

Abstract
Depression is highly prevalent and represents the leading cause of global disability and primary contributor to overall global burden of disease. Several lines of evidence from early-phase experimental trials suggest that serotonergic psychedelics, particularly psilocybin, with therapeutic support show great promise in the treatment of depression with large effect sizes. Neuroimaging data have also revealed the dynamic effects of psilocybin on functional activity within and between neural regions. This chapter reviews the methods and findings from three small human laboratory clinical trials examining the effects of psilocybin therapy for patients with major depressive disorder and treatment-resistant depression. Insights from functional magnetic resonance imaging and qualitative analyses are also presented, as well as a discussion of study limitations and future directions for the research.
Keywords: Depression, Psilocybin, Psychedelics
1. An Essential Need to Help Ease Mental Suffering
Over 300 million people are affected by depression worldwide, rendering it a massive global public health concern (World Health Organization 2019). Depression represents the number one cause of disability (World Health Organization 2019), and the relative risk of all-cause mortality among depressed people is 1.7 times greater than the non-depressed population (Walker et al. 2015). In terms of prevalence, approximately 10% of the United States (U.S.) adult population has been diagnosed with Major Depressive Disorder (MDD) in the past year (Hasin et al. 2018). In addition to the personal burden, the annual economic burden is estimated to be a staggering $210 billion (Greenberg et al. 2015).
A variety of pharmaco- and psychotherapies have been developed to address the public health and personal burden of this condition (Cuijpers et al. 2014; Otto and Hearon 2016). Despite the evidence supporting the relative effectiveness of existing interventions, many people lack access to these treatments and many who are treated experience depression relapse (Collimore and Rector 2014; Coull and Morris 2011; Hofmann et al. 2012; Sinyor et al. 2010; Koen and Stein 2011). For example, although many patients will experience a reduction or remission in depression symptoms after treatment with existing pharmacotherapies (Morilak and Frazer 2004), up to 50% will not respond fully. Additionally, as many as 30% are considered to have treatment-resistant depression (TRD), resulting in effects that are only marginally superior to placebo (Gaynes et al. 2009; Nemeroff 2007). The disparity between the need for effective treatments and an absence of available effective options highlights the need to explore novel ways to treat this debilitating condition.
Within psychiatry, there is an urgent need for improved mental healthcare and novel pharmacological approaches. Many leaders in the field have urged the adoption of a “disruptive pharmacology” approach (Heifets and Malenka 2019) to investigate novel interventions with historically restricted substances, such as classic psychedelics, for treating disabling conditions such as depression (Carhart-Harris et al. 2016, 2018, 2021; Ross et al. 2016; Griffiths et al. 2016; Agin-Liebes et al. 2020; Davis et al. 2021a). Psilocybin (4-phosphoryloxy-N,N-dimethyltryptamine) belongs to a chemical group of naturally occurring serotonergic tryptamines. Psilocybin therapy combines supportive psychotherapy with one or two doses of the classic psychedelic psilocybin, which acts primarily as an agonist of the serotonin-2A (5HT-2A) receptor and has the capacity to occasion profound changes in sensory perceptions, cognition, mood, and alterations in self-related processing mediated by increased neural plasticity (Araújo et al. 2015). Recent studies examining this treatment approach have suggested that it is potentially efficacious in decreasing symptoms of depression among a variety of patient populations (Carhart-Harris et al. 2016, 2018, 2021; Ross et al. 2016; Griffiths et al. 2016; Agin-Liebes et al. 2020; Davis et al. 2021a). For example, two placebo-controlled studies published in 2016 showed that psilocybin therapy continued to decrease depressive symptoms among patients with life-threatening illness up to 6 months after the treatment was completed, and up to 4.5 years in one long-term follow-up study (Ross et al. 2016; Griffiths et al. 2016; Agin-Liebes et al. 2020). In 2017, an open-label study was published assessing the effect of psilocybin therapy for patients with TRD, demonstrating that this treatment decreased depression symptoms lasting up to 3 months (Carhart-Harris et al. 2018). In 2020, the first randomized controlled trial (RCT) was published that examined psilocybin therapy among the general depression population, showing large decreases in depression with about one-half (54%) in remission 1 month after treatment (Agin-Liebes et al. 2020). Furthermore, findings from another recent RCT suggested that psilocybin therapy may be as or more effective than selective serotonin reuptake inhibitors (SSRIs), which are the most commonly prescribed pharmacological treatment for MDD (Davis et al. 2021a).
Given the positive outcomes from several trials, the U.S. Food and Drug Administration (FDA) has granted psilocybin therapy “Breakthrough” status, on the premise that there is meaningful evidence to support rapid and prioritized examination of this treatment approach in large multisite trials. This chapter will review published studies from the extant literature that have explored psilocybin therapy as a treatment for depression. This chapter will limit its review to the trials that have focused exclusively on MDD as a primary clinical indication (Carhart-Harris et al. 2016, 2018; Agin-Liebes et al. 2020; Davis et al. 2021a). We will also include data from neuroimaging and qualitative studies reports and a discussion of possible psychological mechanisms that may explain its antidepressant effects. Future directions for this line of research will also be discussed.
2. Psilocybin Therapy for Depression
All three of the following trials of psilocybin therapy for a primary indication of depression shared a common treatment model. Prior to the psilocybin sessions, participants received preparatory sessions with psychoeducation about the upcoming medication sessions as well as explanation of common reactions and challenges. During the psilocybin experiences, participants were provided eye masks and headphones and were encouraged to listen to a pre-recorded playlist. Participants were encouraged to direct their attention inward during these 8-h psilocybin sessions. The following day participants met with their session facilitators to process insights and emotions that emerged during their psilocybin sessions (commonly referred to as integration).
