

ABSTRACT
Introduction:
Safe motherhood ensures safe pregnancy and childbirth. One of the noteworthy causes of maternal morbidity and mortality is the complications arising from prolonged or obstructed labour. World Health Organization recommends the use of partograph to significantly reduce the maternal mortality crisis. This study aimed to evaluate the effectiveness of a novel partograph in terms of maternal and perinatal outcomes along with its utility.
Materials and Methods:
A total of 400 intranatal women were selected in a non-randomized control trial to evaluate the effectiveness of novel partograph on selected maternal and perinatal outcomes. Subjects in experimental group (n=200) received care with newly developed partograph whereas subjects in control group (n=200) received standard care. Effectiveness was determined at a significance level of α ≤ 0.05. Utility of the novel partograph was determined as perceived by nurses.
Results:
There was significant reduction in the duration of the 1st and 2nd stage of labour (P=0.023 and 0.006 respectively) and number of vaginal examinations performed during labour (P=0.017) among mothers in the experimental group. Significant improvement in the Apgar score (P=0.005) was also observed among the infants of mothers in experimental group. Novel partograph was considered as of having extreme utility by 71% nurses.
Conclusion:
Study concluded that subjects monitored by the partograph experienced improved maternal and perinatal outcomes. It was found to be having extreme utility.
Keywords: India, labor, maternal outcome, partograph, perinatal outcome
Introduction
The government has tried to provide shelter to the safe motherhood by launching various beneficial schemes which, resultantly brought down the maternal mortality rate of 254 per 1 lakh in 2004–2006 to 103 in 2019.[1] For safeguarding motherhood, we have to take stern measures to achieve the 2030 target of sustainable development goals. There is a need to eliminate the preventable causes of maternal mortality as 94% of all maternal deaths is borne by the low- and middle-income countries and India is one of the top contributors of maternal deaths.[2,3,4] Around 25% maternal deaths in India are related to neglected obstructed labor and its complications.[5,6,7]
A simple labor tool called as partograph or “labor curve” can help in detecting labor which is progressing abnormally and timely intervention regarding augmentation of labor, operative delivery or transfer to higher facility can be provided to the mothers.[8,9] It also reduces chances of repeated caesarean sections and still births.[10]
A plethora of studies reveal that abundant investment and over four decades of training has not resulted in effective implementation and correct practice of partograph. Our labor tools which are used to facilitate effective labor monitoring have still not attained their potential.[11,12,13]
Sanghvi et al.[14] mentioned that there is inconsistent use of partograph and in various settings, it is completed retrospectively for recordkeeping purpose. Almost 95 papers were included in a realistic review which concluded that lack of “enabling environment” and being a complex intervention were the reasons for failure of partograph.[15]
Though health professionals provide a global support to this indispensable tool but still its use is low in the developing countries and it has not been able to reach its full potential in giving improved clinical outcomes which in turn has defeated its sole purpose of invention.[12,16,17] This very factor has resulted in certain variations of this tool.[12]
Report from the Cochrane review and other data from the low resource settings display the infrequent and diminished use of existing partograph as the users find it challenging to use.[18,19] Previous studies mainly focused on the importance as well as the low utilization of the existing labor tools. The aim of the current study is to not only determine the effectiveness of the novel partograph devised by the researcher for the low-risk laboring mothers, but also to assess its utility.
Materials and Methods
Study design and setting
Nonequivalent control group posttest only design was used to determine the effectiveness of the novel partograph. The study was conducted in two major hospitals of Punjab, India, from 2019 to 2021.
Survey to assess the utility of the tool was conducted in the civil hospitals, community health centers and primary health centers of Mohali and Patiala districts of Punjab.
Study participants and sampling
The nurses working in the labor room of selected hospitals, who volunteered to collect data were provided training and user manual [Table 1] regarding the administration of novel partograph. Purposive sampling was used to select the intranatal mothers from two main hospitals of Mohali and Patiala districts of Punjab, India. The required sample size for each group was 196, based on the conventional standard method with desired alpha (a) of 0.05 and beta (b) = 0.2. Considering the equal ratio in each group (200 in experimental and 200 in control group), final sample size was estimated to be 400. The developed partographs along with the maternal and perinatal outcome sheets were provided to the nurses (data collectors). In the control group, intranatal mothers received the routine care and the outcome variables were evaluated by the nurses.
Table 1.
