

Abstract
Background
Sutures (stitches), staples and adhesive tapes have been used for many years as methods of wound closure, but tissue adhesives have entered clinical practice more recently. Closure of wounds with sutures enables the closure to be meticulous, but the sutures may show tissue reactivity and can require removal. Tissue adhesives offer the advantages of an absence of risk of needlestick injury and no requirement to remove sutures later. Initially, tissue adhesives were used primarily in emergency room settings, but this review looks at the use of tissue adhesives in the operating room/theatre where surgeons are using them increasingly for the closure of surgical skin incisions.
Objectives
To determine the effects of various tissue adhesives compared with conventional skin closure techniques for the closure of surgical wounds.
Search methods
In March 2014 for this second update we searched the Cochrane Wounds Group Specialised Register; The Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library); Ovid MEDLINE; Ovid MEDLINE (In‐Process & Other Non‐Indexed Citations); Ovid EMBASE and EBSCO CINAHL. We did not restrict the search and study selection with respect to language, date of publication or study setting.
Selection criteria
Only randomised controlled trials were eligible for inclusion.
Data collection and analysis
We conducted screening of eligible studies, data extraction and risk of bias assessment independently and in duplicate. We expressed results as random‐effects models using mean difference for continuous outcomes and risk ratios (RR) with 95% confidence intervals (CI) for dichotomous outcomes. We investigated heterogeneity, including both clinical and methodological factors.
Main results
This second update of the review identified 19 additional eligible trials resulting in a total of 33 studies (2793 participants) that met the inclusion criteria. There was low quality evidence that sutures were significantly better than tissue adhesives for reducing the risk of wound breakdown (dehiscence; RR 3.35; 95% CI 1.53 to 7.33; 10 trials, 736 participants that contributed data to the meta‐analysis). The number needed to treat for an additional harmful outcome was calculated as 43. For all other outcomes ‐ infection, patient and operator satisfaction and cost ‐ there was no evidence of a difference for either sutures or tissue adhesives. No evidence of differences was found between tissue adhesives and tapes for minimising dehiscence, infection, patients' assessment of cosmetic appearance, patient satisfaction or surgeon satisfaction. However there was evidence in favour of using tape for surgeons' assessment of cosmetic appearance (mean difference (VAS 0 to 100) 9.56 (95% CI 4.74 to 14.37; 2 trials, 139 participants). One trial compared tissue adhesives with a variety of methods of wound closure and found both patients and clinicians were significantly more satisfied with the alternative closure methods than the adhesives. There appeared to be little difference in outcome for different types of tissue adhesives. One study that compared high viscosity with low viscosity adhesives found that high viscosity adhesives were less time‐consuming to use than low viscosity tissue adhesives, but the time difference was small.
Authors' conclusions
Sutures are significantly better than tissue adhesives for minimising dehiscence. In some cases tissue adhesives may be quicker to apply than sutures. Although surgeons may consider the use of tissue adhesives as an alternative to other methods of surgical site closure in the operating theatre, they need to be aware that sutures minimise dehiscence. There is a need for more well designed randomised controlled trials comparing tissue adhesives with alternative methods of closure. These trials should include people whose health may interfere with wound healing and surgical sites of high tension.
Plain language summary
Tissue adhesives for closure of surgical skin incisions
Tissue adhesives or glues are increasingly used in place of stitches (sutures) or staples to close wounds. It has been suggested that tissue adhesives may be quicker and easier to use than sutures for closing surgical wounds. Tissue adhesives carry no risk of sharps injury ‐ unlike needles that are used for sutures ‐ and are thought to provide a barrier to infection. This may mean that they also promote healing, and the need for removal of sutures is avoided.
The researchers searched the medical literature up to March 2014, and identified 33 medical studies that investigated the use of tissue adhesives for closure of wounds. They compared tissue adhesive with another method of closure such as sutures, staples, tape, or another type of tissue adhesive. The main outcomes of interest were whether wounds stayed closed ‐ and did not break down ‐ and whether they became infected. The results of the review showed clearly that fewer wounds broke down when sutures were used. Studies also reported that some types of tissue adhesives might be slightly quicker to use than other types. There was no clear difference between tissue adhesives and the alternative closure methods for cosmetic results or costs. Results regarding surgeons' and patients' preferred skin closure method were mixed.
Summary of findings
Summary of findings for the main comparison. Tissue adhesive compared to sutures for surgical incisions.
| Tissue adhesive compared to sutures for surgical incisions | ||||||
| Patient or population: People with surgical incisions Settings: Intervention: Tissue adhesive Comparison: Sutures | ||||||
| Outcomes | Illustrative comparative risks*4 (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Sutures | Tissue adhesive | |||||
| Wound dehiscence | Study population | RR 3.35 (1.53 to 7.32) | 736 (10 studies) | ⊕⊕⊝⊝ low1,2 | ||
| 13 per 1000 | 45 per 1000 (21 to 99) | |||||
| Moderate | ||||||
| Wound infection | Study population | RR 1.72 (0.92 to 3.16) | 744 10 studies | ⊕⊝⊝⊝ very low2,3 | ||
| 38 per 1000 | 76 per 1000 (14 to 397) | |||||
| Moderate | ||||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) CI: Confidence interval; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate Very low quality: we are very uncertain about the estimate | ||||||
1 Possible unit of analyses issues. A sensitivity analysis changes a statistically significant difference to a non‐statistically significant difference 2 Study 95% CIs are wide 3 Possible unit of analysis issues 4 Median control (suture) group risk across studies
Summary of findings 2. Tissue adhesive compared to adhesive tape for surgical incisions.
| Tissue adhesive compared to adhesive tape for surgical incisions | ||||||
| Patient or population: people with surgical incisions Settings: Intervention: tissue adhesive Comparison: adhesive tape | ||||||
| Outcomes | Illustrative comparative risks*3 (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Adhesive tape | Tissue adhesive | |||||
| Wound dehiscence | Study population | RR 0.96 (0.06 to 14.55) | 50 (1 study) | ⊕⊕⊝⊝ low1 | ||
| 42 per 1000 | 40 per 1000 (2 to 606) | |||||
| Moderate | ||||||
| Wound infection | Study population | RR 1.37 (0.39 to 4.81) | 190 (3 studies) | ⊕⊕⊝⊝ low1,2 | ||
| 43 per 1000 | 60 per 1000 (17 to 209) | |||||
| Moderate | ||||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) CI: Confidence interval; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate Very low quality: we are very uncertain about the estimate | ||||||
1 Study 95% CIs are very wide 2 Evidence of inconsistency in point estimates. With the point estimate from one study lying outside the 95% CIs of another 3 Control (tape) group risk in included study
Summary of findings 3. Tissue adhesive compared to staples for surgical incisions.
| Tissue adhesive compared to staples for surgical incisions | ||||||
| Patient or population: people with surgical incisions Settings: Intervention: tissue adhesive Comparison: staples | ||||||
| Outcomes | Illustrative comparative risks*3 (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Staples | Tissue adhesive | |||||
| Wound dehiscence | Study population | RR 0.53 (0.05 to 5.33) | 37 (1 study) | ⊕⊕⊝⊝ low1 | ||
| 105 per 1000 | 56 per 1000 (5 to 561) | |||||
| Moderate | ||||||
| Wound infection | Study population | RR 1.39 (0.3 to 6.54) | 250 (3 studies) | ⊕⊝⊝⊝ very low1,2 | ||
| 71 per 1000 | 99 per 1000 (21 to 463) | |||||
| Moderate | ||||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Study 95% CIs are very wide. 2 Evidence of point estimates lying in opposite directions with the estimate for one study lying outside the 95% CI of another. 3 Control (staples ) group risk for included study.
Summary of findings 4. Tissue adhesive compared to other methods for surgical incisions.
| Tissue adhesive compared to other methods for surgical incisions | ||||||
| Patient or population: people with surgical incisions Settings: Intervention: tissue adhesive Comparison: other methods | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Other methods | Tissue adhesive | |||||
| Wound dehiscence | Study population | RR 0.55 (0.13 to 2.38) | 209 (1 study) | ⊕⊕⊝⊝ low1,2 | ||
| 49 per 1000 | 27 per 1000 (6 to 117) | |||||
| Moderate | ||||||
| Wound infection | Study population | RR 0.41 (0.11 to 1.6) | 209 (1 study) | ⊕⊕⊝⊝ low1,2 | ||
| 66 per 1000 | 27 per 1000 (7 to 105) | |||||
| Moderate | ||||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) CI: Confidence interval; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate Very low quality: we are very uncertain about the estimate | ||||||
1 Study 95% CIs are very wide 2 Single study with low event rate
Summary of findings 5. High viscosity tissue adhesive compared to low viscosity tissue adhesive for surgical incisions.
| High viscosity tissue adhesive compared to low viscosity tissue adhesive for surgical incisions | ||||||
| Patient or population: people with surgical incisions Settings: Intervention: high viscosity tissue adhesive Comparison: low viscosity tissue adhesive | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Low viscosity tissue adhesive | High viscosity tissue adhesive | |||||
| Wound dehiscence | Study population | RR 3.74 (0.21 to 67.93) | 148 (1 study) | ⊕⊝⊝⊝ very low1,2 | ||
| Could not be calculated | Could not be calculated | |||||
| Wound infection | Study population | RR 0.82 (0.16 to 4.31) | 148 (1 study) | ⊕⊝⊝⊝ very low1,2 | ||
| 47 per 1000 | 38 per 1000 (7 to 200) | |||||
| Moderate | ||||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) CI: Confidence interval; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate Very low quality: we are very uncertain about the estimate | ||||||
1 Study 95% CIs are very wide 2 Single study with low event rate
Summary of findings 6. Octylcyanoacrylate compared to butylcyanoacrylate for surgical incisions.
| Octylcyanoacrylate compared to butylcyanoacrylate for surgical incisions | ||||||
| Patient or population: people with surgical incisions Settings: Intervention: octylcyanoacrylate Comparison: butylcyanoacrylate | ||||||
| Outcomes | Illustrative comparative risks*2 (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Butylcyanoacrylate | Octylcyanoacrylate | |||||
| Wound dehiscence | 26 per 1000 |
38 per 1000 (5 to 297) |
RR 1.46 (0.19 to 11) |
80 (2 studies) | ⊕⊕⊝⊝ low1 | |
| Wound infection | Study population | RR 0.63 (0.21 to 1.88) | 37 (1 study) | ⊕⊕⊝⊝ low1 | ||
| 333 per 1000 | 210 per 1000 (70 to 627) | |||||
| Moderate | ||||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) CI: Confidence interval; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate Very low quality: we are very uncertain about the estimate | ||||||
1 The 95% CI estimate around the RR of 1.46 is very wide 2 Median control group risk across studies
Background
Description of the condition
Millions of surgical procedures are conducted around the world each year. The majority of procedures result in surgical wounds that will heal by primary intention ‐ this is where wound edges are brought together (re‐approximated) and held together, e.g. with sutures, to facilitate tissue healing.
Description of the intervention
In the past the options for wound closure have been limited largely to sutures (needle and thread) with other alternatives such as staples, adhesive tapes and tissue adhesives entering clinical practice more recently. Closure of wounds with sutures enables meticulous closure, but skin may react to sutures and they usually require removal. Tissue adhesives (glues) offer the advantages that suture removal is not required at a later date and there is no risk of needlestick injury to the surgeon or assistant.
Tissue adhesives have been used in various forms for many years since the first cyanoacrylate adhesives were synthesised (Coover 1959). The early adhesives were appropriate for small superficial lacerations and incisions, but their limited physical properties prevented use in the management of other wounds. There were also reports of acute and chronic inflammatory reactions (Houston 1969). Further development led to the introduction of the n‐2‐butylcyanoacrlyates that were purer and stronger, but did not receive widespread acceptance because their clinical performance was limited by their low tensile strength and brittleness (Bruns 1996; Quinn 1993). More recently stronger tissue adhesives have been developed by combining plasticisers and stabilisers to increase flexibility and reduce toxicity (Quinn 1997).
Tissue adhesives have been used primarily in emergency rooms and there is increasing support in the literature for their effectiveness in the closure of various traumatic lacerations (Farion 2001; Osmond 1999; Perron 2000; Quinn 1997). Surgeons now also use tissue adhesives in the operating room for the closure of surgical skin incisions.
How the intervention might work
The introduction of tissue adhesives was received enthusiastically as they may produce equivalent tensile strength, improved cosmetic appearance of the scar and a lower infection rate when compared with sutures, staples and adhesive tapes, while avoiding many of the risks and disadvantages of alternative methods (Osmond 1999). As with standard adhesives, tissue adhesives are applied to the wound in a liquid form ‐ following application they undergo polymerisation and bonding and setting occurs.
Why it is important to do this review
It is important that clinical decision‐makers are able to make evidence‐informed decisions regarding the use of tissue adhesives to close surgical incisions. This review was first published in 2004. As tissue adhesives become more widely used, more randomised controlled trials are conducted, and this update is required to incorporate this new evidence.
Objectives
To determine the effects of various tissue adhesives compared with conventional skin closure techniques for the closure of surgical wounds.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs).
Types of participants
People of any age and in any setting requiring closure of a surgical skin incision of any length.
Types of interventions
Surgical skin incision closure with tissue adhesive compared with another tissue adhesive or any alternative conventional closure device such as sutures, staples or adhesive tapes (e.g. Steri‐Strips/butterfly stitches).
Types of outcome measures
Primary outcomes
Proportion of wounds that break down (wound dehiscence).
Secondary outcomes
Proportion of infected wounds (using the study investigator's diagnosis of infection).
Cosmetic appearance at or after three months where the investigator has used a validated measure.
Patient (or in the case of studies performed with participants under the age of 16 years, parents') general satisfaction with skin incision closure technique (this is more than cosmetic appearance as other factors such as suture removal experience may have an input).
Surgeon satisfaction with skin incision closure technique (this may take into account the time for surgeon to close skin incision amongst other factors).
Relative cost of materials required for the skin incision closure techniques being compared (this will be reported in a narrative form).
Time taken to wound closure (at end of surgery) has been added to the review as a post hoc outcome measure. The review authors believe this to be a contributory factor towards both cost‐effectiveness and satisfaction.
Search methods for identification of studies
For an outline of the search methods used in the original version of this review see Appendix 1 For an outline of the search methods used in the first update of this review see Appendix 2.
Electronic searches
For this second update in March 2014 we searched the following electronic databases:
Cochrane Wounds Group Specialised Register (searched 13 March 2014);
The Cochrane Central Register of Controlled Trials (CENTRAL; The Cochrane Library 2014 Issue 1);
Ovid MEDLINE (1946 to March Week 1 2014);
Ovid MEDLINE (In‐Process & Other Non‐Indexed Citations, 12 March 2014);
Ovid EMBASE (1974 to 12 March 2014);
EBSCO CINAHL (1982 to 13 March 2014).
The following strategy was used to search the Cochrane Central Register of Controlled Trials (CENTRAL):
#1 MeSH descriptor: [Wounds and Injuries] explode all trees 15958 #2 surgical next wound* 3679 #3 #1 or #2 19357 #4 MeSH descriptor: [Tissue Adhesives] explode all trees 387 #5 MeSH descriptor: [Fibrin Tissue Adhesive] explode all trees 329 #6 tissue next adhesive* 655 #7 MeSH descriptor: [Cyanoacrylates] explode all trees 154 #8 octylcyanoacrylate* 52 #9 Dermabond 44 #10 MeSH descriptor: [Enbucrilate] explode all trees 42 #11 enbucrilate 62 #12 butylcyanoacrylate* 7 #13 MeSH descriptor: [Acrylates] explode all trees 1757 #14 acrylate* 254 #15 MeSH descriptor: [Bucrylate] explode all trees 0 #16 bucrylate* 6 #17 #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 or #13 or #14 or #15 or #16 2397 #18 #3 and #17 225
The search strategies for Ovid MEDLINE, Ovid EMBASE and Ovid CINAHL can be found in Appendix 3, Appendix 4 and Appendix 5 respectively. The Ovid MEDLINE search was combined with the Cochrane Highly Sensitive Search Strategy for identifying randomised trials in MEDLINE: sensitivity‐ and precision‐maximizing version (2008 revision); (Lefebvre 2011). We combined the EMBASE search with the Ovid EMBASE filter developed by the UK Cochrane Centre (Lefebvre 2011). We combined the CINAHL searches with the trial filters developed by the Scottish Intercollegiate Guidelines Network (SIGN 2011).
Searching other resources
The reviewers checked the bibliographies of new studies included in this updated review for potentially eligible references that had not been identified in the electronic searches outlined above.
Data collection and analysis
Selection of studies
Two review authors independently examined the titles and abstracts of all the articles identified by the search to identify potentially relevant trials and then assessed the full text of these articles independently using a standardised form to check for eligibility in the review. Disagreements about inclusion were resolved by consensus or a further review author where necessary. Two review authors performed validity assessment and data extraction on all studies meeting the inclusion criteria. Studies rejected at this stage were recorded in a table of excluded studies and reasons for exclusion recorded.
Data extraction and management
Data were extracted by at least two review authors independently using specially designed data extraction forms. The data extraction forms were piloted on several papers and modified as required before use. Any disagreements were resolved by discussion and third review author consulted where necessary. All study authors were contacted for clarification, or to request missing information where necessary. Data were excluded if further clarification could not be obtained.
For each trial the following data were recorded:
year of publication, country of origin and source of study funding;
details of the participants including demographic characteristics and criteria for inclusion;
details of the type of intervention (adhesive, suture, staples or adhesive tape) and type of adhesive (butylcyanoacrylate or octylcyanoacrylate);
details of the outcomes reported, including method of assessment and time intervals. Cosmetic appearance was included if the authors stated that was measured on a validated scale.
Assessment of risk of bias in included studies
Two review authors independently assessed each eligible study for risk of bias using the Cochrane ‘Risk of bias assessment tool’. The tool addresses six specific domains (see Appendix 6), namely sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting and other issues that may potentially bias the study (Higgins 2011). They completed a ‘Risk of bias’ table for each eligible study, and a separate assessment of blinding and completeness of outcome data for each outcome. Discrepancies between review authors were resolved through discussion. Findings are presented using the ‘Risk of bias’ summary figure, which presents all of the judgements in a cross‐tabulation of study by risk of bias domain.
Assessment of heterogeneity
This assessment of clinical and methodological heterogeneity will be supplemented by information regarding statistical heterogeneity ‐ assessed using the Chi² test (a significance level of P less than 0.10 will be considered to indicate statistically significant heterogeneity in conjunction with I² measure; Higgins 2003). I² examines the percentage of total variation across RCTs that is due to heterogeneity rather than chance. In general I² values of 25%, or less, may mean a low level of heterogeneity, and values of 75%, or more, indicate very high heterogeneity (Deeks 2011).
Data synthesis
For dichotomous outcomes, the reviewers used risk ratios (RR) to express estimates of effect of an intervention, together with 95% confidence intervals (CI). For continuous outcomes, the reviewers used mean differences and standard deviations to summarize the data for each group. Where there were studies of similar comparisons reporting the same outcome measures, we attempted a meta‐analysis. Risk ratios were combined for dichotomous data, and weighted mean differences (WMD) for continuous data, using a random‐effects model (indicated as RE in the results section) as some heterogeneity between studies was anticipated. We planned to analyse time taken to close wound (after surgery) as survival (time‐to‐event) data, using the appropriate analytical method (as per the Cochrane Reviewers' Handbook guidance Deeks 2011), or as a continuous outcome, if data from all participants were available.
The reviewers intended to meta‐analyse the results of trials with a split wound (different parts of the same wound randomised to alternate treatments), and split body designs (different wounds on the same participant randomised to alternative treatments) using the inverse variance method for paired data if appropriate data were available.
'Summary of findings' tables
In this second update we also present the main results of the review in 'Summary of findings' tables. These tables present key information concerning the quality of the evidence, the magnitude of the effects of the interventions examined, and the sum of the available data for the main outcomes (Schunemann 2011a). The 'Summary of findings' tables also include an overall grading of the evidence related to each of the main outcomes using the GRADE (Grades of Recommendation, Assessment, Development and Evaluation) approach. The GRADE approach defines the quality of a body of evidence as the extent to which one can be confident that an estimate of effect or association is close to the true quantity of specific interest. The quality of a body of evidence involves consideration of within‐trial risk of bias (methodological quality), directness of evidence, heterogeneity, precision of effect estimates and risk of publication bias (Schunemann 2011b). We present the following outcomes in the 'Summary of findings' tables:
wound dehiscence;
wound infection.
Subgroup analysis and investigation of heterogeneity
The reviewers intended to undertake a subgroup analysis of age (under 18 years and 18 years or older), location of incision on body (face and body), length of incision (less than 4 cm and 4 cm or greater), and patient characteristics such as diabetes and source of trial funding (commercially or independently funded), however there were insufficient studies reporting these data to undertake these analyses.
Sensitivity analysis
Where possible we planned to undertake a sensitivity analysis to examine the effect of randomisation, allocation concealment and blinded outcome assessment on the overall estimates of effect. In addition, we also planned a sensitivity analysis to examine the effect of including unpublished literature on the review's findings.
In this second update of the review we conducted a post‐hoc sensitivity analysis where we removed studies from key analyses where we had concerns about possible unit of analysis issues (i.e. where dehiscence and infection had been recorded over multiple time periods and it was not clear from the analyses whether some participants had more than one event).
Results
Description of studies
See Characteristics of included studies; Characteristics of excluded studies and Characteristics of studies awaiting classification .
Characteristics of the trial setting and investigators
In the original review, of the 22 potentially eligible studies of which eight were excluded (Alhopuro 1976; Gorozpe‐Calvillo 1999; Jaibaji 2000; Kuo 2006; Orozco‐Razon 2002; Singer 2002; Silvestri 2006; Steiner 2000) and 14 were included (Blondeel 2004; Cheng 1997; Dowson 2006; Greene 1999; Keng 1989; Maartense 2002; Ong 2002; Ozturan 2001; Ridgway 2007; Shamiyeh 2001; Sinha 2001; Sniezek 2007; Switzer 2003; Toriumi 1998). We excluded one study because no data were presented and none were received after we sent a written request to the authors (Alhopuro 1976). Another study was excluded as we could not use the data for incision closure because they were combined with data for laceration closure (Singer 2002); we wrote to the authors to request data separated by group, but received no reply. The third study was excluded because after full translation we discovered not to be a randomised trial (Gorozpe‐Calvillo 1999). We excluded two papers because their methodology was flawed. The first of these was excluded because the intervention group had a subcuticular suture in place that was thought to bias the outcome in favour of the intervention (Jaibaji 2000). The second was excluded because all participants had a subcuticular suture placed and the review authors thought this adjunct method of closure would invalidate an independent assessment of the primary interventions (Kuo 2006). Three further studies were excluded, as two were not randomised (Silvestri 2006; Steiner 2000), and the third did not appear to be randomised, and although we sought clarification from the trial authors, no reply was received (Orozco‐Razon 2002). In the current update of this review we obtained full text for a total of 36 potentially eligible new studies. Twelve of these were excluded: three because they did not assess a relevant wound type ‐ e.g. lacerations (Ak 2012; Quinn 1998; Wong 2011); three because the studies did not report relevant outcomes (Chen 2010; Chow 2010; Sun 2005); five were not considered to be RCTs (Giri 2004; Matin 2003; Maw 1997; Spencker 2011; Sajid 2009), and one study because the closure approach was not the only systematic difference between groups (Ong 2010). We included 19 new studies in this update, which led to a total of 33 included studies. Five additional studies are awaiting assessment.
The 33 included studies were conducted in Austria (Shamiyeh 2001), Hong Kong (Cheng 1997), the Netherlands (Maartense 2002; van den Ende 2004), Turkey (Avsar 2009; Ozturan 2001), Ireland (Amin 2009), Italy (Chibbaro 2009; Pronio 2011), Austalia (Khan 2006), Mexico (Millan 2011), Portugal (Mota 2009), Germany (Romero 2011), China (Ong 2002); UK (Dowson 2006; Jallali 2004; Keng 1989; Kent 2014; Krishnamoorthy 2009; Livesey 2009; Ridgway 2007; Sinha 2001), USA (Brown 2009; Eggers 2011; Greene 1999; Kouba 2011; Maloney 2013; Sebesta 2004; Sniezek 2007; Switzer 2003; Tierny 2009; Toriumi 1998), and one was multicentre and international (Blondeel 2004). All studies included adults, except for six that included children (Brown 2009; Cheng 1997; Ong 2002; Romero 2011; Toriumi 1998; van den Ende 2004). All trials were of parallel group design except for two that had a split body design (different wounds on same participant randomised; Greene 1999; Kouba 2011), and two that had a split wound design (different portions of the same wound randomised; Sniezek 2007; Tierny 2009). Kent 2014 randomised participants with multiple wounds (port sites) to treatments ‐ with all wounds on the participant receiving the same intervention. Some outcome data were presented by wound rather than at the participant level, thus potentially failing to account for clustering.
Five included trials had more than two arms: Eggers 2011 had four arms and compared two tissue adhesives, staples and sutures for skin closure; Khan 2006 had three arms comparing tissue adhesive, sutures and staples; Maartense 2002 and Shamiyeh 2001 had three arms comparing tissue adhesive, sutures and adhesive tape, and Blondeel 2004 compared two types of tissue adhesive with each other and also other non‐tissue adhesive closure techniques (a mixed comparison group). These studies are thus included in multiple comparisons.
Characteristics of interventions
In total 24 of the 33 included studies compared tissue adhesive with sutures for incision closure (Avsar 2009; Brown 2009; Cheng 1997; Dowson 2006; Eggers 2011; Greene 1999; Jallali 2004; Keng 1989; Khan 2006; Kouba 2011; Krishnamoorthy 2009; Maartense 2002; Millan 2011; Mota 2009; Ong 2002; Ozturan 2001; Sebesta 2004; Shamiyeh 2001; Sinha 2001; Sniezek 2007, Switzer 2003; Tierny 2009; Toriumi 1998; van den Ende 2004). Three trials compared tissue adhesive with adhesive tape (Maartense 2002; Romero 2011; Shamiyeh 2001). One of these studies also compared tissue adhesive with sutures (Maartense 2002). Six trials compared adhesives with staples (Amin 2009; Eggers 2011; Khan 2006; Livesey 2009; Pronio 2011; Ridgway 2007). Three trials compared one type of tissue adhesive with another type (Blondeel 2004; Kent 2014; Maloney 2013). Chibbaro 2009 compared a tissue adhesive with a comparison arm where staples or sutures were used and Blondeel 2004 compared tissue adhesives with any other skin closure techniques. These comparisons are summarised in Table 7.
