

Abstract
Introduction and importance
Bucket-handle mesenteric tear (BHMT) is a type of intestinal mesenteric injury where the intestine separates from its mesentery resulting in ischemia and perforation. Traumatic abdominal wall hernia (TAWH) is a disruption of the abdominal wall muscles and fascia in the presence of intact skin. BHMT and TAWH following bicycle handlebar injury in adults are rare. TAWH and generalized abdominal tenderness led to emergent surgical treatment in our patient. I aim to report these rare clinical entities in an adult patient with the management. This case report can create awareness among primary care physicians to decide on early referral and surgeons on early treatment.
Case presentation
A 55y man presented 4 h after a bicycle handlebar injury to the abdomen. He had generalized abdominal pain but no history of vomiting, smoking, diabetes, or hypertension. Lab results were insignificant. TAWH and generalized tenderness led to the additional diagnosis of hollow-viscus perforation, but laparotomy revealed BHMT of the ileum and transverse colon. We did TAWH repair, bowel resection, and end-to-end anastomosis with excellent results.
Clinical discussion
BHMT following bicycle handlebar injury is rare in adults, with few case reports. Imaging is less sensitive, and surgery is the definitive diagnosis of BHMT.TAWH in adults after bicycle handlebar injury is rare and can be a sign of serious-intraabdominal injuries, and surgical repair is the treatment.
Conclusion
BHMT and TAWH following bicycle handlebar injury are rare in adults. BHMT can be life-threatening if not detected and treated early.
Keywords: Adult, Handlebar hernia, Bucket-handle, Mesenteric injury, Bicycle, ‘Case report’
Highlights
-
•
Bicycle handlebar blunt abdominal trauma is rare in adults.
-
•
Combined BHMT and TAWH in adults are rare bicycle handlebar injuries.
-
•
TAWH in adults indicates more serious intra-abdominal organ injuries.
-
•
Multiple site bucket handles mesenteric tears involving the ileum and transverse colon are rare clinical occurrences.
1. Introduction
In general, bicycle handlebar blunt abdominal trauma is rare in the adult population compared to the pediatric age group. It is attributable to the infrequent and more careful use of a bicycle, and a strong-abdominal wall can prevent significant injury in adults compared to children. Though rare, bicycle handlebar blunt abdominal injuries can result in TAWH, BHMT, intestinal perforations, and pancreatic lacerations in adults [1], [2], [3], [4], [5].
TAWH secondary to bicycle handlebar injury is rare in adults [5]. A bicycle handlebar hernia occurs due to focused force from a narrow caliber bicycle handlebar and increased intra-abdominal pressure that can disrupt the fascia and abdominal wall muscles while the skin elasticity prevents its penetration. The other causes of handlebar hernias include impact against handlebar-like objects (wheelbarrow, plow handles, motorcycle handlebars, axe handles, goring, and a bed post) [6].
A BHMT is a linear mesenteric laceration paralleling the bowel segment with the avulsion of the terminal vascular supply leading to ischemia and perforation if not intervened [7], [8]. It is also called ischemic mesenteric injury. It follows blunt abdominal trauma caused by MVA, fall from a height, handlebar injuries, or physical violence. The underlying mechanism of mesenteric injury is due to rapid deceleration, compression or crush injuries [9]. Bowel perforations can occur from direct trauma or delayed perforation of the devascularized segment due to necrosis within 48 to 72 h [10]. This is associated with significant morbidity and mortality.
Clinical diagnosis of the mesenteric injury is challenging so is the imaging diagnosis [11], [12]. One of the most commonly missed injuries on CT scan by experienced radiologists in trauma setting were bowel and mesenteric injuries [13].
Here is a rare case of 55y old male patient who presented 4 h after blunt abdominal trauma caused by a bicycle handlebar. TAWH and BHMT of distal ileum and transverse colon were the clinical and intraoperative diagnoses, respectively. We managed him with exploratory laparotomy, repair of the hernia, and resection and end-to-end anastomosis with an excellent outcome. This case is presented in line with the SCARE 2020 criteria [14].
