

Abstract
Background
Benign metastasizing leiomyoma (BML) is a rare disease usually observed in women of reproductive or premenopausal age with a history of uterine myomectomy or hysterectomy. The most common sites of metastases are the pulmonary, and other sites include heart, bones, liver, lymph nodes, bladder, skeletal muscles, and central nervous system. Here, we report a case of a 50 year-old woman with a history of hysterectomy who was initially suspected of uterine sarcoma but was finally confirmed to have BML with lung and lymph node metastases, and discuss the treatment and prognosis of BML.
Case presentation
A 50 year-old woman with a history of total abdominal hysterectomy presented with mild but persistent abdominal pain for more than 3 months. She was suspected of having uterine sarcoma before surgery and laparoscopic extensive debulking surgery including bilateral oophorectomy, pelvic and para-aortic lymph node dissection to the level of the left renal vein, and transcutaneous dissection of the right inguinal lymph nodes. Pathology confirmed a benign leiomyoma, and the patient was diagnosed with BML. No medication was administered after the surgery, and the follow-up was of no significance.
Conclusion
Benign metastasizing leiomyoma (BML) is a rare disorder in which histologically benign smooth muscle tumors metastasize to extrauterine sites. Metastases are commonly observed in the lung, liver, lymph nodes, skin, bladder, esophagus, and skeletal muscles. BML is usually misdiagnosed as a malignant tumor before surgery until the pathology confirms its benign nature. However, this treatment remains controversial and undetermined. The prognosis is usually favorable owing to its benign nature.
Keywords: Benign metastasizing leiomyoma, Lymph node, Pulmonary metastases, Case report
Background
Benign metastasizing leiomyoma (BML) is a rare disorder that occurs mainly in women of reproductive or premenopausal age with a history of uterine myomectomy or hysterectomy. Histologically, BML is a benign tumor that originates from smooth muscle cells that metastasize to extrauterine sites. The most common sites of metastases are the pulmonary, and other sites include heart, bones, liver, lymph nodes, skin, bladder, esophagus, skeletal muscles, and central nervous system [1–11]. Multiple metastases simultaneously, including lymph node metastases in BML, are extremely rare, and studies on the prognosis and treatment of BML with multiple lymph node metastases are scarce. Here, we report a case of BML with simultaneous pulmonary and lymph node metastases at the same time and discuss the clinical and radiologic features of BML.
Case presentation
A 50 year-old woman with no significant medical history (parity 2-0-0-2, both normal spontaneous vaginal deliveries) presented with mild but persistent abdominal pain for over 3 months. She underwent abdominal total hysterectomy and bilateral salpingectomy for uterine leiomyoma at a local secondary hospital in January 2019. Pathological examination revealed benign leiomyoma. The post-operative Regular follow-up was not significant. However, she experienced persistent lower abdominal pain in the past 3 months but did not suffer from weight loss or any other respiratory symptoms such as hemoptysis, purulent sputum, or exertional dyspnea. Ultrasound at a local clinic revealed a heterogeneous solid mass measuring 4 cm in diameter in the central pelvis. She was referred to the International Peace Maternity and Child Health Hospital for further work.
Routine laboratory tests showed that the values for biochemical variables, including tumor markers such as alpha-fetoprotein, cancer antigen 19‑9, and cancer antigen 125, were within the normal ranges. Pelvic magnetic resonance imaging (MRI) revealed solid pelvic masses in the central and bilateral pelvis, and enlargement of multiple lymph nodes around the iliac chain and aorta. On chest CT, there were multiple well-circumscribed nodules in the bilateral pulmonary arteries, with the largest nodule 1.5 cm in diameter (Fig. 1). An original pathology slide review and positron emission tomography (PET)-CT were done. According to the original slide review, it was a benign leiomyoma with a mitotic count of < 5/10 high-power fields (HPF), little cytological atypia, and no tumor cell necrosis, but with cellular abundance. Abnormal fluorodeoxyglucose (FDG) uptake in the bi-adnexal mass with the suspicion of para-aortic, aorto-caval, precaval, external iliac, and bilateral inguinal lymph node metastases was found on PET-CT (Fig. 2). Multiple nodules in both lungs without abnormal FDG uptake were considered metastatic cancers. An additional chest computed tomography (CT) scan revealed metastatic lung cancer. Considering the patient’s history of gynecologic surgery, pelvic malignancy of unknown origin was suspected. In December 2020, laparoscopic extensive debulking surgery, including bilateral oophorectomy, pelvic and para-aortic lymph node dissection to the level of the left renal vein, and right inguinal lymph node dissection, was performed. Grossly, there were masses 5 cm in size on the left-side stump of the vagina and along the right pelvic infundibular ligament to the level of the renal vein, measuring 10 × 4 cm (Figs. 3 and 4). All lymph nodes stated above, including the para-aortic, aorto-caval, precaval, and pelvic lymph nodes, were enlarged to approximately 0.5–3 cm in size. The right inguinal lymph nodes were palpable, enlarged to 3 cm in size, and dissected (Fig. 5).
