

ABSTRACT
Background:
Health care systems worldwide have rapidly responded to manage the COVID-19 pandemic by providing screening tests, contact tracing, treatment, and vaccination. However, the long duration of the pandemic has had an enormous load on the health care systems, which disrupted continuity of the essential non-covid services, long waiting time for appointments, and increase in the utilization of telemedicine services. Primary health care was established as an essential foundation for the global response to the COVID-19. In Qatar, Primary Heath Care Corporation (PHCC), the main primary care services provided played a major role in the response to the pandemic. However, its services were affected and disrupted, and new services were added. Hence, the aim of this analysis is to understand the long-term impact of the COVID-19 on the services provided by PHCC in Qatar in terms of PHCC pandemic response, change in utilization of the core, and preventative services, and the introduction of new alternative services.
Methods:
A retrospective data analysis was conducted for all the appointments and visits for all the PHCC health centers in the years of 2020 and 2021. The study conducted a comparison of the services utilizations using the utilization figures of PHCC services between 1st of January and 31st of December 2019 as a reference year. The differences in the utilization per service were presented in frequencies and percentages.
Results:
The in-person services dropped drastically in 2020 at 36% reduction in compassion to 2019. However, the newly introduced virtual consultation services in 2020 reached their highest utilization figures in 2021 at 908,965 virtual visits. The COVID-19 specific related services ranging from the COVID-19 drive-through testing to vaccine administration constituted a total number of 2,836,127 visits corresponding to 44% of the total PHCC services utilization visits in 2021. In 2021, PHCC dental services dropped by 25.2%. The most noticeable utilization drops in 2021 were among the preventative services with 53.2% and 78.9% in colorectal screening and non-communicable diseases (NCDs) risk factors annual screening services, respectively. However, mental health services have witnessed a surge in utilization at 134.1% increase in 2021 in comparison to 2019.
Conclusion:
The COVID-19 pandemic caused a disruption in the PHCC utilization of core services, namely dental services. Additionally, PHCC preventive services utilizations were affected drastically including cancer and NCDs risk factors annual screening. Nevertheless, PHCC managed to provide alternative virtual services and played a vital role in responding to the pandemic by leading the COVID-19 vaccination campaign in Qatar. However, future research is needed to establish which vulnerable patient groups were most affected by the pandemic, to continue to inform strategies and policies directed at mitigating the impact of future potential pandemics.
Keywords: COVID-19, primary health care, preventative services, Qatar
Introduction
Health care systems worldwide have rapidly responded to manage the COVID-19 pandemic through providing screening tests, contact tracing, treatment, and vaccination.[1] The long duration of the pandemic and growing number of the COVID-19 cases has had a dramatic load on the health care systems, which caused disruption in continuity of the essential non-covid services, long waiting time for appointments, and increase in the utilization of telemedicine services.[2,3]
A strong primary health care system is the foundation of an efficient and effective national health service. The World Health Organization (WHO) highlighted the importance of the primary health care as an essential foundation for the global response to the COVID-19. The main functions of primary care in the COVID-19 response include vaccination, diagnose and manage potential cases, reduce the risk of transmission of infection to contacts and health care workers, maintain delivery of essential health services, and strengthen risk communication.[4]
Primary Health Care Corporation (PHCC), the main primary care provider in Qatar is serving 1.6 million individuals throughout a network of 28 primary health care centers covering the country. The services range from preventive services such as disease screening, immunization, and lifestyle counseling to therapeutic services for long-term conditions, antenatal, and urgent care for all age groups. In addition to that, PHCC provides general dental services, pharmacy, and laboratory services.[5]
As of June 9, 2022, more than 370, 000 cases and 677 deaths have been reported in Qatar due to four COVID-19 pandemic waves.[6] The first wave started with the introduction of the virus in February 2020 and peaked in late May 2020.[7] The second wave started in January 2021 and peaked in the first week of March due to the introduction of the Alpha (B.1.1.7) variant. However, the third wave that was triggered by the introduction of the Beta (B.1.351) variant, started in mid-March and peaked in mid-April 2021.[7] The fourth wave was triggered by the introduction of the Omicron (B.1.1.529) variant, which started in December 2021 and peaked in mid of Jan 2022.[8]
PHCC responded rapidly to the pandemic by providing the COVID-19 testing in all primary health centers. In addition to that PHCC opened four COVID-19 centers for testing and holding in the first three waves. As the epidemic continued, PHCC started to open a drive-through for testing in twelve health centers. PHCC maintained only urgent services and walk-in clinics during the peaks and initiated new alternative services such as virtual/telephone consultation and home medication delivery to respond to maintain the continuity of the care.[9,10] At the same time some of the primary care services were suspended, for example, cancer screening and lifestyle medicine clinics.[11] The PHCC response to the COVID-19 pandemic and then later the coping with the pandemic across all the services provided by PHCC over 2 years of the pandemic was not conducted previously; hence, this analysis is novel in this context.