2. Presentation of the case
A 55y old man was brought to our hospital after 4 h of sustaining bicycle accident. He reported that he fell down while riding a bicycle on his way home and the handle bar stuck his abdomen. Since then he had severe abdominal pain which was initially at the site of injury and later became generalized. He had no history of vomiting, bleeding, smoking, alcohol ingestion, diabetes, or hypertension. At presentation his vital signs were BP = 110/70 mmHg, PR = 86 beats/min, RR = 20 breaths/min, T = 36.7 °C. Abdominal examination revealed 2x3cm reducible swelling in the right lower quadrant at the site of trauma with the handlebar mark and surrounding ecchymosed skin (Fig. 1). There was generalized tenderness over the abdomen with guarding. There was no blood on the digital rectal examination.
Fig. 1.
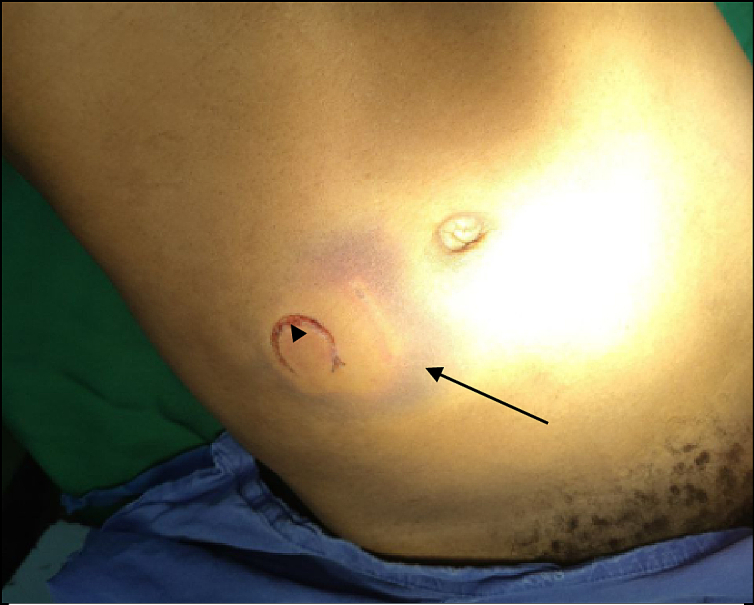
Handlebar mark (arrow head) and surrounding ecchymosed skin in the right lower quadrant (arrow).
Laboratory tests like CBC showed mild anemia (Hgb = 11.9 g/dl) and a leukocyte count of 10,000/microL with 85.9 % neutrophil, normal serum electrolytes, and renal function tests. Imagings were not done as the patient had clear signs of peritonitis.
Exploratory laparotomy was decided for the clinical diagnosis of generalized peritonitis secondary to perforated viscus. An intravenous line secured, normal saline infusion started, ceftriaxone 1 g, and metronidazole 500 mg IV given. After signed consent, under general anesthesia and a supine position, the abdomen was prepped with alcohol and povidone‑iodine and draped. Then the peritoneum entered through a midline incision. The intraoperative findings were 300 ml blood in the general peritoneum, 3 cm traumatic right lower quadrant fascial defect, BHMT of the distal ileum 15 cm from the ileocecal valve with active bleeding (Fig. 2), and BHMT of the mid-transverse colon with active bleeding from right branches of middle colic artery (Fig. 3). We aspirated the blood, did resection and double layer end-to-end anastomosis of both the ileum and transverse colon with the mesenteric injuries using 2-0 vicryl in two layers, and repaired the traumatic fascial defect without mesh as there was no significant tissue loss, from inside using size 1-vicryl. Finally, we did peritoneal irrigation with warm saline, and closed the abdomen in layers (fascia with size 1-vicryl and skin with 2-0 silk). Postoperative recovery was uneventful. The patient was discharged on the sixth postoperative day, advised to avoid heavy lifting, and followed at the SRC at two weeks, one month, and four months postoperatively with no new complaint (Fig. 4). The patient is happy with the treatment result.
Fig. 2.
