

ABSTRACT
Background:
Posttraumatic rehabilitation of sports injuries involves physiotherapy. Additionally, nonsurgical treatment of sports injuries involves regular physiotherapy as a major treatment therapy. This study aimed to evaluate the effects of yoga in addition to regular physiotherapy on these patients.
Materials and Methods:
In the present comparative study, we evaluated the effects of regular physiotherapy alone versus physiotherapy combined with yoga on 212 patients following various knee injuries treated nonsurgically. The study was conducted after obtaining hospital ethical, committee clearance, and written informed consent from patients. The patients were assigned into two groups: group C (Conventional) and group Y (Yoga group). The patients in the regular group received physiotherapy rehabilitation program, whereas the yoga group received additional yoga once every day by a yoga expert during their hospital stay. We provided written guidelines and photographs of the yoga asanas and instructed to perform them 3 days/week once they were home. The data on WOMAC score were collected at 6 weeks, 3 months, and at 6 months from the day of discharge from the hospital.
Results:
We noted that the yoga group patients showed a significant improvement (P < 0.05) in all modalities like pain, stiffness, and function subscales of the WOMAC scale. They experienced significant reduction in pain and stiffness compared with the regular or conventional group on the seventh postinjury day, 6 weeks, 3 months, and 6 months after the initial injury.
Conclusion:
In this study, a combination of regular physiotherapy and yoga provided better functional outcomes than physiotherapy alone.
Keywords: Nonsurgical treatment, physiotherapy, sports injuries, yoga
Introduction
Sports related injuries are common injuries that constitute major joint and ligament dysfunction worldwide. Since the sports industry is very competitive and lucrative for sportspersons along with high intensity of physical and emotional involvement of players, there has lately been an increase in sports related injuries.[1,2,3] This intensified the physical and emotional aspects and burden of sports and its related injuries. In modern competitive sport, injured sportspersons are under constant pressure to return to their games as early as possible. Hence, compared to traditional rehabilitation after injury, sports injuries’ rehabilitation requires more care. Therefore, a highly structured sports-specific approach should be adopted for athletes and injured tissues according to the physical and psychological demands at the highest level of sport. The growing popularity of various sports like football, hockey, badminton, and kabaddi leagues in India is evidence of a growing sports culture in our country apart from the predominantly favored cricket. The awareness regarding the role of yoga in sports related injuries among primary physicians will help in treatment and rehabilitation of those patients who cannot afford costly physiotherapy, especially in rural setups.
This study attempts to evaluate the outcome of rehabilitation using regular or conventional physiotherapy versus physiotherapy combined with yoga in various sports injuries treated nonsurgically.
Injuries in any sports can occur through various mechanisms and may constitute acute or overuse injuries.[4] Sports injuries may involve ligaments, muscle, and fractures. Musculoskeletal injuries are the commonest injuries in sports and comprises 80% of all injuries.[5,6] Joint injuries, especially of the knee, is the commonest of injuries in all sportsmen. Not only the knee but also elbow, hip, and back can get injured depending on the mechanism of injury. These injuries require operative and nonoperative management followed by a long rehabilitation period, as documented by Kujala et al.[7] Musculoskeletal flexibility, stability, muscle strength, and balance can be increased through yoga and physical therapy. These activities bring improvement in injured sportspersons and subsequently increase perception regarding usefulness of the therapeutic yoga and physical therapy. Brewer et al.[8] described a biopsychosocial model that helps to understand rehabilitation following a sport injury. He also explained that physiotherapy and yoga, when combined in rehabilitation, could improve the psychological and biological factors that have a positive and significant effect on the biopsychological outcomes. However, both authors, Whiting[9] and Ravi,[10] have also reported a favorable outcome following inclusion of yoga in rehabilitation program. In our study, we explore the usefulness of yoga in sport injury rehabilitation. Combined efforts of yoga therapists, physiotherapists, sport medicine experts, and trainers might help sportspersons to enhance adherence to sport injury rehabilitation programs.
In spite of the high frequency and morbidity following injuries in sportspersons, there are no studies from India focusing on the outcome of these injuries using yoga along with physiotherapy.
Material and Methods
We included 212 patients with various sports injuries treated in nonsurgical ways in a prospective cohort study. The present study was conducted between April 2018 and July 2021. Approval was obtained from the hospital ethical committee, where the study was conducted.
Inclusion criteria
-
(a)
Age: 15 to 60-year-old
-
(b)
Patient with knee, shoulder, and back injury
-
(c)
On MRI, no major ligaments tear, which requires surgical management
Exclusion criteria
-
(a)
Patients with significant ligament injuries that required surgical management
-
(b)
Patients with neurovascular deficit
Written consent was obtained after a discussion about the study with the included population. The patients were divided into two groups: group C (Conventional) and group Y (Yoga group). Randomization was done using a random number table obtained from the computer and the closed envelopes of the patients were randomly distributed into two groups in a 1:1 ratio (C: Y group). Thus, 105 patients in group C and 107 patients in group Y were included. The conventional group patients received routine physiotherapy protocol, whereas patients in the yoga group received traditional physiotherapy combined with yoga (asanas) wherein the asanas were modified as per injury and requirement. We followed CLARIFY guideline in our yoga therapy as adopted by Moonaz et al.[11]
Delivery of yoga and its period, frequency, and duration of each yoga session in the hospital was monitored. After discharge, adherence to home practice was measured via WhatsApp or video chatting and physical attendance in OPD. Home practice or lesion of yoga was provided in the form of printed pictures of yoga assanas and videos uploaded on the mobiles of the patients. Periodic video chats, questioners, and physical follow ups in OPD was used as strategies and to promote practice adherence.
