

Abstract
Background Fluoride is vital in the prevention of dental caries in children. In 2014, the U.S. Preventive Services Task Force deemed fluoride varnish a recommended preventive service (grade B). Electronic health record-based clinical decision support (CDS) tools have shown variable ability to alter physicians' ordering behaviors.
Objectives This study aimed to increase the application of fluoride varnish in children while analyzing the effect of two passive CDS tools—an order set and a note template.
Methods Data on outpatient pediatric visits over an 18-month period before and after CDS implementation (October 15, 2020–April 15, 2022) were queried, while trends in application rate of fluoride were examined. We constructed a multiple logistic regression model with a primary outcome of whether a patient received fluoride at his/her visit. The primary predictor was a “phase” variable representing the CDS implemented. Physician interaction with CDS as well as the financial effects of the resulting service use were also examined.
Results There were 3,049 well-child visits of children aged 12 months to 5 years. The addition of a fluoride order to a “Well Child Check” order set led to a 10.6% increase in ordering over physician education alone (25.4 vs. 14.8%, p = 0.001), while the insertion of fluoride-specific text to drop-down lists in clinical notes led to a 6.2% increase (31.5 vs. 25.4%, p = 0.005). Whether a patient received topical fluoride was positively associated with order set implementation (odds ratio [OR] = 5.87, 95% confidence interval [CI]: 4.20–8.21) and fluoride-specific drop-down lists (OR = 7.81, 95% CI: 5.41–11.28). Female providers were more likely to use order sets when ordering fluoride (56.2 vs. 40.9% for males, p ≤ 0.0001). Added revenue totaled $15,084.
Conclusion The targeted use of order sets and note templates was positively associated with the ordering of topical fluoride by physicians.
Keywords: clinical decision support, electronic health record, fluoride
Background and Significance
Fluoride as a Preventive Service
Dental caries is a persistent scourge for all children. As the most common chronic disease in kids, caries account for millions of lost school hours per annum, disproportionately affect poor and minority populations, and negatively impact overall quality of life. 1 2 Fluoride plays a seminal role in caries prevention by promoting enamel remineralization, reducing enamel demineralization, and inhibiting bacterial metabolism and coincident acid production. 1 Sources of fluoride include toothpaste, water fluoridation, and topical fluoride varnish. Topical application provides a concentrated dose of fluoride to teeth, is well-tolerated, and causes minimal workflow interruption. Multiple studies have shown it to be both safe and effective, with number needed to treat to prevent one caries lesion of 14. 3 Lastly, a recent study characterizing caries risk assessment at four dental institutions found that children between the ages of 0 and 5 were the least likely age group to receive a caries risk assessment and to receive fluoride treatment for those at elevated risk, 4 emphasizing the importance of making this service more widely available in medical offices.
The U.S. Preventive Services Task Force (USPSTF) preventive services are a group of evidence-based recommendations from an independent, volunteer task force. 5 There are currently over 50 USPSTF services that have a grade A or B recommendation, and most private insurance plans are obligated to cover these without any additional patient copay. 5 6 In pediatrics, these include topical fluoride, depression screening, obesity screening, and vision screening, among others. Topical fluoride was first deemed a grade B recommendation in 2014 7 ; this stance was reiterated in a 2021 USPSTF Evidence Report. 3
Utility of Clinical Decision Support
In the past, the utility of physician education alone in quality improvement has been clouded by waning compliance and at times general ineffectiveness. 8 9 Furthermore, a recent study by Spiegel et al detailed a more significant and durable response in intravenous fluid ordering patterns after instituting clinical decision support (CDS) versus just clinician education. 10
Electronic health record (EHR)-delivered CDS mechanisms are generally classified as either active, if they interrupt the provider's workflow, or passive, if they do not. 11 While active CDS has received some notoriety for associated “alert fatigue” and diminished physician adherence over time, 12 passive CDS is often easier to implement, less intrusive, and may have greater sustainability. 10 Nevertheless, both types have proven effective in achieving desired behaviors or outcomes across multiple health care domains, including limiting unnecessary testing and treatment, 13 14 controlling costs, 13 15 and improving compliance with preventive services and standards of care. 16 17
Objective
We endeavored to standardize the application of topical fluoride in our clinic as a preventive service for all children between the onset of tooth eruption, as early as 6 months of age, and 5 years. In addition to clinician education, we utilized two passive CDS tools, age-targeted order sets and fluoride-specific verbiage in note templates.
Methods
Study Design
Well-child checks (WCCs) at our pediatric continuity clinic are partly resident-led, in which a resident physician evaluates the patient and discusses the plan with a supervising attending, and partly staffed by attendings only. In these encounters, computerized provider order entry is performed by both residents and attendings.
