

Abstract
Advanced practice registered nurses (APRNs) play a pivotal role in providing healthcare, including preventive care services, to the public. However, barriers to APRN practice exist that impact the provision of vital healthcare services that APRNs are authorized to provide based on their education, training, licensure, and certification. This article provides an overview of APRN barriers to practice, including in the face of the COVID-19 pandemic, and discusses key policy and regulatory implications.
Keywords: Advanced practice registered nurses, practice barriers, advanced practice nursing, COVID-19
Advanced practice registered nurses (APRNs), which include nurse practitioners (NPs), certified registered nurse anesthetists (CRNAs), certified nurse-midwives (CNMs), and clinical nurse specialists (CNSs) significantly contribute to meeting national healthcare needs (American Nurses Association [ANA], n.d.). Yet, they face regulatory barriers that limit their ability to provide care based on their educational preparation, training, and certification. The present article summarizes existing barriers (including practice authority restrictions, transition to practice requirements, federal regulations, and economic realities), highlights barrier changes related to COVID-19, and discusses the implications of related policies and regulations.
APRN Practice Barriers
APRN Practice Authority Variation by U.S. State
The American Association of Nurse Practitioners (AANP) defines three types of practice environments for the NP role in the United States: full, reduced, and restricted authority. The same classification is often used in association with other APRN roles. In states with full practice authority (FPA), practice regulations permit APRNs to (a) evaluate patients; (b) diagnose conditions; (c) order and interpret diagnostic tests; and (d) initiate and manage treatments, “including prescribing medications and controlled substances, under the exclusive licensure authority of the state board of nursing” (AANP, 2022a, 2022b). More than half of the 50 U.S. states (n = 26) are classified as FPA states (Figure 1 ) (AANP, 2022b).
FIGURE 1.
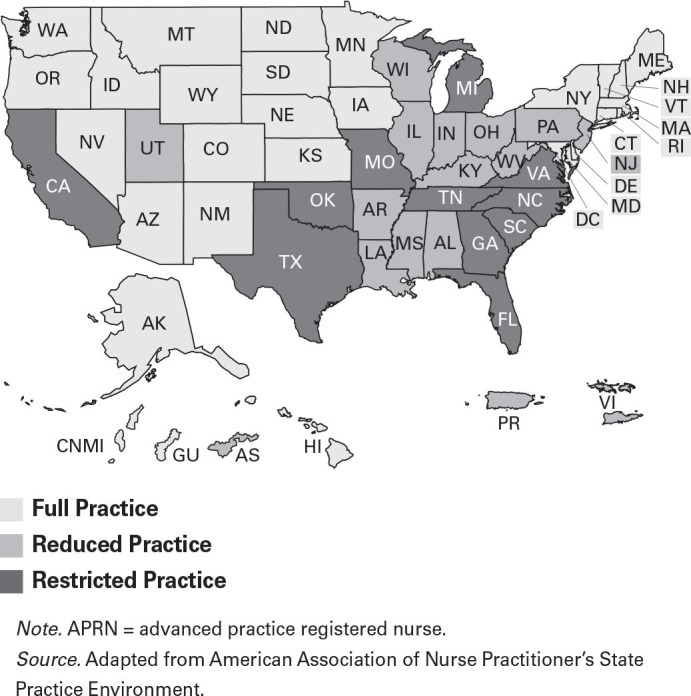
APRN Practice Authority Across the United States and Its Territories
In reduced practice states, “practice and licensure laws reduce the ability of NPs to engage in at least one element of NP practice.” State laws can require a “collaborative agreement with another health provider in order for NPs to provide patient care” or can limit “one or more elements of NP practice” (AANP, 2022b). Currently, 13 U.S. states are classified as reduced practice states (AANP, 2022b). In restricted practice states, “practice and licensure laws restrict the ability of NPs to engage in at least one element of NPs practice. State law requires career-long supervision, delegation, or team management by another health provider in order for the NP to provide care” (AANP, 2022b). Eleven states are classified as restricted practice states (AANP, 2022b).
APRN Transition To Practice Regulations
Transition to practice regulations require newly graduated APRNs to practice under the supervision or mentorship of an experienced clinician (Green, 2022). Transition to practice requirements have become more common in recent years, in part to assuage concerns from FPA opponents in FPA-resistant, often conservative, states and despite a dearth of evidence about the need for or the efficacy of transition to practice requirements. Such requirements vary considerably and are often not consistent with the APRN Consensus Model (National Council of State Boards of Nursing [NCSBN], n.d.-c). The common denominator is the imposition of required supervision or mentorship by an experienced clinician, commonly a physician or APRN, for newly graduated APRNs. The transition phase duration varies from 750 hours to up to several years of supervised practice (Green, 2022).
