

This qualitative study evaluates how experts define and diagnose cesarean scar disorder.
Key Points
Question
How do experts define the clinical condition that constitutes a symptomatic niche in the uterine cesarean scar?
Findings
In this modified Delphi study, which included 31 international gynecologists, consensus was achieved on the definition, symptoms, conditions to exclude, and diagnostic criteria of a cesarean scar disorder, following a modified Delphi procedure.
Meaning
Using a standardized definition for the constellation of symptoms resulting from a symptomatic uterine cesarean scar will allow better recognition of this condition, improve patient care, prevent overtreatment, and create a patient-centric foundation of niche-related research in the future.
Abstract
Importance
Approximately 60% of women develop a uterine niche after a cesarean delivery (CD). A niche is associated with various gynecological symptoms including abnormal uterine bleeding, pain, and infertility, but there is little consensus in the literature on the distinction between the sonographic finding of a niche and the constellation of associated symptoms.
Objective
To achieve consensus on defining the clinical condition that constitutes a symptomatic uterine niche and agree upon diagnostic criteria and uniform nomenclature for this condition.
Design, Setting, and Participants
A consensus based modified electronic Delphi (eDelphi) study, with a predefined Rate of Agreement (RoA) of 70% or higher. Experts were selected according to their expertise with niche-related consultations, publications, and participation in expert groups and received online questionnaires between November 2021 and May 2022.
Main Outcomes and Measures
Definition, nomenclature, symptoms, conditions to exclude, and diagnostic criteria of an illness caused by a symptomatic uterine niche.
Results
In total, 31 of the 60 invited experts (51.7%) participated, of whom the majority worked in university-affiliated hospitals (28 of 31 [90.3%]), specialized in benign gynecology (20 of 31 [64.5%]), and worked in Europe (24 of 31 [77.4%]). Three rounds were required to achieve consensus on all items. All participants underlined the relevance of a new term for a condition caused by a symptomatic niche and its differentiation from a sonographic finding only. Experts agreed to name this condition cesarean scar disorder, defined as a uterine niche in combination with at least 1 primary or 2 secondary symptoms (RoA, 77.8%). Defined primary symptoms were postmenstrual spotting, pain during uterine bleeding, technical issues with catheter insertion during embryo transfer, and secondary unexplained infertility combined with intrauterine fluid. Secondary symptoms were dyspareunia, abnormal vaginal discharge, chronic pelvic pain, avoiding sexual intercourse, odor associated with abnormal blood loss, secondary unexplained infertility, secondary infertility despite assisted reproductive technology, negative self-image, and discomfort during participation in leisure activities. Consensus was also achieved on certain criteria that should be met and conditions that should be excluded before making the diagnosis.
Conclusions and Relevance
In this modified Delphi study, a panel of 31 international niche experts reached consensus for the constellation of symptoms secondary to a uterine niche and named it cesarean scar disorder.
Introduction
Cesarean delivery (CD) is the most commonly performed surgery worldwide.1 A long-term complication of a CD is an unhealed defect in the uterine myometrium, which is often referred to as a uterine niche or cesarean scar defect. This entity is formally defined by the European Niche Taskforce as an “indentation in the uterine myometrium of at least 2 mm at the site of the cesarean scar assessed by transvaginal ultrasound.”2 A niche is observed in 60% of women after a CD and 25% of all women have a large defect with a residual myometrium of less than 3 mm.3,4 Approximately 30% to 40% of women with a CD niche experience symptoms5 such as postmenstrual spotting, dysmenorrhea, chronic pelvic pain, and infertility.3,6,7,8 Symptomatic niches can have a profound impact on patients’ quality of life.9
Given that the CD niche is a fairly new but increasingly common observed entity, the literature reports a wide variety of symptoms, conditions, and therapies for patients with a niche.10,11,12 Studies include heterogenous patient populations from asymptomatic to those with various symptom profiles, where the association with the niche may be tenuous. Consequently, due to lack of clear guidelines, it is difficult to propose optimal treatments and informed counseling to patients with a niche. It is essential that future clinical practice guidelines and policies make the distinction between a sonographic finding of a niche and the constellation of associated symptoms. The objective of this electronic Delphi (eDelphi) study was to reach consensus among international experts on defining the clinical condition that constitutes a symptomatic niche in the uterine CD scar and agree upon diagnostic criteria and uniform nomenclature for this condition.
