the oral cavity: a clinical and pathological study of 101 cases. Oral Oncol. 2009;45:47–51. doi: 10.1016/j.oraloncology.2008.03.014. et al. doi. [DOI] [PubMed] [Google Scholar]
- 18.Gokavarapu S, Parvataneni N, Charan CR, Puthamakula S, Kulkarni G, Reddy BS. Multi centricity of oral verrucous carcinoma: a case series of 22 cases. Indian J Otolaryngol Head Neck Surg. 2015;67:138–42. doi: 10.1007/s12070-015-0835-6. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Rahali L, Omor Y, Mouden K, Mahdi Y, Elkacemi H, Elmajjaoui S. Oral verrucous carcinoma complicating a repetitive injury by the dental prosthesis: a case report. Pan Afr Med J. 2015;20:297. doi: 10.11604/pamj.2015.20.297.6135. et al. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ahn J, Chen CY, Hayes RB. Oral microbiome and oral and gastrointestinal cancer risk. Cancer Causes Control. 2012;23:399–404. doi: 10.1007/s10552-011-9892-7. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Johnson TL, Plieth DA, Crissman JD, Sarkar FH. HPV detection by polymerase chain reaction (PCR) in verrucous lesions of the upper aerodigestive tract. Mod Pathol. 1991;4:461–5. [PubMed] [Google Scholar]
- 22.Fliss DM, Noble-Topham SE, McLachlin M, Freeman JL, Noyek AM, van Nostrand AW. Laryngeal verrucous carcinoma: a clinicopathologic study and detection of human papillomavirus using polymerase chain reaction. Laryngoscope. 1994;104:146–52. doi: 10.1288/00005537-199402000-00005. et al. doi. [DOI] [PubMed] [Google Scholar]
- 23.Mitsuishi T, Ohara K, Kawashima M, Kobayashi S, Kawana S. Prevalence of human papillomavirus DNA sequences in verrucous carcinoma of the lip: genomic and therapeutic approaches. Cancer Lett. 2005;222:139–43. doi: 10.1016/j.canlet.2004.09.019. doi. [DOI] [PubMed] [Google Scholar]
- 24.del Pino M, Bleeker MCG, Quint WG, Snijders PJF, Meijer CJLM, Steenbergen RDM. Comprehensive analysis of human papillomavirus prevalence and the potential role of low-risk types in verrucous carcinoma. Mod Pathol. 2012;25:1354–63. doi: 10.1038/modpathol.2012.91. doi. [DOI] [PubMed] [Google Scholar]
- 25.Odar K, Kocjan BJ, Hošnjak L, Gale N, Poljak M, Zidar N. Verrucous carcinoma of the head and neck - not a human papillomavirus-related tumour? J Cell Mol Med. 2014;18:635–45. doi: 10.1111/jcmm.12211. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Terada T. Verrucous carcinoma of the oral cavity: a histopathologic study of 10 Japanese cases. J Maxillofac Oral Surg. 2011;10:148–51. doi: 10.1007/s12663-011-0197-x. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kamath VV, Varma RR, Gadewar DR, Muralidhar M. Oral verrucous carcinoma. An analysis of 37 cases. J Craniomaxillofac Surg. 1989;17:309–14. doi: 10.1016/s1010-5182(89)80059-9. doi. [DOI] [PubMed] [Google Scholar]
- 28.Sonalika W, Anand T. Oral verrucous carcinoma: a retrospective analysis for clinicopathologic features. J Cancer Res Ther. 2016;12:142–5. doi: 10.4103/0973-1482.172709. doi. [DOI] [PubMed] [Google Scholar]
- 29.Batsakis JG, Hybels R, Crissman JD, Rice DH. The pathology of head and neck tumors: verrucous carcinoma, part 15. Head Neck Surg. 1982;5:29–38. doi: 10.1002/hed.2890050107. doi. [DOI] [PubMed] [Google Scholar]
- 30.Medina JE, Dichtel W, Luna MA. Verrucous-squamous carcinomas of the oral cavity: a clinicopathologic study of 104 cases. Arch Otolaryngol. 1984;110:437–40. doi: 10.1001/archotol.1984.00800330019003. doi. [DOI] [PubMed] [Google Scholar]