Transition to practice requirements are opposed by the Institute of Medicine (2011; now called the National Academy of Medicine), the American Association of Colleges of Nursing (2016), the AANP (2022a), and the ANA (2016). One of the four key messages of the initial Future of Nursing report is that nurses should practice to the full extent of their education (Institute of Medicine, 2011). All APRNs are educated to assume autonomous APRN practice according to competencies assessed by their respective accrediting bodies (American Association of Colleges of Nursing, 2016). The ANA (2016) asserted that transition to practice requirements are “not based on evidence but are the result of political compromise” (p. 2). Similarly, the AANP cites national standards for APRN education, program accreditation, and board certification as evidence-based and decries the unnecessary barriers to patients and NPs, noting geographic health disparities, higher chronic disease burden, primary care shortages, higher cost of care, and lower health-status rankings in non-FPA states compared with FPA states (AANP, 2022b). To add to practice confusion, the requirement for transition to practice varies by state regardless of APRN practice authority status. For example, 10 states with FPA have transition to practice requirements (Colorado, Connecticut, Massachusetts, Maryland, Maine, Minnesota, Nebraska, Nevada, South Dakota, Vermont), seven reduced or restricted practice states have transition to practice requirements (Arizona, California, Florida, Illinois, New York, Virginia, West Virginia), and 19 reduced or restricted practice states have no transition to practice requirements (Alabama, Georgia, Indiana, Kansas, Kentucky, Louisiana, Missouri, Michigan, Mississippi, North Carolina, New Jersey, Ohio, Oklahoma, Pennsylvania, South Carolina, Tennessee, Texas, Utah, Wisconsin) (Table 1 ) (Phillips, 2022).
TABLE 1.
State APRN Transition To Practice Requirements by Practice Authority Status
| Practice Authority Status | With Transition To Practice Requirements | Without Transition To Practice Requirements |
|---|---|---|
| Full Practice Authority | Colorado, Connecticut, Maine, Maryland, Massachusetts, Minnesota, Nebraska, Nevada, South Dakota, Vermont | Alaska, Arizona, Delaware, District of Columbia, Hawaii, Idaho, Iowa, Montana, New Hampshire, New Mexico, North Dakota, Oregon, Rhode Island, Washington, Wyoming |
| Reduced/Restricted Practice Authority | Arizona, California, Florida, Illinois, New York, Virginia, West Virginia | Alabama, Georgia, Indiana, Kansas, Kentucky, Louisiana, Michigan, Mississippi, Missouri, North Carolina, New Jersey, Ohio, Oklahoma, Pennsylvania, South Carolina, Tennessee, Texas, Utah, Wisconsin |
Source.Phillips, S. J. (2022). 34th annual APRN legislative update: Trends in APRN practice authority during the COVID-19 global pandemic. The Nurse Practitioner, 47(1), 21–47. https://doi.org/10.1097/01.NPR.0000802996.14636.1c
Federal Regulatory Barriers to APRN Practice
In addition to state practice regulations that restrict practice authority in reduced and restricted practice states, there are other practice barriers that restrict APRN practice, even in FPA states (Bosse et al., 2017; Hain & Fleck, 2014; Hastings-Tolsma et al., 2018; Lofgren et al., 2017; Peterson, 2017). These barriers include federal regulations, such as those from the Centers for Medicare & Medicaid Services (CMS), as well as institutional and organizational policies that inhibit APRN-provided care and services (Hastings-Tolsma et al., 2018; Lofgren et al., 2017). Institutional and organizational barriers include bylaws that limit APRN roles and authority, including lack of hospital privileges; issues with provider credentialing; limited clinical, admitting, and/or staff privileges; insurance; and reimbursement issues (Hastings-Tolsma et al., 2018; Lofren et al., 2017; Robert Wood Johnson Foundation, 2017). Other restrictions involve requirements for physician cosignatures for prescriptive and hospital admission capabilities, the inability of APRNs to be listed as the providers of record or to carry their own patient panels, and electronic health records that do not capture APRN care (Schirle et al., 2020). These practices interfere with the ability of APRNs to provide patient care follow-up, limit patients’ choice of providers, and limit APRNs’ visibility in care (Poghosyan et al., 2013; Anen & McElroy, 2015). Nonregulatory barriers may vary by practice or geographically within a single state as well as among states (Schorn et al., 2022).
Economic Barriers
For states with a reduced or restricted practice environment, a career-long collaborative practice agreement may be stipulated, which outlines the requirements for APRNs to practice with a physician (AANP, 2022b). Specific requirements may include supervision of procedures, requirements for on-site visits, review of documentation, limitations on medication prescriptions, and requirements for direct payment to the collaborating physician. A national survey of APRNs identified the economic burden and practice restrictions associated with collaborative practice agreements (Martin & Alexander, 2019). APRNs working in rural areas and in APRN-managed private clinics were one and a half to six times more likely to be assessed collaborative practice agreement fees, often exceeding $6,000 and up to $50,000 annually (Martin & Alexander, 2019).