The aim of this analysis is to understand the long-term impact of the COVID-19 on the services provided by PHCC in Qatar in terms of PHCC pandemic response, change in utilization of the core and preventative services, and the introduction of new alternative services.
Material and Methods
Study setting
All the 28 health centers affiliated with the PHCC in Qatar.
Study duration
The study assessed all the PHCC services between January 1, 2019 and December 31, 2021.
Study design
A retrospective data analysis was conducted for the primary care services between 2019 and 2021 in all the PHCC 28 health centers, in addition to the COVID-19 related services between 2020 and 2021.
Sample size and sampling
All the visits in the aforementioned period of time for all the PHCC services were included in the data extraction.
Data collection
The data was extracted annually from the business health intelligence department at the PHCC and included all the appointments and walking visits for all the health centers during the aforementioned period. The business health intelligence department at the PHCC is responsible for collating and reporting on the services utilization across all the PHCC health centers from the health information system.
Data analysis
The yearly all-cause of health center visits in-person and virtual visits prior and post the COVID-19 pandemic between January 1, 2019 and December 31, 2021 have been analyzed. The services utilizations were categorized into three main groups PHCC business as usual services, COVID-19 related services, and the virtual/telemedicine services that were introduced due to the COVID-19. The COVID-19 services at the PHCC were focused on the COVID-19 testing and vaccination services. The PHCC business as usual services were categorized into primary care core services (family medicine, dental services, maternal services); preventative services (well-baby/immunization services, wellness services, smoking cessation, NCD annual health check called SMART check, colorectal cancer screening, and breast cancer screening); additional services (home care, ophthalmology, ENT, dermatology, pharmacy, and laboratory services). In the analysis, we presented the volume of virtual and in-person visits.
The volume of the COVID-19 related services was calculated yearly in the addition to the newly virtual services that were introduced as a part of the PHCC services modifications due to the COVID-19 pandemic. The utilization trends were established to track the differences between the first year and the second year of PHCC the COVID-19 related response.
We conducted a comparison of the services utilization using the utilization figures of the PHCC business as usual services between 1st of January and 31st of December 2019 as a reference year and then calculated the absolute difference in the utilization figures per service between 1st of January and 31st of December for 2020 and 2021, respectively. The percentages of services utilization change were calculated using the 2019 utilization figures as a reference year per service for all the services in 2020 and 2021. Descriptive statistical analysis using STATA 14 was conducted. The service’s types were presented as categorical variables and were reported as frequencies and percentages and compared using the Chi-squared test. P value <0.05 was considered statistically significant.
Ethical considerations
The utilization visits data was extracted anonymously and all the required approval to conduct the study was secured by the PHCC IRB with reference number PHCC/DCR/2020/07/077.