- 31.Devaney KO, Ferlito A, Rinaldo A, El-Naggar AK, Barnes L. Verrucous carcinoma (carcinoma cuniculatum) of the head and neck: what do we know now that we did not know a decade ago? Eur Arch Otorhinolaryngol. 2011;268:477–80. doi: 10.1007/s00405-011-1495-0. doi. [DOI] [PubMed] [Google Scholar]
- 32.Gokavarapu S, Rao.S LMC, Tantravahi US, Gundimeda SD, Rao TS, Murthy S. Oral hybrid verrucous carcinoma: a clinical study. Indian J Surg Oncol. 2014;5:257–62. doi: 10.1007/s13193-014-0345-0. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Gokavarapu S, Chandrasekhara Rao LM, Patnaik SC, Parvataneni N, Raju KVVN, Chander R. Reliability of incision biopsy for diagnosis of oral verrucous carcinoma: a multivariate clinicopathological study. J Maxillofac Oral Surg. 2015;14:599–604. doi: 10.1007/s12663-014-0715-8. et al. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Slaughter DP, Southwick HW, Smejkal W. Field cancerization in oral stratified squamous epithelium; clinical implications of multicentric origin. Cancer. 1953;6:963–8. doi: 10.1002/1097-0142(195309)6:5<963::aidcncr2820060515>3.0.co;2-q. doi. [DOI] [PubMed] [Google Scholar]
- 35.Peng Q, Wang Y, Quan H, Li Y, Tang Z. Oral verrucous carcinoma: from multifactorial etiology to diverse treatment regimens (review) Int J Oncol. 2016;49:59–73. doi: 10.3892/ijo.2016.3501. doi. [DOI] [PubMed] [Google Scholar]
- 36.Vidyasagar MS, Fernandes DJ, Kasturi DP, Akhileshwaran R, Rao K, Rao S. Radiotherapy and verrucous carcinoma of the oral cavity: a study of 107 cases. Acta Oncol. 1992;31:43–7. doi: 10.3109/02841869209088264. et al. doi. [DOI] [PubMed] [Google Scholar]
- 37.Odar K, Boštjančič E, Gale N, Glavač D, Zidar N. Differential expression of microRNAs miR-21, miR-31, miR-203, miR-125a-5p and miR-125b and proteins PTEN and p63 in verrucous carcinoma of the head and neck. Histopathology. 2012;61:257–65. doi: 10.1111/j.1365-2559.2012.04242.x. doi. [DOI] [PubMed] [Google Scholar]
- 38.Kang CJ, Chang JTC, Chen TM, Chen IH, Liao CT. Surgical treatment of oral verrucous carcinoma. Chang Gung Med J. 2003;26:807–12. PMID: 14765750. [PubMed] [Google Scholar]
- 39.Alkan A, Bulut E, Gunhan O, Ozden B. Oral verrucous carcinoma: a study of 12 cases. Eur J Dent. 2010;4:202–7. doi: 10.1055/s-0039-1697831. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Zhu LK, Ding YW, Liu W, Zhou YM, Shi LJ, Zhou ZT. A clinicopathological study on verrucous hyperplasia and verrucous carcinoma of the oral mucosa. J Oral Pathol Med. 2012;4:131–5. doi: 10.1111/j.1600-0714.2011.01078.x. doi. [DOI] [PubMed] [Google Scholar]
- 41.Wang YP, Chen HM, Kuo RC, Yu CH, Sun A, Liu BY. Oral verrucous hyperplasia: histologic classification,prognosis, and clinical implications. J Oral Pathol Med. 2009;38:651–6. doi: 10.1111/j.1600-0714.2009.00790.x. et al. doi. [DOI] [PubMed] [Google Scholar]
- 42.Warnakulasuriya S, Kujan O, Aguirre-Urizar JM, Bagan JV, González-Moles MÁ, Kerr AR. Oral potentially malignant disorders: a consensus report from an international seminar on nomenclature and classification, convened by the WHO collaborating centre for oral cancer. Oral Dis. 2021;27:1862–80. doi: 10.1111/odi.13704. et al. doi. [DOI] [PubMed] [Google Scholar]
- 43.Moussa M, Salem H, ElRefai SM. Oral proliferative verrucous leukoplakia: the unsolved paradox. Madridge J Dent Oral Surg. 2017;2:55–8. doi: 10.18689/mjdl-1000114. doi. [DOI] [Google Scholar]
- 44.Cerero-Lapiedra R, Baladé-Martínez D, Moreno-López LA, Esparza-Gómez G, Bagán JV. Proliferative verrucous leukoplakia: a proposal for diagnostic criteria. Med Oral Patol Oral Cir Bucal. 2010;15:839–45. PMID: 20173704. [PubMed] [Google Scholar]