1. Summary of study comparisons.
|
Tissue adhesive vs tissue adhesive (Comp 5) |
Mixed control (Comp 4) |
Butyl‐2‐ cyanoacrylate vs staples (Comp 3) |
2‐octyl cyanoacrylate vs staples (Comp 3) |
2‐octyl cyanoacrylate vs tape (Comp 2) |
Butyl‐2‐ cyanoacrylate vs sutures (Comp 1) |
2‐octyl cyanoacrylate vs sutures (Comp1) |
Trial ID |
2‐octyl cyanoacrylate |
Butyl‐2‐ cyanoacrylate |
Sutures | Staples | Adhesive tape/strips | Mixed sutures and staples | All non‐tissue adhesive closure methods |
Other viscosity 2‐octyl cyanoacrylate |
| 3 | Amin 2009 | ✓ | ✓ | ||||||||||||
| 1 | Avsar 2009 | ✓ | ✓ | ||||||||||||
| 5 | 4 | Blondeel 2004 | ✓ | ✓ | ✓ | ||||||||||
| 1 | Brown 2009 | ✓ | ✓ | ||||||||||||
| 1 | Cheng 1997 | ✓ | ✓ | ||||||||||||
| 4 | Chibbaro 2009 | ✓ | ✓ | ||||||||||||
| 1 | Dowson 2006 | ✓ | ✓ | ||||||||||||
| 5 | 3 | 3 | 1 | 1 | Eggers 2011 | ✓ | ✓ | ✓ | ✓ | ||||||
| 1 | Greene 1999 | ✓ | ✓ | ||||||||||||
| 1 | Jallali 2004 | ✓ | ✓ | ||||||||||||
| 1 | Keng 1989 | ✓ | ✓ | ||||||||||||
| 5 | Kent 2014 | ✓ | ✓ | ||||||||||||
| 3 | 1 | Khan 2006 | ✓ | ✓ | ✓ | ||||||||||
| 1 | Kouba 2011 | ✓ | ✓ | ||||||||||||
| 1 | Krishnamoorthy 2009 | ✓ | ✓ | ||||||||||||
| 3 | Livesey 2009 | ✓ | ✓ | ||||||||||||
| 2 | 1 | Maartense 2002 | ✓ | ✓ | ✓ | ||||||||||
| 5 | Maloney 2013 | ✓ | ✓ | ||||||||||||
| 1 | Millan 2011 | ✓ | ✓ | ||||||||||||
| 1 | Mota 2009 | ✓ | ✓ | ||||||||||||
| 1 | Ong 2002 | ✓ | ✓ | ||||||||||||
| 1 | Ozturan 2001 | ✓ | ✓ | ||||||||||||
| 3 | Pronio 2011 | ✓ | ✓ | ||||||||||||
| 3 | Ridgway 2007 | ✓ | ✓ | ||||||||||||
| 1 | Sebesta 2004 | ✓ | ✓ | ||||||||||||
| 2 | 1 | Shamiyeh 2001 | ✓ | ✓ | ✓ | ||||||||||
| 1 | Sinha 2001 | ✓ | ✓ | ||||||||||||
| 1 | Sniezek 2007 | ✓ | ✓ | ||||||||||||
| 1 | Switzer 2003 | ✓ | ✓ | ||||||||||||
| 1 | Tierny 2009 | ✓ | ✓ | ||||||||||||
| 1 | Toriumi 1998 | ✓ | ✓ | ||||||||||||
| 2 | Romero 2011 | ✓ | ✓ | ||||||||||||
| 1 | van den Ende 2004 | ✓ | ✓ |
Abbreviation
Comp = comparison
Comparison 1: Tissue adhesive compared with sutures
Butylcyanoacrylate versus sutures
Seven studies investigated the use of butylcyanoacrylate compared with sutures (Cheng 1997; Dowson 2006; Eggers 2011; Keng 1989; Ozturan 2001; Sinha 2001; van den Ende 2004).
Cheng 1997 compared butylcyanoacrylate tissue adhesive with 4.0 catgut suture in boys under 12 years of age requiring elective circumcision.
Dowson 2006 compared butylcyanoacrylate tissue adhesive with interruptible, non‐absorbable suture after laparoscopic procedures.
Eggers 2011 was a four‐arm trial in participants undergoing total knee arthroplasty, with one arm receiving butylcyanoacrylate tissue adhesive and one receiving Monocryl sutures.
Keng 1989 investigated butylcyanoacrylate in patients requiring groin incisions. Skin incisions were closed with either butylcyanoacrylate tissue adhesive or Dexon subcuticular sutures. Three of the 43 patients had bilateral operations when the left side was closed with adhesive (butylcyanoacrylate) and the right with sutures.
Ozturan 2001) compared butylcyanoacrylate tissue adhesive with 6.0 polypropylene sutures for columellar skin closure after the majority of the tension had been taken up using 5.0 chromic catgut.
Sinha 2001 compared butylcyanoacrylate tissue adhesive with 4.0 monofilament suture in adult patients requiring hand or wrist surgery.
van den Ende 2004 compared butylcyanoacrylate tissue adhesive with polyglactin 5‐0 (Vicryl) suture in children undergoing inguinal hernia repair.
Octylcyanoacrylate versus sutures
Eighteen studies investigated the use of octylcyanoacrylate tissue adhesives versus sutures (Avsar 2009; Brown 2009; Eggers 2011; Greene 1999; Jallali 2004; Khan 2006; Kouba 2011; Krishnamoorthy 2009; Maartense 2002; Millan 2011; Mota 2009; Ong 2002; Sebesta 2004; Shamiyeh 2001; Sniezek 2007; Switzer 2003; Tierny 2009; Toriumi 1998).
Avsar 2009 compared high viscosity octylcyanoacrylate tissue adhesive with polypropylene sutures in women undergoing the Pfannenstiel incision in the abdomen.
Brown 2009 compared octylcyanoacrylate tissue adhesive with Monocryl sutures in children undergoing inguinal herniorrhaphy.
Eggers 2011 compared octylcyanoacrylate tissue adhesive with monocryl sutures in people undergoing total knee arthroplasty.
Greene 1999 and Kouba 2011 randomised participants requiring bilateral blepharoplasty. This model with two identical skin sites on the same patient allowed a split‐body study design and each participant to act as his or her own control. The left or right upper eye lid was closed with octylcyanoacrylate and the other eyelid closed with 6.0 suture.
Jallali 2004 compared octylcyanoacrylate tissue adhesive with absorbable sutures in people undergoing laparoscopic cholecystectomy.
Khan 2006 compared octylcyanoacrylate tissue adhesive with Monocryl sutures in people undergoing either a total knee arthroplasty or a total hip arthroplasty.
Krishnamoorthy 2009 compared octylcyanoacrylate tissue adhesive with absorbable sutures in people undergoing saphenous vein harvesting.
Maartense 2002 compared octylcyanoacrylate tissue adhesive with intracutaneous poliglecaprone interrupted sutures in people requiring elective laparoscopic procedures.
Millan 2011 compared cyanoacrylate tissue adhesive (no further details available) compared with monofilament sutures in people undergoing skin biopsies.
Mota 2009 compared octylcyanoacrylate tissue adhesive with rapidly absorbably polyglactin sutures in women undergoing mediolateral episiotomy after a vaginal delivery.
Sebesta 2004 compared octylcyanoacrylate with subcuticular suture in people who had undergone laparoscopic surgery.
Shamiyeh 2001 compared octylcyanoacrylate tissue adhesive with 5.0 monofilament sutures in patients requiring mini‐phlebectomy with the Muller technique. This study also compared tissue adhesive with adhesive tape.
Switzer 2003 compared octylcyanoacrylate tissue adhesive with a subcuticular Monocryl suture for the elective repair of inguinal hernias. Ong 2002 also compared octylcyanoacrylate with a Monocryl subcuticular suture, but in children requiring herniotomies.
Sniezek 2007 followed a split wound design comparing octylcyanoacrylate with a cuticular polypropylene suture on head and neck surgical sites following the removal of carcinomas using the Mohs technique.
Tierny 2009 compared octylcyanoacrylate tissue adhesive with rapid absorbing gut sutures in people undergoing surgery for non‐melanomas skin cancer.
Toriumi 1998 investigated incisions with and without subcutaneous sutures and then randomised for closure with octylcyanoacrylate tissue adhesive or 5.0 or 6.0 nylon suture in people over one year of age and over requiring elective surgery for benign skin lesions predominantly in the face and neck.
Comparison 2: Tissue adhesives compared with adhesive tape
Octylcyanoacrylate versus adhesive tape
Three studies compared octylcyanoacrylate tissue adhesive with adhesive tapes.
Shamiyeh 2001 compared octylcyanoacrylate tissue adhesive with tape in adults requiring mini‐phlebectomy with the Muller technique.
Maartense 2002 compared octylcyanoacrylate tissue adhesive to 76 mm x 6 mm adhesive paper (Steri‐Strips) in people undergoing elective laparoscopic surgery.
Romero 2011 compared octylcyanoacrylate tissue adhesive with standard adhesive strips (strips applied in star‐shaped manner) in children undergoing laparoscopic appendectomy.
Comparison 3: Tissue adhesives compared with staples
Butylcyanoacrylate versus staples
Two studies compared butylcyanoacrylate tissue adhesive with staples.
Livesey 2009 compared butylcyanoacrylate tissue adhesive with staples in people undergoing a total hip replacement.
Eggers 2011 compared butylcyanoacrylate tissue adhesive with staples in people undergoing total knee arthroplasty.
Octylcyanoacrylate versus staples
Five studies compared octylcyanoacrylate tissue adhesives with staples.
Ridgway 2007 compared octylcyanoacrylate tissue adhesives with staples in people requiring thyroid and parathyroid surgery.
Eggers 2011 compared octylcyanoacrylate tissue adhesives with staples in participants undergoing total knee arthroplasty.
Amin 2009 compared octylcyanoacrylate tissue adhesives with staples in people undergoing minimally invasive thyroidectomy.
Khan 2006 compared octylcyanoacrylate tissue adhesives with staples in people undergoing either a total knee arthroplasty or a total hip arthroplasty.
Pronio 2011 compared octylcyanoacrylate tissue adhesives with staples in people undergoing thyroid surgery.
Comparison 4: Tissue adhesives compared with other techniques
Octylcyanoacrylate versus mixture of other closure approaches
Blondeel 2004 was the only study that investigated the use of tissue adhesives in incisions of 4 cm or longer. High viscosity octylcyanoacrylate tissue adhesive was compared with any other commercially available device such as sutures, staples or tapes and also compared with low viscosity octylcyanoacrylate. The high viscosity formulation is six‐times more viscous than the normal adhesive and designed to reduce run‐off of pre‐polymerised adhesive from the application site.
Butylcyanoacrylate versus mixture of other closure approaches
Chibbaro 2009 compared a group allocated to butylcyanoacrylate tissue adhesive with a group allocated to receive either sutures or staples for skin closure ‐ based on clinician choice ‐ in people undergoing elective cranial supratentorial surgery.
Comparison 5: Tissue adhesive compared with tissue adhesive
High versus low viscosity adhesives
Blondeel 2004 compared high and low viscosity adhesive in the trial described above.
Octylcyanoacrylate versus butylcyanoacrylate
Three studies compared octylcyanoacrylate tissue adhesive with butylcyanoacrylate tissue adhesive for skin closure.
Eggers 2011 compared these tissue adhesives in people undergoing total knee arthroplasty.
Kent 2014 compared these tissue adhesives in people undergoing a range of laparoscopic procedures.
Maloney 2013 compared these tissue adhesives in people undergoing a skin incision to remove skin cancer.
Characteristics of outcome measures
Wound dehiscence
Twenty‐three studies reported wound dehiscence. The time of post‐operative wound examination for dehiscence varied between studies. Cheng 1997 reported dehiscence at days 1, 2, 3, 7 and 30; Toriumi 1998 reported dehiscence at 5 to 7 days; Chibbaro 2009, Ozturan 2001, Pronio 2011, Sniezek 2007 and Tierny 2009 at 7 days; Shamiyeh 2001 and van den Ende 2004 at 10 days; Greene 1999 at weeks 1, 2 and 4; and Sinha 2001 at 10 days, 2 weeks and 6 weeks. Ong 2002 assessed dehiscence at 2 to 3 weeks; Keng 1989 and Sebesta 2004 at 2 weeks; Dowson 2006 at day 1, 2 and at 4 to 6 weeks; Switzer 2003 at 2 and 4 weeks; Blondeel 2004 at day 10; Brown 2009 at 6 weeks; Eggers 2011 at 24 hours, 3 weeks and 6 weeks; Maloney 2013 at 2 weeks and 3 months; Mota 2009 from 42 hours to 68 hours; Romero 2011 at day 10 and day 90; and Millan 2011 on days 5, 7, 10 and 14.
We felt there were potential unit of analysis issues in four studies where it was not clear whether one person had more than one episode of dehiscence over multiple time periods (Cheng 1997; Eggers 2011; Millan 2011; Sinha 2001). We acknowledged this in the 'Risk of bias' assessment and sensitivity analysis we conducted.
Wound infection
In total 25 studies measured wound infection. One study noted infection, defined as wound discharge with positive bacterial culture, at days 1, 2, 3, 7 and 30 (Cheng 1997). A second study defined infection as the presence of pus (Keng 1989), and examined wounds at 1 and 4 weeks postoperatively. A third study defined infection as an abscess that required drainage (Ozturan 2001), and examined wounds at 1 week. A fourth study defined infection as a spontaneous drainage of purulent fluid (Maartense 2002), and noted this at 2 weeks and 3 months. Blondeel 2004 defined infection as redness more than 3 mm to 5 mm from the wound margin, swelling, purulent discharge, pain, increased skin temperature, fever or other signs of infection and assessed this at day 10. Switzer 2003 described an infection as a draining sinus. Avsar 2009 assessed infection at 2, 7 and 40 days postoperatively using a definition of infection that was thought to be purulence and accompanying erythema, but the translation we used was not completely clear about this definition. Livesey 2009 defined wound infection as a participant requiring antibiotics specifically for suspected wound infection, this was assessed at 24 hours, 3 weeks and 6 weeks postoperatively. Khan 2006 classed follow‐up as early, which seemed to be the first 3 days after surgery, and then late, which was between 8 weeks and 12 weeks postoperatively; where cultures were positive or there was clinical evidence of cellulitis, the participants were treated with a course of antibiotics and recorded as having an ‘infection'. Romero 2011 assessed wounds at the 10th and 90th days postoperatively and defined infection as an abscess or redness more than 3 mm perpendicular to the wound. One study simply referred to wound complications (Dowson 2006). A further 14 studies reported upon infection, but did not describe how infection would be defined for diagnosis and reporting in the study (Chibbaro 2009; Eggers 2011; Greene 1999; Kent 2014; Ong 2002; Maloney 2013; Pronio 2011; Sebesta 2004; Shamiyeh 2001; Sinha 2001; Sniezek 2007; Tierny 2009; Toriumi 1998; van den Ende 2004).
We felt there were potential unit of analysis issues in two studies where it was not clear whether one person had more than one episode of infection over multiple time periods (Eggers 2011; Khan 2006). While we have reported the total number of infections reported by group it was not clear whether some participants reported more than one infection, as the number of infections was reported rather than number of people having at least one infection. We have acknowledged this in the 'Risk of bias' assessment and sensitivity analysis we conducted.
Cosmetic appearance
Eleven studies reported cosmetic appearance with data that could be used for further analyses. One study asked participants to score their own cosmetic result using a validated visual analogue scale (VAS; Maartense 2002). Participants in the Dunker 1998 trial were also asked to complete the cosmetic scale of the Body Image Questionnaire. Surgical residents who were blinded to the wound closure method also scored the cosmetic appearance with a VAS and the Hollander Wound Evaluation Score (Hollander 1995). These assessments were undertaken at two weeks and three months (with three month data presented). Ozturan 2001 reported cosmetic appearance at 3 months by blinded assessment of photographs using VAS, with best possible scar rated as 100 and worst possible scar as 0 (Quinn 1995), and the Hollander Scale. A third study also reported surgeon‐assessed cosmetic appearance at three months using a modified Hollander Wound Evaluation scale ‐ this was a blinded assessment (Kent 2014). Livesey 2009, Maloney 2013 and Romero 2011 reported surgeon‐assessed cosmetic appearance at three months using a 100 mm VAS, where 0 represented the worst outcome and 100 the best outcome ‐ in all cases the surgeon‐assessed outcome was blinded. Livesey 2009 and Maloney 2013 also used the same VAS scale to assess participant data on cosmetic appearance, but it was unclear whether these assessments were blinded.
Pronio 2011 asked participants to assess cosmetic appearance using the Stony Brook scar evaluation scale composed of five dichotomous, evenly weighted categories. Mean data presented here were calculated by the review authors from data included in the study report. Kouba 2011 reported surgeon‐assessed cosmetic appearance at one month and three months (we report three month data). The cosmetic presence of the wound was scored on a scale of 1 (excellent wound healing, scar matches surrounding skin) to 5 (poor scar wound healing, does not match surrounding skin); this was a blinded assessment.
A number of studies reported data that could not be used further. Toriumi 1998 assessed cosmetic appearance at three months and one year using a modified Hollander scale at three months and a VAS of photographs at one year using two surgeons blinded to treatment group. However, we could not use the data from this study at three months as the standard deviation was not reported and one participant dropped out from an unspecified group. Data at one year could not be used, as the group(s) from which 11 participants had dropped out was not clear. Ong 2002 evaluated cosmesis using a VAS and the Hollander Scale at three weeks and three months, but the first data could not be used as it was too early, and the data at three months could not be used due to large and unspecified loss to follow‐up. Dowson 2006 assessed cosmetic outcome using the Hollander scale at six weeks and three months. The six‐week data were not included as it was too early and the three‐month data did not report mean and standard deviation statistics; we contacted the authors but they did not respond, therefore the data could not be included. Sniezek 2007 also assessed cosmesis at three months using a VAS, but there were insufficient data for inclusion. Amin 2009, Chibbaro 2009 and Tierny 2009 also reported cosmetic appearance at three months, but the data were not clear and were also not used.
Several studies evaluated cosmetic appearance less than three months after surgery (Avsar 2009; Blondeel 2004; Brown 2009; Cheng 1997;Eggers 2011; Greene 1999; Keng 1989; Khan 2006; Krishnamoorthy 2009; Ong 2002; Ridgway 2007; Sebesta 2004; Sinha 2001; Switzer 2003).
Patient/parent satisfaction
Thirteen studies reported satisfaction outcomes. Patient satisfaction interviews in one study included questions about comfort, presence of a pulling sensation and appreciation of lack of suture removal at weeks one, two and four (Greene 1999). Wound comfort at one and four weeks was assessed in another study (Keng 1989). A third study assessed participants at one year using a scale of satisfaction with scar (Shamiyeh 2001). One study assessed patient satisfaction by using a questionnaire that included ratings for cosmetic appearance, overall comfort, ability to shower, dressing changes, tension at the wound, hygienic problems or allergic reaction and overall satisfaction (Blondeel 2004). Amin 2009 assessed patient satisfaction at three months using a self‐completed 10 cm VAS line where 0 was poor and 10 was excellent. Avsar 2009 assessed patient satisfaction at day 40 when participants were asked how satisfied they were with their skin closure and could choose from the following responses: very bad, poor, average, good, very good. Ong 2002 and Khan 2006 assessed participant/parent satisfaction using a VAS scale that ran from 0 to 100, where 100 represented maximal satisfaction. Data for Khan 2006 were presented as median values, and separately for different types of arthroplasty, and are not reported further in this review. Dowson 2006 and Romero 2011 reported patient satisfaction as a simple 'satisfied' or 'not satisfied', but gave little information about the criteria used. Likewise, Kent 2014 report participants' satisfaction with incisional wound closure ‐ options were 'satisfied' or 'dissatisfied'. Pronio 2011 assessed participants' satisfaction with wound management at a seven‐day follow‐up when participants were asked to rate their level of satisfaction with the early postoperative management of the wound (regarding the requirement of a return visit for medications, the possibility of washing oneself, and suture removal) using a numerical scale ranging from 0 to 10. Data were reported in merged categories (e.g. percentage of participants reporting a score of 10 to 9, 8 to 7 etc.), which limited further use of these data. One paper reported upon participant satisfaction as an outcome measure in the text (Sniezek 2007), but no results were reported in the analyses. We attempted to contact the authors, but received no reply.
Surgeon satisfaction
In one study (Greene 1999), surgeon satisfaction included quality of wound closure by assessment of eversion, regularity, approximation and any difficulties in attaining approximation. This was reported at weeks one, two and four. Another study reported surgeon satisfaction at 10 days using a scale of satisfaction with the scar on a five‐point score (where 1 was a 'perfect cosmetic result' to 5 'unsatisfactory result'; Shamiyeh 2001). A third study reported surgeon satisfaction immediately after closure, when the surgeon was asked to give his or her opinion on the time needed for wound closure and the practicality of the materials used by answering multiple choice questions (potential responses included: 'far too long', 'a little too long', 'not too long', 'not practical', 'not very practical' and 'very practical'; Maartense 2002). Due to differences in methods used to measure this outcome, these studies were not included in the meta‐analysis. One study did report surgeon satisfaction via a questionnaire that included ratings for wound cosmetic appearance, safety, effectiveness, applicability for a wide range of incisions, perceived patient satisfaction and overall satisfaction (Blondeel 2004). Kent 2014 assessed surgeons' satisfaction with wound (considering expression, application, delivery and ease of use for product); the options were 'satisfied' or 'dissatisfied'. Maloney 2013 assessed surgeon satisfaction (at time of wound closure) using 100 mm VAS scales for: ease of use (0 'impossible' to 10 'very easy to use') and satisfaction with device and the closure achieved (0 'completely dissatisfied' to 10 'completely satisfied').
Relative cost of materials
Costs of closure devices were reported in five studies (Brown 2009; Eggers 2011; Maartense 2002, Sebesta 2004; Shamiyeh 2001).
Time for wound closure following surgery
Time for closure was reported in 24 studies (Avsar 2009; Brown 2009; Blondeel 2004; Cheng 1997; Chibbaro 2009; Dowson 2006; Eggers 2011; Greene 1999; Jallali 2004; Keng 1989; Kent 2014; Khan 2006; Krishnamoorthy 2009; Livesey 2009; Maartense 2002; Maloney 2013; Ong 2002; Ozturan 2001; Ridgway 2007; Sebesta 2004; Shamiyeh 2001; Switzer 2003; Toriumi 1998; van den Ende 2004). The data from 15 of these studies were excluded as they were insufficient (Avsar 2009; Cheng 1997; Chibbaro 2009; Dowson 2006; Eggers 2011; Greene 1999; Jallali 2004; Keng 1989; Khan 2006; Krishnamoorthy 2009; Livesey 2009; Maartense 2002; Switzer 2003; Toriumi 1998; van den Ende 2004). Data from the remaining nine studies were eligible for inclusion (Blondeel 2004; Brown 2009; Kent 2014; Maloney 2013; Ong 2002; Ozturan 2001; Ridgway 2007; Sebesta 2004; Shamiyeh 2001). The time was recorded as a continuous variable in seconds or minutes elapsed from beginning of wound closure to completion of wound closure. Mean time to closure times were only used in the review if this was measured on all participants, thereby avoiding concerns about time to event data being analysed incorrectly.
Risk of bias in included studies
The results of the quality assessment for included trials is shown in Figure 1 and Figure 2.
1.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study
2.
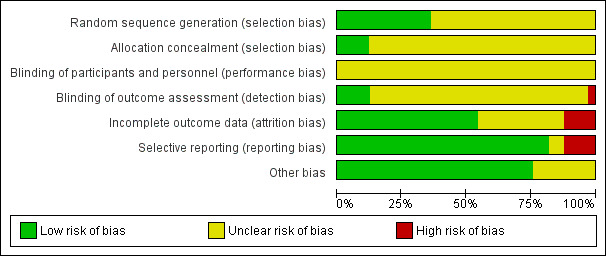
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies
Random sequence generation
Random sequence generation was performed adequately in twelve studies (Amin 2009; Blondeel 2004; Eggers 2011; Khan 2006; Krishnamoorthy 2009; Maartense 2002; Mota 2009; Ong 2002; Romero 2011; Shamiyeh 2001; Sniezek 2007; Switzer 2003). All studies used a random sequences generated by computerised randomisation programmes except for Sniezek 2007, which used coin tossing.
In the remaining 20 studies, the risk of bias in the random sequence generation was unclear. This was largely because, although there was mention of the participants being randomised into different intervention arms, there was no mention of the methods used to achieve this (Brown 2009; Cheng 1997; Chibbaro 2009; Dowson 2006; Greene 1999; Jallali 2004; Keng 1989; Kent 2014; Kouba 2011; Livesey 2009; Maloney 2013; Millan 2011; Ozturan 2001; Pronio 2011; Ridgway 2007; Sebesta 2004; Sinha 2001; Tierny 2009; Toriumi 1998). The partial translation of Avsar 2009 was such that no conclusion could be derived about whether there was adequate evidence of random sequence generation, therefore the judgement remained unclear.
Allocation concealment
Four studies were judged to be at low risk of bias for the domain of allocation concealment: Amin 2009, Dowson 2006, and Ong 2002 reported that they used sealed, sequential envelopes, that were opened shortly before the intervention was given. Livesey 2009 did not indicate that numbered envelopes were used, but stated that envelopes were opened by independent personnel. All remaining studies were deemed to be at unclear risk of bias for allocation concealment. Some studies gave evidence that they used envelopes that were sealed and opaque, but lacked sufficient evidence that they were sequentially numbered or that the process was undertaken by an independent person. Many other studies provided no information on allocation of the randomisation sequence at all.
Blinding of participants and personnel
The risk of bias for blinding of participants and personnel was judged to be unclear in all studies. It was difficult to see how the operating surgeon could be completely blinded to an intervention he/she was supposed to undertake. Only Dowson 2006 and Mota 2009 suggest that participants remained blinded to the intervention they received. Given the difficulties faced in blinding participants (in most cases) and personnel to the intervention, we felt it reasonable to judge all of the included studies as being at unclear risk of bias, as it is uncertain how this influenced the performance of the personnel.
Blinding of outcome assessment
Risk of bias for blinding of outcome assessment was undertaken for each relevant outcome, and thus was often characterised as being at both unclear and high risk of bias within the same study. This was often because numbers of wounds breaking down and wound infection were assessed in a way that was not obviously blinded, but cosmesis was deemed to be blinded. Such examples of studies where blinding of dehiscence was unclear and blinding of cosmesis was adequate were: Blondeel 2004, Dowson 2006, Kent 2014, Livesey 2009, Maloney 2013, Ong 2002, Ozturan 2001, Romero 2011, Shamiyeh 2001, and Toriumi 1998.
There were studies that did give enough evidence for us to infer a low risk of detection bias. These were Amin 2009, Brown 2009, and Maartense 2002, all of which revealed adequate blinding of outcome assessment for all measures extracted for this review. In one study, there was evidence to suggest a high risk of bias (Mota 2009), as the study report indicated that those assessing the wounds were the authors of the paper.
The remaining studies did not provide evidence of adequate blinding of outcome assessments at any stage and were classed as being at unclear risk of bias for this domain.
Incomplete outcome data
Four studies were classed as having a high risk of attrition bias (Dowson 2006; Kent 2014; Ong 2002; Sinha 2001). This was often due to high proportional rates of drop out, or unclear reasons for large numbers of drop outs, or both.
Eleven studies were judged as being at unclear risk of bias for this domain, as reasons for drop out were not clear, or the extent to which the drop‐out rates affected the results were unclear (Amin 2009; Avsar 2009; Eggers 2011; Kouba 2011; Krishnamoorthy 2009; Livesey 2009; Millan 2011; Mota 2009; Ridgway 2007; Romero 2011; Toriumi 1998).
The remaining 18 studies suffered fewer losses to follow‐up and, where these did occur they were fully explained in the literature, so these studies were judged to be at low risk of bias for this domain.
Selective outcome data
Amin 2009, Kouba 2011, Livesey 2009 and Ozturan 2001 were reported to be at high risk of bias due to possible selective reporting of outcomes.Twenty‐seven studies were deemed to have a low risk of reporting bias as they reported on all the outcomes that were outlined in the methodology,
Two studies were judged as unclear, either due to an unclear English translation (Avsar 2009), or because outcomes that were outlined as being assessed were not clearly reported (Sebesta 2004).
Other sources of bias
Eight studies were classed as being at unclear risk of bias for this domain, including six studies where it was it was not possible to exclude unit of analysis issues, for example, we could not establish whether dehiscence or other data, or both, were reported per person, or if the same wounds had more than one infection during the period of the trial (Cheng 1997; Eggers 2011; Jallali 2004; Kent 2014; van den Ende 2004). Avsar 2009 and Millan 2011 were classed as being at unclear risk of bias for this domain, as we could not make a judgement using the translations that we had. The remaining 25 studies were deemed not to offer any other sources of bias.
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5; Table 6
Comparison 1. Tissue adhesives compared with sutures
Primary outcome
Data from 17 trials compared the use of tissue adhesive with sutures for dehiscence, however as seven trials had no cases of dehiscence, only data from the remaining ten trials contributed to the meta‐analysis (Cheng 1997; Dowson 2006; Eggers 2011; Millan 2011; Mota 2009; Sebesta 2004; Shamiyeh 2001; Sinha 2001; Switzer 2003; van den Ende 2004). Overall a significant difference was detected between the proportion of wounds with dehiscence (RR 3.35, 95% CI 1.53 to 7.33; Analysis 1.1), that favoured closure by suture with no evidence of heterogeneity (I2= 0). Taking an assumed control risk of 0.01 (10 per 1000) this returns a number needed to harm of 43. Only one study was deemed to be at low risk of bias for blinded outcome assessment for this outcome (Sinha 2001; Figure 1; Figure 2). Dowson 2006, Mota 2009 and Sinha 2001 had one domain at high risk of bias. The remaining studies had domains classed at low or unclear risk of bias.
1.1. Analysis.