Regulatory barriers also have macroeconomic implications, as revealed by an economic impact analysis conducted regarding the economic benefit of granting Tennessee APRNs FPA (Myers et al., 2020). In 2017 the baseline year of the study, Tennessee APRNs contributed more than $545 billion in total output to the statewide economy, and APRNs supported more than 43,727 jobs. The projected impact of Tennessee APRNs having FPA, projected from 2017 to 2025, was an additional 7,696 jobs and $958,737,154 in total output. Adding population growth, the Affordable Care Act, and inflation, the authors estimated an increase of 25,536 jobs and $3.2 billion in economic output (Myers et al., 2020).
Implications of Barriers to APRN Practice
Restrictive scope of practice imposed by regulatory and other barriers further constrain the ability of APRNs to practice commensurate with their level of education and experiences (Kleinpell et al., 2022). A recent study assessing the association between state scope-of-practice regulations, unsupportive practice environments, and self-reported ratings of quality of care in primary care practices located in healthcare professional shortage areas found that these items were associated with ratings of quality of care, with unsupportive environments having lower ratings of quality of care (Carthon et al., 2020). Another study assessing state limitations on APRN scope of practice in five states identified that scope-of-practice regulations adversely affected practice settings. In states where physician supervision was required, APRNs and agency leaders reported additional costs and administrative burdens related to obtaining and documenting supervision (Chapman et al., 2019). Implementation of FPA allows for more efficient use of APRNs and can increase access to healthcare services (Chapman et al., 2019). Indeed, national organizations such as the National Governors Association (2012), the Federal Trade Commission (2014), and the Bipartisan Policy Center (Collins, 2013) are supportive of FPA.
Overcoming current barriers affecting APRNs has been identified as a major challenge facing the nursing workforce by the recent Future of Nursing 2020–2030 report (National Academy of Medicine, 2021). Barriers to APRN practice reduce the productivity capacity of these healthcare professionals. Not permitting APRNs to practice to the full extent of their licensure and education decreases the types and amounts of healthcare services that can be provided for people who need care (National Academy of Medicine, 2021). As noted in the Future of Nursing 2020–2030 report, this restriction also has significant implications for addressing the disparities in access to healthcare between rural and urban areas. A recent systemic review revealed that FPA is associated with higher numbers of NPs in rural areas; in primary care where there is a shortage of physicians, FPA is associated with increased access to care and utilization of healthcare services, lower cost of care, and no decrease in quality of care (Yang et al., 2021; Xue et al., 2018).
As highlighted in the NCSBN’s 2022 Environmental Scan (NCSBN, 2022), regulators and nurse leaders are responsible for upholding rules and regulations of nursing practice as well as for ensuring that standards of care are met and patients are protected. Of equal importance is regulator awareness of the degree to which barriers continue to impact APRN practice and limit aspects of care that directly influence care quality and access. Nursing leaders can have a significant impact on removing nonregulatory barriers to practice, such as changing outdated hospital bylaws that restrict APRN practice. In turn, regulators can support efforts to remove unnecessary barriers to APRN practice.
Barriers to Practice Before and During the COVID-19 Pandemic: National APRN Study Findings
A U.S. survey was conducted in 2020 to describe state practice barriers prior to the COVID-19 pandemic, determine the effects of COVID-19 pandemic-related suspension of practice restrictions or waiver of select practice agreement requirements in states with reduced or restricted practice, and explore the effects of the COVID-19 pandemic on APRN practice (Kleinpell et al., 2021). A total of 7,467 APRNs responded, including NPs (n = 6,478, 86.8%), CRNAs (n = 592, 7.9%), CNMs (n = 278, 3.7%), and CNSs (n = 242, 3.2%). Respondents represented all 50 states, with the majority being in reduced practice authority states (n = 3,496, 46.8%), followed by states with restricted practice authority (n = 2,617, 35.0%), and then states with FPA (n = 1,354, 18.1%).
A number of barriers to APRN practice prior to the pandemic were identified, with most respondents (n = 6,334, 84.8%) stating that practice barriers limited their ability to provide care during the pandemic (Kleinpell et al., 2021). Various barriers to practice were identified in all states, including those with FPA, including restricted home health approval (n = 2,485, 33.3%), restricted hospital admitting privileges (n = 2,446, 32.8%), requirement of a physician signature to order durable medical supplies (n = 2,273, 30.4%), requirement of physician co-signature on orders (n = 1,708, 22.9%), restricted health insurance credentialing (n = 1,465, 19.6%), requirement for physician supervision for APRNs to conduct procedures within APRN scope of practice (n = 1,227, 16.4%), and others (Table 2 ).
TABLE 2.