Prior to October 2020, the application of topical fluoride varnish was not performed at our clinic. At that time, an order for this procedure was created in our EHR and though most providers were aware that they could order fluoride, they were not provided guidelines or indications for use (deemed the “Pre-Instruction” phase in our statistical model). In February 2021, all clinic providers were given formal instructions for fluoride use via staff email, which included a description of the workflow, patient eligibility, and after visit instructions (“Post-Instruction” phase). In March 2021, an order for topical fluoride application was added to the appropriate age-specific order sets for WCCs, which are used in every pediatric WCC visit (“Order Set” phase). Of note, the order was optional (i.e., not default selected) and included the written guidance “Can be applied up to 3 times a year in a medical office.” To encompass the targeted age range, order sets for the following visits were included: 6 months, 9 months, 12 months, 15 months, 18 months, 24 months, 30 months, 3 years, 4 years, and 5 years. In December 2021, fluoride-specific drop-down lists were added to the “History” and “Assessment and Plan” sections of physician note templates (“Order Set + Note” phase) ( Table 1 ). These drop-down lists were formatted in such a way that providers either had to open and view the list, or delete it, to sign their note. Use of the lists was coded in our EHR and extracted to our clinical database for each encounter.
Table 1. Coded drop-down lists added to WCC visit note templates.
| History drop-down list | A&P drop-down list |
|---|---|
| • Care reviewed • Brushing teeth • Using fluoride toothpaste • Seen by dentist • Not yet seen by dentist • Received fluoride varnish at past clinic/dental visit (yes/no) • a |
• None • Fluoride varnish indicated and applied today • Received fluoride varnish within past 3 months • Fluoride varnish declined • Referral to dentist • a |
Abbreviations: A&P, assessment and plan; WCC, well-child check.
Note: There was no default selection.
Allows for free text entry.
All patients within this age range were eligible to receive fluoride varnish every 3 to 6 months independent of risk status, as per the American Academy of Pediatrics recommendations. 1
This study was part of a quality improvement project and was deemed exempt from review by the University of California, Los Angeles Institutional Review Board.
Data Source and Characteristics
Data were derived from our enterprise data warehouse and represented WCCs at our pediatric continuity clinic. Data queries included encounter-, patient-, provider-, and financial-level data. A Qualtrics survey was administered to physicians to assess note-taking habits.
Though topical fluoride is a recommended and covered benefit for all children between 6 months of age and 5 years, 1 this data set was limited to children between the ages of 11 months and 5 years and 3 months of age. The onset of teeth eruption is variable and commonly occurs between the ages of 6 to 10 months, 18 and thus some providers choose to defer fluoride application until the 12-month WCC visit. In our clinic, although fluoride can be applied at any pediatric visit, for the purposes of this study only WCC encounters, that is, International Classification of Diseases 10th Revision (ICD-10) Z00.129 for encounters with normal findings and Z00.121 for encounters with abnormal findings, were included. We divided WCC visits into two separate data sets, one detailing encounters in which the child received topical fluoride (Current Procedural Terminology code: 99188) and vice versa.
Statistical Analysis
Characteristics and demographic variables of patients and visit providers, all categorical, were grouped by encounter (fluoride ordered vs. not ordered) and presented as percentages. Distribution comparisons were achieved via Pearson's chi-squared test. We also performed a separate analysis of the variability in provider use of CDS tools.
We created a “Phase” categorical variable as a proxy for the implementation of the CDS tools. The “Pre-Instruction” phase encompassed the period from October 15, 2020, to February 18, 2021, during which an order for fluoride existed in our EHR, but no physician education was provided. The “Post-Instruction” phase encompassed the period from February 19, 2021, to March 21, 2021, during which physicians were given written guidelines on the indications for fluoride use. The “Order Set” phase encompassed the period from March 22, 2021 to December 21, 2021, during which the age-specific WCC order sets contained a fluoride order. The “Order Set + Note” phase reflects the period from December 22, 2021, to April 15, 2022, during which note template changes existed. The rates of fluoride use over time, as a percent of eligible encounters (all WCC visits), were calculated for each phase, and phase rate comparisons were done via the Cochran–Armitage trend test. Fluoride application rates by week were also calculated and included in a p control chart ( Fig. 1 ) with upper and lower control limits (±3 standard deviations). Of note, the period from December 21, 2020, to January 1, 2021, was grouped as 1 week due to low patient volumes in the setting of holiday closures. Similarly, dates from December 22, 2021, to January 7, 2022, were grouped as 1 week due to low patient volumes and to account for the start date of the “Order Set + Note” phase.
Fig. 1.