Fig. 1.
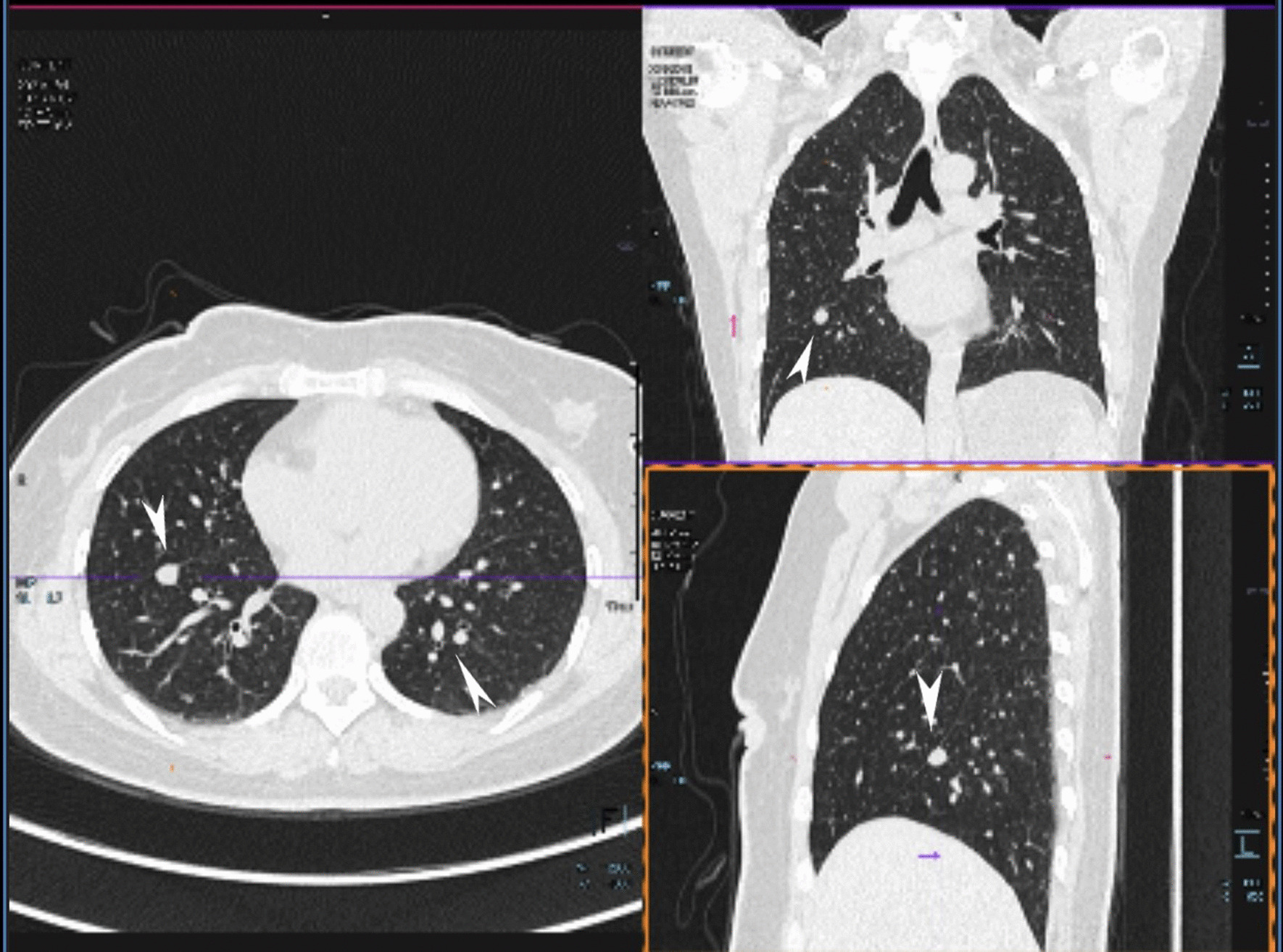
Multiple metastasis in the bilateral lungs (see arrow)
Fig. 2.

Multiple metastasis in pelvic, along post cava and the right inguinal lymph nodes (a Tumor along the right pelvic infundibular ligament; b Retroperitoneal tumor of left pelvic; c Enlarged lymph nodes of right inguinal)
Fig. 3.
