

Abstract
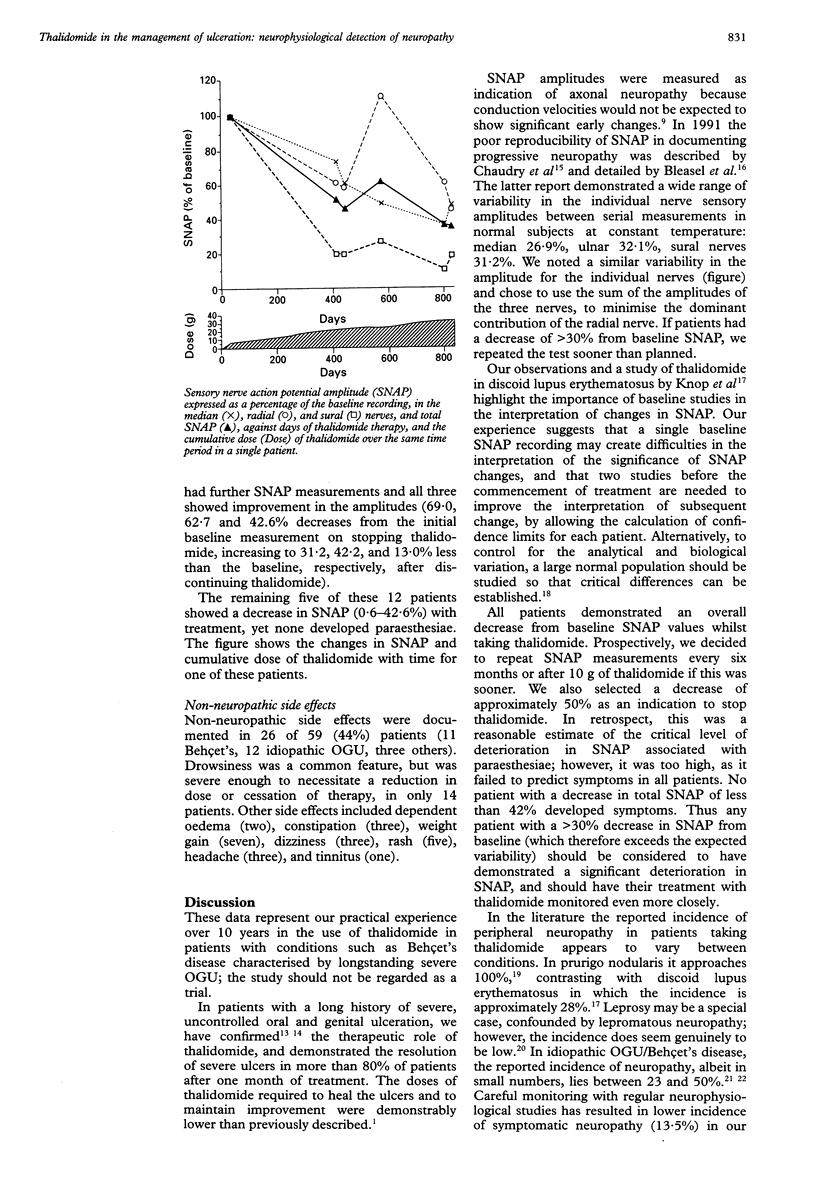
OBJECTIVE--To examine the efficacy, dose, and safety profile, including neurophysiological testing of thalidomide used in 59 patients (including 23 with Behçet's disease) to treat severe oral or genital ulceration (OGU). METHODS--We identified prospectively subjects (including women of childbearing potential) who had persistent OGU over periods lasting one to 40 years and whose active ulceration was not controlled by other therapies. They were treated with thalidomide. Retrospectively, we identified the number of subjects with complete resolution of the ulcers at one and two months of thalidomide therapy, and the dose required to maintain that improvement in those individuals who relapsed after stopping thalidomide. The decrease from the baseline sensory nerve action potential (baseline SNAP) amplitude value (derived from median, radial and sural nerve SNAPs) at which the development of paraesthesiae was likely to occur was also determined. RESULTS--Complete resolution of the ulcers occurred in 81% of patients within one month of thalidomide therapy at doses of 200 mg/day. No further thalidomide was required by 20% of patients responding and in the remainder improvement was maintained with smaller doses (7-200 mg/day). Using an approximate 50% decrease from baseline SNAP as an indication to discontinue thalidomide, the incidence of symptomatic neuropathy was 13.5%. No patients with a decrease of less than 42% developed neuropathy, and a further 13.5% were asymptomatic with a decrease in SNAP between 42 and 69%. Other side effects were seen in 44% of patients. There were no pregnancies and no requirement for urgent pregnancy testing. CONCLUSIONS--Thalidomide provided a useful therapeutic option in severe oral and genital ulceration which had not responded to other therapies. The physician must remain vigilant to the continuing danger of axonal neuropathy and teratogenesis at all times during thalidomide therapy.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bleasel A. F., Tuck R. R. Variability of repeated nerve conduction studies. Electroencephalogr Clin Neurophysiol. 1991 Dec;81(6):417–420. doi: 10.1016/0013-4694(91)90002-l. [DOI] [PubMed] [Google Scholar]
- Bowers P. W., Powell R. J. Effect of thalidomide on orogenital ulceration. Br Med J (Clin Res Ed) 1983 Sep 17;287(6395):799–800. doi: 10.1136/bmj.287.6395.799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burke D., Skuse N. F., Lethlean A. K. Sensory conduction of the sural nerve in polyneuropathy. J Neurol Neurosurg Psychiatry. 1974 Jun;37(6):647–652. doi: 10.1136/jnnp.37.6.647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chaudhry V., Cornblath D. R., Mellits E. D., Avila O., Freimer M. L., Glass J. D., Reim J., Ronnett G. V., Quaskey S. A., Kuncl R. W. Inter- and intra-examiner reliability of nerve conduction measurements in normal subjects. Ann Neurol. 1991 Dec;30(6):841–843. doi: 10.1002/ana.410300614. [DOI] [PubMed] [Google Scholar]