Comparison 1 Adhesive versus suture, Outcome 1 Dehiscence: all studies.
We also conducted a sensitivity analysis in which we removed studies that were at unclear risk of bias for this outcome due to possible unit of analysis issues: these studies were Cheng 1997, Millan 2011, and Sinha 2001 (these authors were contacted where possible to request clarification regarding their data) and also van den Ende 2004, as we were not clear whether this trial reported data at the participant level. When this analysis was undertaken a similar effect size was found, however, there was reduced precision and the findings were no longer statistically significant (RR 2.70, 95% CI 0.95 to 7.68; P value 0.06; Analysis 1.2).
1.2. Analysis.

Comparison 1 Adhesive versus suture, Outcome 2 Dehiscence: sensitivity analysis.
Secondary outcomes
Infection
Eighteen trials that compared the use of tissue adhesives with sutures reported wound infection data, however, as eight of these had no cases of infection, only data from the remaining ten studies contributed to the meta‐analysis (Avsar 2009; Cheng 1997; Eggers 2011; Khan 2006; Maartense 2002; Ozturan 2001; Sebesta 2004; Shamiyeh 2001; Switzer 2003; van den Ende 2004). There was no evidence of a difference in the proportion of participants developing infection in the individual trials, or when data from the trials were pooled (RR 1.72, 95% CI 0.94 to 3.16; Analysis 1.3); again there was no evidence of heterogeneity (I2= 0).
1.3. Analysis.

Comparison 1 Adhesive versus suture, Outcome 3 Infection: all studies.
Three studies were considered to have the potential for unit of analysis issues for this outcome (Eggers 2011; Khan 2006; van den Ende 2004). We conducted a sensitivity analysis removing these studies from the meta‐analysis. Again there was no evidence of a difference in the proportion of participants developing infection between groups (RR 2.03, 95% CI 0.80 to 5.12; Analysis 1.4).
1.4. Analysis.

Comparison 1 Adhesive versus suture, Outcome 4 Infection: sensitivity analysis.
Cosmetic appearance
There was no evidence of a difference in the participants' assessment of cosmetic appearance (MD ‐2.12, 95% CI ‐7.20 to 2.95; Analysis 1.5). Likewise there was no evidence of a difference for the surgeons' assessment of cosmetic appearance based on a 0 to 100 VAS (MD 3.00, 95% CI ‐3.30 to 9.30), or a scar assessment scale (MD ‐0.26, 95% CI ‐0.58 to 0.06; Analysis 1.6; Kouba 2011).
1.5. Analysis.

Comparison 1 Adhesive versus suture, Outcome 5 Cosmetic appearance rated by patient.
1.6. Analysis.

Comparison 1 Adhesive versus suture, Outcome 6 Cosmetic appearance rated by surgeon.
Patient/surgeon satisfaction
There was no evidence of a difference in patient, surgeon or patient/parent satisfaction with treatment (Analysis 1.7; Analysis 1.8; Analysis 1.9; Dowson 2006; Maartense 2002; Ong 2002; Shamiyeh 2001). In one further study 13/20 participants stated that they preferred the tissue adhesive while the remaining seven preferred the sutures (Greene 1999). Avsar 2009 reported that 6/20 participants in the adhesive group reported average satisfaction; 5/20 good and 9/20 very good. This was compared to 13/20 recording good and 7/20 very good in the suture arm.
1.7. Analysis.

Comparison 1 Adhesive versus suture, Outcome 7 Patient/parent satisfaction (% satisfied).
1.8. Analysis.

Comparison 1 Adhesive versus suture, Outcome 8 Patient/parent satisfaction (VAS Scale 0 to 100).
1.9. Analysis.

Comparison 1 Adhesive versus suture, Outcome 9 Surgeon satisfaction (% satisfied).
Costs
Four studies reported costs. Shamiyeh 2001 reported that one tube of tissue adhesive at USD 11.00 could be used to close 3.5 incisions of 5 mm mean length, while one suture at USD 1.10 could be used to close five incisions, and one package of tape (six pieces) at USD 0.24 could be used to close three incisions ‐ this calculation assumes multiple incisions on the same patient. A second study reported that for closure of laparoscopic trocar wounds the costs were EUR 13.90 for one ampoule of octylcyanoacrylate, EUR 2.47 for one package of poliglecaprone suture (used together with a dressing at EUR 0.42 each) and EUR 1.15 per package of adhesive paper tape (Maartense 2002). Eggers 2011 reported that the total cost associated with surgery for each of the closure groups (including all aspects of surgery associated with materials, labour, and operating room expenses) was USD 993.20 for octylcyanoacrylate; USD 878.27 for butylcyanoacrylate and USD 1056.32 for staples. No measures of variation were presented. Sebesta 2004 reported that the mean tissue adhesive cost per patient was USD 65.10 (range USD 40.60 to USD 101.5; standard deviation (SD) USD 13.70) whilst the total cost for surgery in the octylcyanoacrylate group (i.e. cost for operating room time, cost and cost of suture material) was USD 193.32 (range USD 130 to USD 365; SD USD 49.40). For the suture group the mean suture cost per patient was USD 7.74 (range USD 3.60 to USD 10.80; SD USD 2.05) and the total mean cost was USD 497 (range USD 295 to USD 835; SD USD 139.70).
Time for wound closure following surgery
Five studies reported the time taken for closure (Brown 2009; Ong 2002; Ozturan 2001; Sebesta 2004; Shamiyeh 2001). Pooling these trials was not appropriate due to massive heterogeneity (I2 = 100%; Analysis 1.10). Two of the trials suggested that adhesive took longer to apply than sutures, and in one of these trials the difference was statistically significant (Shamiyeh 2001), although the units for this were unclear ‐ if measured in seconds then the difference, although significant, could be small in terms of total time saved with one method compared to the other. In remaining three trials, suturing took significantly more time than adhesive (Brown 2009; Ozturan 2001; Sebesta 2004). Sebesta 2004 reported that application of adhesive took on average 3.7 minutes compared with 14 minutes on average in the suture group. Ong 2002 and Ozturan 2001 were both deemed to be at high risk of bias for one domain (Figure 1; Figure 2).
1.10. Analysis.

Comparison 1 Adhesive versus suture, Outcome 10 Time taken for wound closure.
Summary: tissue adhesives compared with sutures
There was an overall difference favouring sutures over tissue adhesives in that sutures led to a reduced risk of dehiscence, though several studies that contributed data to this analysis had at least one risk of bias domain that was classed as being at high risk. Removal of studies with a possible unit of analysis issue reduced the precision and the results then lay just outside the standard definition of statistical significance.There was no evidence of a difference in the risk of developing a wound infection in trial groups ‐ although the comparison is underpowered and confidence intervals are wide. One study was at both low and unclear risk of bias across domains: its results were statistically significant and suggested that using sutures for closure was slightly faster than using tissue adhesives. However, a second study had opposite findings, which were also statistically significant, suggesting that closure with tissue adhesive was significantly faster than sutures by over 10 minutes on average.
Comparison 2. Tissue adhesives compared with adhesive tape
Three trials provided data comparing tissue adhesives with adhesive tape (Maartense 2002; Romero 2011; Shamiyeh 2001). These trials were rated as being at low or unclear risk of bias for domains (Figure 1; Figure 2).
Primary outcome
There was no significant difference between closure techniques in the single trial that contributed data to this comparison for dehiscence (RR 0.96, 95% CI 0.06 to 14.55; Analysis 2.1; Shamiyeh 2001): this comparison was underpowered, as only one participant experienced dehiscence in each group.
2.1. Analysis.

Comparison 2 Adhesive versus adhesive tape, Outcome 1 Dehiscence.
Secondary outcomes
Infection
All three trials reported wound infection, but there was no evidence of a difference between the groups in the proportion of participants with infection (RR 1.37 95% CI 0.39 to 4.81; Analysis 2.2). Again this comparison was underpowered, with only 10 infection events in total.
2.2. Analysis.

Comparison 2 Adhesive versus adhesive tape, Outcome 2 Infection.
Cosmetic appearance
Maartense 2002 and Romero 2011 found no statistically significant difference for participants' assessment of cosmetic appearance (Analysis 2.3; Analysis 2.4), however both studies reported evidence of a difference for the surgeons' blinded assessment using a VAS favouring closure by adhesive tape (pooled estimate MD 9.56, 95% CI: 4.74 to 14.37; I2 = 14%; Analysis 2.5).
2.3. Analysis.

Comparison 2 Adhesive versus adhesive tape, Outcome 3 Cosmetic appearance rated by patient (VAS).
2.4. Analysis.
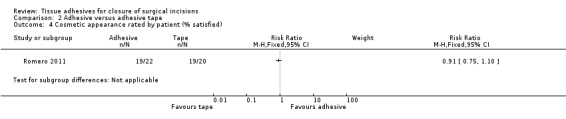
Comparison 2 Adhesive versus adhesive tape, Outcome 4 Cosmetic appearance rated by patient (% satisfied).
2.5. Analysis.

Comparison 2 Adhesive versus adhesive tape, Outcome 5 Cosmetic appearance rated by surgeon (VAS).
Patient/surgeon satisfaction
Shamiyeh 2001 found no difference between the groups for patient satisfaction (Analysis 2.6). Similarly, Maartense 2002 and Shamiyeh 2001 found no evidence of a difference between the groups with respect to surgeons' satisfaction (Analysis 2.7).
2.6. Analysis.

Comparison 2 Adhesive versus adhesive tape, Outcome 6 Patient satisfaction.
2.7. Analysis.

Comparison 2 Adhesive versus adhesive tape, Outcome 7 Surgeon satisfaction.
Time to wound closure following surgery
Shamiyeh 2001 presented data for time to closure and demonstrated that tapes were significantly faster to use than adhesives (MD 0.56, 95% CI 0.42 to 0.70; Analysis 2.8). (Review authors' note: units not reported in trial, we assumed that units are minutes).
2.8. Analysis.

Comparison 2 Adhesive versus adhesive tape, Outcome 8 Time taken for wound closure.
Summary: tissue adhesive compared with adhesive tape
There were limited data for wound dehiscence and wound infection for the comparison of tissue adhesive against adhesive tape. Only one trial reported dehiscence as an outcome, and this was underpowered. Three trials reported wound infection as an outcome, and these were also underpowered. Based on these small studies there is currently no evidence of a difference in the incidence of dehiscence or wound infection when wounds are closed with tissue adhesive or tape. Surgeons' assessment (blinded) of the cosmetic outcome was better in the tape group. One study reported a significant difference in time taken for closure and this favoured adhesive tape (time units not clear).
Comparison 3. Tissue adhesives compared with staples
Six studies compared a tissue adhesive with staples for wound closure (Amin 2009; Eggers 2011; Khan 2006; Livesey 2009; Pronio 2011; Ridgway 2007).
Primary outcome
Two trials that compared the use of tissue adhesives with staples presented data for dehiscence (Eggers 2011; Pronio 2011). As there were no cases of dehiscence in one trial, only one trial contributed data to the comparison (Eggers 2011). There was no statistically significant difference in the proportion of wounds that dehisced in the tissue adhesive group compared to the staples group (RR 0.53, 95% CI 0.05 to 5.33; Analysis 3.1).
3.1. Analysis.

Comparison 3 Adhesive versus staples, Outcome 1 Dehiscence.
Secondary outcomes
Infection
Four trials that compared the use of tissue adhesive with staples presented data on wound infection (Eggers 2011; Khan 2006; Livesey 2009; Pronio 2011), however as there were no cases of wound infection in one trial, data from three trials contribute data to the comparison (Eggers 2011; Khan 2006; Livesey 2009). There was no evidence of a difference in the proportion of wounds that became infected in the tissue adhesive group compared to the staples group (RR 1.39, 95% CI 0.30 to 6.54; Analysis 3.2).
3.2. Analysis.

Comparison 3 Adhesive versus staples, Outcome 2 Infection.
Cosmetic appearance
Pronio 2011 found no evidence of a difference between the groups for patient‐assessed cosmetic outcome (Analysis 3.3). Similarly Livesey 2009 found there was no evidence for a difference between the groups with respect to the cosmetic appearance by surgeons (Analysis 3.4).
3.3. Analysis.

Comparison 3 Adhesive versus staples, Outcome 3 Cosmetic appearance rated by patient (scar scale).
3.4. Analysis.

Comparison 3 Adhesive versus staples, Outcome 4 Cosmetic appearance by plastic surgeons (VAS).
Patient/surgeon satisfaction
Amin 2009 found a statistically significant difference between the groups for patient satisfaction in favour of tissue adhesive (MD 1.10; 95% CI 0.41 to 1.79; Analysis 3.5).
3.5. Analysis.

Comparison 3 Adhesive versus staples, Outcome 5 Patient satisfaction.
Costs
Eggers 2011 reported that the total cost associated with surgery for each of the closure groups (including all aspects of surgery associated with materials, labour, and operating room expenses) was USD 993.20 for octylcyanoacrylate; USD 878.27 for butylcyanoacrylate and USD 802.79 for staples.
Time to wound closure following surgery
Ridgway 2007 reported the time to closure and found a statistically significant difference favouring the use of staples (MD 67.0 seconds, 95% CI 39.3 to 94.7; Analysis 3.6). The study had risk of bias domains classified as both low and unclear.
3.6. Analysis.

Comparison 3 Adhesive versus staples, Outcome 6 Time taken for wound closure.
Summary: tissue adhesive compared with staples
There was no evidence of a difference in wound dehiscence, wound infection, or cosmetic appearance between use of tissue adhesives or staples for wound closure. There was a significant difference in patient satisfaction in favour of tissue adhesives. There was also a significant difference in time taken for closure that favoured staples, however, the difference between groups was only just over 60 seconds, so whilst the result was statistically significant, it was not significant from a clinical point of view.
Comparison 4. Tissue adhesives compared with other techniques
Blondeel 2004 compared high viscosity adhesive with any other commercially available devices such as sutures, staples, tapes or low viscosity adhesive. We requested further information from the authors, specifically data regarding high and low viscosity adhesives compared with the remaining commercially available devices and data for the comparison of high viscosity with low viscosity adhesives for the outcomes of interest to this review. This comparison of data was not reported within the published paper, but the author made the data available to the review team. This paper was designated as being at low risk of bias. Chibbaro 2009 compared tissue adhesive with a comparison group that received sutures or staples.
Primary outcome
Blondeel 2004 found no significant difference between the groups for dehiscence (RR 0.55, 95% CI 0.13 to 2.38; Analysis 4.1). Chibbaro 2009 reported dehiscence, but there were no events in either group.
4.1. Analysis.

Comparison 4 Adhesive versus other method, Outcome 1 Dehiscence.
Secondary outcomes
Infection
Blondeel 2004 found no significant difference between the groups for infection (RR 0.41, 95% CI 0.11 to 1.60; Analysis 4.2). Chibbaro 2009 reported wound infection, but there were no events in either group.
4.2. Analysis.

Comparison 4 Adhesive versus other method, Outcome 2 Infection.
Patient/surgeon satisfaction
Blondeel 2004 reported statistically significant differences in favour of the group treated with other devices such as sutures, staples and tapes for both patient satisfaction (MD 0.40, 95% CI 0.10 to 0.70; Analysis 4.3) and clinician satisfaction (MD 0.53, 95% CI 0.29 to 0.77; Analysis 4.4).
4.3. Analysis.

Comparison 4 Adhesive versus other method, Outcome 3 Patient satisfaction.
4.4. Analysis.

Comparison 4 Adhesive versus other method, Outcome 4 Clinician satisfaction.
Time for closure
Blondeel 2004 reported that closure took significantly less time with tissue adhesive (MD ‐1.05 minutes, 95% CI ‐1.79 to ‐0.31; Analysis 4.5). Data reported for this outcome by Chibbaro 2009 were unclear.
4.5. Analysis.

Comparison 4 Adhesive versus other method, Outcome 5 Time taken for wound closure.
Summary: tissue adhesive compared with other techniques
When tissue adhesives were compared with other techniques there was no evidence of a difference in wound dehiscence or wound infection between groups. When assessing surgeon and patient satisfaction there was a statistical difference favouring the control group (other techniques) over tissue adhesives. In this same analysis there was a statistically significant difference favouring the tissue adhesive for time taken to closure ‐ the mean time saving was one minute.
Comparison 5. Adhesives compared with adhesives
Comparison 5.1. High versus low viscosity adhesives
The data for this comparison were provided by the authors as an additional analysis to that found in the paper.
Primary outcome
Blondeel 2004 found no significant difference between the high viscosity and low viscosity adhesive intervention groups for dehiscence (RR 3.74, 95% CI 0.21 to 67.93; Analysis 5.1). This paper was designated as being at unclear risk of bias.
5.1. Analysis.

Comparison 5 Adhesive versus adhesive: High viscosity versus low viscosity, Outcome 1 Dehiscence.
Secondary outcomes
Infection
No statistically significant differences were found between intervention groups for infection (Analysis 5.2).
5.2. Analysis.

Comparison 5 Adhesive versus adhesive: High viscosity versus low viscosity, Outcome 2 Infection.
Patient/surgeon satisfaction
No statistically significant differences were found between intervention groups for patient or surgeon satisfaction (Analysis 5.3; Analysis 5.4).
5.3. Analysis.

Comparison 5 Adhesive versus adhesive: High viscosity versus low viscosity, Outcome 3 Patient satisfaction.
5.4. Analysis.

Comparison 5 Adhesive versus adhesive: High viscosity versus low viscosity, Outcome 4 Clinician satisfaction.
Time for closure
For time to closure, there was a significant difference favouring low viscosity adhesive (MD 0.54 minutes, 95% CI 0.03 to 1.05; Analysis 5.5).
5.5. Analysis.

Comparison 5 Adhesive versus adhesive: High viscosity versus low viscosity, Outcome 5 Time taken for wound closure.
Comparison 5.2. Octylcyanoacrylate vs butylcyanoacrylate
Three trials compared octylcyanoacrylate tissue adhesive with butylcyanoacrylate tissue adhesive (Eggers 2011; Kent 2014; Maloney 2013). We assessed Maloney 2013 as being at low or unclear risk of bias for domains. Eggers 2011 was assessed as being at unclear risk of bias for incomplete outcome data and Kent 2014 for randomising at the participant level, but presenting unadjusted data at the wound level. We were unable to re‐analyse the Kent 2014 data correctly here, as we had planned to report data at the participant level only, but did not do this because of the amount of missing data.
Primary outcome
Eggers 2011 reported no statistically significant difference in wound dehiscence between groups (RR: 0.95, 95% CI 0.06 to 14.04; Analysis 6.1). Likewise Maloney 2013 did not report a statistically significant difference in wound dehiscence between groups (RR: 2.63, 95% CI 0.11 to 61.05; Analysis 6.1). These data were pooled and returned a result that showed there could be an effect in either direction, or none (RR 1.46, 95% CI 0.19 to 11.30; Analysis 6.1; very low precision due to the small sample size).
6.1. Analysis.
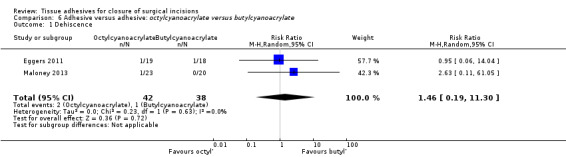
Comparison 6 Adhesive versus adhesive: octylcyanoacrylate versus butylcyanoacrylate, Outcome 1 Dehiscence.
Secondary outcomes
Infection
Eggers 2011 report no statistically significant different between different tissue adhesives in terms of wound infection (RR 0.63, 95% CI 0.21 to 1.88; Analysis 6.2). Maloney 2013 reported no events for either trial arm for infection.
6.2. Analysis.

Comparison 6 Adhesive versus adhesive: octylcyanoacrylate versus butylcyanoacrylate, Outcome 2 Infection.
Cosmetic appearance
Maloney 2013 reported no evidence of a difference in participant‐assessed cosmetic outcome between study groups. Likewise there was no evidence of a difference in blinded surgeon‐assessed cosmetic appearance (Analysis 6.3; Analysis 6.4).
6.3. Analysis.

Comparison 6 Adhesive versus adhesive: octylcyanoacrylate versus butylcyanoacrylate, Outcome 3 Cosmetic assessment rated by patient (VAS).
6.4. Analysis.

Comparison 6 Adhesive versus adhesive: octylcyanoacrylate versus butylcyanoacrylate, Outcome 4 Cosmetic assessment rated by surgeon (VAS).
Patient/surgeon satisfaction
Surgeons' satisfaction with skin incision closure technique, in terms of ease of use and satisfaction with closure, was assessed using a VAS. There was no evidence of a difference between groups for these measures (Analysis 6.5; Analysis 6.6.).
6.5. Analysis.

Comparison 6 Adhesive versus adhesive: octylcyanoacrylate versus butylcyanoacrylate, Outcome 5 Surgeon satisfaction (with device).
6.6. Analysis.

Comparison 6 Adhesive versus adhesive: octylcyanoacrylate versus butylcyanoacrylate, Outcome 6 Surgeon satisfaction (with closure).
Costs
Eggers 2011 reported that the total cost associated with surgery for each of the closure groups (including all aspects of surgery associated with materials, labour, and operating room expenses) was USD 993.20 for octylcyanoacrylate and USD 878.27 for butylcyanoacrylate.
Time for wound closure following surgery
Maloney 2013 reported a significant difference in time for wound closure favouring octylcyanoacrylate (MD ‐25.50, 95% CI ‐39.79 to ‐11.21; Analysis 6.7). It is important to note that the units for this assessment were seconds ‐ so whilst there is a statistically significant difference it is one of, on average, about 26 seconds between treatment arms, which probably does not translate to a significant clinical difference.
6.7. Analysis.