Institutional APRN Barriers Reported by State Practice Authority Status
| Barrier | FPA | Reduced | Restricted |
|---|---|---|---|
| Visiting Nurse Service will not take orders, only physician referrals | ✔ | ||
| Orders for durable medical supplies require a physician signature | ✔ | ✔ | ✔ |
| Unable to sign an emergency psychiatric hold | ✔ | ||
| Physician has to repeat all physical examinations and sign all notes | ✔ | ||
| Social Security disability forms not honored without physician signature | ✔ | ||
| Can pronounce death but unable to sign death certificate | ✔ | ✔ | |
| Collaborating/supervising physician practice/population restricted | ✔ | ✔ | ✔ |
| Unable to clear child for hearing aids without physician signature | ✔ | ||
| Consultations and H&P require physician co-signature | ✔ | ||
| Unable to perform sports physicals | ✔ | ||
| Discharges from PACU or other units require physician signature | ✔ | ✔ | ✔ |
| Unable to order imaging for patients with abnormal mammogram | ✔ | ||
| Prescriptions require a physician signature (or co-signature) | ✔ | ✔ | ✔ |
| Patients have higher copay to see APRN | ✔ | ||
| Home health approval restricted | ✔ | ✔ | ✔ |
| Hospital bylaws restrictions on practice | ✔ | ✔ | ✔ |
| Insurance requires physician to be PCP | ✔ | ||
| 85% reimbursement | ✔ | ||
| Laboratory or imaging results given only to collaborating/supervising physician (not to APRN) | ✔ | ✔ | ✔ |
| Ordering blood products requires physician signature | ✔ | ||
| Pharmaceutical companies require physician signature for samples | ✔ | ||
| Procedures essential to anesthesia (e.g., regional/peripheral nerve blocks, invasive line placement) require physician supervision | ✔ | ✔ | ✔ |
| Procedures essential to quality care and within APRN scope require physician supervision | ✔ | ✔ | ✔ |
| Pronouncing death prohibited (including fetal death) | ✔ | ✔ | ✔ |
| Referral or consultation declined by other providers (only because you are an APRN) | ✔ | ✔ | ✔ |
| Requirement of physician co-signature on orders | ✔ | ✔ | ✔ |
| Pre- and postoperative assessments require physician signature | ✔ | ✔ | ✔ |
| Restricted health insurance credentialing | ✔ | ✔ | ✔ |
Note. APRN = advanced practice registered nurse; FPA = full practice authority; H&P = history and physical examination; PACU = post-anesthesia care unit; PCP = primary care provider.Responses have been lightly edited for journal style.
Source. Adapted from Kleinpell, R., Myers, C. R., Schorn, M. N., & Likes, W. (2021). Impact of COVID-19 pandemic on APRN practice: Results from a national survey. Nursing Outlook, 69(5), 783–792. https://doi.org/10.1016/j.outlook.2021.05.002
Other reported barriers based on institutional regulations rather than state regulations included requiring a physician signature for certain medications, inability to order rehabilitation services after hospital discharge, and inability to order do-not-resuscitate orders; these barriers were even reported by APRNs in FPA states. Overall, most respondents (n = 6,334, 84.8%) identified that practice barriers and restrictions in place before the pandemic further limited their ability as an APRN to provide care during the COVID-19 pandemic.
Changes in Regulations Since the Pandemic
As a result of the COVID-19 pandemic, changes were seen in state and federal regulations, and there has been new interest in the interstate licensure of APRNs and other healthcare providers.
State Regulatory Changes
At the outset of the COVID-19 pandemic in 2020, 22 states were classified as FPA, 16 as reduced practice authority, and 12 as restricted practice authority for NPs (AANP, 2020). In response to the pandemic, 5 reduced practice states temporarily lifted all practice restrictions, 11 reduced practice states and 2 restricted practice states granted temporary waivers of select practice restrictions, and 2 restricted practice states took no action (Kleinpell et al., 2021; Stucky et al., 2021).
Since the start of the COVID-19 pandemic in early 2020, there has been movement toward FPA in some states, including some of the emergency changes becoming permanent. For example, Massachusetts has since adopted FPA, and Arkansas now has a transition to practice provision that creates a path to FPA. Other advances in scope of practice authority occurred in Virginia, where transition to practice requirements were reduced from 5 years to 2 years. In six other states (Florida, Illinois, Louisiana, North Carolina, Oklahoma, and Pennsylvania), select practice authority restrictions have eased (Phillips, 2022).
Additionally, there have been other changes in reimbursement, roles, and APRN authority. In Arkansas, APRNs can now serve as primary care providers, primary care managers, and team leaders for family practice professionals and patient-centered medical homes; they can be reimbursed in the state’s Medicaid program; and they can serve as initial providers to Medicaid patients. Louisiana health plans must now cover CNM services. In Maine, CRNA services must now be covered. In Washington State, reimbursement was increased for APRN Medicaid providers (Phillips, 2022).
