

Summary
At present, it is unclear whether eating behavior traits (EBT) predict objectively measured short‐term energy intake (EI) and longer‐term energy balance as estimated by body mass index (BMI). This systematic review examined the impact of EBT on BMI and laboratory‐based measures of EI in adults ( 18 years) in any BMI category, excluding self‐report measures of EI. Articles were searched up until 28th October 2021 using MEDLINE, PsycINFO, EMBASE and Web of Science. Sixteen EBT were identified and the association between 10 EBT, EI and BMI were assessed using a random‐effects meta‐analysis. Other EBT outcomes were synthesized qualitatively. Risk of bias was assessed with the mixed methods appraisal tool. A total of 83 studies were included (mean BMI = 25.20 kg/m2, mean age = 27 years and mean sample size = 70). Study quality was rated moderately high overall, with some concerns in sampling strategy and statistical analyses. Susceptibility to hunger (n = 6) and binge eating (n = 7) were the strongest predictors of EI. Disinhibition (n = 8) was the strongest predictor of BMI. Overall, EBT may be useful as phenotypic markers of susceptibility to overconsume or develop obesity (PROSPERO: CRD42021288694).
Keywords: eating behavior, energy intake, obesity
1. INTRODUCTION
Obesity is a common, serious, and costly condition with significant health care and societal costs. 1 There is current interest in identifying psychological and physiological markers that characterize individuals who are susceptible to weight gain. Eating behaviors influence amount and types of foods eaten and hence energy intake (EI). 2 Eating behavior traits (EBT) are considered to be reliable, acquired indices of food‐related behaviors. 3 EBT have been extensively studied in an attempt to identify potential markers that detect tendency to overconsume. 4 This has led to the development of several constructs and psychometric measures, which aim to capture important individual differences in eating behavior and disordered eating symptomology, for example, the Three Factor Eating Questionnaire (TFEQ) with sub‐scales for cognitive restraint, susceptibility to hunger and disinhibition. 5 Many EBT have been reported to be associated with excess food intake. 6 , 7 , 8 , 9 However, ‘overconsumption’ is often assessed by other self‐report measures which are prone to misreporting and not truly representative of actual food intake. 10 For example, in a systematic review on the associations between emotions and eating behavior, the majority of studies associated self‐reported emotions with another self‐reported EBT as a proxy of food intake. 11 Associations between EBT and EI have yet to be extensively reviewed and little is known about which EBTs influence objectively measured EI.
Previous systematic reviews have begun to answer these questions indirectly by examining associations between EBT and BMI. 9 , 11 , 12 BMI is an index of long‐term energy balance status. Vainik, Dagher, Dubé and Fellows 12 found that several different personality measures were consistently associated with BMI. However, very few measures included were eating‐related. French, Epstein, Jeffery, Blundell and Wardle 9 reviewed seven eating behavior dimensions and found that most of the available data showed positive cross‐sectional associations with BMI. However, very few studies reported measures of EI and only four measures were eating‐related. Overall, disinhibition had the largest empirical support to link it prospectively with weight gain and a narrative review also found that disinhibition plays a significant role in obesity, diet quality and uncontrolled eating patterns. 13 As few measures associated with psychological eating behavior have been reviewed, this systematic review aimed to assess all possible psychological EBT.
EBT are theoretical constructs operationalized through eating‐related measures. There is currently no database of EBT, and studies often refer to these traits with different names, for example, overeating measures, eating behavior dimensions, appetite measures and eating attitudes. Consequently, a conceptual diagram was developed to capture the scales used to assess EBT and to a‐priori allocate all of the collected scales to theoretical domains (see Figure 1). Firstly, a scoping exercise was conducted to create EBT domains, then subdomains were identified, which formed the basis for the search strategy. Secondly, this systematic review was conducted to identify studies that included measures of both EI and BMI in the same population. This systematic review included only laboratory‐based measures of EI. Use of a controlled environment allows for more standardized, objective measurement of EI. 14 This is more accurate and precise than self‐report EI. 15
FIGURE 1.
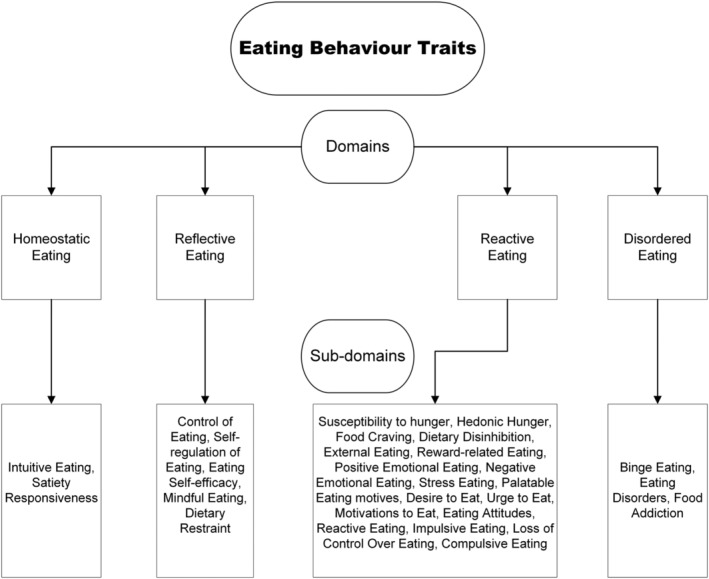
A conceptual diagram of eating behavior traits.
The primary aim of this systematic review was to examine whether EBT predicts short‐term EI and whether there is evidence that this effect translates into longer term energy balance, as estimated by BMI. The specific research questions of the review were: (1) What measures are used to capture EBT? (2) How well do these measures predict short term EI? (3) How well do these measures predict BMI? (4) Do some EBT and questionnaires used to measure EBT better predict EI or BMI than others?
2. METHODS
2.1. Information sources and search strategy
Four electronic databases were searched: MEDLINE (Ovid), PsycINFO (Ovid), EMBASE (Ovid) and Web of Science (core collection). The MEDLINE, Embase and PsychInfo strategies were run simultaneously as a multi‐file search in Ovid on 28th October 2021. Searches for all databases are included in Table S1. The conceptual diagram, alongside the identification of key databases formed the basis for the search strategy (see Figure 1). All proposed EBT and their domains were included in the search. Key databases such as the UCL database for eating behavior questionnaires, 16 NIH obesity measures, 17 and Arab psychology scales 18 were used to find relevant eating‐related questionnaires to include in the search. Because many studies use EBT but not in relation to measured eating behavior, the search also required studies to include key words related to eating behavior or eating traits (see Table S1). The two outcome measures were EI and BMI (and their related terms, see Table S1). Limits were set to include articles published in English (as translating studies into English could lead to relevant information being mistranslated) and humans. The search strategies were peer reviewed by three experts in the field (KB, JS, GF) prior to execution using the PRESS checklist. 19 Duplicates were removed using Screenatron's ‘deduplication’ tool and were checked to ensure all duplicates found were actual duplications. This systematic review followed PRISMA guidelines 20 and was pre‐registered with PROSPERO (registration number = CRD42021288694).
2.2. Study selection, inclusion, and exclusion
Articles were included if they recruited adults ( 18 years including older adults) in any BMI category. The presence of the following was not excluded: type 2 diabetes, pre‐menopausal/post‐menopausal women, cardiovascular diseases. Those with the following comorbidities were excluded: Parkinson's disease, anorexia, bulimia nervosa, binge eating disorder, cancers, inflammatory bowel diseases, intellectual deficiency, psychiatric conditions, sleep disorders, those having undergone weight loss surgery (gastric bypass or bariatric surgery) and those who were pregnant. As binge eating was identified as an EBT in the scoping exercise, any study that used a binge eating scale (e.g., binge eating scale 21 ) to classify binge eaters was included. However, if studies identified participants with binge eating disorder using a version of the DSM, for example, DSM‐5, 22 this was not recognized as an EBT and these studies were excluded. Studies that measured psychological variables, for example, stress or mood, were excluded unless an EBT was also measured, for example, emotional eating. In cases where studies measured other variables alongside EBT, the reviewers discussed whether these variables would be considered potential contaminates of the outcomes. For example, an alcohol preload or a food craving protocol were considered potential contaminates and were excluded if no data was given for a control condition. Self‐report measures of EI were excluded as this systematic review focused on laboratory‐based measures of EI but were saved for a future review. Laboratory‐based measures of EI also included studies where EI was measured in a laboratory and weighed food was given to participants to take home and bring back to be re‐weighed, as this measure of EI is considered in the literature to be ad‐libitum EI.
All titles and abstracts were assessed for eligibility by the main author (CD) and were also independently screened by three researchers (MH, JS, GF), with uncertainty regarding eligibility discussed among the researchers. Reference lists from the resulting reviews were also screened to identify additional articles. Full texts were retrieved and assessed for eligibility by CD and were also independently assessed by JS and GF. Intervention studies that included results for a control condition or baseline measures were included. Studies that only measured one of the outcomes variables (EI or BMI) were excluded. If a study measured both outcome variables but the results for one of the outcome measures was missing, the study authors were contacted for the missing outcome results. In this case, the study was included for data extraction as both outcome variables were measured. Thirty‐three authors were contacted about missing data. Five authors responded with the necessary data.
2.3. Data extraction and synthesis
Data was extracted by one author (CD) and was cross‐checked for data extraction errors by JS and GF. Data was extracted using the data collection form for intervention reviews (randomized control trials and non‐randomized control trials) from the Cochrane group. 23 The characteristics of each included article consisted of title, study ID, publication type, study design, aim of the study, ethical information, number of participants, population characteristics (age, BMI, % female, ethnicity, population description, method of recruitment, inclusion/exclusion criteria), description of EBT, description of outcomes (method, definition, unit of measurement and validation information for the collection and measurement of BMI and EI), study funding sources, possible conflicts of interests, data and analysis (results, including number of participants, means and standard deviations where possible, unit of analysis, statistical methods used and appropriateness of these), key conclusions of study authors and references to other available studies. Where means and standard deviations were not reported, correlations, F‐values or t‐values were extracted, and standard errors were converted to standard deviations. Effects on EI and BMI were examined using a random‐effects meta‐analysis because it was anticipated that there would be considerable between‐study heterogeneity. All analyses were carried out in the R environment, version 2021.09.0. 24 The following R packages were used: dmetar, 25 esc, 26 tidyverse, 27 and meta. 28
Meta‐analysis of the effect of each EBT on BMI and EI was performed when ≥2 effect sizes were available for each trait. For each analysis, effect sizes were pooled using the r value from correlations and were transformed to Fisher's Z. 29 Where correlations were not present, the available raw data were transformed into Fisher's Z. Where one study provided data for more than one questionnaire (e.g., all participants completed the DEBQ and TFEQ), the sample size was halved to prevent ‘double counting’, which can artificially inflate effect sizes and distort results. 30 , 31 If studies provided data for multiple types of EI outcome, for example, sweet, and savory EI, or provided data for multiple preloads, the selected outcomes were pooled to provide a single ‘total EI’ correlation, to prevent overpowering of a single study. Effect sizes based on Fisher's Z were interpreted as very small (≤0.05), small (>0.05–<0.10), moderate (>0.10–<0.30), large (>0.30–<0.40), and very large (≥0.40). 32 The restricted maximum likelihood estimator was used to calculate heterogeneity variance and heterogeneity was also evaluated using the I‐squared statistic (I 2), with values inferred as low (<25%), moderate (25%–75%), and high (>75%). However, the I 2 statistic was interpreted cautiously when the number of studies in each meta‐analysis was <7. In this case, it is advised that confidence intervals should supplement the I 2 statistic; therefore, confidence intervals were also provided for each meta‐analysis. 33 Knapp‐Hartung adjustments 34 were also used to calculate the confidence interval around the pooled effect. The Knapp‐Hartung adjustment can reduce the chance of false positives, especially when the number of studies is small. 35 The results of the meta‐analyses are presented as forest plots, which include the authors, standard error (SE), questionnaire type, correlation (COR), 95% confidence intervals, weight and Hedges G 36 that is converted from Fisher's Z.
Further analysis of outliers and influential cases was conducted using a leave‐one‐out analysis in addition to identifying influential cases, and results are reported for both the main meta‐analyses and further analyses where outliers or influential cases were removed. Publication bias was assessed by visually inspecting the funnel plot and Egger's regression test when the number of included studies was <10. Duval and Tweedie's trim‐and‐fill method was also used. Two subgroup analyses were conducted to test whether the effect of restraint on BMI and EI was influenced by the type of questionnaire used because the questionnaires used to measure restraint varied across studies. Additionally, a subgroup analysis tested whether the use of a preload influenced the correlation between restraint and EI. Studies were split into ‘no preload’ and ‘preload’ categories. For the preload studies, effect sizes were conducted for both no preload and preload groups, and sample size was halved to prevent double counting. 30 , 31 Where studies included multiple preload conditions, the largest preload condition was used to calculate the effect size. Subgroup analyses were also conducted to test the influence of meal type (1 test meal vs. multiple test meals) where there were ≥10 effect sizes available for each EBT and ≥2 per category.
2.4. Quality assessment
To assess risk of bias, the excel version of the mixed method appraisal tool (MMAT) for appraising studies was used. 37 It is a critical appraisal tool designed for systematic mixed studies reviews (including qualitative, quantitative, and mixed methods studies). The MMAT has been pilot tested and has high content validity. 38 The following questions were answered to determine the risk of bias: is the sampling strategy relevant to address the research question, is the sample representative of the target population, are the measurements appropriate, is the risk of nonresponse bias low and is the statistical analysis appropriate to answer the research question? The four assessment items represented flaws if answered “No/cannot tell.” It is discouraged to calculate an overall score from the ratings of each criterion; therefore, a detailed discussion of the ratings follows. Quality assessment was completed by the main reviewer (CD) and was cross‐checked by JS and GF.