Comparison 6 Adhesive versus adhesive: octylcyanoacrylate versus butylcyanoacrylate, Outcome 7 Time taken for wound closure.
Summary: tissue adhesive compared with other tissue adhesive
There was no evidence of a difference in any outcome assessed when different types of tissue adhesives were compared, except for high viscosity compared with low viscosity adhesives where there was a statistical difference favouring the low viscosity adhesive for time taken for closure (mean difference approximately 1 minute). Likewise, one study reported a significant difference in time taken for wound closure favouring octylcyanoacrylate but the size of the difference was small.
Overall summary of results by outcome
Dehiscence
When tissue adhesives were compared with sutures, pooled data from 17 studies (with 10 contributing data towards the analysis) showed a statistically significant difference favouring sutures, as they reduced the risk of dehiscence. It is possible this result may have been influenced by unit of analysis issues, as it was not clear whether more than one dehiscence event per participant had been recorded in studies with multiple follow‐up points. No other comparison of tissue adhesives with other closure methods showed a statistically significant difference in the risk of wound dehiscence.
Wound infection
There was no evidence of a difference in the risk of wound infection between wounds closed with tissue adhesives and wounds closed using other methods reported here.
Cosmetic appearance
Two studies with blinded outcome assessment reported a statistically significant difference in surgeon‐assessed appearance score that favoured the tape group over tissue adhesives.
Patient/surgeon satisfaction
When tissue adhesives were compared with a mixed control group (i.e. sutures, staples and tape), one study reported a statistically significant difference in patient and surgeon satisfaction scores that favoured the mixed control group, while another study that compared tissue adhesive with staples found a significant difference in patient satisfaction that favoured the tissue adhesive.
Time to wound closure (following surgery)
One study suggested that, on average, it took 10 minutes longer to close a wound with sutures than with tissue adhesives, but this was not borne out in all the studies and may depend on factors such as wound type. There was a statistically significant difference in time taken for closure between tissue adhesives and tape‐closed wounds, that favoured the tape group. There was also a significant difference in time taken for closure between tissue adhesives compared with staples that favoured the staples group, however, the difference between groups was only just over 60 seconds, so whilst it was statistically significant it was not clinically significant. Another study that compared tissue adhesive with a mixed control group (i.e. staples, sutures and tape) found a statistically significant difference in time to closure that favoured tissue adhesive, although the mean difference between groups was again approximately one minute. Finally, one study reported that there was a small, but statistically significant difference in time to closure that favoured low viscosity adhesive over high viscosity adhesive, and favoured octylcyanoacrylate tissue adhesive over butylcyanoacrylate tissue adhesive.
'Summary of findings' table
We present 'Summary of findings' tables for the dehiscence and infection outcomes. These tables confirm our conclusion that the available evidence is generally underpowered and is limited in some cases by a lack of reported methodological information that would permit full analysis of the data. (Table 1; Table 2; Table 3; Table 4; Table 5; Table 6)
Discussion
Summary of main results
Traditional methods of surgical incision closure have been used for many years. However, these techniques are not without some problems and it is therefore important to consider new developments ‐ such as tissue adhesives ‐ which may offer some advantages for patients. This review included a total of 33 studies: 23 studies compared tissue adhesives with sutures; three studies compared tissue adhesives with adhesive tape, which is often used for smaller incisions; six studies compared adhesives with staples; two studies compared tissue adhesives with mixed control groups; and two studies compared different types of tissue adhesives. A notable finding in this review was that, when data from ten studies that compared tissue adhesives with sutures were pooled, a significant difference in risk of wound dehiscence became apparent, with a higher risk of dehiscence associated with tissue adhesives. No other comparison showed evidence for a difference in risk of wound dehiscence for alternative treatments. It is important to note the often unclear and sometime high risk of bias of included studies. Many studies were also underpowered, and the primary outcome here ‐ dehiscence ‐ was not used as a basis for sample size calculation. The surgical procedures described by the studies were diverse and included blepharoplasty, circumcision, and excision of benign skin lesions. Incision in areas of high tension and in those patients whose medical health may have reduced their ability to heal were excluded and so tissue adhesives have not been evaluated in this population.
Postoperative site infection is a common problem and has a significant impact on patients and healthcare systems. More than 70% of surgical procedures are now performed on a outpatient basis, which poses major problems for surveillance of surgical site infections (Emori 1993). In one study of 2345 patients undergoing surgery, the overall incidence of surgical site infection was 8.5% (Malone 2002). One might anticipate that a tissue adhesive offers a barrier to micro‐organisms at the site of the healing incision and may therefore contribute towards reducing wound infection. However, the studies identified for this review did not demonstrate any significant difference in the proportion of infections in incisions closed with tissue adhesives compared with other conventional techniques. No study reported an a priori calculation for the sample size, and this may be relevant. Even the largest of the studies would have been unlikely to have been adequately powered to show any significant difference given the relatively low incidence of wound infections following many types of surgery.
Cosmetic outcome is an important long‐term outcome of wound repair for the patient and we considered appearance at or beyond three months after surgery to be meaningful. Some studies reported cosmetic outcome earlier than this three month time point (Blondeel 2004). Whilst is has been reported that an individual patient's cosmetic outcome at three months is predictive of cosmetic appearance at one year (Quinn 1998), the same investigation reported that early outcome, such as at five or 10 days, is poorly predictive of the three month appearance. This can present a problem for trials, as attrition bias may influence the results. The only difference identified in cosmetic appearance was for the comparison of tissue adhesive with adhesive tape ‐ this was a blinded assessment by surgeons that favoured tape. Assessments for this comparison were limited, so there was a great deal of uncertainty regarding the comparative risk of wound dehiscence and infection when tape was compared with tissue adhesive.
Patient satisfaction is also important when comparing alternative incision closure devices providing that the primary efficacy variables of dehiscence, infection and cosmetic appearance are satisfactory. Patient satisfaction may include ratings for cosmesis, overall comfort, ability to shower, dressing changes, tension on wounds, hygiene problems, allergic reactions and overall satisfaction. Another important benefit of tissue adhesives is that they do not need to be removed. One small study suggested that patients had a preference for adhesive rather than sutures (Greene 1999), although it was not clear what dimensions it measured. A further small study also suggested that patients were had higher satisfaction with tissue adhesive than staples. Conversly, one study that compared traditional closure methods to tissue adhesives demonstrated a significant patient preference for the alternatives to tissue adhesives (Blondeel 2004): this was the largest of the studies to assess patient satisfaction. It would be helpful if validated questionnaires were available to use in studies.
Surgeon satisfaction assessments typically sought ratings for wound cosmesis or ease of use for the technique. Certainly there is no risk of needle‐stick injury to the surgeon whilst using adhesive rather than sutures, and this may be a factor in favour of adhesives, though none of the studies in this review considered this. In one study physicians completed a questionnaire that measured satisfaction with the ease of use of a device, wound cosmesis, safety, effectiveness, applicability to a wide range of incisions, perceived patient satisfaction and overall satisfaction (Blondeel 2004). This study showed that clinicians significantly preferred the alternative to tissue adhesive, but when comparing high viscosity adhesives to other adhesives, operators showed no difference in preference.
We included time to closure as an outcome measure in the review post hoc, as the review authors believe this to be a contributory factor towards both cost‐effectiveness and satisfaction. Studies suggested that tissue adhesives might be significantly quicker than suturing for some wounds, although there was heterogeneity around this that might be related to the type and size of wound being assessed, and suturing was reported to be the faster method in other studies. In other comparisons closure with tape and staples was found to be faster than with tissue adhesives ‐ but the differences in time, whilst statistically significant, were generally only small periods of difference ‐ for example 60 seconds.
Whilst time taken is an attractive aspect for surgeons, it should be noted that although there maybe a significant difference in time taken for closure, the overall time taken was still relatively small in both groups with even the longest closure times rarely exceeding two minutes. In clinical practice the reduction of wound closure time through using the quickest method may be insufficient to increase the number of operations in a given operating room schedule. However, a faster wound closure technique may increase surgeon satisfaction and may also be attractive to patients when surgery is undertaken using only local anaesthetic. Alternatively, patients may be happy with a lengthier closure time for a technique that achieves better outcomes.
Generally, tissue adhesives cost more than the alternatives. An ampoule of tissue adhesive may be three times or more the cost of the suture required to close the same length of incision. However, a dressing is not required over the tissue adhesive, but is routinely used with alternatives. Also, when taking into account the overall cost of the surgical procedure, this small difference may be of less significance. It may be considered important to use a specific closure device, even if the cost is greater, if significant superiority is demonstrated for wound healing, including cosmetic outcome and patient satisfaction. Thus the length of time for closure and cost may be important only after other outcomes such as dehiscence, cosmesis and infection have been considered.
In summary, there is some evidence that dehiscence rates may be higher in wounds closed with tissue adhesives than with sutures. This finding agrees with a review published in 2010 that includes similar wound dehiscence data to this review (Chow 2010), although the authors did not perform a sensitivity analysis based on possible unit of analysis issues, as we have here.
There was no evidence of any difference between sutures and tissue adhesive for outcomes such as cosmetic appearance and satisfaction. The relative time taken using sutures for wound closure rather than tissue adhesives seems to vary, with one study showing use of adhesive to be significantly faster than sutures and another study showing suturing to be significantly faster than tissue adhesive. Other studies reported that tissue adhesive took longer to apply than staples and tape. Generally, there was limited comparative evidence to determine whether tissue adhesives led to lower or higher levels of dehiscence, infection, satisfaction with cosmetic outcome, or patient or surgeon general satisfaction. Surgeons and patients were significantly more satisfied with the alternatives to adhesives in one analysis, but this finding was not replicated in other studies. There was no evidence of a difference in outcomes between tissue adhesive types except that high viscosity adhesives took significantly more time for skin closure, adding a minute on average to the procedure.
Authors' conclusions
Implications for practice.
Thirty‐three studies, including 2793 participants, compared tissue adhesives with alternative methods of surgical wound closure. These provided no evidence of a difference in rates of wound infection after surgical incision closure with tissues adhesives, sutures, tapes, staples or amongst different tissue adhesives. When adhesive was compared with suture there was evidence of a benefit for using sutures for minimising dehiscence.
Although there was some evidence that surgeons and patients may prefer alternative methods to tissue adhesives, there was also evidence that patient satisfaction with tissue adhesives was higher than for staples. Although some analyses demonstrated that alternatives to tissue adhesives were less time consuming to use, this does not contraindicate their use, and this conclusion was refuted by the results of other studies. However, these trials did not consider incisions in areas of high tension, such as the elbow and knee, which therefore have not been evaluated with tissue adhesives. Similarly, trials excluded patients whose general health may have had the potential to impair wound healing, so tissue adhesives have not been evaluated in these populations.
Implications for research.
Further adequately powered trials should be undertaken to investigate the effects of tissue adhesives in clinical situations commonly excluded in trials, specifically, wound closure in areas of high tension and in patients with general health that could potentially impair wound healing. Trials should be sufficiently powered to detect any differences in the rate of wound infection or dehiscence as statistically significant when comparing different incision closure devices. As any future trial would need to be large, it would probably be multicentred. It would require methodological rigour to address the outstanding uncertainties in this area appropriately. Development and validation of patient satisfaction and surgeon satisfaction questionnaires would be helpful.
What's new
| Date | Event | Description |
|---|---|---|
| 1 August 2014 | New citation required but conclusions have not changed | New search, risk of bias updated for all studies into current format, revisions to text, no change to conclusions |
| 1 August 2014 | New search has been performed | Second update: 19 new studies added: Amin 2009; Avsar 2009; Brown 2009; Chibbaro 2009; Eggers 2011; Jallali 2004; Kent 2014; Khan 2006; Kouba 2011; Krishnamoorthy 2009; Livesey 2009; Maloney 2013; Millan 2011; Mota 2009; Pronio 2011; Romero 2011; Sebesta 2004; Tierny 2009; van den Ende 2004. Five studies are awaiting assessment: Gennari 2004; Handschel 2006; Jan 2013; Nipshagen 2008; Yoon 2006 |
History
Protocol first published: Issue 3, 2003 Review first published: Issue 2, 2004
| Date | Event | Description |
|---|---|---|
| 3 August 2010 | Amended | Contact details updated. |
| 23 November 2009 | New search has been performed | New search and an additional 6 studies included in the review (Blondeel 2004; Dowson 2006; Ong 2002; Ridgway 2007; Sniezek 2007; Switzer 2003). Three studies were excluded (Jaibaji 2000; Orozco‐Razon 2002; Steiner 2000) and 7 studies are awaiting assessment. |
| 23 November 2009 | New citation required and conclusions have changed | Time to closure as an outcome measure was included in the review at the time of this update (post hoc). The review authors believe this to be a contributory factor towards both cost‐effectiveness and satisfaction. An additional review author has joined the review team for this first update. |
| 16 May 2002 | New citation required and conclusions have changed | Substantive amendment |
Acknowledgements
We wish to thank Sally Bell‐Syer and Ruth Foxlee (Cochrane Wounds Group) for their assistance with literature searching the preparation of this review. We would also like to thank the following referees: Nicky Cullum, David Margolis, Michelle Briggs, Seokyung Hahn, James V Quinn, Ken Farion and Jac Dinnes. We also thank Matthew Fortnam who extracted data and checked quality of data extraction for this second review update.
Appendices
Appendix 1. Search strategy used in the original version of this review ‐ 2007
In order to identify studies to be considered for this review the following databases were searched:
Cochrane Wounds Group Trials Register ‐ November 2007 The Cochrane Central Register of Controlled Trials (CENTRAL) ‐ The Cochrane Library Issue 2, November 2007 MEDLINE 1966 ‐ November 2007 EMBASE 1980 ‐ November 2007
The Cochrane Wounds Group Trials Register has been compiled through searching of the major health databases including MEDLINE, Cinahl and EMBASE and is regularly updated through searching of the Cochrane Central Register of Controlled Trials, handsearching of wound care journals and relevant conference proceedings. See: Collaborative review group search strategy (http:/www.cochranewounds.org).
The following search strategy was used for searching the Cochrane Wounds Group Trials Register and CENTRAL:
1 WOUNDS‐AND‐INJURIES*:ME 2 INCISION* 3 WOUND* 4 (SURGICAL and WOUND*) 5 (((#1 or #2) or #3) or #4) 6 TISSUE‐ADHESIVES*:ME 7 ADHESIVES*:ME 8 ACRYLATES*:ME 9 (TISSUE* and ADHESIVE*) 10 ACRYLATE* 11 CYANOACRYLATE* 12 (GLU or GLUES) 13 (GLUE or GLUES) 14 FIBRIN‐TISSUE‐ADHESIVE*:ME 15 BUCRYLATE*:ME 16 BUCRYLATE* 17 SUTURES*:ME 18 SUTUR* 19 SURGICAL‐STAPLING*:ME 20 STAPLE* 21 TAPE* 22 (((((((((((((((#6 or #7) or #8) or #9) or #10) or #11) or #12) or #13) or #14) or #15) or #16) or #17) or #18) or #19) or #20) or #21) 23 (#5 and #22)
Search strategies were developed for Medline and Embase and these search strategies combined a sensitive search strategy for RCTs revised from phases 1 and 2 of the Cochrane Sensitive Search Strategy for RCTs (as published in Appendix 6c in the Cochrane Handbook). The subject search used a combination of controlled vocabulary and free text terms based on the search strategy for searching the Cochrane Wounds Group Trial Register.
LANGUAGE There were no language restrictions.
UNPUBLISHED STUDIES Authors of the identified RCTs were written to in order to obtain further information about the trial and to attempt to identify unpublished or ongoing studies. In addition, wound care product manufacturers were contacted.
HANDSEARCHING Trials for Wounds Group Trials Register are identified by systematically handsearching specialised journals, relevant conference proceedings and abstracts. A list of journals currently being handsearched by the group may be found at http:/www.cochranewounds.org.
Appendix 2. Search strategy for the first update of this review ‐ 2009
In order to identify studies to be considered for this review the following databases were searched:
Cochrane Wounds Group Specialised Register (November 2009;); The Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2009, Issue 4); Ovid MEDLINE (1996 to November week 1 2009); Ovid MEDLINE (In‐Process & Other Non‐Indexed Citations, November 16 2009); Ovid EMBASE (1996 to 2009 week 46); EBSCO CINAHL (1982 to 11 November 2009)
The Cochrane Wounds Group Trials Register has been compiled through searching of the major health databases including MEDLINE, Cinahl and EMBASE and is regularly updated through searching of the Cochrane Central Register of Controlled Trials, handsearching of wound care journals and relevant conference proceedings. See: Collaborative review group search strategy (http:/www.cochranewounds.org).
The following search strategy was used for searching the Cochrane Central Register of Controlled Trials (CENTRAL):
#1 MeSH descriptor Wounds and Injuries explode all trees #2 surgical next wound* #3 (#1 OR #2) #4 MeSH descriptor Tissue Adhesives explode all trees #5 MeSH descriptor Fibrin Tissue Adhesive explode all trees #6 tissue next adhesive* #7 MeSH descriptor Cyanoacrylates explode all trees #8 octylcyanoacrylate* #9 Dermabond #10 MeSH descriptor Enbucrilate explode all trees #11 enbucrilate #12 butylcyanoacrylate* #13 MeSH descriptor Acrylates explode all trees #14 acrylate* #15 MeSH descriptor Bucrylate explode all trees #16 bucrylate* #17 (#4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16) #18 (#3 AND #17) with New in Record Status
Appendix 3. Ovid MEDLINE search strategy
Undertaken for second update in 2014
1 exp "Wounds and Injuries"/ (691113) 2 (surgical adj wound$).mp. (35309) 3 or/1‐2 (721540) 4 exp Tissue Adhesives/ (12636) 5 exp Fibrin Tissue Adhesive/ (3859) 6 tissue adhesive$.mp. (8303) 7 exp Cyanoacrylates/ (3816) 8 octylcyanoacrylate$.mp. (103) 9 Dermabond.mp. (114) 10 exp Enbucrilate/ (1496) 11 enbucrilate.mp. (1236) 12 butylcyanoacrylate$.mp. (119) 13 exp Acrylates/ (41800) 14 acrylate$.mp. (8636) 15 exp Bucrylate/ (280) 16 bucrylate$.mp. (309) 17 or/4‐16 (51986) 18 3 and 17 (3841) 19 randomized controlled trial.pt. (366703) 20 controlled clinical trial.pt. (87802) 21 randomi?ed.ab. (318385) 22 placebo.ab. (143748) 23 clinical trials as topic.sh. (168638) 24 randomly.ab. (189528) 25 trial.ti. (114737) 26 or/19‐25 (860509) 27 exp animals/ not humans.sh. (3901060) 28 26 not 27 (791299) 29 18 and 28 (276)
Appendix 4. Ovid EMBASE search strategy
Undertaken for second update in 2014
1 exp Surgical Wound/ (3914) 2 (surgical adj wound$).mp. (8021) 3 or/1‐2 (8021) 4 exp Tissue Adhesive/ (13492) 5 exp Fibrin Glue/ (6712) 6 (tissue adj adhesive$).mp. (5179) 7 exp Cyanoacrylate Derivative/ (1595) 8 exp Cyanoacrylic Acid Octyl Ester/ (340) 9 octylcyanoacrylate$.mp. (130) 10 Dermabond.mp. (343) 11 exp ENBUCRILATE/ (2847) 12 enbucrilate.mp. (2852) 13 butylcyanoacrylate$.mp. (190) 14 exp Acrylic Acid/ (3718) 15 acrylate$.mp. (6120) 16 exp Bucrilate/ (623) 17 bucrylate$.mp. (138) 18 or/4‐17 (23772) 19 3 and 18 (181) 20 Randomized controlled trials/ (47799) 21 Single‐Blind Method/ (17933) 22 Double‐Blind Method/ (114456) 23 Crossover Procedure/ (38119) 24 (random$ or factorial$ or crossover$ or cross over$ or cross‐over$ or placebo$ or assign$ or allocat$ or volunteer$).ti,ab. (1300258) 25 (doubl$ adj blind$).ti,ab. (143978) 26 (singl$ adj blind$).ti,ab. (14109) 27 or/20‐26 (1365111) 28 exp animals/ or exp invertebrate/ or animal experiment/ or animal model/ or animal tissue/ or animal cell/ or nonhuman/ (19982416) 29 human/ or human cell/ (14519180) 30 and/28‐29 (14472519) 31 28 not 30 (5509897) 32 27 not 31 (1177074) 33 19 and 32 (35)
Appendix 5. EBSCO CINAHL search strategy
Undertaken for second update in 2014
S29 S16 AND S28 S28 S17 or S18 or S19 or S20 or S21 or S22 or S23 or S24 or S25 or S26 or S27 S27 TX allocat* random* S26 (MH "Quantitative Studies") S25 (MH "Placebos") S24 TX placebo* S23 TX random* allocat* S22 (MH "Random Assignment") S21 TX randomi* control* trial* S20 TX ( (singl* n1 blind*) or (singl* n1 mask*) ) or TX ( (doubl* n1 blind*) or (doubl* n1 mask*) ) or TX ( (tripl* n1 blind*) or (tripl* n1 mask*) ) or TX ( (trebl* n1 blind*) or (trebl* n1 mask*) ) S19 TX clinic* n1 trial* S18 PT Clinical trial S17 (MH "Clinical Trials+") S16 S5 and S15 S15 S6 or S7 or S8 or S9 or S10 or S11 or S12 or S13 or S14 S14 TI Dermabond or AB Dermabond S13 TI enbucrilate or AB enbucrilate S12 TI bucrylate* or AB bucrylate* S11 TI acrylate* or AB acrylate* S10 TI butylcyanoacrylate* or AB butylcyanoacrylate* S9 TI octylcyanoacrylate* or AB octylcyanoacrylate* S8 TI cyanoacrylate* or AB cyanoacrylate* S7 TI tissue adhesive* or AB tissue adhesive* S6 (MH "Fibrin Tissue Adhesive") S5 S1 or S2 or S3 or S4 S4 TI surgical wound* or AB surgical wound* S3 (MH "Surgical Wound Care") S2 (MH "Surgical Wound") S1 (MH "Tears and Lacerations")
Appendix 6. Risk of bias assessment
1. Was the allocation sequence randomly generated?
Low risk of bias
The investigators describe a random component in the sequence generation process such as: referring to a random number table; using a computer random number generator; coin tossing; shuffling cards or envelopes; throwing dice; drawing of lots.
High risk of bias
The investigators describe a non‐random component in the sequence generation process. Usually, the description would involve some systematic, non‐random approach, for example: sequence generated by odd or even date of birth; sequence generated by some rule based on date (or day) of admission; sequence generated by some rule based on hospital or clinic record number.
Unclear
Insufficient information about the sequence generation process provided to permit a judgement of low or high risk of bias.
2. Was the treatment allocation adequately concealed?
Low risk of bias
Participants and investigators enrolling participants could not foresee assignment because one of the following, or an equivalent method, was used to conceal allocation: central allocation (including telephone, web‐based and pharmacy‐controlled randomisation); sequentially numbered drug containers of identical appearance; sequentially numbered, opaque, sealed envelopes.
High risk of bias
Participants or investigators enrolling participants could possibly foresee assignments and thus introduce selection bias, such as allocation based on: using an open random allocation schedule (e.g. a list of random numbers); assignment envelopes were used without appropriate safeguards (e.g. if envelopes were unsealed or non opaque or not sequentially numbered); alternation or rotation; date of birth; case record number; any other explicitly unconcealed procedure.
Unclear
Insufficient information provided to permit a judgement of low or high risk of bias. This is usually the case if the method of concealment is not described or not described in sufficient detail to allow a definite judgement, for example if the use of assignment envelopes is described, but it remains unclear whether envelopes were sequentially numbered, opaque and sealed.
3. Blinding ‐ was knowledge of the allocated interventions adequately prevented during the study?
Low risk of bias
Any one of the following.
No blinding, but the review authors judge that the outcome and the outcome measurement are not likely to be influenced by lack of blinding.
Blinding of participants and key study personnel ensured, and unlikely that the blinding could have been broken.
Either participants or some key study personnel were not blinded, but outcome assessment was blinded and the non‐blinding of others unlikely to introduce bias.
High risk of bias
Any one of the following.
No blinding or incomplete blinding, and the outcome or outcome measurement is likely to be influenced by lack of blinding.
Blinding of key study participants and personnel attempted, but likely that the blinding could have been broken.
Either participants or some key study personnel were not blinded, and the non‐blinding of others was likely to introduce bias.
Unclear
Any one of the following.
Insufficient information provided to permit a judgement of low or high risk of bias.
The study did not address this outcome.
4. Were incomplete outcome data adequately addressed?
Low risk of bias
Any one of the following.
No missing outcome data.
Reasons for missing outcome data unlikely to be related to true outcome (for survival data, censoring unlikely to be introducing bias).
Missing outcome data balanced in numbers across intervention groups, with similar reasons for missing data across groups.
For dichotomous outcome data, the proportion of missing outcomes compared with observed event risk not enough to have a clinically relevant impact on the intervention effect estimate.
For continuous outcome data, plausible effect size (difference in means or standardised difference in means) among missing outcomes not enough to have a clinically relevant impact on observed effect size.
Missing data have been imputed using appropriate methods.
High risk of bias
Any one of the following.
Reason for missing outcome data likely to be related to true outcome, with either imbalance in numbers or reasons for missing data across intervention groups.
For dichotomous outcome data, the proportion of missing outcomes compared with observed event risk enough to induce clinically relevant bias in intervention effect estimate.
For continuous outcome data, plausible effect size (difference in means or standardised difference in means) among missing outcomes enough to induce clinically relevant bias in observed effect size.
‘As‐treated’ analysis done with substantial departure of the intervention received from that assigned at randomisation.
Potentially inappropriate application of simple imputation.
Unclear
Either of the following.
Insufficient reporting of attrition/exclusions to permit judgement of low or high risk of bias (e.g. number randomised not stated, no reasons for missing data provided).
The study did not address this outcome.
5. Are reports of the study free of suggestion of selective outcome reporting?
Low risk of bias
Either of the following.
The study protocol is available and all of the study’s pre‐specified (primary and secondary) outcomes that are of interest in the review have been reported in the pre‐specified way.
The study protocol is not available but it is clear that the published reports include all expected outcomes, including those that were pre‐specified (convincing text of this nature may be uncommon).
High risk of bias
Any one of the following.
Not all of the study’s pre‐specified primary outcomes have been reported.
One or more primary outcomes are reported using measurements, analysis methods or subsets of the data (e.g. subscales) that were not pre‐specified.
One or more reported primary outcomes were not pre‐specified (unless clear justification for their reporting is provided, such as an unexpected adverse effect).
One or more outcomes of interest in the review are reported incompletely so that they cannot be entered in a meta‐analysis.
The study report fails to include results for a key outcome that would be expected to have been reported for such a study.
Unclear:
Insufficient information to permit judgement of low or high risk of bias. It is likely that the majority of studies will fall into this category.
6. Other sources of potential bias
Low risk of bias
The study appears to be free of other sources of bias.
High risk of bias
There is at least one important risk of bias. For example, the study:
had a potential source of bias related to the specific study design used; or
has been claimed to have been fraudulent; or
had some other problem.
Unclear
There may be a risk of bias, but there is either:
insufficient information to assess whether an important risk of bias exists; or
insufficient rationale or evidence that an identified problem will introduce bias.
Data and analyses
Comparison 1. Adhesive versus suture.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dehiscence: all studies | 17 | 1225 | Risk Ratio (M‐H, Random, 95% CI) | 3.35 [1.53, 7.33] |
| 2 Dehiscence: sensitivity analysis | 13 | 935 | Risk Ratio (M‐H, Random, 95% CI) | 2.70 [0.95, 7.68] |
| 3 Infection: all studies | 18 | 1239 | Risk Ratio (M‐H, Random, 95% CI) | 1.72 [0.94, 3.16] |
| 4 Infection: sensitivity analysis | 15 | 977 | Risk Ratio (M‐H, Random, 95% CI) | 2.03 [0.80, 5.12] |
| 5 Cosmetic appearance rated by patient | 2 | 199 | Mean Difference (IV, Random, 95% CI) | ‐2.12 [‐7.20, 2.95] |
| 5.1 VAS 0 to 100 | 2 | 199 | Mean Difference (IV, Random, 95% CI) | ‐2.12 [‐7.20, 2.95] |
| 6 Cosmetic appearance rated by surgeon | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6.1 VAS scale 0 to 100 | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 Scar assessment (0 to 5 scale) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 Patient/parent satisfaction (% satisfied) | 2 | 206 | Risk Ratio (M‐H, Random, 95% CI) | 1.01 [0.96, 1.07] |
| 8 Patient/parent satisfaction (VAS Scale 0 to 100) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 9 Surgeon satisfaction (% satisfied) | 2 | 150 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [0.58, 2.19] |
| 10 Time taken for wound closure | 5 | Mean Difference (IV, Random, 95% CI) | Subtotals only |
Comparison 2. Adhesive versus adhesive tape.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dehiscence | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 2 Infection | 3 | 190 | Risk Ratio (M‐H, Random, 95% CI) | 1.37 [0.39, 4.81] |
| 3 Cosmetic appearance rated by patient (VAS) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 4 Cosmetic appearance rated by patient (% satisfied) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5 Cosmetic appearance rated by surgeon (VAS) | 2 | 139 | Mean Difference (IV, Random, 95% CI) | 9.56 [4.74, 14.37] |
| 6 Patient satisfaction | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 7 Surgeon satisfaction | 2 | 141 | Risk Ratio (M‐H, Random, 95% CI) | 0.87 [0.63, 1.19] |
| 8 Time taken for wound closure | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only |