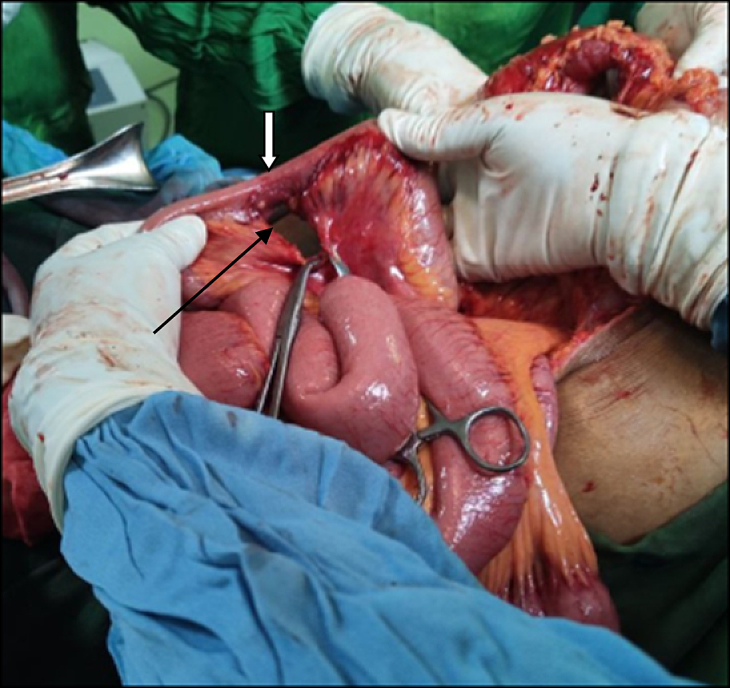
Bucket handle mesenteric injury of distal ileum (black arrow) with the handle of the bucket showed (white arrow).
Fig. 3.

Bucket-handle mesenteric injury of transverse colon (arrow).
Fig. 4.

Post-operative photo at 4 month, showing midline scar (star) and depression over the repaired TAWH under the circular scar (handlebar injury site) (arrowhead).
3. Discussion
Literature is scarce on bicycle handlebar abdominal injuries in adults [1]. This is because adults are less likely to use bicycles, use bicycles with care, and have well-developed abdominal walls compared to children. Although rare, bicycle handlebar blunt abdominal injuries can cause TAWH and catastrophic intra-abdominal organ injuries in adults.
TAWH is a condition in which intra-abdominal contents come through fascial defect following blunt abdominal trauma secondary to motor vehicle accidents, fall from a height, and bicycle handlebars. A literature review done in 2013 found 248 cases of TAWH, of which bicycle handlebar injury was the second most common cause in 25 %, the leading cause being car accidents in 49 % of the cases [15]. The most common site of occurrence of TAWH is in the lower abdomen. In a case report and literature review done in 2018, there were 80 cases of handlebar hernias, of which only 10 were adults with motorbike injury in 3, gear-poke car in 1, and bicycle injury in 6 patients [16]. In a case report and review of works of literature from Turkey done on adult bicycle handlebar hernia, they reported 10 cases of handlebar hernia, including their own [17].
TAWH is often associated with concomitant intraabdominal injuries. In a review of 248 patients, 43 % had minimal injuries, while 53 % had significant intraabdominal injuries like liver laceration, spleen rapture, pancreatic injuries, and bowel injuries requiring surgical intervention [15]. In adults, there are case reports of bicycle handlebar hernias with concomitant small bowel mesenteric injuries and small bowel perforations, stomach perforation, and liver laceration [5], [17].
Diagnosis of TAWH can be by a physical examination which is also true in the case presented here, or with the aid of imaging like a CT scan or Ultrasound. TAWH can be confused for abdominal wall hematoma on physical examination or missed on imaging [6]. With the high suspicion of intraabdominal injuries, a CT scan is the diagnostic imaging of choice. The treatment of TAWH is surgery, but few case reports in pediatric patients show spontaneous resolution [6]. The surgical repair can be by a direct incision over the swelling or internally without a separate incision if a concomitant injury that needs laparotomy or laparoscopic intervention is present. TAWH was repaired internally in the case presented here.
