

Abstract
Global climate change and extreme weather events are associated with epigenetic modifications in immune cells, leading to the possible increased risk and prevalence of allergies and autoimmune diseases.

Subject Categories: Evolution & Ecology, Molecular Biology of Disease, Respiratory System
Human activity, particularly the burning of fossil fuels and the industrialization of agriculture, has contributed to global climate change through the generation of carbon dioxide (CO2) and other greenhouse gases (GHGs). In 2019, GHG emissions were approximately 60 gigatons of CO2 equivalent (GtCO2‐eq), 54% higher than in 1990 (Intergovernmental Panel on Climate Change, 2022). GHGs, by trapping heat within the atmosphere, have raised Earth's average surface temperature by 1.1°C since preindustrial times. Deforestation and urbanization further exacerbate climate change by removing plants and trees, which have the ability to absorb and decrease atmospheric CO2 levels.
Elevated surface temperatures have altered global weather patterns and the frequency and severity of extreme weather events, including heat waves, droughts, sandstorms, wildfires, floods, and tropical storms. Wildfires release large amounts of toxic pollutants into the atmosphere that heighten the risk of pulmonary diseases and allergies (Intergovernmental Panel on Climate Change, 2022). Higher levels of CO2 and ozone (O3), along with a warmer climate, can expand the geographic spread of plants and lengthen their flowering season, thereby prolonging the pollen season. Pollen exposure elicits nasal congestion in people with allergic rhinitis and has been found to enhance susceptibility to respiratory viral infections such as COVID‐19, regardless of allergy status (Perera & Nadeau, 2022). Droughts, storms, and sandstorms also release large amounts of fine particular matter (PM) into the atmosphere, which again can elevate the risk of respiratory diseases and allergies. In summary, by increasing exposure to novel pollutants, allergens, and disease vectors, climate change may play a role in the development of allergic and autoimmune diseases (Fig 1).
Figure 1. Climate change, environmental pollutants, and allergic and autoimmune diseases.
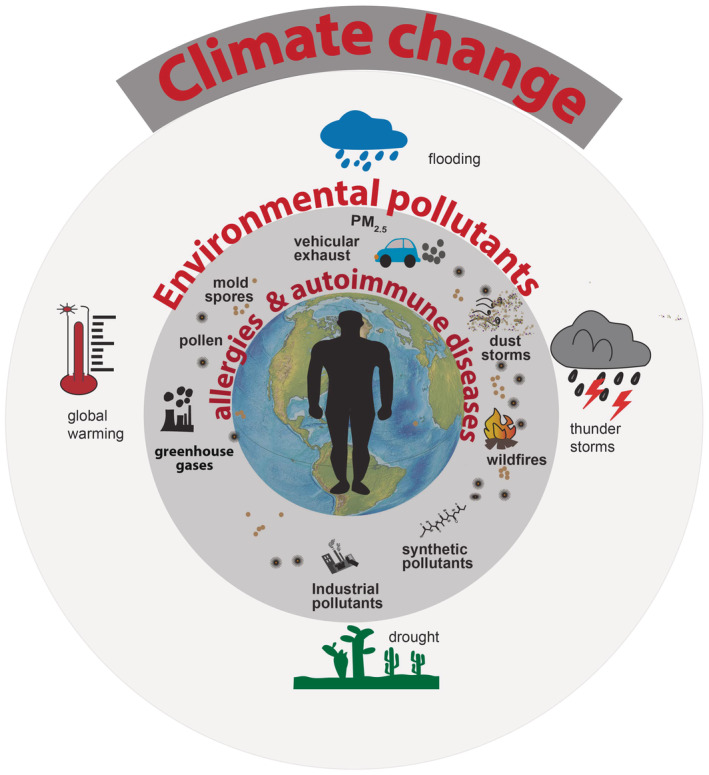
The outer circle of the figure represents the various factors that contribute to climate change, such as greenhouse gas emissions and wildfires. These factors lead to changes in temperature, humidity, and other environmental conditions, which can in turn alter the distribution and prevalence of allergens and autoimmune diseases.