- 45.Carrard VC, Brouns EREA, van der Waal I. Proliferative verrucous leukoplakia: a critical appraisal of the diagnostic criteria. Med Oral Patol Oral Cir Bucal. 2013;18:411–3. doi: 10.4317/medoral.18912. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Palaia G, Bellisario A, Pampena R, Pippi R, Romeo U. Oral proliferative ver-rucous leukoplakia: progression to malignancy and clinical implications. Systematic review and meta-analysis. Cancers. 2021;13:4058. doi: 10.3390/cancers13164085. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Capella DL, Gonçalves JM, Abrantes AAA, Grando LJ, Daniel FI. Proliferative verrucous leukoplakia: diagnosis, management and current advances. Braz J Otorhinolaryngol. 2017;83:585–93. doi: 10.1016/j.bjorl.2016.12.005. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Proaño-Haro A, Bagan L, Bagan JV. Recurrences following treatment of proliferative verrucous leukoplakia: A systematic review and meta-analysis. J Oral Pathol Med. 2021;50:820–8. doi: 10.1111/jop.13178. doi. [DOI] [PubMed] [Google Scholar]
- 49.Alan H, Agacayak S, Kavak G, Ozcan A. Verrucous carcinoma and squamous cell papilloma of the oral cavity: report of two cases and review of literature. Eur J Dent. 2015;9:453–6. doi: 10.4103/1305-7456.163224. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Santosh ABR, Boyd D, Laxminarayana KK. Proposed clinico-pathological classification for oral exophytic lesions. J Clin Diagnostic Res. 2015;9 doi: 10.7860/JCDR/2015/12662.6468. ZE01-8. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Bouckaert Munzhelele TI, Feller L, Lemmer J, Rag K. The clinical characteristics of oral squamous cell carcinoma in patients attending the Medunsa Oral Health Centre, South Africa. Integr Cancer Sci Ther. 2016;3:575–8. doi: 10.15761/ICST.1000207. doi. [DOI] [Google Scholar]
- 52.Wang YH, Tian X, Liu OS, Fang XD, Quan HZ, Xie S. Gene profiling analysis for patients with oral verrucous carcinoma and oral squamous cell carcinoma. Int J Clin Exp Med. 2014;7:1845–52. et al. [PMC free article] [PubMed] [Google Scholar]
- 53.Mohtasham N, Babakoohi S, Shiva A, Shadman A, Kamyab-Hesari K, Shakeri MT. Immunohistochemical study of p53, Ki-67, MMP-2 and MMP-9 expression at invasive front of squamous cell and verrucous carcinoma in oral cavity. Pathol Res Pract. 2013;209:110–4. doi: 10.1016/j.prp.2012.11.002. et al. doi. [DOI] [PubMed] [Google Scholar]
- 54.Vallonthaiel AG, Singh MK, Dinda AK, Kakkar A, Thakar A, Das SN. Expression of cell cycle-associated proteins p53, pRb, p16, p27, and correlation with survival: A comparative study on oral squamous cell carcinoma and verrucous carcinoma. Appl Immunohistochem Mol Morphol AIMM. 2016;24:193–200. doi: 10.1097/PAI.0000000000000179. doi. [DOI] [PubMed] [Google Scholar]
- 55.Zargaran M, Eshghyar N, Baghaei F, Moghimbeigi A. Assessment of cellular proliferation in oral verrucous carcinoma and well-differentiated oral squamous cell carcinoma using Ki67: a non-reliable factor for differential diagnosis? Asian Pac J Cancer Prev. 2012;13:5811–5. doi: 10.7314/apjcp.2012.13.11.5811. doi. [DOI] [PubMed] [Google Scholar]
- 56.de Spíndula-Filho JV, da Cruz AD, Oton-Leite AF, Batista AC, Leles CR, de Cássia Gonçalves Alencar R. Oral squamous cell carcinoma versus oral verrucous carcinoma: an approach to cellular proliferation and negative relation to human papillomavirus (HPV) Tumour Biol. 2011;32:409–16. doi: 10.1007/s13277-010-0135-4. et al. doi. [DOI] [PubMed] [Google Scholar]