Federal Regulatory Changes
At the federal level, CMS removed some barriers to APRN practice in response to the COVID-19 pandemic. NPs are approved to provide certain medical services at skilled nursing facilities (CMS, 2022a) and to provide telehealth at long-term care facilities (CMS, 2022b). NPs are now permitted to certify Medicare home healthcare benefit eligibility and oversee patient care plans (CMS, 2022a). As a component of the Coronavirus Aid, Relief, and Economic Security (CARES) Act, NPs and CNSs are authorized to certify home healthcare for patients who are Medicare beneficiaries without physician approval (ANA, 2020). The pandemic led to changes for NPs, CNSs, CNMs, and physician assistants to supervise diagnostic tests. The interim rule applied to tests performed in physician offices, hospital outpatient departments, and provider-based facilities. CMS extended these reforms in its 2021 rules, but there is ambiguity in the new rules with respect to which levels of diagnostic tests allow supervision under the more flexible requirements (CMS, 2020; Greeson & Pitts, 2021).
The APRN Compact
The COVID-19 pandemic highlighted the potential value of the APRN Compact. The APRN Compact, developed and adopted by the NCSBN in 2020, permits APRNs to hold a single, multistate license that permits practice in other compact states. The implementation of the APRN Compact will be enacted when seven states have enacted the legislation necessary to become a compact state (NCSBN, n.d.-a, n.d.-b). At present, Delaware, North Dakota, and Utah are compact states; Delaware had a companion bill to the APRN compact while North Dakota was a FPA state prior to joining the APRN Compact (NCSBN, n.d.-a, n.d.-b; Phillips, 2022).
The APRN Compact aligns with the APRN Consensus Model (NCSBN, n.d.-c) and allows APRNs to practice in states with a single license. Multistate licenses benefit APRNs and other healthcare providers who are part of military families, those who provide locum tenens work, and those who complete online education, and they facilitate the mobilization of APRNs and other healthcare providers in emergencies and telehealth across state lines (Wilcox, 2022).
Addressing Challenges That Still Need Resolution
Significant restrictions on APRN practice persist at many levels. Currently, 11 states have restrictive NP practice authority (AANP, 2022a). In Tennessee, the executive waiver during the pandemic addressing some of these restrictions was lifted after only 3 months (Farmer, 2020; Tenn. Exec. Order No. 15, 2020), and efforts to remove practice authority restrictions were once again thwarted by the General Assembly in 2022.
The NCSBN has advocated for standardization of APRN practice authority based on the APRN Consensus Model and subsequently with the APRN Compact. These efforts have been blocked by significant policy variations across states in the adoption of the Consensus Model for a variety of state-specific—and often political—reasons (Buck, 2021). There are economic implications because reciprocity would limit the amount of money states receive for licensure of APRNs compared with the current requirement to pay for a license in every state in which an APRN practices. In addition, the AANP (2020) is opposed to the APRN Compact because the compact calls for practice hours as a prerequisite for a multistate APRN license. The AANP asserts this requirement conflicts with the Consensus Model for APRN Regulation and creates a potential financial burden for well-qualified APRNs and for practices with evidence to support this requirement (Kaplan, 2021). Additional other concerns include compact administration, which does not include a APRN Advisory Board; disparities across states, which could result in being disciplined across compact states; differences in initial licensure and renewal requirements; and variations across compact states in prescribing authority (Kaplan, 2021).
APRNs are still limited in what they are allowed to provide in skilled nursing facilities and long-term-care facilities (Oliver et al., 2014; Rantz et al., 2017). Inconsistent regulations regarding whether APRNs may conduct an initial comprehensive visit, write admission orders and treatments, and certify/recertify admissions based purely on whether the APRN is employed by the facility remain (U.S. Department of Health and Human Services, 2013).
Inequitable CMS payment for the same provider services is an ongoing problem. CMS pays NPs and CNSs at 80% of the lesser of the actual charge or 85% of the amount a physician receives for the same services (CMS, 2022a). In contrast, CNMs are paid at 80% of the actual charge or 100% of the amount a physician receives for the same service, whereas CRNAs are paid at 100% of physician payment (CMS, 2022a). Another disparity is “incident to” payment that requires NP billing to be done under a physician’s name (Bischof & Greenburg, 2021).
Policy Implications and Recommendations
Awareness of the variable state regulations on APRN practice that impact patient access to care and patient outcomes is important for state regulators, nurse leaders, and other stakeholders. Additionally, knowing the impact that practice barriers have on APRN practice and patient care should empower nurse regulators and leaders to advocate for removal of barriers to APRN practice. Policymaking regarding APRN practice authority is based more on politics and entrenched interests of organized medicine than evidence. Continued resistance to FPA persists despite the lack of evidentiary support for this position and despite support from a plethora of respected organizations.
The case for promoting FPA in the remaining 24 reduced and restricted practice states should focus on improving patient and population outcomes and reducing health and healthcare disparities. It is ineffective and inefficient to present FPA as a turf battle between physicians and APRNs. A population perspective, focused on population outcomes, costs, and the economic impact of improved health and healthcare on communities, should frame an evidence-based case for the value of FPA. To gain the support necessary to advance FPA in FPA-resistant states, it is imperative that APRNs and other advocates seek support from diverse stakeholders with a special emphasis on building support among the business and local and state government sectors.