User manual for the nurses (data collectors)
| Heading | Interpretation |
|---|---|
| Alert etd | Delivery is expected to take place by this time. Considering the normal rate of cervical dilatation to be 1 cm/hour, number of hours are added in the determined cervical dilatation to get expected time of delivery. |
| Action etd | After adding 4 hours to ALERT EDD, we can get ACTION ETD where we need to be vigilant & take action. |
| The progress of labour | Cervical dilatation Station of head Uterine contractions (write frequency in 10 minutes, to be charted every half an hourly) |
| The fetal condition | Fetal heart rate (√ mark in column showing appropriate range) Liquor (write symbol mentioned in the graph) |
| The Maternal condition | Pulse (to use. as symbol to mark pulse every half an hourly) Blood pressure (to use as a symbol. Upper arrow for systolic and lower arrow for diastolic measurement) Temperature (as per the frequency mentioned) Drugs, IV fuids |
| Delivery notes | maternal and newborn outcome of delivery as mentioned in the graph |
ETD- Estimated Time of Delivery
Inclusion criteria were intranatal women in active phase of labor, singleton pregnancy, gestational age of at least 37 weeks and vertex presentation. Exclusion criteria were breech presentation, medical disorders in pregnancy, height less than 145 cm, cervical dilatation of more than 7 cm and elective caesarean section.
Hospitals of Mohali and Patiala districts of Punjab, India were conveniently selected as experimental and control settings, respectively. Both the study settings were found to be similar in terms of selected characteristics such as; both were district hospitals with the obstetric nurses and doctors (in case of emergency) caring for the intranatal mothers and having antepartum, labor room as well as postpartum rooms with rooming in. These hospitals cater both low- and high-risk women. Further, homogeneity was evaluated by comparing the labor outcomes of 50 subjects taken from each hospital.
For evaluating utility, 52 labor room nurses were selected from nine health centers of Mohali and Patiala districts of Punjab.
Data collection tools and techniques
A valid and reliable partograph was developed by researcher using methodological approach [Figure 1]. Data collection instruments included the newly developed partograph, maternal and perinatal outcome sheet along with utility assessment tool.
Figure 1.

Novel partograph
An extensive theoretical and empirical literature review along with multiple focus group discussions with the obstetric nurses and educators were conducted to prepare a preliminary draft of partograph which was further sent for peer review. The prepared draft was validated by 13 experts of obstetric and pediatric speciality from nursing and medical field. Common consensus was established after three rounds with 0.97 as the CVI-total of final round. In addition, dependability and equivalency of the developed partograph was calculated having kappa values of 0.73 and 0.71, respectively.
Maternal and perinatal outcome sheet consisted of subjects’ obstetric profile. Maternal outcome includes the mode of delivery, duration of labor, number of vaginal examinations, augmentation of labor, maternal morbidity, and mortality. Perinatal outcomes included the Apgar score at 1 and 5 minutes, perinatal morbidity, and mortality. Content validity index of maternal and perinatal outcome sheet was calculated and found to be 0.92. Equivalency of the maternal and perinatal outcome sheet was determined and was found to be reliable.
The valid (CVI-i = 0.94) and reliable (internal consistency = 0.89 and stability = 0.99) ‘utility assessment tool’ was developed. It was semantic differential scale having 17 items. Nurses filled this tool after conducting deliveries with the help of novel partograph.
Statistical analysis
Statistical package for social sciences (IBM SPSS. Ver. 22) was used. Effectiveness of intervention was evaluated by comparing the changes in the outcome variables of postintervention assessment in both experimental and control group by using t-test. Comparison of categorical variables was done with Chi-square test. A P value < 0.05 was taken as statistically significant.
Results
Participants’ characteristics
A total of 400 intranatal mothers (participants) were included in the study (200 in experimental and 200 in control group). The mean ages (in years) of the intranatal mothers were 25.62 ± 3.30 in experimental group and 26.05 ± 3.91 in control group (P = 0.23). Mean gestational age (in weeks) was 38.58 ± 0.82 in experimental group and 38.51 ± 0.85 in control group (P = 0.42). In experimental group, 92 mothers were primipara and 108 mothers were multipara (P = 0.92). In control group, 93 mothers were primipara and 107 mothers were multipara (P = 0.42). Both the groups were not having any significant difference in terms of age, gestational age, parity, and booking status.
Mode of delivery
Mode of delivery comprised normal vaginal delivery, instrumental delivery, and LSCS. The Chi-square value shows no significant difference in the mode of delivery among experimental and control group (P = 0.45) as shown in [Table 2].