Results
Overall services utilization
The in-person services dropped drastically since the start of the COVID-19 pandemic in March 2020 at the PHCC health centers in comparison to number of in-person visits in 2019 with the lowest number of visits captured in 2020 at 2,228,910 as illustrated in Figure 1. The reduction in person visits was 36% when compared to the visits in 2019. However, there was a steady increase in the virtual consultation services since their inception in March 2020 due to the needs that emerged after the pandemic. The number of PHCC virtual consultations was the highest in 2021 at 908,965 virtual visits as shown in Figure 1.
Figure 1.
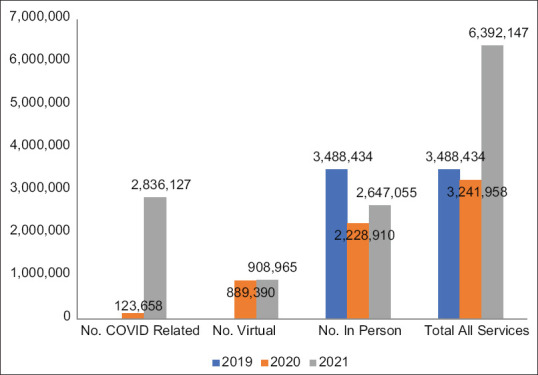
PHCC services utilization by service type grouped into in-person, virtual, and COVID-19 specific services 2019–2021
COVID-19 related services
The COVID-19 related services provided by PHCC health centers from mid-March 2020 and onwards were demonstrated in Table 1. The PHCC started providing the COVID-19 specific services ranging from the COVID-19 drive-through testing at 18 health centers to the COVID-19 vaccine administration services at PHCC 28 affiliated health centers. The latter two services constituted a total number of visits of 2,836,127 corresponding to 44% of the total PHCC services utilization in 2021. The vaccination services utilization reached 2,219,894 visits in 2021.
Table 1.
PHCC COVID-19 services utilization in 2020 and 2021
| Type of Services | Utilization 2020 | Utilization 2021 |
|---|---|---|
| No. of drive-through testing | 119,791 | 616,233 |
| No. of vaccine administrated | 3,867 | 2,219,894 |
| Total no. of COVID related services | 123,658 | 2,836,127 |
Preventative services
In 2020, preventative services utilization rates were the most affected by the COVID-19 pandemic with significant reductions in the utilization rates in comparison to 2019, as illustrated in Table 2. The most drastic decline occurred in the utilization rate of breast cancer screening services at 79.5 and 100% reduction in the rates in 2020 and 2021, respectively. Colorectal cancer screening was among the preventative services that were affected significantly with a drop in the utilization rate by 83.7% in 2020 and 53.2% in 2021.
Table 2.
PHCC services utilization by type of service and the effect of COVID-19 on the utilization in 2020 and 2021 in reference to 2019
| Service type No. of visits by type of service | 2019 as baseline year No. of utilization | Year of 2020 | Year of 2021 | P | ||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||
| No. of utilization year 2020 | Difference in absolute number of service utilization to baseline year 2019 | Percentage of change compared to baseline year 2019 | No. of utilization 2021 | Difference in absolute number of service utilization to baseline year 2019 | Percentage of change compared to baseline year 2019 | |||
| Primary care core services | ||||||||
| Family medicine | 2,349,295 | 2,220,951 | −128,344 | −5.5 | 2,492,434 | 143,139 | 6.1 | <0.001 |
| Dental services | 385,155 | 269,116 | −116,039 | −30.1 | 288,015 | −97,140 | −25.2 | <0.001 |
| Maternal services | 45,905 | 40,217 | −5,688 | −12.4 | 44,564 | −1,341 | −2.9 | <0.001 |