… by increasing exposure to novel pollutants, allergens and disease vectors, climate change may play a role in the development of allergic and autoimmune diseases.
Epigenetic changes
Epigenetics mechanisms may mediate allergies and auto‐inflammatory diseases as exposure to extreme temperatures, pollen, and polycyclic aromatic hydrocarbons (PAHs)—organic chemicals generated by the combustion of organic materials—can lead to epigenetic changes that promote inflammation and disease development. These mechanisms, involving DNA and RNA modifications, may regulate canonical allergic pathways in gene–environment interactions.
Recent studies have highlighted the unique role of PAHs in the epigenetic remodeling of immune cells (Intergovernmental Panel on Climate Change, 2022). Owing to their small size, PAHs infiltrate cells lining the bronchial mucosa and bind to aryl hydrocarbon receptors (AhRs). An AhR bound to its ligand then forms an active complex with aryl nucleotide receptor translocator (ARNT). The AhR‐ARNT complex subsequently binds with xenobiotic response elements on enhancer regions of genes such as cytochrome P450 (CYP), thereby increasing their expression. CYP mediates the conversion of PAHs, such as benzo[a]pyrene, and other pollutants into reactive diol‐epoxide intermediates. These compounds covalently bind to DNA's nitrogenous bases, resulting in adduct formation at CpG island regions. This process is associated with alterations in methylation patterns in genes encoding specific immune signaling molecules, including upregulation of GATA‐3, a T‐helper type 2 (Th2) transcription factor, and prototypic Th2 cytokines, such as interleukin (IL)‐4, IL‐5, IL‐9, and IL‐13. The epigenetic relationship between PAH exposure and asthma has further been linked to abnormal methylation patterns in regulatory T cell function.
Epigenetic mechanisms are also involved in allergic reactions to pollen. Upon entry into the respiratory system, pollen proteins are recognized by dendritic cells and pollen‐derived antigens are presented to naïve T‐helper cells. Once activated, these cells differentiate into Th2 cells and produce Th2 cytokines that promote the activation and proliferation of other immune cells such as eosinophils and B cells. There is increasing evidence that transcriptional control of Th differentiation by epigenetic regulation—that is, methylation or histone acetylation—may be an important way by which differentiation and cytokine memory of Th subtypes are controlled. These epigenetic modifications regulate the expression of genes that maintain the Th2 cell phenotype and promote the persistence of pollen‐induced inflammation, which can eventually lead to allergic asthma (Tumes et al, 2017).
Given epigenetic and other mechanistic links between pollen exposure and allergies, the prevalence of allergies and autoimmune disorders may increase in future. Models of climate‐driven changes in pollen‐emission season length and magnitude suggest that extreme weather can raise pollen concentrations, thus increasing exposure to pollen and the risk of asthma and allergic rhinitis (Klingbeil et al, 2014). A study by Paudel et al (2021) used time‐series regression models between 2002 and 2019 to show that the number of weeks per year without any pollen in the atmosphere decreased over time. When working with an autoregressive integrated moving model on mold, pollen, and meteorological data, they also found that the concentrations of weed and tree pollens were positively associated with temperature and precipitation changes, respectively (Paudel et al, 2021).
Given epigenetic and other mechanistic links between pollen exposure and allergies, the prevalence of allergies and autoimmune disorders may increase in the future.
Allergic mechanisms
There has been great progress in understanding mechanisms by which the environment can mediate immune reactions and allergy risks. These pathways generally begin with environmental assaults that lead to epithelial barrier disfunction and penetration of both allergens and pollutants into underlying tissue. In the human gut, the loss of epithelial integrity, sometimes referred to as leaky gut syndrome, can permit the entry of endotoxins into the intestinal lumen. In the respiratory tract, a disrupted epithelium may increase the risk of infections by facilitating the passage of respiratory pathogens. For instance, the loss of barrier integrity in atopic dermatitis has been associated with greater concentrations of Staphylococcus aureus.