Comparison 3. Adhesive versus staples.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dehiscence | 2 | 107 | Risk Ratio (M‐H, Random, 95% CI) | 0.53 [0.05, 5.33] |
| 2 Infection | 4 | 320 | Risk Ratio (M‐H, Random, 95% CI) | 1.39 [0.30, 6.54] |
| 3 Cosmetic appearance rated by patient (scar scale) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 4 Cosmetic appearance by plastic surgeons (VAS) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 5 Patient satisfaction | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 6 Time taken for wound closure | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only |
Comparison 4. Adhesive versus other method.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dehiscence | 2 | 249 | Risk Ratio (M‐H, Random, 95% CI) | 0.55 [0.13, 2.38] |
| 2 Infection | 2 | 249 | Risk Ratio (M‐H, Random, 95% CI) | 0.41 [0.11, 1.60] |
| 3 Patient satisfaction | 1 | 187 | Mean Difference (IV, Fixed, 95% CI) | 0.40 [0.10, 0.70] |
| 4 Clinician satisfaction | 1 | 209 | Mean Difference (IV, Fixed, 95% CI) | 0.53 [0.29, 0.77] |
| 5 Time taken for wound closure | 1 | 209 | Mean Difference (IV, Fixed, 95% CI) | ‐1.05 [‐1.79, ‐0.31] |
Comparison 5. Adhesive versus adhesive: High viscosity versus low viscosity.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dehiscence | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2 Infection | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3 Patient satisfaction | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 4 Clinician satisfaction | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 5 Time taken for wound closure | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only |
Comparison 6. Adhesive versus adhesive: octylcyanoacrylate versus butylcyanoacrylate.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Dehiscence | 2 | 80 | Risk Ratio (M‐H, Random, 95% CI) | 1.46 [0.19, 11.30] |
| 2 Infection | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3 Cosmetic assessment rated by patient (VAS) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 4 Cosmetic assessment rated by surgeon (VAS) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 5 Surgeon satisfaction (with device) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 6 Surgeon satisfaction (with closure) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 7 Time taken for wound closure | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Amin 2009.
| Methods | RCT with 3 months follow‐up. 72 participants randomised, but only 60 had 3‐month outcome data collected and reported | |
| Participants | 72 participants receiving minimally invasive thyroidectomy using either video‐assisted thyroidectomy or minimal incision thyroidectomy Surgery performed in 1 centre in Ireland. All cases were performed by the senior surgeon Exclusion criteria: autoimmune thyroiditis, diabetes mellitus and/or poor general health Trial conducted in Dublin, Ireland |
|
| Interventions | Group 1 (n = 38; results reported for 33): 2‐octylcyanoacrylate (Dermabond®) tissue adhesive (Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) Group 2 (n = 34; results reported for 27): staples |
|
| Outcomes | Cosmetic appearance by participant and by surgeon (at 3 months) using the Manchester scar scale Patient satisfaction (self assessed at 3 months): collected using a 10 cm VAS line where 0 was poor and 10 was excellent. Data for overall patient satisfaction score (n = 60) was calculated by the review authors using summary data presented in the study report. The patient satisfaction assessment form also measured: cosmesis; ability to shower same day (as operation); need to visit GP for wound; pain on removing clips; pain/tightness of wound; overall wound comfort and allergic reactions. Only ability to shower data was reported in addition to overall satisfaction score ‐ ability to shower data are not presented here |
|
| Notes | Cosmetic appearance outcome data not clearly presented for participants or surgeons. Authors contacted Study also reports pain at 1 and 10 days after surgery ‐ not reported here Cost of tissue adhesive reported as EUR22 ‐ no corresponding data for staples |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was performed prior to commencement of the study as follows: Opaque envelopes were numbered sequentially from 1 to 75. A table of random numbers was generated by a computer program and used for group assignment; if the last digit of the random number was from 0 to 4, the assignment was to Group A (tissue adhesive), and if the last digit was from 5 to 9, the assignment was to Group B (staples)." Comment: adequate method of random sequence generation |
| Allocation concealment (selection bias) | Low risk | Quote: "The assignments were then placed into the opaque envelopes and the envelopes sealed. As eligible participants were entered into the trial, these envelopes were opened in sequential order to give each patient his or her random group assignment. The envelopes were opened by the operating surgeon following patient consent and just prior to the surgical procedure." Comment: use of sealed, numbered opaque envelopes considered robust |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "Blinding was not feasible at the time of skin closure, nor was it of any benefit at the two‐week postoperative visit, as wound cosmesis at this stage is not considered predictive of the long‐term cosmetic outcome." Comment: understandably difficult to blind operating surgeon and participants to the intervention.Staff would have been aware of allocation on wound closure and during short‐term post‐operative assessment ‐ however none of these outcomes are reported here. Participants were not blinded. Unclear whether this would have led to bias in the study in terms of satisfaction in favour of 1 treatment |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Blinding was achieved during evaluation of the surgical wound at or after three months postoperatively as surgeons were unaware of the wound closure method used. A three‐month appointment was arranged for each participant for wound evaluation by a surgeon who was not involved in the patient management." Comment: blinded outcome assessment undertaken at 3 months for surgeon cosmetic outcome data although we were unable to extract these data for the review. Participant assessment not blinded (as noted above) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "Sixty out of the 72 patients agreed to come back for the three‐month postoperative evaluation. The remainder did not attend do to the long travelling [sic]/commuting distance to the tertiary service" Comment: data from only 60 of the 72 participants randomised were available at 3 months. Also possible differential attrition (adhesive 13%, staples 21%). Deemed to be at unclear risk of bias |
| Selective reporting (reporting bias) | High risk | Comment: multiple dimensions of patient satisfaction assessed with ability to shower selectively reported ‐ data not presented here. Study protocol not sought |
| Other bias | Low risk | None noted |
Avsar 2009.
| Methods | RCT with 40 participants with 40 days follow‐up | |
| Participants | 40 women undergoing the Pfannenstiel incision Exclusion criteria: known allergy to trial products Conducted in Turkey |
|
| Interventions | Group 1 (n = 20): high viscosity 2‐octylcyanoacrylate (High Viscocity Dermabond®; Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) tissue adhesive Group 2 (n = 20): polypropylene sutures All participants had skin cleansed with povidone iodine and 1 g antibiotic prophylaxis |
|
| Outcomes | Wound infection (at 2, 7 and 40 days after surgery: 7‐day data used for analyses, as these data were most clear from the translation) Time for skin closure Participant satisfaction at day 40. Participants were asked how satisfied they were with their skin closure they could select from the following responses: very bad, poor, average, good, very good |
|
| Notes | Data extraction based on English language abstract and partial translation of report text that was published in Turkish The study reports an outcome ‐ wound disruption ‐ as yet we have been unable to translate whether this can be interpreted as wound dehiscence Cometic appearance not used in this review as assessed at less than 3 months |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: unable to gauge from translation |
| Allocation concealment (selection bias) | Unclear risk | Comment: unable to gauge from translation |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: unable to gauge from translation |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: unable to gauge from translation |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: unable to gauge from translation. We acknowledge risk of selection bias from reporting infection outcome data from the time point where statistical significance was observed |
| Selective reporting (reporting bias) | Unclear risk | Comment: unable to gauge from translation |
| Other bias | Unclear risk | Comment: unable to gauge from translation |
Blondeel 2004.
| Methods | RCT with 1‐month follow‐up | |
| Participants | 217 adults requiring any skin incision closure 4 cm or greater in length. Multicentre study conducted at: Department of Plastic Surgery, University Hospital Gent, Gent, Belgium; Intitute Mutualiste Montsouris, Paris, France; Crestwood Hospital, Huntsville, AL, USA; Gynecologic Oncology Research and Development, LLC, Greenville, SC, USA; Naval Medical Centre, San Diego, CA, USA; University Dental Hospital, Manchester, UK Exclusion criteria: a history of peripheral vascular disease; insulin‐dependent diabetes; a blood‐clotting disorder or taking anticoagulants within 7 days of surgery; concurrent use of steroids; or a personal or family history of keloid formation or hypertrophy; impaired wound healing; or a known allergy to cyanoacrylate or formaldehyde |
|
| Interventions | Group 1 (n = 106): high viscosity 2‐octylcyanoacrylate (High Viscocity Dermabond®; Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) tissue adhesive Group 2 (n = 103): any other commercially available device such as sutures, staples, or tapes or compared with low viscosity 2‐octylcyanoacrylate (n = 42; Dermabond®, Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) |
|
| Outcomes | Wound dehiscence, infection, patient satisfaction and surgeon satisfaction at 10 days | |
| Notes | Cosmetic appearance data not used as measured at less than 3 months | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: " . . . patients at each study site were randomised by computer generated code in a 1:1 ratio to epidermal incision closure with high viscosity 2‐octylcyanoacrlate or a commercially available device" Comment: use of computer generated code constitutes low risk |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Sealed envelopes containing the concealed treatment allocations were opened in the operating room immediately before epidermal closure." Comment: judgement of unclear risk of bias made as not clear whether envelopes were sequentially numbered and opaque. Not clear who was responsible for allocation |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "Blinding to type of treatment was not feasible", due to the nature of the personnel‐led intervention Comment: understandably difficult to fully blind participants and personnel to intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "On day 10, wounds were assessed for adequate progress in healing, wound‐related infection, and indicators of an acute inflammatory reaction." Similarly, " . . . on day 10, physicians completed a questionnaire that measured satisfaction with each use of a device.", also, “a counterpart questionnaire [given to patients] for patient satisfaction for cosmesis, overall comfort, ability to shower, dressing changes, tension at the wound, hygienic problem, allergic reaction, and overall satisfaction" Comment: there is no mention that the wound was assessed by a blinded assessor. Such assessment would be difficult for satisfaction scores ‐ as noted above |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "The study was not completed by 4 patients assigned to high viscosity group 2 octylcyanoacrylate because of voluntary withdrawal (n=2), or loss to follow up (n=2) and by 6 patients to the control devices because of voluntary withdrawal (n=2), loss to the follow up (n=3), or death (n=1) [attributed to Burkitt's Lymphoma]". Comment: the numbers were fairly small and were fairly evenly distributed between the treatment arms. Therefore we do not believe this represented a significant risk of bias |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all the variables outlined in the methodology were accounted for in the results Comment: judged as low risk. Study protocol not sought |
| Other bias | Low risk | No other sources of bias were detected |
Brown 2009.
| Methods | Parallel RCT with 6 weeks follow‐up. No withdrawals reported | |
| Participants | 134 children undergoing inguinal herniorrhaphy (ages ranged from 1 month to 12 years) All operations performed by 1 of 4 paediatric surgeons No other inclusion or exclusion data reported Undertaken in 1 centre in the USA |
|
| Interventions | Group 1 (n = 64): 2‐octylcyanoacrylate (Dermabond®) tissue adhesive (Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) Group 2 (n = 70): sutures (5.0 Monocryl) Group numbers calculated from data in paper as not reported directly |
|
| Outcomes | Wound dehiscence (6 weeks) Time for skin closure Relative costs of materials required for skin closure |
|
| Notes | Surgeon cosmetic appearance data not used as measured at < 3 months | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Just before wound closure, a sealed envelope indicating randomization to skin adhesive or suture closure was revealed." Comment: no information about how the randomisation sequence was generated |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Just before wound closure, a sealed envelope indicating randomization to skin adhesive or suture closure was revealed." Comment: no information about whether envelopes were opaque and sequential and who prepared or opened these. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "Masking as to skin adhesive vs suture closure was not possible for the operating surgeon because of the nature of the intervention." Comment: understandably difficult to blind operating surgeon and participants to the intervention. Staff would have been aware of allocation on wound closure |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "However, subsequent interviewers were masked as to group during assessment of cosmetic outcome measures, as well as those related to efficiency, cost, and complications of wound closure." Comment: deemed at low risk of bias for debridement and costs outcomes |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No report of any loss to follow‐up Comment: judged as low risk |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all the variables outlined in the methodology were accounted for in the results Comment: judged as low risk. Study protocol not sought |
| Other bias | Low risk | No other sources of bias were detected |
Cheng 1997.
| Methods | RCT with 1‐month follow‐up | |
| Participants | 86 healthy male patients under the age of 12 years requiring elective circumcision. Study conducted at Duchess of Kent Hospital, Hong Kong. No specific exclusion criteria were described | |
| Interventions | Group 1 (n =40): butylcyanoacrylate (Histoacryl®) tissue adhesive Group 2 (n = 46): 4.0 catgut sutures |
|
| Outcomes | Dehiscence and infection at days 1, 2, 3, 7 and 30. Cosmetic appearance, bleeding and wound inflammation were also assessed at these time points. Bleeding and wound inflammation were not of interest to this review | |
| Notes | Cosmetic appearance data were not used as measured at < 3 months | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: " . . . [patients were] randomised into two groups" Comment: no method of random sequence generation was actively discussed; therefore the risk of bias for this domain is unclear |
| Allocation concealment (selection bias) | Unclear risk | Quote: Patients were " . . . randomised into two groups" as previously mentioned Comment: no method of allocation concealment was made clear. Therefore, the risk of bias is again unclear |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported whether the participants or personnel were blinded to the intervention Comment: as the participants were under the age of 12 and under general anaesthesia, it is reasonable to assume that they were blinded to the intervention. However, the personnel were probably not blinded as they carried out the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "The wounds of all the patients were then assessed on day 1, day 2 and day 3, 1 week and 1 month after the operation. Wound inflammation, infection, bleeding, cosmetic result and dehiscence were assessed. A questionnaire was completed" Comment: no mention of whether the assessors of the wound and the cosmetic results were blinded to the intervention. It is not clear if the questionnaire was filled out by parents of the children, who may have been blinded to the intervention, or the assessors, who were likely to know which intervention was given. The judgement for this domain is therefore unclear |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No direct quotations, but no losses to follow‐up were reported Comment: therefore judged as low risk |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but the results account for the all the assessment methods identified to qualify the success of the intervention Comment: no evidence of reporting bias, therefore judged as low risk |
| Other bias | Unclear risk | Possible unit of analysis issue for dehiscence outcome |
Chibbaro 2009.
| Methods | RCT with up to 12 months follow‐up, with assessment at 1, 3, 5‐7 and 14 days, then 1, 3, 6 and 12 months | |
| Participants | 40 participants undergoing elective cranial supratentorial surgery Exclusion criteria: undergoing a procedure for infective pathology; head trauma; admission to the intensive care unit; a dermatologic disease; previous cranial radiotherapy; diabetes mellitus; known blood‐clotting disorders; and allergy to cyanoacrylate products Undertaken in 1 centre in Italy |
|
| Interventions | Group 1 (n = 20): n‐butyl‐cyanoacrylate (Liquiband®; MedLogic Global Ltd, Plymouth, Devon, UK) tissue adhesive Group 2 (n = 20): sutures (Monosof 2/0, Tyco United States Surgical, Norwalk, CT, USA) or staples (Auto Suture Appose ULC 35, Tyco United States Surgical) All participants received the same antibiotic prophylaxis (1 dose of 3rd‐generation cephalosporin 20 min prior to surgical incision) Wound dressings were not used for those allocated to tissue adhesive because this formed its own waterproof and antimicrobial wound dressing Participants in the tissue adhesive group (Group 1) were permitted to shower from the day after the surgical procedure, while those participants allocated to sutures were instructed to keep their wounds clean and dry until the removal of the sutures |
|
| Outcomes | Wound dehiscence (collected to 7th day postoperatively) Wound infection (collected to 7th day postoperatively; infection not defined) Cosmetic appearance (nurse‐blinded) using modified Hollander Wound Score scale (up to 12 months) Skin closure time |
|
| Notes | Cosmetic appearance (patient and surgeon) using a VAS of 1 to 10 where a score of 10 reflected optimal cosmetic outcome. It is not clear at what time points these data were collected. Authors were contacted Supplmentary material referenced in the main paper also checked |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote:"At the moment of skin closure, they [the patients] were randomly allocated into one of two groups (A or B) of 20 patients each." Comment: no reporting on how the patients were randomly allocated or the method used |
| Allocation concealment (selection bias) | Unclear risk | Quote: "The randomization sequence was arranged on the same day as surgery; each patient’s name was randomly assigned to one of 40 envelopes (20 marked as LiquiBand, 10 as TTS and 10 as SC)." Comment: no indication that the allocation was concealed |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No direct quotations. Did not report that the participants or personnel were blinded to the intervention Comment: understandably difficult to blind the operating surgeon to the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "All of the patients were followed up post‐operatively on days 1, 3, 5‐7 by the same ward nurse who initially recorded details regarding their wound aspects" "After discharge, a second nurse (not from the neurosurgical department), using the same scale, continued the follow‐up, initially at 2 weeks, and then at 1, 3, 6 and 12 months post‐operatively”. Noted in abstract that this second nurse was blinded Comment: although the study intimates that the nurse was not from the department and the second nurse was blinded it is not clear that the first nurse was blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "Only 39 patients (19 in group A and 20 in group B) were available at the 12 month follow up, as one patient in group A developed a post‐operative intracranial haematoma. This required an emergency evacuation procedure and the wound was subsequently closed with stitched" Comment: given that 39/40 participants had 12‐month data available, we made an overall judgment of low risk of attrition bias |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all the variables outlined in the methodology were accounted for in the results Comment: judged as low risk. Study protocol not sought |
| Other bias | Low risk | No other sources of bias detected |
Dowson 2006.
| Methods | Parallel group RCT with 3‐month follow‐up | |
| Participants | 168 patients recruited for laparoscopic procedures at Queen's Medical Centre, Nottingham. 154 participants included in the final analysis. Withdrawals were accounted for. Exclusion criteria included insulin dependant diabetes, prolonged corticosteroid use; known keloid scarring; wounds greater than 5cm in length without deep layer sutures; those undergoing emergency surgery; patients unable to give informed consent. | |
| Interventions | Group 1 (n = 76): n‐butyl‐cyanoacrylate (Liquiband®; MedLogic Global Ltd, Plymouth, Devon, UK) tissue adhesive Group 2 (n = 78): interrupted, non‐absorbable suture |
|
| Outcomes | Time to closure, dehiscence, satisfaction, cosmesis and infection (we used 24 to 48 h figures to avoid unit of analysis issues for dehiscence and infection) | |
| Notes | Unclear reference to subcutaneous layers being dealt with. Authors contacted for mean and standard deviations of time to closure and cosmesis, but as we received no reply, this information was not included | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Randomisation was performed using consecutively numbered, sealed envelopes by a person not involved with the study" Comment: although allocation was concealed, there was no specific mention of how the sequence was randomly generated |
| Allocation concealment (selection bias) | Low risk | Quote: "Randomisation was performed using consecutively numbered, sealed envelopes by a person not involved with the study" Comment: allocation was concealed adequately |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "Participants in the trial were not informed of the wound closure method they had been allocated to until they had undergone surgery. The investigators were not blinded" Comment: the risk of performance bias was unclear as it was not possible to blind the investigators to the procedure they were carrying out |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "Patients were followed up at 24 to 48 hours, 4 to 6 weeks and 3 months postoperatively by C.C.D, A.D.G., or W.J.S. At these times it was documented if wounds showed any of the following characteristics; erythema, oedema, tenderness, inflammation, drainage/discharge and/or malodorous smell." Concurrently, at the 3 month cosmetic evaluation, "a blinded assessment by a qualified nurse or surgical registrar not involved in the study also being made at 3 months" Comment: adequate blinding of assessment at 3 months. Potential for high risk of detection bias for outcomes reported prior to this |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Flow chart suggests no loss to follow‐up in first 48 h postoperatively. At 4‐6 weeks 20 participants were lost to follow‐up in the suture arm and 15 in the adhesive arm. There was further loss to follow‐up at 3 months: the suture arm suffered a total loss of 14 (with 7 missing both the 4‐6 week and the 3‐month follow‐up), while the adhesive group had 8 missing the 3‐month follow‐up (with 6 missing both follow‐ups) Comment: relative high attrition of data from study for outcomes collected at later time points |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all the variables outlined in the methodology were accounted for in the results Comment: judged as low risk. Study protocol not sought |
| Other bias | Low risk | No other sources of bias identified |
Eggers 2011.
| Methods | 4‐arm parallel RCT with 90 participants with 6 weeks of follow‐up (assessment at 24 h, 3 and 6 weeks). Only data on 75 of participants were reported | |
| Participants | Participants undergoing total knee arthroplasty Exclusion criteria: medical conditions or personal circumstances that would prevent participation and completion of physical therapy and follow‐up visits; current participation in another clinical trial; preoperative systemic infections; uncontrolled diabetes; diseases or conditions known to effect the wound healing process; known hypersensitivity to cyanoacrylate, formaldehyde, or the dye D&C Violet #2 (Aesculap, Inc, Center Valley, PA); prior knee hardware fixation devices; prior knee incisions greater than 9 cm, and arthrofibrosis as evidence by limited ROM of 80° or higher Study performed in 1 centre in the USA |
|
| Interventions | Group 1 (n = 19): subcutaneous closure method: sutures at 1.5/cm; skin closure method: 2‐octylcyanoacrylate (Dermabond®) tissue adhesive (Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) Group 2 (n = 18): subcutaneous closure method: sutures at 1.5/cm; skin closure method: butylcyanoacrylate tissue adhesive (Histoacryl Blue tissue adhesive B Braun Corp) Group 3 (n = 19): subcutaneous closure method: sutures at 1.0/cm; skin closure method: staples (Visistat 35W Stapler (Teleflex Corp) Group 4 (n = 19): subcutaneous closure method: sutures at 1.0/cm; skin closure method: Monocryl suture (poliglecaprone 25; Ethicon) Data on 15 participants were excluded from analysis data: it was not reported which trial groups these participants were from. We note there were slight difference to the procedures in each group for the method of closure of the sub‐cutaneous layer. Details for (1) sub‐cutaneous closure methods and (2) skin closure method are provided above. |
|
| Outcomes | Wound dehiscence (24 h, 3 weeks, and 6 weeks postoperatively) Wound infection (24 h, 3 weeks, and 6 weeks postoperatively; infection not defined. We have taken the total number of infections reported over the 6‐week period, however, it is not clear whether some participants reported more than 1 infection as the number of infections was reported rather than number of people having an infection Relative costs of materials required for skin closure Skin closure time |
|
| Notes | Surgeon cosmetic appearance data not used as measured at < 3 months | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: " . . . the eligible subjects were randomly categorized (via a pseudo‐random number generator algorithm) into 1 of 4 cohorts" Comment: adequate random sequence generation |
| Allocation concealment (selection bias) | Unclear risk | Quote: " . . . the eligible subjects were randomly categorized (via a pseudo‐random number generator algorithm) into 1 of 4 cohorts". The study also states, "The surgeon was blinded to the closure technique before and during the operation until subcutaneous closure" Comment: although sequence generation was adequate and there is evidence to suggest that allocation was concealed, there is not enough evidence to suggest how this was done and how allocation was concealed to the personnel |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "The surgeon was blinded to the closure technique and during the operation until subcutaneous closure" Comment: although attempts were made to conceal the allocated treatment, it would be difficult to blind the operating surgeon to the intended intervention, therefore our judgement is unclear. No information was provided about the extent to which participants were blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "At each visit, a physical examination was conducted; and adverse events were recorded. The physical examinations after TKA included evaluation of peripheral edema, infection, and dehiscence as well as pain level (0‐10 scale) and cosmesis (100‐mm visual analogue scale (VAS)) evaluation by patient. General health and wellness were further evaluated by an SF‐12v2 survey" Comment: the extent to which the participants were blinded to the intervention is unclear; it is also unclear whether those conducting the examinations were aware of the treatment given. The outcome of cosmesis was evaluated before the our specified time‐frame for the purposes of our review. The judgement remains unclear in this case |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote:"Of the 90 subjects recruited, 15 were excluded because of screen failure; 6 were diagnosed with arthrofibrosis after surgery, 4 failed to follow preferred physical therapy, and 5 sustained unrelated co‐morbidities preventing study completion." "Consequently, a total of 75 subjects, 19 per cohort with the exception of 18 for the n‐butyl‐2 adhesive cohort, completed the study; and their data are presented in the following section." Comment: it seems that these participants were excluded post‐randomisation |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all the variables outlined in the methodology were accounted for in the results Comment: judged as low risk. Study protocol not sought |
| Other bias | Unclear risk | Possible issues with clustering for infection outcome data |
Greene 1999.
| Methods | Randomised split‐body design study with 1‐month follow‐up. No participants lost to follow‐up | |
| Participants | 20 adults requiring bilateral blepharoplasty for functional or aesthetic indications (40 eyelids were treated). Procedure conducted at: Division of Otolaryngology ‐ Head and Neck Surgery, Plastic and Reconstructive Surgery, Standford University Medical Centre and Palo Alto Veterans Healthcare System, Palo Alto, California, and Department of Otolayngology ‐ Head and Neck Surgery, Cleveland Clinic Florida, Naples, USA. Used a blepharoplasty model with identical skin sites on the same participant and each participant acted as his or her own control. No specific exclusion criteria were described | |
| Interventions | Group 1 (n = 20): left or right upper eye lid incision closed with 2‐octylcyanoacrylate (Dermabond®, Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) Group 2 (n = 20): other eyelid incision closed with 6.0 suture (10 fast‐absorbing gut or 10 polypropylene, Prolene, Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) Blepharoplasties were closed on the tissue adhesive side by using Castroviejo forceps to approximate the skin edges in 15 participants and by using 3‐4 sutures as handles to facilitate apposition and eversion of edges in 5 participants |
|
| Outcomes | Dehiscence, infection, patient satisfaction, and surgeon satisfaction at 1, 2, and 4 weeks. Time for closure at end of procedure | |
| Notes | Cosmetic appearance data could not be used as measured at < 3 months | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Each patient had been randomised to have either the right or left upper eyelid serve as the experimental closure [with adhesive] . . . and the opposite eyelid as the control with sutures" Comment: despite stating that each patient was randomised to treatment group, there was no specific description of how the randomisation process was done or achieved |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Each patient had been randomised . . . " Comment: no description of how allocation was undertaken and whether it was concealed |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported whether participants or personnel were blinded to the intervention Comment: understandably difficult to blind surgeon to the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "The photographs were shown to 5 observers blinded to the technique of closure" to evaluate wound quality post operatively." Comment: blinding of outcome assessment achieved for cosmetic appearance, which was not included in this review. Not clear whether blinded assessment was undertaken for other outcomes |
| Incomplete outcome data (attrition bias) All outcomes | Low risk |
Quote: "The 5 blinded observers using the visual analogue scale to rate the 40 treated eyelids did not find any statistically significant difference between the wound quality . . ." Comment: suggested that all participants were accounted for, as the study had 20 participants (40 eyelids). |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all the variables outlined in the methodology were accounted for in the results Comment: judged as low risk. Study protocol not sought |
| Other bias | Low risk | No other sources of bias detected |