Baseline WOMAC scores for pain and stiffness were evaluated on the seventh postinjury day. The yoga group received yoga asanas at least once every day from the hospital yoga expert during their stay. At the time of discharge, patients were handed out written instructions and photographs of the asanas. All patients were followed up and WOMAC response was recorded at 6 weeks and 3 months from the day of discharge. All the patients were available for follow-up till 6 months as they resided in the same cantonment and could be contacted over the telephone. Frequency of yoga was advised 3 days/week after discharge from the hospital.
Initial management protocol involved only RICE for first 3–7 days (rest, ice, immobilization, and analgesic) and from 7–14th day, yoga was started by the instructor along with physiotherapy; after discharge, yoga was recommended thrice a week on their own via pictures/videos etc.
The yoga asanas are the combination of many body functional postures, which are included in the present study as shown in Figure 1.
Figure 1.

Yoga asanas and their pictorial posture, used in the present study
For Knee injury
Regular physiotherapy: Ultrasonic and short-wave therapy for 5–7 days followed by hamstring and quadriceps strengthening exercises after 7th postinjury days.
Additional yoga asanas for yoga group
-
(a)
3–7 days postinjury: Shavasana, Tadasana, and Paschimottanasana was started twice daily for 10 min
-
(b)
After 1 week: Pavanamuktanasana and Baddha-konasana was started thrice daily for 10 min
-
(c)
3rd week postinjury: Ardha shalabasana was started thrice daily for 10 min
-
(d)
6th weeks: Virbhadrasana and Utkatasana was started thrice daily for 15 min
For shoulder injury
Regular physiotherapy: Ultrasonic and short-wave therapy for 5–7 days followed by deltoid and rotator cuff strengthening and ROM exercises after 7th postinjury days.
Additional yoga asanas for yoga group
-
(a)
3–7 days postinjury: Shavasana, Tadasana, and Paschimottanasana was started twice daily for 10 min
-
(b)
After 1 week: Garudasana and Parsvottanasana was started twice daily for 10 min
-
(c)
3rd week postinjury: Ardha shalabasana was started thrice daily for 15 min
-
(d)
6th weeks: Virbhadrasana II, Prasarita Padotanasana, Phalakasana, and Gomukasana was started thrice daily for 15 min
For back injury
Regular physiotherapy: After initial RICE application, hot pack therapy was applied for 20 min and ultrasonic therapy for 5 min in continuous form at a frequency of 1 MHz and a density of 1.5 W/cm2 daily for 7 days. Additionally, TENS (Transcutaneous epidermal nerve stimulation) treatment was provided in continuous form with strength of 100 Hz, 40 μSN for 30 min after 7th postinjury days for thrice a day for 7 to 10 days.
Additional yoga asanas for yoga group
-
(a)
3–7 days postinjury: Shavasana and Bhujangasana was started twice daily for 10 min
-
(b)
After 1 week: Makarasana Supta was started twice daily for 10 min
-
(c)
3rd week postinjury: Padangustasana was started thrice daily for 15 min
-
(d)
6th weeks: Tiryak Bhujangasana, Shashankasana, Supta padangustasana, and Parivrtta supata padangustasana was started thrice daily for 15 min
All yoga sessions were delivered using audio-visual screen in the presence of yoga instructor.
Sample size calculation
For each group to achieve a power of 80% and a level of significance of 5% (two sided), for detecting a true difference in means between the test and the reference group of a sample size of 10 units in total comes to 72 (assuming equal size group, 36 in each group). At 95% confidence interval (α = 0.05) with population variance of 0.64° and 80% power (β = 0.2), was 385. Considering 10% was lost to follow up during a study period, a sample size of 36 patients in each group was required (our N = 105 and 107).
Statistical analysis
We used SPSS version 19 (IMB USA) and MS Excel 2007 for data analysis. Relative differences were calculated for the time duration in both groups, and Mann–Whitney U test was used to compare. Wilcoxon sign ranked test was used for paired scores. Spearman’s correlation coefficient was used for comparison and Mann–Whitney U test was used for the difference between genders in functional scores. The level of significance was taken when P < 0.05.
Results
We divided our study population into two groups: Conventional group (C group) with 105 patients and Yoga group (Y group) with 107 patients with mean age 37.5 ± ± 4.12 and 36.3 ± 3.27 years, respectively. There were 72 males and 33 females in C group and 89 males and 18 females in Y group. The mean BMI for all the subjects was 23.34 ± 9.45 (16.3–35.4). Cricket and football contributed to a significant amount of injuries while knee joint was predominantly involved [Table 1].
