

ABSTRACT
A routine clinical assessment in a 39-year-old male revealed liver function tests at 1.4–2.3 times the normal limit. He was asymptomatic, had no personal/family history of liver disease, and did not drink or use recreational drugs. He was in good physical condition and engaged in regular running and resistance exercise. Negative workup included tests for hepatitis A, B, and C, M-proteins, and antimitochondrial antibodies. Abdominal ultrasound was unremarkable. The patient was referred to a gastroenterologist who ordered repeat liver function tests (LFTs) and a liver biopsy. Before his follow-up assessment the patient abstained from exercise for seven days, after which all LFTs had normalized. The abnormal liver panel was thus likely due to exercise-induced muscle damage and/or changes in hepatocyte membrane permeability. Importantly, the diagnostic pathway did not include any assessment of muscle biomarkers (e.g., creatine kinase) or the patient’s exercise training habits. This case highlights a knowledge gap in primary care regarding the possible causes of LFT abnormalities in young adults.
Keywords: Case report, exercise, liver, liver function tests, muscle damage
Introduction
The liver is the largest organ in the body and has key roles in metabolism, protein production, and detoxification. So-called “liver function tests (LFTs),” used in medicine since at least the 1950s, measure proteins and enzymes released by liver cells into the blood. A standard liver panel comprises alanine aminotransferase (ALT), aspartate aminotransferase (AST), and alkaline phosphatases (APs) to assess liver “injury,” albumin to assess excretory function, bilirubin to assess metabolic function, and sometimes γ-glutamyltransferase (GGT) to assess cholestatic injury or bile duct dysfunction.[1,2]
Despite the widespread importance and utility of LFTs in primary care (and beyond), reservations about the nomenclature extend as far back as the 1940s. Klatskin noted that the term LFT is misleading because most of the measured variables are not restricted to the liver (e.g., AST originates in the liver, skeletal muscle, cardiac muscle, red blood cells, brain, pancreas, and lungs) and are not a direct measure of its function.[3] This case study describes a healthy adult male who presented with LFTs more than double the normal range. Although this abnormal finding was eventually deemed to be the result of intense exercise training, the patient’s diagnostic pathway included no assessment of muscle biomarkers and no exploration of his physical activity regimen. This report therefore highlights a potential knowledge gap in primary care and draws attention to the “LFT misnomer” that, according to Klatskin, “may be the basis for misunderstanding and misinterpretation.”[3]
Case History
While abroad in October 2021, a 39-year-old physically active male underwent a routine clinical assessment for an issue unrelated to liver function. Blood tests revealed modestly elevated AP and GGT. The patient was advised to follow up with his primary care provider upon returning to the United States. In March 2022, he submitted to a full liver panel which revealed values that were further elevated, with AP, ALT, and AST above the reference ranges. When repeated a week later, the liver panel was “elevated and worsening” with values at 1.4–2.3 times the normal upper limit [see Table 1]. Liver function tests in this patient have been historically elevated, but values for aminotransferases as of March 2022 were considerably higher than those previously noted.
Table 1.
Chronological trend in liver function tests
| Marker | Normal range | Jun 2010 | Jun 2013 | Oct 2021 | Mar 2022 | Mar 2022 | May 2022 |
|---|---|---|---|---|---|---|---|
| Alanine transaminase (IU/L) | 0-44 | 44* | 42 | 22 | 96* | 101* | 47* |
| Aspartate transaminase (IU/L) | 0-40 | 45* | 30 | 17 | 49* | 59* | 28 |
| Alkaline phosphatase (IU/L) | 44-121 | 95 | 151* | 131* | 128* | 130* | 113 |
| Albumin (g/L) | 40-50 | 41 | 42 | 49.7 | 47 | 47 | 51* |
| Total Bilirubin (µmol/L) | 0.0-20.5 | 20 | 21* | 19.3 | 13.7 | 8.6 | 18.8 |
| γ-glutamyltransferase (IU/L) | 0-65 | 53 | 104* | 68* | - | 90* | 60 |
*Outside normal range
The patient was asymptomatic, had no personal or family history of liver disease, did not drink, smoke, or use recreational drugs, and had not suffered any recent viral infections. He was in good physical condition and engaged in regular running exercise (30–40 km/week) and resistance training characterized by standard progressive overload.