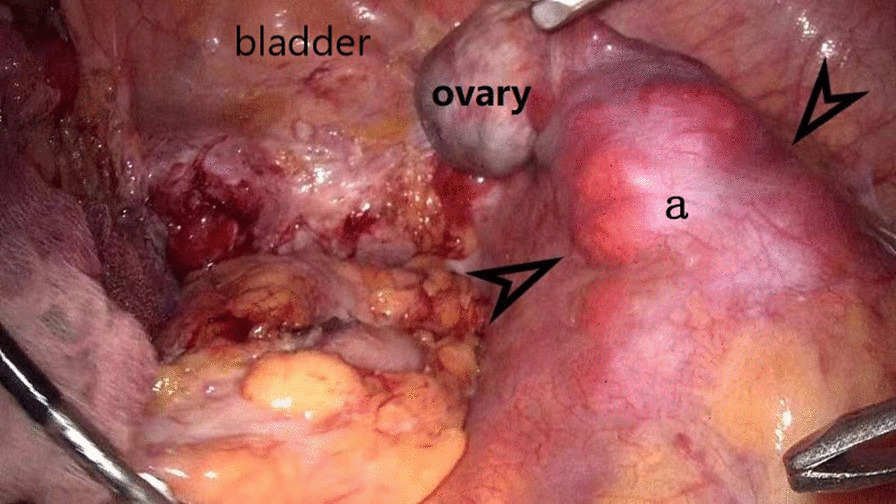
Leiomyoma metastasis along the post cava seen in the laparoscopic surgery (a tumor along the right pelvic infundibular ligament to the level of renal vein)
Fig. 4.
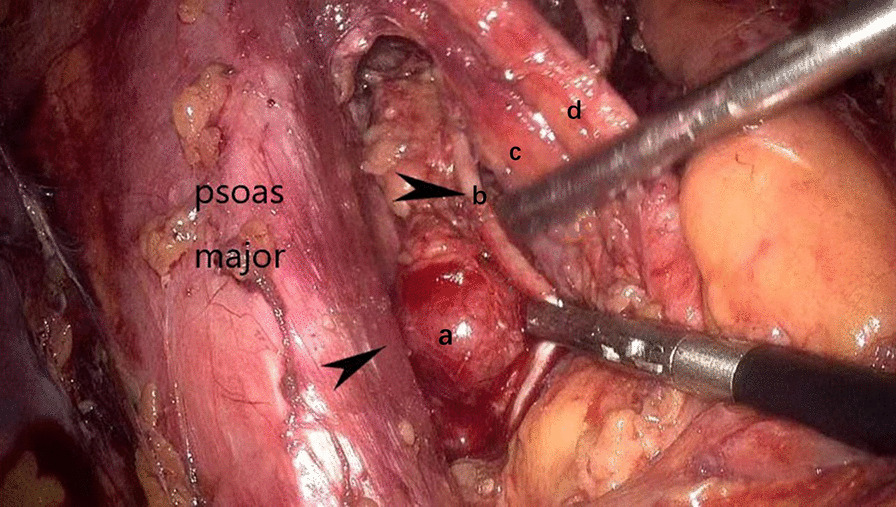
Leiomyoma metastasis to the internal iliac lymph nodes seen in the laparoscopic surgery (a Enlarged left internal iliac lymph nodes; b Left obturator nerve; c Vena iliaca externa; d External iliac artery)
Fig. 5.
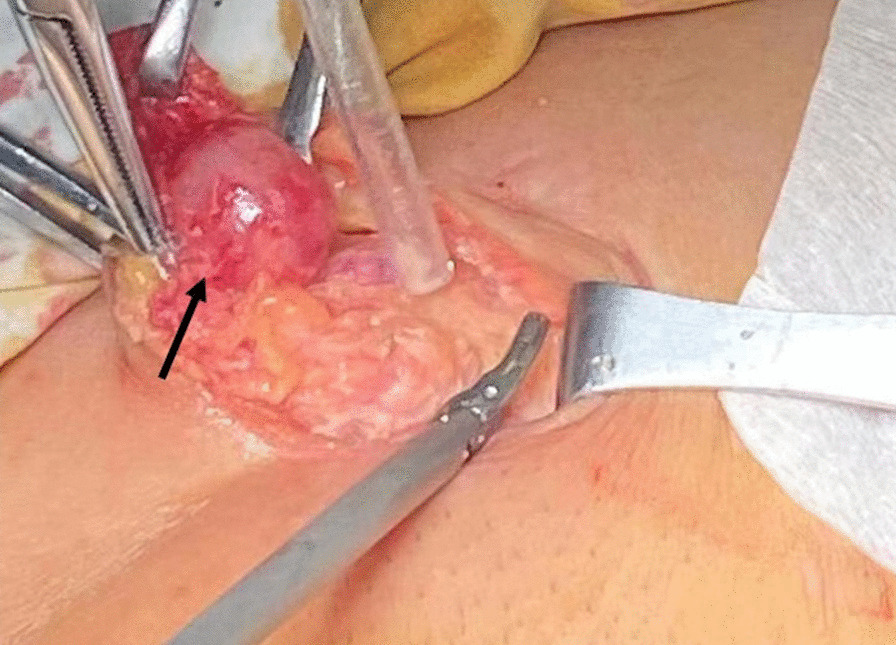
Tumor metastasis to the right inguinal lymph nodes (see arrow)
Pathology of the pelvic masses also revealed benign leiomyoma with mitosis < 5/10 HPF, little cytological atypia, and no tumor necrosis, but with cellular abundance and a few singular kernels (Fig. 6). Metastases to the meso-ovarium, bilateral pelvic infundibular ligaments, pelvic lymph nodes, para-aortic lymph nodes, and bilateral inguinal lymph nodes were confirmed in the final pathology report. Metastatic lesions were also reported to have a histology similar to that of the original mass with a mitotic count < 2/10 HPF, little cytological atypism, and no necrosis. On immunohistochemical staining, cells were all positive for estrogen/progesterone receptors, p53, SMA+, HMB45-, Ki67(5%), CD31, and ERG. Clinicopathologically, BML was selected as the final diagnosis after discussion with our pathologists. The patient was discharged from the hospital on post-operative day 7 without any early post-operative complications. No specific treatments were administered. Her current general condition was satisfactory without any postoperative complications. However, long-term follow-up is required to assess disease recurrence and distant metastasis.