Jallali 2004.
| Methods | RCT in which participants (with multiple port wounds) were randomised. Follow‐up was for between 6 and 8 weeks. No withdrawals reported | |
| Participants | Participants undergoing laparoscopic cholecystectomy No other inclusion or exclusion information Undertaken in 1 UK centre |
|
| Interventions | Group 1 (12 participants; 48 wounds): 2‐octylcyanoacrylate Group 2 (13 participants; 51 wounds): absorbable sutures Participants in the suture arms had a dressing placed over the wound. Those in the tissue adhesive arm did not require a dressing |
|
| Outcomes | Skin closure time (not clear if these data were collected for multiple wounds on the same person) | |
| Notes | Outcome reporting was unclear, so not sure if results were reported for a reference wound for each participant or if outcome data from multiple wounds were collected Cosmetic appearance data could not be used in the review as measured at < 3 months Wound complications reported as an outcome ‐ but nature of the complications was not clear |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Randomization was performed by asking the patient to select an envelope out of a hat" Comment: although it seems efforts were in place to randomise patients, it is not wholly clear that a truly randomised sequence was generated |
| Allocation concealment (selection bias) | Unclear risk | Quote:"Randomization was performed by asking the patient to select an envelope out of a hat" Comment: there was no mention of whether allocation was concealed to the investigators |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No direct quotations about whether the participants or personnel were blinded in this study. It would be difficult to blind personnel in a surgical procedure |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No direct quotations about whether the participants or personnel were blinded in this study. It would be difficult to blind personnel in a surgical procedure. The only outcome reported here relevant to the review was time to skin closure. It is not clear if this was assessed by a blinded assessor |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "All patients were followed up. In the suture group one patient refused to have a photograph taken" Comment: adequate outcome data gathered |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all the variables outlined in the methodology were accounted for in the results Comment: judged as low risk. Study protocol not sought |
| Other bias | Unclear risk | Based on information collected it is not clear whether data were presented for an incorrectly analysed cluster trial |
Keng 1989.
| Methods | RCT with 7‐month follow‐up. 3 participants lost to follow‐up: 1 from the suture group and 2 from the tissue adhesive group | |
| Participants | 43 people requiring groin incisions (for: inguinal hernia, femoral hernia, sapheno ligations, testicular operations and lymph node biopsies). Skin incisions were closed with either butylcyanoacrylate (Histoacryl) tissue adhesive or Dexon subcuticular suture. In bilateral operations the left side was closed with Histoacryl and the left with Dexon. Conducted at Burton General Hospital, Burton‐on‐Trent, UK | |
| Interventions | Group 1: butylcyanoacrylate (Histoacryl) tissue adhesive Group 2: Dexon suture on straight needle using anchoring knot both ends or opposing the wound with forceps |
|
| Outcomes | Infection, inflammation, cosmetic appearance, wound closing time, wound comfort and haematoma | |
| Notes | Exclusion criteria were not stated. Cosmetic appearance data not used in the review, as measured at < 3 months | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote:"The patients were randomised just prior to skin closure into two groups. Even numbers were closed with Dexon subcuticular suture (Dexon group) and odd numbers were closed with Histoacryl‐Blue tissue adhesive (Histoacryl)" Comment: whilst use of odd and even numbers is detailed in terms of how the randomisation was implemented there was no detail about how the sequence was generated |
| Allocation concealment (selection bias) | Unclear risk | Quote:"Even numbers were closed with Dexon subcuticular suture (Dexon group) and odd numbers were closed with Histoacryl‐Blue tissue adhesive (Histoacryl)" Comment: no indication mention that this sequence was concealed from surgeons. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No direct quotation. Not reported whether participants or personnel were blinded to the intervention. It is possible that participants may have been aware of 2 different methods of closure. "When the patients had bilateral operations, the left side was closed with Histoacryl and the right side with Dexon". Comment: understandably difficult to blind operating surgeon to intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk |
Quote: "Cosmesis was assessed by an independent observer (the experienced clinic sister) on a scale of one to five . . . " "The patients and wounds were assessed at one week and one month postoperatively in the surgical outpatients clinic. A simple scheme was used to assess the wound . . ." Comment: blinding of outcome assessment achieved for wound appearance, but this was not used in this review. Blinding not clear with regard to the other outcomes |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: 3/43 participants were lost to follow‐up. Considered low risk of bias |
| Selective reporting (reporting bias) | Low risk | All the variables outlined in the methodology were accounted for in the results Comment: judged as low risk. Study protocol not sought |
| Other bias | Low risk | No other sources of bias detected |
Kent 2014.
| Methods | Parallel RCT in 433 participants with 3 months follow‐up | |
| Participants | 433 participants undergoing a range of laparoscopic procedures Exclusion criteria: known sensitivity to cyanoacrylates; pregnancy or breastfeeding; or conditions known to interfere with wound healing (no further information provided) 4 UK centres |
|
| Interventions | Group 1 (216 participants; 636 treated wounds): high viscosity 2‐octylcyanoacrylate (High Viscocity Dermabond®; Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) tissue adhesive Group 2 (217 participants; 618 treated wounds): n‐butyl‐cyanoacrylate (Liquiband®) tissue adhesive (LiquiBand. MedLogic Global Ltd, Plymouth, Devon, UK) |
|
| Outcomes | Wound dehiscence (evaluated at 14 days and 3 months postoperatively) Wound infection (evaluated at 14 days and 3 months postoperatively; infection not defined) Cosmetic appearance by surgeon (at 3 months) using a modified Hollander Wound Evaluation scale Participants' satisfaction with incisional wound closure ‐ options were 'satisfied' or 'dissatisfied' Sugeons' satisfaction with wound (considering expression, application, delivery and ease of use for product): options were 'satisfied' or 'dissatisfied' Skin closure time |
|
| Notes | Unit of randomisation was person with some data reported per wound (with multiple port incisions on each participant) Cosmetic appearance by participants and surgeon (at 3 months). Participants and surgeons were asked to assess whether they were 'satisfied' or 'dissatisfied' with the overall appearance of the wound. Whilst this was referred to as satisfaction in the study we deemed it to be an unvalidated measure of cosmetic appearance |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Subjects were randomised into 1 of 2 treatment groups: LB or DB. Although the adhesive user was not masked, both the study subject and evaluators were blinded to the randomised study treatment assignment" Comment. it is unclear how the randomisation sequence was achieved. Judged as unclear |
| Allocation concealment (selection bias) | Unclear risk | Quote:"Subjects were randomised into 1 of 2 treatment groups: LB or DB. Although the adhesive user was not masked, both the study subject and evaluators were blinded to the randomised study treatment assignment" Comment: no method of allocation concealment described, therefore judged as unclear |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "The adhesive user was not masked, both the study subject and evaluators were blinded to the randomised study treatment assignment" Comment: this indicates that personnel were not blinded to the procedure, whilst participants were blinded. Given that this was a study investigating two adhesives, blinding might have been possible. The judgement is unclear |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "Wound cosmesis was evaluated by a masked panel at the 3‐month visit. Cosmesis was measured using a modified 6‐point Hollander Wound Evaluation Scale (HWES) score." Comment: adequate blinding of outcome assessment Quote: Satisfaction measures were obtained from different study participants throughout the course of this trial. First, the surgical user was asked to indicate his/her satisfaction with the expression, application, delivery as ease of use of products. The user marked on a sheet that he/she was either "satisfied" or "dissatisfied". At the 3‐month follow up visit, the masked evaluators were requested to state whether they were satisfied with the healing and the overall appearance of the incisions" Comment: satisfaction outcome blinded adequately Not clear if wound dehiscence and infection were blinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Quote:"A total of 76 subjects withdrew from the study, primarily because they were lost to follow up, resulting in a loss to follow up rate of 17.6%. Final data analysis was performed on 373 subjects and a total of 1089 incisions" Comment: high number of missing data at the participant level |
| Selective reporting (reporting bias) | Low risk | All the variables outlined in the methodology were accounted for in the results Comment: judged as low risk. Study protocol not sought |
| Other bias | Unclear risk | Data presented and analysed as an individual trial, but this is a cluster trial (wounds clustered per person) |
Khan 2006.
| Methods | 3‐arm parallel trial with 187 participants. No withdrawals reported Follow‐up was classed as 'early', which seems to have been the first 3 days after surgery, and then 'late' which was between 8 and 12 weeks after surgery |
|
| Participants | 187 participants undergoing either a total knee arthroplasty or a total hip arthroplasty Exclusion criteria: having a revision or with a previous incision in the operative field; a history of keloid formation; allergy to superglue; regular anticoagulation therapy; or an underlying malignancy The study was performed in 1 centre in Australia |
|
| Interventions | Group 1 (n = 60): 2‐octylcyanoacrylate (Dermabond®) tissue adhesive (Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) Group 2 (n = 64): continuous 3.0 subarticular absorbable poliglecaprone suture (Monocryl, Johnson and Johnson) Group 3 (n = 63): skin staples |
|
| Outcomes | Wound infection: (report states that"where cultures were positive or there was clinical evidence of cellulitis, the patients were treated with a course of antibiotics and recorded as having an ‘infection") data collected at 2 time points ‐ early and late Patient satisfaction with the techniques of skin closure was assessed with a VAS between 0 and 100, where 100 represented maximal satisfaction Skin closure time |
|
| Notes | Cosmetic appearance data (surgeon) could not be used in this review as measured at < 3 months | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The patients were randomised using a computer‐generated method . . . " Comment: Adequate random sequence generation method utilised |
| Allocation concealment (selection bias) | Unclear risk | Quote: "The patients were randomised using a computer‐generated method stored in sealed identical opaque envelopes. Allocation took place in the operating theatre after closure of the deep layers. Enrolment, generation of the allocation sequence and assignment of the patients was performed by the lead author." Comment: not clear if envelopes were numbered or otherwise labelled or stored so that allocation was concealed |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "The patients and assessors remained blinded to the treatment allocated until the dressings were changed, prior to discharge. At follow‐up, the assessors were not informed of the technique of closure." Comment: no mention of whether the personnel were blinded to the procedure, although this would be understandably difficult for a surgical procedure |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "The patients and assessors remained blinded to the treatment allocated until the dressings were changed, prior to discharge. At follow‐up, the assessors were not informed of the technique of closure." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No direct quotation, but no account of a loss to follow‐up, therefore judged as low risk |
| Selective reporting (reporting bias) | Low risk | No direct quotation, but no outcomes selectively reported, therefore judged as adequate |
| Other bias | Unclear risk | Possible issues with clustering for infection outcome data |
Kouba 2011.
| Methods | Split‐body design RCT with 12 weeks of follow‐up. Data missing for 1 participant | |
| Participants | Adults undergoing upper lid blepharoplasty who had not previously undergone this procedure Participants were recruited from a singe site, Henry Ford Health System, USA 1 cosmetic surgeon performed whole procedure Exclusion criteria: taking salicylates and/or anticoagulants; taking oral retinoids in the last 3 months; an unexplained history of excessive bleeding; a history of acute glaucoma or Sjogren’s syndrome; having resurfacing or laser techniques for the eyelid |
|
| Interventions | Group 1 (24 participants; 24 eyes): 2‐octylcyanoacrylate (Dermabond®) tissue adhesive (Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) Group 2 (24 participants; 24 eyes): standard monofilament suture (6‐0 fast‐absorbing gut or polypropylene) The study authors randomised each participant to have either (1) one eye treated with adhesive and the other with gut sutures; or (2) one eye treated with adhesive and the other with polypropylene sutures; or (3) one eye treated with gut sutures and the other treated with polypropylene sutures. For this review the adhesive data and the suture data from the two separate 'sub‐studies' involving adhesives have been pooled together and treated as one study |
|
| Outcomes | Wound dehiscence: assessed at 1 week Cosmetic appearance (surgeon‐rated): assessed at 1 month and 3 months (we report 3‐month data). Scoring performed using a scale of 1 (excellent wound healing, scar matches surrounding skin) to 5 (poor scar wound healing, does not match surrounding skin). This was a blinded assessment. The data presented here were calculated by the review authors from raw data presented in the study report |
|
| Notes | The following outcome was reported, but was not thought to be a validated measure for cosmetic appearance, "Participant cosmetic evaluation: (thickness, width, texture, color change, overall cosmetic outcome) was assessed at 3 months. A composite score was calculated as the sum of the scores for thickness, width, texture, and color change." No clear information was reported on wound dehiscence No comparative baseline data reported Funding source not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote:"They [the patients] were randomised for treatment in three subgroups in which each eyelid was repaired with a different material" Comment: no indication that there was randomised sequence generation |
| Allocation concealment (selection bias) | Unclear risk | Quote: "They [the patients] were randomised for treatment in three subgroups in which each eyelid was repaired with a different material" Comment: no indication allocation was concealed to the personnel |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No direct quotation, but no indication that there was blinding of the participant or the personnel during the procedure. However, there are obvious difficulties in blinding the operating surgeon to the procedure |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "Incidence of wound dehiscence and side effects of itching, bleeding, and pain were assessed at 1 week" Comment: no indication that this wound evaluation was undertaken by a blinded assessor Quote. [At 3 months] "A blinded physician assessed cosmetic outcome of wound closure technique using standardized photographs" Comment: adequate blinding of this outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No direct information regarding drop out rates, however different numbers used in total participants at 1 month to those at 3 months. Therefore the judgement is unclear |
| Selective reporting (reporting bias) | High risk | Quote: "Incidence of wound dehiscence and side effects of itching, bleeding, and pain were assessed at 1 week" Comment: incidence of wound dehiscence not clearly reported in the results |
| Other bias | Low risk | None reported |
Krishnamoorthy 2009.
| Methods | A parallel RCT with follow‐up at 7 days and 6 weeks postoperatively. No missing data reported, but the number included in analysis was not clear | |
| Participants | 106 participants undergoing saphenous vein harvesting (for coronary artery bypass grafting). Participants were recruited from a single UK site Excluded patients with high risk of vein harvest failure (defined as those with varicose veins, those with small or thin legs and those who required emergency or repeat procedures) |
|
| Interventions | Group 1 (n = 53): 2‐octylcyanoacrylate (Dermabond®) tissue adhesive (Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) Group 2 (n = 53): sutures (monofilament synthetic absorbable Biosyn 3–0; Covidien PLC, Dublin, Ireland) In the suture group the wound was dressed with Mepore dressing (Mölnlycke Health Care, Manchester, United Kingdom),and a pressure bandage was applied for 48 h In the adhesive group a pressure bandage and Steri‐Strips (3M, St Paul,MN) were applied to hold the edges together for 24 h |
|
| Outcomes | Skin closure time | |
| Notes | Cosmetic appearance (surgeon‐reported) data not used in this review as measured at < 3 months An outcome that study authors referred to as a 'patient satisfaction score' was also measured, however, this seemed to focus on satisfaction of cosmetic appearance so was deemed a cosmetic evaluation; as it was collected at 6 weeks after surgery it is not reported here |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "A computerized randomization system was used to place patients into two groups of 53 each." Comment: judged as adequate evidence of sequence randomisation |
| Allocation concealment (selection bias) | Unclear risk | Quote: "A computerized randomization system was used to place patients into two groups of 53 each." Comment: no indication that allocation was concealed from personnel |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No direct quotation or indication that either participants or personnel were blinded from the study. However it is understandably difficult for personnel to be blinded in this case as it is a surgical procedure |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote:"Two surgeons independent of the study who were blinded to the type of skin closure rated photographs at the same time points using a visual analogue scale evaluating cosmetic appearance and the previously validated Hollander wound evaluation scale." Comment: although this would correlate to a perceived low risk of bias, the cosmesis outcome should be excluded at less than 3 months as per the systematic review protocol. No direct quotation available regarding blinding related to the time to skin closure study outcome |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote "We identified and excluded as additional 12 patients . . . " Comment: this quote is presented in the results. It is not clear if these were post‐randomisation exclusions |
| Selective reporting (reporting bias) | Low risk | All the variables outlined in the methodology were accounted for in the results Comment: judged as low risk. Study protocol not sought |
| Other bias | Low risk | None detected |
Livesey 2009.
| Methods | RCT with a 3‐month follow‐up period. In total 13 participants did not contribute data at 3 months | |
| Participants | 90 people having a total hip replacement Exclusion criteria: revision total hip replacement; a previous incision in the operative field, local skin conditions such as psoriasis, eczema or dermatitis; history of keloid formation; underlying malignancy; peripheral vascular disease; insulin‐dependant diabetes; allergy to skin adhesive or metal staples Undertaken in 1 UK centre |
|
| Interventions | Group 1 (n = 45): butylcyanoacrylate (LiquiBand®. MedLogic Global Ltd, Plymouth, Devon, UK) Group 2 (n = 45): staples (appose UCL 35W, Tyco, Norfolk, Connecticut) Data at 3 months only available for 38 in Group 1 and 39 in Group 2 thanks to missing data |
|
| Outcomes | Wound infection: defined as participant requiring antibiotics specifically for suspected wound infection Cosmetic appearance (participant‐rated) at 3 months: used a 100 mm VAS where 0 = worst outcome and 100 = best outcome. Median rather than mean data presented for this outcome Cosemtic appearance (surgeon‐rated) at 3 months: used a 100 mm VAS where 0 = worst outcome and 100 = best outcome |
|
| Notes | Data on participant satisfaction with scar and appearance of the wound in relation to expected appearance were also collected using a VAS scale (as above). Reviewers considered this to be a variation of cosmetic appearance and so it is not reported in the review Surgeons also reported cosmetic appearance using modified version of the Hollander wound evaluation score and modified Vancover scar score. The modified versions were deemed to be not validated (they only included 3 items) Time to wound closure data and ease of wound closure were collected on a sub‐set of 10 participants in each trial arm. There was no information about how these sub‐sets were selected, so these data could not be considered as data from an RCT per se and have not been presented here Follow‐up appointments took place a mean of 14.4 weeks after surgery (no evidence of significant difference between groups) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote:"Randomisation was performed, using the sealed envelope method, which involved identical sealed envelopes containing a card stating either 'skin adhesive' or 'staple' being opened by an independent researcher on the day of surgery" Comment: no indication that adequate randomised sequence generation was performed |
| Allocation concealment (selection bias) | Low risk | Quote: "Randomisation was performed, using the sealed envelope method, which involved identical sealed envelopes containing a card stating either 'skin adhesive' or 'staple' being opened by an independent researcher on the day of surgery. The operating surgeon was blinded to the skin closure method until the patient was in theatre" Comment: although it was not indicated that the envelopes were numbered sequentially, there is reasonable evidence here to describe the allocation concealment as adequate, and as it was undertaken by an independent researcher it has been judged accordingly |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "All patients had the same post‐operative care pathways and were blinded to the method of skin closure until the dressings were changed post‐operatively" Comment: adequate blinding of participants, however study design unable to blind personnel effectively, as a surgical intervention required |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "A researcher collected information on the presence of oozing and wound infection, which was defined as the patient requiring antibiotics specifically for suspected wound infection. Patients whose wound was closed with staples had these removed between ten and 14 days post‐operatively" Comment: indication that those evaluating the wounds were not blinded to the procedure, however this is not explicit, therefore the judgment remains unclear Quote: "An orthopaedic surgeon (AWB) also evaluated the scars using the VAS for cosmetic appearance. Both the plastic and orthopaedic surgeon were blinded to which method of skin closure had been used to each patient, and to each others' scores" Comment: adequate blinding of cosmesis outcome |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "In all, 12 patients (of 90) were lost to follow‐up because of non‐attendance or cancellation of the three‐month outpatient appointment. These patients have been seen subsequently with no reported adverse occurrences, but were not included in the final analysis as the time point for the last follow‐up in the study was three months" Comment: impact of these missing data unclear |
| Selective reporting (reporting bias) | High risk | Quote: "Evaluation of the cosmetic appearance of the scars was completed by a plastic surgeon (CME) using a modified version of the Hollander wound evaluation score and the Vancouver scar score, a Likert Scale and a VAS". . Comment: The results section reports only the Vancouver scar score, the Likert Scale and the VAS . The Hollander wound evaluation score has been omitted the judgement here is of high risk of bias. |
| Other bias | Low risk | None reported |
Maartense 2002.
| Methods | Randomised parallel group study with 16‐month follow‐up. There were no withdrawals, however 7 patients treated with paper tape and 3 with tissue adhesive were converted to the suture group | |
| Participants | 140 adults requiring elective laparoscopic surgery. Patients were excluded if they had undergone previous laparotomy or were pregnant. The study was undertaken at 2 centres, Department of Surgery, Academic Medical Centre, Amsterdam; and The Netherlands and Department of Surgery, Isala Clinics, Zwolle, the Netherlands | |
| Interventions | Group 1 (n = 48): octylcyanoacrylate (Dermabond®, Johnson & Johnson, Amersfoot, the Netherlands) tissue adhesive Group 2 (n = 42): 76 mm x 6 mm adhesive paper tape (SteriStrip® Bioplasty/Uroplasty, Geleen, the Netherlands) Group 3 (n = 50): intracutaneous poliglecaprone (Monocryl®) 4/0, Johnson & Johnson) interrupted sutures |
|
| Outcomes | Infection, cosmetic appearance, and surgeon satisfaction at 2 weeks and 3 months, and costs. | |
| Notes | We wrote to the authors who confirmed that there were no withdrawals | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Patients were allocated to one of the three groups using a computer randomization" Comment: random sequence generation undertaken by computer |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Patients were allocated to one of the three groups using a computer randomization" Comment: not reported whether this allocation was concealed from the operating surgeon |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported whether participants or personnel were blinded to the intervention Comment: understandably difficult to blind the operating surgeon to the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "At follow up [at 10‐14 days and 3 months], the incidence of wound infection and cosmesis were scored. Patients were also asked to score their own cosmetic results. Surgical residents scored wound infection and cosmetic results, they were blinded to the method used for wound closure" Comment: this infers a low risk of detection bias at both intervals for outcomes assessed by surgeons |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No direct relevant quotations, although some patients who underwent closure with adhesive tape or adhesive liquid had to be converted intra‐operatively to suture closure. These seem to be analysed in the groups to which they were randomised (intention‐to‐treat analysis) Comment: judgement of low risk of attrition bias |
| Selective reporting (reporting bias) | Low risk | No direct relevant quotations, but all variables listed in the methods section are listed in the tables in the Results section Comment: a low risk of reporting bias is inferred |
| Other bias | Low risk | No other sources of bias were detected |
Maloney 2013.
| Methods | Parallel RCT in 43 participants. Follow‐up was for 3 months (assessment at 2 weeks and 3 months after surgery). No withdrawals noted | |
| Participants | 43 participants undergoing a skin incision to remove skin cancer Exclusion criteria: known sensitivity to cyanoacrylates; wounds under high tension forces; wounds < 2 cm or > 5 cm in length; or participant pregnant or breastfeeding Study undertaken in USA, number of centres involved was unclear |
|
| Interventions | Group 1 (n = 23): high viscosity 2‐octylcyanoacrylate (High Viscocity Dermabond®; Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) tissue adhesive Group 2 (n = 20): n‐butyl‐cyanoacrylate (Liquiband®) tissue adhesive (LiquiBand. MedLogic Global Ltd, Plymouth, Devon, UK) |
|
| Outcomes | Wound dehiscence (2 weeks and 3 months after surgery ‐ no events reported at 3 months and 1 event only at 2 weeks, no unit of analysis issue) Wound infection (not defined) Cosmetic appearance at 3 months (blinded evaluators ‐ panel of 6 doctors) using 100 mm VAS scale where 0 = worst scar and 10 = best scar Cosmetic appearance at 3 months (participant‐reported) using VAS scale on worst scar (0) to best scar (10) Surgeon satisfaction (at time of wound closure) assessed using 100 mm VAS scales for: ease of use (0 = impossible; 10 = very easy to use) and satisfaction with device and the closure achieved (0 = completely dissatisfied; 10 = completely satisfied) |
|
| Notes | Wound infection listed as outcome, but not clearly reported Cosmetic appearance assessed by blinded evaluator was also measured using Modifed Hollander Wound Evaluation Scale (modified to measure 5 not 6 items). This was not deemed to be validated, and so reviewers did not present the data |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Subjects were randomly assigned to receive either LB or DB for wound closure. Randomization occurred immediately following placement of the subcuticular sutures" Comment: unclear how the randomised sequence was generated |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Randomization occurred immediately following placement of the subcuticular sutures. Due to the fact that the devices are packaged differently, it was not possible for the surgeon to be masked from the knowledge of the randomised treatment assignments" Comment: no evidence of adequate concealment of allocation |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "Due to the fact that devices are packaged differently, it was not possible for the surgeon to be masked from the knowledge of the randomised treatment assignments, however, the study subjects and the follow up assessments were masked to the device being used" Comment: adequate evidence that participants were blinded to the intervention, but personnel were not blinded. This is understandable due to the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: " . . . subjects were asked to return at two weeks and three months post surgery at which time any applicable wound complications (erythema, pain, infection, and dehiscence) were captured along with any reported adverse events" Comment: no indication that the 2 week assessment was undertaken by a blinded assessor Quote " . . . the photos were independently evaluated by a masked panel for cosmesis using the same 100mm VAS as well as a modified Hollander Wound Evaluation Scale (HWES)." "The masked panel consisted of 6 physicians: 2 general dermatologists, 1 dermatologic surgeon, 1 oculoplastic surgeon, 1 facial plastic surgeon, and 1 plastic surgeon." Comment: adequate blinding of assessment outcome of cosmetic appearance at 3 months |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "A total of 43 subjects participated in this trial completing all study visits including 2‐week and 3‐month follow up" Comment: adequate evidence that no loss to follow‐up occurred |
| Selective reporting (reporting bias) | Low risk | All the variables outlined in the methodology were accounted for in the results Comment: judged as low risk. Study protocol not sought |
| Other bias | Low risk | None detected |
Millan 2011.
| Methods | RCT with 60 participants and 14 days of follow‐up | |
| Participants | 60 people undergoing a skin biopsy with chronically inflamed skin Exclusion criteria: infection at location where biopsy was planned and known hypersensitivity to cyanoacrylate or other tissue adhesive Surgery was undertaken in 1 centre in Mexico |
|
| Interventions | Group 1 (n = 30): 2‐octylcyanoacrylate tissue adhesive (no further details) Group 2 (n = 30): monofilament suture (no further details) |
|
| Outcomes | Wound dehiscence (on days 5, 7, 10 and 14 after surgery) Skin closure time |
|
| Notes | Data extraction based on English language abstract and partial translation of report text which was published in Spanish | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: study described as randomised. No further detail |
| Allocation concealment (selection bias) | Unclear risk | Comment: no detail reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: no detail reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: no detail reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: no detail reported |
| Selective reporting (reporting bias) | Low risk | Comment: wound dehiscence was the only outcome listed in the methods and reported |
| Other bias | Unclear risk | Comment: not noted from the translation available |
Mota 2009.
