

Abstract
Aim
The Norwegian Action Plan for a Healthier Diet (2017–2021) set the target that 25% of infants should be exclusively breastfed for 6 months by 2022. Our aim was to determine trends in the prevalence and duration of breastfeeding in the municipality of Bergen.
Methods
Data on breastfeeding status in 2010–2018 were extracted from a standardised electronic medical record kept by public child health centres and recorded as exclusive, partial or none, at 6 weeks and 6 months of age.
Results
We found that 28,503 and 26,735 infants attended the 6‐week and 6‐month consultations, respectively. The prevalence of any breastfeeding was 92.0% at 6 weeks and 78.0% at 6 months with no trend over time between 2010 and 2018. The prevalence of exclusive breastfeeding at 6 weeks was 73.9% and stable over time, but it declined at 6 months, from 28.1% in 2010 to 11.1% in 2014 and remained stable thereafter.
Conclusion
During 2010–2018, the prevalence of any and exclusive breastfeeding at 6 weeks and any breastfeeding at 6 months was stable. Exclusive breastfeeding at 6 months declined halfway through the study period, to a stable, but low, prevalence of 11.1% by 2014.
Keywords: breastfeeding, guidelines, infant, prevalence, trends
Abbreviation
- WHO,
World Health Organization.
Key Notes.
Norwegian authorities recommend exclusive breastfeeding up to 6 months of age, and this study examined the prevalence in the municipality of Bergen between 2010 and 2018.
Standardised records from public child health centres showed that the prevalence of any breastfeeding was stable at 6 weeks and 6 months of age and that of exclusive breastfeeding also at 6 weeks.
Exclusive breastfeeding at 6 months declined halfway through the study period, to a stable, but low, prevalence.
1. BACKGROUND
Breastfeeding has important health benefits for mothers and children. 1 , 2 Promoting breastfeeding is an important part of the World Health Organization's (WHO) maternal and infant health policies and is reinforced by most national health authorities, including Norway. In line with current WHO recommendations, 3 Norwegian health authorities recommend exclusive breastfeeding for the first 6 months of life and partial breastfeeding until at least 12 months of age. 4 Exclusive breastfeeding means that the infant receives no other liquids or solids than breastmilk, except for vitamin D supplements. 5 However, complementary solid feeding may be introduced from around 4 months of age if the intake of breastmilk is considered inadequate. 4
The Norwegian Action Plan for a Healthier diet (2017–2021), published by the Ministry of Health and Care Services in 2017, introduced the target that 25% of mothers should exclusively breastfeed their infants for the first 6 months by 2022. 6 National surveys had reported a downward trend in exclusive breastfeeding in Norway at the age of 5.5 months, from 12% in 2006 to 5% in 2018–2019. 7 , 8 The participation rate in these two studies were 67% and 73%, respectively, and the maternal educational level was above the national average, which is a common bias in such surveys. 9 In contrast, population‐based registers tend to have a low risk of selection bias as they prospectively collect clearly defined data on a large number of subjects. In 2010, the Bergen municipality implemented an electronic medical record called HealthProfile 0–20 (Visma, Bergen, Norway) to enable a standardised registration of health information collected at the child health centres. For example, breastfeeding is routinely registered as exclusive, partial or none. A previous study, based on HealthProfile 0–20 data, found that, in 2010–11, information on the duration of breastfeeding until 6 months of age was available for approximately 86% of the infants in the municipality. 10
The aim of the current study was to use the database to investigate annual trends in the prevalence of any and exclusive breastfeeding during the first 6 months of life from 2010 to 2018.
2. METHODS
2.1. Study population
Data on breastfeeding were extracted from HealthProfile 0–20 for all children who attended one of the 19 public child health centres in the municipality of Bergen, Norway, between 1 January 2010 and 31 December 2018. Bergen is the second largest city in Norway with a population of 279,792 (1 January 2018). The data related to breastfeeding at the 6‐week and 6‐month visits took place between 5–8 weeks and 24–30 weeks, respectively. Infants who did not attend the visits during those age ranges were excluded from the analyses and so were those with unknown breastfeeding status.