Blunt abdominal trauma is associated with bowel or mesenteric injuries in 1–6 % of the cases [7]. The mesenteric injury can be non-ischemic like mesenteric hematoma or ischemic which denotes avulsion of the mesentery from the segment of the bowel resulting in necrosis of the affected segment. A BHMT is the term used for the ischemic bowel injury with the devascularized bowel segment [8]. The bucket handle is the segment of the bowel detached from its mesentery. The common site of occurrence of BHMT in blunt abdominal trauma is near the junctions of fixed and mobile bowel segments like proximal jejunum and distal ileum [7]. BHMT occurred in both ileum and transverse colon in the case presented above.
BHMT commonly follows seat belt injury in MVA, falls from a height, handlebar injuries, and physical violence [18]. The mechanisms of BHMT include deceleration in MVA if seatbelts are used, compression forces in the case of handlebar injuries, and direct abdominal trauma. Preoperative diagnosis of BHMT is challenging clinically and radiologically [19]. This is because clinical presentations and imaging findings are often nonspecific and subtle, with a delayed manifestation of peritonitis. Although CT scan is the investigation of choice, a definitive diagnosis is surgery. Surgery is indicated immediately in patients with peritonitis, hemodynamically unstable patients, or those with significant bleeding, with or without investigations. Immediate laparotomy was decided in the case presented here for the signs of peritonitis.
Like TAWH, BHMT secondary to bicycle handlebar injuries are rare. In 2022 works of literature review of 22 patients and a case series of 4 patients, only 2 cases of BHMT secondary to bicycle handlebar were reported [20].
The strength of this study is that it discussed the unusual occurrence of concomitant TAWH, and BHMT of the ileum and transverse colon secondary to bicycle handlebar injury in an adult patient. All the limitations of the case reports are applicable.
4. Conclusion
Based on available evidences, TAWH and BHMT secondary to bicycle handlebar blunt abdominal trauma are rare. TAWH following bicycle handlebar injury can be a clue for severe intraabdominal injuries like BHMT in adults, and presence of peritonitis needs immediate laparotomy. To my knowledge, TAWH and BHMT in the distal ileum and mid-transverse colon secondary to bicycle handlebar injury in an adult patient is not reported before.
Provenance and peer review
Not commissioned, externally peer reviewed.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor–in-Chief of this journal on request.
Ethical approval
The study is exempt from ethical approval in our institution.
Sources of funding
This case report did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contribution
All the work is done by one author.
Guarantor
Gosa Hundie Bejiga.
Research registration
Not applicable.
Declaration of competing interest
The authors declare that there is no conflict of interest.
References
- 1.Bohmer J.H., Proust A.F. Adult bicycle handlebar injury. Am. J. Emerg. Med. Sep. 2006;24(5):624–625. doi: 10.1016/j.ajem.2005.12.022. [DOI] [PubMed] [Google Scholar]
- 2.Neofytou K., Michailidou M., Petrou A., Loizou S., Andreou C., Pedonomou M. Isolated jejunal perforation following bicycle handlebar injury in adults: a case report. Case Rep. Emerg. Med. 2013;2013:1–4. doi: 10.1155/2013/678678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wang A., Lin T., Chen S. Isolated traumatic duodenal rupture due to bicycle handlebar injury in an adult patient. Hong Kong J. Emerg. Med. Mar. 2015;22(2):113–117. doi: 10.1177/102490791502200206. [DOI] [Google Scholar]