Fig. 6.
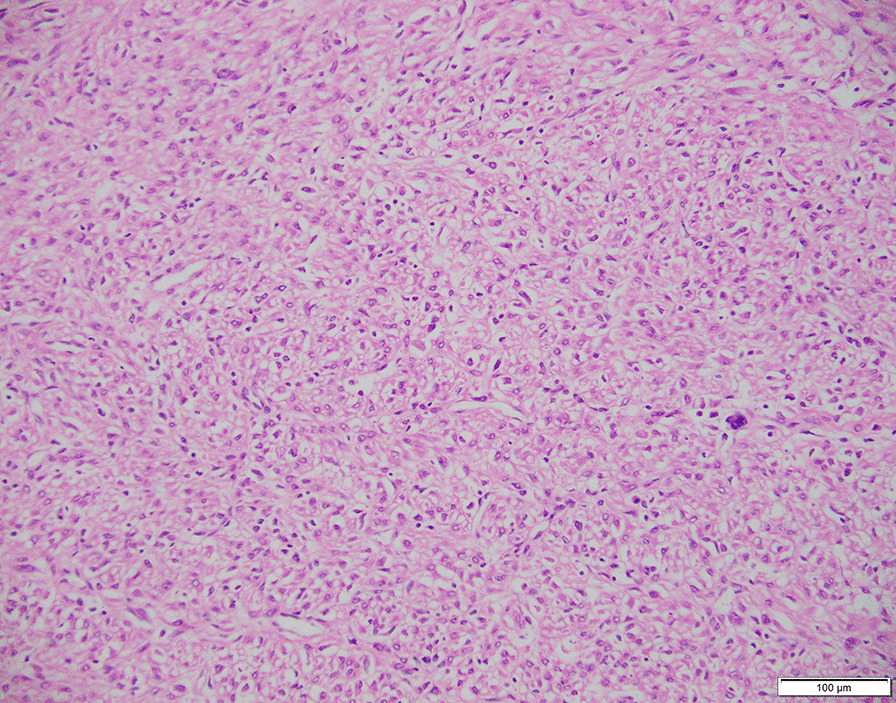
Hematoxylin and eosin (HE) staining of the pelvic tumor specimen
Discussion and conclusions
Benign metastasizing leiomyoma (BML) is a rare disorder in which histologically benign smooth muscle tumors metastasize to extrauterine sites [12]. In 1939 Steiner [13] first reported it as a fibroleiomyomatous hamartoma. Approximately 150 cases of BML have been reported in literature.
The disease commonly occurs in women of late reproductive or premenopausal age, most of whom have a history of leiomyomas treated surgically with myomectomy or hysterectomy [14]. The most frequent site of metastasis was the lungs (80%). Metastases to other organs reported to date include the heart (approximately 10 cases), liver, lymph nodes, skeletal muscle, skin, esophagus, and central nervous system. Multiple metastases, including to lymph nodes, are extremely rare, as reported in this case. BML with lymph node metastasis reported in the literature are shown in Table 1.
Table 1.