Table 2.
Comparison of intranatal mothers as per their mode of delivery and augmentation of labor
| Mode of delivery | Experimental group | Comparison group | P | ||
|---|---|---|---|---|---|
|
|
|
||||
| n=200 | % | n=200 | % | ||
| NVD | 179 | 89.5 | 177 | 88.5 | |
| Instrumental | 13 | 6.5 | 10 | 0.5 | 0.45† |
| LSCS | 08 | 04 | 13 | 6.5 | 0.57† |
| Augmentation of labor | |||||
| No | 157 | 78.5 | 152 | 76 | |
| ARM | 08 | 04 | 05 | 2.5 | |
| Oxytocin | 18 | 09 | 19 | 9.5 | |
| Both | 15 | 8.5 | 24 | 12 | |
NVD, normal vaginal delivery; LSCS, lower segment caesarean section; ARM, artificial rupture of membranes. †Non significant by Chi-square-test
Labor augmentation
The method of augmentation of labor used in experimental and control groups were artificial rupture of membranes, oxytocin, and both medical as well as surgical methods of induction of labor. Chi-square value did not reveal any significant difference in both the groups as depicted in [Table 2].
Duration of labor
The mothers in experimental group experienced significant reduction in the duration of 1st stage of labor in active phase (in hours.) as compared to mothers in control group (P = 0.023). Five mothers in experimental group and eight mothers in control group went for emergency LSCS in 1st stage of labor; hence, were excluded from mean calculation. Significant reduction was also observed in the duration of second stage of labor (P = 0.006). Out of 195 women of experimental group in first stage of labor, three mothers went for LSCS in 2nd stage and out of 192 mothers in control group, six mothers went for emergency LSCS; hence labor duration of those mothers was excluded from mean calculation [Table 3].
Table 3.
Comparison of duration of 1st and 2nd stage of labor among experimental and control group
| Experimental group | Control group | P | |
|---|---|---|---|
| Duration of 1st stage of labor in active stage (in hours) Duration of second stage of labor (in min.) |
(n=195) Mean±SD 5.12±1.26 (n=192) 30.81±12.85 |
(n=192) Mean±SD 5.43±1.05 (n=186) 36.03±14.79 |
0.023* 0.006* |
SD, standard deviation, *Significant by t-test
Frequency of per-vaginal examination
Considering the per-vaginal examinations, there was significant difference in the number of times examination was performed in the experimental and control group (P = 0.017). Mothers in the experimental group were examined less frequently as compared to control group [Table 4].
Table 4.
Comparison of frequency of per-vaginal examination in experimental and control group
| Number of vaginal examination | Experimental group | Comparison group | P | ||
|---|---|---|---|---|---|
|
|
|
||||
| n=200 | % | n=200 | % | ||
| 2 | 125 | 62.5 | 95 | 47.5 | |
| 3 | 52 | 26.0 | 67 | 33.5 | 0.017** |
| ≥4 | 23 | 11.5 | 38 | 19 | |
**Significant by Chi-square- test
Apgar score
Significant difference was found in Apgar score at 5 minutes in experimental and control group, respectively (P = 0.005). Neonates in the experimental group had improved Apgar score at 5 minutes [Table 5].
Table 5.
Comparison of Apgar score at 5 minutes in experimental and control group
| Experimental group | Comparison group | P | |
|---|---|---|---|
| Apgar score at 5 minutes | Mean±SD | Mean±SD | 0.005* |
| 9.44±0.89 | 9.18±0.97 |
*Significant by t-test
Maternal and neonatal morbidities
Maternal morbidity was experienced by four mothers in experimental group and by seven mothers in control group. The main conditions experienced by mothers were postpartum hemorrhage and perineal tears. Neonatal morbidities such as meconium aspiration and respiratory distress affected four neonates in experimental group and seven in control group. No significant difference was observed by Chi-square values (P = 0.359 and 0.35).
Utility of the novel partograph
The developed partograph was perceived to be of extreme utility by 73.1% of labour room nurses.
The overall observed mean ± SD and mean percentage was 93.15 ± 10.78 and 78.27%, respectively. The mean score of various dimensions of utility are described in the Figure 2. Out of all the items, “easy to interpret the findings,” obtained the maximum mean; followed by “clear instructions.” Minimum mean is obtained by the item “time saving” [Figure 2].
Figure 2.