The working diagnosis was chronic transaminitis. Further negative workup included tests for hepatitis A, B, and C, M-proteins, and antimitochondrial antibodies. Abdominal ultrasound was also unremarkable. The patient was referred to the gastroenterologist’s office, who suggested a repeat liver panel in six weeks, followed by a liver biopsy if values remained elevated. Before his follow-up assessment the patient took it upon himself to abstain from exercise training for seven days. On re-evaluation, all LFTs—including previously elevated ALT, AST, AP, and GGT—had essentially normalized. He was discharged by the specialist and primary care provider and instructed to repeat liver panels periodically. The patient returned to regular training, remained asymptomatic, and monitored his LFTs through his primary care provider twice yearly following a seven-day rest period.
Discussion
Hepatic injury is a primary cause of deranged LFTs and can be due to a wide range of issues, including alcohol consumption, nonalcoholic fatty liver disease, hemochromatosis, hepatitis B, hepatitis C, and use of performance-enhancing drugs (e.g., anabolic/androgenic steroids).[4] Investigations by the primary care provider excluded these as causal factors in the patient’s elevated LFTs. At the time of his assessment, the patient was taking a dietary supplement (creatine monohydrate) that was not considered a prominent risk for liver damage.[5] Intense exercise is an extrahepatic cause of elevated LFTs that should be considered in clinical practice.[6] Because the patient’s liver markers had essentially normalized following one week’s training cessation, exercise-induced changes in muscle and/or liver function were deemed the most probable cause.
Despite several case reports[7,8,9] and one controlled study[6] showing acute transaminitis following intense exercise training in otherwise healthy adults, this clinical case makes at least three unique observations. First, transaminitis following intense exercise has not been observed alongside elevated GGT. Yet, we present evidence of exercise-associated increases in ALT, ASP, AP, and GGT—all of which normalized following seven days of rest. Second, mild increases in transaminases are often transient, with around one-third of cases resolving on repeat testing,[10] whereas this patient presents with a 12-year history of mild, likely fluctuating elevations in liver enzymes [Table 1]. Lastly, muscle damage-induced transaminitis has generally been reported in untrained individuals engaged in strenuous exercise to which they are were unaccustomed. The case study presented here shows transaminitis in a lifelong athlete, fully accustomed to prolonged bouts of running and intense resistance training. This report, therefore, makes unique observations that may inform primary care by extending our understanding of the causes of elevated LFTs in active individuals.
Both AST and ALT are included in the standard liver panel because they are highly concentrated in the liver, even though the net quantities are higher in skeletal muscle.[11] These enzymes also play an important role in amino acid metabolism, catalyzing the conversion of L-alanine and α-ketoglutarate into L-glutamate and pyruvate via the TCA cycle [Figure 1]. Hence, unlike GGT, which can effectively distinguish the liver from skeletal muscle damage,[12] AST and ALT are not specific to the liver nor a sensitive measure of its function. The most likely cause for the elevated AST and ALT observed presently is exercise-induced muscle damage/inflammation.
Figure 1.