3. RESULTS
2,760 articles were retrieved from the four databases. After deduplication, 1955 articles remained for title and abstract screening. The reasons for excluding any studies that did not meet the inclusion criteria during full text screening are shown in the flow diagram in Figure 2. Seventy‐seven papers met the inclusion criteria and were included in this systematic review, with some papers consisting of several studies. In total, 83 studies were included. Several studies could not be synthesized for each EBT meta‐analysis; therefore, the number of studies included in each meta‐analysis varies. Where meta‐analysis was not possible, associations between the EBT and outcome variables are qualitatively summarized. Table 1 gives the included questionnaires used to measure EBT and their abbreviations.
FIGURE 2.
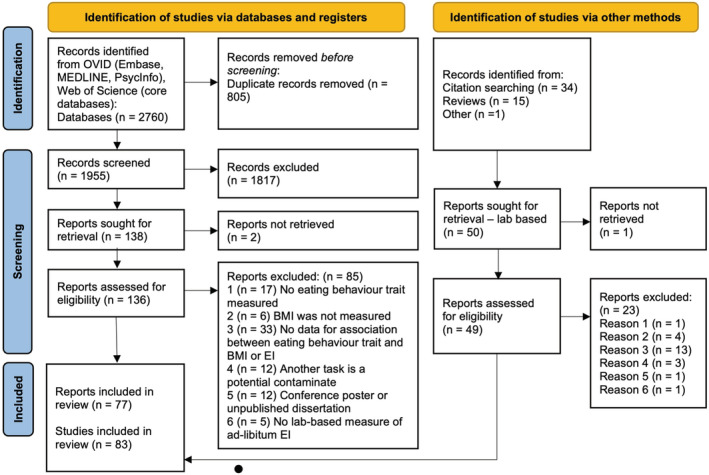
Flow diagram of study selection
TABLE 1.
Table of questionnaires included and their abbreviations
| Questionnaire | Abbreviation | Subscales | Reference paper |
|---|---|---|---|
| Intuitive Eating Scale | IES | Reliance On Hunger and Satiety (RHSC), Unlimited Permission to Eat (UPE), Eating for Physical Rather Than Emotional Reasons (EPR) | Tylka 39 |
| Intuitive Eating Scale‐2 | IES‐2 | RHSC, UPE, EPR, Body‐Food Choice Congruence (B‐FCC) | Tylka and Kroon Van Diest 40 |
| Mindful Eating Questionnaire | MEQ | Disinhibition, Awareness, External Cues, Emotional Response, Distraction | Framson, Kristal, Schenk, Littman, Zeliadt and Benitez 41 |
| Satiety Quotient | SQ | Desire To Eat, Hunger, Fullness, Satiety, Prospective Food Consumption (PFC) | Green, Delargy, Joanes and Blundell 42 |
| Adult Eating Behavior Questionnaire | AEBQ | Hunger (H), Food Responsiveness (FR), Emotional Over‐Eating (EOE), Enjoyment of Food (EF), Satiety Responsiveness (SR), Emotional Under‐Eating (EUE), Food Fussiness (FF), Slowness in Eating (SE) | Hunot, Fildes, Croker, Llewellyn, Wardle and Beeken 43 |
| Three Factor Eating Questionnaire | TFEQ | Disinhibition, Dietary Restraint, Susceptibility to Hunger | Stunkard and Messick 5 |
| Restraint Scale | RS | Herman and Mack 44 | |
| Revised Restraint Scale | RRS | Herman, Polivy and Silver 45 | |
| Dutch Eating Behavior Questionnaire | DEBQ | Restraint Eating, Emotional Eating, External Eating | van Strien, Frijters, Bergers and Defares 46 |
| Control of Eating Questionnaire | COEQ | Craving Control, Positive Mood, Craving for Sweet, Craving for Savory | Dalton, Finlayson, Blundell and Hill 47 |
| Power of Food Scale | PFS | Food Available, Food Present, Food Tasted | Lowe, Butryn, Didie, Annunziato, Thomas, Crerand, Ochner, Coletta, Bellace and Wallaert 48 |
| Food Craving Inventory | FCI | High fats, Sweets, Carbohydrates, Fast‐Food Fats and Subjective, Behavioral | White, Whisenhunt, Williamson, Greenway and Netemeyer 49 |
| Binge Eating Scale | BES | Gormally, Black, Daston and Rardin 21 | |
| Eating Disorders Examination Questionnaire | EDE‐Q | Restraint, Eating Concern, Shape Concern, Weight Concern | Fairburn, Cooper and O'Connor 50 |
| Eating Disorders Assessment Scale | EDAS | Restrained Eating, Binge Eating, Purging, Preoccupation with Body Image, and Body Weight. | Akkermann, Herik, Aluoja and Järv 51 |
| Eating Disorders Diagnostics Scale | EDDS | Anorexia Nervosa, Bulimia Nervosa, Binge Eating Disorder, Noneating Disordered | Stice, Telch and Rizvi 52 |
| Eating Disorders Inventory | EDI‐2 | EBT related subscales: Drive for Thinness, Bulimia, Body Dissatisfaction | Garner 53 |
| Eating Self‐Efficacy | WEL | Negative Emotions, Availability, Social Pressure, Physical Discomfort, Positive Activities | Clark, Abrams, Niaura, Eaton and Rossi 54 |
| Reward‐based Eating Drive Questionnaire | RED‐9, RED‐13, RED‐X5 | Loss of Control Over Eating, Lack of Satiety, Preoccupation with Food | Vainik, Eun Han, Epel, Janet Tomiyama, Dagher and Mason 55 |
| Yale Food Addiction Scale‐2 | YFAS‐2 | Gearhardt, Corbin and Brownell 56 |
3.1. Study characteristics
Study characteristics are summarized in Table 2 (see Table S2 for more detailed characteristics). The studies were published between 1975 and 2021. All data from the studies are cross‐sectional. The following EBT were identified, restraint (n = 50), disinhibition (n = 17), emotional eating (n = 12), binge eating (n = 8), external eating (n = 7), susceptibility to hunger (n = 6), hedonic hunger (n = 4), satiety responsiveness (n = 3 via Satiety Quotient, SQ) and n = 1 via AEBQ), intuitive eating (n = 3), food craving (n = 1), mindful eating (n = 1), eating disorders (n = 1), food addiction (n = 1), eating self‐efficacy (n = 1), control of eating (n = 1), reward‐related eating (n = 1). The mean (range) of the total sample size was 70 (18–273). The mean (range) age of participants was 27 years (19–59 years); BMI was 25.20 kg/m2 (21.0–36.8 kg/m2). Males and females were included in 25 studies, females only in 56 studies, males only in 1 study and no data was given for 1 study. BMI was objectively measured in 52 studies, self‐reported in 10 studies, and in 21 studies, there was no information for how BMI was measured. Measures of EI varied widely across studies. EI was measured over one test meal in 69 studies and across multiple test meals in 14 studies. Studies also used various types of food to measure EI. Overall, snack foods were the most popular EI measure (n = 29). Multiple food items (n = 21), pasta (n = 8), cookies (n = 5), ice cream (n = 5), popcorn (n = 3), sandwiches (n = 3), vending machines (n = 2), beef casserole (n = 2), risotto (n = 1), pizza (n = 1), milkshake (n = 1), Boost (a nutritionally complete liquid supplement, n = 1) and breakfast foods (n = 1) were also used.
TABLE 2.
Eating behavior traits: Summary of included studies
| Eating behavior trait | Questionnaire used to assess eating behavior trait | Cross‐sectional study reference | Associations with | |
|---|---|---|---|---|
| EI | BMI | |||
| Intuitive eating (IE) | IES | Anderson, Schaumberg, Anderson and Reilly 57 | NS and ↑ | ↓ |
| IES | Anderson, Reilly, Schaumberg, Dmochowski and Anderson 58 | NS | NS | |
| IES‐2 | Ruzanska and Warschburger 59 | NS and ↑ | ↓ | |
| Total |
3 NS 2 ↑ |
1 NS 2 ↓ |
||
| Mindful eating | MEQ | Anderson, Reilly, Schaumberg, Dmochowski and Anderson 58 | NS |
NS |
| Total | 1 NS | 1 NS | ||
| Satiety Responsiveness | SQ | Dalton, Hollingworth, Blundell and Finlayson 60 | ↓ | NS |
|
SQ desire to eat SQ for PFC SQ for fullness SQ for hunger |
Drapeau, Blundell, Therrien, Lawton, Richard and Tremblay 61 |
NS NS ↓ NS |
NS NS NS NS |
|
| SQ | Drapeau, Jacob, Panahi and Tremblay 62 | NS | NS | |
| AEBQ | Zuraikat, Roe, Smethers, Reihart and Rolls 63 | ↓ | NS* | |
| Total |
4 NS 3 ↓ |
7 NS | ||
| Dietary restraint | TFEQ | Anderson, Reilly, Schaumberg, Dmochowski and Anderson 58 | NS | ↑ |
| TFEQ | Ard, Desmond, Allison and Conway 64 | ↓ | ||
| TFEQ | Bellisle, Dalix, Airinei, Hercberg and Péneau 65 | NS | NS | |
| TFEQ | Bryant, Caudwell, Blundell, Hopkins and King 66 | NS | ||
| TFEQ | Chambers and Yeomans 67 | NS | NS | |
| RS | Coelho, Polivy, Herman and Pliner 68 | ↑ | ↑ | |
| RRS | Cools, Schotte and McNally 69 | ↓ | ||
| RS | de Witt Huberts, Evers and de Ridder 70 study 1 | NS | ↑ | |
| RS | de Witt Huberts, Evers and de Ridder 70 study 2 | NS | ↑ | |
| RS | de Witt Huberts, Evers and de Ridder 70 study 3 | NS | NS | |
| DEBQ | Dweck, Jenkins and Nolan 71 | ↑ | ||
| RRS | Fedoroff, Polivy and Herman 72 | ↓ | ||
| TFEQ | Finlayson, Blundell, Bordes, Griffioen‐Roose and de Graaf 73 | NS | NS | |
| DEBQ | Finlayson et al. 73 | NS and ↑ | ||
| RS | Guerrieri, Nederkoorn, Schrooten, Martijn and Jansen 74 | ↑ | ↑ | |
| TFEQ | Haynes, Lee and Yeomans 75 | ↓ | NS | |
| DEBQ | Herhaus and Petrowski 76 | NS | NS | |
| RS | Herman and Mack 44 | ↑ and ↓ | NS | |
| RS | Herman, Polivy and Silver 45 | ↑ | ||
| DEBQ | Higgs, Williamson and Attwood 77 | NS | NS | |
| TFEQ | Hofmann and Friese 78 | ↓ | ||
| DEBQ | Hopkins et al. 113 | ↓ | NS | |
| DEBQ | Jansen 79 study 1 | ↑ | NS | |
| Jansen 79 study 2 | ↑ | ↑ | ||
| RS | Jansen, Merckelbach, Oosterlaan, Tuiten and Van Den Hout 80 | NS | ↑ | |
| RS | Lattimore and Maxwell 81 | NS | ||
| TFEQ | Martin, Williamson, Geiselman, Walden, Smeets, Morales and Redmann Jr 82 | NS | NS | |
| TFEQ | McNeil, Lamothe, Cameron, Riou, Cadieux, Lafreniere, Goldfield, Willbond, Prud'homme and Doucet 83 | NS | ||
| RRS | Myhre, Buchwald, Kratz, Goldberg, Polivy, Melhorn, Schur and Cummings 84 | NS | NS | |
| DEBQ | Oliver, Wardle and Gibson 85 | NS | ||
| DEBQ | Ouwens, van Strien and van der Staak 86 | NS | ||
| TFEQ | Ouwens, van Strien and van der Staak 86 | NS | ||
| RS | Ouwens, van Strien and van der Staak 86 | NS | ||
| TFEQ | Peluso 87 | NS | NS | |
| TFEQ | Rideout, McLean and Barr 88 | ↓ | NS | |
| DEBQ | Robinson and Haynes 115 | NS | NS | |
| TFEQ | Rolls, Castellanos, Shide, Miller, Pelkman, Thorwart and Peters 89 | NS | NS | |
| TFEQ | Ruddock, Field and Hardman 90 | ↓ | NS | |
| TFEQ | Schoch and Raynor 91 | ↓ | ↑ | |
| RRS | Schotte, Cools and McNally 92 | NS | ↑ | |
| RS | Shapiro and Anderson 93 | NS | ||
| DEBQ | Sim, Lee and Cheon 94 | NS | ||
| TFEQ | Smith, Geiselman, Williamson, Champagne, Bray and Ryan 95 | NS | ↑ | |
| RS and TFEQ | Stice, Fisher and Lowe 96 study 1 | NS | NS | |
| TFEQ and EDEQ‐R | Stice, Fisher and Lowe 96 study 2 | NS | ||
| TFEQ | Stice, Sysko, Roberto and Allison 97 | NS | ||
| TFEQ | Stinson, Votruba, Venti, Krakoff, Gluck and Perez 98 | ↓ | NS | |
| DEBQ | van Strien and Ouwens 99 | NS | ||
| TFEQ | Visona and George 100 | NS | NS | |
| DEBQ | Wallis and Hetherington 101 | NS | NS | |
| DEBQ | Wallis and Hetherington 102 | ↓ | ↑ | |
| DEBQ | Wardle and Beales 103 | ↑ | NS | |
| TFEQ | Westenhoefer, Broeckmann, Münch and Pudel 104 | NS | ↑ | |
| RRS | Westenhoefer, Broeckmann, Münch and Pudel 104 | ↑ | ↑ | |
| TFEQ | Yeomans and Coughlan 105 | NS | NS | |
| TFEQ | Yeomans, Tovey, Tinley and Haynes 106 | NS | ||
| TFEQ | Zambrowicz, Schebendach, Sysko, Mayer, Walsh and Steinglass 107 | ↓ | ||
| EDE‐2 | Zambrowicz, Schebendach, Sysko, Mayer, Walsh and Steinglass 107 | NS | ||
| Total |
36 NS 9 ↑ 13 ↓ |
24 NS 14 ↑ |
||
| Control of eating |
COEQ Craving control Positive mood Lack of Craving for sweet a |
Dalton, Finlayson, Blundell and Hill 47 |
↓ ↓ ↓ |
↓ ↓ ↓ |
| Total | 3 ↓ | 3 ↓ | ||
| Hedonic hunger/food reward sensitivity | PFS | Appelhans, Liebman, Woolf, Pagoto, Schneider and Whited 108 | NS | NS |