Methods
We performed an eDelphi study between November 22, 2021, and May 16, 2022. A Delphi is an iterative process with anonymous consultation, feedback, and qualitative analysis of the responses. This technique has been used widely in health care research, within the field of education, and in developing clinical practice.13,14 To this end, we designed an electronic platform to efficiently obtain consensus from international experts. The purpose of this design was to continue with rounds until consensus was achieved for all questions. To determine the first round of questions, we performed a systematic review of the available evidence, followed by a focus group discussion with experts. After formulating the questionnaire, we assembled the Delphi panel and started the first round. Approval of this study was granted by the institutional review board of Amsterdam University Medical Center (location VUmc) and registered at Open Science Framework registries. Participants provided written informed consent. The Standards for Reporting Qualitative Research (SRQR) and Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guidelines guided the study process.15
Systematic Literature Review and Focus Group Discussion
A systematic literature search was performed to evaluate symptoms that are reported in association with a niche. We used the previously published systematic review of Stegwee et al9 and updated this search in November 2021 (the search strategy and results are presented in the eAppendix and eFigure in Supplement 1). We included full-text English language studies that reported on symptoms associated with CD niche. These studies were evaluated by 2 independent researchers (S.K. and R.L.) who extracted baseline characteristics of the studies, methods, reported symptoms, and their prevalence. According to this literature review, a focus group of 5 Dutch niche experts helped determine the list of symptoms and questions to be included in the first round of the eDelphi. These experts evaluate at least 50 patients with niche-related issues annually. The first round consisted of items categorized into the following 6 themes: (1) nomenclature, (2) gynecological symptoms, (3) fertility-related symptoms, (4) social relationships and participation, (5) obstetrical symptoms, and (6) conditions to exclude and diagnostic criteria.
Expert Panel Recruitment
We defined a niche expert as an obstetrician or gynecologist who consults on more than 30 niche-related issues annually and has participated or is actively participating in niche or CD-related research. Potential experts were identified through our literature search and society membership (European Niche Taskforce, Cesarean Scar Pregnancy Registry Team Steering Group, and International Society for Placenta Accreta Spectrum). Potential eligible experts were invited to complete a questionnaire to determine eligibility and were subsequently invited to participate if they met inclusion criteria.
Patient Representative Endorsement
It was important for us to incorporate the patient perspective in this process. The questions of the first round of the Delphi were based on a focus group discussions among patients, which has been published separately.9 Finally, after the Delphi was completed, we performed a focus interview with experienced representatives to discuss the results. The patients who were involved were recruited from Amsterdam University Medical Centre or were representatives of the Dutch niche Facebook group.16 Those with a large symptomatic niche were invited to participate in an online meeting to discuss the proposed definition, symptoms, conditions to exclude, and diagnostic criteria. Women who volunteered to participate signed an informed consent.
Statistical Analysis
eDelphi Rounds 1 to 3
All questions in the first round (see eTable in Supplement 1) were accompanied by an overview of the available literature. In the survey, participants were asked to evaluate each statement using a 3-point Likert scale (agree, neutral, or disagree), or indicate “not my expertise.” We used the following definitions: agreement: “I agree with the following statement;” disagreement: “I do not agree with the following statement;” neutral: “I do not have an opinion about the following statement.” These definitions are consistent with previously published work.17,18 All survey items included space for comments and reflections. In subsequent rounds, an overview of the results of the previous round was provided. When consensus was not reached for a particular concept, the arguments of all experts were anonymously shown in the next round for participant consideration. This allowed us to emulate the spirit of discussion that is essential in Delphi consensus such that anonymized arguments could be shared between the experts. The questions that did not reach consensus were then either repeated or rephrased according to the input given. Additional clarifying questions were included as required. The Figure shows the flow diagram showing agreement or rejection of items during the Delphi procedure.
Figure. Flow Diagram Summarizing Agreement or Rejection of Items During Delphi Procedure.