| Primary care preventative services | ||||||||
| Well-baby/immunization services | 186,753 | 167,882 | −18,871 | −10.1 | 163,038 | −23,715 | −12.7 | <0.001 |
| Healthy lifestyle clinics | 120,807 | 73,764 | −47,043 | −38.9 | 118,404 | −2,403 | −2.0 | <0.001 |
| Smoking cessation | 3,809 | 2,280 | −1,529 | −40.1 | 3,286 | −523 | −13.7 | <0.001 |
| SMART annual health check | 10,211 | 3,694 | −6,517 | −63.8 | 2,158 | −8,053 | −78.9 | <0.001 |
| Colorectal cancer screening services | 18,868 | 3,076 | −15,792 | −83.7 | 8,821 | −10,047 | −53.2 | <0.001 |
| Breast cancer screening services | 10,552 | 2,165 | −8,387 | −79.5 | 0 | −10,552 | −100.0 | <0.001 |
| Primary care additional services | ||||||||
| Home health care services | 90,336 | 82,920 | −7,416 | −8.2 | 83,364 | −6,972 | −7.7 | <0.001 |
| Specialist Ophthalmology services | 90,650 | 64,703 | −25,947 | −28.6 | 85,924 | −4,726 | −5.2 | <0.001 |
| Specialist ENT services | 28,409 | 22,378 | −6,031 | −21.2 | 35,146 | 6,737 | 23.7 | <0.001 |
| Specialist dermatology services | 26,827 | 22,033 | −4,794 | −17.9 | 32,698 | 5,871 | 21.9 | <0.001 |
| Pharmacy services | 2,399,709 | 1,923,128 | −476,581 | −19.9 | 2,293,848 | −105,861 | −4.4 | <0.001 |
| Laboratory services | 671,099 | 992,757 | 321,658 | 47.9 | 1,665,583 | 994,484 | 148.2 | <0.001 |
| Radiology services | 172,328 | 137,887 | −34,441 | −20.0 | 174,261 | 1,933 | 1.1 | <0.001 |
| Mental health specialized services | 1,301 | 1,407 | 106 | 8.1 | 3,046 | 1,745 | 134.1 | <0.001 |
The annual health check for non-communicable diseases behavioral and metabolic risk factors called SMART check at PHCC demonstrated a steep decline in the services utilization in 2020 and 2021 at 63.8 and 78.9% reduction in the utilization rate in comparison to the 2019 level, respectively, as illustrated in Table 2. The associated healthy lifestyle clinics and smoking cessations’ services related to the non-communicable diseases risk factors showed a reduction in the services utilization in 2020 in 2021 with the highest reduction in 2020 compared to 2019 at 38.9 and 40.1%, respectively. Well-baby and immunization services showed a reduction in the utilization rate by 10.1 and 12.7% in 2020 and 2021, respectively.
Dental services
While the utilization rate of the PHCC dental services dropped by 30.1% in 2020 and 25.2% in 2021, family medicine services started inclining in 2021 in comparison to 2019 with 6.1% increase as demonstrated in Table 2. Home health care services demonstrated a slight reduction in the utilization in 2020 and 2021 in comparison to 2019 at 8.2 and 7.7%, respectively.
Additional services
Primary care-based mental health and laboratory services showed a sharp increase in utilization. Mental health services demonstrated a significant increase in services utilization in 2020 and 2021 with an increase of 134.1% captured in 2021. Laboratory services demonstrated a steady increase in the utilization rate in comparison to 2019 due to the additional COVID-19 testing services offered by the PHCC at the community level with the highest utilization rate increase at 148.2% in 2021, as shown in Table 2.