3. Psilocybin Therapy for People Diagnosed with Treatment-Resistant Depression
In 2016, Carhart-Harris and colleagues at Imperial College, London published findings from a small open-label feasibility study assessing the effects of psilocybin on TRD (Carhart-Harris et al. 2016, 2018). The investigators attempted to increase the sample size from 12 to 20 midway through the trial reportedly to achieve adequate statistical power for brain imaging analyses; the investigators conducted a 6-month follow-up analysis with the larger (N = 20) sample (Carhart-Harris et al. 2017). All participants met criteria for MDD and endorsed a score of 16 or greater on the Hamilton Depression Rating Scale (HAM-D) (Iannuzzo et al. 2006). They also were required to have failed two previous courses of antidepressant medication treatment (from separate pharmacological classes) with 6 weeks of duration during the depressive episode.
The study involved two psilocybin administration sessions separated by 1 week. In the first session, participants received 10 mg of psilocybin, followed by 25 mg in the second session. In addition to feasibility and safety, the investigators assessed the preliminary efficacy of psilocybin in reducing self-reported depression scores with the Quick Inventory of Depressive Symptomatology (QIDS-SR16) (Rush et al. 2003). Secondary outcomes included trait anxiety (STAI-T) (Spielberger 2010) and anhedonia (Snaith-Hamilton Pleasure Scale; SHAPS) (Snaith et al. 1995). Participants also underwent a functional MRI (fMRI) scanning session at baseline and 1 day after the high-dose psilocybin session (see further details below) (Araújo et al. 2015).
Results revealed significant within-group reductions on the QIDS-SR16 relative to baseline at the 1-week time point, and these reductions persisted until the 6-month follow-up. These findings were corroborated by clinician-administered ratings. Within-subject effect sizes were very large (Cohen’s d 1.4–2.3). In the original analysis (N = 12), 67% of participants met clinical criteria for remission (defined as a score of ≤9 on the Beck Depression Inventory; BDI (Beck et al. 1996)) from depression at the 1-week time point, and 42% continued to meet remission criteria at the 3-month follow-up. There were also significant reductions, relative to baseline, on suicidality at the 1-week and 2-week follow-ups and on trait anxiety and anhedonia measures at the 1-week and 3-month follow-ups. None of the participants resumed antidepressant medications within 5 weeks after their psilocybin sessions. Significant reductions on the QIDS-SR16 remained significant at the 6-month follow-up (Cohen’s d = 1.4). Reductions in depressive symptoms at the 5-week follow-up were significantly associated with ratings of acute psychedelic experience [on the 11-Dimension altered states of consciousness (11D-ASC)] (Studerus et al. 2010).
There were no serious adverse events (SAEs) reported in the trial. The most common AEs reported were transient anxiety (100%), confusion (75%), and nausea (33%) during the psilocybin session and headache 1 day after the session. All AEs resolved by the end of the session, with the exception of headache, which tended to resolve 1–2 days following psilocybin treatment. This pilot study provided important scientific insights informing future research but was limited by the absence of a control group, possible favorable expectancy effects and participant self-selection biases. Additionally, for the majority of participants, positive outcomes did not persist beyond the 3-week follow-up time point. Lastly, the majority of participants (75%) were non-Hispanic White, which limits the generalizability to more diverse groups of individuals.
The investigators also conducted a series of fMRI analyses with the same TRD study sample at baseline and 1 day after participants’ high-dose psilocybin session. They assessed changes (relative to baseline) in cerebral blood flow, functional connectivity, and amygdala responsiveness during an emotional face paradigm (Araújo et al. 2015; Roseman et al. 2018; Mertens et al. 2020). fMRI whole-brain analysis data revealed significant reductions in cerebral blood flow in the temporal cortex (including the amygdala) that correlated with reductions in depressed mood. They also found increased resting state functional connectivity in the following two brain regions: (1) the default mode network (DMN), a network involved in self-related processing and mind wandering and has been found to be hyper-engaged in a variety of psychiatric disorders, including MDD (Hamilton et al. 2015) and (2) the ventromedial prefrontal cortex (vmPFC)-bilateral inferior-lateral parietal cortex (ilPC), a network involved in regulating and inhibiting emotional responses. These findings contrast with previous findings of acute decreases in DMN activity captured during psilocybin sessions (Carhart-Harris et al. 2012). The investigators speculate that these acute and post-acute (1 day after psilocybin) dynamics may reflect an initial acute disintegration of DMN connectivity during psilocybin followed by reintegration of normalized functioning, which may serve a psychological “reset” function (Araújo et al. 2015). Additionally, exploratory analyses showed that acute, subjective mystical-type experiences during the psilocybin session predicted changes in these DMN and limbic (emotion network) regions (Araújo et al. 2015).
With regard to amygdala responsiveness in the same group of participants, the investigators found that participants showed increased amygdala responses to both fearful and joyful faces during an emotional face-processing paradigm administered 1 day after the high-dose psilocybin session (Studerus et al. 2010; Roseman et al. 2018). The post-acute increases in amygdala activity predicted reductions in depression scores (on the QIDS-SR16 and BDI) at the 1-day, 1-week, and 3-week follow-ups. Additionally, the investigators found reductions in connectivity between the vmPFC and right amygdala. Although these alterations did not predict depression changes, they did predict rumination levels (a strong maintaining factor of depression) at the 1-week follow-up. Taken together, these findings could suggest that psilocybin may heighten depressed individuals’ sensitivity to experiencing emotions while reducing the top-down inhibitory control of prefrontal control regions on limbic regions. The investigators propose that these mechanisms might explain phenomenological insights regarding participants’ increased access to a full range of previously avoided emotions and subsequent emotional catharsis, processing, and release (Studerus et al. 2010; Roseman et al. 2018).
4. Psilocybin Therapy for the Treatment of Major Depressive Disorder
In 2021, Davis and colleagues reported on findings from a randomized controlled trial (RCT) conducted at Johns Hopkins University. The investigators randomized 27 participants (24 completers) with moderate-to-severe MDD to either an immediate intervention group or delayed (waitlist) group. The study involved two psilocybin medication sessions separated by 1 week (i.e., 20 mg/70 kg in session 1 and 30 mg/70 kg in session 2). The intervention period was 8 weeks in duration. Participants in the waitlist group were monitored on a weekly basis and completed assessments at weeks 5 and 8 (corresponding to the 1-week and 1-month time points in the immediate intervention group). The primary study outcome was the GRID-HAM-D, which was assessed by blinded clinician raters. The QIDS-Self Report (QIDS-SR) (Iannuzzo et al. 2006) was also administered as a self-report measure of the rapid (1-day) response to the treatment. The study also included secondary measures of suicidality, anxiety, trait anxiety, and persisting positive effects.