| Methods | Parallel RCT with 100 women and 30‐day follow‐up Data on the primary outcome was not available for 2 participants in the adhesive arm and 1 participant in the suture arm |
|
| Participants | 100 women undergoing mediolateral episiotomy after a vaginal delivery in the absence of any other perianal or vaginal lesions Exclusion criteria: existing local infections or lesions; body mass index 35 (kg/m2); severe pulmonary disease; collagen disease; known immunodeficiency; diabetes mellitus; or currently receiving immunosuppressive treatment The study was conducted in 1 hospital centre in Portugal |
|
| Interventions | Group 1 (n = 53): 2‐octylcyanoacrylate (Dermabond®) tissue adhesive (Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) Group 2 (n = 47): continuous subcuticular suture (rapidly absorbable polyglactin 910) |
|
| Outcomes | Wound dehiscence (42 h‐68 h post‐partum) | |
| Notes | The main outcome measure for the paper was self‐assessed perineal pain during the first 30 days after delivery. This was not deemed to be an outcome relevant to the review given the outcomes listed Skin closure time not reported ‐ only time for whole procedure |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Allocation was decided by opening a previously prepared, opaque, sealed envelope containing a 1:1 computer‐generated random number, assigning the patient to one of the two arms" Comment: use of computer‐generated randomisation adequate |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Allocation was decided by opening a previously prepared, opaque, sealed envelope containing a 1:1 computer‐generated random number, assigning the patient to one of the two arms" Comment: use of opaque, sealed envelopes but not noted whether numbered in such a way as to ensure maintenance of robust allocation concealment. Not clear if person who opened the envelopes was independent |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "Women were not informed of the technique that was used to close the perineal skin throughout the study period." "As both groups required stitching of other layers, it is believed that they were not able to see or feel the difference between the two types of perineal skin closure, at the time of repair or thereafter." Comment: participants were blinded. Understandably difficult to blind the operating surgeon to the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "Other outcomes evaluated were . . . duration of surgical repair and perineal wound complications observed at hospital discharge, 42‐68 hours post ‐partum. This observation was carried out in all cases by one of two authors (RM, FC)" Comment: as the authors were aware of the intervention undertaken, the judgement is that this potentially carries a high risk of bias |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "Intra‐operative data was available for all participants. Data from 42‐68 hours post‐op was missing for 2 participants in the adhesive arm and one in the suture arm." Quote: "Eighty‐six women returned the questionnaires, 49 (92%) from the skin adhesive arm and 37 (79%) from the subcuticular suture arm. This difference was very close to achieving statistical difference p= 0.05 . . .". The results also indicated that the reason for loss of follow up was the participants "did not return questionnaire", rather than "discontinued intervention" Comment: unclear risk of bias |
| Selective reporting (reporting bias) | Low risk | Quote: No direct quotations, but all variables listed in methods section were listed in the tables in the results section Comment: a low risk of reporting bias is inferred |
| Other bias | Low risk | None detected |
Ong 2002.
| Methods | RCT with 3‐month follow‐up. 50 withdrawals at 3‐month follow‐up | |
| Participants | 59 patients requiring unilateral or bi‐lateral herniotomies at KK Womens' and Childrens' Hospital, Singapore | |
| Interventions | Group 1 (n = 26): 2‐octylcyanoacrylate (Dermabond®) tissue adhesive (Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) Group 2 (n = 33): subcuticular polyglecaprone (Monocryl®) suture |
|
| Outcomes | Infection, dehiscence, parent satisfaction and time for closure | |
| Notes | Cosmesis scores at 3 weeks not usable as too early and those at 3‐months not usable due to large loss to follow‐up. Viewed as a high risk of bias with 50 participants dropping out | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "All enrolled patients were allocated to glue or suture by opening serial sealed envelopes prepared with computerised randomisation" Comment: computerised randomisation probably represents randomised sequence generation |
| Allocation concealment (selection bias) | Low risk | Quote: "All enrolled patients were allocated to glue or suture by opening serial sealed envelopes prepared with computerised randomisation" Comment: the use of sequential sealed envelopes would reduce risk of selection bias. We have taken serial to mean that envelopes were kept in a pre‐arranged and transparent fixed order and therefore judged this study to be at low risk of bias for this domain |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported whether the patients or personnel were blinded to the intervention Comment: understandably difficult to blind the operating surgeon to the procedure |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: " . . . assessment was done by an independent, blinded observer (staff nurse) using a previously validated score [The Hollander score] . . . Parent satisfaction with wound cosmesis was recorded at the same time on a 100mm visual analogue scale (VAS)" Comment: reasonable to deduce that this represents a low risk of detection bias for nurse‐assessed cosmetic outcome, but not necessarily participant‐assessed outcomes. Not clear if other outcomes such as wound infection or dehiscence were collected via blinded assessment |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Quote: "We were unable to do a 3‐month wound assessment on most of the patients, as only 9 returned for late follow up" Comment: it is difficult to draw any conclusions from the results of the long‐term outcomes due to high rates of losses to follow‐up. This leads to a high risk of attrition bias |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all variables listed in the methods are listed in the tables in the results section Comment: a low risk of reporting bias is inferred |
| Other bias | Low risk | No other sources of bias were detected |
Ozturan 2001.
| Methods | RCT with 3‐month follow‐up. There were no withdrawals | |
| Participants | 101 people requiring rhinoplasty or septorhinoplasty entered the study Exclusion criteria: a history of peripheral vascular disease; diabetes mellitus; a clotting disorder; keloid or hypertrophic scarring; or an allergy to cyanoacrylate or formaldehyde Conducted at Inonu University Hospital, Turkey |
|
| Interventions | Group 1 (n = 34): butylcyanoacrylate (LiquiBand®. MedLogic Global Ltd, Plymouth, Devon, UK) tissue adhesive Group 2 (n = 67): 6.0 polypropylene sutures for columellar skin closure after the majority of the tension had been taken up using 5.0 chromic catgut |
|
| Outcomes | Dehiscence and infection at 1 week Cosmesis at 3 months by blinded assessment of photographs using VAS and Hollander scale Time required for skin closure |
|
| Notes | We wrote to the authors to clarify the numbers in each group randomised by coin toss and received confirmation that the numbers were correct. We also received clarification that the standard deviations were presented after the means in the results section of the paper | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomly allocated by coin toss" Comment: random sequence generated |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Patients were randomly allocated by coin toss" Comment: no mention of allocation concealment from personnel |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No mention of blinding of participants or personnel Comment: understandably difficult to blind the operating surgeon to the procedure |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "All patients were examined once every week in the first post‐operative month, and once a month for the second and third months. Columellar wounds were examined for infection, inflammation, dehiscence and scarring in addition to cosmetic and functional nasal evaluations". "The three month basal view photograph of each subject were given to two otolaryngologic surgeons who were blinded to the method of repair of the columellar incision" Comment: 3‐month cosmetic assessment blinded. Unclear whether assessments at prior time points were blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "One hundred and one patients . . . were eligible for inclusion"; this figure corresponds with the 101 participants accounted for in the results table Comment: no evidence of loss to follow‐up |
| Selective reporting (reporting bias) | High risk | No direct quotations, but all variables listed in methods are listed in the tables in the results section Comment: a low risk of reporting bias is inferred |
| Other bias | Low risk | No other sources of bias were identified |
Pronio 2011.
| Methods | RCT with follow up at 7 days, 15 days, 1 month, 3 months, 6 months and 12 months. There were no withdrawals | |
| Participants | 70 people who underwent thyroid surgery from November 2005 to May 2007 No inclusion/exclusion criteria were stated In all cases, participants underwent thyroidectomy following a cervical incision The study took place in Italy, although no further information is given regarding the exact location of the trial |
|
| Interventions | Group 1 (n = 32): 2‐octylcyanoacrylate (Dermabond, Ethicon Inc) Group 2 (n = 38): skin staples (Proximate, Ethicon Inc) Prophylactic antibiotics in the form of ceftriaxone were administered to both groups |
|
| Outcomes | Wound dehiscence (7days) Wound infection (7 days; not defined) Cosmetic appearance (assessments by participants at 3, 6 and 12 months relevant here). Data were recorded using the Stony Brook scar evaluation scale composed of 5 dichotomous, evenly weighted categories. Scars are assigned 0–1 point for the presence or absence of a width greater than 2 mm at any point of the scar, a raised (or depressed) scar, a darker coloration than surrounding skin, any hatch or staples marks, an overall poor appearance, the total score ranging from 0 (worst) to 5 (best) Patient's satisfaction with wound management (7 days). Participants were asked to rate their level of satisfaction with the early postoperative management of the wound (regarding the requirement of a return visit for medications, the possibility of washing oneself, the suture removal) using a numerical scale ranging from 0–10 |
|
| Notes | Study records how many closures were considered rapid (between 30 and 60 seconds). These data were not extracted as it was felt that they reported skin closure time in a way that could not be summarised meaningfully Participants were also asked to provide a score using a verbal rating response regarding their scar (at 7 days, 15 days and 3, 6, 9 and 12 months after surgery). Scores could range from 0 to 10: 0–4, poor; 5–6, mild; 7–8, good; and 9–10, excellent. These data were only presented categorically and are not extracted ‐ instead the scar evaluation scale data are presented |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Only when the surgical procedure was completed, after the closure of the platysma, each patient was randomly assigned to the two treatment groups" Comment: no indication that there was evidence of randomised sequence allocation |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Only when the surgical procedure was completed, after the closure of the platysma, each patient was randomly assigned to the two treatment groups" Comment: no indication of allocation concealment from personnel |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No direct quotations, but no indication that the participants or the personnel were blinded to treatment. It is understandably difficult to blind personnel to the intervention arm given during an operation |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "In the follow‐up over 7 and 15 days, 1‐month, 3, 6 and 12‐months periods wound‐healing process was monitored by clinical assessment and documented by digital photographs." Comment: there was no indication that the clinical assessments were made by people who were blinded to the intervention. Therefore the risk of bias here is unclear |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No direct quotations, but no losses to follow‐up encountered |
| Selective reporting (reporting bias) | Low risk | No direct quotations, although all methods of evaluating the interventions were accounted for in the results Comment: adequate outcome reporting |
| Other bias | Low risk | None detected |
Ridgway 2007.
| Methods | RCT with 6‐week follow‐up. 1 withdrawal but no explanation | |
| Participants | 30 participants recruited for cervicotomy for thyroid and para thyroid surgery at Scunthorpe General Hospital, North Lincs, UK. 29 successfully randomised. No reference to inclusion/exclusion criteria | |
| Interventions | Group 1 (n = 14): 2‐octylcyanoacrylate (Dermabond®) tissue adhesive (Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) Group 2 (n = 15): staples (Vivistat®) |
|
| Outcomes | Time to closure, neck mobility, cosmesis and adverse events | |
| Notes | Cosmesis results could not be included as they were measured too early to be usable. No explanation of what characterised an adverse event or the occurrence of such outcomes was provided | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Randomisation to glue or stapled closure was performed following induction of general anaesthesia by random envelope allocation" Comment: method of random sequence allocation not stated |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Randomisation to glue or stapled closure was performed following induction of general anaesthesia by random envelope allocation" Comment: It is not clear whether the envelope was sealed or ordered and marked to be sequential, therefore without further information, the judgement is of an unclear risk of selection bias |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No statement made about whether the personnel were blinded to the procedure Comment: understandably difficult to blind the operating surgeon to the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "Scar cosmesis assessment by both patient, surgeon and independent blinded assessor at 6 weeks." Comment: this assessment was not included in the review (as conducted at less than 3 months) no other information about blinded assessment of other outcomes provided |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No direct quotations, although no losses to follow‐up were reported, and all participants accounted for in results Comment: judged as low risk |
| Selective reporting (reporting bias) | Low risk | No direct quotations although all methods of evaluating the interventions were accounted for in the results Comment: adequate outcome reporting |
| Other bias | Low risk | None detected |
Romero 2011.
| Methods | RCT with 90 days of follow‐up (assessment at 10 and 90 days postoperatively). Assumed all participants' wounds assessed at day 10. There were 6 withdrawals from 90 day follow‐up (2 from adhesives and 4 from strips) | |
| Participants | 49 children undergoing laparoscopic appendectomy Exclusion criteria: presence of concomitant chronic diseases; immunosuppression; malignancies; and conversion to laparotomy or intraoperative enlargement of incisions for intact specimen extractions Conducted in 1 centre in Germany |
|
| Interventions | Group 1 (n = 23): 2‐octylcyanoacrylate (Dermabond®) tissue adhesive (Dermabond, Ethicon, Sommerville, NJ) Group 2 (n = 24): standard adhesive strips ( strips applied in star‐shaped manner) Postoperative antibiotic therapy with cefotaxime and metronidazole was administered intravenously |
|
| Outcomes | Wound dehiscence (assessment at 10 and 90 days after surgery) Wound infection (defined as abscess or redness > 3 mm perpendicular to incision) Cosmetic appearance (surgeon‐rated; at day 10 and day 90 ‐ day 90 data reported here) using a 100 mm VAS where 0 = best scar and 100 = worse scar and assessed by 2 blinded surgeons using macrophotos of each scar (3 photos per participant). Mean value of the 2 assessments has been taken Cosmetic appearance (participant‐rated; at day 10 and day 90 ‐ day 90 data reported here) assessed using a dichotomous question (wording of question not clear but results were reported as % expressing dissatisfaction with cosmetic result) |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "For randomization, a computer‐generated randomization pattern was implemented and patients were intraoperatively assigned to a procedure by means of a blind envelope system" Comment: adequate random sequence generation |
| Allocation concealment (selection bias) | Unclear risk | Quote: "For randomization, a computer‐generated randomization pattern was implemented and patients were intraoperatively assigned to a procedure by means of a blind envelope system" Comment: although attempts made to conceal allocation of the intervention, it was not stated whether the envelopes were sealed sequentially, whether they were sealed, or whether they were opaque, therefore the judgement remains unclear |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No direct quotations, however it is understandably difficult to blind the operating surgeon from the intervention, therefore the judgement is unclear |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "Follow up examinations were carried out on the 10th and 90th postoperative day . . . Follow‐up included clinical investigation and a questionnaire to assess satisfaction with the cosmetic results, postoperative pain at port sites, wound infections, wound dehiscence, and any other adverse events associated with the wound" Comment: no indication that the follow‐up examination on the 10th postoperative day was undertaken by a blinded assessor Quote: [At 90 days] "This assessment was completed by 2 pediatric surgeons blinded to the method of wound repair" Comment: adequate blinding of cosmesis outcome at 3 months |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "A total of 49 patients (24 DermabondTM, 25 Steri‐StripTM) were enrolled between August 2007 and August 2008". "Photographs were taken from 21 patients in the Steri‐StripTM Group and from 22 patients in the DermabondTM Group" Comment: there is a discrepancy concerning 6 participants that were unaccounted for the in the final outcome assessment without clear reporting of why they were not included in the results. Therefore there is a risk of attrition bias, leaving the judgement unclear |
| Selective reporting (reporting bias) | Low risk | No direct quotations, although all methods of evaluating the interventions were accounted for in the results Comment: adequate outcome reporting |
| Other bias | Low risk | None detected |
Sebesta 2004.
| Methods | RCT with 2‐week follow‐up. No participants were lost to follow‐up | |
| Participants | 59 participants were enrolled, in whom 228 trocar sites were closed following undergoing laparoscopic surgery performed by one surgeon in the department of Urology, Wilford Hall Medical Center, Texas, USA No inclusion/exclusion criteria were stated |
|
| Interventions | Group 1 (30 participants; 118 incisions): 2‐octylcyanoacrylate (Dermabond, Ethicon, Sommerville, NJ) Group 2 (29 participants; 110 incisions): subcuticular suture (4‐0 absorbable sutures, either Vicryl or Monocryl) Data presented at participant, not wound, level The fascia of all sites > 1 cm were closed with absorbable suture. Wounds in both groups that did not closely approximate to 1 cm received interrupted, subcutaneous sutures Those who received subcuticular sutures had their wounds dressed with steri‐strips, a 2 x 2xm gauze pad, and tape or a Tegaderm dressing No dressings were applied to the octylcyanoacrylate‐closed wounds |
|
| Outcomes | Wound dehiscence (2 weeks after surgery) Wound infection (2 weeks after surgery; not defined) Mean closure time Cost per patient |
|
| Notes | Cosmetic appearance measured at < 3 months so not included | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "All patients undergoing laparoscopic surgery by one surgeon (JTB) were randomised to receive skin closure with either subcuticular suture of octylcyanoacrylate" Comment: no further information given regarding how the randomised sequence was generated, and therefore the judgement is unclear |
| Allocation concealment (selection bias) | Unclear risk | Quote: "All patients undergoing laparoscopic surgery by one surgeon (JTB) were randomised to receive skin closure with either subcuticular suture of octylcyanoacrylate" Comment: no further information given regarding how the allocation was concealed to the operating surgeon (if at all), therefore the judgement remains unclear |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No direct quotations, but no information given regarding blinding of participants or personnel in this study. It is understandably difficult to blind the operating surgeon to the intervention. Therefore the judgement here is unclear |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "Patients were evaluated 2 weeks postoperatively for evidence of infection, dehiscence, seroma, and general cosmetic appearance." Comment: unclear whether this evaluation was undertaken by a blinded assessor |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No direct quotations, but no reported loss to follow‐up, therefore judgment of low risk |
| Selective reporting (reporting bias) | Unclear risk | Quote: "Postoperative wound complications were similar for both groups. Five patients in the octylcyanoacrylate group had wound complications in 9 incisions. Two patients experienced skin separation in 5 incisions. One patient had a minor wound infection at one incision site treated with oral antibiotics. Two patients experienced small seromas at 2 incision sites, requiring incision opening and healing by secondary intention. We noted small seromas in 2 patients receiving suture closure. These healed by secondary intention after skin opening and drainage. Table 4 presents a summary of the results." Comment: however the table shown does not compare rates of wound complication and the reporting of the outcomes is unclear, it is this author's judgement therefore that the risk of bias here is unclear |
| Other bias | Low risk | None detected |
Shamiyeh 2001.
| Methods | RCT with 9‐month follow‐up. 2 participants were lost to follow‐up from the suture group due to failure to attend and could not be traced by mail or phone | |
| Participants | 79 adults requiring varicose vein surgery on the leg. Trial conducted at Ludwick Boltzmann Institure, Linz, Austria Exclusion criteria: a history of chronic venous insufficiency with dermatosclerosis; previous phlebectomies; or allergy to plaster or octylcyanoacrylate |
|
| Interventions | Mullerian phlebectomy performed creating an average wound length of 5 mm. Used 5 min wound compression followed by skin closure with: Group 1 (n = 26): octylcyanoacrylate tissue adhesive Group 2 (n = 28): 5.0 monofilament suture Group 3 (n = 25): tape A small plaster was placed over each wound |
|
| Outcomes | Wound dehiscence, infection at 10 days, and patient and surgeon satisfaction, and cosmetic appearance at 1 year and costs. Time required for incision closure was also recorded | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote:"Randomisation was done by a computer [during] the morning of the operation day" Comment: this was judged to be an adequate method of generating the randomisation sequence i.e. ‘by computer’ |
| Allocation concealment (selection bias) | Unclear risk | Quote:"Randomisation was done by a computer [during] the morning of the operation day". Comment: there is no mention of the method used to conceal allocation |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No mention of blinding of participants or personnel Comment: understandably difficult to blind the operating surgeon to the procedure |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "The follow up by the operating surgeon was performed [at] 10 days and 6 weeks after the operation" and, "Eight to 14 months after the operation all patients had been investigated by one senior dermatologist who was blinded to the method of skin closure, the scars were examined for color, width, and cosmetic appearance . . ." Comment: blinded outcome assessment achieved for outcomes collected after 8 months. Not clear if blinding was implemented for earlier follow‐up times when wound dehiscence and infection were assessed |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote:"Only 2 of 79 patients were lost to follow‐up, resulting in 77 patients with postoperative control" Comment: no reasons reported for those lost to follow‐up, but as they only represented a small percentage of the total participants, this was judged overall to be at low risk of attrition bias |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all variables listed in methods are listed in the tables in the results section Comment: a low risk of reporting bias is inferred |
| Other bias | Low risk | No other sources of bias were identified |
Sinha 2001.
| Methods | RCT with 6‐month follow‐up. 6 participants were lost to follow‐up: 5 in tissue adhesive and 1 in suture group | |
| Participants | 50 adults requiring hand or wrist surgery (carpal tunnel syndrome, trigger finger, De Quervain's tenosynovitis, ganglions of wrist and hand, and cysts of fingers) Exclusion criteria: requiring surgery for Dupuytren's contracture; repeat surgery; a history of skin allergy or keloid formation; diabetes; or corticosteroid use Trial conducted at Monklands Hospital, Airdre, UK |
|
| Interventions | Skin approximated with skin hooks then: Group 1 (n = 20): application of butylcyanoacrylate adhesive (Indermil), or Group 2 (n = 24): suturing with 4.0 monofilament All cases had local anaesthetic infiltration with or without general anaesthesia |
|
| Outcomes | Dehiscence, infection, cosmetic appearance at 10 days, 2 weeks and 6 weeks | |
| Notes | Cosmetic appearance data not used as assessed at < 3 months | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomised to wound adhesive or suture on the basis of 50 previously prepared and sealed envelopes (25 of each)" Comment: whilst the trial was reported as randomised there was no information about how the sequence was generated |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Patients were randomised to wound adhesive or suture on the basis of 50 previously prepared and sealed envelopes (25 of each)" Comment: judgement of unclear risk of bias, as not clear if envelopes were sequentially numbered and opaque. Not clear who was responsible for allocation |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No information provided about blinding of participants or surgeons Comment: it would be difficult to blind the operating surgeon |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Patients were subsequently assessed at 2 and 6 weeks post‐surgery by a designated tissue viability nurse who was blinded to the method of closure" Comment: outcome assessment blinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Quote: "Of the study 50 participants, six were lost to follow up (five in the adhesive group and one in the suture group)" Comment: the sample size of the study is small, 6 participants lost represents over 20% of the total sample. No information reported on reasons for withdrawal |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all variables listed in methods are listed in the tables in the results section Comment: a low risk of reporting bias is inferred |
| Other bias | Low risk | No other sources of bias were identified |
Sniezek 2007.
| Methods | RCT with 3‐month follow‐up. No reference to withdrawals | |
| Participants | 14 participants recruited for removal of basal cell carcinoma or squamous cell carcinoma of the head and neck using the Mohs technique at the Department of Dermatology at University Hospital Iowa | |
| Interventions | Split wound design, so both methods of closure were used for part of each wound Intervention 1: 2‐octylcyanoacrylate (Dermabond®; Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) Intervention 2: polypropylene cuticular suture |
|
| Outcomes | Dehiscence, infection and cosmesis | |
| Notes | As a split wound design the data were paired. The authors were contacted for the mean difference and the standard deviation of the cosmetic scores on a participant basis. No reply was received, therefore this information was not included in the review | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Half of the surgical wound was randomly selected (by coin toss) for epidermal approximation . . ." Comment: use of coin toss judged to constitute adequate random sequence generation |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Half of the surgical wound was randomly selected (by coin toss) for epidermal approximation . . ." Comment: no information given about whether the personnel were concealed to the allocation |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No reporting of either participants or personnel being blinded to the intervention Comment: as the nature of the intervention was that the two methods of closure were placed together to close the same incision, there is potential that participants may have understood the method of closure. Similarly it is understandably difficult to blind the operating surgeon to the intervention. The judgement is therefore unclear |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "Patients returned in 7 days for suture removal and were evaluated for early complications such as wound separation, or dehiscence, inflammation or infection. High resolution photographs were obtained immediately post‐operatively and 3 months postoperatively" and, "The primary outcome measure was scar cosmesis, evaluated by comparing both halves of the scar from the 3 month photographs by five blinded dermatologists" Comment: unclear whether assessment at day 7 was blinded. 3‐month assessment of cosmesis was blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "All 14 patients completed all study end points" Comment: judged as low risk. |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all variables listed in methods are listed in the tables in the results section Comment: a low risk of reporting bias is inferred |
| Other bias | Low risk | No other sources of bias were identified |
Switzer 2003.
| Methods | RCT with 4‐week follow‐up. 2 withdrawals accounted for | |
| Participants | 45 participants recruited for elective repair of inguinal hernias at the Eisenhower Army Medical Centre, Fort Gordon, Georgia, USA Inclusion/exclusion criteria not reported |
|
| Interventions | Group 1 (n = 24): 2‐octylcyanoacrylate (Dermabond®) tissue adhesive (Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) Group 2 (n = 22): subcuticular polyglecaprone (Monocryl®) suture |
|
| Outcomes | Dehiscence, infection, cosmesis and time taken to closure | |
| Notes | The cosmetic data were not included as the data were taken at < 3 months. The authors were contacted for the mean and standard deviations for the time to closure, but since no response has been received these data were not included | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: " . . . patients were then randomised with the use of a computerized random number generator to receive either 2‐octylcyanoacrylate tissue adhesive or subcuticular running 4‐0 poliglecaprone 25 (Monocryl, Ethicon, Inc) skin closure" Comment: judgement of a low risk of selection bias due to use of computer to generate random number sequence |
| Allocation concealment (selection bias) | Unclear risk | Quote: " . . . patients were then randomised with the use of a computerized random number generator to receive either 2‐octylcyanoacrylate tissue adhesive or subcuticular running 4‐0 poliglecaprone 25 (Monocryl, Ethicon, Inc) skin closure" Comment: No specific mention of how sequence was allocated. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported whether participants or personnel were blinded to the intervention Comment: understandably difficult to blind operating surgeon to intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "Patients were monitored postoperatively for complications of their closures, and all patients were scheduled for post‐operative visits at 2 weeks and at 4 weeks" Comment: it is not reported whether those monitoring for post‐operative complications were blinded to the intervention. Cosmesis assessment was blinded, but these data were not extracted here as taken at < 3 months after surgery |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Not directly stated, but no participants were reported to have been lost to follow‐up and all were accounted for in results Comment: judged as low risk of attrition bias |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all variables listed in methods are listed in the tables in the results section Comment: a low risk of reporting bias is inferred |
| Other bias | Low risk | None detected |
Tierny 2009.
| Methods | Split body design RCT with 3 months follow‐up | |
| Participants | 8 participants undergoing surgery for non‐melanomas skin cancer Exclusion criteria: on immuno‐suppressive medication and/or recipients of organ transplants Undertaken in 1 centre in the USA |