2.2. Registration and extraction of data
HealthProfile 0–20 is a template used by public child health centres to systematically collect age‐appropriate information on current health issues, including growth, nutrition, psychomotor development and suspected or confirmed illnesses. The Norwegian Directorate of Health guidelines state that children should be monitored during routine consultations at 6 weeks, 6 months and 2, 6, 8 and 13 years of age. 11 Public health nurses and physicians record information on structured, age‐specific electronic forms. The data can then be extracted for health surveillance and epidemiologic research. The current analyses are based on data on infant feeding, which was recorded by the public health nurse at the 6‐week and 6‐month visits. The options were exclusive breastfeeding, partial breastfeeding or no breastfeeding. The present analyses focus on data on any breastfeeding and the subgroup of exclusive breastfeeding.
2.3. Statistical analysis
Data were grouped by the year of registration, from 2010 to 2018, and by the scheduled 6‐week and 6‐month visits. The annual prevalence of breastfeeding at the age of 6 weeks and 6 months was estimated with a linear adjustment for the actual age at the time of the consultation, within the accepted variations of 5–8 weeks and 24–30 weeks, respectively. Trends in the prevalence of breastfeeding over time were adjusted for the child's age at the time of the visit, using multiple linear regression. Results are expressed as the absolute difference in prevalence from 1 year to the next, with 95% confidence intervals (95% CI). The time trend for exclusive breastfeeding was estimated with a single breakpoint using segmented, broken stick regression with the segmented package in R version 4.0 (The R Foundation).
2.4. Ethics
The project was approved by the Regional Committee for Medical and Health Research Ethics in Western Norway (ref. 2010/3276/REK vest).
3. RESULTS
Approximately 99% of all infants in Bergen attended the structured programme of visits at the public child health centres from 2010 to 2018. Data on breastfeeding were used, according to the study protocol, for 94.6% of the infants who attended the 6‐week visit and for 90.6% who attended the 6‐month visit.
A total of 30,131 infants attended the 6‐week visit during the study period and 28,505 (94.6%) were examined between 5 and −8 weeks of age. Breastfeeding data were missing for 2 of these infants, leaving 28,503 (51.4% boys) eligible for the analysis (Figure S1A). The majority (83.3%) of these infants were examined at 6 or 7 weeks of age. The age‐adjusted prevalence of exclusive breastfeeding at the 6‐week visits ranged from 72.2% to 75.4% during the study period and any breastfeeding ranged from 91.4% to 93.0% (Table 1, Figure 1). There was no significant trend by year of examination for exclusive (−0.2% difference between successive years; 95% CI −0.8 to 0.3%; p = 0.3) or any breastfeeding (95% CI −0.1%; −0.4–0.1%; p = 0.3).
TABLE 1.
Age‐adjusted percentage (95% CI) of infants who were breastfed at 6 weeks and 6 months of age by the year of registration
| Breastfeeding at 6 weeks | 6 months | |||||
|---|---|---|---|---|---|---|
| n | Exclusive | Any | n | Exclusive | Any | |
| 2010 | 3163 | 75.4 (73.5–77.1) | 92.0 (90.8–93.0) | 2873 | 28.8 (26.8–30.9) | 78.7 (76.7–80.6) |
| 2011 | 3201 | 75.4 (73.6–77.2) | 93.0 (91.9–94.0) | 2782 | 22.9 (21.0–24.9) | 82.3 (80.4–84.1) |
| 2012 | 3085 | 73.6 (71.6–75.4) | 91.4 (90.2–92.6) | 2806 | 22.8 (20.9–24.8) | 82.6 (80.7–84.3) |
| 2013 | 3123 | 73.5 (71.7–75.3) | 92.4 (91.3–93.4) | 2900 | 17.3 (15.6–19.1) | 75.6 (73.6–77.5) |
| 2014 | 3175 | 72.2 (70.3–74.0) | 91.6 (90.4–92.7) | 3030 | 11.1 (9.8–12.5) | 76.9 (75.0–78.7) |
| 2015 | 3261 | 72.3 (70.0–74.5) | 91.4 (89.9–92.7) | 3081 | 11.9 (10.5–13.3) | 76.0 (74.1–77.8) |
| 2016 | 3354 | 74.4 (72.1–76.5) | 91.4 (89.9–92.7) | 3283 | 11.0 (9.7–12.4) | 75.9 (74.0–77.7) |
| 2017 | 3056 | 73.5 (71.1–75.8) | 91.7 (90.1–93.1) | 3024 | 10.3 (9.0–11.6) | 78.1 (76.2–79.8) |
| 2018 | 3085 | 75.3 (73.1–77.5) | 92.6 (91.1–93.9) | 2956 | 13.1 (11.6–14.6) | 77.4 (75.5–79.3) |
| Total | 28,503 | 73.9 (73.3–74.6) | 92.0 (91.6–92.4) | 26,735 | 16.1 (15.6–16.7) | 78.0 (77.4–78.6) |
FIGURE 1.
