

Abstract
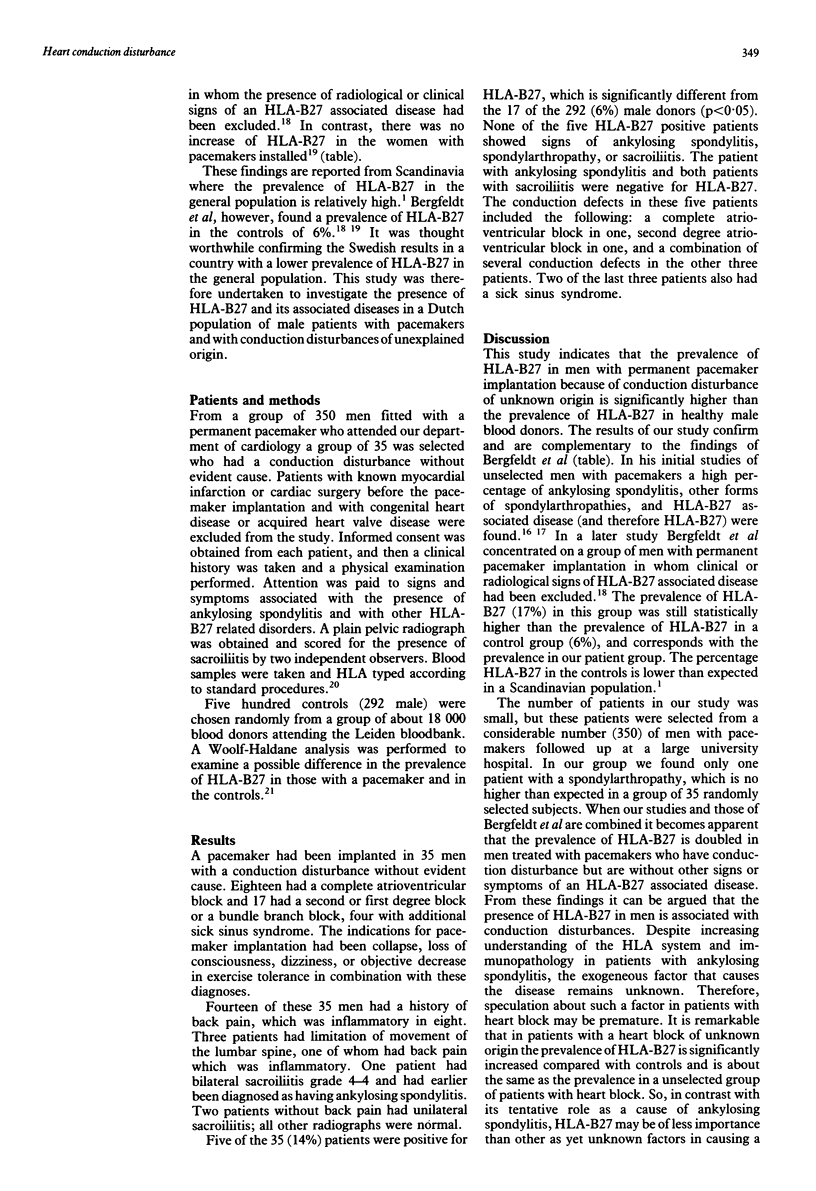
In recent studies from Sweden an increased prevalence of HLA-B27 associated diseases and of HLA-B27 was found in an unselected group of men with permanently implanted pacemakers and with a heart block. Furthermore, a significantly increased prevalence of HLA-B27 was found in men with a pacemaker who had no clinical or radiological signs of HLA-B27 associated disease. To obtain more insight into the association between HLA-B27 and heart block, and the possible role of HLA-B27 in causing this block, a study was made of 35 patients with a pacemaker and heart block of unknown cause, selected from a total group of 350 men with pacemakers who were still alive at the time of the study. One of these 35 men had ankylosing spondylitis and two patients had an asymptomatic sacroiliitis, but all three were HLA-B27 negative. HLA-B27 was present in five (14%) patients, which is a significantly higher prevalence than in healthy controls (17/292, 6%). This percentage is equal to the percentage of HLA-B27 positivity found in the Swedish study on unselected men with an implanted pacemaker, in whom the presence of an HLA-B27 associated disease had been excluded. It suggests that factors other than HLA-B27 are important in the pathogenesis of heart block in most patients.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bergfeldt L., Edhag O., Vallin H. Cardiac conduction disturbances, an underestimated manifestation in ankylosing spondylitis. A 25-year follow-up study of 68 patients. Acta Med Scand. 1982;212(4):217–223. doi: 10.1111/j.0954-6820.1982.tb03203.x. [DOI] [PubMed] [Google Scholar]
- Bergfeldt L., Edhag O., Vedin L., Vallin H. Ankylosing spondylitis: an important cause of severe disturbances of the cardiac conduction system. Prevalence among 223 pacemaker-treated men. Am J Med. 1982 Aug;73(2):187–191. doi: 10.1016/0002-9343(82)90177-2. [DOI] [PubMed] [Google Scholar]
- Bergfeldt L. HLA B27-associated rheumatic diseases with severe cardiac bradyarrhythmias. Clinical features and prevalence in 223 men with permanent pacemakers. Am J Med. 1983 Aug;75(2):210–215. doi: 10.1016/0002-9343(83)91193-2. [DOI] [PubMed] [Google Scholar]
- Bergfeldt L., Möller E. Complete heart block--another HLA B27 associated disease manifestation. Tissue Antigens. 1983 May;21(5):385–390. doi: 10.1111/j.1399-0039.1983.tb00188.x. [DOI] [PubMed] [Google Scholar]
- Bergfeldt L., Möller E. Pacemaker treated women with heart block have no increase in the frequency of HLA-B27 and associated rheumatic disorders in contrast to men--a sex linked difference in disease susceptibility. J Rheumatol. 1986 Oct;13(5):941–943. [PubMed] [Google Scholar]