- 4.Luu A.M., Meurer K., Herzog T., Uhl W., Braumann C. Diagnostic double strike in the emergency room - two cases of complete pancreatic ruptures due to bicycle handlebar injuries on two consecutive days. J. Med. Case Rep. Dec. 2018;12(1):85. doi: 10.1186/s13256-018-1594-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ghosh S., Nolan G., Simpson R. A concealed small bowel perforation in an adult secondary to bicycle handlebar trauma. Annals. 2013;95(4):e4–e5. doi: 10.1308/003588413X13511609957894. May. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Litton K., Izzidien A.Y., Hussien O., Vali A. Conservative management of a traumatic abdominal wall hernia after a bicycle handlebar injury (case report and literature review) J. Pediatr. Surg. Apr. 2008;43(4):e31–e32. doi: 10.1016/j.jpedsurg.2007.12.059. [DOI] [PubMed] [Google Scholar]
- 7.Extein J.E., Allen B.C., Shapiro M.L., Jaffe T.A. CT findings of traumatic bucket-handle mesenteric injuries. Am. J. Roentgenol. Dec. 2017;209(6):W360–W364. doi: 10.2214/AJR.17.17927. [DOI] [PubMed] [Google Scholar]
- 8.Boscak A.R., Bodanapally U.K., Elshourbagy T., Shanmuganathan K. Segmental bowel hypoenhancement on CT predicts ischemic mesenteric laceration after blunt trauma. Am. J. Roentgenol. Jul. 2021;217(1):93–99. doi: 10.2214/AJR.20.23108. [DOI] [PubMed] [Google Scholar]
- 9.Hughes T.M.D., Elton C. The pathophysiology and management of bowel and mesenteric injuries due to blunt trauma. Injury. May 2002;33(4):295–302. doi: 10.1016/S0020-1383(02)00067-0. [DOI] [PubMed] [Google Scholar]
- 10.Tilden W., Griffiths M., Cross S. Vascular bowel and mesenteric injury in blunt abdominal trauma: a single centre experience. Clin. Radiol. Mar. 2021;76(3):213–223. doi: 10.1016/j.crad.2020.09.022. [DOI] [PubMed] [Google Scholar]
- 11.LeBedis C.A., et al. CT imaging signs of surgically proven bowel trauma. Emerg. Radiol. Jun. 2016;23(3):213–219. doi: 10.1007/s10140-016-1380-7. [DOI] [PubMed] [Google Scholar]
- 12.Malhotra A.K., Fabian T.C., Katsis S.B., Gavant M.L., Croce M.A. Blunt bowel and mesenteric injuries: the role of screening computed tomography. J. Trauma. Jun. 2000;48(6):991–1000. doi: 10.1097/00005373-200006000-00001. [DOI] [PubMed] [Google Scholar]
- 13.Lawson C.M., Daley B.J., Ormsby C.B., Enderson B. Missed injuries in the era of the trauma scan. J. Trauma. Feb. 2011;70(2):452–458. doi: 10.1097/TA.0b013e3182028d71. [DOI] [PubMed] [Google Scholar]
- 14.Agha R.A., et al. The SCARE 2020 guideline: updating consensus surgical CAse REport (SCARE) guidelines. Int. J. Surg. Dec. 2020;84:226–230. doi: 10.1016/j.ijsu.2020.10.034. [DOI] [PubMed] [Google Scholar]
- 15.Liasis L., Tierris I., Lazarioti F., Clark C.C., Papaconstantinou H.T. Traumatic abdominal wall hernia: is the treatment strategy a real problem? J. Trauma Acute Care Surg. Apr. 2013;74(4):1156–1162. doi: 10.1097/TA.0b013e318283d88d. [DOI] [PubMed] [Google Scholar]
- 16.Shukla A., Verma V., Lal Kapoor K., Gupta B., Chaudhary R. Handlebar hernia with triple herniation and perforation: a case report and literature review. BEAT. Jun. 2018;6(3):257–261. doi: 10.29252/beat-060313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hefny A.F., Jagdish J., Salim E.N.A. A rare case of an adult traumatic bicycle handlebar hernia: a case report and review of the literature. Turk. J. Emerg. Med. Dec. 2018;18(4):179–181. doi: 10.1016/j.tjem.2018.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Altadill A., Deng F. Radiopaedia.org. Radiopaedia.org; 2021. Bucket handle mesenteric injury. [DOI] [Google Scholar]
- 19.Densley A., Wali A., Mathew S., Cox C.W. Early imaging identification of traumatic mesenteric and bowel injury: an illustrative case of bucket-handle mesenteric avulsion injury with delayed presentation as small bowel obstruction. 2022;2(4):4. [Google Scholar]
- 20.Chowdhury A., Burford C., Pangeni A., Shrestha A. Bucket-handle mesenteric tears: a comprehensive review of their presentation and management. Cureus. Sep. 2022 doi: 10.7759/cureus.28692. [DOI] [PMC free article] [PubMed] [Google Scholar]