Discussion
The current study demonstrates a substantial reduction in the in-person visits in 2020 in comparison to 2019, as well as a progressive restoration of the in-person utilization rate in 2021, corresponding with the initial COVID-19 outbreak and the subsequent control of the outbreak, respectively. In person, the utilization rate had not recovered to its pre-COVID-19 level. The abrupt reduction in the number of PHCC health center visits was likely attributed to social distancing and restrictions associated with the COVID-19 outbreak[12] and the suspension of the PHCC non-urgent services in 2020 and 2021.[9] The inadequate knowledge of the virus and the fear of contracting the disease made patients and their family members reluctant to visit the health facilities.[12-15] Patients may have chosen to postpone or cancel their in-person care at the health centers even when the lockdown and the restrictions were lifted or relaxed.[12,15] The results show that there was a conversion of many in-person visits to the newly introduced teleconsultation services at the primary health care corporation. The latter trend was observed in many countries during SARC-COV-2 outbreak.[16,17] In China, due to the quarantine and social distancing needed, there has been a surge in the utilization of telehealth and virtual services provided by the traditional health facilities or via the technology companies during the pandemic.[17,18]
COVID-19 related services
Globally as all the countries started to roll out vaccines against SARS-COV-2, primary care providers have been playing a significant role.[19,20] In Qatar, the primary health care health centers have been at the forefront of the COVID-19 vaccination campaign. This was reflected in the increased utilization number of the COVID-19 related services, namely, the vaccination administration services especially in 2021. The increased vaccination utilization might be attributed to the trust in the primary health care staff, as trusted professionals who know their patients and are well placed to address the vaccine hesitancy among their target population.[21] Additionally, it might be attributed to the availability and accessibility of the primary health care centers in Qatar in which 27 health centers were operating in 2020.[22] Therefore, there was a trend observed in the increased number of people residing in Qatar registering at the PHCC health centers in 2020 and 2021.[23] However, the scale of the challenge of achieving high levels of vaccination, leaving no-one unprotected is great.[21] Due to the efforts put in place in Qatar, the two doses of COVID-19 vaccination coverage reached 89.7% of the total population by June 2022.[24]
Core health care services
Dental services
The delivery of dental services across much of the world has been affected heavily by the pandemic as of March 2020, due to the high infection risk associated with the aerosol-generated procedures, such as the use of high-speed drill.[25] The latter trend was observed in the PHCC dental services delivery where the services utilization was dropped significantly as of 2020. Additionally, many dental personnel during the pandemic were redeployed to frontline health services to provide a range of clinical procedures beyond their usual scope of practice which affected the dental services provision.[26] The teleconsultation dental services unlike the family medicine teleconsultation were limited due to the nature of dental cases and treatment.
Mental Health
The mental health services at the PHCC demonstrated a significant increase in the services utilization during the pandemic. The latter might be a result of the new strategies that were put in place including providing teleconsultations and allocating hotline for people seeking psychosocial support operating 24 h 7 days a week. In addition, communication campaigns were established to encourage the public to utilize the psychosocial teleconsultation services.[27]
Preventative health care services
Cancer screening
The cancer screening services for breast and colorectal cancer have been suspended and disrupted since the beginning of the COVID-19 outbreak which resulted in a substantial reduction in the services utilization in 2020 and 2021. The same pattern was observed in Italy and the UK, due to the implementation of the social distancing policies and the health care workers allocation to manage the COVID-19 cases.[28,29] In the UK, the number of people being screened and referred to a hospital with suspected lower gastrointestinal cancer, reduced sharply during the first lockdown and a deficit persisted up until September 2020.[30] The survival from colorectal cancer is closely associated with the stage of disease, with over 90% of those diagnosed at stage I surviving 5 years compared with only 10% at stage IV.[31] As delays in diagnosed enable tumors to continue to grow and advance.[32,33] Hence, the bottleneck in the diagnostic pathway is likely to have a profoundly detrimental impact on colorectal cancer outcomes in Qatar.[33] However, the cancer screening program at the PHCC has been working on developing a catch-up strategy to expand the services working hours in 2022 to reach out to the missed screening appointments.
Non-communicable diseases risk factors screening
The COVID-19 pandemic had an enormous effect on the PHCC efforts on screening for non-communicable diseases (NCDs) behavioral and metabolic risk factors. The PHCC health needs assessment in 2019 found out that the burden of NCDs among the PHCC registered population was high with almost 12–14% with type 2 diabetes, 12–16% with hypertension, and 9–11% with dyslipidemia.[22] Hence, the COVID-19 pandemic affected the PHCC efforts for early diagnostics and treatment for people with NCDs. The latter effect was observed in Europe during the restrictive measures such as social distancing, lockdown, and travel restrictions where people living with NCDs were impacted due to the limitation of their activity, ability to secure healthy foods, and access to prevention or health promotion services.[34]
Well-baby/immunization services
The well-baby and immunization services were slightly disrupted during the COVID-19 pandemic in 2020 and 2021. The disruption in the latter services might raise a concern that some of the public health gains realized by the immunization might be hindered.[35]
Finally, we found that nearly all the utilization rates for primary health care core and preventative services across the 28health centers had not recovered to per COVID-19 levels in 2019, despite relaxing the restriction measures as of June 2021. These reductions and stagnations in preventative services will be most likely to have substantial collateral effects on the population health that considerably exceed the direct effects of the infection.