- Downie A. W., Scott T. R. An improved technique for radial nerve conduction studies. J Neurol Neurosurg Psychiatry. 1967 Aug;30(4):332–336. doi: 10.1136/jnnp.30.4.332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- FULLERTON P. M., KREMER M. Neuropathy after intake of thalidomide (distaval). Br Med J. 1961 Sep 30;2(5256):855–858. doi: 10.1136/bmj.2.5256.855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fullerton P. M., O'Sullivan D. J. Thalidomide neuropathy: a clinical electrophysiological, and histological follow-up study. J Neurol Neurosurg Psychiatry. 1968 Dec;31(6):543–551. doi: 10.1136/jnnp.31.6.543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GILLIATT R. W., SEARS T. A. Sensory nerve action potentials in patients with peripheral nerve lesions. J Neurol Neurosurg Psychiatry. 1958 May;21(2):109–118. doi: 10.1136/jnnp.21.2.109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grinspan D. Significant response of oral aphthosis to thalidomide treatment. J Am Acad Dermatol. 1985 Jan;12(1 Pt 1):85–90. doi: 10.1016/s0190-9622(85)70014-x. [DOI] [PubMed] [Google Scholar]
- Jenkins J. S., Powell R. J., Allen B. R., Littlewood S. M., Maurice P. D., Smith N. J. Thalidomide in severe orogenital ulceration. Lancet. 1984 Dec 22;2(8417-8418):1424–1426. doi: 10.1016/s0140-6736(84)91622-2. [DOI] [PubMed] [Google Scholar]
- Knop J., Bonsmann G., Happle R., Ludolph A., Matz D. R., Mifsud E. J., Macher E. Thalidomide in the treatment of sixty cases of chronic discoid lupus erythematosus. Br J Dermatol. 1983 Apr;108(4):461–466. doi: 10.1111/j.1365-2133.1983.tb04600.x. [DOI] [PubMed] [Google Scholar]
- Mascaro J. M., Lecha M., Torras H. Thalidomide in the treatment of recurrent, necrotic, and giant mucocutaneous aphthae and aphthosis. Arch Dermatol. 1979 May;115(5):636–637. [PubMed] [Google Scholar]
- Sampaio E. P., Moreira A. L., Sarno E. N., Malta A. M., Kaplan G. Prolonged treatment with recombinant interferon gamma induces erythema nodosum leprosum in lepromatous leprosy patients. J Exp Med. 1992 Jun 1;175(6):1729–1737. doi: 10.1084/jem.175.6.1729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sampaio E. P., Sarno E. N., Galilly R., Cohn Z. A., Kaplan G. Thalidomide selectively inhibits tumor necrosis factor alpha production by stimulated human monocytes. J Exp Med. 1991 Mar 1;173(3):699–703. doi: 10.1084/jem.173.3.699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saylan T., Saltik I. Thalidomide in the treatment of Behçet's syndrome. Arch Dermatol. 1982 Aug;118(8):536–536. [PubMed] [Google Scholar]
- Sheskin J. Therapeutische Erfahrungen über den Einfluss des Thalidomids bei der Lepra-Reaktion. Hautarzt. 1975 Jan;26(1):1–5. [PubMed] [Google Scholar]
- Wulff C. H., Høyer H., Asboe-Hansen G., Brodthagen H. Development of polyneuropathy during thalidomide therapy. Br J Dermatol. 1985 Apr;112(4):475–480. doi: 10.1111/j.1365-2133.1985.tb02323.x. [DOI] [PubMed] [Google Scholar]