| PFS | Ely, Howard and Lowe 109 | NS and ↑ | ↑ | |
| PFS | Finlayson et al. 73 | NS | NS | |
| PFS | Nolan‐Poupart, Veldhuizen, Geha and Small 110 | NS | ||
| Total |
4 NS 1 ↑ |
2 NS 1 ↑ |
||
| Food craving | FCI | Martin, O'Neil, Tollefson, Greenway and White 111 | ↑ | |
| Total | 1 ↑ | |||
| Dietary disinhibition | TFEQ | Ard, Desmond, Allison and Conway 64 | NS | |
| TFEQ | Bryant, Caudwell, Blundell, Hopkins and King 66 | NS | ||
| TFEQ | Chambers and Yeomans 67 | NS and ↑ | ||
| TFEQ | Epstein, Lin, Carr and Fletcher 112 | ↑ | ↑ | |
| TFEQ | Finlayson, Blundell, Bordes, Griffioen‐Roose and de Graaf 73 | NS and ↑ | ↑ | |
| TFEQ | Haynes, Lee and Yeomans 75 | ↑ | NS | |
| TFEQ | Higgs, Williamson and Attwood 77 | NS | NS | |
| TFEQ | Martin, Williamson, Geiselman, Walden, Smeets, Morales and Redmann Jr 82 | NS | ||
| TFEQ | McNeil, Lamothe, Cameron, Riou, Cadieux, Lafreniere, Goldfield, Willbond, Prud'homme and Doucet 83 | NS | ||
| DEBQ | Ouwens, van Strien and van der Staak 86 | ↑ | ||
| TFEQ | Ouwens, van Strien and van der Staak 86 | ↑ | ||
| TFEQ | Ruddock, Field and Hardman 90 | ↑ | NS | |
| TFEQ | Smith, Geiselman, Williamson, Champagne, Bray and Ryan 95 | ↑ | ↑ | |
| TFEQ | Stinson, Votruba, Venti, Krakoff, Gluck and Perez 98 | NS | ↑ | |
| TFEQ | Westenhoefer, Broeckmann, Münch and Pudel 104 | ↑ | ↑ | |
| TFEQ | Yeomans and Coughlan 105 | NS | ↑ | |
| TFEQ | Yeomans, Tovey, Tinley and Haynes 106 | ↑ | ↑ | |
| TFEQ | Zambrowicz, Schebendach, Sysko, Mayer, Walsh and Steinglass 107 | NS | ||
| Total |
9 NS 10 ↑ |
4 NS 7 ↑ |
||
| Susceptibility to Hunger | TFEQ | Bryant, Caudwell, Blundell, Hopkins and King 66 | ↑ | |
| TFEQ | Finlayson, Blundell, Bordes, Griffioen‐Roose and de Graaf 73 | NS | NS | |
| TFEQ | McNeil, Lamothe, Cameron, Riou, Cadieux, Lafreniere, Goldfield, Willbond, Prud'homme and Doucet 83 | ↑ | ||
| TFEQ | Stinson, Votruba, Venti, Krakoff, Gluck and Perez 98 | NS | ↑ | |
| TFEQ | Westenhoefer, Broeckmann, Münch and Pudel 104 | ↑ | ↑ | |
| TFEQ | Zambrowicz, Schebendach, Sysko, Mayer, Walsh and Steinglass 107 | NS | ||
| Total |
3 NS 3 ↑ |
1 NS 2 ↑ |
||
| External eating | DEBQ | Dweck, Jenkins and Nolan 71 | NS | |
| DEBQ | Finlayson et al. 73 | ↑ | NS | |
| DEBQ | Hopkins, Michalowska, Whybrow, Horgan and Stubbs 113 | NS | NS | |
| DEBQ | Kakoschke, Kemps and Tiggemann 114 | ↑ | ||
| DEBQ | Robinson and Haynes 115 | NS | NS | |
| DEBQ | van Strien, Donker and Ouwens 116 | ↑ | ||
| DEBQ | van Strien and Ouwens 99 | NS | ||
| Total |
3 NS 3 ↑ |
4 NS | ||
| Emotional eating | DEBQ | Dweck, Jenkins and Nolan 71 | NS | NS |
| DEBQ | Evers, de Ridder and Adriaanse 117 study 3 | NS | NS | |
| DEBQ | Evers, de Ridder and Adriaanse 117 study 4 | NS | NS | |
| DEBQ | Evers, de Ridder and Adriaanse 117 study 5 | NS | NS | |
| DEBQ | Finlayson et al. 73 | NS and ↑ | ↑ | |
| DEBQ | Hopkins, Michalowska, Whybrow, Horgan and Stubbs 113 | NS | NS | |
| DEBQ | Oliver, Wardle and Gibson 85 | NS | ||
| DEBQ | Raspopow, Abizaid, Matheson and Anisman 118 | NS | NS* | |
| DEBQ | Robinson and Haynes 115 | NS | NS | |
| DEBQ | van Strien, Donker and Ouwens 116 | ↑ | ||
| DEBQ | van Strien, Herman, Anschutz, Engels and de Weerth 119 | ↑ | ||
| DEBQ | van Strien and Ouwens 99 | ↑ | ||
| DEBQ | Wallis and Hetherington 101 | NS | NS | |
| DEBQ | Wallis and Hetherington 102 | NS | ||
| Total |
10 NS 3 ↑ |
9 NS 2 ↑ |
||
| Binge eating | BES | Alger, Seagle and Ravussin 120 | ||
| EDAS | Arumae, Kreegipuu and Vainik 121 | ↑ | NS | |
| BES | Dalton, Blundell and Finlayson 122 | ↑ | NS* | |
| BES | Dalton, Blundell and Finlayson 123 | ↑ | NS* | |
| BES | Finlayson, Arlotti, Dalton, King and Blundell 4 | ↑ | ↑ | |
| BES | Finlayson et al. 73 | NS | ↑ | |
| BES | Nasser, Gluck and Geliebter 124 | NS | NS | |
| BES | Stinson, Votruba, Venti, Krakoff, Gluck and Perez 98 | NS | ↑ | |
| Total |
3 NS 4 ↑ |
4 NS 3 ↑ |
||
| Eating disorders | EDDS | Anderson, Reilly, Schaumberg, Dmochowski and Anderson 58 | NS | ↑ |
| EDI‐2 | Long, Meyer, Leung and Wallis 125 | NS | ||
| Total | 2 NS | 1 ↑ | ||
| Food addiction | YFAS 2.0 | Schulte, Sonneville and Gearhardt 126 | NS | NS |
| Total | 1 NS | 1 NS | ||
| Eating self‐efficacy | WEL | Vijayvargiya, Chedid, Wang, Atieh, Maselli, Burton, Clark, Acosta and Camilleri 127 | ↓ | |
| Total | 1 ↓ | |||
| Reward‐related eating |
RED‐X5 RED‐9 RED‐13 |
Vainik, Eun Han, Epel, Janet Tomiyama, Dagher and Mason 55 Total |
↑ 1 ↑ |
↑ 1 ↑ |
| Total scores | TFEQ | Bellisle and Dalix 128 | NS | NS |
| DEBQ | Bellisle and Dalix 128 | NS | NS | |
| TFEQ | Nolan‐Poupart, Veldhuizen, Geha and Small 110 | NS | ||
| Total | 3 NS | 2 NS | ||
Note: blank = outcome was measured but the data was not available as authors were contacted but did not reply, NS = non‐significant, NS* = significant association with body fat or body weight, ↑ = significance positive association, ↓ = significant negative association,
= reverse coded. If two results are presented for one outcome (e.g., NS and ↑), the effect differed depending on the group or condition tested.
3.2. Study quality
Overall, studies scored relatively high on study quality for four out of five quality criteria. Studies scored low for sampling strategies because none used probability sampling and most recruited via opportunity sampling. Studies did define their target population by presenting inclusion and exclusion criteria, and some included a‐priori sample size calculations. Respondents and the target population were well matched and the reasons why certain individuals were excluded were made clear. All questionnaires have been validated and in 51 studies, BMI was measured objectively in the laboratory. The measurements of EI were, for most studies, not previously validated and the most frequently used type of food was snacks (n = 28). The extent to which findings of eating behavior, using energy dense snacks can generalize to wider and more typical eating behavior is unknown. The majority of studies also attempted to reduce possible confounders by providing participants with a standardized breakfast, testing during normal lunch hours and keeping testing times between participants consistent.
The risk of non‐response bias in studies included in this systematic review was low, no studies reported high drop‐out rates. Lastly, study quality was high for the appropriateness of statistical analysis used in studies. However, in some studies, the method used to split participants into groups was a limitation. Using a median split to identify low or high scorers could have misclassified individuals and lead to null findings. 11 Indeed, van Strien, Herman, Anschutz, Engels and de Weerth 119 found that if a median split was used, their results would have become non‐significant. Additionally, in Dalton, Hollingworth, Blundell and Finlayson, 60 40% of the participants were unclassified based on their SQ score. Therefore, any findings cannot be generalized to a wider population if almost half of the sample could not be classified into a level of satiety responsiveness.
3.3. Study findings
3.3.1. Intuitive eating
A meta‐analysis of 2 studies (n = 262) found no significant correlation between intuitive eating and EI (r = 0.32 [−0.30, 2.00], p = 0.096). A meta‐analysis of 3 studies (n = 317) found that intuitive eating was negatively correlated with BMI (r = −0.26 [−0.45, −0.04], p = 0.036, Figure S1) and this represents a moderate effect size. Heterogeneity was low (I 2 = 0.0%, Q = 1.66, p = 0.436). One study was identified as an influential case. 57 With this study removed from the meta‐analysis, the overall effect size increased; however, the effect became non‐significant (r = −0.30 [−0.86, 0.58], p = 0.156). The trim‐and‐fill method suggested no missing studies.
3.3.2. Mindful eating
Anderson, Reilly, Schaumberg, Dmochowski and Anderson 58 found no significant association between mindful eating and EI (r = 0.15) or mindful eating and BMI (r = 0.01).
3.3.3. Satiety responsiveness
Only one effect size was available; therefore, meta‐analysis could not be conducted. However, of the four studies that measured satiety responsiveness, three reported that higher satiety responsiveness as associated with reduced EI 60 , 62 , 63 and one reported no significant effect. 62 A meta‐analysis of 3 studies (n = 197) found a moderate negative correlation between satiety responsiveness and BMI (r = −0.18 [−0.31, −0.04], p = 0.031, Figure S2). Heterogeneity was low (I 2 = 0.0%, Q = 0.41, p = 0.815). No studies were identified as outliers or influential cases. Two missing studies were suggested to the right (adjusted r = −0.15 [−0.24, −0.06], p = 0.009).
3.3.4. Restraint
Meta‐analysis of 49 studies (n = 2,594) showed a small but significant, negative correlation between restraint and EI (52 study arms, r = −0.07, [−0.12, −0.01], p = 0.015, Figure 3). Heterogeneity was moderate (I 2 = 41.8%, Q = 87.70, p = 0.001). Four outliers were identified 68 , 74 , 78 , 79 and the one‐study‐removed procedure identified one influential case. 74 With these outliers removed, the effect size slightly increased (r = −0.09 [−0.14, −0.05], p < 0.001). Heterogeneity was low (I 2 = 10.2%) and the Q test was non‐significant (Q = 52.32, p = 0.275). The funnel plot did not suggest any evidence of publication bias (Figure S3), no missing studies were suggested, and Egger's test was non‐significant (p = 0.680). The association between restraint and EI was influenced by the type of questionnaire used to measure restraint (p < 0.001, Table S3). For the TFEQ, RRS and EDE‐Q, restraint was negatively correlated with EI. Whereas, for the RS and DEBQ, restraint was positively correlated with EI. A random‐effects meta‐regression was undertaken to test for differences in effect sizes between questionnaires used to measure restraint and EI. The meta‐regression was significant (p < 0.05); however, TFEQ was the only variable that was significantly associated with EI (p < 0.01). Further subgroup analyses revealed that the effect of restraint on EI was not significantly influenced by the number of test meals (one vs. multiple test meals, p = 0.103) or BMI group (healthy, overweight, obese, p = 0.553). Lastly, the association between restraint and EI was influenced by a preload. Consuming a preload was associated with increased EI, while not consuming a preload was associated with decreased EI (p = 0.040, see Table S4).
FIGURE 3.