This study is the first to quantify the effect of COVID-19 pandemic on the primary health care services in the state of Qatar over two years 2020–2021. The analysis is comprehensive with detailed services utilization data as per the type of services during and after the outbreak, covering the entire services provisions. Our results are subject to several limitations including the data collection errors, services type classification cannot be ruled out even though routine data were extracted and reported using standardized procedures.
Conclusion
In conclusion, our findings highlighted the crucial role that PHCC has played in the health system response to the COVID-19 and has continued to do so through the recovery phase. PHCC in Qatar has been the leader of the COVID-19 vaccination campaign and the COVID-19 drive-through testing services. Additionally, it provided alternative services such as telemedicine to overcome the barriers of the physical inaccessibility factors associated with the COVID-19 outbreak. Our study demonstrates the disruption in the PHCC core and preventive services utilizations due to the COVID-19 outbreak in addition to highlighting the vital role that PHCC stepped up in terms of leading the COVID-19 vaccination campaign in Qatar.
However, future research is needed to establish which vulnerable patient groups were most affected by the pandemic, to continue to inform strategies and policies directed at mitigating the impact of future potential pandemics.
Ethical approval
The impact of the COVID-19 on primary health care services in Qatar study was approved by the PHCC scientific and IRB committee with reference number PHCC/DCR/2020/07/077.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to extend their gratitude to all the frontline health care workers at the PHCC health centers for their continued efforts and dedication throughout the pandemic.
References
- 1.Majeed A, Maile EJ, Bindman AB. The primary care response to COVID-19 in England's National Health Service. J R Soc Med. 2020;113:208–10. doi: 10.1177/0141076820931452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Leszczyński PK, Sobolewska P, Muraczyńska B, Gryz P, Kwapisz A. Impact of COVID-19 pandemic on quality of health services provided by emergency medical services and emergency departments in the opinion of patients: Pilot study. Int J Environ Res Public Health. 2022;19:1232. doi: 10.3390/ijerph19031232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Moynihan R, Sanders S, Michaleff ZA, Scott AM, Clark J, To EJ, et al. Impact of COVID-19 pandemic on utilisation of healthcare services: A systematic review. BMJ Open. 2021;11:e045343. doi: 10.1136/bmjopen-2020-045343. doi: 10.1136/bmjopen-2020-045343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.World Health Organization. Regional Office for the Western Pacific. Role of primary care in the COVID-19 response. Manila: WHO Regional Office for the Western Pacific; 2020. [Last accessed on 2022 Feb 17]. Available from: https://apps.who.int/iris/handle/10665/331921 . [Google Scholar]
- 5.Primary Health Care Corporation. Annual Statistical Report 2019. Doha: Primary Health Care Corporation; 2020. [Last accessed on 2022 Feb 20]. Available from: https://www.phcc.gov.qa/assets/phcc/PHCC%20Annual%20Statistical%20Report%20%202019.pdf . [Google Scholar]
- 6.Ministry of Public Health. Coronavirus Disease 2019 (COVID-19) Updates. Qatar. 2022. [Last accessed on 2022 Jun 09]. Available from: https://covid19.moph.gov.qa/EN/Pages/default.aspx .