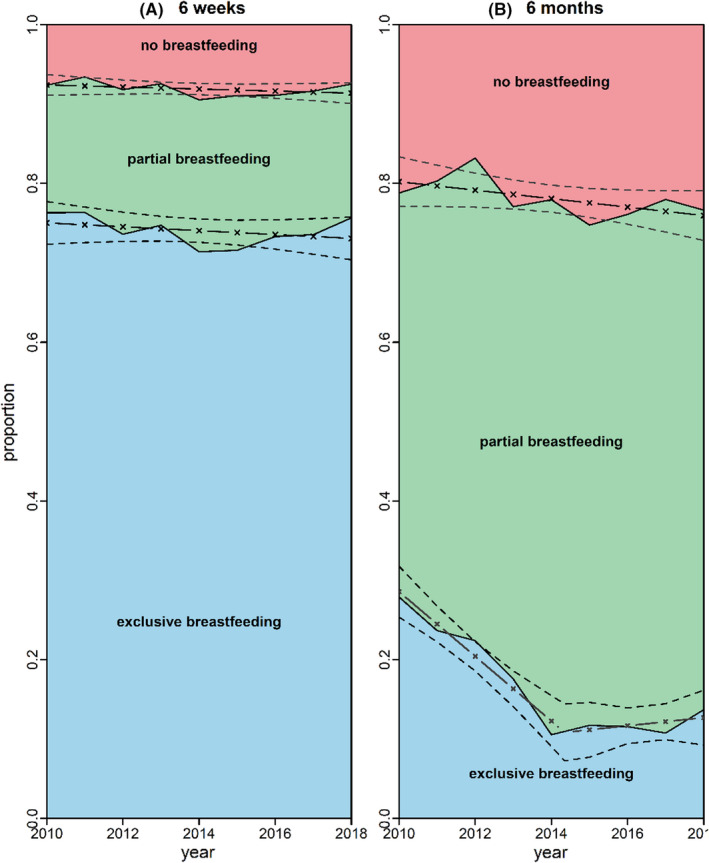
Annual age‐adjusted prevalence of breastfeeding at 6 weeks (left panel) and 6 months (right panel) of age. The trend over time was not statistically significant for exclusive (−0.2%, −0.8–0.3%), (p = 0.3) or any (−0.1%, −0.4–0.1%), (p = 0.3) breastfeeding at 6 weeks of age
In total, 29,519 infants attended the 6‐month consultation and 27,411 (92.9%) of them were examined at the eligible age range of 24–30 weeks. The breastfeeding category was recorded for 26,735 (90.6%) of all infants (51.5% boys) (Figure S1B). Most (86.4%) of the infants were examined at 26 or 27 weeks of age. The prevalence of any breastfeeding ranged between 75.6% and 82.6% during the study period, with a small but statistically significant decrease in 0.5% (0.3%–0.7%; p < 0.001) per year over time (Table 1, Figure 1). The age‐adjusted prevalence of exclusive breastfeeding decreased considerably from 28.8% in 2010 and reached its lowest level, of 10.3%, in 2017. The prevalence of exclusive breastfeeding decreased markedly during the first 4 years but not after 2014. Segmented regression analysis estimated the break to be during the year 2014. The annual decrease between 2010 and 2014 was 3.3% (2.9%–3.7%), but there was no significant trend thereafter (−0.2% per year, −0.7%–0.3%).