Summary of BML cases with lymph nodes metastasis
| Metastasis | Age | History of gynecologic surgery | Surgical treatment |
|---|---|---|---|
| Lymph nodes only | 52 [15] | N/A | Total abdominal hysterectomy, bilateral salpingo-oophorectomy, and lymphadenectomy |
| 27 [16] | N/A | N/A | |
| 69 [17] | N/A | Complete inguinal lymph node excision | |
| 32 [18] | N/A | N/A | |
| Lymph nodes and biceps | 47 [19] | Hysterectomy 2 years earlier | Open laparotomy and extirpation of the abdominal tumors |
| Lymph nodes/retroperitoneal mass and pulmonary | 48 [20] | Myomectomy 20 years earlier and then a total abdominal hysterectomy 8 years later | Retroperitoneal mass excision and bilateral salpingo-oophorectomy |
| 34 [10] | Abdominal myomectomy 1 year earlier | Extensive debulking surgery including total abdominal hysterectomy, bilateral salpingo-oophorectomy, pelvic and paraaortic lymph node dissection to the level of the left renal vein, and gonadal lymph node dissection | |
| 50 [21] | Cesarean sections 16, 13 and 11 years previously | A total abdominal hysterectomy bilateral salpingo-oophorectomy and a dissection of the pelvic and para-aortic lymph nodes | |
| Multiple metastasis (lung, skin, lymph nodes, bone and perhaps the brain) | 55 [22] | 14 years after uterine myomectomy | N/A |
The pathological origin of BML remains unclear and controversial. Several hypotheses have been proposed: (i) mechanical dissemination or intravascular metastases of smooth muscle cells from the uterus to distant locations, (ii) derivation from multifocal but independent smooth muscle proliferation, and (iii) derivation from low-grade leiomyosarcoma [23, 24]. The most commonly accepted theory is the hematogenous spread of a monoclonal element in a benign smooth muscle tumor. Chromosomal abnormalities can be found in 25% of such tumors, including balanced translocation, trisomy 12, or rearrangement of 6p [25, 26]. Other possible mechanisms include lymphovascular embolization, mesothelial mesenchymal metaplasia, and metastases from misdiagnosed low-grade uterine leiomyosarcomas [27, 28].
Histologically, BML has been mainly associated with leiomyomas; however, the type of leiomyoma is not yet clear (eg. Cellular, hemorrhagic cellular, mitotically active, atypical, myxoid, vascular, epithelioid, or lipoleiomyoma). Some studies suggest that BML is a low-grade endometrial stromal sarcoma or malignant uterine leiomyoma, but the evidence supporting these concepts is not very strong.
On imaging examination, such as CT scans of the lungs, BML present as well-circumscribed nodules in the lungs. Bilateral lung nodules are more commonly observed than multiple unilateral lesions or solitary nodules. The nodules of BML can be large or small and cavitate, which can lead to thin-walled or thick-walled cysts [29].
For PET-CT scans, some authors propose that 18‑FDG‑PET/CT is useful for distinguishing malignant leiomyosarcoma from benign leiomyoma, as a number of reports have demonstrated that there is a lack of 18‑FDG uptake in PBML [30]. The SUV of leiomyosarcoma were significantly greater than those of leiomyoma. However, there are numerous reports of 18‑FDG‑avid leiomyoma. Theoretically, PET-CT with 18F–FDG is helpful in assessing the significant metabolic activity of both pulmonary and extra-pulmonary nodules, which should be unexpected in BML and otherwise would raise concern for malignant disease [31, 32]. As in our case, the PET-CT of the patient showed 18-FDG-avid lymph node metastases and lack of 18-FDG uptake in pulmonary lesions, which should raise the concern for the diagnosis of BML.
The immunohistochemical profile of BML is positive for actin, desmin, and smooth muscle actin and has low Ki-67 expression (< 5%) [33], and is difficult to distinguish from primary uterine leiomyoma. High levels of the tumor suppressor gene p53 have also been found in BML lesions; however, its role in pathogenesis has not been clarified.
In theory, BML is estrogen and progesterone receptor positive, and estrogen is known to stimulate tumor growth, while progesterone is known to inhibit tumor growth [34]. However, in a few cases, BML cells were found to lack estrogen or progesterone receptors, suggesting that the site of origin was not the uterus. Another possible explanation is that these receptors are downregulated. Genetic studies have shown that BML is clonal in origin. Most BML lesions have been reported to be nonreactive to the antibody HMB-45, which recognize Pmel17, a melanosomal protein expressed in lung hamartomas, PEComas, and LAM; however, BML lesions may also show low reactivity.
Most patients with BML present with multiple pulmonary nodules, which usually develop after myomectomy or hysterectomy for the treatment of uterine fibroids. To date, there are no standard clinical criteria for diagnosing BML. In many cases, BML lung metastases are asymptomatic. Lung biopsies have been used to confirm the diagnosis of BML and rule out malignant tumors. For lymph node metastases of BML, as in our case, leiomyomatosis must be distinguished from several other spindle cell tumors involving the lymph nodes (primarily or secondary), such as Kaposi’s sarcoma, dendritic reticulum cell tumor, intranodal neurilemmoma, and metastatic spindle cell tumor.
Careful history taking and physical examination are useful to rule out many of the listed disorders, and another common differential diagnosis is pulmonary lymphangioleiomyomatosis (LAM). Pulmonary LAM is a rare slowly progressive lung disease that affects almost exclusively young women of reproductive age [35]. It is caused by mutations in the tuberous sclerosis genes [36] and characterized by cystic remodeling of the lung parenchyma. The most common clinical manifestations are progressive dyspnea on exertion, pneumothorax and chylous effusions. On the other hand, lack of systemic symptoms or no symptoms, along with a history of uterine fibroids or prior uterine surgery, is highly suggestive of BML. CT imaging of the chest and abdomen may suggest malignancy or infection. Ultimately, a histological diagnosis is required to rule out the diagnoses listed above and establish the diagnosis of BML. This may consist of lung biopsy and lesion resection.