Table 1.
Demographical characteristics of the study population
| Parameters | C-group (n=105) | Y group (n=107) | P |
|---|---|---|---|
| Mean Age in years | 37.5±4.12 | 36.3±3.27 | 0.361 |
| Sex | |||
| Male | 72 | 89 | 0.562 |
| Female | 33 | 18 | 0.024 |
| BMI ( in kg/m2) | |||
| 16-18.5 (mean 13±6.12) | 13 | 9 | 0.043 |
| 18.5-25 (mean 15±12.43) | 49 | 63 | 0.051 |
| 25-30 (mean 18±13.17) | 34 | 29 | 0.673 |
| 30-35 (mean 26±16.23) | 9 | 6 | 0.624 |
| Mode of Injury | |||
| Badminton | 17 | 11 | 0.545 |
| Cricket | 23 | 29 | 0.442 |
| Football | 41 | 36 | 0.723 |
| Running | 15 | 19 | 0.651 |
| Basketball | 9 | 12 | 0.035 |
| Site of injury | |||
| Shoulder | 17 | 12 | 0.675 |
| Knee | 77 | 79 | 0.645 |
| Back | 11 | 16 | 0.623 |
| Types of injury | |||
| Knee MCL sprain | 23 | 31 | 0.692 |
| Hamstring strain | 29 | 23 | 0.765 |
| Knee LCL sprain | 9 | 4 | 0.612 |
| Quadriceps strain | 18 | 28 | 0.021 |
| Knee fat pad injury | 11 | 7 | 0.042 |
| Patello-femoral pain syndrome | 19 | 14 | 0.373 |
| Biceps tendinitis Shoulder | 8 | 2 | 0.056 |
| Acromioclavicular joint sprain | 5 | 3 | 0.512 |
| Rotator cuff injury shoulder | 4 | 7 | 0.564 |
| Lumbar sacral strain | 9 | 7 | 0.673 |
| Acute muscle spasm of lower back | 8 | 9 | 0.576 |
The mean scores of WOMAC pain and stiffness and the function score at 7th postinjury day at 6 weeks, 3 months, and 6 months were recorded and a significant difference in pain and stiffness was noted at 6 months with C group: 6.33 ± 1.34. In Y group, it was 1.66 ± 1.12 (P = 0.0024) [Table 2].
Table 2.
Pain, stiffness and function subscale of WOMAC scale in conventional and Yoga group at 7th postinjury day, 6 weeks, 3 months, and 6 months
| Group | Pain and stiffness | Function | |||||
|---|---|---|---|---|---|---|---|
|
|
|
||||||
| 7th days postinjury | 6 weeks | 3 months | 6 months | 6 weeks | 3 months | 6 months | |
| C | 35.54±6.12 | 21.23±5.42 | 12.38±4.11 | 6.33±1.34 | 13.09±4.22 | 9.44±3.25 | 7.02±2.88 |
| Y | 30.24±8.18 | 16.31±3.04 | 4.01±4.08 | 1.66±1.12 | 10.32±5.16 | 5.03±4.09 | 5.41±1.31 |
| P | 0.0021* | 0.0034* | 0.0042* | 0.0024* | 0.0033* | 0.0014* | 0.00132* |
*Denote significance
We recorded lower absolute values of the variables in the yoga group than in the conventional group. We considered the 7th postinjury days as the baseline and compared it with subsequent follow-ups at 6 weeks, 3 months, and 6 months. We recorded a significant improvement in all scores at 6 weeks, 3 months, and 6 months as compared with the 7th postinjury days in both the groups [Table 3].
Table 3.
Pain, stiffness and function subscale of WOMAC scale in both groups
| Group | Pain and stiffness | Function | |||||
|---|---|---|---|---|---|---|---|
|
|
|
||||||
| 7th days postinjury | 6 weeks | 3 months | 6 months | 6 weeks | 3 months | 6 months | |
| C | P=0.002 | P=0.003 | P=0.004 | P=0.002 | P=0.004 | P=0.003 | P=0.005 |
| Y | P=0.001 | P=0.002 | P=0.001 | P=0.003 | P=0.001 | P=0.002 | P=0.003 |
Mann-Whitney u test was used to compare between both groups for which P<0.05
While comparing the percentage reduction in pain and stiffness at 6 months in both groups, we recorded significant improvement in WOMAC scores in yoga group (48.52 vs. 9.11, P = 0.0012) as compared to conventional group. We also noted significant overall functional improvement in yoga group (63.23 vs. 23.65, P = 0.0011) as compared to conventional group [Table 4].
Table 4.
Percentage reduction in pain, stiffness and function subscale of WOMAC scale in conventional physiotherapy and physiotherapy combined with Yoga group
| Group | Improvement in Pain and stiffness at 6 weeks (%) | Improvement in Pain and stiffness at 3 months (%) | Improvement in Pain and stiffness at 6 months (%) | Improvement in Function at 6 months (%) |
|---|---|---|---|---|
| C | 18.12 | 12.43 | 9.11 | 23.65 |
| Y | 24.86 | 32.18 | 48.52 | 63.23 |
| P | 0.0027 | 0.0032 | 0.0012 | 0.0011 |
Percentage reduction of pain, stiffness score at 6 weeks, 3 months, and 6 months, compared to 7th postinjury days, and percentage reduction in function score at 6 months compared to 6 weeks.