- 7.Bsat R, Chemaitelly H, Coyle P, Tang P, Hasan MR, Al Kanaani Z, et al. Characterizing the effective reproduction number during the COVID-19 pandemic: Insights from Qatar's experience. J Glob Health. 2022;12:05004. doi: 10.7189/jogh.12.05004. doi: 10.7189/jogh. 12.05004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Altarawneh HN, Chemaitelly H, Hasan MR, Ayoub HH, Qassim S, AlMukdad S, et al. Protection against the Omicron variant from previous SARS-CoV-2 Infection. N Engl J Med. 2022;386:1288–90. doi: 10.1056/NEJMc2200133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Al-Kuwari MG, Abdulmalik MA, Haj Bakri A, John G, Kandy MC, Swamy S, et al. The COVID-19 pandemic impact on primary health care services: An experience from Qatar. Middle East J Family Med. 2021;19:105–10. [Google Scholar]
- 10.Al-Zaidan M, Mohamed Ibrahim MI, Al-Kuwari MG, Mohammed AM, Nawaz Mohammed M, Al Abdulla S. Qatar's primary health care medication home delivery service: A response toward COVID-19. J Multidiscip Healthc. 2021;14:651–7. doi: 10.2147/JMDH.S282079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Al-Kuwari MG, Abdulmalik MA, Al-Mudahka HR, Bakri AH, Al-Baker WA, Abushaikha SS, et al. The impact of COVID-19 pandemic on the preventive services in Qatar. J Public Health Res. 2021;10:1910. doi: 10.4081/jphr.2021.1910. doi: 10.4081/jphr.2021.1910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Delamou A, El Ayadi AM, Sidibe S, Delvaux T, Camara BS, Sandouno SD, et al. Effect of Ebola virus disease on maternal and child health services in Guinea: A retrospective observational cohort study. Lancet Global Health. 2017;5:e448–57. doi: 10.1016/S2214-109X(17)30078-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Madhuripan N, Cheung HMC, Alicia Cheong LH, Jawahar A, Willis MH, Lar- son DB. Variables influencing radiology volume recovery during the next phase of the coronavirus disease 2019 (COVID-19) pandemic. J Am Coll Radiol. 2020;17:855–64. doi: 10.1016/j.jacr.2020.05.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Zhao J, Li H, Kung D, Fisher M, Shen Y, Liu R. Impact of the COVID-19 epidemic on stroke care and potential solutions. Stroke. 2020;51:1996–2001. doi: 10.1161/STROKEAHA.120.030225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Modesti PA, Wang J, Damasceno A, Agyemang C, Van Bortel L, Persu A, et al. Indirect implications of COVID-19 prevention strategies on non-commu- nicable diseases: An opinion paper of the european society of hypertension working group on hypertension and cardiovascular risk assessment in subjects living in or emigrating from low resource settings. BMC Med. 2020;18:256. doi: 10.1186/s12916-020-01723-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mann DM, Chen J, Chunara R, Testa PA, Nov O. COVID-19 transforms health care through telemedicine: Evidence from the field. J Am Med Inf Assoc. 2020;27:1132–5. doi: 10.1093/jamia/ocaa072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Liu S, Yang L, Zhang C, Xiang YT, Liu Z, Hu S, et al. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry. 2020;7:e17–8. doi: 10.1016/S2215-0366(20)30077-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mou M. Covid-19 gives boost to China's telemedicine industry: The wall street journal. 2020. [Last accessed on 2022 Apr 11]. Available from: https://www.wsj.com/articles/covid-19-gives-boost-to-chinas-telemedicine- industry-11603379296#:~:text=The%20coronavirus%20pandemic%20has%20led,medical%20advice%20from%20doctors%20online.&text=And%20JD%20Health% 2C%20the%20health, an%20online%20family%2Ddoctor%20service .
