

Abstract
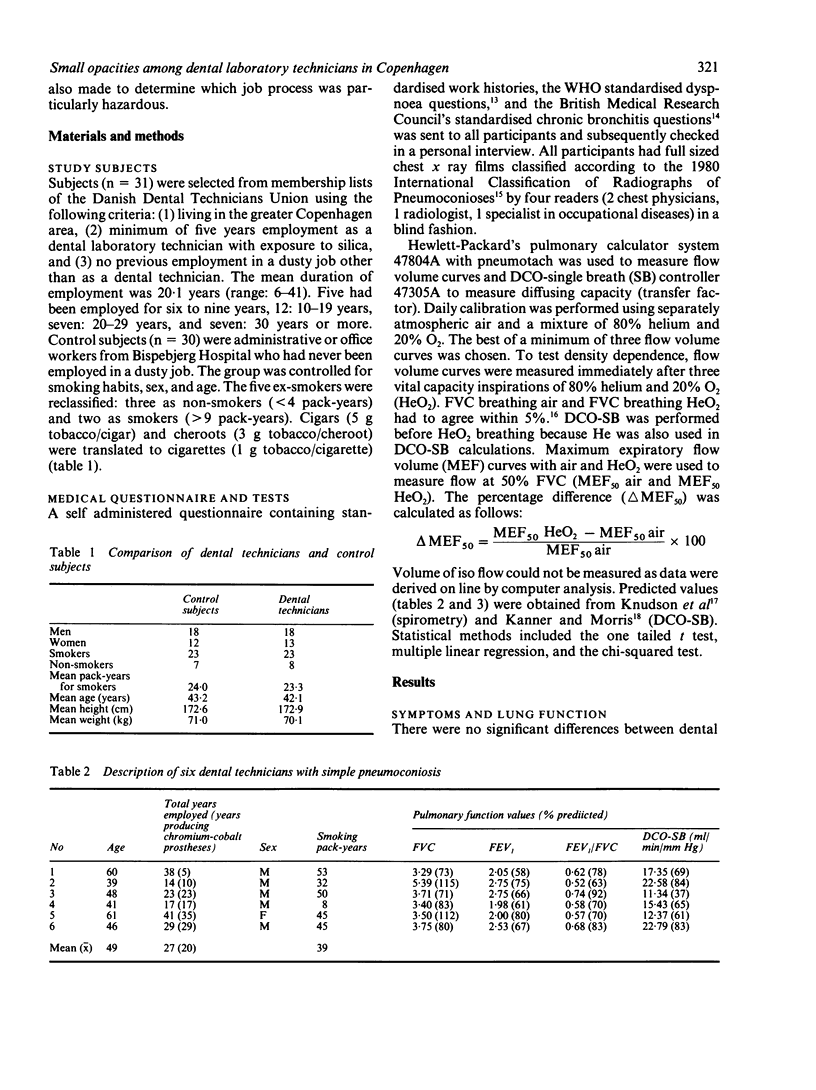
After a case of advanced pneumoconiosis occurred in a dental laboratory technician, 31 other dental technicians and 30 control subjects controlled for smoking habits, sex, and age were investigated. More technicians (55%) than controls (30%) had at least grade 1 dyspnoea (p greater than 0.05). Multiple regression analysis showed that 13 technicians who had produced dental prostheses for at least 15 years had consistently lower lung function (FVC, FEV1, FEV1/FVC, MEF50, and DCO single breath), although the differences were not statistically significant. All mean lung function values for technicians and controls were within normal limits. Increases in MEF50 after breathing 80% helium and 20% O2 failed to show small airways dysfunction among the technicians. Of the six with radiological pneumoconiosis (5 simple, 1 advanced) four had symptoms. All three biopsy specimens showed varying degrees of pulmonary fibrosis. DCO single breath was diminished in four of the six. One male dental technician had scleroderma and possibly Erasmus syndrome. Blind readings showed an increased number of suspicious chest x rays films (greater than or equal to category 0/1) among older smokers and ex-smokers (p = 0.013) regardless of occupation. Our results support other evidence that dental technicians are at risk of developing pneumoconiosis. Therefore, adequate hygienic control of dental laboratories is indicated.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Ahlberg J. E. The development of ethics in dentistry. Scand J Dent Res. 1981 Feb;89(1):1–5. doi: 10.1111/j.1600-0722.1981.tb01268.x. [DOI] [PubMed] [Google Scholar]
- Brune D., Beltesbrekke H., Melsom S. Dust in workroom air of dental laboratories. Swed Dent J. 1981;5(5-6):247–251. [PubMed] [Google Scholar]
- Carles P., Fabre J., Pujol M., Duprez A., Bollinelli R. Pneumoconioses complexes chez les prothésistes dentaires. Poumon Coeur. 1978;34(3):189–192. [PubMed] [Google Scholar]
- De Vuyst P., Vande Weyer R., De Coster A., Marchandise F. X., Dumortier P., Ketelbant P., Jedwab J., Yernault J. C. Dental technician's pneumoconiosis. A report of two cases. Am Rev Respir Dis. 1986 Feb;133(2):316–320. doi: 10.1164/arrd.1986.133.2.316. [DOI] [PubMed] [Google Scholar]
- Dosman J., Bode F., Urbanetti J., Martin R., Macklem P. T. The Use of a Helium-Oxygen Mixture during Maximum Expiratory Flow to Demonstrate Obstruction in Small Airways in Smokers. J Clin Invest. 1975 May;55(5):1090–1099. doi: 10.1172/JCI108010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hansen H. M. Silikose hos en tandtekniker. Ugeskr Laeger. 1983 Aug 1;145(31):2378–2379. [PubMed] [Google Scholar]