Discussion
The objective of our study was to evaluate the effects of additional yoga combined with regular or conventional physiotherapy for functional outcome of patients after various sports injuries. We noted that patients using yoga experienced better pain relief, less stiffness, and better outcome. We did not record any adverse effects in any group. We believe yoga asanas are safe for rehabilitation following various sports related injuries, which were treated nonsurgically as few published data supports our view.[12,13]
In the present study, we noted that pain relief was significant in yoga group, as compared to the regular therapy group. Our finding is supported by similar results obtained by few authors.[1 3,12] Role of yoga in osteoarthritis knee and chronic back pain has been recorded by Kolasinski et al.[14] and Chang et al.,[15] respectively. However, Sadiri et al.[16] and Garfinkel et al.[17] reported a favorable outcome in pain relief in musculoskeletal discomfort and in carpel tunnel syndrome of wrist post yoga, respectively. They also recorded that yogasanas are beneficial in reducing the intensity of pain and improving function. From the above published data, it is encouraging to add additional yoga therapy along with conventional physiotherapy for faster rehabilitation.
Shavasana had contributed in the reduction of pain by relaxation of Musculoskeletal system. This further reduces nerve signals and helps in the relaxation of the skeletal muscles.[18,19]
Stimulation of inhibitory pain pathways can be activated by the conscious relaxation in Shavasana. It would help in reduction of impulses in the motor neuron and thus assist in muscle relaxation and in turning pain to relief.[18,19] Therefore, the yoga group experienced the dual advantage of muscle strengthening and relaxation of the muscles enabling faster recovery. Bera et al.[20] and Sharma et al.,[21] have found Shavasana as very effective in reducing the effects of stress. Büssing et al.[22] and Malathi et al.[23] recorded positive effects of yoga on subjective well-being. Hagins et al.[24] and Chaudhary et al.[25] noted positive effects of Shavasana in hypertension. Streeter et al.[26] noted a 27% increase in GABA levels in 19 patients in the yoga practice group than walking group after the yoga session (0.20 mmol/kg). They also reported more improvement in mood and anxiety after the 12-week yoga compared with an only walking exercise group.
According to Maughan RJ and Shirreffs SM, after the injury, muscles around joints usually develop spasms and tightness because of the acute phase.[27] After the acute phase, gait difficulties may appear due to low pain tolerance, which directly affects the knee and hip flexors.
Muscle spasm can be reduced by various physiotherapy protocols and there was significant improvement in both the groups in our study as well. By adding yoga asanas, it may influence many body parts in a positive way.
Yoga asanas like Virabhadrasana, Ardha-shalabhasana, Badhakonasana, Pawanamuktasana, Utkatasana, Utthita Trikonasana, and Bhujangasana involve isometric contraction of agonists and stretching of antagonists.[8] Kisner C in his book described that Shavasana helps in relaxation and improvement of psychological well-being.[28] Holding postures leads to increase in joint stability, relaxation of muscles in spasm improving their excursion around the joints, thus overall improvement in function and pain relief. Many authors noted the role of Golgi tendon organs (GTO) in muscle relaxation during Yoga practice.[29 32] They also noted that during yoga, on applying slow stretch to the muscle, firing of GTO occurs and reduces tension in the muscle, allowing it to relax.
Carlson et al.[33] demonstrated that yoga stretches the muscle and tendon and reduces pain and suffering in the study population. Stretching of muscle affects EMG activity of the muscles. Therefore, relaxation of muscle and tendon leads to a feeling of well-being. Hip and back pain can be improved by using Ardha Shalabhasana, which acts on the hip flexor, back extensors muscle, and forward placement of the pelvis and trunk. That may shift the center of gravity slightly anterior to the hip and lead to relaxation of these muscles. Thus, by doing so, Ardha Shalabhasana stretches the hip flexors and extensors, which helps to reduce the spasm and improve function and gait.
Yoga, along with conventional physiotherapy, has demonstrated improvement in knee function and quality of life in patients with sport injuries treated nonsurgically. This could be possible because yoga has the ability to offer better emotional stability.[34 36] In many sports, it has been noted that the injured patients are psychologically depressed of fear whether they will ever return to sports and if injury will have an adverse impact on outcomes. Many authors have reported the beneficial effects of yoga in psychological distress.[37 40] Various authors noted that yoga helps in reducing psychological stress. It further induces pain relief through increased endorphins secretion in the brain, which improves function.[41 43]
Mechanism of effects of yoga
Mahajan[44] has recorded the mechanisms involved in the therapeutic effects of yoga. Yoga may have influence on the central nervous system, ANS, limbic system, HPA (Hypothalamo pituitary adrenal) axis, and the immune system to work together to maintain the hormonal homeostasis as shown in Figure 2.