There were significant between-group effects favoring the immediate intervention group at the 1-week follow-up, which remained significant at the 4-week follow-up, compared to the delayed intervention group. Between-group effect sizes were very large at the 1-week and 4-week follow-ups in the immediate treatment group compared to weeks 5 and 8 in the waitlist group (Cohen’s d range = 2.5–2.6). Across the entire sample, reductions in depression on the QIDS-SR revealed immediate reductions in depression between baseline and 1 day after the psilocybin session, which remained significant at the 4-week follow-up (following session 2). At 1 month after treatment, 71% of participants demonstrated a clinically significant response (defined as greater than 50% decrease in GRID-HAM-D scores), and 54% were in complete remission from depression (a score of ≤7 on the GRID-HAM-D). All secondary depression, suicidality, and anxiety measures showed significant between-group differences and within-subjects reductions at all time points. Participants overwhelmingly (85–90%) rated their psilocybin experiences to be one of the top five most personally meaningful and psychologically insightful experiences of their lives. Decreases in depression scores at 1 month were significantly correlated with peak ratings of the degree to which the psilocybin sessions were personally meaningful (r = −0.70, p < 0.01), psychological insightful (r = −0.60, p < 0.01), and spiritually significant (r = −0.57, p < 0.01). There were no SAEs reported in the trial. The most frequent physiological AE was transient headache (29–33%). Greater than half the participants endorsed experiencing a variety of challenging emotions and physical sensations during psilocybin sessions that resolved before the end of the session. As in other contemporary clinical trials (Carhart-Harris et al. 2016, 2018; Griffiths et al. 2016; Ross et al. 2016) there were no reports of persistent visual perceptual changes, psychosis, or psilocybin use/misuse behaviors as none of the participants reported consuming psilocybin outside of the trial during the 4-week follow-up period.
Despite some notable strengths including the randomized controlled design and the use of a clinician-administered rating scale with blinded raters, the study carried a few limitations. Although the delayed waitlist design controlled for the passage of time, it did not control for other non-pharmacological therapeutic elements such as the preparatory and post-psilocybin therapy sessions and expectancy effects. As in the Carhart-Harris and colleagues’ study (Koen and Stein 2011), the majority of participants were non-Hispanic White (92%), and presented with low risk of suicide, which may not generalize to other individuals with moderate-to-severe depression. The study sample was also relatively small, and although the sample size was determined to be well-powered enough to detect significant effects, trials with larger sample sizes are needed.
5. Direct Comparison of Psilocybin Therapy and Antidepressant Medication Therapy
More recently, Carhart-Harris et al. (2021) conducted a double-blind RCT at Imperial College London with 59 participants with moderate-to-severe MDD (Davis et al. 2021a). Participants were randomized to one of two groups. One group received psilocybin (25 mg) followed by daily capsule doses of placebo (microcrystalline cellulose) for the subsequent 3 weeks. The second group received low-dose psilocybin (1 mg) followed by daily doses of escitalopram (10 mg). At the 3-week time point, participants in the former group received a second dose of high-dose psilocybin followed by daily capsule doses of placebo for the subsequent 3 weeks. The latter group received a second dose of low-dose psilocybin followed by additional daily doses of escitalopram (20 mg) for the subsequent 3 weeks. Both groups were provided one preparatory therapeutic session prior to the first dosing day and psychological debriefing/integration on the days after each dosing day. At the 6-week time point (3 weeks after the second dosing day), participants completed final study assessments. The participants in the escitalopram/active comparator group collaborated with their general physicians to discontinue the escitalopram medication. The primary study outcome was self-reported depression change-score (relative to baseline) on the QIDS-SR16 (Iannuzzo et al. 2006). Secondary outcomes included depression response (defined as a decrease in score of ≥50% from baseline) and remission rate at 6 weeks according to the QIDS-SR-16 (defined as a score of 0–1).
The investigators found larger decreases in depression scores on the QIDS-SR16 at the 6-week time point (−8.0 ± 1.0 from baseline) in the psilocybin group compared with the escitalopram group (−6.0 ± 1.0). However, this difference did not reach statistical significance in the 95% confidence interval [CI], −5.0 to 0.9; p = 0.17. Although there was no significant difference in response rate at the 6-week point, there were significant differences in depression remission favoring the psilocybin group (57%) over the escitalopram group (28%; CI, 2.3–53.8). There were also significant between-group differences in secondary measures of change-scores on measures of depression, anxiety, emotional avoidance, work and social functioning, anhedonia, well-being, and suicidality, all favoring the psilocybin therapy group.
There were no SAEs reported during the 6 weeks of the trial among either group, with equivalent total rates of AEs reported in the psilocybin (87%) and escitalopram groups (83%). As in other contemporary clinical trials (Agin-Liebes et al. 2020; Carhart-Harris et al. 2016, 2018; Griffiths et al. 2016; Ross et al. 2016) there were no reports of persistent visual perceptual changes, psychosis, or use/misuse behaviors during the 6-week period of the study. There were, however, significantly greater reports of anxiety (14%) and dry mouth (14%), sexual dysfunction (3%) and flat affect (7%) in the escitalopram group compared to the psilocybin group (in which all of these symptoms were absent). Further, 17% of the participants in the escitalopram group either prematurely terminated or halved their daily dose of escitalopram due to perceive adverse effects of this medication. Among the psilocybin group, AEs generally occurred during the 24 h after the psilocybin dosing day, with the most common AE being transient headache (67%) (compared with 52% in the escitalopram group), which is consistent with previous studies (Agin-Liebes et al. 2020; Carhart-Harris et al. 2016, 2018; Griffiths et al. 2016; Ross et al. 2016). Additionally, participants in the psilocybin group reported greater access to emotions and catharsis.