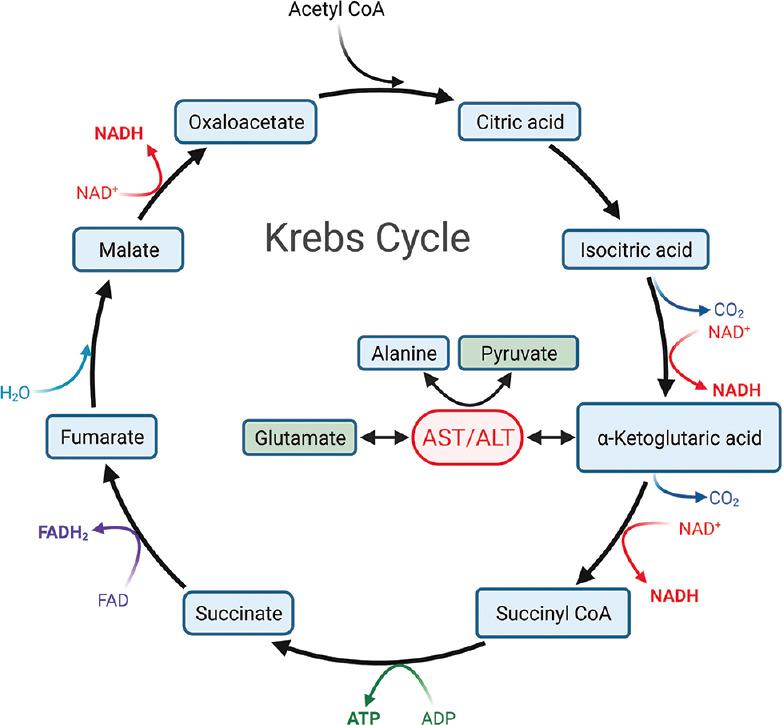
The Krebs Cycle showing the important role of alanine aminotransferase and aspartate aminotransferase in amino acid metabolism, catalyzing the conversion of L-alanine and α-ketoglutarate into L-glutamate and pyruvate. Original image created with BioRender.com
Exercise can also influence liver function directly. For instance, decreases in hepatic blood flow and oxygen saturation during strenuous exercise can increase hepatocyte membrane permeability and subsequently raise liver enzymes. In fact, GGT has been observed to increase acutely from baseline following half-marathon running, despite values not exceeding the upper limit of normal.[13] Epidemiological studies have also shown that GGT may be an early and sensitive indicator of oxidative stress[14]—a phenomenon that is widely known to be influenced by exercise. More research is needed to elucidate the complex interplay between intense exercise and GGT responses.
Traditional biomarkers of “liver injury” have been shown to correlate with biomarkers of muscle damage (e.g., creatine kinase) following prolonged exercise.[15] Yet, muscle biomarkers and patient exercise habits are not routinely assessed alongside liver panels in primary care. Such omissions in the diagnostic pathway can result in the misdiagnosis of liver problems and unnecessary follow-up tests and referrals.[6] We thus concur with Pavletic and Pao that markers of muscle damage, and a full workup of the patient’s exercise training regimen, should be incorporated into standard screening and clinical investigations (in primary care and beyond), particularly those pertaining to the liver.[8] Presently, these assessments could have spared the patient a diagnostic pathway that included several expensive, time-consuming, and potentially invasive follow-up tests, as well as the associated anxiety. Based on the present findings, we further advocate exercise abstinence for at least seven days before an LFT. Revising current practices to align with these recommendations may be particularly important, given that muscle-strengthening exercises are included in physical activity guidelines disseminated by the Department for Health and Human Services, the American Medical Association, and the World Health Organization.
In conclusion, our understanding of the myriad causes of elevated liver enzymes remains incomplete. Still, in this case report, we present novel data that challenge our understanding of the paradigm and that to expose a potential gap in primary care regarding the ways that exercise affects liver enzymes, including GGT. We advocate for better education on the diverse causes of elevated LFTs in young, active people.
Declaration of patient consent
The patient provided informed consent for his data to be used in this case report.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors declare no conflict of interest. The results of the study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation. NBT is supported by a postdoctoral fellowship from the Tobacco-Related Disease Research Program (award no. T31FT1692).