Figure 2.
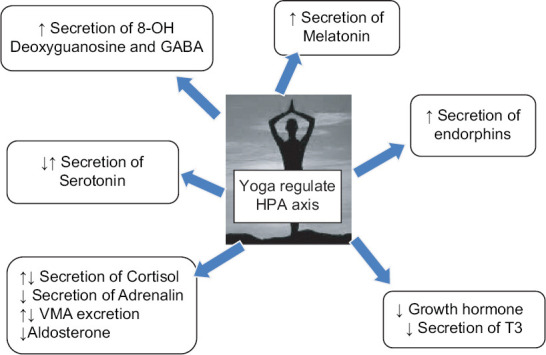
Yoga regulates the level of hormones and neurotransmitters that affect physiological functions
Yoga and hormones/neurotransmitters
Many authors studied and evaluated the effect of yoga in the endocrine homeostasis. Walton et al.[45] and Jevning et al.[46] have noted that plasma cortisol and testosterone concentration changes during the “transcendental meditation.” Arora et al.[47] observed effect of yoga on stress and the immune system and noted that yoga plays a vital role in regulating the cytokine levels and hence, the immune responses during stress. Bevan[48] reported an alteration in hypothalamic and pituitary function following yoga. Vandana et al.[49] have shown a decrease in the serum adrenaline and cortisol levels following Amrita meditation. Vera et al.[50] have reported an increase in serum cortisol level in patients involving long-term yoga practices.
Yoshihara et al.[51] noted that decreased levels of 8-hydroxydeoxyguanosine may be an indicator of psychological stress. Newberg et al.[52] recorded increased levels of β endorphin in the individuals practicing yoga daily.
Chatterjee et al.[53] recorded improvement in T4, T4, and TSH level following yoga therapy; similarly, Chatterjee et al.[54] observed improvement in GH (growth hormone) and dehydroepiandrosterone sulfate (DHEAS) level following yoga therapy. However, yogic practices such as the Sarvangasana increases the protein bound serum iodine and improves function of the thyroid gland.[53,55] Streeter et al.[56] noted a sharp increase in GABA following an hour of yoga practice, as shown by magnetic resonance spectroscopy. Both Shettyet et al.[57] and Jevning et al.[58] have noted the increased level of serum prolactin following meditation, especially “sudarshan kriya”.
Yoga in specific condition
-
(a)
Back pain: In spinal region, mal-alignment of the musculoskeletal components of neck and lower back is the commonest cause for backache and neck pain. Relaxation asanas [shavasana, makarasana] followed by stretching [ardhamatsyendrasana, ardhakati chakrasana,] and muscle strengthening asanas [Bhujangasana and shalabhasana] help, as suggested by Williams et al.[59] However, strengthening asanas should not be incorporated too early as they can aggravate the pain.
-
(b)
Neuropathic pain: Neuropathic pain is caused by nerve damage proximal to the sensory nerve endings or over stretching. A holistic approach is to be adopted for recovery. Yogas like “yoga nidra” with visualization, body awareness, breathing, and gentle equivalent stretch asanas is used for muscle group relaxation. Garfinkel et al.[17] demonstrated that by improving flexibility; correcting alignment of shoulder, arms, wrist, and hand is important in alleviation pain. He also advocated stretching and increasing awareness of optimal joint position to minimize symptoms of specific areas like carpal tunnel syndrome.
-
(c)
Knee pain: Few authors reported encouraging results of yoga in knee rehabilitation following surgery on skier, and they suggested that yoga and physiotherapy as a combined modality may increase the biological and psychological well-being.[10]
Recently, Sharma et al.[60] included patients of 18–60 years in a randomized wait list-controlled trial; diagnosed with musculoskeletal conditions including rheumatoid arthritis, osteoarthritis, low back pain, joint pain, muscle pain, or chronic nonmalignant pain with mild to moderate intensity. He noted that after 16 weeks of yoga, an effective pain relief was achieved in patients with chronic musculoskeletal pain. To summarize, all these cumulative data suggest that yoga greatly influences endocrine homeostasis and plays a vital role in psychological well-being, cheerfulness, modified immune system, and overall musculoskeletal function.
Limitations of the study
The study includes a few limitations that need to be addressed. First, level of activities and environment in which injury occurred were not considered. Second, seasonal variation of these injuries was also not considered. Third, the difference in number of women patients in the control versus yoga group is also a limitation of this study.
Role of primary physician
Primary physician can play a vital role in timely and supervised yoga sessions and provide awareness regarding importance of yoga in sports injury rehabilitation.
Key point: The results of present study indicated that when yoga combined with conventional physiotherapy in rehabilitation of sports related injuries gives better result as compared with physiotherapy alone.
Conclusion
The present study showed that the yoga group experienced significant improvements in all WOMAC scale subscales compared to the conventional physiotherapy group. A more extensive randomized controlled study will be required to validate the results further to reach a definitive conclusion. Yoga may influence the pain pathway and its management and improve function in sports injury when used in conjunction with conventional physiotherapy.