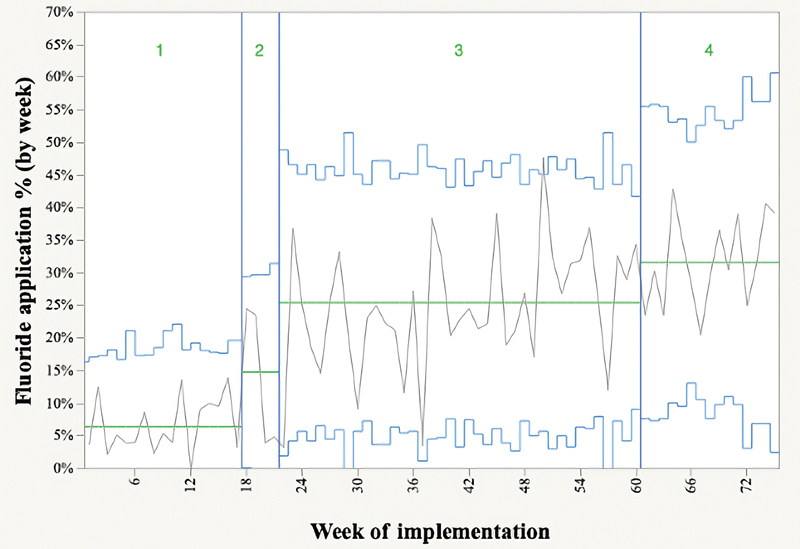
P control chart of fluoride application rates by week (green lines). Vertical blue lines delineate the four phases, which are numbered; horizontal, jagged blue lines represent control limits; flat, red center lines represent phase average application rates. Phase 1: “Pre-Instruction”; Phase 2: “Post-Instruction”; Phase 3: “Order Set”; Phase 4: “Order Set + Note.”
We constructed a multiple logistic regression model to evaluate the association of whether fluoride was ordered at an individual WCC encounter (outcome variable) with the phase variable and all independent variables noted in Table 2 . Interaction terms “phase”-“resident status,” “phase”-“provider sex,” and “number of diagnoses”-“WCC age category” were included to assess the independence of these terms. Backward stepwise regression control, calibrated to achieve minimum Bayesian Information Criterion (BIC), yielded the following statistically significant variables: WCC age category, number of diagnoses, phase, and the interaction term “phase-resident status.” WCC age category, number of diagnoses, phase, and resident status were included in the final model, while the interaction term was omitted for simplicity. All statistical analyses were conducting using JMP version 16.0.0.
Table 2. Demographic/characteristics of patients and providers.
| Patient/provider characteristics | +Fluoride ( n = 662, 21.7%) | –Fluoride ( n = 2,387, 78.3%) | p -Value |
|---|---|---|---|
| Patient characteristics | |||
| WCC category % ( n ) | <0.0001 | ||
| • 12 months | 22.8 (151) | 13.3 (318) | |
| • 15 mo | 12.7 (84) | 11.4 (271) | |
| • 18 mo | 19.8 (131) | 13.8 (329) | |
| • 24 mo | 16.9 (112) | 11.6 (277) | |
| • 30 mo | 7.4 (49) | 4.9 (118) | |
| • 36 mo | 8.8 (58) | 13.6 (324) | |
| • 48 mo | 8.0 (53) | 17.2 (410) | |
| • 60 mo | 3.6 (24) | 14.2 (340) | |
| Sex % ( n ) female | 42.2 (279) | 44.3 (1,058) | 0.32 |
| Race and ethnicity % ( n ) | 0.66 | ||
| • Asian | |||
| • Hispanic | 1.1 (7) | 0.7 (16) | |
| • Non-Hispanic | 12.4 (82) | 12.3 (294) | |
| • Black | |||
| • Hispanic | 1.1 (7) | 1.0 (24) | |
| • Non-Hispanic | 6.8 (45) | 6.8 (163) | |
| • White | |||
| • Hispanic | 11.2 (74) | 9.7 (231) | |
| • Non-Hispanic | 16.6 (110) | 15.7 (375) | |
| • Other race | |||
| • Hispanic | 23.4 (155) | 24.3 (580) | |
| • Non-Hispanic | 22.4 (148) | 22.0 (526) | |
| • Unknown/not reported | |||
| • Hispanic | 4.8 (32) | 7.1 (170) | |
| • Non-Hispanic | 0.3 (2) | 0.3 (8) | |
| Preferred language % ( n ) | 0.45 | ||
| • English | 88.8 (588) | 87.6 (2,091) | |
| • Spanish | 9.4 (62) | 9.8 (233) | |
| • Other | 1.8 (12) | 2.6 (63) | |
| Payor mix % ( n ) | 0.20 | ||
| • Medicaid | 49.4 (327) | 53.1 (1,268) | |
| • HMO | 21.4 (142) | 19.1 (456) | |
| • PPO | 29.2 (193) | 27.8 (663) | |
| No. of diagnoses % ( n ) | < 0.0001 | ||
| • 1–3 | 38.5 (255) | 45.8 (1,093) | |
| • 4–6 | 39.6 (262) | 39.4 (940) | |
| • 7–9 | 18.7 (124) | 13.2 (314) | |
| • 10+ | 3.2 (21) | 1.7 (40) | |
| Provider characteristics | |||
| Resident % ( n ) | 49.8 (330) | 54.7 (1,306) | 0.03 |
| Sex % ( n ) female | 67.8 (449) | 65.6 (1,565) | 0.28 |
Abbreviations: HMO, health maintenance organization; PPO, preferred provider organization; WCC, well-child check.