Addressing the differences in perspectives between nursing organizations on transition to practice and the APRN Compact is another opportunity to build support for FPA. Nursing organizations need to work collaboratively to achieve consensus on important topics related to APRN practice authority for the priority purpose of improving access to high-quality, cost-effective care.
Lessons derived from experiences related to the COVID-19 pandemic must be translated into actionable policy solutions that support high-performing emergency and ongoing healthcare delivery. Gaining support for these policy solutions requires coordinated multi-sector discussions and decisions. The COVID-19 pandemic exposed the need for less variability in licensure requirements across U.S. states and the need to be nimbler when faced with a national emergency. The calls for national licensure are louder now because of difficulties faced during the pandemic and rapid growth in telehealth services. National initiatives, including the APRN Compact, with attention to minimizing variation in state rules and regulations, are needed to ensure that barriers to APRN practice are removed (NCSBN, n.d.-a, n.d.-b).
As identified in the Future of Nursing 2020-2030 report, until all APRNs are permitted to practice to the full extent of their education and training, significant and preventable gaps in access to care will continue (National Academy of Medicine, 2021). Academic institutions preparing APRNs can advocate and impact policy changes in states that do not have FPA, including supporting lobbying efforts within their state to remove unnecessary barriers to APRN practice. Nurse administrators and APRN leaders can act to reduce unnecessary health system practice barriers, which will in turn decrease unnecessary APRN barriers to practice (Kleinpell et al., 2022). Institutional barriers such as those related to the granting of hospital admitting and other privileges, organizational bylaws, provider credentialing policies and practices, and electronic medical records that do not capture APRN care should be addressed (Schirle et al., 2020). Ultimately, addressing barriers to APRN practice can help to enhance patient care and patient access to healthcare, improve health equity, and advance the APRN role.
Footnotes
Conflicts of Interest: None.
References
- American Association of Colleges of Nursing Adult-gerontology acute care and primary care NP competencies. 2016. https://www.aacnnursing.org/Portals/42/AcademicNursing/pdf/Adult-Gero-NP-Comp-2016.pdf
- American Association of Nurse Practitioners APRN Compact Licensure: The American Association of Nurse Practitioners (AANP) opposes the revised APRN Compact. 2020. https://www.aanp.org/advocacy/advocacy-resource/position-statements/aprn-compact-licensure
- American Association of Nurse Practitioners Issues at a glance: Full practice authority. 2022, October. https://www.aanp.org/advocacy/advocacy-resource/policy-briefs/issues-full-practice-brief Retrieved December 1, 2022 , from.
- American Association of Nurse Practitioners State practice environment. 2022, October. https://www.aanp.org/advocacy/state/state-practice-environment Retrieved December 1, 2022, from.
- American Nurses Association. (n.d.). Advanced practice registered nurse (APRN). Retrieved December 1, 2022, from https://www.nursingworld.org/practice-policy/workforce/what-is-nursing/aprn/
- American Nurses Association ANA’s principles for advanced practice registered nurse (APRN) full practice authority. 2016. https://www.nursingworld.org/~49f695/globalassets/docs/ana/ethics/principles-aprnfullpracticeauthority.pdf
- American Nurses Association Congress passes and the president signs into law third COVID-19 package. Capitol Beat. 2020 https://anacapitolbeat.org/2020/03/27/congress-passes-and-the-president-signs-into-law-third-covid-19-package/ [Google Scholar]
- Anen T., McElroy D. Infrastructure to optimize APRN practice. Nurse Leader. 2015;13(2):50–56. doi: 10.1016/j.mnl.2015.01.004. [DOI] [Google Scholar]
- Bischof A., Greenburg S.A. Post COVID-19 reimbursement parity for nurse practitioners. OJIN: The Online Journal of Issues in Nursing. 2021;26(2), Manuscript 3 https://ojin.nursingworld.org/table-of-contents/volume-26-2021/number-2-may-2021/post-covid-19-reimbursement-parity-for-nurse-practitioners/ [Google Scholar]
- Bosse J., Simmonds K., Hanson C., Pulcini J., Dunphy L., Vanhook P., Poghosyan L. Position statement: Full practice authority for advanced practice registered nurses is necessary to transform primary care. Nursing Outlook. 2017;65(6):761–765. doi: 10.1016/j.outlook.2017.10.002. [DOI] [PubMed] [Google Scholar]