Declarations
-
(a)
Declaration of Conflicting Interests: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
-
(b)
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
-
(c)
Authors declare no patents, no copyrights, or royalties applicable to present study.
-
(d)
Authors also declare no relationships or activities that could have influenced the content of the submitted work.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
Authors will like to acknowledge the wholly hearted participation of patients and those helped in this study.
References
- 1.Patel DR, Yamasaki A, Brown K. Epidemiology of sports-related musculoskeletal injuries in young athletes in United States. Transl Pediatr. 2017;6:160–6. doi: 10.21037/tp.2017.04.08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.McKeever CK, Schatz P. Current issues in the identification, assessment, and management of concussions in sports-related injuries. Appl Neuropsychol. 2003;10:4–11. doi: 10.1207/S15324826AN1001_2. [DOI] [PubMed] [Google Scholar]
- 3.Hind K, Konerth N, Entwistle I, Theadom A, Lewis G, King D, et al. Cumulative sport-related injuries and longer term impact in retired male Elite-and Amateur-Level rugby code athletes and non-contact athletes:A retrospective study. Sports Med. 2020;50:2051–61. doi: 10.1007/s40279-020-01310-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ardern CL, Glasgow P, Schneiders A, Witvrouw E, Clarsen B, Cools A, et al. 2016 Consensus statement on return to sport from the First World Congress in Sports Physical Therapy, Bern. Br J Sports Med. 2016;50:853–64. doi: 10.1136/bjsports-2016-096278. [DOI] [PubMed] [Google Scholar]
- 5.Rice SG. Care of the Young Athlete. Elk Grove Village (IL): American Academy of Orthopaedic Surgeons and American Academy of Pediatrics; 2000. Risks of Injury During Sports Participation; pp. 9–18. [Google Scholar]
- 6.Patel DR, Luckstead EF, Greydanus DE. Sports injuries. In: Greydanus DE, Patel DR, Pratt HD, editors. Essential Adolescent Medicine. McGraw-Hill; New York: 2006. pp. 677–92. [Google Scholar]
- 7.Kujala UM, Taimela S, Antti-Poika I, Orava S, Tuominen R, Myllynen P. Acute injuries in soccer, ice hockey, volleyball, basketball, judo, and karate:Analysis of national registry data. BMJ. 1995;311:1465–8. doi: 10.1136/bmj.311.7018.1465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Brewer BW. The role of psychological factors in sport injury rehabilitation outcomes. Int Rev Sport Exerc Psychol. 2010;3:40–61. [Google Scholar]
- 9.Whiting ND. The role of yoga therapy in knee rehabilitation. Int J Yoga Ther. 2006;16:79–94. [Google Scholar]
- 10.Ravi S. Customised sport injury rehabilitation with yoga and physiotherapy for ACL-12 week rehabilitation progress of an injured young alpine skier. Br J Sports Med. 2016;50:e4. [Google Scholar]
- 11.Moonaz S, Nault D, Cramer H, Ward L. CLARIFY 2021:Explanation and elaboration of the Delphi-based guidelines for the reporting of yoga research. BMJ Open. 2021;11:e045812. doi: 10.1136/bmjopen-2020-045812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bedekar N, Prabhu A, Shyam A, Sancheti K, Sancheti P. Comparative study of conventional therapy and additional yogasanas for knee rehabilitation after total knee arthroplasty. Int J Yoga. 2012;5:118–22. doi: 10.4103/0973-6131.98226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ebnezar J, Bali MY, John R, Gupta O. Role of integrated approach of yoga therapy in a failed post-total knee replacement of bilateral knees. Int J Yoga. 2014;7:160–4. doi: 10.4103/0973-6131.133932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kolasinski SL, Garfinkel M, Tsai AG, Matz W, Dyke AV, Schumacher HR., Jr Iyengar yoga for treating symptoms of osteoarthritis of the knees:A pilot study. J Altern Complement Med. 2005;11:689–93. doi: 10.1089/acm.2005.11.689. [DOI] [PubMed] [Google Scholar]
- 15.Chang DG, Holt JA, Sklar M, Groessl EJ. Yoga as a treatment for chronic low back pain:A systematic review of the literature. J Orthop Rheumatol. 2016;3:1–8. [PMC free article] [PubMed] [Google Scholar]
- 16.Sadiri SN, Mohammed M, Naji FL, Chian CP, Sangelaji B. Yoga as a treatment for musculoskeletal discomforts:A hypothesis. Revista Pesquisa em Fisioterapia. 2016;6 doi:10.17267/2238-2704rpf.v6i3.984. [Google Scholar]
- 17.Garfinkel MS, Singhal A, Katz WA, Allan DA, Reshetar R, Schumacher HR., Jr Yoga-based intervention for carpal tunnel syndrome:A randomized trial. JAMA. 1998;280:1601–3. doi: 10.1001/jama.280.18.1601. [DOI] [PubMed] [Google Scholar]