Note: n represents number of encounters. Pearson's chi-squared used as significance test.
Results
A total of 3,049 12- to 60-month WCCs took place at the intervention clinic during the 18-month intervention period, with fluoride given in 21.7% overall. Table 2 shows the characteristics and demographic variables of patients and visit providers. Younger patients accounted for a greater proportion of fluoride recipients. Residents were primary providers for a greater proportion of visits at which fluoride was not ordered versus visits at which fluoride was ordered. Lastly, patients who received fluoride also tended to have more diagnoses addressed at their visit.
Unadjusted fluoride application rates are compared for the four phases of implementation (“Pre-Instruction,” “Post-Instruction,” “Order Set,” “Order Set + Note”) in Fig. 1 . In the “Pre-Instruction” phase, prior to giving basic instructions/education to physicians on fluoride guidelines and indication, only 6.4% of eligible patients received fluoride at their clinic visit. This increased to 14.8% during the “Post-Instruction” phase; to 25.4% during the “Order Set” phase; and to 31.5% during the “Order Set + Note” phase (trend p < 0.0001). In the subset of 557 encounters during the “Order Set + Note” phase, physicians who interacted with the fluoride-specific drop-down lists ordered fluoride at a much greater frequency than physicians who did not use these features (78.8 vs. 16.9%, p < 0.0001). Of note, these two drop-down lists are encoded in all age-appropriate visit note templates ( Table 1 ). A physician was categorized as having interacted with the fluoride-specific elements in the list if they selected “received fluoride varnish at past clinic/dental visit: yes/no” in the “History/Drop-Down List,” or if they selected any of “fluoride varnish indicated and applied today,” “received fluoride varnish within past 3 months,” or “fluoride varnish declined” from the “A&P Drop-Down List.”
Table 3 illustrates the breakdown of CDS tool use (order set and note drop-down lists) by visit provider characteristics. During the “Order Set” phase, a total of 590 fluoride encounters occurred. Female physicians used order sets to place fluoride orders more frequently than did male physicians. There was no significant difference in order set use between residents and attendings. During the “Order Set + Note” phase, a total of 176 fluoride encounters occurred. In these encounters, female physicians utilized fluoride-specific drop-down lists more commonly than their male counterparts, as did attendings versus residents although neither finding was statistically significant. Lastly, all 73 physicians in our clinic (64 residents and 9 attendings) were surveyed on their note-taking habits to determine when they work on notes. Twenty-three (21 residents and 2 attendings) responded, with the 12/23 reporting that they work on the “History” section of the note during a visit, while the remaining 11/23 reporting that they work on all parts of the note during a visit.
Table 3. Provider characteristics and their use of CDS in fluoride-only encounters.
| Provider characteristics | Use of order set and note drop-down lists at fluoride encounters | |||
|---|---|---|---|---|
| Order Set | p -Value | Lists | p -Value | |
| Gender | <0.0001 | 0.18 | ||
| Female | 56.2% (227/404) | 64.5% (80/124) | ||
| Male | 40.9% (76/186) | 53.9% (28/52) | ||
| Training | 0.42 | 0.26 | ||
| Resident | 53.0% (158/298) | 58.2% (64/110) | ||
| Attending | 49.7% (145/292) | 66.7% (44/66) | ||
Abbreviation: CDS, clinical decision support.
Note: Values are listed as row percents, e.g., female physicians used order sets for fluoride in 227 of 404 encounters and used note drop-down lists in 80 of 124. Pearson's chi-squared used as significance test.
The multiple logistic regression output is detailed in Table 4 . Overall model performance was notable for an area under the curve (AUC) of 0.74, sensitivity of 0.75, and specificity of 0.61. Whether a patient received topical fluoride was increasingly positively associated with each implementation phase. In addition, greater use of fluoride was associated with having more visit diagnoses and with seeing an attending only. Age, as represented by WCC visit category, had a negative association with fluoride application at 36, 48, and 60 months. As noted, the interaction term was omitted from the final model as it had minimal effect on model performance (AUC difference of 0.005), and for simplicity of presentation.