- 57.Patil GB, Hallikeri KS, Balappanavar AY, Hongal SG, Sanjaya PR, Sagari SG. Cyclin B1 overexpression in conventional oral squamous cell carcinoma and verrucous carcinoma - a correlation with clinicopathological features. Med Oral Patol Oral Cir Bucal. 2013;18:e585–90. doi: 10.4317/medoral.18220. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Menaka TR, Ravikumar SS, Dhivya K, Thilagavathi N, Dinakaran J, Kalaichelvan V. Immunohistochemical expression and evaluation of cyclin D1 and minichromosome maintenance 2 in oral squamous cell carcinoma and verrucous carcinoma. J Oral Maxillofac Pathol. 2022;26:44–51. doi: 10.4103/jomfp.jomfp_446_21. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Lin HP, Wang YP, Chiang CP. Expression of p53, MDM2, p21, heat shock protein 70, and HPV 16/18 E6 proteins in oral verrucous carcinoma and oral verrucous hyperplasia. Head Neck. 2011;33:334–40. doi: 10.1002/hed.21452. doi. [DOI] [PubMed] [Google Scholar]
- 60.Adegboyega PA, Boromound N, Freeman DH. Diagnostic utility of cell cycle and apoptosis regulatory proteins in verrucous squamous carcinoma. Appl Immunohistochem Mol Morphol AIMM. 2005;13:171–7. doi: 10.1097/01.pai.0000132190.39351.9b. doi. [DOI] [PubMed] [Google Scholar]
- 61.Arduino PG, Carrozzo M, Pagano M, Broccoletti R, Scully C, Gandolfo S. Immunohistochemical expression of basement membrane proteins of verrucous carcinoma of the oral mucosa. Clin Oral Investig. 2010;14:297–302. doi: 10.1007/s00784-009-0296-y. doi. [DOI] [PubMed] [Google Scholar]
- 62.Angadi VC, Angadi P V. GLUT-1 immunoexpression in oral epithelial dysplasia, oral squamous cell carcinoma, and verrucous carcinoma. J Oral Sci. 2015;57:115–22. doi: 10.2334/josnusd.57.115. doi. [DOI] [PubMed] [Google Scholar]
- 63.El-Rouby DH.. Association of macrophages with angiogenesis in oral verrucous and squamous cell carcinomas. J Oral Pathol Med. 2010;39:559–64. doi: 10.1111/j.1600-0714.2010.00879.x. doi. [DOI] [PubMed] [Google Scholar]
- 64.Gao HW, Ho JY, Lee HS, Yu CP. The presence of Merkel cells and CD10- and CD34-positive stromal cells compared in benign and malignant oral tumors. Oral Dis. 2009;15:259–64. doi: 10.1111/j.1601-0825.2009.01518.x. doi. [DOI] [PubMed] [Google Scholar]
- 65.Paral KM, Taxy JB, Lingen MW. CD34 and α smooth muscle actin distinguish verrucous hyperplasia from verrucous carcinoma. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014;117:477–82. doi: 10.1016/j.oooo.2013.12.401. doi. [DOI] [PubMed] [Google Scholar]
- 66.Odar K, Zidar N, Bonin S, Gale N, Cardesa A, Stanta G. Desmosomes in verrucous carcinoma of the head and neck. Histol Histopathol. 2012;27:467–74. doi: 10.14670/HH-27.467. doi. [DOI] [PubMed] [Google Scholar]
- 67.Huang TT, Hsu LP, Hsu YH, Chen PR. Surgical outcome in patients with oral verrucous carcinoma: long-term follow-up in an endemic betel quid chewing area. ORL. 2009;71:323–8. doi: 10.1159/000267306. doi. [DOI] [PubMed] [Google Scholar]
- 68.Candau-Alvarez A, Dean-Ferrer A, Alamillos-Granados FJ, Heredero Jung S, García-García B, Ruiz-Masera JJ. Verrucous carcinoma of the oral mucosa: an epidemiological and follow-up study of patients treated with surgery in 5 last years. Med Oral Patol Oral Cir Bucal. 2014;19:506–11. doi: 10.4317/medoral.19683. et al. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Verma DK, Bansal S, Gupta D, Bansal A. Neck dissection in verrucous carcinoma: a surgical dilemma. IJSS Case Reports Rev. 2015;1:42–5. doi: 10.17354/cr/2015/28. doi. [DOI] [Google Scholar]