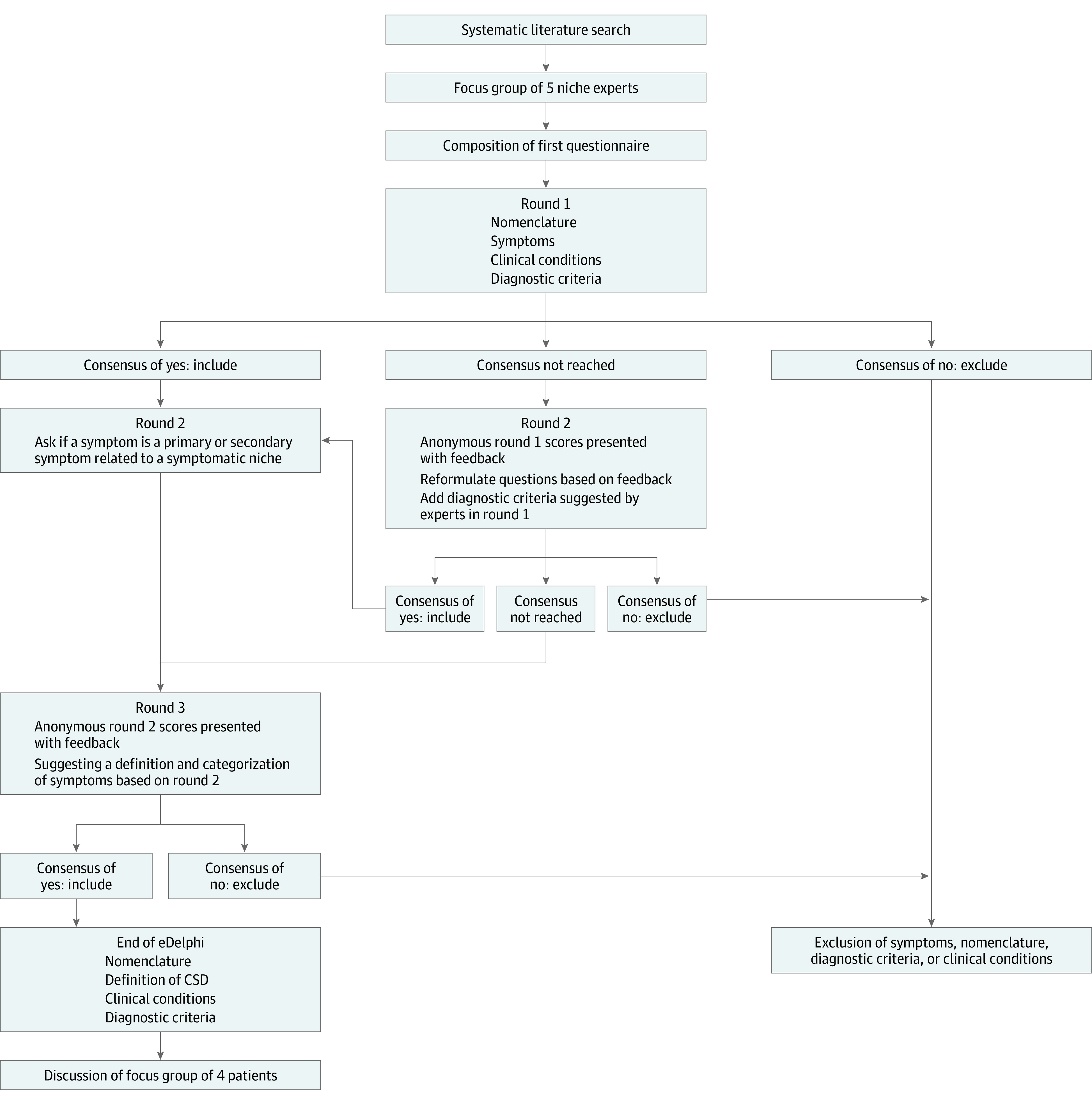
Items were accepted if consensus agreement of at least 70% was reached.
Definition of Consensus
Consensus was predefined, in keeping with previously published work,17,18,19 as a Rate of Agreement (RoA) of 70% or greater, where RoA = (agreement – disagreement)/ (agreement + disagreement + neutral) × 100%. The experts who selected “not my expertise” were not included in the RoA calculation for that question. All analyses were done in SPSS version 28 (IBM).
Results
Among the 31 experts who met the inclusion criteria (51.7%), the majority worked in university-affiliated hospitals (28 of 31 participants [90.3%]). Participating experts represented 3 continents and obstetrics (7 of 31 participants [22.6%]), benign gynecology (20 of 31 participants [64.5%]) and fertility (4 of 31 participants [12.9%]) subspecialties. In total, 29 (93.5%) experts completed all rounds. Originally, we invited 57 potential experts to participate; 3 experts were subsequently invited following recommendation by their colleagues. Baseline characteristics are presented in Table 1. A total of 20 of 21 items of the SRQR checklist were met.