Table 4. Multiple logistic regression final model of whether a patient received fluoride at their visit.
| Final model variables | OR (95% CI) | p -Value | |
|---|---|---|---|
| Phase | |||
| • Preinstruction | Reference | 6.4/5.3% | |
| • Postinstruction | 2.54 (1.52–4.24) | 14.8/12.5% | 0.0004 |
| • Order set | 5.87 (4.20–8.21) | 25.4/24.8% | <0.0001 |
| • Order set + note | 7.81 (5.41–11.28) | 31.5/30.5% | <0.0001 |
| WCC | |||
| • 12 mo | Reference | ||
| • 15 mo | 0.81 (0.57–1.13) | 0.22 | |
| • 18 mo | 1.19 (0.86–1.64) | 0.30 | |
| • 24 mo | 1.17 (0.84–1.64) | 0.36 | |
| • 30 mo | 1.12 (0.73–1.71) | 0.60 | |
| • 36 mo | 0.45 (0.31–0.65) | <0.0001 | |
| • 48 mo | 0.27 (0.19–0.40) | <0.0001 | |
| • 60 mo | 0.16 (0.10–0.26) | <0.0001 | |
| Resident status | |||
| • Yes | Reference | ||
| • No | 1.42 (1.18–1.71) | 0.0003 | |
| No. of diagnoses | |||
| • 1–3 | Reference | ||
| • 4–6 | 1.86 (1.49–2.31) | <0.0001 | |
| • 7–9 | 2.30 (1.70–3.11) | <0.0001 | |
| • 10+ | 3.28 (1.78–6.04) | 0.0001 | |
Abbreviations: CI, confidence interval; OR, odds ratio; WCC, well-child check.
Note: The “Phase” variable also includes the fluoride application rate for a given phase reported as unadjusted/adjusted (adjusted for variables “WCC,” “Resident Status,” “# Diagnoses”).
In terms of financials, the inventory price for a single McKesson applicator during this study was approximately $2. The insurance mix of our resident clinic is predominantly Medi-Cal, California's version of Medicaid ( Table 2 ). Managed care Medi-Cal, which comprises most of our Medi-Cal plans, is a capitated plan and thus did not reimburse for this service. Nonmanaged care Medi-Cal remitted $18 per application, while preferred provider organization plans in our region, representing 28% of our payor mix, paid an average of $68 per application.
At our clinic, the application of varnish is done by both medical assistants (MAs) and licensed vocational nurses (LVNs). Anecdotally they have reported that acknowledging the order, preparing the materials, and applying the varnish takes 5 minutes per patient. According to the U.S. Bureau of Labor Statistics, in 2021, the mean hourly wage for MAs employed in California was $21.53, 19 while the mean hourly wage for LVNs was $31.32. 20 Assuming a mean MA/LVN wage of $26.43, each application procedure incurs a labor cost of approximately $2.20.
Over this 18-month period, the added revenue, net of material costs, and estimated labor costs, totaled $15,084. Of note, providers in this clinic had no knowledge of and did not receive any financial incentives related to this intervention.
Discussion
In our study combining two forms of passive CDS in the implementation of a USPSTF recommended service, we found a statistically significant increase in fluoride application rates associated with our CDS interventions. As expected, clinician education provided an initial boost, but this appears to have been amplified by both CDS mechanisms, which have so far resulted in sustained rate increases.
Studies have shown that customized order sets can be used to alter clinician ordering behavior. 10 21 22 Indeed, in our study, after age-specific order sets were modified to include topical fluoride, orders sustainably increased by more than 10% over clinician education alone. Interestingly, female physicians were much more likely to utilize order sets for fluoride ordering than were their male counterparts. However, this did not lead to a statistically significant difference in the increase in fluoride-ordering rates between genders (females +10.3% vs. males +11.2%, p = 0.88). This finding is difficult to explain. Given that our “Post-Instruction” period, which took place prior to order set implementation, accounted for only 196 (6.4%) of all encounters, it is possible that the increase in application rates during the “Order Set” phase is a result of increased provider awareness and assimilation rather than direct order set use for fluoride orders. Nevertheless, given that all providers in our clinic utilize age-specific order sets for every WCC visit, the visibility of the fluoride order as part of the WCC workflow likely still has indirect effects on ordering, that is, by making physicians aware that topical fluoride may be given at the visit.
In a recent study of medical intensivists' EHR use and perceptions, Khairat et al found that female physicians demonstrated greater efficiency and lower levels of frustration with the EHR, as well as higher satisfaction with its ease of use and marginally higher perceived overall EHR usability as compared with their male counterparts. 23 As it relates to our study, it is possible that female providers were simply more receptive to using order sets. Compared with the use of a standalone order, ordering fluoride via the order set is more efficient, requiring fewer keystrokes and automatically associating the procedure with the appropriate diagnosis. Though not statistically significant, female physicians were also more responsive to our other CDS tool, as they utilized fluoride-specific drop-down lists more commonly than their male counterparts in both fluoride visits and across all visits during the “Order Set + Note” phase.
The use of note templates has been associated with improved documentation, 24 25 data capture, 26 and clinician education. 24 27 Other research has shown that the effects of targeted templates on physician decision-making specifically to be mixed. Linder et al implemented a documentation-based CDS (“Smart Form”) aimed at improving the prescription of antibiotics for the treatment of acute respiratory infections (ARIs) but found no significant reduction in overall prescriptions or “improved appropriateness” of use. The authors attributed the findings to poor uptake of the Smart Form. 28 A similar study by Litvin et al reported a “sustained impact on reducing the use” of unnecessary antibiotics for ARIs with the use of a progress note template customized as a CDS system. 29 Both efforts employed detailed, disease-specific templates that required data entry and used branch logic. The projects were also buttressed with extensive, ongoing education and support on both the CDS tool itself and ARI best practices.