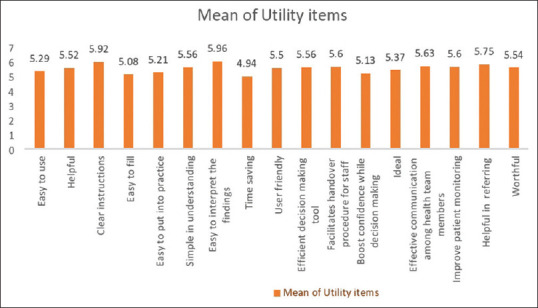
Mean of utility items
Discussion
The present study mentions about the effectiveness and utility of the partograph. The t-test showed the significant difference in the duration of first stage of labor, second stage of labor and Apgar score at 5 minutes in experimental and control group. Chi-square test also depicted that after monitoring of mothers in experimental group with the partograph, there was significant difference in the number of per vaginal examinations performed among the experimental and control groups. The nurses perceived the developed partograph as of possessing extreme utility.
Mode of delivery
A quasi-experimental study performed by Magnus[20] mentioned the effect of modified partograph on the outcomes of 544 women in labor in Zaria. Decrease was observed in LSCS deliveries from 16.2% to 10.3% and operative deliveries (P = 0.019). In this regard, a retrospective observational study was also done by Sanya et al.[21] to see the role of partograph on outcome of labor in 500 women having singleton pregnancy with vertex presentation. Maximum number of women, that is, 79.2% delivered vaginally and 5.2% required instrumental delivery. Most common cause of LSCS was abnormal labor pattern.
In the present study, majority of women (89.5%) in the experimental group delivered vaginally and 6.5% had instrumental delivery. Difference was observed in LSCS deliveries as 13% in control group and 8% in experimental group, but it was not statistically significant which may be due to the fact that both the settings are government district hospitals with trained staff. Nonprogress of labor was the most common indication for LSCS.
Labor augmentation
In almost alike study, Valvekar[22] compared the outcomes of labor with and without the use of partograph among 300 women with 37–42 weeks of period of gestation. Among primipara and multipara, there was no significant difference in requirement of augmentation. In the present study also, no significant difference has been observed in both the groups.
Duration of labor
A similar study was conducted by Tayade[23] on 100 cases with uncomplicated full-term pregnancies and 100 historical matched controls to find the effectiveness of partograph. It was revealed that after using partograph there was no case of prolonged labor. Comparison with the matched controls clarified that cases had reduced duration of labor (P < 0.01). Similar findings regarding labor duration were observed in another study conducted by Shereen and Shoib[24] (P < 0.001). The results of the study done by Sanya et al.[21] also saw decreasing trends in the labor duration with the use of partogram. As the partograph provided timely intervention, it minimized the incidence of prolonged labor. In line to the findings of the present study, Ahmed et al.[25] performed a randomized comparative study in a hospital of Chattisgarh, India where women were divided in two groups and their labor durations were monitored. Labor duration of the women being monitored by partograph was significantly reduced during active phase (P < 0.001), second stage (P < 0.0001) and there was the reduction of overall duration of labor (P < 0.001).
Similar trend was observed in the present study also in terms of duration of labor. The study demonstrates that with partogram, total duration of labor is shortened and timely effective intervention is decided, resulting in precise actions.
Frequency of per vaginal examination
A perspective interventional case control study conducted by Shereen and Shoib[24] on 1000 laboring women saw improvement in outcomes such as significant impact on reduction in vaginal examination (P < 0.001). Results of the present study also declares about less frequency of vaginal examinations performed in experimental group. This can be due to the availability of a user-friendly labor tool which acts as an important medium of communication between health care team.
Apgar score
Magnus[20] in his study mentioned the improvement in Apgar score at 1 and 5 minutes (P = 0.003 and 0.001). Better neonatal outcome was also seen with few newborns having Apgar score <7 (P < 0.05) in a study done by Ahmed et al.[25] Likewise, significant improvement in the Apgar score at 5 minutes was observed in the present study as the partograph is an important decision making tool which not only helps avoiding unnecessary augmentation, but also suggests timely interventions.
Maternal and neonatal morbidities
A retrospective study done by Anokye et al.[26] Ghana, reveals that use of partograph was associated with birth outcomes with less nonasphyxiated infants (AOR [95% CI] 4.29 [1.35–14.81]). Use of partograph was related to 5.3 times less chances of asphyxiated births. Reduction was also observed in maternal morbidities such as perineal lacerations (P = 0.0001) and post partum hemorrhage (PPH) (P = 0.047) in a study done by Magnus.[20]
The main conditions experienced by mothers in the current study were vaginal tears and postpartum hemorrhage. There was no significant difference in maternal and neonatal morbidity status. This can be attributed to the experienced health care staff and tertiary level of facilities in both the settings.