Although this study provides important scientific insights and improves upon previous research designs in rigor, it is limited by several important methodological issues. First, there was no inactive placebo group, which limits the ability to determine the treatment effect of either the psilocybin or escitalopram intervention alone. This also rendered the weak antidepressant effect in the escitalopram group less apparent compared to the effects seen in escitalopram versus placebo trials (Gründer and Mertens 2021). Although the investigators pre-registered their hypotheses, they did not adjust for multiple comparisons, and therefore no definitive clinical or statistical conclusions can be drawn about the data. Further, the duration of escitalopram treatment in the trial was only 6 weeks, which is much briefer than typically used in clinical practice, as the drug is known to have a delayed antidepressant therapeutic effect (Trivedi et al. 2006). As in the open-label trial (Carhart-Harris et al. 2016), the majority of participants were non-Hispanic White (83–93%). Additionally, the selection of study volunteers was likely biased toward selection of individuals favorably disposed toward psilocybin, which further limits generalizability of the findings. The titration of participants off of antidepressant medication might have also weakened the antidepressant effects in the escitalopram group. Lastly, expectancy effects were not controlled for, and the integrity of the blind was not assessed. Participants may have been able to identify to which study medication group they were assigned, which could have introduced additional bias in favor of the psilocybin effect.
6. Qualitative Reports from Depression Study Volunteers
Despite a resurgence in research involving psilocybin therapy as a treatment for depression, its therapeutic mechanism of action remains poorly understood. Accumulating evidence suggests that psilocybin stimulates a host of neural changes including modulations in brain connectivity, cerebral blood flow, and transient amygdala activation in response to emotional cues (Araújo et al. 2015; De Gregorio et al. 2018; Studerus et al. 2010; Yaden and Griffiths 2020). The functional and structural neural plasticity effects of psilocybin have been linked to emotion regulation and learning processes, however, the phenomenological effects can vary widely (Aday et al. 2021). In this section we present qualitative narratives highlighting the salient subjective features of the psilocybin therapy experience, which suggest key psychological processes.
As a follow-up to the Imperial open-label trial, Watts and colleagues (2017) conducted a thematic analysis of participant reports (N = 20) and identified two primary psychological change processes (Watts et al. 2017). Participants reported enhanced feelings of connectedness with self, others, and the world and a sense of interconnectedness with all of humanity, which helped to counteract long-standing feelings of disconnection that characterized their depressive states. Participants also reported an enhanced ability to confront, process, and accept difficult emotions that had been suppressed or avoided. Many participants described a deep catharsis and release, which culminated in resolution of long-held grief, as the following reported:
There was a lot of sadness, really, really deep sadness: the loss the grief, it was love and sadness together, and letting go, I could feel the grief and then let it go because holding onto it was hurting me, holding me back. It was a process of unblocking. (P2).
Excursions into grief, loneliness and rage, abandonment. Once I went into the anger it went ‘pouf’ and evaporated. I got the lesson that you need to go into the scary basement, once you get into it, there is no scary basement to go into [anymore]. (P3).
There was this huge terrifying creature with a rifle, and instead of running away, I looked at it, and it wasn’t as scary as it had seemed. [My] fear subsided, it suddenly seemed ridiculous, I started laughing. If I had avoided it, it would have got more terrifying. (P4).
Participants in the RCT at Johns Hopkins University described similar therapeutic processes of emotional release and resolution (Davis et al. 2021a). The following description is from one young adult participant who had been depressed and anxious for many years. (The information has been augmented to protect their confidentiality; the singular use of the pronoun “they” is used in order to mask the gender of the participant.) This participant presented to the trial with moderate levels of depression and anxiety. During the preparation therapy in the weeks leading up to the psilocybin session they reported feeling guarded and nervous but hoped to discover relief from the depression that had kept him feeling emotionally stuck.
During the first psilocybin session (20 mg/70 kg) the participant experienced the following (condensed from qualitative report):
Shivering cold. The concept of time is lost. Body is rocking, rolling, and writhing with the music. On inhales I’m soaring up a mountain in the clouds in unison with the crescendo. On exhales my body and mind are slipping into a darkness and quiet that has no end to its depths. Other times I feel the loud, turbulent, diffuse mix of thoughts, feelings, memories, anticipations, and the occasional moment of stillness.
I felt an infinite series of expansions and contractions. I wanted to see and have ultimate realities revealed to me. I kept asking for answers but I saw nothing. What I did receive was an internal brief feeling of peace, a knowing, and an understanding without really knowing what I was understanding. Acceptance.
I thought the experience would have a deep long-lasting impact on me, but I do not feel a strong emotional attachment to what happened. Like it wasn’t powerful enough to create a profound noticeable change in me. I don’t feel like I learned something clear and concise for me to take away from it. Like it didn’t make a powerful or lasting impression. I’m disappointed in myself. I felt like I was on the edge of something deeper. I felt like I could have seen or understood things more clearly if I was able to go deeper.
During the second psilocybin session (30 mg/70 kg) the participant experienced the following (condensed from qualitative report):
The main theme was healing and letting go. Healing came in many forms and feelings. I felt as if pain and sadness and trauma and guilt were draining from my body. As if it were being washed away and cleansed. I felt guided and compelled to let go of hurtful memories and recognized it was time to let go and okay to move on from the past. I felt the music was playing an integral role in guiding where the healing needed to take place in my body, mind, and heart. I felt it flowing through my body as a bright silver light traveling where it needed to go and guiding my thoughts to tranquility and acceptance.
I truly felt embraced and taken care of completely by some un-named force. That force allowed me to be open and willing to dissolve and dissipate the depression that was stuck in my mind. It allowed me to trust in myself and to be comfortable opening my once closed and guarded heart. I had a profoundly clear understanding that everything was happening exactly as it needed to be and everything will be okay no matter what.
