

Abstract
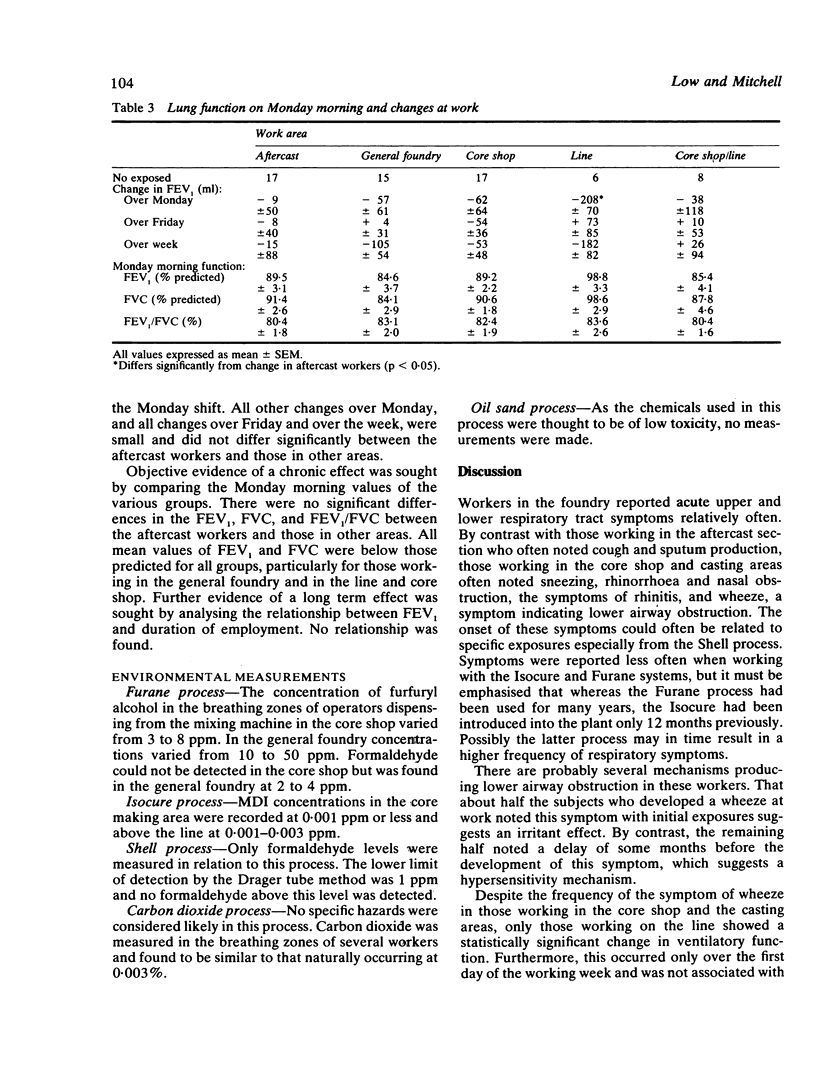
A survey was carried out in a steel foundry in Brisbane to evaluate the nature and frequency of respiratory symptoms and to assess ventilatory function. The foundry used many moulding processes including the Furane, Isocure, Shell, carbon dioxide, and oil sand systems. Nasal symptoms and wheeze were often reported, particularly by workers in the general foundry and core shop, and on a semiautomated line. By contrast, workers in the aftercast section not exposed to fumes or vapours from the various moulding processes reported these symptoms less often. Of 46 workers exposed to moulding fumes and vapours, 11 had developed a wheeze while working at the foundry. Wheeze and other respiratory tract symptoms were often attributed by the workers to exposure to substances at work, particularly from the Shell process which uses phenol formaldehyde resin and hexamethylenetetramine. Symptoms were reported also, but less often, on exposure to materials used in the Furane process (urea formaldehyde and furfuryl alcohol) and the Isocure process (methylene diphenyl diisocyanate, phenol formaldehyde, and dimethylethylamine). Ventilatory function studied over Monday and Friday showed a small and inconsistent changes. The six subjects working on the semiautomated line showed a small decrease in FEV1 (+/- SEM) (208 +/- 70 ml) only on Monday; this differed significantly from that in 17 aftercast workers (9 +/- 50 ml, p less than 0.05). Ventilatory function recorded before work on Monday morning showed no evidence of chronic airway obstruction in any group. Most environmental measurements were below the threshold limit values (TLV) except in the general foundry, where furfuryl alcohol was detected at concentrations of up to 50 ppm and formaldehyde at 4 ppm. The onset of symptoms in relation to exposure to various fumes and vapours suggests that both irritant and hypersensitivity mechanisms are present. As environmental modifications had occurred recently the apparent hypersensitivity may relate to past exposure levels above the TLV.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Cockcroft D. W., Cartier A., Jones G., Tarlo S. M., Dolovich J., Hargreave F. E. Asthma caused by occupational exposure to a furan-based binder system. J Allergy Clin Immunol. 1980 Dec;66(6):458–463. doi: 10.1016/0091-6749(80)90006-8. [DOI] [PubMed] [Google Scholar]
- Gibson J., Gallagher H., Johansen A., Webster I. Lung function in an Australian population: 1. Spirometric standards for non-smoking adults. Med J Aust. 1979 Apr 7;1(7):292–295. doi: 10.5694/j.1326-5377.1979.tb112111.x. [DOI] [PubMed] [Google Scholar]
- Malo J. L., Zeiss C. R. Occupational hypersensitivity pneumonitis after exposure to diphenylmethane diisocyanate. Am Rev Respir Dis. 1982 Jan;125(1):113–116. doi: 10.1164/arrd.1982.125.1.113. [DOI] [PubMed] [Google Scholar]
- Marazzini L., Pelosi V., Vezzoli F., Pennasi R., Longhini E. Prospective study of airway obstruction in a population with small airway disease. Bull Eur Physiopathol Respir. 1977 Mar-Apr;13(2):219–229. [PubMed] [Google Scholar]
- Mikov M. I. Chronic bronchitis in foundry workers in Vojvodina: ventilatory capacity in foundry workers. Arch Environ Health. 1974 Nov;29(5):261–267. doi: 10.1080/00039896.1974.10666584. [DOI] [PubMed] [Google Scholar]
- Peters J. M., Murphy R. L., Ferris B. G., Jr Ventilatory function in workers exposed to low levels of toluene diisocyanate: a six-month follow-up. Br J Ind Med. 1969 Apr;26(2):115–120. doi: 10.1136/oem.26.2.115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schoenberg J. B., Mitchell C. A. Airway disease caused by phenolic (phenol-formaldehyde) resin exposure. Arch Environ Health. 1975 Dec;30(12):574–577. doi: 10.1080/00039896.1975.10666782. [DOI] [PubMed] [Google Scholar]