Table 1. Demographic Characteristics of Experts Who Responded to the Questionnaires.
| Characteristic | Experts responded in rounds 1 and 2, No. (%) (n = 31) | Experts responded in round 3, No. (%) (n = 29) |
|---|---|---|
| Primary location | ||
| Europe | 24 (77.4) | 22 (75.9) |
| North America | 2 (6.5) | 2 (6.9) |
| Asia | 5 (16.1) | 5 (17.2) |
| Primary subspecialization | ||
| Benign gynecology | 20 (64.5) | 19 (65.5) |
| Fertility | 4 (12.9) | 4 (13.8) |
| Obstetrics | 7 (22.6) | 6 (20.7) |
| Main level of care | ||
| Private clinic | 1 (3.2) | 1 (3.4) |
| Referral center for niche related problems | 2 (6.5) | 2 (6.9) |
| University hospital | 28 (90.3) | 26 (89.7) |
| Niche operations performed a year | ||
| 0-15 | 6 (19.4) | 5 (17.2) |
| 16-30 | 2 (6.5) | 1 (3.4) |
| 31-50 | 6 (19.4) | 6 (20.7) |
| >50 | 9 (29.0) | 9 (31.0) |
| Not applicable | 8 (25.8) | 8 (27.6) |
eDelphi Rounds 1 to 3
In the first round, experts evaluated 29 symptoms potentially associated with a niche, which were identified by the literature search and suggested by the focus group. The process is shown in the Figure. They also assessed 5 potential diagnostic criteria, 5 potential conditions requiring exclusion before a niche could be diagnosed, and 2 questions about niche nomenclature. All experts participated in the first and second rounds. Twenty-nine experts (93.5%) participated in the third round, after which consensus was reached for the classification on all symptoms and nomenclature. Detailed round-by-round consensus results can be found in the eTable in Supplement 1.
Relevance of the Disorder
There was consensus on the statement that “it is important to differentiate between a sonographic finding of a niche and a condition caused by a niche-related symptoms and the effect on quality of life” (RoA 100%). There was also consensus that the sonographic finding should be defined and evaluated as previously published by Jordans et al2 (ie, an indentation at the site of the CD scar with a depth of at least 2 mm) (RoA 77.8%).
Nomenclature
The preferred term for a niche that caused symptoms was Cesarean Scar Disorder (CSDi) (RoA 96.2%). Other options that were discussed included niche disorder, niche disease, cesarean scar disease and cesarean scar syndrome. The most salient argument that led experts to choose CSDi as the preferred term was that the name implied the origin of the symptoms and emphasized that as an abnormal condition.
Symptoms
During the eDelphi rounds, the desire to classify the symptoms related to a niche emerged. After completion of the final round, consensus was reached (RoA 77.8%) defining a CSDi as a condition that includes at least 1 primary or 2 secondary symptoms in combination with a sonographic finding of a niche, according to the definition by Jordans et al.2 Table 2 outlines the primary and secondary niche-related symptoms, with the corresponding RoA.
Table 2. Consensus-Based Definition of Primary and Secondary Symptoms of Cesarean Scar Disorder.
| Primary symptom/problems | RoA, % | Secondary symptoms | RoA, % |
|---|---|---|---|
| Postmenstrual spotting | 80.6 | Dyspareunia | 72.7 |
| Pain during uterine bleeding | 84.2 | Abnormal vaginal discharge | 87.5 |
| Technical issues with catheter insertion during embryo transfer | 73.1 | Chronic pelvic pain | 87.1 |
| Secondary unexplained infertility combined with intrauterine fluid | 70.4 | Avoiding sexual intercourse | 90.3 |
| NA | NA | Odor associated with abnormal blood loss | 83.4 |
| NA | NA | Secondary unexplained infertility | 70.0 |
| NA | NA | Secondary infertility despite ART | 72.4 |
| NA | NA | Negative self-image | 88.0 |
| NA | NA | Discomfort during participation in leisure activities | 77.3 |
Abbreviations: ART, assisted reproductive technology; NA, not applicable; RoA, rate of agreement.
The experts concluded that obstetrical issues related to a niche, such as a Cesarean Scar Pregnancy, uterine dehiscence/rupture, or placenta accreta spectrum should be reported as complications of the CSDi (RoA 70.4%) and should not be classified as a primary or secondary symptom. Experts agreed that there was insufficient literature to determine whether a miscarriage in patients with a niche should be classified as a symptom related to the CSDi or that it should be considered as an independent problem with a different cause (RoA 96.7%). This was identified as a relevant knowledge gap that requires additional research before it can be considered in future updates of the CSDi definition, which should be reevaluated after 1 year.