The first psilocybin session dramatically broke up and cracked and loosened all the stuck energy and rigid patterns of my mind. Once it was loosened and broken up, in the second session it was able to clear all that once hardened debris free. Step 1. Jackhammer my mind and soul and show me I can survive that pain. Step 2. Gently and lovingly cleanse everything out and allow myself to let go and heal. I felt such a strong sense of soft, glowing, healing light assuring me that there was nothing to fear or feel sorrow for. I felt I was in the presence of a pure and perfect energy that was healing me.
I never once felt fear during the session. I knew I was going to be okay. I am okay. And for the first time in my life, I discovered the possibility of what it feels like to love myself. I have never felt that way before. And I truly value the psilocybin journey for showing me that I can honor myself and others as equals on a deep and soulful level.
This participant’s mental health outcomes are displayed in Fig. 1. As the figure shows, this participant experienced a large reduction in depression and anxiety symptoms throughout the study, which was persistent until the 12-month follow-up.
Fig. 1.
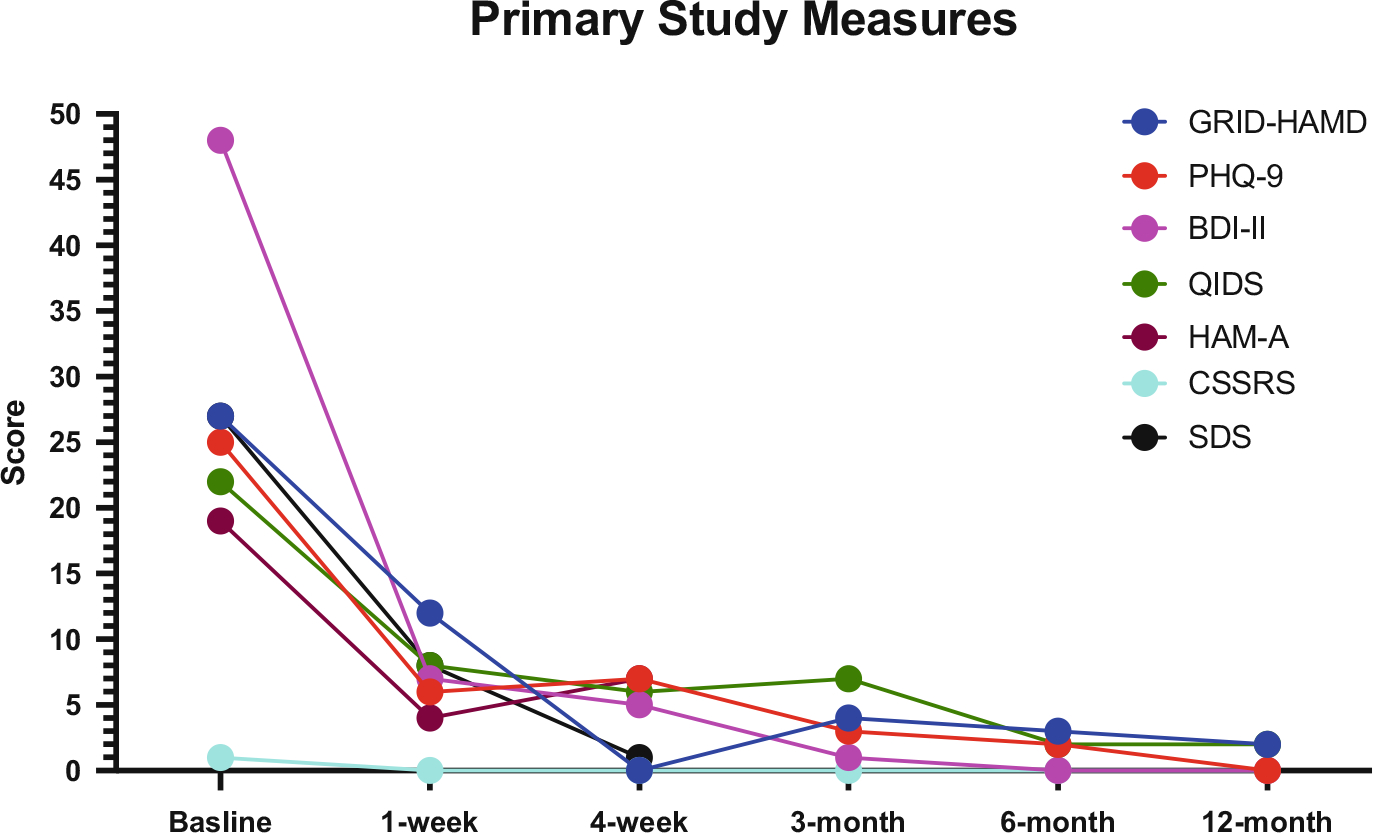
Primary outcome measures for participant from the John’s Hopkins Depression Trial. Measures include: Grid Hamilton Depression Rating Scale (GRID-HAMD), Nine item Patient Health Questionnaire (PHQ-9), Beck Depression Inventory – 2nd version (BDI-II), Quick Inventory of Depressive Symptoms (QIDS), Hamilton Anxiety Scale (HAM-A), Columbia Suicide Severity Rating Scale (CSSRS), Sheehan Disability Scale (SDS)
How psychedelics promote psychological processes in ways conducive to resolving depression is currently a fervent area of theoretical and empirical inquiry. As the narrative account and study data suggest, this participant reported enormous psychological benefit from psilocybin therapy, including notable improvements in depression, anxiety, and quality-of-life. Although not every participant in this study improved, or improved this dramatically, for some participants the psilocybin sessions provided a powerful opportunity to reevaluate or reappraise their past behaviors and life circumstances in a therapeutically productive manner. This participant reported acute psilocybin effects that ranged from physically challenging to deeply meaningful with psychological insights. While some reports documented in the literature feature elements of spiritual or mystical-type experiences (Ross et al. 2016; Griffiths et al. 2016), other experiences, such as the one featured here, involve more psychological and relational feelings of self- and other- forgiveness, compassion, and love, as well as emotional catharsis and acceptance. The psilocybin sessions tend to evoke psychological content and processes that are personally meaningful and relevant to each individual. These qualitative descriptions are supported by Carhart-Harris and Friston’s relaxed beliefs under psychedelics (REBUS) model (Carhart-Harris and Friston 2019), which proposes that psychedelics promote conditions conducive to relaxing and revising high-level, maladaptive beliefs (e.g., self-protective but maladaptive self-beliefs, “I am a failure, I will no longer venture anything new”). However, it is unclear to what extent the biological mechanisms account for therapeutic benefits and to what extent they explain the subjective psychological phenomena. It is also unclear to what extent the treatment depends on “set and setting” variables including the psychological support, preparation, and post-psilocybin therapy sessions. These questions deserve rigorous scientific investigation and may eventually reveal important insights regarding key change mechanisms.