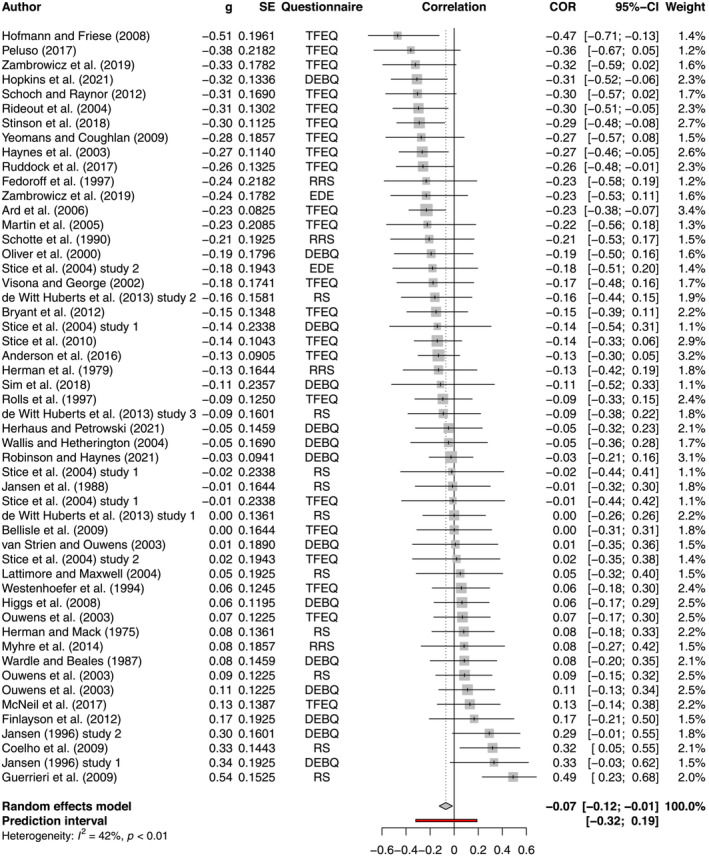
Forest plot of the effect of restraint on EI
Meta‐analysis of 32 studies (n = 1869) showed that restraint was positively correlated with BMI, and this effect was moderate (r = 0.20 [0.12, 0.28], p < 0.001, Figure 4). Heterogeneity was moderate (I 2 = 61.2%, Q = 79.86, p < 0.001). Four outliers were identified. 58 , 79 , 89 , 100 Without these studies included, there was no change in the overall effect size (r = 0.20 [0.13, 0.26], p < 0.001). However, heterogeneity decreased (I 2 = 34.8%, Q = 41.38, p = 0.038). Using the leave‐one‐out method, no studies were identified as influential. The funnel plot (Figure S4) suggested little evidence of publication bias, no missing studies were identified, and Egger's test was non‐significant (p = 0.753). The effect of restraint on BMI did not depend on the type of questionnaire used to measure restraint (p = 0.103).
FIGURE 4.
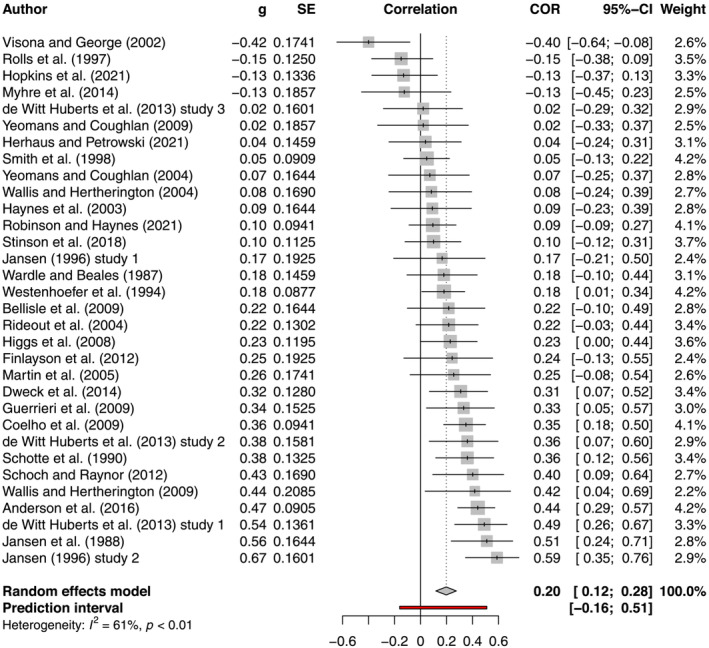
Forest plot of the effect of restraint on BMI
3.3.5. Control of eating
Dalton, Finlayson, Blundell and Hill 47 found that craving control and positive mood were negatively associated with EI (r = −0.20, p < 0.05, r = −0.21, p < 0.05) and BMI (r = −0.31, p < 0.001, r = −0.23, p < 0.01) respectively, whereas craving for sweet foods was positively associated with EI (r = 0.40, p < 0.001) and BMI (r = 0.23, p < 0.01).
3.3.6. Hedonic hunger
A meta‐analysis of 4 studies (n = 183) found no significant correlation between hedonic hunger and EI (r = 0.13 [−0.08, 0.33], p = 0.147). Additionally, a meta‐analysis of 2 studies (n = 92) also found a non‐significant association between hedonic hunger and BMI (r = 0.05 [−1.00, 1.00], p = 0.868).
3.3.7. Food craving
Martin et al. 111 reported that scores on the FCI were associated with increased total EI (r = 0.22, p < 0.05); however, there was no data for the effect of FCI on BMI.
3.3.8. Susceptibility to hunger
A meta‐analysis of 6 studies (n = 362) found susceptibility to hunger was positively associated with EI, and this effect was moderate‐to‐large (r = 0.27 [0.19, 0.35], p < 0.001, see Figure S5). Heterogeneity was low (I 2 = 0.0%, Q = 2.05, p = 0.843). No outliers or influential cases were identified. Three missing studies were identified to the left (adjusted r = 0.22 [0.13, 0.31], p < 0.001). A meta‐analysis of 3 studies (n = 245) found a moderate positive correlation between susceptibility to hunger and BMI (r = 0.20 [0.11, 0.28], p = 0.011; Figure S6). Heterogeneity was small (I 2 = 0.0%, Q = 0.20, p = 0.903). No outliers or influential cases were identified. Two missing studies were identified to the left (adjusted r = 0.17 [0.11, 0.23], p = 0.002).
3.3.9. External eating
A meta‐analysis of 6 studies (n = 583) found that external eating was positively correlated with EI, and this effect was moderate (r = 0.17 [0.07, 0.27], p = 0.007, see Figure S7). Heterogeneity was low (I 2 = 0.0%, Q = 4.46, p = 0.485). Two influential studies were identified. 115 , 116 With these studies removed, the effect size slightly increased (r = 0.18 [0.01, 0.34], p = 0.044). Heterogeneity was low (I 2 = 0.0%, Q = 2.21, p = 0.531). One missing study was identified to the left (adjusted r = 0.16 [0.06, 0.26], p = 0.008). A meta‐analysis of 4 studies (n = 269) found no significant correlation between external eating and BMI (r = −0.08 [−0.28, 0.12], p = 0.285).
3.3.10. Emotional eating
A meta‐analysis of 10 studies (n = 608) found a small‐to‐moderate, positive correlation between emotional eating and EI (r = 0.12 [0.00, 0.24], p = 0.042, see Figure S8). Heterogeneity was moderate (I 2 = 32.1%, Q = 13.26, p = 0.151). No influential studies were identified. The funnel plot did not suggest any publication bias (Figure S9), one missing study was identified to the left (adjusted r = 0.11 [−0.02, 0.23], p = 0.088) and the Egger's regression test was non‐significant (p = 0.800). The effect of emotional eating on EI was not influenced by the number of test meals (p = 0.342). A meta‐analysis of 10 studies (n = 737) found that emotional eating was positively correlated with BMI (r = 0.19 [0.13, 0.25] p < 0.001). This effect was moderate (Figure S10). Heterogeneity was low (I 2 = 0.0%, Q = 5.17, p = 0.819). No influential cases were identified. The funnel plot did not suggest any publication bias (Figure S11), No missing studies were suggested, and the Egger's test was non‐significant (p = 0.860).
3.3.11. Disinhibition
A meta‐analysis of 14 studies (n = 1,172) found a moderate positive correlation between disinhibition and EI (r = 0.19 [0.14, 0.24], p < 0.001, see Figure S12). Heterogeneity was low (I 2 = 0.0%, Q = 9.74, p = 0.715). Influence diagnostics identified one influential case. 112 With this study removed, the overall effect size increased (r = 0.21 [0.14, 0.27], p < 0.001). Heterogeneity was low (I 2 = 0.0%, Q = 8.88, p = 0.713). The funnel plot showed little evidence of publication bias (Figure S13), one missing study was suggested to the right (adjusted r = 0.20 [0.14, 0.25], p < 0.001), and Egger's test was non‐significant (p = 0.973). The effect of disinhibition on EI was not influenced by the number of test meals (p = 0.341). Meta‐analysis of 8 studies (n = 618) showed a moderate‐to‐large, positive correlation between disinhibition and BMI (r = 0.28 [0.19, 0.38], p < 0.001, Figure S14). Heterogeneity was low (I 2 = 13.8%, Q = 8.12, p = 0.322). One influential case was identified. 95 Without this study included, there was a small decrease in the overall effect size (r = 0.25 [0.16, 0.33], p < 0.001). Heterogeneity was low (I 2 = 0.0%, Q = 3.68, p = 0.720). No missing studies were suggested.
3.3.12. Binge eating
A meta‐analysis of 7 studies (n = 249) found a moderate, positive correlation between binge eating and EI (r = 0.26 [0.08, 0.43], p < 0.001, see Figure S15). Heterogeneity was low (I 2 = 0.0%, Q = 3.68, p = 0.720). Two influential studies were identified. 98 , 123 With these studies removed, the overall effect size increased slightly (r = 0.28 [0.11, 0.43], p = 0.010). Heterogeneity was low (I 2 = 0.0%, Q = 2.02, p = 0.731). Two missing studies were suggested to the left (adjusted r = 0.17 [−0.04, 0.37], p = 0.098). A meta‐analysis of 7 studies (n = 277) found a moderate positive correlation between binge eating and BMI (r = 0.21 [0.07, 0.34], p = 0.011, see Figure S16). Heterogeneity was low (I 2 = 0.0%, Q = 5.30, p = 0.506). No influential studies were identified. One missing study was identified to the right (adjusted r = 0.23 [0.09, 0.36], p = 0.006).
3.3.13. Disordered eating
A meta‐analysis of 2 studies (n = 152) was conducted to test the correlation between eating disorder symptomology and EI. The analysis was non‐significant (r = −0.17 [−0.98, 0.96], p = 0.499).
Only one effect size was available to test the effect of eating disorders on BMI; therefore, a meta‐analysis could not be conducted. However, Anderson, Reilly, Schaumberg, Dmochowski and Anderson 58 did report that increased scores on the EDDS were associated with increased BMI (r = 0.40, p < 0.05). The YFAS 2.0 was not significantly associated with EI or BMI. 126
3.3.14. Other EBT
Eating self‐efficacy was negatively associated with EI (r = −0.26, p < 0.05). 127 Three measures of reward‐related eating were positively correlated with EI (RED‐X5: r = 0.31, p < 0.05, RED‐9: r = 0.35, p < 0.05, RED‐13: r = 0.32, p < 0.05) and BMI (RED‐X5: r = 0.18, p < 0.05, RED‐9: 0.17, p < 0.06, RED‐13: r = 0.18, p < 0.05).
3.3.15. Summary of meta‐analyses findings
Figure 5 displays the overall effect sizes for each EBT on EI and BMI. A positive effect size indicates that the EBT is positively correlated with EI or BMI. A negative effect size indicates that the EBT is negatively correlated with EI or BMI. Intuitive eating and eating disorder symptomology are not displayed in Figure 5 due to the small number of studies included in these meta‐analyses and the large variability in their correlations with EI and BMI. Figure 6 displays the effect sizes for the subgroup analysis testing the correlation between restraint and EI influenced by the questionnaire used to measure restraint. Error bars in both figures reflect standard error.
FIGURE 5.
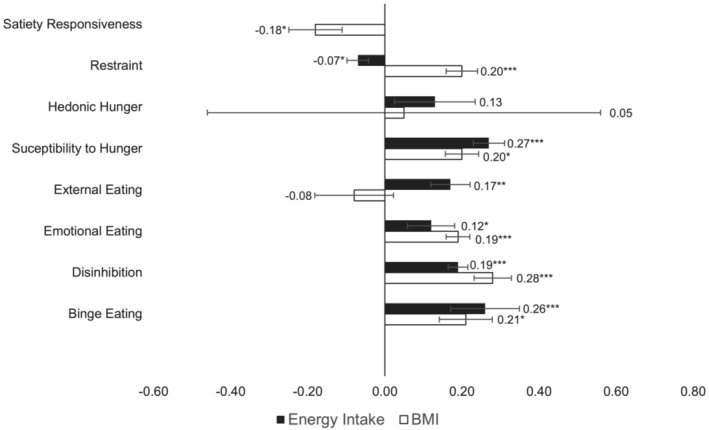
Summary of meta‐analyses findings. Note: black line = Energy Intake, white line with black border = BMI, error bars indicate standard error, *p < 0.05, **p < 0.01, ***p < 0.001.
FIGURE 6.
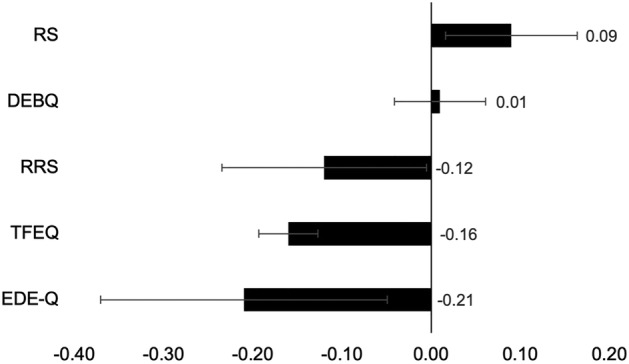
Bar graph of the subgroup analysis results, testing the correlation between restraint and EI influenced by the questionnaire used to measure restraint
4. DISCUSSION
The aims of this systematic review and meta‐analyses were to (1) identify which measures are used to capture EBT, (2) assess how well these measures associate with short term EI and (3), BMI, (4) and evaluate whether some EBT and questionnaires used to measure EBT are better at predicting EI or BMI than others. Sixteen EBT were identified. However, the majority of EBT included were restraint, disinhibition, emotional eating, external eating, and binge eating. Considering the >45 years of research on human eating behavior, this systematic review demonstrates that relatively few studies on EBT have been conducted in relation to indices of objectively measured short‐term EI as well as long‐term energy balance status (BMI). For most of the EBT identified (aside from restraint), this research has been accomplished in only a small number of studies. Additionally, the majority of traits were measured using a single questionnaire (see Table 1), which were often older measures such as TFEQ or RS. This means that there are additional, typically newer questionnaires with no research that met the inclusion criteria for this systematic review, for example, the Positive and Negative Emotional Eating Scale. 129 Future research should assess the validity of these traits in relation to EI and BMI.
