

Dear Editor,
Schwannomas are slow-growing, benign, and well-encapsulated tumors composed of well-differentiated Schwann cells.[1] They may arise along the course of cranial nerve III to XII or any peripheral nerve.[1] Ninety-five percent of all schwannomas arise from the eighth cranial nerve.[1] An isolated palsy of the hypoglossal nerve is a very rare entity with a myriad of etiologies. Hypoglossal nerve schwannomas are the rarest among all cranial nerve schwannomas, with their imaging characteristics being limited to only case reports.[1] We report one such rare case of a hypoglossal nerve schwannoma presenting with occipital headache and ipsilateral genioglossus muscle palsy.
A 35-year-old female presented with persistent occipital headache, slowly progressive dysarthria, and impairment of tongue mobility since the last six months. There was no other relevant neurological history. On neurological examination, she had dysarthria with deviation of the tongue to the left side and hemiatrophy of the left half of the tongue [Figure 1]. The rest of the neurological examination was within normal limits. Magnetic resonance imaging (MRI) of the brain with contrast administration was then performed.
Figure 1.

Deviation of the tongue to the left side and hemiatrophy of the left half of the tongue
MRI brain with contrast showed a large dumbbell-shaped solid cystic lesion in the left perimedullary cistern along the course of the left hypoglossal nerve. The lesion appeared hyperintense on T2-weighted imaging (T2W) [Figure 2a, 2c] and iso- to hypo-intense on T1-weighted imaging (T1W) [Figure 2b]. On post contrast images, it showed heterogenous enhancement [Figure 2d]. Posteriorly, it was causing a mass effect over the medulla and cervico-medullary junction [Figure 2e]. Inferiorly, extra-foraminal extension was seen into the upper neck. The lesion was seen to be causing secondary expansion of the left hypoglossal canal and the underlying destruction of the left occipital condyle.
Figure 2.
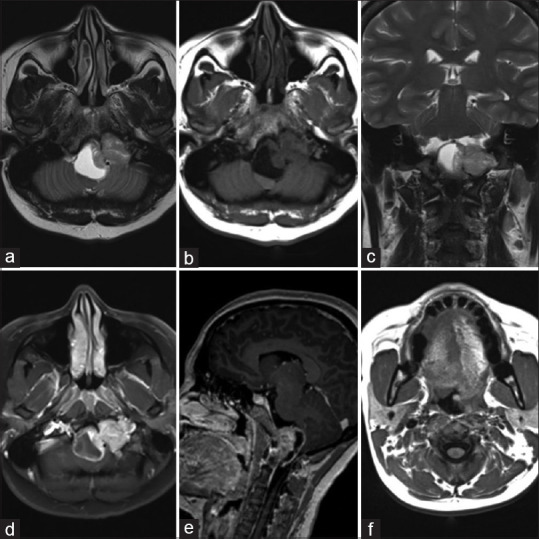
Large dumbbell-shaped solid cystic lesion in the left perimedullary cistern along the course of the left hypoglossal nerve appearing hyperintense on T2 (a, c) and iso- to hypo-intense on T1 (b). On post-contrast study, it showed heterogenous enhancement (d). Posteriorly, it was causing a mass effect over the medulla and cervico-medullary junction (e). Secondary hemiatrophy of the left half of the tongue with fatty infiltration and prolapse of left hemi-tongue into the oropharynx (f)
Secondary hemiatrophy of the left half of the tongue with fatty infiltration and prolapse of the left hemi-tongue into the oropharynx was also noted [Figure 2f].
The hypoglossal nerve arises from the hypoglossal nucleus in the medulla, passes through the hypoglossal canal, and provides motor fibers innervating the muscles of the tongue.[2]
The most common symptoms associated with hypoglossal schwannomas are headache and dizziness.[3,4] The most distinguishing clinical features of patients with hypoglossal nerve schwannoma are unilateral tongue atrophy and fasciculations.[5] Our patient presented with gradually progressive persistent occipital headache, slowly progressive dysarthria, and impairment of tongue mobility since the last six months. Clinical examination revealed atrophy of the left half of the tongue with deviation to the same side. These features pointed toward an isolated palsy of the left hypoglossal nerve.