References
- 1.Levinson M, Holbert J, Blackwell C, Wruble LD. Serum gamma-glutamyl transpeptidase:Its specificity and clinical value. South Med J. 1979;72:837–41. doi: 10.1097/00007611-197907000-00021. [DOI] [PubMed] [Google Scholar]
- 2.Kasarala G, Tillmann H. Standard liver tests. Clin Liver Dis. 2016;8:13–8. doi: 10.1002/cld.562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Klatskin G. Some observations on liver function tests. Yale J Biol Med. 1948;21:127–43. [PMC free article] [PubMed] [Google Scholar]
- 4.Oh RC, Hustead TR. Causes and evaluation of mildly elevated liver transaminase levels. Am Fam Physician. 2011;84:1003–8. [PubMed] [Google Scholar]
- 5.Kreider RB, Kalman DS, Antonio J, Ziegenfuss TN, Wildman R, Collins R, et al. International Society of Sports Nutrition position stand:Safety and efficacy of creatine supplementation in exercise, sport, and medicine. J Int Soc Sports Nutr. 2017;14:18. doi: 10.1186/s12970-017-0173-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pettersson J, Hindorf U, Persson P, Bengtsson T, Malmqvist U, Werkström V, et al. Muscular exercise can cause highly pathological liver function tests in healthy men. Br J Clin Pharmacol. 2008;65:253–9. doi: 10.1111/j.1365-2125.2007.03001.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Khatri P, Neupane A, Sapkota SR, Bashyal B, Sharma D, Chhetri A, et al. Strenuous exercise-induced tremendously elevated transaminases levels in a healthy adult:A diagnostic dilemma. Case Rep Hepatol. 2021;2021:6653266. doi: 10.1155/2021/6653266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pavletic AJ, Pao M. Exercise-induced elevation of liver enzymes in a healthy female research volunteer. Psychosomatics. 2015;56:604–6. doi: 10.1016/j.psym.2015.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Delicata NP, Delicata J, Delicata LA. Strenuous exercise—An unusual cause of deranged liver enzymes. Case Rep Clin Med. 2018;7:177–81. [Google Scholar]
- 10.Lazo M, Selvin E, Clark JM. Brief communication:Clinical implications of short-term variability in liver function test results. Ann Intern Med. 2008;148:348–52. doi: 10.7326/0003-4819-148-5-200803040-00005. [DOI] [PubMed] [Google Scholar]
- 11.Kohli R, Harris DC, Whitington PF. Relative elevations of serum alanine and aspartate aminotransferase in muscular dystrophy. J Pediatr Gastroenterol Nutr. 2005;41:121–4. doi: 10.1097/01.wno.0000161657.98895.97. [DOI] [PubMed] [Google Scholar]
- 12.Rosales XQ, Chu ML, Shilling C, Wall C, Pastores GM, Mendell JR. Fidelity of gamma-glutamyl transferase (GGT) in differentiating skeletal muscle from liver damage. J Child Neurol. 2008;23:748–51. doi: 10.1177/0883073808314365. [DOI] [PubMed] [Google Scholar]
- 13.Lippi G, Schena F, Montagnana M, Salvagno GL, Banfi G, Guidi GC. Significant variation of traditional markers of liver injury after a half-marathon run. Eur J Intern Med. 2011;22:e36–8. doi: 10.1016/j.ejim.2011.02.007. [DOI] [PubMed] [Google Scholar]
- 14.Lee DH, Blomhoff R, Jacobs DR. Is serum gamma glutamyltransferase a marker of oxidative stress? Free Radic Res. 2004;38:535–9. doi: 10.1080/10715760410001694026. [DOI] [PubMed] [Google Scholar]
- 15.Tirabassi JN, Olewinski L, Khodaee M. Variation of traditional biomarkers of liver injury after an ultramarathon at altitude. Sports Health. 2018;10:361–5. doi: 10.1177/1941738118764870. [DOI] [PMC free article] [PubMed] [Google Scholar]