Overall, the meta‐analyses demonstrated that EBT do significantly predict both EI and BMI. Effect sizes were generally moderate, with some analyses reaching larger effects. Susceptibility to hunger and binge eating were the strongest predictors of EI, whereas disinhibition was the strongest predictor of BMI. Although intuitive eating was moderately correlated with BMI, this meta‐analysis was based on a very small number of studies. If there are not at least two adequately powered studies per meta‐analysis, there may not be enough information to contribute an accurate conclusion of evidence about that EBT. 130 Therefore, drawing conclusions about intuitive eating and satiety responsiveness requires caution. Below, the main outcomes of the systematic review are discussed.
4.1. Restraint
Restraint as a concept relates to a cognitive intention to restrict food intake, which is not necessarily reflected in actual reduction in EI or adherence to a weight reducing diet. 103 This meta‐analysis found a positive association between restraint and BMI, which is consistent with previous cross‐sectional studies. 131 , 132 However, negative findings between restraint and BMI have also emerged in the literature. 133 The finding of this systematic review could suggest that although restrained individuals attempt to restrict their food intake, increased restraint puts them at a higher risk of overeating (disinhibition), leading to a positive energy balance and consequently an increased BMI. However, the results of this systematic review do not agree with this prediction. Increased restraint was associated with decreased short‐term EI. This finding is more consistent with the interpretation that people with a higher BMI invoke strategies of dietary restraint to manage their weight. Approximately 40% of the adult population report at least one weight management attempt in the preceding 12 months. 134 It is also evident from the weight management literature that the majority of weight management attempts have limited success and are subject to weight regain. 135
Previous literature examining associations between restraint and EI have also been inconsistent, which is demonstrated in this systematic review as both positive and negative associations were found between restraint and EI. Research has highlighted that the different measures used to assess restraint could be influencing the different outcomes (research question 4). Heatherton, Herman, Polivy, King and McGree 136 suggest that the TFEQ may be better able to identify individuals who are successful in restricting their food intake, whereas the RS is better able to identify individuals who are unsuccessful in dieting. Indeed, the subgroup analysis found a significant effect of questionnaire type, such that the TFEQ was associated with decreased EI, whereas the RS was associated with increased EI (see Appendix). The EDE‐Q and TFEQ had the largest effect size therefore suggesting these measures may be better at predicting EI. This analysis suggests that each questionnaire may not be measuring exactly the same construct and generates questions about which scale is best at measuring restraint. The RS, for example, could be contaminated by other constructs such as disinhibition, as items on this scale refer to overeating, for example, “Do you have feelings of guilt after overeating?” This may explain why the RS was positively associated with EI. 103 Moreover, there is also a potential need to re‐evaluate what is meant by the construct of restraint. Is restraint a measure of concern controlling intake and its consequences, or could it be a measure of motivation or success in restraining intake like the TFEQ appears to measure or perhaps a combination of these considerations? There is a need to clearly define and achieve consensus about what restraint is and what it is not.
A prediction of restraint theory is that the likelihood of a binge/overeating episode should be increased after consuming a preload only in high restraint individuals. This is because dieters who have just broken their diet are predicted to subsequently overeat. 103 , 137 In the current analysis, the correlation between restraint and EI was influenced by a preload such that the use of a preload was associated with increased EI, whereas no preload was associated with decreased EI (see Supporting Information). Nevertheless, Ouwens, van Strien and van der Staak 86 reported no significant effect of restraint on EI influenced by a preload. The researchers highlight that not all dieters will show this disinhibition effect; but a particular subgroup might. Restrained eaters can therefore be split into two subpopulations: successful dieters and unsuccessful dieters. Successful dieters are characterized by high restraint and low levels of tendency toward overeating. Unsuccessful dieters are characterized by high restraint and are prone to overeating, meaning they are more likely to show a disinhibition effect after a preload. Westenhoefer, Broeckmann, Münch and Pudel 104 provided evidence for this idea and found that overeating only occurred in participants who displayed high scores on both restraint and disinhibition, as measured by the TFEQ.
More recent research such as Bryant, Caudwell, Blundell, Hopkins and King 66 and Chambers and Yeomans 67 have tested this effect by splitting participants into four groups based on their restraint (high vs. low; HR vs. LR) and disinhibition (high vs. low; HD vs. LD) scores using the TFEQ (HD/HR, HD/LR, LD/HR, LD/LR). A limitation of the current systematic review is that effect sizes were pooled so that high restraint included high and low disinhibition and low restraint included both high and low disinhibition. By not keeping the four groups separate, the analysis may have been insensitive to the effects of differing disinhibition levels. Consequently, future research could conduct a multi‐level meta‐analysis of restraint on EI, which can account for the influence of other variables such as disinhibition and emotional eating. Based on these findings, one must consider that restraint itself may not be a homogenous construct. Westenhoefer, Broeckmann, Münch and Pudel 104 proposed that restraint can be split into rigid and flexible control, with rigid control relating to an all‐or‐nothing approach. In contrast, flexible control reflects a less stringent approach to restriction of intake. These subscales could reflect successful and unsuccessful dieters and may better account for the differing effects of restraint on EI. Unfortunately, only two studies in this review 66 , 104 split restraint into flexible and rigid control and therefore testing the validity of this concept is currently not possible. Overall, this systematic raises questions about the current definition of restraint and whether it should be altered. If restraint is associated with increased BMI, then attempting to restrain intake as a dietary approach to weight loss may not be effective and other approaches should be utilized.
4.2. Emotional eating
Another interesting finding of this systematic review was that emotional eating was positively correlated with short term EI and BMI, although there were two studies in the meta‐analysis that found a negative correlation between emotional eating and EI. 71 , 101 The small‐to‐moderate effect size could have been influenced by the inclusion of only control conditions in this systematic review. Conditions that attempted to influence the emotional state of participants were excluded to reduce potential contaminates of the specific emotional eating trait effect. However, studies have shown that emotional eaters increased their food intake after a negative mood induction, compared with a neutral or positive mood induction. 119 , 138 A limitation of this systematic review was that only one study presented data for the positive and negative subscales of emotional eating, 116 and therefore the influence of positive or negative emotional eating could not be assessed. Further research should look to test systematically whether emotion valence, as well as emotion induction conditions increase EI in high emotional eaters versus low emotional eaters.
4.3. Disinhibition
The overall finding that disinhibition was positively associated with short‐term EI and BMI supports previous research 6 , 9 and suggests that associations between uncontrolled eating and food intake are more consistently measured by scales capturing disinhibition, potentially because disinhibition is a ‘pure’ measure of uncontrolled eating. These findings suggest that increased disinhibition is an indicator of risk for potential weight gain and could be targeted in weight loss interventions characterize participants at risk of weight regain. Disinhibition could influence weight regain 139 and research has found that participants who maintained weight loss were characterized by lower disinhibition scores. 140 Niemeier, Phelan, Fava and Wing 141 found that higher internal disinhibition predicted less successful weight loss and studies have consistently shown that successful weight loss is associated with a decrease in disinhibition. 142 , 143 , 144 If weight loss interventions can successfully target and reduce participants' uncontrolled eating behavior (disinhibition), this approach may improve weight outcomes.
Furthermore, binge eating and susceptibility to hunger were also consistent predictors of EI and BMI and may be useful constructs to target in weight loss interventions. Assessing whether other traits are associated with behavior change is another important direction for future research. For example, studies have found that higher baseline emotional eating was associated with more weight gain over time, 145 meaning emotional eating could also be targeted in weight loss interventions. Mindfulness‐based interventions have also been used to help participants decrease their tendency to eat in response to negative emotions. 146 Future research should assess which traits are prospectively associated with weight change or weight maintenance, as well as investigating the long‐term efficacy of interventions utilizing EBT. Ultimately, disinhibition is a robust EBT that should be used in weight loss interventions and further research should strive to find ways to reduce levels of disinhibition in those scoring high on this subscale.
4.4. Methodological comments
This systematic review included only laboratory‐based measures of EI because there is substantial evidence that self‐report measures are susceptible to misreporting. 10 However, laboratory‐based measures of EI are highly susceptible to experimental design and demand characteristics. For example, Long, Meyer, Leung and Wallis 125 highlight that eating in a laboratory is an unnaturalistic setting and could distract and impede a participant's focus on internal signals of hunger and satiety, which could influence their EI. Another concern relates to how well one single eating episode can generalize to usual eating behavior. 59 Snacking once in a test meal (often involving unusual foods) may not be an accurate reflection on a participants normal EI. Fourteen studies did test EI over multiple test meals, which helps to reduce this limitation. However, there were still 68 studies that tested a single eating episode and therefore, multiple test meal methods are not commonplace in eating behavior research. There are also issues relating to the ‘observer effect’, whereby participants behavior is biased by the awareness that they are being observed and that they are participating in a food‐related study. 147 Studies rarely attempt to disguise that a meal is being used to measure food consumption and this transparency may alter the way a participant eats. 14 Laboratory measures of food intake may have limited generalizability to normal every day eating behavior. However, the current meta‐analyses generalize over multiple test designs and test meals which helps to overcome the role of specific research designs.
Another limitation of many studies included in this systematic review is the potential for other variables measured to contaminate the EI outcome. Although studies that included potential contaminates were excluded, there were still some tasks which may have influenced the outcomes. For example, Coelho, Polivy, Herman and Pliner, 68 included a control condition that required participants to complete an arithmetic problem‐solving task and a word‐recall task. The researchers found that the participants could not complete the test within the time provided and could have exposed the participants to task failure or ego threat which may have affected the participant mood/emotions.
4.5. Conceptual comments
An important consideration of EBT is uncertainty over the extent to which individuals are capable of accurately assessing their own eating behavior, for example, emotional eating. Evers, de Ridder and Adriaanse 117 suggests a ‘triple recall bias’, whereby people are generally unable to perceive their own behavior, they underreport their EI and personality disturbances, and retrospective emotional ratings are known to be highly sensitive to recall bias. Consequently, questionnaires that measure emotional eating are asking participants to recall their negative or positive emotions, food intake and association between both, all three of which may be biased. It is therefore possible that in some populations, for example, the elderly and young children, recall methods may not yield accurate findings and as such, should not be used. However, recommendations for specific population where EBT assessments should not be measured is beyond the scope of this analysis. The triple recall bias can also be extended to other psychological EBT, which raises concerns over their construct validity and questions whether EBT measuring what they were designed to measure? Interestingly, new developments in real time digital tracking of energy balance behaviors, 148 , 149 , 150 , 151 , 152 digital ecological momentary assessments and mobile video recording 153 could be a new avenue for more ecological assessments of EI to capture EBT.
Most studies test the validity of EBT against very short‐term EI, often over one test day. In order to relate EBT to long‐term outcomes, EI and BMI need to be measured longitudinally. This also holds true for studies that aim to assess how EBT change in weight management interventions. In the short term, EBT are not expected to change because they are long‐term processes. Therefore, to examine how EBT are associated with behavior change, they also need to be measured over a longer period of time.
5. CONCLUSIONS
The outcome of this review has demonstrated that many EBT are associated with short‐term EI and BMI, with disinhibition, susceptibility to hunger and binge eating having the largest effect sizes for EI and BMI. These findings highlight the potential use of these EBT as phenotypic markers of susceptibility to overconsume, develop obesity, or to influence outcomes in weight management interventions. Dietary restraint is evidently a complex construct and further research with preload conditions and separate subscales are needed to fully understand its effect on EI. The effect of emotional eating may have been limited by not including mood or stress induction conditions. However, this review still indicates it plays a role in EI and BMI. Importantly, there are methodological and conceptual issues with EBT that need to be stressed when utilizing these traits in eating behavior research. This does not mean they should not be used but a greater focus on objective indices of what such traits should predict (food intake and EI, BMI or weight change) might improve their use in explaining eating behavior and energy balance in the wider population.
CONFLICTS OF INTEREST
Pr. James Stubbs consults for Slimming World UK through The University of Leeds. Slimming World was not involved in the analysis or interpretation of this review.
AUTHOR CONTRIBUTIONS
CD, JS, GF, and MH performed the literature search, study selection, data extraction, and quality assessment. CD performed the meta‐analysis and drafted the manuscript. All authors critically revised the manuscript.
Supporting information
Table S1: Search strategy.
Table S2: Characteristics of included studies.
Table S3: Results of the subgroup‐meta‐analysis for the effect of restraint on EI, influenced by questionnaire type.
Table S4: Results of a subgroup meta‐analysis on the effects of restraint on EI influenced by a preload.
Figure S1. Forest plot of the effect of IES on BMI.
Figure S2. Forest plot of the effect of satiety responsiveness on BMI.
Figure S3: Funnel plot of the effect of restraint on EI.
Figure S4: Funnel plot of the effect of restraint on BMI.
Figure S5. Forest plot of the effect of susceptibility to hunger on EI.
Figure S6. Forest plot of the effect of susceptibility to hunger on BMI.
Figure S7. Forest plot of the effect of external eating on EI.
Figure S8. Forest plot of the effect of emotional eating on EI.
Figure S9. Funnel plot of the effect of emotional eating on EI.
Figure S10. Forest plot of the effect of emotional eating on BMI.
Figure S11. Funnel plot of the effect of emotional eating on BMI.
Figure S12. Forest plot of the effect of disinhibition on EI.
Figure S13. Funnel plot of the effect of disinhibition on EI.
Figure S14. Forest plot of the effect of disinhibition on BMI.
Figure S15. Forest plot of the effect of binge eating on EI.
Figure S16. Forest plot of the effect of binge eating on BMI.
ACKNOWLEDGMENT
The authors would like to thank Slimming World for supporting and funding this work.