The mechanism by which loss of epithelial barrier integrity and entry of allergens mediate allergenic responses starts with the release of proinflammatory cytokines, thymic stromal lymphopoietin (TSLP), IL‐25, and IL‐33 by keratinocytes. These molecules are also known as alarmins, as they “sound the alarm” and facilitate the conversion of naive T cells to proinflammatory Th2 cells with the release of type 2 inflammatory cytokines, such as IL‐4, IL‐5, IL‐9, and IL‐13. Alarmins also mediate immunoglobulin E (IgE) class switching by B cells and release of allergen‐specific IgE, which then bind to FcεRI receptors and prime mast cells and basophils. Further encounters with allergens facilitate crosslinking of FcεRI‐bound IgE antibodies, leading to the degranulation of mast cells and basophils and the release of inflammatory mediators: histamine, prostaglandin D2, leukotrienes, and tryptase. Intolerance in the immune pathway leads to the differentiation of naïve T cells into CD4+ regulatory T cells and the production of transforming growth factor beta (TGF‐β) and IL‐10, which promote class switching of B cells to secrete immunoglobulin G4 (IgG4) and immunoglobulin A (IgA). IgG4 attaches to IgE and prevents its binding to FcεRI receptors on mast cells and basophils, and IgA binds antigens by preventing attachment of the antigen to barrier surfaces (Tomar & Hogan, 2020).
Air pollutants can also stimulate immune cells through pathways involving toll‐like receptors, reactive oxygen species, or aryl hydrocarbon receptors to activate proinflammatory signals and support the inflammatory response through synergistic effects. An in vitro cell culture study showed that stimulation with pollutant extracts of bronchial epithelial cells increased the production of proinflammatory cytokines (for instance, IL‐1α, IL‐1β, IL‐6, and IL‐8), while particulate matter stimulated proinflammatory cytokine production with macrophages (Mitschik et al, 2008).
Extreme weather and respiratory diseases
With intensifying climate change, increased the accumulation of flammable material in forests, and shifting land management practices, local fire seasons are gradually starting earlier and ending later. Wildfire events worldwide are growing more extreme in terms of area, duration, intensity, casualties, and property loss. Recent years have seen increasingly devastating wildfires in the Amazon Rainforest (2019), Australia (2019–2020), Siberia (2020–2021), the USA (2020), and Europe (2022). Wildfires contribute significantly to air pollution by releasing PM and CO2, carbon monoxide (CO), complex hydrocarbons, NOx, trace minerals, heavy metals, and other toxic and carcinogenic compounds (European Environment Agency, 2022). Many studies have reported increased rates of respiratory diseases, such as asthma and chronic obstructive pulmonary disease (COPD), after exposure to wildfires.
Many studies have reported increased rates of respiratory diseases, such as asthma and chronic obstructive pulmonary disease (COPD), after exposure to wildfires.
One wildfire‐related pollutant of growing concern to respiratory health is PM. Its composition and size are highly variable with a mix of both inorganic and organic man‐made substances. PM may include silicates, clay, minerals, quartz, silicon dioxide, and heavy metals and can carry pollen, fungal spores, bacteria, and viruses for thousands of miles. PM10 (particles with a diameter of 10 micrometers or less) are small enough to enter the respiratory tract, and PM2.5 (particles with a diameter of 2.5 micrometers or less) are small enough to enter the blood circulation and cause systemic inflammation. Long‐term exposure to PM has been associated with a greater risk of autoimmune diseases, particularly rheumatoid arthritis, connective tissue diseases, inflammatory bowel disease, and lupus. People with chronic exposure to PM2.5 at levels higher than 20 μg/m3 may have a 13% higher risk of developing autoimmune diseases such as rheumatoid arthritis and multiple sclerosis (Adami et al, 2022).