- Kilburn K. H. Cigarette smoking does not produce or enhance the radiologic appearance of pulmonary fibrosis. Am J Ind Med. 1981;2(3):305–308. doi: 10.1002/ajim.4700020311. [DOI] [PubMed] [Google Scholar]
- Kilburn K. H., Lilis R., Anderson H. A., Miller A., Warshaw R. H. Interaction of asbestos, age, and cigarette smoking in producing radiographic evidence of diffuse pulmonary fibrosis. Am J Med. 1986 Mar;80(3):377–381. doi: 10.1016/0002-9343(86)90709-6. [DOI] [PubMed] [Google Scholar]
- Knudson R. J., Bloom J. W., Kaltenborn W. T., Burrows B., Lebowitz M. D. Assessment of air vs helium-oxygen flow-volume curves as an epidemiologic screening test. Chest. 1984 Sep;86(3):419–423. doi: 10.1378/chest.86.3.419. [DOI] [PubMed] [Google Scholar]
- Knudson R. J., Slatin R. C., Lebowitz M. D., Burrows B. The maximal expiratory flow-volume curve. Normal standards, variability, and effects of age. Am Rev Respir Dis. 1976 May;113(5):587–600. doi: 10.1164/arrd.1976.113.5.587. [DOI] [PubMed] [Google Scholar]
- Leclerc P., Fiessinger J. N., Capron F., Ameille J., Rochemaure J. Syndrome d'Erasmus chez un prothésiste dentaire. Intérêt de la prévention des nuisances professionnelles. Ann Med Interne (Paris) 1983;134(7):653–655. [PubMed] [Google Scholar]
- Paré P. D., Brooks L. A., Coppin C. A., Wright J. L., Kennedy S., Dahlby R., Mink S., Hogg J. C. Density-dependence of maximal expiratory flow and its correlation with small airway disease in smokers. Am Rev Respir Dis. 1985 Apr;131(4):521–526. doi: 10.1164/arrd.1985.131.4.521. [DOI] [PubMed] [Google Scholar]
- Rom W. N., Lockey J. E., Lee J. S., Kimball A. C., Bang K. M., Leaman H., Johns R. E., Jr, Perrota D., Gibbons H. L. Pneumoconiosis and exposures of dental laboratory technicians. Am J Public Health. 1984 Nov;74(11):1252–1257. doi: 10.2105/ajph.74.11.1252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wesselius L. J., Witztum K. F., Taylor A. T., Hartman M. T., Moser K. M. Computer-assisted versus visual lung gallium-67 index in normal subjects and in patients with interstitial lung disorders. Am Rev Respir Dis. 1983 Dec;128(6):1084–1089. doi: 10.1164/arrd.1983.128.6.1084. [DOI] [PubMed] [Google Scholar]
- Zuskin E., Loke J., Bouhuys A. Helium-oxygen flow-volume curves in detecting acute response to hair spray. Int Arch Occup Environ Health. 1981;49(1):41–44. doi: 10.1007/BF00380807. [DOI] [PubMed] [Google Scholar]