|
| Interventions | 8 participants, each having half of incisional wound randomised to each intervention Intervention 1 (8 half wounds): 2‐octylcyanoacrylate (Dermabond®) tissue adhesive (Ethicon Inc, a Johnson & Johnson company, Somerville, New Jersey, USA) Intervention 2 (8 half wounds): rapid absorbing gut suture |
|
| Outcomes | Wound dehiscence (1 week postoperatively) Wound infection (1 week postoperatively ‐ no definition provided) |
|
| Notes | Cosmetic appearance (surgeon) at 3 months and cosmetic appearance (participant) at 3 months were collected but the data are not clear and not presented here. The report suggests that outcome data were reported on a 1 to 4 point scale but some data are > 4 so this is unclear. Also unclear what the scale measured Patient reference data not extracted |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomised for epidermal closure with one half of the wounds (chest (n=6) and upper extremities n=2)) with rapid absorbing gut structure and on the other half with 2‐octylethylcyanoacrylate tissue adhesive" Comment: no information given about the method of randomisation |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Patients were randomised for epidermal closure with one half of the wounds (chest (n=6) and upper extremities n=2)) with rapid absorbing gut structure and on the other half with 2‐octylethylcyanoacrylate tissue adhesive" Comment: no information given about whether allocation was concealed from the participants |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "All wounds were closed by a single surgeon (DJK) using a linear, bilayered closure method . . ." Comment: no information given about whether the participants or the personnel were blinded to the intervention. However, it would be difficult to blind personnel to a surgical intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "Patients were seen for evaluation at postoperative visits at both 1 week and 3 months after the procedure. Incidence of wound dehiscence and side effects of itching, bleeding, and pain were assessed at 1 week" Comment: unclear whether those evaluating the wounds at 1 week were blinded to the intervention |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No direct quotations, although there was no loss to follow‐up reported within the study |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all variables listed in methods are listed in the tables in the results section Comment: a low risk of reporting bias is inferred |
| Other bias | Low risk | None detected |
Toriumi 1998.
| Methods | RCT with 1‐year follow‐up. 11 participants were lost to follow‐up, but the groups from which they came were not specified | |
| Participants | People over 1 year of age requiring elective surgery for benign skin lesions predominantly in face and neck Exclusion criteria: a history of significant trauma; peripheral vascular disease; diabetes mellitus; blood clotting disorder; keloid or hypertrophy scarring; known allergy to cyanoacrylate or formaldehyde Trial conducted at University of Illinois, Chicago, USA |
|
| Interventions | Incisions with and without subcutaneous sutures were randomised for closure with: Group 1: 2‐octylcyanoacrylate, or Group 2: 5.0 or 6.0 nylon suture |
|
| Outcomes | Dehiscence, infection, cosmesis and closure time | |
| Notes | Participants lost to follow up were not reported by group | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Using clinical indications as evaluated by the surgeon, patients were assigned to one of the two treatment groups". Later trial report mentions "Patients were randomised . . ." Comment: no method of randomised sequence generation stated. The initial quotation suggests clinicians had some autonomy in deciding which participants were to receive which treatment, which in turn represents a high risk of bias, but this is unclear |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Using clinical indications as evaluated by the surgeon, patients were assigned to one of the two treatment groups" Comment: no mention of allocation concealment and possible evidence that surgeon was aware of allocation |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No mention of blinding of participants or personnel Comment: due to the nature of the surgical procedure, it would be difficult to blind either the operating surgeon or participants |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "At each postoperative visit, wounds were examined for infection, inflammation, wound dehiscence or separation, and scarring." and, "At the 90 day follow up visit, the wounds were graded for cosmesis using the modified Hollander wound evaluation scale”, and, at one year, the patients were assessed by way of a standardised method of photography of the wound, "The photographs were then given to two facial plastic surgeons that were unfamiliar with the study design, the purpose or the site of the surgical incision, or the type of treatment received" Comment: no indication of blinded outcome assessment for outcomes assessed prior to one year. Blinded outcome assessment of wound appearance at 12 month follow‐up |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No direct quotations given, but results show that of the 100/111 (90%) patients enrolled in the study for their long term 1‐year follow‐up wound evaluation Comment: 10% loss of follow‐up data at 12 months |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all variables listed in methods are listed in the tables in the results section Comment: a low risk of reporting bias is inferred |
| Other bias | Low risk | No other sources of bias were identified |
van den Ende 2004.
| Methods | 2‐arm RCT with 6 week follow‐up | |
| Participants | 100 children undergoing correction of hernia inguinalis No inclusion or exclusion criteria stated |
|
| Interventions | Group 1 (n = 50): butylcyanoacrylate (Indermil) tissue adhesive Group 2 (n = 50): polyglactin 5‐0 (Vicryl) sutures |
|
| Outcomes | Wound dehiscence (10 days after surgery) Wound infection (not defined; 10 days after surgery) Mean closure time |
|
| Notes | It is noted that 100 participants were randomised and that some had surgery on both sides of the abdomen. It was not clear from the study results whether outcomes were presented at the participant level. In one instance where % data are presented the denominator used was 50 for each group suggesting that there is no unit of analysis issue but this is not clear Wound cosmesis assessed at 6 weeks ‐ not presented here |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were selected randomly to receive wound adhesive or suture on the basis of 100 previously prepared and sealed envelopes containing slips for either suture closure or the use of Indermil (50 of each)" Comment: use of opaque, sealed envelopes, but not noted whether numbered in such a way as to ensure robust allocation concealment maintained. Not clear if person who opened envelopes was independent |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No mention of blinding of participants or personnel Comment: due to the nature of the surgical procedure, it would be difficult to blind either the operating surgeon |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No mention of blinded outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No mention of loss to follow‐up |
| Selective reporting (reporting bias) | Low risk | No direct quotations, but all variables listed in methods are listed in the tables in the results section Comment: a low risk of reporting bias is inferred |
| Other bias | Unclear risk | Comment: it is noted that 100 participants were randomised and that some had surgery on both sides of the abdomen. It is not clear from the study results if outcomes are presented at the participant level. Where % data is presented in one case the denominator used was 50 for each group suggesting that there is no unit of analysis issue but this is not clear |
Abbreviations
h = hour(s) min = minute(s) RCT = randomised controlled trial ROM = range of motion VAS = visual analogue scale
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Ak 2012 | Not relevant wound type (not surgical wound) |
| Alhopuro 1976 | No data given in the paper. We have contacted authors but did not receive a reply |
| Chen 2010 | Does not include any outcome relevant to this review |
| Chow 2010 | Does not include any outcome relevant to this review |
| Giri 2004 | Not an RCT |
| Gorozpe‐Calvillo 1999 | After full translation, found not to be an RCT |
| Jaibaji 2000 | All participants in the intervention group had a precautionary subcuticular suture placed. The reviewers viewed this as an inherent bias to the outcome of this group and thus the study was excluded |
| Kuo 2006 | All participants had a subcuticular suture placed and described the intervention as a method of "superficial" closure. The reviewers viewed this as unnecessary and counter‐intuitive as the aim of the study is to assess the adhesive as an alternative to other methods of closure of incisions, not as an adjunct |
| Matin 2003 | Not an RCT ‐ see quotation below ‐ considered alternation Quote: "Randomization was performed weekly. Each odd numbered week of the study (first week, third week, etc. was randomized to either OCA or suturing by a biostatistician, and then the subsequent even numbered week (second week, fourth week, etc) received the opposite treatment." |
| Maw 1997 | Not considered an RCT |
| Ong 2010 | Skin closure method was not the only systematic difference between groups |
| Orozco‐Razon 2002 | There was no reference to randomisation. The authors have been contacted but we have received no reply |
| Quinn 1998 | Not relevant wound type (not surgical wound) |
| Sajid 2009 | Not an RCT |
| Silvestri 2006 | Not an RCT |
| Singer 2002 | Data could not be used because combined with data for lacerations. We wrote to the authors requesting data by group but did not receive a reply |
| Spencker 2011 | Not an RCT |
| Steiner 2000 | Not an RCT |
| Sun 2005 | No relevant outcomes (based on translation) |
| Wong 2011 | Not relevant wound type (not surgical wounds) |
Abbreviation
RCT = randomised controlled trial
Characteristics of studies awaiting assessment [ordered by study ID]
Gennari 2004.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | Citation retrieved through handsearching awaiting full text retrieval |
Handschel 2006.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | Citation retrieved through handsearching awaiting full text retrieval |
Jan 2013.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | Conference abstract with limited data ‐ contacting authors to find out if there is a pending publication or if further information available |
Nipshagen 2008.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | Citation retrieved through handsearching awaiting full text retrieval |
Yoon 2006.
| Methods | Requires translation |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes |
Differences between protocol and review
Time to closure as an outcome measure was included in the review post hoc as the review authors believe this to be a contributory factor towards both cost‐effectiveness and satisfaction.
Contributions of authors
Jo Dumville: coordinated the second review update. Extracted data and checked quality of data extraction. Undertook and checked quality assessment. Analysed and interpreted data. Performed statistical analysis and checked quality of statistical analysis. Performed part of writing and editing the review. Approved final review update prior to submission. Secured funding. Is the guarantor of the review. Paul Coulthard: conceived, designed and co‐ordinated the initial review. Undertook the searches for the original review and screened search results. Appraised quality and extracted data, wrote to trial authors for additional information. Managed data for the review and entered data into RevMan. Analysed and interpreted data and wrote the review. Undertook previous work that was the foundation of the current review. Approved final review update prior to submission. Philip Riley: analysed and interpreted data for the second review update. Performed statistical analysis and checked quality of statistical analysis. Performed part of writing and editing the review. Approved final review update prior to submission. Helen Worthington: analysed and interpreted data for all versions of the review. Performed statistical analysis and checked quality of statistical analysis. Performed part of writing and editing the review. screened search output for the second update. Approved final review update prior to submission Neil Patel: undertook quality assessment and checked quality assessment for the first update. Performed part of writing and editing the review. Approved final review update prior to submission. Marco Esposito: developed the search strategy, undertook the searches for the original review and advised on the review and commented on all updates of the review. Maarten van der Elst: Provided general advice on the original version of the review and undertook previous work that was the foundation of the current review. Oscar JF van Waes: screened search results against the inclusion criteria and retrieved papers, appraised quality and extracted data, wrote to trial authors for additional information for the original version of the review. Undertook previous work that was the foundation of the current review. James Darcey: screened search results against the inclusion criteria, retrieved papers, appraised quality and extracted data, wrote to trial authors for additional information for the for the first review update, managed data for the first review update and entered data into RevMan. Analysed and interpreted data and wrote the first review update.
Contributions of editorial base
Nicky Cullum: edited the review, advised on methodology, interpretation and review content. Approved the final review and review update prior to submission. Sally Bell‐Syer: co‐ordinated the editorial process. Advised on methodology, interpretation and content. Edited and copy edited the review and the updated review. Amanda Briant: ran the searches and edited the search methods section for the update.
Sources of support
Internal sources
The University of Manchester, UK.
Renier de Graaf Hospital, Netherlands.
The Sahlgrenska Academy at Goteborg University, Sweden.
External sources
Swedish Medical Research Council (9495), Sweden.
The Hjalmar Svensson Research Fund, Sweden.
The National Institute for Health Research (NIHR) is the sole funder of the Cochrane Wounds Group, UK.
Declarations of interest
Jo C Dumville: None known Paul Coulthard: was a co‐author in the Blondeel 2004 study. This study was also commercially supported by Ethicon. Philip Riley: None known Helen V Worthington: None known Neil Patel: None known Marco Esposito: None known Maarten van der Elst: None known Oscar J F van Waes: None known James Darcey: None known
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Amin 2009 {published data only}
- Amin M, Glynn F, Timon C. Randomised trial of tissue adhesive vs staples in thyroidectomy integrating patient satisfaction and Manchester score. Otolaryngology ‐ Head and Neck Surgery 2009;140(5):703‐8. [DOI] [PubMed] [Google Scholar]
Avsar 2009 {published data only}
- Avsar A, Ustunnner I, Keskin L, Ozturk O, Tas E. 2‐octylcyanoacrylate tissue adhesive versus polypropylene suture for skin closure of Pfannenestiel incision. Tűrk Jinekoloji ve Obstetrik Derneği Dergisi 2009;6:117‐22. [Google Scholar]
Blondeel 2004 {published data only}
- Blondeel P, Murphy J, Debrosse D, Nix, J, Puls LE, Theodore N, et al. Closure of long surgical incisions with a new formulation of 2‐octylcyanoacrylate tissue adhesive versus commercially available methods. American Journal of Surgery 2004;188:307‐13. [DOI] [PubMed] [Google Scholar]
Brown 2009 {published data only}
- Brown JK, Campbell BT, Drongowski RA, Alderman AK, Geiger JD, Teitelbaum DH, et al. A prospective, randomized comparison of skin adhesive and subcuticular suture for closure of pediatric hernia incisions: cost and cosmetic considerations. Journal of Paediatric Surgery 2009;44(7):1418‐22. [DOI] [PubMed] [Google Scholar]
Cheng 1997 {published data only}
- Cheng W, Saing H. A prospective randomised study of wound approximation with tissue glue in circumcision in children. Journal of Paediatric Child Health 1997;33:515‐6. [DOI] [PubMed] [Google Scholar]
Chibbaro 2009 {published data only}
- Chibbaro S, Tacconi L. Use of skin glue versus traditional wound closure methods in brain surgery: a prospective, randomized, controlled study. Journal of Clinical Neuroscience 2009;16(4):535‐9. [DOI] [PubMed] [Google Scholar]
Dowson 2006 {published data only}
- Dowson C, Gilliam A, Speake W, Lobo D, Beckingham. A prospective, randomised controlled trial comparing n‐butyl cyanoacrylate tissue adhesive (Liquiband) with sutures for skin closure after laparoscopic general surgical procedures. Surgical Laparoscopy, Endoscopy and Percutaneous Techniques 2006;16(3):146‐50. [DOI] [PubMed] [Google Scholar]
Eggers 2011 {published data only}
- Eggers MD, Fang L, Lionberger DR. A comparison of wound closure techniques for total knee arthroplasty. Journal of Arthroplasty 2011;26(8):1251‐8. [DOI] [PubMed] [Google Scholar]
Greene 1999 {published data only}
- Greene D, Kock RJ, Goode RL. Efficacy of octyl‐2‐cyanoacrylate tissue glue in blepharoplasty. Archives of Facial Plastic Surgery 1999;1:292‐6. [DOI] [PubMed] [Google Scholar]
Jallali 2004 {published data only}
- Jallali N, Haji A, Watson CJ. A prospective randomized trial comparing 2‐octylcyanoacrylate to conventional suturing in closure of laparoscopic cholecystectomy incisions. Journal of Laparoendoscopic and Advanced Surgical Techniques 2004 Aug;14(4):209‐11. [DOI] [PubMed] [Google Scholar]
Keng 1989 {published data only}
- Keng TM, Bucknall TE. A clinical trial of tissue adhesive (histoacryl) in skin closure of groin wounds. Medical Journal of Malaysia 1989;44(2):122‐8. [PubMed] [Google Scholar]
Kent 2014 {published data only}
- Kent A, Liversedge N, Dobbins B, McWhinnie D, Haider J. A prospective randomised controlled double‐masked multi‐center clinical trial of medical adhesives for the closure of laparoscopic incisions. Journal of Minimally Invasive Gynecology 2014;21:252‐8. [DOI] [PubMed] [Google Scholar]
Khan 2006 {published data only}
- Khan RJK, Fick D, Yao F, Tang K, Hurworth M, Nivbrant B, et al. A comparison of three methods of wound closure following arthroplasty: a prospective randomised controlled trial. The Journal of Bone and Joint Surgery 2006;88:238‐42. [DOI] [PubMed] [Google Scholar]
Kouba 2011 {published data only}
- Kouba DJ, Tierney E, Mahmoud BH, Woo D. Optimizing closure materials for upperlid blepharoplasty: a randomized, controlled trial. Dermatologic Surgery 2011;37(1):19‐30. [DOI] [PubMed] [Google Scholar]
Krishnamoorthy 2009 {published data only}
- Krishnamoorthy B, Najam O, Khan UA, Waterworth P, Fildes JE, Yonan N. Randomized prospective study comparing conventional subcuticular skin closure with Dermabond skin glue after saphenous vein harvesting. The Annals of Thoracic Surgery 2009;88(5):1445‐9. [DOI] [PubMed] [Google Scholar]
Livesey 2009 {published data only}
- Livesey C, Wylde V, Descamps S, Estela CM, Bannister GC, Learmonth ID, et al. Skin closure after total hip replacement: a randomised controlled trial of skin adhesive versus surgical staples. Journal of Bone and Joint Surgery 2009;91(6):725‐9. [DOI] [PubMed] [Google Scholar]
Maartense 2002 {published data only}
- Maartense S, Bemelman WA, Dunker MS, Lint C, Pierik EGJM, Busch ORC, et al. Randomised study of the effectiveness of closing laparoscopic trocar wounds with octylcyanoacrylate, adhesive papertape or poliglecaprone. British Journal of Surgery 2002;89:1370‐5. [DOI] [PubMed] [Google Scholar]
Maloney 2013 {published data only}
- Maloney J, Rogers GS, Kapadia M. Surgical corner: a prospective randomized evaluation of cyanoacrylate glue devices in the closure of surgical wounds. The Journal of Drugs in Dermatology 2013;12(7):810‐4. [PubMed] [Google Scholar]
Millan 2011 {published data only}
- Millan P, Olivera R, Sanchez A. Efficacy and safety of 2‐octylcyanoacrylate versus simple suture in surgical wound closure of chronic skin inflammation. Dermatologia Revista Mexicana 2011;55(4):185‐7. [Google Scholar]
Mota 2009 {published data only}
- Mota R, Costa F, Amaral A, Oliveira F, Santos CC, Ayres‐De‐Campos D. Skin adhesive versus subcuticular suture for perineal skin repair after episiotomy ‐ a randomized controlled trial. Acta Obstetricia et Gynecologica Scandinavica 2009;88(6):660‐6. [DOI] [PubMed] [Google Scholar]
Ong 2002 {published data only}
- Ong C, Jacobsen A, Joseph V. Comparing wound closure using tissue glue versus subcuticular suture for paediatric surgical incisions: a prospective, randomised trial. Paediatric Surgery International 2002;18:553‐5. [DOI] [PubMed] [Google Scholar]
Ozturan 2001 {published data only}
- Ozturan O, Miman MC, Aktas D, Oncel S. Butylcyanoacrylate tissue adhesive for columellar incision closure. The Journal of Laryngology and Otology 2001;115:535‐40. [DOI] [PubMed] [Google Scholar]
Pronio 2011 {published data only}
- Pronio A, Fillippo A, Narillii P, Caporilli D, Vestri A, Ciamberlaon B, et al. Closure of cutaneous incision after thyroid surgery: a comparison between metal clips and cutaneous octyl‐2‐cyanoacrylate adhesive. A prospective randomized clinical trial. European Journal of Plastic Surgery 2011;34:103‐10. [Google Scholar]
Ridgway 2007 {published data only}
- Ridgway D, Mahmood F, Moore L, Bramley D, Moore P. A blinded, randomised, controlled trial of stapled versus tissue glue closure of neck surgery incisions. Annals of the Royal College of Surgeons of England 2007;89(3):242‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Romero 2011 {published data only}
- Romero P, Frongia G, Wingerter S, Holland‐Cunz S. Prospective, randomized,controlled trial comparing a tissue adhesive (Dermabond™) with adhesive strips (Steri‐Strips™) for the closure of laparoscopic trocar wounds in children. European Journal of Pediatric Surgery 2011;21(3):159‐62. [DOI] [PubMed] [Google Scholar]
Sebesta 2004 {published data only}
- Sebesta MJ, Bishoff JT. Octylcyanoacrylate skin closure in laparoscopy. Journal of the Society of Laparoendoscopic Surgery 2004;8(1):9‐14. [PMC free article] [PubMed] [Google Scholar]
Shamiyeh 2001 {published data only}
- Shamiyeh A, Schrenk P, Stelzer T, Wayand WU. Prospective randomised blind controlled trial comparing sutures, tape, and octylcyanoacrylate tissue adhesive for skin closure after phlebectomy. Dermatologic Surgery 2001;27(10):877‐80. [DOI] [PubMed] [Google Scholar]
Sinha 2001 {published data only}
- Sinha S, Naik M, Wright V, Timmons J, Campbell AC. A single blind, prospective, randomised trial comparing n‐butyl 2‐cyanoacrylate tissue adhesive (Indermil) and sutures for skin closure in hand surgery. Journal of Hand Surgery 2001;26B(3):264‐5. [DOI] [PubMed] [Google Scholar]
Sniezek 2007 {published data only}
- Sniezek P, Walling H, DeBloom III J, Messingham M, VanBeek M, Kreiter C, et al. A randomised controlled trial of high‐viscosity 2‐octyl cyanoacrylate tissue adhesive versus sutures in repairing facial wounds following Mohs micrographic surgery. Dermatological Surgery 2007;33(8):966‐71. [DOI] [PubMed] [Google Scholar]
Switzer 2003 {published data only}
- Swtizer E, Dinsmore R, North J. Subcuticular closure versus dermabond: a prospective randomised trial. The American Surgeon 2003;69:434‐6. [PubMed] [Google Scholar]
Tierny 2009 {published data only}
- Tierney EP, Moy RL, Kouba DJ. Rapid absorbing gut suture versus 2‐octylethylcyanoacrylate tissue adhesive in the epidermal closure of linear repairs. Journal of Drugs in Dermatology 2009;8(2):115‐9. [PubMed] [Google Scholar]
Toriumi 1998 {published data only}
- Toriumi DM, O'Grady K, Desai D, Bagal AB. Use of octyl‐2‐cyanoacrylate for skin closure in facial plastic surgery. Plastic and Reconstructive Surgery 1998;102(6):2209‐19. [DOI] [PubMed] [Google Scholar]
van den Ende 2004 {published data only}
- Ende ED, Vriens PWHE, Allema JH, Breslau PJ. Adhesive bonds or percutaneous absorbable suture for closure of surgical wounds in children. Results of a prospective randomized trial. Journal of Pediatric Surgery 2004;39:1249‐51. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Ak 2012 {published data only}
- Ak G, Alpkılıç Başkırt E, Kürklü E, Koray M, Tanyeri H, Zülfikar B. The evaluation of fibrin sealants and tissue adhesives in oral surgery among patients with bleeding disorders. Turkish Journal of Hematology 2012;29(1):40‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Alhopuro 1976 {published data only}
- Alhopuro S, Rintala A, Salo H, Ritsila V. Tissue adhesive versus sutures in closure of incision wounds. A comparative study in human skin. Annales Chirurgiae et Gynaecologiae 1976;65:308‐12. [PubMed] [Google Scholar]
Chen 2010 {published data only}
- Chen K, Klapper AS, Voige H, Priore G. A randomized, controlled study comparing two standardized closure methods of laparoscopic port sites. Journal of the Society of Laparoendoscopic Surgery 2010;14(3):391‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Chow 2010 {published data only}
- Chow A, Marshall H, Zacharakis E, Paraskeva P, Purkayastha S. Use of tissue glue for surgical incision closure: a systematic review and meta‐analysis of randomized controlled trials. Journal of the American College of Surgery 2010;211:115‐25. [DOI] [PubMed] [Google Scholar]
Giri 2004 {published data only}
- Giri P, Das MK, Majumdar Giri A. Management of different types of wound by cyanoacrylate glue fixation: a random study of 213 patients. Journal of the Indian Medical Association 2004;102(11):624, 626. [PubMed] [Google Scholar]
Gorozpe‐Calvillo 1999 {published data only}
- Gorozpe‐Calvillo JI, Gonzalez‐Villamil J, Santoya‐Haro S. Closure of the skin with cyanoacrylate in caesarian surgery [Cierre de la piel con cianoacrilato en las cesareas]. Ginecologia y Obstetricia de Mexico 1999;67:491‐5. [PubMed] [Google Scholar]
Jaibaji 2000 {published data only}
- Jaibaji M, Liddington M, Geary P, Darcy C, Batchelor A, Roberts A. Evaluation of the long term outcome of wounds closed with "Indermil" adhesive. European Journal of Plastic Surgery 2000;23:330‐2. [Google Scholar]
Kuo 2006 {published data only}
- Kuo F, Lee D, Rodgers G. Prospective, randomised, blinded study of a new wound closure film versus cutaneous suture for surgical wound closure. Dermatological Surgery 2006;32:676‐81. [DOI] [PubMed] [Google Scholar]
Matin 2003 {published data only}
- Matin SF. Prospective randomized trial of skin adhesive versus sutures for closure of 217 laparoscopic port‐site incisions. Journal of the America College of Surgeons 2003;196(6):845‐53. [DOI] [PubMed] [Google Scholar]
Maw 1997 {published data only}
- Maw JL, Quinn JV, Wells GA, Ducic Y, Odell PF, Lamothe A, et al. A prospective comparison of octylcyanoacrylate tissue adhesive and suture for the closure of head and neck incisions. Journal of Otolaryngology 1997;26(1):26‐30. [PubMed] [Google Scholar]
Ong 2010 {published data only}
- Ong J, Ho KS, Chew MH, Eu KW. Prospective randomised study to evaluate the use of DERMABOND ProPen (2‐octylcyanoacrylate) in the closure of abdominal wounds versus closure with skin staples in patients undergoing elective colectomy. International Journal of Colorectal Disease 2010;25(7):899‐905. [DOI] [PubMed] [Google Scholar]
Orozco‐Razon 2002 {published data only}
- Orozco‐Razon LF, Millan‐Guerrero RO, Vera‐Rodriguez SE. Butylcyanoacrylate tissue adhesive for columellar incision closure [Cyanoacrylate compared with traditional surgery in tension‐free incision closure [Spanish]]. Gaceta Medica de Mexico 2002;138(6):505‐9. [PubMed] [Google Scholar]
Quinn 1998 {published data only}
- Quinn J, Wells G, Sutcliffe T, Jarmuske M, Maw J, Stiell I, et al. Tissue adhesive versus suture wound repair at 1 year: randomized clinical trial correlating early, 3‐month, and 1‐year cosmetic outcome. Annals of Emergency Medicine 1998;32(6):645‐9. [DOI] [PubMed] [Google Scholar]
Sajid 2009 {published data only}
- Sajid MS, Siddiqui MR, Khan MA, Baig MK. Meta‐analysis of skin adhesives versus sutures in closure of laparoscopic port‐site wounds. Surgical Endoscopy 2009;23(6):1191‐7. [DOI] [PubMed] [Google Scholar]
Silvestri 2006 {published data only}
- Silvestri A, Brandi C, Grimaldi L, Nisi G, Brafa A, Calabro M, et al. Octyl‐2‐cyanoacrylate adhesive for skin closure and prevention of infection in plastic surgery. Aesthetic Plastic Surgery 2006;30:695‐9. [DOI] [PubMed] [Google Scholar]
Singer 2002 {published data only}
- Singer AJ, Quinn JV, Clarke RE, Hollander JE. Closure of lacerations and incisions with octylcyanoacrylate: a multicentre randomised controlled trial. Surgery 2002;131:270‐6. [DOI] [PubMed] [Google Scholar]
Spencker 2011 {published data only}
- Spencker S, Coban N, Koch L, Schirdewan A, Mueller D. Comparison of skin adhesive and absorbable intracutaneous suture for the implantation of cardiac rhythm devices. European Journal of Pacing, Arrhythmias and Cardiac Electrophysiology 2011;13(3):416‐20. [DOI] [PubMed] [Google Scholar]
Steiner 2000 {published data only}
- Steiner Z, Mogilner J. Histoacryl vs Dermabond cyanoacrylate glue for closing small operative wounds. Harefuah 2000;139(11‐12):409‐11, 496. [PubMed] [Google Scholar]
Sun 2005 {published data only}
- Sun J, Chen Q‐M, Zhang M, Shi C. Octylcyanoacrylate versus absorbable suture in the repair of skin wounds in children. Zhongguo Linchuang Kangfu 2005;9(19):186‐7. [Google Scholar]
Wong 2011 {published data only}
- Wong EM, Rainer TH, Ng YC, Chan MS, Lopez V. Cost‐effectiveness of Dermabond versus sutures for lacerated wound closure: a randomised controlled trial. Hong Kong Medical Journal 2011;17 Suppl 6:4‐8. [PubMed] [Google Scholar]
References to studies awaiting assessment
Gennari 2004 {published data only}
Handschel 2006 {published data only}
Jan 2013 {published data only}
Nipshagen 2008 {published data only}
Yoon 2006 {published data only}
Additional references
Bruns 1996
- Bruns TB, Simon HK, McLario DJ. Laceration repair using a tissue adhesive in a children's emergency department. Pediatrics 1996;98:673‐5. [PubMed] [Google Scholar]
Coover 1959
- Coover HN, Joyner FB, Sheere NH. Chemistry and performance of cyanoacrylate adhesive. Journal of the Society of Plastic Surgery of England 1959;1:5‐6. [Google Scholar]
Deeks 2011
- Deeks JJ, Higgins JPT, Altman DG (editors). Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. available from www.cochrane‐handbook.org.
Dunker 1998
- Dunker MS, Stiggelbout AM, Hogezand RA, Ringers J, Griffioen G, Bemelman WA. Cosmesis and body image after laparoscopic assisted and ileocolic resection for Crohn's disease. Surgical Endoscopy 1998;12:1334‐40. [DOI] [PubMed] [Google Scholar]
Emori 1993
- Emori TG, Gaynes RP. An overview of nosocomial infections, including the role of the microbiological laboratory. Clinical Microbiology 1993;6:428‐42. [DOI] [PMC free article] [PubMed] [Google Scholar]
Farion 2001
- Farion KJ, Russell KF, Osmond MH, Hartling L, Klassen TP, Durec T, et al. Tissue adhesives for traumatic lacerations in children and adults. Cochrane Database of Systematic Reviews 2001, Issue 4. [DOI: 10.1002/14651858.CD003326] [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Altman DG, Sterne JAC (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Hollander 1995
- Hollander JE, Singer AJ, Valentine S, Henry MC. Wound registry: development and validation. Annals of Emergency Medicine 1995;25:675‐85. [DOI] [PubMed] [Google Scholar]
Houston 1969
- Houston S, Hodge JW Jr, Ousterhout DK, Leonard F. The effect of alpha‐cyanoacrylates on wound healing. Journal of Biomedical Materials Research 1969;3(2):281‐9. [DOI] [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org 2011.
Malone 2002
- Malone DL, Genuit T, Tracy JK. Surgical site infections: reanalysis of risk factors. Journal of Surgical Research 2002;103:89‐95. [DOI] [PubMed] [Google Scholar]
Osmond 1999
- Osmond MH. Pediatric wound management: the role of tissue adhesives. Pediatric Emergency Care 1999;15(2):137‐40. [PubMed] [Google Scholar]
Perron 2000
- Perron AD, Garcia JA, Hays EP. The efficacy of cyanoacrylate‐derived surgical adhesive for use in the repair of lacerations during competitive athletics. American Journal of Emergency Medicine 2000;18:261‐3. [DOI] [PubMed] [Google Scholar]
Quinn 1993
- Quinn JV, Drzewiecki A, Li MM, Stiell IG, Sutcliffe T, Elmslie TJ, et al. A randomised, controlled trial comparing a tissue adhesive with suturing in the repair of paediatric facial lacerations. Annals of Emergency Medicine 1993;22:1130‐5. [DOI] [PubMed] [Google Scholar]
Quinn 1995
- Quinn JV, Drzewiecki AE, Stiell IG, Elmslie TJ. Appearance scales to measure cosmetic outcomes of healed lacerations. American Journal of Emergency Medicine 1995;13:229‐31. [DOI] [PubMed] [Google Scholar]
Quinn 1997
- Quinn J, Wells G, Sutcliffe T. A randomized trial comparing octylcyanoacrylate tissue adhesive and sutures in the management of lacerations. JAMA 1997;277(19):1527‐30. [PubMed] [Google Scholar]
Schunemann 2011a
- Schünemann HJ, Oxman AD, Higgins JPT, Vist GE, Glasziou P, Guyatt GH. Chapter 11: Presenting results and 'Summary of findings' tables. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Schunemann 2011b
- Schünemann HJ, Oxman AD, Higgins JPT, Deeks JJ, Glasziou P, Guyatt GH. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
SIGN 2011
- Scottish Intercollegiate Guidelines Network (SIGN). Search filters. http://www.sign.ac.uk/methodology/filters.html#random 2011.