A 2019 study in the EU found that general PM2.5 exposure was correlated with 175,702 years lived with disabilities attributable to chronic obstructive pulmonary disease in 30 countries. Exposure to nitrogen dioxide (NO2) was linked to 175,070 years lived with disabilities such as diabetes mellitus type 2 (DM2). Lower respiratory tract infections attributable to acute ozone exposure were associated with 12,253 hospital admissions in 23 European countries (European Environment Agency, 2022). In addition, a retrospective analysis of people exposed to wildfire smoke versus those not exposed showed associations between exposure and two key proinflammatory markers, C‐reactive protein (CRP) and IL‐1β (Prunicki et al, 2020). Greater concentrations of CRP have been previously linked with airway inflammation and obstruction, suggesting the protein's potential to serve as a biomarker for asthmatic airway inflammation, while IL‐1β may serve important functions in inflammasome stimulation (Prunicki et al, 2020). These findings are supported by larger studies in moderately polluted areas unaffected by wildfire exposure. For instance, exposure to PM10 was similarly associated with elevated levels of IL‐1β in adults in Lausanne, Switzerland, and exposure to PM2.5 was associated with greater concentrations of CRP in adults in Boston, USA. When considering how minor increases in inflammatory cytokine concentrations may have the potential to poorly affect cardiovascular health, the observation of these two key inflammatory markers across populations exposed to wildfires or air pollutants is especially concerning (Prunicki et al, 2020).
Anthropogenic climate change has also exacerbated the frequency of sand and dust storms, primarily in Northern Africa and Asia, that release particulate matter. A 2008 study conducted in Nicosia, Cyprus, reported significantly elevated cardiovascular hospital admissions during Saharan dust storms. Another study in Madrid, Spain, found that daily mean concentrations of PM2.5 were 1.4 times higher and 1.9 times higher for PM10–2.5 on days of Saharan dust storms (Tobías et al, 2011).
A 2008 study conducted in Nicosia, Cyprus, reported significantly elevated cardiovascular hospital admissions during Saharan dust storms.
Other extreme weather events like thunderstorms and flooding continue to grow in severity. In a phenomenon known as thunderstorm asthma, weather conditions can break down pollen either by electric charge or osmotic rupture into smaller fragments that can more easily penetrate the lungs and trigger allergic asthma attacks in vulnerable individuals. An often‐cited and catastrophic example of thunderstorm asthma occurred in the UK in 1997, when a thunderstorm was linked to 640 hospital visits during a 30‐h period, nearly 10 times the expected number. Similarly, following a 2004 thunderstorm in Naples, Italy, seven cases of bronchial asthma attacks resulted in emergency department visits, one of which was escalated to the intensive care unit (D'Amato et al, 2016).
In addition, greater fungal growth and allergenic mold spores have been observed in floods ensuing thunderstorms. Moreover, a study conducted by the European Community Respiratory Health Survey found that indoor mold exposure, which was highest in homes with recent water damage, was associated with a higher prevalence of asthma (Zock et al, 2002).
Climate change's influence on human health is not limited to seasonal allergies and asthma. Its rapid and intensifying nature may have aided the global spread of disease vectors, such as Aedes aegypti mosquitos and lone star ticks. The lone star tick is associated with the alpha‐gal syndrome, which is more commonly known as red meat allergy, in parts of Europe, Australia, Asia, South Africa, and South and Central America. By transmitting a sugar called alpha‐gal into a person's bloodstream, the tick elicits an allergic reaction characterized by hives, swelling, difficulty breathing, and anaphylaxis in humans after consumption of mammal meat (Altshuler et al, 2021).
Policy recommendations
The 2015 UN Paris Accord announced the signatories' goal of reducing global GHG emissions and halting the increase in global temperature to 1.5°C above preindustrial levels. This accord was a major milestone and paved the way for the One Health Approach that strives to balance and optimize the health of people, animals, and the environment to address the impact of climate change. However, in 2022, the UN Intergovernmental Panel on Climate Change (IPCC) warned that the “current plans to address climate change are not ambitious enough to limit warming to 1.5°C above preindustrial levels—a threshold scientists believe is necessary to curtail catastrophic impacts” (Intergovernmental Panel on Climate Change, 2022).
These findings have highlighted the critical state of the situation and fostered greater collaboration globally. Nevertheless, additional action is needed at the individual, local, national, and international scales. Decreasing fossil fuel consumption remains of utmost importance, and ongoing strategies include transitioning toward sustainable energy sources. The recent nuclear fusion breakthrough by scientists at the Lawrence Livermore Laboratory, USA, offers tremendous hope for a future of an abundant clean source of energy, but it will take many more years before fusion can provide a safe and sustainable energy source.