Utility of partograph
Peter et al.[27] did study on 150 nurses to find the utilization of partograph in Tanzania hospital. Low utilization was observed in 61.3% of the nurses whereas 38.7% had high utilization. Similar findings were reported by Ayenew and Zewudu[28] in their systematic review of 15 studies, where the utilization of the graph was mentioned to be 57.1%. In the present study, nurses perceived the novel partograph to be having extreme utility as it is more user friendly.
The results of the present study highlighted that novel partograph improved various aspects of maternal and perinatal outcomes and is found of having extreme utility.
Limitations and strength
There were certain limitations to this study. First, the study lacks randomization which may affect the internal validity even though equivalence was ensured between subjects in experimental and control group, thus this might limit the generalizability. The present approach was found feasible in collecting data from two different settings. Second, the effectiveness of partograph was assessed only in tertiary hospitals. Hence, the results need to be validated at peripheral centers.
Homogeneity of the hospitals was assessed in advance and both the settings were found to be well matched in terms of labor outcomes. To the best of our knowledge, this is the first study to assess the utility of the developed partograph in terms of perception of nurses, who have to actually implemented it.
Conclusion
Recent findings suggest that the partograph has been relatively successful in improving maternal and perinatal outcomes. Therefore, it is recommended that the developed partograph may be used by more labor room nurses of various health facilities to further generalize its effectiveness. Randomized controlled trial may be done to better understand the effectiveness of the developed partograph.
Ethical approval
Ethical approval had been obtained from the Institutional ethics and review committee (SOCON/9954/B) and District Health Officer (Memo No. MCH/Pb/19/493) Punjab, India. Written informed consent was obtained from the nurses who volunteered to collect the data and the intranatal mothers whose information was obtained.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The researchers experience deep gratitude to the data collectors and the subjects for their invaluable contribution.
References
- 1.Manglik PG. Safe motherhood day:Challenges in fostering safe motherhood in India and way forward:Times of India. [Last accessed on 2022 May 25];2022 April; Available from:https://timesofindia.indiatimes.com/blogs/voices/safe-motherhood-day-challenges-in-fostering-safe-motherhood-in-india-and-way-forward/ [Google Scholar]
- 2.World Health Organization. [Last accessed on 2021 May 19];Maternal mortality. 2019 Available from:https://www.who.int/news-room/fact-sheets/detail/maternal-mortality . [Google Scholar]
- 3. [Last accessed on 2020 Jan 20];NHM. Guidelines of maternal death and surveillance and response. 2017 Available from:https://nhm.gov.in/images/pdf/programmes/maternal-health/guidelines/Guideline_for_MDSR.pdf . [Google Scholar]
- 4.Alkema L, Chou D, Hogan D, Zhang S, Moller AB, Gemmill A, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030:A systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet. 2016;387:462–74. doi: 10.1016/S0140-6736(15)00838-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Harrison SH, Mabeya H, Godenberg RL, McClure EM. Urogenital fistula reviewed:A marker of severe maternal morbidity and an indicator of the quality of maternal healthcare delivery. Matern Health Neonatol Perinatol. 2015;1:20. doi: 10.1186/s40748-015-0020-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ayenew AA. Incidence, causes, and maternofetal outcomes of obstructed labor in Ethiopia:Systematic review and meta-analysis. Reprod Health. 2021;18:61. doi: 10.1186/s12978-021-01103-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.World Health Organization. The World Health Report 2005:Make every Mother and Child Count. Geneva: World Health Organization; 2008. [Google Scholar]
- 8.Allauddin M, Bal R, De A, Mandal P, Chakraborty M. Monitoring labour with WHO modified partograph- A study report. Nepal J Obstet Gynaecol. 2008;3:8–11. [Google Scholar]