- 70.Rath S, Gandhi AK, Rastogi M, Agarwal A, Singhal A, Sharma V. Treatment pattern and outcomes in verrucous carcinoma of oral cavity: a single institutional retrospective analysis from a tertiary cancer center and review of literature. Indian J Otolaryngol Head Neck Surg. 2022;74(Suppl 2):1790–6. doi: 10.1007/s12070-020-01798-w. et al. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Sadasivan A, Thankappan K, Rajapurkar M, Shetty S, Sreehari S, Iyer S. Verrucous lesions of the oral cavity treated with surgery: analysis of clinicopathologic features and outcome. Contemp Clin Dent. 2012;3:60–3. doi: 10.4103/0976-237X.94548. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Lundgren JA, van Nostrand AW, Harwood AR, Cullen RJ, Bryce DP. Verrucous carcinoma (Ackerman’s tumor) of the larynx: diagnostic and therapeutic considerations. Head Neck Surg. 1986;9:19–26. doi: 10.1002/hed.2890090105. doi. [DOI] [PubMed] [Google Scholar]
- 73.Ferlito A, Rinaldo A, Mannarà GM. Is primary radiotherapy an appropriate option for the treatment of verrucous carcinoma of the head and neck? J Laryngol Otol. 1998;112:132–9. doi: 10.1017/s0022215100140137. doi. [DOI] [PubMed] [Google Scholar]
- 74.Kraus FT, Perezmesa C. Verrucous carcinoma: clinical and pathologic study of 105 cases involving oral cavity, larynx and genitalia. Cancer. 1966;19:26–38. doi: 10.1002/1097-0142(196601)19:1<26::aid-cncr2820190103>3.0.co;2-l. doi. [DOI] [PubMed] [Google Scholar]
- 75.Memula N, Ridenhour GDL. Radiotherapeutic management of oral verrucous carcinoma. Oncol Biol Phys. 1980;6:1404. [Google Scholar]
- 76.Nair MK, Sankaranarayanan R, Padmanabhan TK, Madhu CS. Oral verrucous carcinoma. Treatment with radiotherapy. Cancer. 1988;61:458–61. doi: 10.1002/1097-0142(19880201)61:3<458::aid-cncr2820610309>3.0.co;2-t. doi. [DOI] [PubMed] [Google Scholar]
- 77.Chang BA, Katz S, Kompelli AR, Nathan CAO. Is primary radiotherapy an acceptable treatment modality for verrucous carcinoma of the larynx? Laryngoscope. 2019;129:1964–5. doi: 10.1002/lary.27985. doi. [DOI] [PubMed] [Google Scholar]
- 78.Huang SH, Lockwood G, Irish J, Ringash J, Cummings B, Waldron J. Truths and myths about radiotherapy for verrucous carcinoma of larynx. Int J Radiat Oncol Biol Phys. 2009;73:1110–5. doi: 10.1016/j.ijrobp.2008.05.021. et al. doi. [DOI] [PubMed] [Google Scholar]
- 79.Tharp ME, Shidnia H. Radiotherapy in the treatment of verrucous carcinoma of the head and neck. Laryngoscope. 1995;105:391–6. doi: 10.1288/00005537-199504000-00011. doi. [DOI] [PubMed] [Google Scholar]
- 80.Demian SD, Bushkin FL, Echevarria RA. Perineural invasion and anaplastic transformation of verrucous carcinoma. Cancer. 1973;32:395–401. doi: 10.1002/1097-0142(197308)32. doi. 2<395::aid-cncr2820320217>3.0.co;2-e. [DOI] [PubMed] [Google Scholar]
- 81.Schwade JG, Wara WM, Dedo HH, Phillips TL. Radiotherapy for verrucous carcinoma. Radiology. 1976;120:677–9. doi: 10.1148/120.3.677. doi. [DOI] [PubMed] [Google Scholar]
- 82.Naik AN, Silverman DA, Rygalski CJ, Zhao S, Brock G, Lin C. Postoperative radiation therapy in oral cavity verrucous carcinoma. Laryngoscope. 2022;132:1953–61. doi: 10.1002/lary.30009. et al. doi. [DOI] [PubMed] [Google Scholar]
- 83.Wu CF, Chen CM, Shen YS, Huang IY, Chen CH, Chen CY. Effective eradication of oral verrucous carcinoma with continuous intraarterial infusion chemotherapy. Head Neck. 2008;30:611–7. doi: 10.1002/hed.20751. et al. doi. [DOI] [PubMed] [Google Scholar]