Dakin C, Beaulieu K, Hopkins M, Gibbons C, Finlayson G, Stubbs RJ. Do eating behavior traits predict energy intake and body mass index? A systematic review and meta‐analysis. Obesity Reviews. 2023;24(1):e13515. doi: 10.1111/obr.13515
[Correction added on 18 November 2022, after first online publication: The order of author names have been corrected in this version.]
Funding information Slimming World
REFERENCES
- 1. De Onis M, Blössner M, Borghi E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr. 2010;92(5):1257‐1264. doi: 10.3945/ajcn.2010.29786 [DOI] [PubMed] [Google Scholar]
- 2. Blundell JE, Stubbs R, Golding C, et al. Resistance and susceptibility to weight gain: individual variability in response to a high‐fat diet. Physiol Behav. 2005;86(5):614‐622. doi: 10.1016/j.physbeh.2005.08.052 [DOI] [PubMed] [Google Scholar]
- 3. Llewellyn C, Wardle J. Behavioral susceptibility to obesity: gene–environment interplay in the development of weight. Physiol Behav. 2015;152(Pt B):494‐501. doi: 10.1016/j.physbeh.2015.07.006 [DOI] [PubMed] [Google Scholar]
- 4. Finlayson G, Arlotti A, Dalton M, King N, Blundell JE. Implicit wanting and explicit liking are markers for trait binge eating. A susceptible phenotype for overeating. Appetite. 2011;57(3):722‐728. doi: 10.1016/j.appet.2011.08.012 [DOI] [PubMed] [Google Scholar]
- 5. Stunkard AJ, Messick S. The three‐factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J Psychosom Res. 1985;29(1):71‐83. doi: 10.1016/0022-3999(85)90010-8 [DOI] [PubMed] [Google Scholar]
- 6. Vainik U, Garcia‐Garcia I, Dagher A. Uncontrolled eating: a unifying heritable trait linked with obesity, overeating, personality and the brain. Eur J Neurosci. 2019;50(3):2430‐2445. doi: 10.1111/ejn.14352 [DOI] [PubMed] [Google Scholar]
- 7. Blundell JE, King NA, Bryant EJ. Disinhibition: its effects on appetite and weight regulation. Obes Rev. 2008;9(5):409‐419. doi: 10.1111/j.1467-789X.2007.00426.x [DOI] [PubMed] [Google Scholar]
- 8. Espel‐Huynh HM, Muratore AF, Lowe MR. A narrative review of the construct of hedonic hunger and its measurement by the power of food scale. Obes Sci Pract. 2018;4(3):238‐249. doi: 10.1002/osp4.161 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. French A, Epstein LH, Jeffery RW, Blundell JE, Wardle J. Eating behavior dimensions. Associations with energy intake and body weight. A review. Appetite. 2012;59(2):541‐549. doi: 10.1016/j.appet.2012.07.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Stubbs RJ, O'Reilly LM, Whybrow S, et al. Measuring the difference between actual and reported food intakes in the context of energy balance under laboratory conditions. Br J Nutr. 2014;111(11):2032‐2043. doi: 10.1017/S0007114514000154 [DOI] [PubMed] [Google Scholar]
- 11. Devonport TJ, Nicholls W, Fullerton C. A systematic review of the association between emotions and eating behaviour in normal and overweight adult populations. J Health Psychol. 2019;24(1):3‐24. doi: 10.1177/1359105317697813 [DOI] [PubMed] [Google Scholar]
- 12. Vainik U, Dagher A, Dubé L, Fellows LK. Neurobehavioural correlates of body mass index and eating behaviours in adults: a systematic review. Neurosci Biobehav Rev. 2013;37(3):279‐299. doi: 10.1016/j.neubiorev.2012.11.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Bryant EJ, Rehman J, Pepper LB, Walters ER. Obesity and eating disturbance: the role of TFEQ restraint and disinhibition. Curr Obes Rep. 2019;8(4):363‐372. doi: 10.1007/s13679-019-00365-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Robinson E, Haynes A, Hardman CA, Jones A, Kemps E, Higgs S. The bogus taste test: validity as a measure of laboratory food intake. Appetite. 2017;116:223‐231. doi: 10.1016/j.appet.2017.05.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Dhurandhar NV, Schoeller D, Brown AW, et al. Energy balance measurement: when something is not better than nothing. Int J Obes (Lond). 2015;39(7):1109‐1113. doi: 10.1038/ijo.2014.199 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. UCL . Eating Behavior Questionnaires. Accessed 21/03/2022. https://www.ucl.ac.uk/epidemiology-health-care/research/behavioural-science-and-health/resources/questionnaires/eating-behaviour-questionnaires
- 17. Grid‐Enabled Measures Database . Obesity. Accessed 21/03/2022. https://www.gem-measures.org/Public/GEMSearchResults.aspx?allm=true&srchterm=obesity
- 18. Arab Psychology . Psychological Scales. Accessed 21/03/2022. https://scales.arabpsychology.com
- 19. McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40‐46. doi: 10.1016/j.jclinepi.2016.01.021 [DOI] [PubMed] [Google Scholar]
- 20. Shamseer L, Moher D, Clarke M, et al. Preferred reporting items for systematic review and meta‐analysis protocols (PRISMA‐P) 2015: elaboration and explanation. BMJ. 2015;349:g7647. [DOI] [PubMed] [Google Scholar]
- 21. Gormally J, Black S, Daston S, Rardin D. The assessment of binge eating severity among obese persons. Addict Behav. 1982;7(1):47‐55. doi: 10.1016/0306-4603(82)90024-7 [DOI] [PubMed] [Google Scholar]
- 22. American Psychiatric Association . Diagnostic and statistical manual of mental disorders: DSM‐5. 5thed. Washington, DC: American Psychiatric Sssociation; 2013. doi: 10.1176/appi.books.9780890425596. [DOI] [Google Scholar]
- 23. Cochrane . Data Extraction Forms. Accessed 21/03/2022. https://dplp.cochrane.org/data-extraction-forms
- 24. R Core Team . R: A language and environment for statistical computing. R Foundation for Statistical Computing. https://www.R-project.org/
- 25. Harrer M, Cuijpers P, Furukawa T, Ebert D. Companion R Package For The Guide 'Doing Meta‐Analysis in R. 2019. http://dmetar.protectlab.org/
- 26. Lüdecke D. esc: Effect Size Computation for Meta Analysis (Version 0.5.1). 2019; doi: 10.5281/zenodo.1249218, https://CRAN.R-project.org/package=esc [DOI]
- 27. Wickham, Averick M, Bryan J, et al. Welcome to the tidyverse. J Open Source Softw. 2019;4(43):1686. doi: 10.21105/joss.01686 [DOI] [Google Scholar]
- 28. Balduzzi S, Rücker G, Schwarzer G. How to perform a meta‐analysis with R: a practical tutorial. Evid Based Ment Health. 2019;22(4):153‐160. doi: 10.1136/ebmental-2019-300117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Fisher RA. Statistical methods for research workers. In: Breakthroughs in statistics. Springer; 1992:66‐70. doi: 10.1007/978-1-4612-4380-9_6. [DOI] [Google Scholar]
- 30. Higgins JP, Thomas J, Chandler J, et al. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons; 2019. doi: 10.1002/9781119536604. [DOI] [Google Scholar]
- 31. Harrer M, Cuijpers P, Furukawa TA, Ebert DD. Doing meta‐analysis with R: A hands‐on guide. Chapman and Hall/CRC; 2021. doi: 10.1201/9781003107347. [DOI] [Google Scholar]
- 32. Funder DC, Ozer DJ. Evaluating effect size in psychological research: sense and nonsense. Adv Methods Pract Psychol Sci. 2019;2(2):156‐168. doi: 10.1177/2515245919847202 [DOI] [Google Scholar]
- 33. von Hippel PT. The heterogeneity statistic I 2 can be biased in small meta‐analyses. BMC Med Res Methodol. 2015;15(1):1, 35‐8. doi: 10.1186/s12874-015-0024-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Knapp G, Hartung J. Improved tests for a random effects meta‐regression with a single covariate. Stat Med. 2003;22(17):2693‐2710. doi: 10.1002/sim.1482 [DOI] [PubMed] [Google Scholar]
- 35. IntHout J, Ioannidis J, Borm GF. The Hartung‐Knapp‐Sidik‐Jonkman method for random effects meta‐analysis is straightforward and considerably outperforms the standard DerSimonian‐Laird method. BMC Med Res Methodol. 2014;14(1):1‐12. doi: 10.1186/1471-2288-14-25 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Hedges LV. Distribution theory for Glass's estimator of effect size and related estimators. J Educ Stat. 1981;6(2):107‐128. doi: 10.3102/10769986006002107 [DOI] [Google Scholar]
- 37. Hong Q, Pluye P, Fàbregues S, et al. Mixed Methods Appraisal Tool (MMAT) Version 2018. Accessed 21/03/2022. http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf
- 38. Hong QN, Fàbregues S, Bartlett G, et al. The mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. 2018;34(4):285‐291. doi: 10.3233/EFI-180221 [DOI] [Google Scholar]
- 39. Tylka TL. Development and psychometric evaluation of a measure of intuitive eating. J Couns Psychol. 2006;53(2):226‐240. doi: 10.1037/0022-0167.53.2.226 [DOI] [Google Scholar]
- 40. Tylka TL, Kroon Van Diest AM. The intuitive eating scale–2: item refinement and psychometric evaluation with college women and men. J Couns Psychol. 2013;60(1):137‐153. doi: 10.1037/a0030893 [DOI] [PubMed] [Google Scholar]
- 41. Framson C, Kristal AR, Schenk JM, Littman AJ, Zeliadt S, Benitez D. Development and validation of the mindful eating questionnaire. J am Diet Assoc. 2009;109(8):1439‐1444. doi: 10.1016/j.jada.2009.05.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Green S, Delargy H, Joanes D, Blundell J. A satiety quotient: a formulation to assess the satiating effect of food. Appetite. 1997;29(3):291‐304. doi: 10.1006/appe.1997.0096 [DOI] [PubMed] [Google Scholar]
- 43. Hunot C, Fildes A, Croker H, Llewellyn CH, Wardle J, Beeken RJ. Appetitive traits and relationships with BMI in adults: development of the adult eating behaviour questionnaire. Appetite. 2016;105:356‐363. doi: 10.1016/j.appet.2016.05.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Herman CP, Mack D. Restrained and unrestrained eating. J Pers. 1975;43(4):647‐660. doi: 10.1111/j.1467-6494.1975.tb00727.x [DOI] [PubMed] [Google Scholar]
- 45. Herman CP, Polivy J, Silver R. Effects of an observer on eating behavior: the induction of “sensible” eating. J Pers. 1979;47(1):85‐99. doi: 10.1111/j.1467-6494.1979.tb00616.x [DOI] [PubMed] [Google Scholar]
- 46. van Strien T, Frijters JE, Bergers GP, Defares PB. The Dutch eating behavior questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int J Eat Disord. 1986;5(2):295‐315. doi: 10.1002/1098-108X(198602)5:23.0.CO;2-T [DOI] [Google Scholar]
- 47. Dalton M, Finlayson G, Blundell J, Hill A. Preliminary validation and principal components analysis of the control of eating questionnaire (CoEQ) for the experience of food craving. Eur J Clin Nutr. 2015;69(12):1313‐1317. doi: 10.1038/ejcn.2015.57 [DOI] [PubMed] [Google Scholar]
- 48. Lowe MR, Butryn ML, Didie ER, et al. The power of food scale. A new measure of the psychological influence of the food environment. Appetite. 2009;53(1):114‐118. doi: 10.1016/j.appet.2009.05.016 [DOI] [PubMed] [Google Scholar]
- 49. White MA, Whisenhunt BL, Williamson DA, Greenway FL, Netemeyer RG. Development and validation of the food‐craving inventory. Obes Res. 2002;10(2):107‐114. doi: 10.1038/oby.2002.17 [DOI] [PubMed] [Google Scholar]
- 50. Fairburn CG, Cooper Z, O'Connor M. The eating disorder examination. Int J Eat Disord. 1993;6:1‐8. [Google Scholar]
- 51. Akkermann K, Herik M, Aluoja A, Järv A. Constructing an assessment scale for eating disorders. Tartu: Department of Psychology of University of Tartu; 2010. [Google Scholar]
- 52. Stice E, Telch CF, Rizvi SL. Development and validation of the eating disorder diagnostic scale: a brief self‐report measure of anorexia, bulimia, and binge‐eating disorder. Psychol Assess. 2000;12(2):123‐131. doi: 10.1037/1040-3590.12.2.123 [DOI] [PubMed] [Google Scholar]
- 53. Garner DM. Eating disorder Inventory‐2; pro‐fessional manual. Psychological assessment resources; 1991. [Google Scholar]
- 54. Clark MM, Abrams DB, Niaura RS, Eaton CA, Rossi JS. Self‐efficacy in weight management. J Consult Clin Psychol. 1991;59(5):739‐744. doi: 10.1037/0022-006X.59.5.739 [DOI] [PubMed] [Google Scholar]
- 55. Vainik U, Eun Han J, Epel ES, Janet Tomiyama A, Dagher A, Mason AE. Rapid assessment of reward‐related eating: the RED‐X5. Obesity. 2019;27(2):325‐331. doi: 10.1002/oby.22374 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Gearhardt AN, Corbin WR, Brownell KD. Development of the Yale food addiction scale version 2.0. Psychol Addict Behav. 2016;30(1):113‐121. doi: 10.1037/adb0000136 [DOI] [PubMed] [Google Scholar]
- 57. Anderson DA, Schaumberg K, Anderson LM, Reilly EE. Is level of intuitive eating associated with plate size effects? Eat Behav. 2015;18:125‐130. doi: 10.1016/j.eatbeh.2015.05.005 [DOI] [PubMed] [Google Scholar]