Diagnostic Criteria and Conditions to Exclude
Before a symptom-based diagnosis of CSDi can be made, experts agreed that certain minimum criteria should be met. These included a minimum of 3 regular menstrual cycles after a CD before diagnosis (RoA 93.5%); a patient needing to be premenopausal (RoA 100%); and the complaints of a symptomatic niche starting after a CD or significantly worsening after a CD (RoA 80.6%). Consensus was also reached about a statement that a patient can be cured from a symptomatic niche, however this does not mean that all symptomatic niches should be treated (RoA 87.1%). Experts also felt that before confirming a diagnosis of CSDi, certain conditions should be excluded, including cervical dysplasia (RoA 74.2%), vaginal or uterine infections (RoA 74.2%), other uterine intracavitary pathology (RoA 93.5%), anovulatory cycles (RoA 100%), or other causes of postmenstrual spotting (RoA 80.6%) (Table 3).
Table 3. Criteria Required for Diagnosis of Cesarean Scar Disorder and Conditions That Should Be Ruled Out Before Confirming the Diagnosis.
| Diagnostic criteria | RoA, % | Conditions to exclude | RoA, % |
|---|---|---|---|
| Minimum of 3 regular menstrual cycles after CD before diagnosis can be made | 93.5 | Cervical dysplasia | 74.2 |
| A patient needs to be premenopausal | 100 | Vaginal/uterine infections | 74.2 |
| The complaints of a symptomatic niche should start after a CD or should worsen significantly after a CD | 80.6 | Other uterine intracavitary pathology | 93.5 |
| A patient can be cured from a symptomatic niche (this does not mean that all symptomatic niche should be treated) | 87.1 | Other causes of postmenstrual spotting (such as continuous oral contraceptive use or intrauterine device) | 80.6 |
| NA | NA | Anovulatory cycles | 100 |
Abbreviations: CD, cesarean delivery; NA, not applicable; RoA, rate of agreement.
Patient Representative Endorsement
In total 4 patient representatives participated in the online meeting to provide input on the relevance, clarity of the consensus statements, and suggested possible missing items from a patients’ perspective. All patient representatives agreed with the proposed definition and suggested no additional terms from their perspective. They approved the intended revision after 1 year. They underlined the need for clear diagnostic criteria and urged the development of clinical guidelines on diagnosis and therapy to guide clinicians in the management of CSDi.
Discussion
Main Findings
In this modified Delphi study, international experts specializing in the management of CD niche agreed that the constellation of symptoms resulting from a CD niche should be termed Cesarean Scar Disorder (CSDi). The agreed definition for CSDi was at least 1 primary or 2 secondary symptoms in the presence of a sonographic finding of a niche, according to the definition by Jordans et al2 (ie, an indentation at the site of the CD scar with a depth of at least 2 mm). CSDi is a condition that affects premenopausal women who are symptomatic for at least 3 months following their CD. This definition helps to discriminate between a sonographic finding and a relevant condition that impacts quality of life. Experts also emphasized that before a diagnosis of CSDi is made, certain conditions must be excluded (eg, cervical dysplasia, infection, uterine cavity pathology, or abnormal uterine bleeding from ovulatory or other iatrogenic causes).
Clinical Implications
The ability to diagnose CSDi is of great clinical value. It is important to state that a diagnosis of CSDi does not necessarily mean that treatment is indicated. The decision to investigate and treat CSDi is influenced by the symptom burden, impact on quality of life, size of the niche, and the individualized expectations of the patient.
This consensus by international experts and patients to formally recognize a disorder caused by a CD niche creates for the first time a medical condition, with specific diagnostic and exclusion criteria. This will have significant ramifications for various groups. First, it will allow patients to be recognized and their symptoms to be taken seriously. It will also enable them to advocate for themselves as we already know the burden that niche-related symptoms can have on patients’ emotional, physical, and social quality of life.8 Second, by formally creating and recognizing a specific disorder, along with associated inclusion and exclusion criteria, it provides an opportunity for frontline women’s health physicians to be educated about this issue and consequently improve the care they provide for these patients. Lastly, this newly agreed upon entity of CSDi and its clear definition will facilitate standardization of care and niche-related research. It will therefore be useful for the development of future systematic reviews, meta-analyses and guidelines. Hopefully these all will prevent both the over- and undertreatment of CD niches.