Given the rarity of this disease, no standardized treatment for BML has been proposed. Several suggestions published in the literature include regular and careful observation, surgical resection with oophorectomy, progesterone therapy, and medical castration using aromatase inhibitors, estrogen receptor blockers (e.g., tamoxifen and raloxifene), tyrosine kinase inhibitors (e.g., imatinib), and GnRH agonists [37, 38]. Jennifer et al. [12] reported a case of pelvic leiomyoma with lung metastases in a patient who underwent bi-salpingo-oophorectomy and opted for HRT after surgery. Thoracic CT tomography showed an enlarged pulmonary nodule, and HRT was stopped. Letrozole was administered by a gynecologic oncologist for a slightly enlarged lung nodule on CT surveillance. Two years later, surveillance imaging confirmed the stability of the pulmonary BML, and the patient remained asymptomatic. This implies that the impact of estrogen on the tumor and HRT treatment should be carefully assessed before administration to the patient. Careful follow-up was also indicated. In our case, the patient underwent bi-oophorectomy and no special treatment was administered. Follow-up until now has been uneventful.
The reported prognosis of patients with BML is favorable. Pulmonary lesions are usually discovered several years (months to more than 30 years) after hysterectomy or myomectomy, and the growth rate of these tumors is slow. Although lung BML is rare and simultaneous metastases of the retroperitoneal lymph nodes after previous hysterectomy or myomectomy are even rarer, such patients are suggested to have prolonged surveillance and careful follow-up for early detection of recurrence or distant metastases. As therapeutic options are limited, new drugs or therapeutic strategies should be studied and considered. In addition, long-term follow-up may be useful in studying their implications in clinical practice.
Acknowledgements
Not applicable.
Abbreviations
- BML
Benign metastasizing leiomyoma
- MRI
Magnetic resonance imaging
- PET
Positron emission tomography
- HPF
High-power fields
- FDG
Fluorodeoxyglucose
- SUV
Standard uptake value
Author contributions
TT: Writing of manuscript. FQ: Provides case details. LYH: Writing and Editing of the manuscript. WYD: Edited the manuscript. All authors read and approved the final manuscript.
Funding
This research was supported by the Shanghai Key Department of Gynaecologic Oncology.
Availability of data and materials
There was no dataset, as this was a case report. Patient data and details are available upon request by email.
Declarations
Ethics approval and consent to participate
The Institutional Review Board of (International Peace Maternity and Child Health Hospital) approved this study.
Consent for publication
Written informed consent for the publication of clinical data, details, and images was obtained from the patient. A copy of the consent form is available for review by the editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Tong Tong, Email: 18017310267@163.com.
Yudong Wang, Email: wangyudong@shsmu.edu.cn.
References
- 1.Jo JH, Lee JH, Kim DC, Kim SH, Kwon HC, Kim JS, Kim HJ. A case of benign metastasizing leiomyoma with multiple metastasis to the soft tissue, skeletal muscle, lung and breast. Korean J Intern Med. 2006;21(3):199–201. doi: 10.3904/kjim.2006.21.3.199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Arai T, Yasuda Y, Takaya T, Shibayama M. Natural decrease of benign metastasizing leiomyoma. Chest. 2000;117(3):921–922. doi: 10.1378/chest.117.3.921. [DOI] [PubMed] [Google Scholar]
- 3.Kwon YI, Kim TH, Sohn JW, Yoon HJ, Shin DH, Park SS. Benign pulmonary metastasizing leiomvomatosis: case report and a review of the literature. Korean J Intern Med. 2006;21(3):173–177. doi: 10.3904/kjim.2006.21.3.173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rivera JA, Christopoulos S, Small D, Trifiro M. Hormonal manipulation of benign metastasizing leiomyomas: report of two cases and review of the literature. J Clin Endocrinol Metab. 2004;89(7):3183–3188. doi: 10.1210/jc.2003-032021. [DOI] [PubMed] [Google Scholar]