7. Future Directions
Although the preliminary quantitative and qualitative data are promising, it is premature to conclude the treatment is efficacious in the much larger population of depressed individuals. The studies described above carry a number of limitations including the absence of control conditions in some studies and small sample sizes (Carhart-Harris et al. 2016), which increase the possibility that statistical effects will be detected when in fact there is indeed no treatment effect. The study samples in psychedelic research are also characterized by higher rates of self-selection biases and positive expectancies, which have not been adequately controlled for. Additionally, most trial participants have primarily been White and college educated, which greatly limits the generalizability of findings to other ethnic and socioeconomic groups, of which there are many. Indeed, there is a substantial lack of diversity within psychedelic research and a gross underrepresentation of Black, Indigenous and People of Color (BIPOC). As a developing field, the psychedelic research community faces an ethical imperative to conduct culturally inclusive and equitable trials through proactive community outreach recruitment efforts, anti-racism trainings for research staff, and the provision of meaningful compensation for participants’ time for those with financial barriers. Additionally, the focus on depression as a clinical outcome also neglects the potential role that psilocybin therapy holds in the treatment of conditions that are prevalent in BIPOC communities such as anxiety and depression that emerges as a result of ethnic/racial trauma (Davis et al. 2021b; Williams et al. 2021), which may be diagnosed as post-traumatic stress disorder. In fact, preliminary self-report evidence suggests that the use of psychedelics is increasing among BIPOC communities in non-clinical settings use as a means to address racial trauma, demonstrating an important need to focus on this topic in new clinical trials.
Despite substantial limitations, there is mounting evidence to suggest that psilocybin may carry rapid and sustained antidepressant properties, which have meaningful implications for the clinical management of depression. The findings have informed the basis of phase II/III trials that are currently underway for the treatment of MDD and TRD. The U.S. FDA and European Medicines Agency has granted two organizations fast-track status to conduct phase II multisite trials. The pharmaceutical biotechnology company COMPASS Pathways PLC is conducting a psilocybin therapy RCT for the treatment of TRD (NCT03775200), and the non-profit organization Usona Institute is conducting a psilocybin therapy RCT for the treatment of MDD (NCT03866174). Additional psilocybin studies for depression are taking place at various other sites including Johns Hopkins (depression associated with mild cognitive impairment; NCT04123314), Imperial College (MDD; NCT03429075), Yale (MDD; NCT03554174), University of Zurich (MDD; NCT03715127), and Central Institute of Mental Health/Charité Berlin (TRD; NCT04670081).
An important area of concern is identifying for whom psilocybin therapy is most clinically appropriate. In depressed patients, it will be important to consider various psychological, social, and genetic variables that may increase risk or predispose an individual to respond to psilocybin in a manner that is unsafe or ineffective. For instance, individuals presenting with acute suicidality might not be appropriate candidates for this type of intervention as these experiences can be acutely psychologically challenging and destabilizing. An additional consideration and area of research is which individual and situational features predict acute and longer-term responses to psilocybin. Baseline trait variables such as absorption, openness, and acceptance have been found to strongly moderate the effects of psychedelics (Hartogsohn 2016; Haijen et al. 2018). These and other factors should be carefully considered to help inform the development of optimal clinical and empirical guidelines, which will serve to mitigate adverse reactions and maximize the likelihood of positive therapeutic effects.
An additional challenge that clinician-researchers will face in the coming years is the development of rigorous, effective, and scalable clinical training methodologies. It will be important to establish training programs that ensure good clinical practice and that are structured, manualized, and closely monitored for quality assurance. Thoughtfully designed educational programs have been developed such as the training program at the California Institute of Integral Studies, which spearheaded the first academically accredited certificate program in Psychedelic-Assisted Therapy and Research in 2014 (Phelps 2017). Other programs have emerged, and many more are likely on the horizon. An additional key challenge facing clinicians and researchers are the barriers to dissemination and delivering the treatment at scale. Although only a couple of medication doses are typically required, current models are expensive as they involve intensive clinician time and high costs associated with regulatory challenges.
To overcome these limitations, additional research is needed. However, funding for psychedelic research in the U.S. is mostly restricted to private, philanthropic sources. It will be a critical landmark if/when the National Institutes of Health grants funding for advanced phase research into psilocybin for depression. Given the growing clinical evidence base, regulatory support, and cultural momentum surrounding this movement, public demand for further scientific inquiry may encourage such funding. This could enable a pathway for psilocybin to be rescheduled as a medication, making it available for therapeutic use in the treatment of depression in clinical populations.
8. Conclusion
The urgent need to address the mental health crisis associated with depression demands a dedicated approach to supporting quality research as well as the fortitude to pave a new road with innovative treatments that address the complex nature of such suffering. Psilocybin therapy may provide an opportunity to address the impact of debilitating depression as many people fail to respond to traditional behavioral, cognitive, and pharmacological evidence-based interventions. Although current research indicates that psilocybin therapy could improve depression, further research is needed with larger samples, more diverse participants, and across geographic settings. Furthermore, psilocybin therapy is not a panacea, human suffering is not a simple problem, and depression is a dynamic, heterogenous process. Even if psilocybin therapy garners regulatory approval in the coming years, it will not dissolve the structures and determinants that create an environment wherein a diathesis for depression is fostered. Whether the effects of psilocybin therapy will meet the impossibly high expectations it is garnering in the public is also yet to be determined. Nevertheless, because psilocybin therapy offers a disruptive pharmacological approach that threatens our current understanding of the chronic and debilitating lifetime course of depression, there is hope that it may offer an alternative effective treatment option for those in desperate need of relief.