In contrast, our study shows how introducing subtle changes in a note template, in this case by adding fluoride-specific language to preexisting drop-down lists, can have an outsized effect. Furthermore, this was easily integrated into common, universally used templates, required no additional education or support, and did not appreciably alter a workflow. The intent of these modified lists was to serve as a passive reminder to the physician to consider topical fluoride during the visit. Physicians who interacted with fluoride-specific drop-down lists ordered fluoride at a far greater frequency than did physicians who did not use these features. This could be at least partially explained by the fact that when a patient receives fluoride, the provider may be more inclined to document that in their note after the visit, that is, by choosing the appropriate entry from our coded drop-down lists. This does not explain the measurable fluoride rate increase in the “Order Set + Note” phase (31.5%) versus in the “Order Set” phase (25.4%). Furthermore, in our survey of clinic physicians, all 23 responded that they work on the visit note in tandem with seeing the patient. Twelve of 23 respondents said that they only work on the “History” section of the note during the visit (which includes 1 of 2 of our coded drop-down lists), while the remainder said that they work on both the “History” and the “Assessment & Plan” sections of the note. Thus, it is plausible that aspects of a templated note influence physician decision-making.
Of the covariates, younger patients accounted for a greater number of fluoride applications. This is consistent with the fact that regular dentist visits increase with age, 30 likely having a negative effect on the ordering of topical fluoride for older children in a medical office. Additionally, there was a positive association between fluoride use and the number of diagnoses addressed at the WCC visit. In our model, all higher numbered diagnosis categories had statistically significant odds ratios (ORs) versus the reference category of 1 to 3 diagnoses. Children receive most childhood vaccines within the first 2 years of life, and each usually carries its own specific ICD-10 diagnosis. Intuitively, younger patients, who are more likely to receive fluoride because of their age, are also more likely to receive vaccines at the same encounter. Finally, attending physicians were 42% more likely to order fluoride than resident physicians, which may be expected given presumed experience disparities.
Lastly, our study makes a strong financial argument for standardizing USPSTF recommended services (grade A or B), such as depression and obesity screening in pediatrics, with the help of CDS. Topical fluoride in particular is well-reimbursed with little added cost and potentially averts future costs related to caries. Prior research has shown that establishing preventive dental care at younger ages leads to a decrease in the average cost of the first visit with a dentist due to earlier identification and prevention of caries. 31 Scherrer and Naavaal studied the application of fluoride varnish in primary clinics in Virginia. They estimate that delivering fluoride to all pediatric Medicaid patients under the age of 3 in that state would result in savings of nearly $2 million per year thanks to averted restoration care. 32
Limitations
Our study has limitations. Our “Post-Instruction” phase was brief relative to our other phases, with total number of encounters of 196 representing only 6.4% of all encounters during the study. Nevertheless, both CDS changes resulted in statistically significant rate increases. For operational reasons, the “Order Set” phase was longer than the “Order Set + Note” phase, but both phases had sufficient data to carry out the analysis. We also did not evaluate for baseline secular trends, though this study was not designed as an interrupted time series. It was not possible to assess the clinical outcome of caries prevention due to the relatively small time period of the study and to the limited documentation of caries in the medical record, but the linkage of fluoride application to caries prevention is well-established. Similarly, we do not have data on dental history and dentist visits, both of which most likely affect our primary outcome. We were not able to discriminate the separate effects of the two drop-down lists added to our provider notes (e.g., by including a drop-down list variable), as the small sample size added bias to our model. Furthermore, the effects of our note changes may be blunted by the fact that an unknown number of individual providers make customized copies of note templates that do not receive system-wide updates. Lastly, this study was performed at a single academic resident clinic (for a single USPSTF procedural service), a unique set of circumstances that may limit generalizability.
Conclusion
By implementing passive CDS tools, we were able to sustainably increase rates of topical fluoride application in children with minimal added EHR burden for clinicians. This led to a significant increase in revenue net of material cost and can be expected to decrease the incidence of caries in our patients over time.
Clinical Relevance Statement
This study quantifies the subtle yet notable effects of CDS tools on physician ordering patterns. Such methods could be similarly used to optimize many ambulatory workflows, including additional USPSTF recommended services.
Multiple-Choice Questions
-
Which of the following is an example of passive (noninterruptive) clinical decision support?