Although surgical management of CSDi has been investigated in an RCT for the amelioration of abnormal uterine bleeding,20 data for treating other niche-related symptoms is very scarce.21 Currently 1 RCT22 has been registered that compares the effect of a laparoscopic niche resection vs expectant management in infertile women with a large niche, and an RCT23 that evaluates the effect of a laparoscopic niche resection compared with hormonal treatment in women with niche-related spotting complaints is underway as well. With respect to hysteroscopic niche resection, 1 study evaluated the effect on clinical pregnancy rate in 61 secondary infertile patients and showed superiority of the hysteroscopic niche resection compared with expectant management.24 As part of good clinical practice, other conditions should be considered as a part of differential diagnosis dependent on the patients’ symptoms, such as the presence of adenomyosis or deep endometriosis in women with dysmenorrhea. Additionally, imaging, dynamic ultrasound,25 or MRI can help to differentiate between these disorders.
A CSDi is an iatrogenic consequence of a CD. However, current international guidelines on Cesarean deliveries do not include information on the potential development of niche-related symptoms such as postmenstrual spotting or niche-related fertility problems after a CD.26,27 Given the high incidence of these problems and the acknowledged relevance by both patients and experts, we propose to inform patients on the possibility of developing CSDi after a CD. In addition, more attention should be given by clinicians to women who report these symptoms after a CD. The agreed upon nomenclature, definitions, and criteria for CSDi will increase awareness of these problems both by women and clinicians. Furthermore, as discussed before, it may also contribute to the development of evidence-based guidelines that may prevent both over- and under treatment.
Comparison to Other Literature
Although the number of published studies on CD niche–related issues and applied therapies has increased over the last decade, to the best of our knowledge, there is no uniform, international definition of a disorder caused by a symptomatic niche. In the literature different terms are used, such as isthmocele,28 cesarean scar syndrome,29 cesarean scar defect,6,30 or even CD disorder.31 However, none of the studies reported a clear definition or diagnostic criteria.
The results of this study are intended to guide appropriate clinical decision-making and the unambiguous inclusion of women in niche-related research. However, using 1 primary or 2 secondary symptoms as diagnostic criteria has not been clinically tested. We realize that there is currently no information on the weight of individual symptoms or classification of their clinical implications. We would like to stress that the proposed definition of CSDi and related diagnostic criteria are only a starting point and that the relevance of the number and weight of these symptoms should be assessed in future studies. This is in line with the development of the definitions of many other disorders. As an example, current polycystic ovary syndrome (PCOS) criteria evolved over many years with the diagnosis changing over time as new information became available.32
Strengths and Limitations
The most important strength of our study is the use of a Delphi technique. This procedure allows multiple experts to discuss and consent to complex questions, with the assurance of anonymity and the benefit of equal input in the final consensus statement. Another strength was the rigorous systematic review of the literature that guided the creation of the first questionnaire and to guide experts in the first Delphi round.9 Additionally, the expert panel was diverse in subspecialization, country of origin, and expertise.
Our results should be interpreted in the context of the study design. Although we tried to define preselected criteria, we appreciate that there will be a selection bias according to the experts approached to participate and that not all countries are represented. Furthermore, in the focus group to design the first questionnaire, only Dutch experts participated, which may have influenced the content of the first questionnaire. For this reason, international experts were encouraged to add free text in each round on topics or items that may have been missed. Another consideration with our findings is that due to the novelty of this subject there is an exponential growth of literature on this topic, with addition of new findings continuously. For these reasons, we encourage this definition to be revisited regularly in a context that includes more experts and incorporates the latest data and findings on the topic with validation using diverse patient groups. The ethno-cultural impact of niche-related symptoms is an important consideration as the definition of CSDi is applied worldwide.