- Brewerton D. A., Gibson D. G., Goddard D. H., Jones T. J., Moore R. B., Pease C. T., Revell P. A., Shapiro L. M., Swettenham K. V. The myocardium in ankylosing spondylitis. A clinical, echocardiographic, and histopathological study. Lancet. 1987 May 2;1(8540):995–998. doi: 10.1016/s0140-6736(87)92268-9. [DOI] [PubMed] [Google Scholar]
- Bulkley B. H., Roberts W. C. Ankylosing spondylitis and aortic regurgitation. Description of the characteristic cardiovascular lesion from study of eight necropsy patients. Circulation. 1973 Nov;48(5):1014–1027. doi: 10.1161/01.cir.48.5.1014. [DOI] [PubMed] [Google Scholar]
- Calin A., Fries J. F., Stinson E. B., Payne R. Letter: Normal frequency of HL-A B27 in aortic insufficiency. N Engl J Med. 1976 Feb 12;294(7):397–397. [PubMed] [Google Scholar]
- Feltkamp T. E. New views on B27 associated diseases. Neth J Med. 1989 Oct;35(3-4):119–122. [PubMed] [Google Scholar]
- GRAHAM D. C., SMYTHE H. A. The carditis and aortitis of ankylosing spondylitis. Bull Rheum Dis. 1958 Nov;9(3):171–174. [PubMed] [Google Scholar]
- Hollingworth P., Hall P. J., Knight S. C., Newman R. Lone aortic regurgitation, sacroiliitis, and HLA B27. Case history and frequency of association. Br Heart J. 1979 Aug;42(2):229–230. doi: 10.1136/hrt.42.2.229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kinsella T. D., Johnson L. G., Ian R. Cardiovascular manifestations of ankylosing spondylitis. Can Med Assoc J. 1974 Dec 21;111(12):1309–1311. [PMC free article] [PubMed] [Google Scholar]
- Qaiyumi S., Hassan Z. U., Toone E. Seronegative spondyloarthropathies in lone aortic insufficiency. Arch Intern Med. 1985 May;145(5):822–824. [PubMed] [Google Scholar]
- Sukenik S., Pras A., Buskila D., Katz A., Snir Y., Horowitz J. Cardiovascular manifestations of ankylosing spondylitis. Clin Rheumatol. 1987 Dec;6(4):588–592. doi: 10.1007/BF02330598. [DOI] [PubMed] [Google Scholar]
- Svejgaard A., Jersild C., Nielsen L. S., Bodmer W. F. HL-A antigens and disease. Statistical and genetical considerations. Tissue Antigens. 1974;4(2):95–105. doi: 10.1111/j.1399-0039.1974.tb00230.x. [DOI] [PubMed] [Google Scholar]
- Tan P. L., Butler M. J., Woodfield D. G., Jacobson C., Grigor R. R., Caughey D. E. HLA antigens in isolated aortic incompetence. J Rheumatol. 1980 Sep-Oct;7(5):757–758. [PubMed] [Google Scholar]
- Thomsen N. H., Hørslev-Petersen K., Beyer J. M. Ambulatory 24-hour continuous electrocardiographic monitoring in 54 patients with ankylosing spondylitis. Eur Heart J. 1986 Mar;7(3):240–246. doi: 10.1093/oxfordjournals.eurheartj.a062058. [DOI] [PubMed] [Google Scholar]