Order set
Templated note
Best practice alert
Both a and b
Correct Answer: The correct answer is option d. Order sets and templated physician notes are both examples of passive clinical decision support which reinforce best practices without requiring action from the provider. Best practice alerts, often appearing as “pop-ups,” are a type of active (interruptive) CDS and can be specific to a patient's condition. They require direct action from the provider, for example, acknowledging the alert or ordering an intervention.
-
In this study, which of the following model variables showed a negative association with the ordering of fluoride varnish?
Older patient age
The visit provider was an attending
More visit diagnoses
An order set containing a fluoride order
Correct Answer: The correct answer is option a. In Table 4 , patients aged 36, 48, and 60 months had ORs of 0.45, 0.27, and 0.16. As noted in the discussion, older patients are more likely to have seen a dentist and to have received fluoride varnish at that visit. Answers b, c, and d all showed positive associations with fluoride ordering.
Funding Statement
Funding This research was supported by NIH National Center for Advancing Translational Science (NCATS) UCLA CTSI grant number: TL1TR001883.
Conflict of Interest None declared.
Protection of Human and Animal Subjects
This study was conducted for quality improvement and deemed exempt from review by the University of California, Los Angeles Institutional Review Board.
References
- 1.SECTION ON ORAL HEALTH . Clark M B, Keels M A, Slayton R L. Fluoride use in caries prevention in the primary care setting. Pediatrics. 2020;146(06):e2020034637. doi: 10.1542/peds.2020-034637. [DOI] [PubMed] [Google Scholar]
- 2.Seow W K. Early childhood caries. Pediatr Clin North Am. 2018;65(05):941–954. doi: 10.1016/j.pcl.2018.05.004. [DOI] [PubMed] [Google Scholar]
- 3.Chou R, Pappas M, Dana T. Screening and interventions to prevent dental caries in children younger than 5 years: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2021;326(21):2179–2192. doi: 10.1001/jama.2021.15658. [DOI] [PubMed] [Google Scholar]
- 4.Bangar S, Neumann A, White J M. Caries risk documentation and prevention: eMeasures for dental electronic health records. Appl Clin Inform. 2022;13(01):80–90. doi: 10.1055/s-0041-1740920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.U.S. Preventive Services Task Force USPSTF: Who We Are & How We WorkAccessed May 13, 2022, at:https://www.uspreventiveservicestaskforce.org/uspstf/sites/default/files/inline-files/uspstf-who-we-are-how-we-work_1.pdf
- 6.U.S. Preventive Services Task Force A & B Recommendations. Accessed May 13, 2022, at:https://www.uspreventiveservicestaskforce.org/uspstf/recommendation-topics/uspstf-a-and-b-recommendations
- 7.Prevention of dental caries in children from birth through five years of age: recommendation statement. Am Fam Physician. 2015;91(03):190A. [PubMed] [Google Scholar]
- 8.Bruno C, Pearson S A, Daniels B, Buckley N A, Schaffer A, Zoega H. Passing the acid test? Evaluating the impact of national education initiatives to reduce proton pump inhibitor use in Australia. BMJ Qual Saf. 2020;29(05):365–373. doi: 10.1136/bmjqs-2019-009897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.The Cochrane Effective Practice and Organization of Care Review Group Bero L A, Grilli R, Grimshaw J M, Harvey E, Oxman A D, Thomson M A.Closing the gap between research and practice: an overview of systematic reviews of interventions to promote the implementation of research findings BMJ 1998317(7156):465–468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Spiegel M C, Simpson A N, Philip A. Development and implementation of a clinical decision support-based initiative to drive intravenous fluid prescribing. Int J Med Inform. 2021;156:104619. doi: 10.1016/j.ijmedinf.2021.104619. [DOI] [PubMed] [Google Scholar]
- 11.Bell G C, Crews K R, Wilkinson M R.Development and use of active clinical decision support for preemptive pharmacogenomics J Am Med Inform Assoc 201421(e1):e93–e99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.with the HITEC Investigators . Ancker J S, Edwards A, Nosal S, Hauser D, Mauer E, Kaushal R. Effects of workload, work complexity, and repeated alerts on alert fatigue in a clinical decision support system. BMC Med Inform Decis Mak. 2017;17(01):36–17. doi: 10.1186/s12911-017-0430-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Escovedo C, Bell D, Cheng E. Noninterruptive clinical decision support decreases ordering of respiratory viral panels during influenza season. Appl Clin Inform. 2020;11(02):315–322. doi: 10.1055/s-0040-1709507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.McGinn T G, McCullagh L, Kannry J. Efficacy of an evidence-based clinical decision support in primary care practices: a randomized clinical trial. JAMA Intern Med. 2013;173(17):1584–1591. doi: 10.1001/jamainternmed.2013.8980. [DOI] [PubMed] [Google Scholar]