- 58. Anderson LM, Reilly EE, Schaumberg K, Dmochowski S, Anderson DA. Contributions of mindful eating, intuitive eating, and restraint to BMI, disordered eating, and meal consumption in college students. Eat Weight Disord. 2016;21(1):83‐90. doi: 10.1007/s40519-015-0210-3 [DOI] [PubMed] [Google Scholar]
- 59. Ruzanska UA, Warschburger P. How is intuitive eating related to self‐reported and laboratory food intake in middle‐aged adults? Eat Behav. 2020;38:101405. doi: 10.1016/j.eatbeh.2020.101405 [DOI] [PubMed] [Google Scholar]
- 60. Dalton M, Hollingworth S, Blundell J, Finlayson G. Weak satiety responsiveness is a reliable trait associated with hedonic risk factors for overeating among women. Nutrients. 2015;7(9):7421‐7436. doi: 10.3390/nu7095345 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Drapeau V, Blundell J, Therrien F, Lawton C, Richard D, Tremblay A. Appetite sensations as a marker of overall intake. Br J Nutr. 2005;93(2):273‐280. doi: 10.1079/BJN20041312 [DOI] [PubMed] [Google Scholar]
- 62. Drapeau V, Jacob R, Panahi S, Tremblay A. Effect of energy restriction on eating behavior traits and psychobehavioral factors in the low satiety phenotype. Nutrients. 2019;11(2):245. doi: 10.3390/nu11020245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Zuraikat FM, Roe LS, Smethers AD, Reihart LW, Rolls BJ. Does the cost of a meal influence the portion size effect? Appetite. 2018;127:341‐348. doi: 10.1016/j.appet.2018.05.020 [DOI] [PubMed] [Google Scholar]
- 64. Ard JD, Desmond RA, Allison DB, Conway JM. Dietary restraint and disinhibition do not affect accuracy of 24‐hour recall in a multiethnic population. J am Diet Assoc. 2006;106(3):434‐437. doi: 10.1016/j.jada.2005.12.006 [DOI] [PubMed] [Google Scholar]
- 65. Bellisle F, Dalix A‐M, Airinei G, Hercberg S, Péneau S. Influence of dietary restraint and environmental factors on meal size in normal‐weight women. A laboratory study. Appetite. 2009;53(3):309‐313. doi: 10.1016/j.appet.2009.07.006 [DOI] [PubMed] [Google Scholar]
- 66. Bryant EJ, Caudwell P, Blundell JE, Hopkins ME, King NA. Psycho‐markers of weight loss. The roles of TFEQ disinhibition and restraint in exercise‐induced weight management. Appetite. 2012;58(1):234‐241. doi: 10.1016/j.appet.2011.09.006 [DOI] [PubMed] [Google Scholar]
- 67. Chambers L, Yeomans MR. Individual differences in satiety response to carbohydrate and fat. Predictions from the three factor eating questionnaire (TFEQ). Appetite. 2011;56(2):316‐323. doi: 10.1016/j.appet.2011.01.003 [DOI] [PubMed] [Google Scholar]
- 68. Coelho JS, Polivy J, Herman CP, Pliner P. Wake up and smell the cookies. Effects of olfactory food‐cue exposure in restrained and unrestrained eaters. Appetite. 2009;52(2):517‐520. doi: 10.1016/j.appet.2008.10.008 [DOI] [PubMed] [Google Scholar]
- 69. Cools J, Schotte DE, McNally RJ. Emotional arousal and overeating in restrained eaters. J Abnorm Psychol. 1992;101(2):348‐351. doi: 10.1037/0021-843X.101.2.348 [DOI] [PubMed] [Google Scholar]
- 70. de Witt Huberts JC, Evers C, de Ridder DT. Double trouble: restrained eaters do not eat less and feel worse. Psychol Health. 2013;28(6):686‐700. doi: 10.1080/08870446.2012.751106 [DOI] [PubMed] [Google Scholar]
- 71. Dweck JS, Jenkins SM, Nolan LJ. The role of emotional eating and stress in the influence of short sleep on food consumption. Appetite. 2014;72:106‐113. doi: 10.1016/j.appet.2013.10.001 [DOI] [PubMed] [Google Scholar]
- 72. Fedoroff ID, Polivy J, Herman CP. The effect of pre‐exposure to food cues on the eating behavior of restrained and unrestrained eaters. Appetite. 1997;28(1):33‐47. doi: 10.1006/appe.1996.0057 [DOI] [PubMed] [Google Scholar]
- 73. Finlayson G, Blundell JE, Bordes I, Griffioen‐Roose S, de Graaf C. Susceptibility to overeating affects the impact of savory or sweet drinks on satiation, reward, and food intake in nonobese women. J Nutr. 2012;142(1):125‐130. doi: 10.3945/jn.111.148106 [DOI] [PubMed] [Google Scholar]
- 74. Guerrieri R, Nederkoorn C, Schrooten M, Martijn C, Jansen A. Inducing impulsivity leads high and low restrained eaters into overeating, whereas current dieters stick to their diet. Appetite. 2009;53(1):93‐100. doi: 10.1016/j.appet.2009.05.013 [DOI] [PubMed] [Google Scholar]
- 75. Haynes C, Lee MD, Yeomans MR. Interactive effects of stress, dietary restraint, and disinhibition on appetite. Eat Behav. 2003;4(4):369‐383. doi: 10.1016/j.eatbeh.2003.07.005 [DOI] [PubMed] [Google Scholar]
- 76. Herhaus B, Petrowski K. The effect of restrained eating on acute stress‐induced food intake in people with obesity. Appetite. 2021;159:105045. doi: 10.1016/j.appet.2020.105045 [DOI] [PubMed] [Google Scholar]
- 77. Higgs S, Williamson AC, Attwood AS. Recall of recent lunch and its effect on subsequent snack intake. Physiol Behav. 2008;94(3):454‐462. doi: 10.1016/j.physbeh.2008.02.011 [DOI] [PubMed] [Google Scholar]
- 78. Hofmann W, Friese M. Impulses got the better of me: alcohol moderates the influence of implicit attitudes toward food cues on eating behavior. J Abnorm Psychol. 2008;117(2):420‐427. doi: 10.1037/0021-843X.117.2.420 [DOI] [PubMed] [Google Scholar]
- 79. Jansen A. How restrained eaters perceive the amount they eat. Br J Clin Psychol. 1996;35(3):381‐392. doi: 10.1111/j.2044-8260.1996.tb01192.x [DOI] [PubMed] [Google Scholar]
- 80. Jansen A, Merckelbach H, Oosterlaan J, Tuiten A, Van Den Hout M. Cognitions and self‐talk during food intake of restrained and unrestrained eaters. Behav Res Ther. 1988;26(5):393‐398. doi: 10.1016/0005-7967(88)90072-1 [DOI] [PubMed] [Google Scholar]
- 81. Lattimore P, Maxwell L. Cognitive load, stress, and disinhibited eating. Eat Behav. 2004;5(4):315‐324. doi: 10.1016/j.eatbeh.2004.04.009 [DOI] [PubMed] [Google Scholar]
- 82. Martin CK, Williamson DA, Geiselman PJ, et al. Consistency of food intake over four eating sessions in the laboratory. Eat Behav. 2005;6(4):365‐372. doi: 10.1016/j.eatbeh.2005.03.002 [DOI] [PubMed] [Google Scholar]
- 83. McNeil J, Lamothe G, Cameron JD, et al. Investigating predictors of eating: is resting metabolic rate really the strongest proxy of energy intake? Am J Clin Nutr. 2017;106(5):ajcn153718. doi: 10.3945/ajcn.117.153718 [DOI] [PubMed] [Google Scholar]
- 84. Myhre R, Buchwald D, Kratz M, et al. A twin study of differences in the response of plasma ghrelin to a milkshake preload in restrained eaters. Physiol Behav. 2014;129:50‐56. doi: 10.1016/j.physbeh.2014.02.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85. Oliver G, Wardle J, Gibson EL. Stress and food choice: a laboratory study. Psychosom Med. 2000;62(6):853‐865. doi: 10.1097/00006842-200011000-00016 [DOI] [PubMed] [Google Scholar]
- 86. Ouwens MA, van Strien T, van der Staak CP. Tendency toward overeating and restraint as predictors of food consumption. Appetite. 2003;40(3):291‐298. doi: 10.1016/S0195-6663(03)00006-0 [DOI] [PubMed] [Google Scholar]
- 87. Peluso A. Comparison of mindful and slow eating strategies on acute energy intake. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2017;78(5‐B[E]). [Google Scholar]
- 88. Rideout CA, McLean JA, Barr SI. Women with high scores for cognitive dietary restraint choose foods lower in fat and energy. J am Diet Assoc. 2004;104(7):1154‐1157. doi: 10.1016/j.jada.2004.04.024 [DOI] [PubMed] [Google Scholar]
- 89. Rolls BJ, Castellanos VH, Shide DJ, et al. Sensory properties of a nonabsorbable fat substitute did not affect regulation of energy intake. Am J Clin Nutr. 1997;65(5):1375‐1383. doi: 10.1093/ajcn/65.5.1375 [DOI] [PubMed] [Google Scholar]
- 90. Ruddock HK, Field M, Hardman CA. Exploring food reward and calorie intake in self‐perceived food addicts. Appetite. 2017;115:36‐44. doi: 10.1016/j.appet.2016.12.003 [DOI] [PubMed] [Google Scholar]
- 91. Schoch AH, Raynor HA. Social desirability, not dietary restraint, is related to accuracy of reported dietary intake of a laboratory meal in females during a 24‐hour recall. Eat Behav. 2012;13(1):78‐81. doi: 10.1016/j.eatbeh.2011.11.010 [DOI] [PubMed] [Google Scholar]
- 92. Schotte DE, Cools J, McNally RJ. Film‐induced negative affect triggers overeating in restrained eaters. J Abnorm Psychol. 1990;99(3):317‐320. doi: 10.1037/0021-843X.99.3.317 [DOI] [PubMed] [Google Scholar]
- 93. Shapiro JR, Anderson DA. Counterregulatory eating behavior in multiple item test meals. Eat Behav. 2005;6(2):169‐178. doi: 10.1016/j.eatbeh.2004.08.001 [DOI] [PubMed] [Google Scholar]
- 94. Sim AY, Lee LL, Cheon BK. When exercise does not pay: counterproductive effects of impending exercise on energy intake among restrained eaters. Appetite. 2018;123:120‐127. doi: 10.1016/j.appet.2017.12.017 [DOI] [PubMed] [Google Scholar]
- 95. Smith CF, Geiselman PJ, Williamson DA, Champagne CM, Bray GA, Ryan DH. Association of dietary restraint and disinhibition with eating behavior, body mass, and hunger. Eat Weight Disord: EWD. 1998;3(1):7‐15. doi: 10.1007/BF03354907 [DOI] [PubMed] [Google Scholar]
- 96. Stice E, Fisher M, Lowe MR. Are dietary restraint scales valid measures of acute dietary restriction? Unobtrusive observational data suggest not. Psychol Assess. 2004;16(1):51‐59. doi: 10.1037/1040-3590.16.1.51 [DOI] [PubMed] [Google Scholar]
- 97. Stice E, Sysko R, Roberto CA, Allison S. Are dietary restraint scales valid measures of dietary restriction? Additional objective behavioral and biological data suggest not. Appetite. 2010;54(2):331‐339. doi: 10.1016/j.appet.2009.12.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Stinson EJ, Votruba SB, Venti C, Krakoff J, Gluck ME, Perez M. Food insecurity is associated with maladaptive eating behaviors and objectively measured overeating. Obesity. 2018;26(12):1841‐1848. doi: 10.1002/oby.22305 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99. van Strien T, Ouwens MA. Counterregulation in female obese emotional eaters: Schachter, Goldman, and Gordon's (1968) test of psychosomatic theory revisited. Eat Behav. 2003;3(4):329‐340. doi: 10.1016/S1471-0153(02)00092-2 [DOI] [PubMed] [Google Scholar]
- 100. Visona C, George VA. Impact of dieting status and dietary restraint on postexercise energy intake in overweight women. Obes Res. 2002;10(12):1251‐1258. doi: 10.1038/oby.2002.170 [DOI] [PubMed] [Google Scholar]
- 101. Wallis DJ, Hetherington MM. Stress and eating: the effects of ego‐threat and cognitive demand on food intake in restrained and emotional eaters. Appetite. 2004;43(1):39‐46. doi: 10.1016/j.appet.2004.02.001 [DOI] [PubMed] [Google Scholar]
- 102. Wallis DJ, Hetherington MM. Emotions and eating. Self‐reported and experimentally induced changes in food intake under stress. Appetite. 2009;52(2):355‐362. doi: 10.1016/j.appet.2008.11.007 [DOI] [PubMed] [Google Scholar]
- 103. Wardle J, Beales S. Restraint and food intake: an experimental study of eating patterns in the laboratory and in normal life. Behav Res Ther. 1987;25(3):179‐185. doi: 10.1016/0005-7967(87)90044-1 [DOI] [PubMed] [Google Scholar]
- 104. Westenhoefer J, Broeckmann P, Münch A‐K, Pudel V. Cognitive control of eating behavior and the disinhibition effect. Appetite. 1994;23(1):27‐41. doi: 10.1006/appe.1994.1032 [DOI] [PubMed] [Google Scholar]
- 105. Yeomans MR, Coughlan E. Mood‐induced eating. Interactive effects of restraint and tendency to overeat. Appetite. 2009;52(2):290‐298. doi: 10.1016/j.appet.2008.10.006 [DOI] [PubMed] [Google Scholar]
- 106. Yeomans MR, Tovey H, Tinley E, Haynes C. Effects of manipulated palatability on appetite depend on restraint and disinhibition scores from the three‐factor eating questionnaire. Int J Obes (Lond). 2004;28(1):144‐151. doi: 10.1038/sj.ijo.0802483 [DOI] [PubMed] [Google Scholar]
- 107. Zambrowicz R, Schebendach J, Sysko R, Mayer LES, Walsh BT, Steinglass JE. Relationship between three factor eating questionnaire‐restraint subscale and food intake. Int J Eat Disord. 2019;52(3):255‐260. doi: 10.1002/eat.23014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108. Appelhans BM, Liebman R, Woolf K, Pagoto SL, Schneider KL, Whited MC. Inhibiting food reward: delay discounting, food reward sensitivity, and palatable food intake in overweight and obese women. Obesity. 2011;19(11):2175‐2182. doi: 10.1038/oby.2011.57 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109. Ely AV, Howard J, Lowe MR. Delayed discounting and hedonic hunger in the prediction of lab‐based eating behavior. Eat Behav. 2015;19:72‐75. doi: 10.1016/j.eatbeh.2015.06.015 [DOI] [PubMed] [Google Scholar]