Conclusion
In this modified Delphi study, criteria for a cesarean scar disorder were defined as a condition with at least 1 primary or 2 secondary symptoms in association with a niche in the uterine CD scar. Our study should be considered a good starting point that aims to develop future guidelines to give women with a CSDi the recognition and care they need.
eAppendix. Search Strategy
eFigure. Flowchart Showing Studies Identified Through Literature Search
eTable. Results of Consensus Rounds
Nonauthor Collaborators. The CSDi Study Group
Data Sharing Statement
References
- 1.Sung S, Mahdy H. Cesarean Section. StatPearls; 2022. [PubMed] [Google Scholar]
- 2.Jordans IPM, de Leeuw RA, Stegwee SI, et al. Sonographic examination of uterine niche in non-pregnant women: a modified Delphi procedure. Ultrasound Obstet Gynecol. 2019;53(1):107-115. doi: 10.1002/uog.19049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.van der Voet LF, Bij de Vaate AM, Veersema S, Brölmann HA, Huirne JA. Long-term complications of caesarean section. The niche in the scar: a prospective cohort study on niche prevalence and its relation to abnormal uterine bleeding. BJOG. 2014;121(2):236-244. doi: 10.1111/1471-0528.12542 [DOI] [PubMed] [Google Scholar]
- 4.Stegwee SI, Jordans IPM, van der Voet LF, et al. Single- versus double-layer closure of the caesarean (uterine) scar in the prevention of gynaecological symptoms in relation to niche development - the 2Close study: a multicentre randomised controlled trial. BMC Pregnancy Childbirth. 2019;19(1):85. doi: 10.1186/s12884-019-2221-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bij de Vaate AJ, van der Voet LF, Naji O, et al. Prevalence, potential risk factors for development and symptoms related to the presence of uterine niches following Cesarean section: systematic review. Ultrasound Obstet Gynecol. 2014;43(4):372-382. doi: 10.1002/uog.13199 [DOI] [PubMed] [Google Scholar]
- 6.Wang L, Wang J, Lu N, Liu J, Diao F. Pregnancy and perinatal outcomes of patients with prior cesarean section after a single embryo transfer in IVF/ICSI: a retrospective cohort study. Front Endocrinol (Lausanne). 2022;13:851213. doi: 10.3389/fendo.2022.851213 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Vissers J, Sluckin TC, van Driel-Delprat CCR, et al. Reduced pregnancy and live birth rates after in vitro fertilization in women with previous Caesarean section: a retrospective cohort study. Hum Reprod. 2020;35(3):595-604. doi: 10.1093/humrep/dez295 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Stegwee SI, Hehenkamp WJK, de Leeuw RA, de Groot CJM, Huirne JAF. Improved health-related quality of life in the first year after laparoscopic niche resection: a prospective cohort study. Eur J Obstet Gynecol Reprod Biol. 2020;245:174-180. doi: 10.1016/j.ejogrb.2020.01.003 [DOI] [PubMed] [Google Scholar]
- 9.Stegwee SI, Beij A, de Leeuw RA, Mokkink LB, van der Voet LF, Huirne JAF. Niche-related outcomes after caesarean section and quality of life: a focus group study and review of literature. Qual Life Res. 2020;29(4):1013-1025. doi: 10.1007/s11136-019-02376-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Donnez O. Cesarean scar defects: management of an iatrogenic pathology whose prevalence has dramatically increased. Fertil Steril. 2020;113(4):704-716. doi: 10.1016/j.fertnstert.2020.01.037 [DOI] [PubMed] [Google Scholar]
- 11.Mashiach R, Burke YZ. Optimal isthmocele management: hysteroscopic, laparoscopic, or combination. J Minim Invasive Gynecol. 2021;28(3):565-574. doi: 10.1016/j.jmig.2020.10.026 [DOI] [PubMed] [Google Scholar]
- 12.Vitale SG, Ludwin A, Vilos GA, et al. From hysteroscopy to laparoendoscopic surgery: what is the best surgical approach for symptomatic isthmocele? A systematic review and meta-analysis. Arch Gynecol Obstet. 2020;301(1):33-52. doi: 10.1007/s00404-020-05438-0 [DOI] [PubMed] [Google Scholar]
- 13.Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000;32(4):1008-1015. [PubMed] [Google Scholar]
- 14.Jones J, Hunter D. Consensus methods for medical and health services research. BMJ. 1995;311(7001):376-380. doi: 10.1136/bmj.311.7001.376 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245-1251. doi: 10.1097/ACM.0000000000000388 [DOI] [PubMed] [Google Scholar]