Other strategies to address climate change include reforestation and restoration of habitats to increase the biodiversity of animal and plant life. Greening and biodiversity have also been positively associated with immune health: children enrolled in daycare characterized by a biodiverse yard area were shown to have a greater concentration of healthy bacteria and a lower risk of allergies compared with control groups (Roslund et al, 2020). At the 2022 UN Biodiversity conference, delegates from nearly 200 countries approved a sweeping UN agreement to protect 30 percent of the planet's land mass and oceans by 2030 and to implement proactive measures to prevent biodiversity loss. In addition to mitigation measures, adaptation strategies are also needed. For instance, people plagued by extreme air pollution like wildfires would benefit from clean‐air refuges that reduce exposure to PM by adding high‐efficiency air filters and limit indoor air pollution.
Even if worldwide warming is successfully limited at 1.5°C above preindustrial levels, the scientific and epidemiological evidence suggest that allergic and autoimmune diseases may continue to climb in prevalence and severity, further affecting vulnerable populations. More evidence and knowledge are necessary to define the extent of the situation ahead, inform public health and environmental policies, and improve healthcare systems. The additional investigation should include more comprehensive, longitudinal studies on health consequences linked to displacement and stress triggered by extreme weather events in groups at higher risk such as children or pregnant women. Such research would allow for better characterization of underlying immunological mechanisms and pathways. As global leaders continue to implement mitigation and adaptation practices, principles of justice, equity, diversity, and inclusion should inform policymaking. Communities of lower socio‐economic standing bear a disproportionate burden of climate change and have limited resources to meet these challenges.
More evidence and knowledge are necessary to define the extent of the situation ahead, inform public health and environmental policies, and improve healthcare systems.
Moreover, studies should look at the health outcomes of mitigation and adaptation approaches, such as limiting PM2.5 exposure by limiting household fossil fuel usage, and the potential cost‐effectiveness of these strategies. By modeling prospective reductions in hospitalizations and other medical expenses, these analyses could incentivize rapid implementation of mitigation and adaptation policies and interventions. Such frameworks will require a multidisciplinary perspective, involving collaboration between researchers, policymakers, and practitioners to ensure that the most effective strategies are developed and implemented. The onus lies on physicians and climate scientists alike to draw attention to these related issues so that concrete steps can be taken by policymakers toward transitioning to a more equitable, sustainable, biodiverse, and healthy future.
Author contributions
Alexandra S Lee: Conceptualization; writing – original draft; writing – review and editing. Juan Aguilera: Writing – review and editing. Jo Ann Efobi: Writing – review and editing. Youn Soo Jung: Writing – review and editing. Hana Seastedt: Writing – original draft; writing – review and editing. Mihir M Shah: Writing – original draft; writing – review and editing. Emily Yang: Writing – review and editing. Katherine Konvinse: Writing – review and editing. Paul J Utz: Writing – review and editing. Vanitha Sampath: Writing – original draft; writing – review and editing. Kari C Nadeau: Writing – original draft; writing – review and editing.
Disclosure and competing interests statement
Dr. Kari Nadeau reports grants from the National Institute of Allergy and Infectious Diseases (NIAID), the National Heart, Lung and Blood Institute (NHLBI), the National Institute of Environmental Health Sciences (NIEHS), and the Food Allergy Research & Education (FARE); Director of World Allergy Organization (WAO), advisor at Cour Pharma, co‐founder of Before Brands, Alladapt, Latitude, and IgGenix; and the National Scientific Committee member at Immune Tolerance Network (ITN) and the National Institutes of Health (NIH) clinical research centers, outside the submitted work; patents include, “Mixed allergen composition and methods for using the same,” “Granulocyte‐based methods for detecting and monitoring immune system disorders,” and “Methods and Assays for Detecting and Quantifying Pure Subpopulations of White Blood Cells in Immune System Disorders.” Dr. Konvinse is supported by NIH NHLBI funds R38 HL143615. All other authors have nothing to disclose.