Contributor Information
Gabrielle Agin-Liebes, Department of Psychiatry, University of California, San Francisco, San Francisco, CA, USA; Neuroscape, Sandler Neurosciences Center, San Francisco, CA, USA.
Alan K. Davis, Department of Psychiatry, College of Social Work, The Ohio State University, Columbus, OH, USA Center for Psychedelic and Consciousness Research, Johns Hopkins University, Baltimore, MD, USA.
References
- Aday JS, Davis AK, Mitzkovitz CM, Bloesch EK, Davoli CC (2021) Predicting reactions to psychedelic drugs: a systematic review of states and traits related to acute drug effects. ACS Pharmacol Transl Sci 4(2):424–435 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Agin-Liebes GI, Malone T, Yalch MM, Mennenga SE, Ponté KL, Guss J, Bossis AP, Grigsby J, Fischer S, Ross S (2020) Long-term follow-up of psilocybin-assisted psychotherapy for psychiatric and existential distress in patients with life-threatening cancer. J Psychopharmacol 34(2):155–166 [DOI] [PubMed] [Google Scholar]
- Araújo AM, Carvalho F, Bastos MD, Pinho PG, Carvalho M (2015) The hallucinogenic world of tryptamines: an updated review. Arch Toxicol 89(8):1151–1173 [DOI] [PubMed] [Google Scholar]
- Beck AT, Steer RA, Brown GK (1996) Beck depression inventory (BDI-II). Pearson [Google Scholar]
- Carhart-Harris RL, Friston KJ (2019) REBUS and the anarchic brain: toward a unified model of the brain action of psychedelics. Pharmacol Rev 71(3):316–344 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carhart-Harris RL, Erritzoe D, Williams T, Stone JM, Reed LJ, Colasanti A, Tyacke RJ, Leech R, Malizia AL, Murphy K, Hobden P (2012) Neural correlates of the psychedelic state as determined by fMRI studies with psilocybin. Proc Natl Acad Sci U S A 109(6):2138–2143 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carhart-Harris RL, Bolstridge M, Rucker J, Day CMJ, Erritzoe D, Kaelen M, Bloomfield M, Rickard J, Forbes B, Feilding A et al. (2016) Psilocybin with psychological support for treatment-resistant depression: an open label feasibility study. Lancet Psychiatry 3(7):619–627 [DOI] [PubMed] [Google Scholar]
- Carhart-Harris RL, Roseman L, Bolstridge M, Demetriou L, Pannekoek JN, Wall MB, Tanner M, Kaelen M, Mcgonigle J, Nutt DJ (2017) Psilocybin for treatment-resistant depression: fMRI-measured brain mechanisms. Sci Rep 7(1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carhart-Harris RL, Bolstridge M, Day CM, Rucker J, Watts R, Erritzoe DE, Kaelen M, Giribaldi B, Bloomfield M, Pilling S, Rickard JA (2018) Psilocybin with psychological support for treatment-resistant depression: six-month follow-up. Psychopharmacology (Berl) 235(2):399–408 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carhart-Harris R, Giribaldi B, Watts R, Baker-Jones M, Murphy-Beiner A, Murphy R, Martell J, Blemings A, Erritzoe D, Nutt DJ (2021) Trial of psilocybin versus escitalopram for depression. New Engl J Med 384(15):1402–1411 [DOI] [PubMed] [Google Scholar]
- Collimore KC, Rector NA (2014) Treatment of anxiety disorders with comorbid depression: a survey of expert CBT clinicians. Cogn Behav Pract 21(4):485–493 [Google Scholar]
- Coull G, Morris PG (2011) The clinical effectiveness of CBT-based guided self-help interventions for anxiety and depressive disorders: a systematic review. Psychol Med 41(11):2239–2252 [DOI] [PubMed] [Google Scholar]
- Cuijpers P, Sijbrandij M, Koole SL, Andersson G, Beekman AT, Reynolds CF (2014) Adding psychotherapy to antidepressant medication in depression and anxiety disorders: a meta-analysis. World Psychiatry 13(1):56–67 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis AK, Barrett FS, May DG et al. (2021a) Effects of psilocybin-assisted therapy on major depressive disorder: a randomized clinical trial. JAMA Psychiatry 78(5):481–489 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis AK, Xin Y, Sepeda ND, Garcia-Romeu A, Williams MT (2021b) Increases in psychological flexibility mediate the relationship between acute psychedelic drug effects and decreases in racial trauma symptoms among people of color. Chron Stress:1–10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Gregorio D, Enns JP, Nuñez NA, Posa L, Gobbi G (2018) d-lysergic acid diethylamide, psilocybin, and other classic hallucinogens: mechanism of action and potential therapeutic applications in mood disorders. Prog Brain Res 242:69–96 [DOI] [PubMed] [Google Scholar]
- Gaynes BN, Warden D, Trivedi MH, Wisniewski SR, Fava M, Rush AJ (2009) What did STAR*D teach us? Results from a large-scale, practical, clinical trial for patients with depression. Psychiatr Serv 60(11):1439–1445. 10.1176/ps.2009.60.11.1439 [DOI] [PubMed] [Google Scholar]
- Greenberg PE, Fournier A-A, Sisitsky T, Pike CT, Kessler RC (2015) The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J Clin Psychiatry 76(02):155–162. 10.4088/JCP.14m09298 [DOI] [PubMed] [Google Scholar]
- Griffiths RR, Johnson MW, Carducci MA, Umbricht A, Richards WA, Richards BD, Cosimano MP, Klinedinst MA (2016) Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: a randomized double-blind trial. J Psychopharmacol 30(12):1181–1197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gründer G, Mertens L (2021) Psilocybin for depression. N Engl J Med 385(9):863. [DOI] [PubMed] [Google Scholar]