- 16.Niche of niche zwangerschap. 2022. Accessed October 5, 2022. https://www.facebook.com/groups/1315558241877808
- 17.Jordans IPM, Verberkt C, De Leeuw RA, et al. Definition and sonographic reporting system for Cesarean scar pregnancy in early gestation: modified Delphi method. Ultrasound Obstet Gynecol. 2022;59(4):437-449. doi: 10.1002/uog.24815 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Janssen PF, Brölmann HA, Huirne JA. Recommendations to prevent urinary tract injuries during laparoscopic hysterectomy: a systematic Delphi procedure among experts. J Minim Invasive Gynecol. 2011;18(3):314-321. doi: 10.1016/j.jmig.2011.01.007 [DOI] [PubMed] [Google Scholar]
- 19.Sadi J, Torchia E, Faber KJ, et al. Posterior shoulder instability classification, assessment, and management: an international delphi study. J Orthop Sports Phys Ther. 2020;50(7):373-380. doi: 10.2519/jospt.2020.9225 [DOI] [PubMed] [Google Scholar]
- 20.Vervoort A, van der Voet LF, Hehenkamp W, et al. Hysteroscopic resection of a uterine caesarean scar defect (niche) in women with postmenstrual spotting: a randomised controlled trial. BJOG. 2018;125(3):326-334. doi: 10.1111/1471-0528.14733 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Verberkt C, Klein Meuleman SJM, Ket JCF, et al. Fertility and pregnancy outcomes after a uterine niche resection in women with and without infertility: a systematic review and meta-analysis. F S Rev. 2022;3(3):174-189. doi: 10.1016/j.xfnr.2022.05.003 [DOI] [Google Scholar]
- 22.Huirne JAF. LAPRESS study. February 20, 2017. Updated August 18, 2022. Accessed February 23, 2023. https://www.clinicaltrialregister.nl/nl/trial/28650
- 23.Huirne JAF. Symptomatic niches for laparoscopic niche resection, a randomized clinical trial. June 11, 2021. Accessed February 23, 2023. https://trialsearch.who.int/Trial2.aspx?TrialID=NL9534
- 24.Abdou AM, Ammar IMM. Role of hysteroscopic repair of cesarean scar defect in women with secondary infertility. Middle East Fertil Soc J. 2018;23(4):505-509. doi: 10.1016/j.mefs.2018.06.005 [DOI] [Google Scholar]
- 25.Harmsen MJ, Van den Bosch T, de Leeuw RA, et al. Consensus on revised definitions of Morphological Uterus Sonographic Assessment (MUSA) features of adenomyosis: results of modified Delphi procedure. Ultrasound Obstet Gynecol. 2022;60(1):118-131. doi: 10.1002/uog.24786 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.ACOG Committee Opinion No . ACOG committee opinion no. 761: cesarean delivery on maternal request. Obstet Gynecol. 2019;133(1):e73-e77. doi: 10.1097/AOG.0000000000003006 [DOI] [PubMed] [Google Scholar]
- 27.National Institute for Health and Care Excellence . Caesarean birth (NICE guideline 192). Accessed February 16, 2023. https://www.nice.org.uk/guidance/ng192/chapter/Recommendations#benefits-and-risks-of-caesarean-and-vaginal-birth
- 28.Raimondo G, Grifone G, Raimondo D, Seracchioli R, Scambia G, Masciullo V. Hysteroscopic treatment of symptomatic cesarean-induced isthmocele: a prospective study. J Minim Invasive Gynecol. 2015;22(2):297-301. doi: 10.1016/j.jmig.2014.09.011 [DOI] [PubMed] [Google Scholar]
- 29.Tsuji S, Takahashi A, Higuchi A, et al. Pregnancy outcomes after hysteroscopic surgery in women with cesarean scar syndrome. PLoS One. 2020;15(12):e0243421. doi: 10.1371/journal.pone.0243421 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wang CB, Chiu WW, Lee CY, Sun YL, Lin YH, Tseng CJ. Cesarean scar defect: correlation between Cesarean section number, defect size, clinical symptoms and uterine position. Ultrasound Obstet Gynecol. 2009;34(1):85-89. doi: 10.1002/uog.6405 [DOI] [PubMed] [Google Scholar]
- 31.Thurmond AS, Harvey WJ, Smith SA. Cesarean section scar as a cause of abnormal vaginal bleeding: diagnosis by sonohysterography. J Ultrasound Med. 1999;18(1):13-16. doi: 10.7863/jum.1999.18.1.13 [DOI] [PubMed] [Google Scholar]
- 32.Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group . Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. 2004;81(1):19-25. doi: 10.1016/j.fertnstert.2003.10.004 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eAppendix. Search Strategy
eFigure. Flowchart Showing Studies Identified Through Literature Search
eTable. Results of Consensus Rounds
Nonauthor Collaborators. The CSDi Study Group
Data Sharing Statement