- 5.Jautzke G, Müller-Ruchholtz E, Thalmann U. Immunohistological detection of estrogen and progesterone receptors in multiple and well differentiated leiomyomatous lung tumors in women with uterine leiomyomas (so-called benign metastasizing leiomyomas). A report on 5 cases. Pathol Res Pract. 1996;192(3):215–223. doi: 10.1016/S0344-0338(96)80224-X. [DOI] [PubMed] [Google Scholar]
- 6.Goyle KK, Moore DF, Jr, Garrett C, Goyle V. Benign metastasizing leiomyomatosis: case report and review. Am J Clin Oncol. 2003;26(5):473–476. doi: 10.1097/01.coc.0000037737.78080.E3. [DOI] [PubMed] [Google Scholar]
- 7.Schneider T, Kugler C, Kayser K, Dienemann H. Benignes, pulmonal metastasierendes Leiomyom des Uterus [Benign, pulmonary metastatic leiomyoma of the uterus] Chirurg. 2001;72(3):308–311. doi: 10.1007/s001040051311. [DOI] [PubMed] [Google Scholar]
- 8.Andrade LA, Torresan RZ, Sales JF, Jr, Vicentini R, De Souza GA. Intravenous leiomyomatosis of the uterus. A report of three cases. Pathol Oncol Res. 1998;4(1):44–47. doi: 10.1007/BF02904695. [DOI] [PubMed] [Google Scholar]
- 9.Abramson S, Gilkeson RC, Goldstein JD, Woodard PK, Eisenberg R, Abramson N. Benign metastasizing leiomyoma: clinical, imaging, and pathologic correlation. AJR Am J Roentgenol. 2001;176(6):1409–1413. doi: 10.2214/ajr.176.6.1761409. [DOI] [PubMed] [Google Scholar]
- 10.Yoon G, Kim TJ, Sung CO, Choi CH, Lee JW, Lee JH, Bae DS, Kim BG. Benign metastasizing leiomyoma with multiple lymph node metastasis: a case report. Cancer Res Treat. 2011;43(2):131–133. doi: 10.4143/crt.2011.43.2.131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Egberts JH, Schafmayer C, Bauerschlag DO, Jänig U, Tepel J. Benign abdominal and pulmonary metastasizing leiomyoma of the uterus. Arch Gynecol Obstet. 2006;274(5):319–322. doi: 10.1007/s00404-006-0165-8. [DOI] [PubMed] [Google Scholar]
- 12.Bakkensen JB, Samore W, Bortoletto P, Morton CC, Anchan RM. Pelvic and pulmonary benign metastasizing leiomyoma: a case report. Case Rep Womens Health. 2018;31(18):e00061. doi: 10.1016/j.crwh.2018.e00061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Steiner PE. Metastasizing fibro-leiomyoma of the uterus: report of a case and review of the literature. Am J Pathol. 1939;15:89–110. [PMC free article] [PubMed] [Google Scholar]
- 14.Barnaś E, Książek M, Raś R, Skręt A, Skręt-Magierło J, Dmoch-Gajzlerska E. Benign metastasizing leiomyoma: a review of current literature in respect to the time and type of previous gynecological surgery. PLoS ONE. 2017;12(4):e0175875. doi: 10.1371/journal.pone.0175875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Glassman D, Patel JM, Hathout L, et al. Benign metastasizing leiomyoma in retroperitoneal lymph nodes with concurrent early stage cervical cancer. Gynecol Oncol Rep. 2022;6(40):100975. doi: 10.1016/j.gore.2022.100975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Abell MR, Littler ER. Benign metastasizing uterine leiomyoma. Multiple lymph nodal metastases. Cancer. 1975;36(6):2206–2213. doi: 10.1002/cncr.2820360938. [DOI] [PubMed] [Google Scholar]
- 17.Laban KG, Tobon-Morales RE, Hodge JA, et al. Single benign metastasising leiomyoma of an inguinal lymph node. BMJ Case Rep. 2016;2016:bcr2016216546. doi: 10.1136/bcr-2016-216546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Deppe G, Clachko M, Deligdisch L. Uterine fibroleimoyomata with aortic lymph node metastases. Int J Gynaecol Obstet. 1980;18(1):1–3. doi: 10.1002/j.1879-3479.1980.tb00229.x. [DOI] [PubMed] [Google Scholar]
- 19.Tori M, Akamatsu H, Mizutani S, et al. Multiple benign metastasizing leiomyomas in the pelvic lymph nodes and biceps muscle: report of a case. Surg Today. 2008;38(5):432–435. doi: 10.1007/s00595-007-3609-2. [DOI] [PubMed] [Google Scholar]
- 20.Lim SY, Park JC, Bae JG, et al. Pulmonary and retroperitoneal benign metastasizing leiomyoma. Clin Exp Reprod Med. 2011;38(3):174–177. doi: 10.5653/cerm.2011.38.3.174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Akar S, Ugras S, Sahin G, Demir F, Çelik Ç. Benign metastasising leiomyoma with lymph node metastases in a patient with endometrial cancer after caesarean section. J Obstet Gynaecol. 2019;39(3):420–421. doi: 10.1080/01443615.2018.1468743. [DOI] [PubMed] [Google Scholar]
- 22.Giove S, Scappaticci E, Baldi S, et al. Benign metastasizing leiomyoma of the uterus. Case report. Minerva Med. 1984;75(30–31):1819–1821. [PubMed] [Google Scholar]