On review of literature, we found that imaging characteristics of hypoglossal schwannomas have been largely limited to case reports.[6,7,8] A case series by Nonaka et al.[9] described hypoglossal schwannomas as hypointense on T1 and hyperintense on T2 with heterogenous post-contrast enhancement. Associated non-enhancing intralesional cystic foci have been previously reported in proven cases of hypoglossal schwannoma[6,7,8] with cystic foci most often developing within large tumors showing necrosis or spontaneous intratumoral hemorrhage.[6,7] Most of the hypoglossal neurinomas have a dumbbell shape and involve both intracranial and extracranial segment of the hypoglossal nerve.[10] In our case, further imaging revealed a large dumbbell-shaped solid cystic tumor along the course of the left hypoglossal nerve with associated widening of the left hypoglossal canal and underlying bony destruction. Imaging characteristics were found to be similar to these past case studies.
Our patient then underwent surgery for the same and the diagnosis was confirmed on histopathological examination of the postoperative specimen.
Isolated hypoglossal neuropathy is a rare entity. Tumor, infection, trauma of skull base, radiation, and vascular insult may cause isolated hypoglossal nerve palsy.[11]
In summary, hypoglossal nerve schwannomas are very rare tumors and preoperative diagnosis can be difficult. MRI is the most accurate diagnostic modality and plays a vital role in identification of the nerve of origin, its characteristics, and extent.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Osborn AG, Hedlund GL, Salzman KL. Salt Lake City: Amirsys; 2013. Osborn's brain: imaging, pathology, and anatomy. [Google Scholar]
- 2.Thomposn EO, Smoker WR. Hypoglossal nerve palsy: A segmental approach. Radiographics. 1994;14:939–58. doi: 10.1148/radiographics.14.5.7991825. [DOI] [PubMed] [Google Scholar]
- 3.Fujiwara S, Hachisuga S, Numaguchi Y. Intracranial hypoglossal neurinoma: Report of a case. Neuroradiology. 1980;20:87–90. doi: 10.1007/BF00339552. [DOI] [PubMed] [Google Scholar]
- 4.Morelli RJ. Intracranial neurilemmoma of the hypoglossal nerve. Review and case report. Neurology. 1966;16:709–13. doi: 10.1212/wnl.16.7.709. [DOI] [PubMed] [Google Scholar]
- 5.Okura A, Shigemori M, Abe T, Yamashita M, Kojima K, Noguchi S. Hemiatrophy of the tongue due to hypoglossal schwannoma shown by MRI. Neuroradiology. 1994;36:239–40. doi: 10.1007/BF00588142. [DOI] [PubMed] [Google Scholar]
- 6.Li WC, Hong XY, Wang LP, Ge PF, Fu SL, Luo YN. Large cystic hypoglossal schwannoma with fluid-fluid level: A case report. Skull Base. 2010;20:193–7. doi: 10.1055/s-0029-1246219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Takahashi T, Tominaga T, Sato Y, Watanabe M, Yoshimoto T. Hypoglossal neurinoma presenting with intratumoral hemorrhage. J Clin Neurosci. 2002;9:716–9. doi: 10.1054/jocn.2001.1109. [DOI] [PubMed] [Google Scholar]
- 8.Hoshi M, Yoshida K, Ogawa K, Kawase T. Hypo- glossal neurinoma: Two case reports. Neurol Med Chir (Tokyo) 2000;40:489–93. doi: 10.2176/nmc.40.489. [DOI] [PubMed] [Google Scholar]
- 9.Nonaka Y, Grossi PM, Bulsara KR, Tani-guchi RM, Friedman AH, Fukushima T. Micro- surgical management of hypoglossal schwanno-mas over 3 decades: A modified grading scale to guide surgical approach. Neurosurgery. 2011;69(2 Suppl Operative):ons121–40. doi: 10.1227/NEU.0b013e31822a547b. [DOI] [PubMed] [Google Scholar]
- 10.Jia G, Wang Z, Zhang J. Diagnosis and treatment ofhypoglossal neurinoma. Chung Hua I Hsueh Tsa Chih. 2001;81:1264–5. [PubMed] [Google Scholar]
- 11.Combarros O, Alvarez de Arcaya A, Berciano J. Isolated unilateral hypoglossal nerve palsy: Nine cases. J Neurol. 1998;245:98–100. doi: 10.1007/s004150050185. [DOI] [PubMed] [Google Scholar]