Supporting information
Review Process File
Acknowledgements
This study was funded by the Sean N. Parker Center for Allergy and Asthma Research at Stanford University and NIH NHLBI funds R38 HL143615.
EMBO reports (2023) 24: e56821
References
- Adami G, Pontalti M, Cattani G, Rossini M, Viapiana O, Orsolini G, Benini C, Bertoldo E, Fracassi E, Gatti D et al (2022) Association between long‐term exposure to air pollution and immune‐mediated diseases: a population‐based cohort study. RMD Open 8: e002055 [DOI] [PMC free article] [PubMed] [Google Scholar]
- European Environment Agency (2022) Air quality in Europe 2022.
- Altshuler E, Kirkpatrick J, Aryan M, Miralles F (2021) Mammalian meat allergy emerges after tick‐bite: the alpha gal syndrome. BMJ Case Rep 14: e245488 [DOI] [PMC free article] [PubMed] [Google Scholar]
- D'Amato G, Vitale C, D'Amato M, Cecchi L, Liccardi G, Molino A, Vatrella A, Sanduzzi A, Maesano C, Annesi‐Maesano I (2016) Thunderstorm‐related asthma: what happens and why. Clin Exp Allergy 46: 390–396 [DOI] [PubMed] [Google Scholar]
- Intergovernmental Panel on Climate Change (2022) Climate change 2022: impacts, adaptation and vulnerability 2022. https://www.ipcc.ch/report/sixth‐assessment‐report‐working‐group‐ii/. Accessed December 13, 2022
- Klingbeil EC, Hew KM, Nygaard UC, Nadeau KC (2014) Polycyclic aromatic hydrocarbons, tobacco smoke, and epigenetic remodeling in asthma. Immunol Res 58: 369–373 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitschik S, Schierl R, Nowak D, Jörres R (2008) Effects of particulate matter on cytokine production in vitro: a comparative analysis of published studies. Inhal Toxicol 20: 399–414 [DOI] [PubMed] [Google Scholar]
- Paudel B, Chu T, Chen M, Sampath V, Prunicki M, Nadeau KC (2021) Increased duration of pollen and mold exposure are linked to climate change. Nat Sci Rep 11: 12816 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perera F, Nadeau K (2022) Climate change, fossil‐fuel pollution, and children's health. N Engl J Med 386: 2303–2314 [DOI] [PubMed] [Google Scholar]
- Prunicki MM, Dant CC, Cao S, Maecker H, Haddad F, Kim JB, Snyder M, Wu J, Nadeau K (2020) Immunologic effects of forest fire exposure show increases in IL‐1β and CRP. Allergy 75: 2356–2358 [DOI] [PubMed] [Google Scholar]
- Roslund MI, Puhakka R, Grönroos M, Nurminen N, Oikarinen S, Gazali AM, Cinek O, Kramná L, Siter N, Vari HK et al (2020) Biodiversity intervention enhances immune regulation and health‐associated commensal microbiota among daycare children. Sci Adv 6: eaba2578 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tobías A, Pérez L, Díaz J, Linares C, Pey J, Alastruey A, Querol X (2011) Short‐term effects of particulate matter on total mortality during Saharan dust outbreaks: a case‐crossover analysis in Madrid (Spain). Sci Total Environ 412–413: 386–389 [DOI] [PubMed] [Google Scholar]
- Tomar S, Hogan SP (2020) Recent advances in mechanisms of food allergy and anaphylaxis. F1000Res 9: 863 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tumes DJ, Papadopoulos M, Endo Y, Onodera A, Hirahara K, Nakayama T (2017) Epigenetic regulation of T‐helper cell differentiation, memory, and plasticity in allergic asthma. Immunol Rev 278: 8–19 [DOI] [PubMed] [Google Scholar]
- Zock JP, Jarvis D, Luczynska C, Sunyer J, Burney P, European Community Respiratory Health Survey (2002) Housing characteristics, reported mold exposure, and asthma in the European Community Respiratory Health Survey. J Allergy Clin Immunol 110: 285–292 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Review Process File