- 23.Lee HJ, Choi J, Kim KR. Pulmonary benign metastasizing leiomyoma associated with intravenous leiomyomatosis of the uterus: clinical behavior and genomic changes supporting a transportation theory. Int J Gynecol Pathol. 2008;27(3):340–345. doi: 10.1097/PGP.0b013e3181656dab. [DOI] [PubMed] [Google Scholar]
- 24.Wu RC, Chao AS, Lee LY, Lin G, Chen SJ, Lu YJ, Huang HJ, Yen CF, Han CM, Lee YS, Wang TH, Chao A. Massively parallel sequencing and genome-wide copy number analysis revealed a clonal relationship in benign metastasizing leiomyoma. Oncotarget. 2017;8(29):47547–47554. doi: 10.18632/oncotarget.17708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Esteban JM, Allen WM, Schaerf RH. Benign metastasizing leiomyoma of the uterus: histologic and immunohistochemical characterization of primary and metastatic lesions. Arch Pathol Lab Med. 1999;123(10):960–962. doi: 10.5858/1999-123-0960-BMLOTU. [DOI] [PubMed] [Google Scholar]
- 26.Uchida T, Tokumaru T, Kojima H, Nakagawaji K, Imaizumi M, Abe T. A case of multiple leiomyomatous lesions of the lung: an analysis of flow cytometry and hormone receptors. Surg Today. 1992;22(3):265–268. doi: 10.1007/BF00308833. [DOI] [PubMed] [Google Scholar]
- 27.Beck MM, Biswas B, D'Souza A, Kumar R. Benign metastasising leiomyoma after hysterectomy and bilateral salpingo-oophorectomy. Hong Kong Med J. 2012;18(2):153–155. [PubMed] [Google Scholar]
- 28.Awonuga AO, Rotas M, Imudia AN, Choi C, Khulpateea N. Recurrent benign metastasizing leiomyoma after hysterectomy and bilateral salpingo-oophorectomy. Arch Gynecol Obstet. 2008;278(4):373–376. doi: 10.1007/s00404-008-0581-z. [DOI] [PubMed] [Google Scholar]
- 29.Pacheco-Rodriguez G, Taveira-DaSilva AM, Moss J. Benign metastasizing leiomyoma. Clin Chest Med. 2016;37(3):589–595. doi: 10.1016/j.ccm.2016.04.019. [DOI] [PubMed] [Google Scholar]
- 30.Sawai Y, Shimizu T, Yamanaka Y, Niki M, Nomura S. Benign metastasizing leiomyoma and 18-FDG-PET/CT: a case report and literature review. Oncol Lett. 2017;14(3):3641–3646. doi: 10.3892/ol.2017.6609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Chen S, Liu RM, Li T. Pulmonary benign metastasizing leiomyoma: a case report and literature review. J Thorac Dis. 2014;6(6):E92–E98. doi: 10.3978/j.issn.2072-1439.2014.04.37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Abu Saadeh F, Riain CO, Cormack CM, Gleeson N. Lung metastases from benign uterine leiomyoma: Does 18-FDG-PET/CT have a role to play? Ir J Med Sci. 2019;188(2):619–624. doi: 10.1007/s11845-018-1876-0. [DOI] [PubMed] [Google Scholar]
- 33.Kayser K, Zink S, Schneider T, Dienemann H, André S, Kaltner H, Schüring MP, Zick Y, Gabius HJ. Benign metastasizing leiomyoma of the uterus: documentation of clinical, immunohistochemical and lectin-histochemical data of ten cases. Virchows Arch. 2000;437(3):284–292. doi: 10.1007/s004280000207. [DOI] [PubMed] [Google Scholar]
- 34.Mavroudi M, Zarogoulidis P, Katsikogiannis N, Tsakiridis K, Huang H, Sakkas A, Kallianos A, Rapti A, Sarika E, Karapantzos I, Zarogoulidis K. Lymphangioleiomyomatosis: current and future. J Thorac Dis. 2013;5(1):74–79. doi: 10.3978/j.issn.2072-1439.2013.01.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Banner AS, Carrington CB, Emory WB, Kittle F, Leonard G, Ringus J, Taylor P, Addington WW. Efficacy of oophorectomy in lymphangioleiomyomatosis and benign metastasizing leiomyoma. N Engl J Med. 1981;305(4):204–209. doi: 10.1056/NEJM198107233050406. [DOI] [PubMed] [Google Scholar]
- 36.Henske EP, McCormack FX. Lymphangioleiomyomatosis: a wolf in sheep's clothing. J Clin Invest. 2012;122(11):3807–3816. doi: 10.1172/JCI58709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Hague WM, Abdulwahid NA, Jacobs HS, Craft I. Use of LHRH analogue to obtain reversible castration in a patient with benign metastasizing leiomyoma. Br J Obstet Gynaecol. 1986;93(5):455–460. doi: 10.1111/j.1471-0528.1986.tb08653.x. [DOI] [PubMed] [Google Scholar]
- 38.Nasu K, Tsuno A, Takai N, Narahara H. A case of benign metastasizing leiomyoma treated by surgical castration followed by an aromatase inhibitor, anastrozole. Arch Gynecol Obstet. 2009;279(2):255–257. doi: 10.1007/s00404-008-0698-0. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
There was no dataset, as this was a case report. Patient data and details are available upon request by email.