- 18.Telles S, Sayal N, Nacht C, Chopra A, Patel K, Wnuk A, et al. Yoga:Can it be integrated with treatment of neuropathic pain? Ann Neurosci. 2019;26:82–91. doi: 10.5214/ans.0972.7531.260208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Vallath N. Perspectives on yoga inputs in the management of chronic pain. Indian J Palliat Care. 2010;16:1. doi: 10.4103/0973-1075.63127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bera TK, Gore MM, Oak JP. Recovery from stress in two different postures and in Shavasana—A yogic relaxation posture. Indian J Physiol Pharmacol. 1998;42:473–8. [PubMed] [Google Scholar]
- 21.Sharma G, Mahajan KK, Sharma L. Shavasana—relaxation technique to combat stress. J Bodyw Mov Ther. 2007;11:173–80. [Google Scholar]
- 22.Büssing A, Michalsen A, Khalsa SB, Telles S, Sherman KJ. Effects of yoga on mental and physical health:A short summary of reviews. Evid Based Complement Alternat Med. 2012;2012:165410. doi: 10.1155/2012/165410. doi:10.1155/2012/165410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Malathi A, Damodaran AS, Shah NI, Patil NE, Maratha SR. Effect of yogic practices on subjective well being. Indian J Physiol Pharmacol. 2000;44:202–6. [PubMed] [Google Scholar]
- 24.Hagins M, Selfe T, Innes K. Effectiveness of yoga for hypertension:Systematic review and meta-analysis. Evid Based Complement Alternative Med. 2013;2013 doi: 10.1155/2013/649836. doi:10.1155/2013/649836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Chaudhary AK, Bhatnagar HN, Bhatnagar LK, Chaudhary K. Comparative study of the effect of drugs and relaxation exercise (yoga shavasan) in hypertension. J Assoc Phys India. 1988;36:721–3. [PubMed] [Google Scholar]
- 26.Streeter CC, Jensen JE, Perlmutter RM, Cabral HJ, Tian H, Terhune DB, et al. Yoga Asana sessions increase brain GABA levels:A pilot study. J Altern Complement Med. 2007;13:419–26. doi: 10.1089/acm.2007.6338. [DOI] [PubMed] [Google Scholar]
- 27.Maughan RJ, Shirreffs SM. Muscle cramping during exercise:Causes, solutions, and questions remaining. Sports Med. 2019;49:115–24. doi: 10.1007/s40279-019-01162-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kisner C, Colby LA, Borstad J. Therapeutic exercise:foundations and techniques. Fa Davis. 2017 [Google Scholar]
- 29.Riley D. Hatha yoga and the treatment of illness. Altern Ther Health Med. 2004;10:20–5. [PubMed] [Google Scholar]
- 30.Long R. Bandha Yoga Publications LLC; 2009. The key poses of yoga. [Google Scholar]
- 31.Fishman L. Yoga in medicine. Alternative Medicine in Rehabilitation:A Guide for Practitioners. Wainappel SF. 2003:139–73. [Google Scholar]
- 32.Madhukar LS, Bhatnagar V, Nivrutti BA. A critical review study on importance of anatomical knowledge while practicing yoga asana. Indian J Ancient Med Yoga. 2018;5500:85. [Google Scholar]
- 33.Carlson CR, Collins FL, Jr, Nitz AJ, Sturgis ET, Rogers JL. Muscle stretching as an alternative relaxation training procedure. J Behav Ther Exp Psychiatry. 1990;21:29–38. doi: 10.1016/0005-7916(90)90046-n. [DOI] [PubMed] [Google Scholar]
- 34.Ebnezar J, Nagarathna R, Bali Y, Nagendra HR. Effect of an integrated approach of yoga therapy on quality of life in osteoarthritis of the knee joint:A randomized control study. Int J Yoga. 2011;4:55–63. doi: 10.4103/0973-6131.85486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Villacres MD, Jagannathan A, Nagarathna R, Ramakrsihna J. Decoding the integrated approach to yoga therapy:Qualitative evidence based conceptual framework. Int J Yoga. 2014;7:22–31. doi: 10.4103/0973-6131.123475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Nagendra HR. Integrated yoga therapy for mental Illness. Indian J Psychiatry. 2013;55((Suppl 3)):S337–9. [PMC free article] [PubMed] [Google Scholar]
- 37.Dumbala S, Bhargav H, Satyanarayana V, Arasappa R, Varambally S, Desai G, et al. Effect of yoga on psychological distress among women receiving treatment for infertility. Int J Yoga. 2020;13:115–9. doi: 10.4103/ijoy.IJOY_34_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Harvey R, Andriopoulou P, Grogan S. Perceived mechanisms of change in therapeutic yoga targeting psychological distress. J Bodywork Mov Ther. 2020;24:274–80. doi: 10.1016/j.jbmt.2019.06.014. [DOI] [PubMed] [Google Scholar]
- 39.Rouhi S, Etemadi S, Pooraghajan M. Laughter in combination with yoga exercises:Changes in psychological distress and quality of life in patients with coronary heart disease (CHD) Open Psychol J. 2020;13 doi:10.2174/1874350102013010144. [Google Scholar]