- Buck M. An update on the Consensus Model for APRN regulation: More than a decade of progress. Journal of Nursing Regulation. 2021;12(2):23–33. doi: 10.1016/S2155-8256(21)00053-3. [DOI] [Google Scholar]
- Carthon M.B., Brom H., Nikpour J., Todd B., Aiken L., Poghosyan L. Supportive practice environments are associated with higher quality ratings among nurse practitioners working in underserved areas. Journal of Nursing Regulation. 2020;13(1):5–12. doi: 10.1016/S2155-8256(22)00028-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Medicare & Medicaid Services Summary of policies in calendar year (CY) 2020 Medicare physician fee schedule (MPFS) public health emergency (PHE) interim final rules [Pub 100-20] 2020, May 22. https://www.cms.gov/files/document/r10160otn.pdf
- Centers for Medicare & Medicaid Services Advanced practice registered nurses, anesthesiology assistants, & physician assistants. 2022. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/Medicare-Information-for-APRNs-AAs-PAs-Booklet-ICN-901623.pdf
- Centers for Medicare & Medicaid Services Physicians and other clinicians: CMS flexibilities to fight COVID-19. 2022. https://www.cms.gov/files/document/physicians-and-other-clinicians-cms-flexibilities-fight-covid-19.pdf
- Chapman S.A., Toretsky C., Phoenix B.J. Enhancing psychiatric mental health nurse practitioner practice: Impact of state scope of practice regulations. Journal of Nursing Regulation. 2019;10(1):35–43. doi: 10.1016/S2155-8256(19)30081-X. [DOI] [Google Scholar]
- Collins B. Bipartisan Policy Center; 2013, August 8. Strengthening the health professional workforce.https://bipartisanpolicy.org/blog/strengthening-health-professional-workforce/ [Google Scholar]
- Farmer B. WKNO 91.1 FM. 2020. TN nurse practitioners return to pre-pandemic paperwork as emergency rules expire.https://www.wknofm.org/post/tn-nurse-practitioners-return-pre-pandemic-paperwork-emergency-rules-expire#stream/0 [Google Scholar]
- Federal Trade Commission Policy perspectives: Competition and the regulation of advanced practice nurses. 2014, March. https://www.ftc.gov/reports/policy-perspectives-competition-regulation-advanced-practice-nurses
- Green S.B. Inside the Beltway. National Association of Pediatric Nurse Practitioners; 2022, February. Transition to practice.https://www.napnap.org/inside-the-beltway-february-2022/ [Google Scholar]
- Greeson T.W., Pitts P.W. ReedSmith; 2021, May 12. Diagnostic test supervision: CMS relaxes rules but also creates ambiguities.https://www.reedsmith.com/en/perspectives/outlook/2021/05/diagnostic-test-supervision-cms-relaxes-rules-but-also-creates-ambiguity?section=authors [Google Scholar]
- Hain D., Fleck L.M. Barriers to NP practice that impact healthcare redesign. OJIN: The Online Journal of Issues in Nursing. 2014;19(2) doi: 10.3912/OJIN.Vol19No02Man02. Manuscript 2. [DOI] [PubMed] [Google Scholar]
- Hastings-Tolsma M., Foster S.W., Brucker M.C., Nodine P., Burpo R., Camune B., Griggs J., Callahan T.J. Nature and scope of certified nurse-midwifery practice: A workforce study. Journal of Clinical Nursing. 2018;27(21-22):4000–4017. doi: 10.1111/jocn.14489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Institute of Medicine . National Academies Press; 2011. Future of nursing: Leading change, advancing health. [DOI] [PubMed] [Google Scholar]
- Kaplan L. Should NPs advocate for the APRN Compact? The Nurse Practitioner. 2021;46(10):14–15. doi: 10.1097/01.NPR.0000790520.41080.5a. [DOI] [PubMed] [Google Scholar]
- Kleinpell R., Myers C.R., Schorn M.N., Likes W. Impact of COVID-19 pandemic on APRN practice: Results from a national survey. Nursing Outlook. 2021;69(5):783–792. doi: 10.1016/j.outlook.2021.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kleinpell R., Myers C.R., Likes W., Schorn M. Breaking down institutional barriers to advanced practice registered nurse practice. Nursing Administration Quarterly. 2022;2:137–143. doi: 10.1097/NAQ.0000000000000518. [DOI] [PubMed] [Google Scholar]
- Lofgren M.A., Berends S.K., Reyes J., Wycoff C., Kinnetz M., Frohling A., Baker L., Whitty S., Dirks M., O’Brien M. Scope of practice barriers for advanced practice registered nurses: A state task force to minimize barriers. JONA: The Journal of Nursing Administration. 2017;47(9):465–469. doi: 10.1097/NNA.0000000000000515. [DOI] [PubMed] [Google Scholar]
- Martin B., Alexander M. The economic burden and practice restrictions associated with collaborative practice agreements: A national survey of advanced practice registered nurses. Journal of Nursing Regulation. 2019;9(4):22–30. doi: 10.1016/S2155-8256(19)30012-2. [DOI] [Google Scholar]