- 19.Harnden A, Lim WS, Earnshaw A. COVID-19 vaccination programme: A central role for primary care. Br J Gen Pract. 2021;71:52–3. doi: 10.3399/bjgp21X714929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.World Health Organization, United Nations Children's Fund. Guidance on developing a national deployment and vaccination plan for COVID-19 vaccines: Interim guidance, 16 November 2020. Geneva: World Health Organization; 2020. [Last accessed on 2022 May 14]. Available from https://apps.who.int/iris/handle/10665/336603 . [Google Scholar]
- 21.Kluge H, McKee M. COVID-19 vaccines for the European region: An unprecedented challenge. Lancet. 2021;397:1689–91. doi: 10.1016/S0140-6736(21)00709-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Al-Kuwari MG, Al-Abdulla SA, Abdulla MY, Haj Bakri A, Mohammed AM, Kandy MC, et al. Epidemiological health assessment in primary healthcare in the State of Qatar-2019. Qatar Med J. 2021;2021:57. doi: 10.5339/qmj.2021.57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Primary Health Care Corporation. Annual Statistical Report 2021. Doha: Primary Health Care Corporation; 2022. [Google Scholar]
- 24.Ministry of Public Health. Coronavirus Disease 2019 (COVID-19) Updates Qatar, 2022. [Lases accessed 2022 Jun 14]. Available from: https://covid19.moph.gov.qa/EN/Pages/Vaccination-Program-Data.aspx .
- 25.BBC. Coronavirus: Man refused appointment pulls out tooth at home April 18, 2020. [Last accessed on 2022 May 29]. Available from: https://www.bbc.co.uk/news/uk-englanddevon-52321910 .
- 26.Watt R. COVID-19 is an opportunity to reform in dentist. [Last accessed 2022 Apr 10];Lancet. 2020 396 doi: 10.1016/S0140-6736(20)31529-4. Available from: https://www.thelancet.com/action/showPdf?pii=S0140-6736%2820%2931529-4 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Nazeer S, Issa S. Community mental health interventions during the Covid19 pandemic. J Community Med Public Health. 2020;4:198. [Google Scholar]
- 28.National Institute for Health and Care Excellence. National Institute for Health and Care Excellence; July 26, 2017. Suspected Cancer: Recognition and referral. [Last accessed on 2022 May 15]. Available from: https://www.nice.org.uk/guidance/ng12 .
- 29.Maringe C, Spicer J, Morris M, et al. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020;21:1023–34. doi: 10.1016/S1470-2045(20)30388-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Morris EJA, Goldacre R, Spata E, Mafham M, Finan PJ, Shelton J, et al. Impact of the COVID-19 pandemic on the detection and management of colorectal cancer in England: A population-based study. Lancet Gastroenterol Hepatol. 2021r;6:199–208. doi: 10.1016/S2468-1253(21)00005-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cancer Research UK. Colorectal cancer survival by stage. 2020. [Last accessed 2022 Apr 10]. Available from: https://www.cancerresearchuk.org/health-professional/cancerstatistics/statistics-by-cancer-type/bowel-cancer/survival#heading-Three .
- 32.Lee YH, Kung PT, Wang YH, Kuo WY, Kao SL, Tsai WC. Effect of length of time from diagnosis to treatment on colorectal cancer survival: A population-based study. PLoS One. 2019;14:e0210465. doi: 10.1371/journal.pone.0210465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hanna TP, King WD, Thibodeau S, Jalink M, Paulin GA, Harvey-Jones E, et al. Mortality due to cancer treatment delay: Systematic review and meta-analysis. BMJ. 2020;371:m4087. doi: 10.1136/bmj.m4087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.WHO. Noncommunicable diseases in emergencies. Geneva: World Health Organization; 2016. [Last accessed 2022 Jun 10]. Available from: https://apps.who.int/iris/bitstream/handle/10665/204627/WHO_NMH_NVI_16.2_eng.pdf . [Google Scholar]
- 35.Ota MOC, Badur S, Romano-Mazzotti L, Friedland LR. Impact of COVID-19 pandemic on routine immunization. Ann Med. 2021;53:2286–97. doi: 10.1080/07853890.2021.2009128. [DOI] [PMC free article] [PubMed] [Google Scholar]