- 40.Forfylow AL. Integrating yoga with psychotherapy:A complementary treatment for anxiety and depression. Can J Couns Psychother. 2011;45:132–50. [Google Scholar]
- 41.Suri M, Sharma R, Saini N. Neuro-physiological correlation between yoga, pain and endorphins. Int J Adapt Phys Educ Yoga. 2017 [Google Scholar]
- 42.Asvadi NH, Morgan M, Hewavitharana AK, Shaw PN, Cabot PJ. Biotransformation of beta-endorphin and possible therapeutic implications. Front Pharmacol. 2014;5:18. doi: 10.3389/fphar.2014.00018. doi:10.3389/fphar. 2014.00018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Shrihari TG. Beta Endorphins–Novel Holistic Palliative Approach in Management of Cancer Pain. J Preview. 2019:9. [Google Scholar]
- 44.Mahajan A. Role of yoga in hormonal homeostasis. Int J Clin Exp Physiol. 2014;1:173. [Google Scholar]
- 45.Walton KG, Pugh ND, Gelderloos P, Macrae P. Stress reduction and preventing hypertension:Preliminary support for a psychoneuroendocrine mechanism. J Altern Complement Med. 1995;1:263–83. doi: 10.1089/acm.1995.1.263. [DOI] [PubMed] [Google Scholar]
- 46.Jevning R, Wilson AF, Davidson JM. Adrenocortical activity during meditation. Hormones Behav. 1978;10:54–60. doi: 10.1016/0018-506x(78)90024-7. [DOI] [PubMed] [Google Scholar]
- 47.Arora S, Bhattacharjee J. Modulation of immune responses in stress by Yoga. Int J Yoga. 2008;1:45–55. doi: 10.4103/0973-6131.43541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Bevan AJ. Endocrine changes in relaxation procedures (Doctoral dissertation). 1980 [Google Scholar]
- 49.Vandana B, Vaidyanathan K, Saraswathy LA, Sundaram KR, Kumar H. Impact of integrated amrita meditation technique on adrenaline and cortisol levels in healthy volunteers. Evid Based Complement Altern Med. 2011;2011 doi: 10.1155/2011/379645. doi:10.1155/2011/379645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Vera FM, Manzaneque JM, Maldonado EF, Carranque GA, Rodriguez FM, Blanca MJ, et al. Subjective sleep quality and hormonal modulation in long-term yoga practitioners. Biol Psychol. 2009;81:164–8. doi: 10.1016/j.biopsycho.2009.03.008. [DOI] [PubMed] [Google Scholar]
- 51.Yoshihara K, Hiramoto T, Sudo N, Kubo C. Profile of mood states and stress-related biochemical indices in long-term yoga practitioners. Biopsychosoc Med. 2011;5:1–8. doi: 10.1186/1751-0759-5-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Newberg AB, Iversen J. The neural basis of the complex mental task of meditation:Neurotransmitter and neurochemical considerations. Med Hypotheses. 2003;61:282–91. doi: 10.1016/s0306-9877(03)00175-0. [DOI] [PubMed] [Google Scholar]
- 53.Chatterjee S, Mondal S. Effect of combined yoga programme on blood levels of thyroid hormones:A quasi-experimental study [Google Scholar]
- 54.Chatterjee S, Mondal S. Effect of regular yogic training on growth hormone and dehydroepiandrosterone sulfate as an endocrine marker of aging. Evid Based Complement Altern Med. 2014;2014 doi: 10.1155/2014/240581. doi:10.1155/2014/240581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Udupa KN, Singh RH, Settiwar RM. Physiological and biochemical studies on the effect of yogic and certain other exercises. Indian J Med Res. 1975;63:620–4. [PubMed] [Google Scholar]
- 56.Streeter CC, Whitfield TH, Owen L, Rein T, Karri SK, Yakhkind A, et al. Effects of yoga versus walking on mood, anxiety, and brain GABA levels:A randomized controlled MRS study. J Altern Complement Med. 2010;16:1145–52. doi: 10.1089/acm.2010.0007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Shetty KT, Subbakrishna DK, Meti BL, Raju TR. Therapeutic efficacy of Sudarshan Kriya Yoga (SKK) in dysthymic disorder. Nimhans J. 1998. pp. 21–8. Available from: https://www.yoga-als-therapie.de/assets/Studien/Downloads/Janakiramaiah-1998-nimhans-j.pdf .
- 58.Jevning R, Wilson AF, VanderLaan EF. Plasma prolactin and growth hormone during meditation. Psychosom Med. 1978;40:329–33. doi: 10.1097/00006842-197806000-00005. [DOI] [PubMed] [Google Scholar]
- 59.Williams KA, Petronis J, Smith D, Goodrich D, Wu J, Ravi N, et al. Effect of Iyengar yoga therapy for chronic low back pain. Pain. 2005;115:107–17. doi: 10.1016/j.pain.2005.02.016. [DOI] [PubMed] [Google Scholar]
- 60.Sharma N, John PJ, Meghwal N, Owen A, Mishra V. Effect of yoga therapy on patients with chronic musculoskeletal pain:A prospective randomized wait list-controlled trial. Clin Med. 2019;19:87. [Google Scholar]