- 15.Goetz C, Rotman S R, Hartoularos G, Bishop T F. The effect of charge display on cost of care and physician practice behaviors: a systematic review. J Gen Intern Med. 2015;30(06):835–842. doi: 10.1007/s11606-015-3226-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Dexter P R, Perkins S M, Maharry K S, Jones K, McDonald C J. Inpatient computer-based standing orders vs physician reminders to increase influenza and pneumococcal vaccination rates: a randomized trial. JAMA. 2004;292(19):2366–2371. doi: 10.1001/jama.292.19.2366. [DOI] [PubMed] [Google Scholar]
- 17.Demakis J G, Beauchamp C, Cull W L. Improving residents' compliance with standards of ambulatory care: results from the VA Cooperative Study on Computerized Reminders. JAMA. 2000;284(11):1411–1416. doi: 10.1001/jama.284.11.1411. [DOI] [PubMed] [Google Scholar]
- 18.Lunt R C, Law D B. A review of the chronology of eruption of deciduous teeth. J Am Dent Assoc. 1974;89(04):872–879. doi: 10.14219/jada.archive.1974.0484. [DOI] [PubMed] [Google Scholar]
- 19.Occupational Employment and Wages May 2021. U.S. Bureau of Labor Statistics. Updated March 31, 2022. Accessed November 14, 2022, at:https://www.bls.gov/oes/current/oes319092.htm
- 20.Occupational Employment and Wages May 2021. U.S. Bureau of Labor Statistics. Updated March 31, 2022. Accessed November 14, 2022, at:https://www.bls.gov/oes/current/oes292061.htm
- 21.Olson J, Hollenbeak C, Donaldson K, Abendroth T, Castellani W. Default settings of computerized physician order entry system order sets drive ordering habits. J Pathol Inform. 2015;6:16–3539. doi: 10.4103/2153-3539.153916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Chan A J, Chan J, Cafazzo J A. Order sets in health care: a systematic review of their effects. Int J Technol Assess Health Care. 2012;28(03):235–240. doi: 10.1017/S0266462312000281. [DOI] [PubMed] [Google Scholar]
- 23.Khairat S, Coleman C, Ottmar P, Bice T, Koppel R, Carson S S. Physicians' gender and their use of electronic health records: findings from a mixed-methods usability study. J Am Med Inform Assoc. 2019;26(12):1505–1514. doi: 10.1093/jamia/ocz126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Grogan E L, Speroff T, Deppen S A. Improving documentation of patient acuity level using a progress note template. J Am Coll Surg. 2004;199(03):468–475. doi: 10.1016/j.jamcollsurg.2004.05.254. [DOI] [PubMed] [Google Scholar]
- 25.Seligson M T, Lyden S P, Caputo F J, Kirksey L, Rowse J W, Smolock C J. Improving clinical documentation of evaluation and management care and patient acuity improves reimbursement as well as quality metrics. J Vasc Surg. 2021;74(06):2055–2062. doi: 10.1016/j.jvs.2021.06.027. [DOI] [PubMed] [Google Scholar]
- 26.Hye R J, Inui T S, Anthony F F. A multiregional registry experience using an electronic medical record to optimize data capture for longitudinal outcomes in endovascular abdominal aortic aneurysm repair. J Vasc Surg. 2015;61(05):1160–1166. doi: 10.1016/j.jvs.2014.12.055. [DOI] [PubMed] [Google Scholar]
- 27.Shirazian S, Wang R, Moledina D. A pilot trial of a computerized renal template note to improve resident knowledge and documentation of kidney disease. Appl Clin Inform. 2013;4(04):528–540. doi: 10.4338/ACI-2013-07-RA-0048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Linder J A, Schnipper J L, Tsurikova R. Documentation-based clinical decision support to improve antibiotic prescribing for acute respiratory infections in primary care: a cluster randomised controlled trial. Inform Prim Care. 2009;17(04):231–240. doi: 10.14236/jhi.v17i4.742. [DOI] [PubMed] [Google Scholar]
- 29.Litvin C B, Ornstein S M, Wessell A M, Nemeth L S, Nietert P J. Adoption of a clinical decision support system to promote judicious use of antibiotics for acute respiratory infections in primary care. Int J Med Inform. 2012;81(08):521–526. doi: 10.1016/j.ijmedinf.2012.03.002. [DOI] [PubMed] [Google Scholar]
- 30.Edelstein B L, Chinn C H. Update on disparities in oral health and access to dental care for America's children. Acad Pediatr. 2009;9(06):415–419. doi: 10.1016/j.acap.2009.09.010. [DOI] [PubMed] [Google Scholar]
- 31.Savage M F, Lee J Y, Kotch J B, Vann W F., Jr Early preventive dental visits: effects on subsequent utilization and costs. Pediatrics. 2004;114(04):e418–e423. doi: 10.1542/peds.2003-0469-F. [DOI] [PubMed] [Google Scholar]
- 32.Scherrer C R, Naavaal S.Cost-savings of fluoride varnish application in primary care for Medicaid-enrolled children in Virginia J Pediatr 2019212201–207..e1 [DOI] [PubMed] [Google Scholar]