- 84.Strojan P, Ferlito A, Wu CF, Rinaldo A. Intraarterial chemotherapy: a valid option in the treatment of verrucous carcinoma? Eur Arch Oto-Rhino-Laryngology. 2010;267:835–7. doi: 10.1007/s00405-009-1178-2. doi. [DOI] [PubMed] [Google Scholar]
- 85.Strojan P, Šoba E, Budihna M, Auersperg M. Radiochemotherapy with vinblastine, methotrexate, and bleomycin in the treatment of verrucous carcinoma of the head and neck. J Surg Oncol. 2005;92:278–83. doi: 10.1002/jso.20422. doi. [DOI] [PubMed] [Google Scholar]
- 86.De Keukeleire S, De Meulenaere A, Deron P, Huvenne W, Fréderic D, Bouckenooghe O. Verrucous hyperplasia and verrucous carcinoma in head and neck: use and benefit of methotrexate. Acta Clin Belg. 2021;76:487–91. doi: 10.1080/17843286.2020.1752455. et al. doi. [DOI] [PubMed] [Google Scholar]
- 87.Karagozoglu KH, Buter J, Leemans CR, Rietveld DHF, Van Den Vijfeijken S, Van Der Waal I. Subset of patients with verrucous carcinoma of the oral cavity who benefit from treatment with methotrexate. Br J Oral Maxillofac Surg. 2012;50:513–8. doi: 10.1016/j.bjoms.2011.09.011. doi. [DOI] [PubMed] [Google Scholar]
- 88.Salesiotis A, Soong R, Diasio RB, Frost A, Cullen KJ. Capecitabine induces rapid, sustained response in two patients with extensive oral verrucous carcinoma. Clin Cancer Res. 2003;9:580–5. [PubMed] [Google Scholar]
- 89.Yoshimura Y, Mishima K, Obara S, Nariai Y, Yoshimura H, Mikami T. Treatment modalities for oral verrucous carcinomas and their outcomes: contribution of radiotherapy and chemotherapy. Int J Clin Oncol. 2001;6:192–200. doi: 10.1007/PL00012104. doi. [DOI] [PubMed] [Google Scholar]
- 90.Yu CH, Lin HP, Cheng SJ, Sun A, Chen HM. Cryotherapy for oral precancers and cancers. J Formos Med Assoc. 2014;113:272–7. doi: 10.1016/j.jfma.2014.01.014. doi. [DOI] [PubMed] [Google Scholar]
- 91.Yeh CJ. Treatment of verrucous hyperplasia and verrucous carcinoma by shave excision and simple cryosurgery. Int J Oral Maxillofac Surg. 2003;32:280–3. doi: 10.1054/ijom.2002.0331. doi. [DOI] [PubMed] [Google Scholar]
- 92.Chen HM, Yu CH, Lin HP, Cheng SJ, Chiang CP. 5-Aminolevulinic acid-mediated photodynamic therapy for oral cancers and precancers. J Dent Sci. 2012;7:307–5. doi: 10.1016/j.jds.2012.03.023. doi. [DOI] [Google Scholar]
- 93.Chen HM, Chen CT, Yang H, Lee MI, Kuo MYP, Kuo YS. Successful treatment of an extensive verrucous carcinoma with topical 5-aminolevulinic acid-mediated photodynamic therapy. J Oral Pathol Med. 2005;34:253–6. doi: 10.1111/j.1600-0714.2004.00267.x. et al. doi. [DOI] [PubMed] [Google Scholar]
- 94.Hsu CK, Lee JYY, Yu CH, Hsu MML, Wong TW. Lip verrucous carcinoma in a pregnant woman successfully treated with carbon dioxide laser surgery. Vol. 157, The British journal of dermatology. Br J Dermatol. 2007;157:813–5. doi: 10.1111/j.1365-2133.2007.08078.x. doi. [DOI] [PubMed] [Google Scholar]
- 95.Azevedo LH, Galletta VC, de Paula Eduardo C, de Sousa SOM, Migliari DA. Treatment of oral verrucous carcinoma with carbon dioxide laser. J Oral Maxillofac Surg. 2007;65:2361–6. doi: 10.1016/j.joms.2006.10.024. doi. [DOI] [PubMed] [Google Scholar]
- 96.Lee CN, Huang CC, Lin IC, Lee JYY, Ou CY, Wong TW. Recalcitrant lip verrucous carcinoma successfully treated with acitretin after carbon dioxide laser ablation. JAAD case reports. 2018;4:576–8. doi: 10.1016/j.jdcr.2018.02.002. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]