- Myers C.R., Chang C., Mirvis D., Stansberry T. The macroeconomic benefits of Tennessee APRNs having full practice authority. Nursing Outlook. 2020;68(2):155–161. doi: 10.1016/j.outlook.2019.09.003. [DOI] [PubMed] [Google Scholar]
- National Academy of Medicine . The National Academies Press; 2021. The future of nursing 2020-2030: Charting a path to achieve health equity. [PubMed] [Google Scholar]
- National Council of State Boards of Nursing. (n.d.-a). APRN Compact.https://www.ncsbn.org/aprn-compact.htm
- National Council of State Boards of Nursing. (n.d.-b). Key provisions of the APRN Compact.https://www.ncsbn.org/public-files/APRN_Key_Provisions_2020.pdf
- National Council of State Boards of Nursing. (n.d.-c). APRN consensus model: The consensus model for APRN regulation, licensure, accreditation, certification and education.https://www.ncsbn.org/aprn-consensus.htm
- National Council of State Boards of Nursing The NCSBN 2022 environmental scan: Resiliency, achievement, and public protection. Journal of Nursing Regulation. 2022;12:S3–S55. doi: 10.1016/S2155-8256(22)00015-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Governors Association The role of nurse practitioners in meeting increased demand for primary care. 2012, December 20. https://www.nga.org/center/issues/health-issues/the-role-of-nurse-practitioners-in-meeting-increasing-demand-for-primary-care/
- Oliver G.M., Pennington L., Revelle S., Rantz M. Impact of nurse practitioners on health outcomes of Medicare and Medicaid patients. Nursing Outlook. 2014;62(6):440–447. doi: 10.1016/j.outlook.2014.07.004. [DOI] [PubMed] [Google Scholar]
- Peterson M.E. Barriers to practice and the impact on health care: A nurse practitioner focus. Journal of Advanced Practice Oncology. 2017;8(1):74–81. [PMC free article] [PubMed] [Google Scholar]
- Phillips S.J. 34th annual APRN legislative update: Trends in APRN practice authority during the COVID-19 global pandemic. The Nurse Practitioner. 2022;47(1):21–47. doi: 10.1097/01.NPR.0000802996.14636.1c. [DOI] [PubMed] [Google Scholar]
- Poghosyan L., Nannini A., Clarke S. Organizational climate in primary care settings: Implications for nurse practitioner practice. Journal of the American Association of Nurse Practitioners. 2013;25(3):134–140. doi: 10.1111/j.1745-7599.2012.00765.x. [DOI] [PubMed] [Google Scholar]
- Rantz M.J., Birtley N.M., Flesner M., Crecelius C., Murray C. Call to action: APRNs in U.S. nursing homes to improve care and reduce costs. Nursing Outlook. 2017;65(6):689–696. doi: 10.1016/j.outlook.2017.08.011. [DOI] [PubMed] [Google Scholar]
- Robert Wood Johnson Foundation Charting Nursing’s Future: The case for removing barriers to APRN practice [Issue No. 30] 2017, March. https://www.rwjf.org/en/library/research/2017/03/the-case-for-removing-barriers-to-aprn-practice.html Retrieved from.
- Schirle L., Norful A.A., Rudner N., Poghosyan L. Organizational facilitators and barriers to optimal APRN practice: An integrative review. Health Care Management Review. 2020;45(4):311–320. doi: 10.1097/HMR.0000000000000229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schorn M.N., Myers C., Barroso J., Hande K., Hudson T., Kim J., Kleinpell R. Results of a national survey: Ongoing barriers to APRN practice in the United States. Policy, Politics, & Nursing Practice. 2022;23(2):118–129. doi: 10.1177/15271544221076524. [DOI] [PubMed] [Google Scholar]
- Stucky C.H., Brown W.J., Stucky M.G. COVID 19: An unprecedented opportunity for nurse practitioners to reform healthcare and advocate for permanent full practice authority. Nursing Forum. 2021;56(1):222–227. doi: 10.1111/nuf.12515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tenn. Exec. Order No. 15. 2020, March 19. https://publications.tnsosfiles.com/pub/execorders/exec-orders-lee15.pdf
- Wilcox L. CompHealth; 2022, August 30. What NPs and CRNAs need to know about the APRN Compact.https://comphealth.com/resources/aprn-compact-np-crna/ [Google Scholar]
- Xue Y., Kannan V., Greener E., Smith J.A., Brasch J., Johnson B.A., Spetz J. Full scope-of-practice regulation is associated with higher supply of nurse practitioners in rural and primary care health professional shortage counties. Journal of Nursing Regulation. 2018;8(4):5–13. doi: 10.1016/S2155-8256(17)30176-X. [DOI] [Google Scholar]
- Yang B.K., Johantgen M.E., Trinkoff A.M., Idzik S.R., Wince J., Tomilson C. Select nurse practitioner practice regulations and U.S. health care delivery outcomes: A systematic review. Medical Care Research and Review. 2021;78(3):183–196. doi: 10.1177/1077558719901216. [DOI] [PubMed] [Google Scholar]