- 110. Nolan‐Poupart S, Veldhuizen MG, Geha P, Small DM. Midbrain response to milkshake correlates with ad libitum milkshake intake in the absence of hunger. Appetite. 2013;60:168‐174. doi: 10.1016/j.appet.2012.09.032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111. Martin CK, O'Neil PM, Tollefson G, Greenway FL, White MA. The association between food cravings and consumption of specific foods in a laboratory taste test. Appetite. 2008;51(2):324‐326. doi: 10.1016/j.appet.2008.03.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112. Epstein LH, Lin H, Carr KA, Fletcher KD. Food reinforcement and obesity. Psychological moderators. Appetite. 2012;58(1):157‐162. doi: 10.1016/j.appet.2011.09.025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113. Hopkins M, Michalowska J, Whybrow S, Horgan GW, Stubbs RJ. Identification of psychological correlates of dietary misreporting under laboratory and free‐living environments. Br J Nutr. 2021;126(2):264‐275. doi: 10.1017/S000711452000389X [DOI] [PubMed] [Google Scholar]
- 114. Kakoschke N, Kemps E, Tiggemann M. External eating mediates the relationship between impulsivity and unhealthy food intake. Physiol Behav. 2015;147:117‐121. doi: 10.1016/j.physbeh.2015.04.030 [DOI] [PubMed] [Google Scholar]
- 115. Robinson E, Haynes A. Individual differences and moderating participant characteristics in the effect of reducing portion size on meal energy intake: pooled analysis of three randomized controlled trials. Appetite. 2021;159:105047. doi: 10.1016/j.appet.2020.105047 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116. van Strien T, Donker MH, Ouwens MA. Is desire to eat in response to positive emotions an 'obese' eating style: is kummerspeck for some people a misnomer? Appetite. 2016;100:225‐235. doi: 10.1016/j.appet.2016.02.035 [DOI] [PubMed] [Google Scholar]
- 117. Evers C, de Ridder DTD, Adriaanse MA. Assessing yourself as an emotional eater: mission impossible? Health Psychol. 2009;28(6):717‐725. doi: 10.1037/a0016700 [DOI] [PubMed] [Google Scholar]
- 118. Raspopow K, Abizaid A, Matheson K, Anisman H. Anticipation of a psychosocial stressor differentially influences ghrelin, cortisol and food intake among emotional and non‐emotional eaters. Appetite. 2014;74:35‐43. doi: 10.1016/j.appet.2013.11.018 [DOI] [PubMed] [Google Scholar]
- 119. van Strien T, Herman CP, Anschutz DJ, Engels RC, de Weerth C. Moderation of distress‐induced eating by emotional eating scores. Appetite. 2012;58(1):277‐284. doi: 10.1016/j.appet.2011.10.005 [DOI] [PubMed] [Google Scholar]
- 120. Alger S, Seagle H, Ravussin E. Food‐intake and energy expenditure in obese female bingers and non‐bingers. Int J Obes (Lond). 1995;19(1):11‐16. [PubMed] [Google Scholar]
- 121. Arumae K, Kreegipuu K, Vainik U. Assessing the overlap between three measures of food reward. Front Psychol. 2019;10:883. doi: 10.3389/fpsyg.2019.00883 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122. Dalton M, Blundell J, Finlayson G. Effect of BMI and binge eating on food reward and energy intake: further evidence for a binge eating subtype of obesity. Obes Facts. 2013;6(4):348‐359. doi: 10.1159/000354599 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123. Dalton M, Blundell J, Finlayson GS. Examination of food reward and energy intake under laboratory and free‐living conditions in a trait binge eating subtype of obesity. Front Psychol. 2013;4:757. doi: 10.3389/fpsyg.2013.00757 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124. Nasser JA, Gluck ME, Geliebter A. Impulsivity and test meal intake in obese binge eating women. Appetite. 2004;43(3):303‐307. doi: 10.1016/j.appet.2004.04.006 [DOI] [PubMed] [Google Scholar]
- 125. Long S, Meyer C, Leung N, Wallis DJ. Effects of distraction and focused attention on actual and perceived food intake in females with non‐clinical eating psychopathology. Appetite. 2011;56(2):350‐356. doi: 10.1016/j.appet.2010.12.018 [DOI] [PubMed] [Google Scholar]
- 126. Schulte EM, Sonneville KR, Gearhardt AN. Subjective experiences of highly processed food consumption in individuals with food addiction. Psychol Addict Behav. 2019;33(2):144‐153. doi: 10.1037/adb0000441 [DOI] [PubMed] [Google Scholar]
- 127. Vijayvargiya P, Chedid V, Wang XJ, et al. Associations of gastric volumes, ingestive behavior, calorie and volume intake, and fullness in obesity. Am J Physiol Gastrointest Liver Physiol. 2020;319(2):G238‐G244. doi: 10.1152/ajpgi.00140.2020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128. Bellisle F, Dalix AM. Cognitive restraint can be offset by distraction, leading to increased meal intake in women. Am J Clin Nutr. 2001;74(2):197‐200. doi: 10.1093/ajcn/74.2.197 [DOI] [PubMed] [Google Scholar]
- 129. Sultson H, Kukk K, Akkermann K. Positive and negative emotional eating have different associations with overeating and binge eating: construction and validation of the positive‐negative emotional eating scale. Appetite. 2017;116:423‐430. doi: 10.1016/j.appet.2017.05.035 [DOI] [PubMed] [Google Scholar]
- 130. Turner RM, Bird SM, Higgins JP. The impact of study size on meta‐analyses: examination of underpowered studies in Cochrane reviews. PLoS ONE. 2013;8(3):e59202. doi: 10.1371/journal.pone.0059202 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131. de Lauzon‐Guillain B, Basdevant A, Romon M, et al. Is restrained eating a risk factor for weight gain in a general population? Am J Clin Nutr. 2006;83(1):132‐138. doi: 10.1093/ajcn/83.1.132 [DOI] [PubMed] [Google Scholar]
- 132. Lluch A, Herbeth B, Mejean L, Siest G. Dietary intakes, eating style and overweight in the Stanislas family study. Int J Obes (Lond). 2000;24(11):1493‐1499. doi: 10.1038/sj.ijo.0801425 [DOI] [PubMed] [Google Scholar]
- 133. Johnson F, Pratt M, Wardle J. Dietary restraint and self‐regulation in eating behavior. Int J Obes (Lond). 2012;36(5):665‐674. doi: 10.1038/ijo.2011.156 [DOI] [PubMed] [Google Scholar]
- 134. Santos I, Sniehotta FF, Marques MM, Carraça EV, Teixeira PJ. Prevalence of personal weight control attempts in adults: a systematic review and meta‐analysis. Obes Rev. 2017;18(1):32‐50. doi: 10.1111/obr.12466 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135. Stubbs RJ, Duarte C, O'Driscoll R, Turicchi J, Michalowska J. Developing evidence‐based behavioural strategies to overcome physiological resistance to weight loss in the general population. Proc Nutr Soc. 2019;78(4):576‐589. doi: 10.1017/S0029665119001083 [DOI] [PubMed] [Google Scholar]
- 136. Heatherton TF, Herman CP, Polivy J, King GA, McGree ST. The (mis) measurement of restraint: an analysis of conceptual and psychometric issues. J Abnorm Psychol. 1988;97(1):19‐28. doi: 10.1037/0021-843X.97.1.19 [DOI] [PubMed] [Google Scholar]
- 137. Mela DJ. Determinants of food choice: relationships with obesity and weight control. Obes Res. 2001;9(S11):249S‐255S. doi: 10.1038/oby.2001.127 [DOI] [PubMed] [Google Scholar]
- 138. van Strien T, Cebolla A, Etchemendy E, et al. Emotional eating and food intake after sadness and joy. Appetite. 2013;66:20‐25. doi: 10.1016/j.appet.2013.02.016 [DOI] [PubMed] [Google Scholar]
- 139. Elfhag K, Rössner S. Who succeeds in maintaining weight loss? A conceptual review of factors associated with weight loss maintenance and weight regain. Obes Rev. 2005;6(1):67‐85. doi: 10.1111/j.1467-789X.2005.00170.x [DOI] [PubMed] [Google Scholar]
- 140. Karlsson J, Hallgren P, Kral J, Lindroos A‐K, Sjöström L, Sullivan M. Predictors and effects of long‐term dieting on mental well‐being and weight loss in obese women. Appetite. 1994;23(1):15‐26. doi: 10.1006/appe.1994.1031 [DOI] [PubMed] [Google Scholar]
- 141. Niemeier HM, Phelan S, Fava JL, Wing RR. Internal disinhibition predicts weight regain following weight loss and weight loss maintenance. Obesity. 2007;15(10):2485‐2494. doi: 10.1038/oby.2007.295 [DOI] [PubMed] [Google Scholar]
- 142. Chaput J‐P, Drapeau V, Hetherington M, Lemieux S, Provencher V, Tremblay A. Psychobiological impact of a progressive weight loss program in obese men. Physiol Behav. 2005;86(1–2):224‐232. doi: 10.1016/j.physbeh.2005.07.014 [DOI] [PubMed] [Google Scholar]
- 143. Foster G, Wadden T, Swain R, Stunkard A, Platte P, Vogt R. The eating inventory in obese women: clinical correlates and relationship to weight loss. Int J Obes (Lond). 1998;22(8):778‐785. doi: 10.1038/sj.ijo.0800659 [DOI] [PubMed] [Google Scholar]
- 144. Pekkarinen T, Takala I, Mustajoki P. Two year maintenance of weight loss after a VLCD and behavioural therapy for obesity: correlation to the scores of questionnaires measuring eating behaviour. Int J Obes Relat Metab Disord. 1996;20(4):332‐337. [PubMed] [Google Scholar]
- 145. Konttinen H. Emotional eating and obesity in adults: the role of depression, sleep and genes. Proc Nutr Soc. 2020;79(3):283‐289. doi: 10.1017/S0029665120000166 [DOI] [PubMed] [Google Scholar]
- 146. Mantzios M, Wilson JC. Mindfulness, eating Behaviours, and obesity: a review and reflection on current findings. Curr Obes Rep. 2015;4(1):141‐146. doi: 10.1007/s13679-014-0131-x [DOI] [PubMed] [Google Scholar]
- 147. Nichols AL, Maner JK. The good‐subject effect: investigating participant demand characteristics. J Gen Psychol. 2008;135(2):151‐166. doi: 10.3200/GENP.135.2.151-166 [DOI] [PubMed] [Google Scholar]
- 148. O'Driscoll R, Turicchi J, Hopkins M, et al. Comparison of the validity and generalizability of machine learning algorithms for the prediction of energy expenditure: validation study. JMIR Mhealth Uhealth. 2021;9(8):e23938. doi: 10.2196/23938 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149. O'Driscoll R, Turicchi J, Hopkins M, Horgan GW, Finlayson G, Stubbs JR. Improving energy expenditure estimates from wearable devices: a machine learning approach. J Sports Sci. 2020;38(13):1496‐1505. doi: 10.1080/02640414.2020.1746088 [DOI] [PubMed] [Google Scholar]
- 150. Sanghvi A, Redman LM, Martin CK, Ravussin E, Hall KD. Validation of an inexpensive and accurate mathematical method to measure long‐term changes in free‐living energy intake. Am J Clin Nutr. 2015;102(2):353‐358. doi: 10.3945/ajcn.115.111070 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151. Shook RP, Hand GA, O'Connor DP, et al. Energy intake derived from an energy balance equation, validated activity monitors, and dual X‐ray absorptiometry can provide acceptable caloric intake data among young adults. J Nutr. 2018;148(3):490‐496. doi: 10.1093/jn/nxx029 [DOI] [PubMed] [Google Scholar]
- 152. Peng J, Shi P, Qiu J, et al. Clustering Egocentric Images in Passive Dietary Monitoring with Self‐Supervised Learning. arXiv preprint arXiv:220812160. 2022.
- 153. Lo FPW, Jobarteh ML, Sun Y, et al. An Intelligent Passive Food Intake Assessment System with Egocentric Cameras. arXiv preprint arXiv:210503142. 2021.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1: Search strategy.
Table S2: Characteristics of included studies.
Table S3: Results of the subgroup‐meta‐analysis for the effect of restraint on EI, influenced by questionnaire type.
Table S4: Results of a subgroup meta‐analysis on the effects of restraint on EI influenced by a preload.
Figure S1. Forest plot of the effect of IES on BMI.
Figure S2. Forest plot of the effect of satiety responsiveness on BMI.
Figure S3: Funnel plot of the effect of restraint on EI.
Figure S4: Funnel plot of the effect of restraint on BMI.
Figure S5. Forest plot of the effect of susceptibility to hunger on EI.
Figure S6. Forest plot of the effect of susceptibility to hunger on BMI.
Figure S7. Forest plot of the effect of external eating on EI.
Figure S8. Forest plot of the effect of emotional eating on EI.
Figure S9. Funnel plot of the effect of emotional eating on EI.
Figure S10. Forest plot of the effect of emotional eating on BMI.
Figure S11. Funnel plot of the effect of emotional eating on BMI.
Figure S12. Forest plot of the effect of disinhibition on EI.
Figure S13. Funnel plot of the effect of disinhibition on EI.
Figure S14. Forest plot of the effect of disinhibition on BMI.
Figure S15. Forest plot of the effect of binge eating on EI.
Figure S16. Forest plot of the effect of binge eating on BMI.