- 9.Haile Y, Tafese F, Weldemarium TD, Rad MH. Partograph utilization and associated factors among obstetric care providers at public health facilities in Hadiya Zone, Southern Ethiopia. J Pregnancy. 2020:3943498. doi: 10.1155/2020/3943498. doi:10.1155/2020/3943498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rajole KM, Agrawal V. Evaluation of role of partograph in the management of labour in previous caesarean section cases at tertiary care centre. MedPulse Int J Gynaecol. 2020;13:48–52. [Google Scholar]
- 11.Dalal AR, Purandare AC. 'The partograph in childbirth:An absolute essentiality or a mere exercise? J Obstet Gnaecol India. 2018;68:3–14. doi: 10.1007/s13224-017-1051-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lavender T, Bernitz S. Use of the partograph-Current thinking. Best Pract Res Clin Obstet Gynaecol. 2020;67:33–43. doi: 10.1016/j.bpobgyn.2020.03.010. [DOI] [PubMed] [Google Scholar]
- 13.Laisser R, Danna VA, Bonet M, Oladopo OT, Lavender T. An exploration of midwives'views of the new World Health Organization labour care guide. Afr J Midwifery Womens Health. 2021;15:1. [Google Scholar]
- 14.Sanghvi H, Mohan D, Litwin L, Bazant E, Gomez P, MacDowell T, et al. Effectiveness of an electronic partogram:A mixed-method quasi experimental study among skilled birth attendants in Kenya. Glob Health Sci Pract. 2019;7:521–39. doi: 10.9745/GHSP-D-19-00195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bedwell C, Levin K, Pett C, Lavender DT. A realist review of the partograph:When and how does it work for labour monitoring? BMC Pregnancy Childbirth. 2017;17:31. doi: 10.1186/s12884-016-1213-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lavender T, Cuthbert A, Smyth RM. Effect of partograph use on outcomes for women in spontaneous labour at term and their babies. Cochrane Database Syst Rev. 2018;8:CD005461. doi: 10.1002/14651858.CD005461.pub5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kushwah B, Singh AP, Singh S. The partograph:An essential yet underutilized tool. J Evol Med Dent Sci. 2013;24:4373–9. [Google Scholar]
- 18.Mathai M. The partograph for the prevention of obstructed labor. Clin Obstet Gynecol. 2009;52:256–69. doi: 10.1097/GRF.0b013e3181a4f163. [DOI] [PubMed] [Google Scholar]
- 19.Lavender T, Hart A, Smyth RM. Effect of partogram use on outcomes for women in spontaneous labour at term. Cochrane Database Syst Rev. 2013;10:CD005461. doi: 10.1002/14651858.CD005461.pub4. [DOI] [PubMed] [Google Scholar]
- 20.Magnus OO. The effects of modified WHO partograph on maternal and perinatal outcomes of labour in Gambo Sawaba hospital, Zaria. [dissertation] Ahmadu Bello University Zaria. 2016 [Google Scholar]
- 21.Sanyal U, Goswami S, Mukhopadhyay P. The role of partograph in the outcome of spontaneous labour. Nepal J Obstet Gynaecol. 2014;9:52–7. [Google Scholar]
- 22.Valvekar UR. Labour and its outcome compared with and without partogram use in primiparous and multiparous women. MedPulse Int J Gynaecol. 2021;17:52–7. [Google Scholar]
- 23.Tayade S. The impact of use of modified WHO partograph on maternal and perinatal outcome. Res Gate. 2012;3:257–60. [Google Scholar]
- 24.Shereen JI, Shoib T. Role of partograph in preventing augmented labour. J Pak med Assoc. 2001;18:11–5. [Google Scholar]
- 25.Ahmed B, Jain M, Bharwani H. Partograph versus no partograph:Effect on labour progress and delivery outcome:A comparative study. Int J Reprod Contracept Obstet Gynecol. 2017;6:4928–34. [Google Scholar]
- 26.Anokye R, Acheampong E, Anokye J, Ainooson AB, Amekudzie E, Owusu I, et al. Use and completion of partograph during labour is associated with a reduced incidence of birth asphyxia:A retrospective study at per-urban setting in Ghana. J Health Popul Nutr. 2019;38:12. doi: 10.1186/s41043-019-0171-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Peter DE, Millanzi WC, Joho AA. Practice and factors influencing partograph utilization on the delivery of nursing care:An analytical Cross –Sectional Study among nurses in Singida, Tanzania. Res Sq. 2020 doi:10.21203/rs.3.rs-70920/v1. [Google Scholar]
- 28.Ayenew AA, Zewdu BF. Partograph utilization as a decision-making tool and associated factors among obstetric care providers in Ethiopia:A systematic review and meta-analysis. Syst Rev. 2020;9:251. doi: 10.1186/s13643-020-01505-4. [DOI] [PMC free article] [PubMed] [Google Scholar]