- Haijen EC, Kaelen M, Roseman L, Timmermann C, Kettner H, Russ S, Nutt D, Daws RE, Hampshire AD, Lorenz R, Carhart-Harris RL (2018) Predicting responses to psychedelics: a prospective study. Front Pharmacol 9:897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamilton JP, Farmer M, Fogelman P, Gotlib IH (2015) Depressive rumination, the default-mode network, and the dark matter of clinical neuroscience. Biol Psychiatry 78(4):224–230 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hartogsohn I (2016) Set and setting, psychedelics and the placebo response: an extra-pharmacological perspective on psychopharmacology. J Psychopharmacol 30(12):1259–1267 [DOI] [PubMed] [Google Scholar]
- Hasin DS, Sarvet AL, Meyers JL et al. (2018) Epidemiology of adult DSM-5 major depressive disorder and its specifiers in the United States. JAMA Psychiatry 75(4):336. 10.1001/jamapsychiatry.2017.4602 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heifets BD, Malenka RC (2019) Disruptive psychopharmacology. JAMA Psychiatry 76(8):775–776 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hofmann SG, Asnaani A, Vonk IJ, Sawyer AT, Fang A (2012) The efficacy of cognitive behavioral therapy: a review of meta-analyses. Cognit Ther Res 36(5):427–440 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iannuzzo RW, Jaeger J, Goldberg JF, Kafantaris V, Sublette ME (2006) Development and reliability of the HAM-D/MADRS interview: an integrated depression symptom rating scale. Psychiatry Res 145(1):21–37 [DOI] [PubMed] [Google Scholar]
- Koen N, Stein DJ (2011) Pharmacotherapy of anxiety disorders: a critical review. Dialogues Clin Neurosci 13(4):423–437 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mertens LJ, Wall MB, Roseman L, Demetriou L, Nutt DJ, Carhart-Harris RL (2020) Therapeutic mechanisms of psilocybin: changes in amygdala and prefrontal functional connectivity during emotional processing after psilocybin for treatment-resistant depression. J Psychopharmacol 34(2):167–180 [DOI] [PubMed] [Google Scholar]
- Morilak DA, Frazer A (2004) Antidepressants and brain monoaminergic systems: a dimensional approach to understanding their behavioural effects in depression and anxiety disorders. Int J Neuropsychopharmacol 7(2):193–218. 10.1017/S1461145704004080 [DOI] [PubMed] [Google Scholar]
- Nemeroff CB (2007) Prevalence and management of treatment-resistant depression. J Clin Psychiatry 68(Suppl 8):17–25 [PubMed] [Google Scholar]
- Otto MW, Hearon BA (2016) Combination treatment for anxiety and mood disorders: benefits and issues for the combination of cognitive-behavioral therapy and pharmacotherapy. In: The Oxford handbook of cognitive and behavioral therapies. Oxford University Press, New York, pp 482–493 [Google Scholar]
- Phelps J (2017. Sep) Developing guidelines and competencies for the training of psychedelic therapists. J Humanist Psychol 57(5):450–487 [Google Scholar]
- Roseman L, Nutt DJ, Carhart-Harris RL (2018) Quality of acute psychedelic experience predicts therapeutic efficacy of psilocybin for treatment-resistant depression. Front Pharmacol 17(8):974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ross S, Bossis T, Guss J, Agin-Liebes G, Malone T, Cohen B, Mennenga S, Belser A, Kalliontzi K, Babb J et al. (2016) Rapid and sustained symptom reduction following psilocybin treatment for anxiety and depression in patients with life-threatening cancer: a randomized controlled trial. J Psychopharmacol 30(12):1165–1180 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rush AJ, Trivedi MH, Ibrahim HM, Carmody TJ, Arnow B, Klein DN, Markowitz JC, Ninan PT, Kornstein S, Manber R, Thase ME (2003) The 16-item quick inventory of depressive symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry 54(5):573–583 [DOI] [PubMed] [Google Scholar]
- Sinyor M, Schaffer A, Levitt A (2010) The sequenced treatment alternatives to relieve depression (star*d) trial: a review. Can J Psychaitry 55(3):126–135 [DOI] [PubMed] [Google Scholar]
- Snaith RP, Hamilton M, Morley S, Humayan A, Hargreaves D, Trigwell P (1995) A scale for the assessment of hedonic tone the Snaith–Hamilton Pleasure Scale. Br J Psychiatry 167(1):99–103 [DOI] [PubMed] [Google Scholar]
- Spielberger CD (2010) State-trait anxiety inventory. In: The Corsini encyclopedia of psychology, vol 30, p 1 [Google Scholar]
- Studerus E, Gamma A, Vollenweider FX (2010) Psychometric evaluation of the altered states of consciousness rating scale (OAV). PLoS One 5:e12412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trivedi MH, Rush AJ, Wisniewski SR, Nierenberg AA, Warden D, Ritz L, Norquist G, Howland RH, Lebowitz B, McGrath PJ, Shores-Wilson K (2006) Evaluation of outcomes with citalopram for depression using measurement-based care in STAR* D: implications for clinical practice. Am J Psychiatry 163(1):28–40 [DOI] [PubMed] [Google Scholar]
- Walker ER, McGee RE, Druss BG (2015) Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiatry 72(4):334. 10.1001/jamapsychiatry.2014.2502 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watts R, Day C, Krzanowski J, Nutt D, Carhart-Harris R (2017) Patients’ accounts of increased “connectedness” and “acceptance” after psilocybin for treatment-resistant depression. J Humanist Psychol 57(5):520–564 [Google Scholar]
- Williams MT, Davis AK, Xin Y, Sepeda ND, Grigas PC, Sinnott S, Haeny AM (2021) People of color in North America report improvements in racial trauma and mental health symptoms following psychedelic experiences. Drugs (Abingdon Engl) 28(3):215–226 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization. Depression fact sheet . World Health Organization. Published December 2019. Accessed 11 Jan 2020. http://www.who.int/mediacentre/factsheets/fs369/en/ [Google Scholar]
- Yaden DB, Griffiths RR (2020) The subjective effects of psychedelics are necessary for their enduring therapeutic effects. ACS Pharmacol Transl Sci 4(2):568–572 [DOI] [PMC free article] [PubMed] [Google Scholar]