4. DISCUSSION
The overall breastfeeding rate in Bergen was high in comparison with international data, and earlier surveys suggest it was similar to the national Norwegian average. 10 There has been a long Norwegian tradition of recognising breastfeeding as the optimal way to feed infants, and mothers receive substantial encouragement to initiate and maintain breastfeeding. Despite this, the prevalence of exclusive breastfeeding at 6 months had declined by the end of the 2010–2018 study period instead of increasing to reach the national goal of 25% by 2022. 6 Bergen failed to even approach the goal, even though several programmes that encouraged breastfeeding were initiated. These included the creation of mother and baby‐friendly obstetric departments, and the gradual implementation of baby‐friendly community health services in all the public child health centres. Both programmes endorsed the good breastfeeding practices laid out by the WHO and United Nations Children's Fund in the Ten Steps for Successful Breastfeeding. 12 Furthermore, the mothers could also benefit from the free breastfeeding guidance offered by a national voluntary organisation. 13 Similar trends and even less exclusive breastfeeding at 6 months have been reported by other Norwegian surveys published in 2008 and 2020. 7 , 8
The underlying causes of the decline in long‐term exclusive breastfeeding are not known, and the data presented by this study does not allow any conclusive interpretations on causal relationships. However, it is relevant to highlight some changes in policies and practice during the 2010–2018 study period. Most of the women included in this study gave birth at Haukeland University Hospital, known to be a mother and baby‐friendly obstetric department since 1994. There were ongoing debates about postpartum care and breastfeeding guidance in the department during the study period. Factors such as adhering to guidelines, practical assistance and staffing may have varied, and this may have had an impact on breastfeeding practices.
The Bergen municipality established the first baby‐friendly community health services in two of the centres in 2010 and all 19 child health centres were offering this by the end of 2015. A Norwegian cluster quasi‐randomised controlled trial including data from 2032 mothers from 54 municipalities in six counties, suggested that baby‐friendly initiatives increased the likelihood of exclusive breastfeeding until 6 months. 14 These interventions may have been effective in promoting breastfeeding, compared with previous routine care, by slowing down, but not halting, the downward trends in exclusive breastfeeding 6 months of age. However, this is just speculation, as we did not have a control group.
We believe, however, that research contradicting some of the claimed benefits of exclusive breastfeeding up to 6 months may have been of particular significance for the decline. Studies suggest that it does not prevent allergies and infections 15 , 16 and may lead to inadequate vitamin B12 17 and iodine 18 intake. Those findings were relevant to the ongoing revision of Norwegian breastfeeding guidelines published 2016 and revised in 2017. 4 The main controversy among healthcare professionals was whether to encourage exclusive breastfeeding for 6 months or recommend the introduction of complementary solids from 4 months of age. The national guidelines concluded that exclusive breastfeeding for 6 months was safe if the baby thrived, and the mother felt comfortable with this. They also stated that complementary solid food could be introduced from the age of 4 months if needed. 4 The controversy surrounding the revised guidance was discussed widely in public at the time and may have influenced women's individual choices regarding exclusive breastfeeding during this period of their infants' lives.
A national survey published in 2020 showed that only 5% of the 2182 mothers breastfed exclusively at 5.5 months. 8 However, that study was biased because highly educated women were overrepresented, and the results could suggest that well‐educated women choose to discontinue exclusive breastfeeding early.
Most high‐income countries, like Norway, fall short of the international recommendation to provide exclusive breastfeeding until 6 months of age. 19 However, although most high‐income countries have increased their rate of any and exclusive breastfeeding at 6 months of age during the last two decades, 19 our study found a decreasing prevalence.
4.1. Strengths and limitations
The main strength of the current study was that we included continuously recorded data from a routine healthcare programme that covered virtually all infants from the Bergen municipality, a large region likely to be representative of Norway as a whole. The risk of selection bias was low. It has previously been shown that collecting information on breastfeeding from mothers was a reliable indicator of actual practice. 20 , 21 The limitations were that we did not have information on the mothers' socioeconomic status or motives for their breastfeeding choices. This would have allowed us to carry out in‐depth analyses on the probable causes of the observed trends. Furthermore, we did not have any information about breastfeeding between 6 weeks and 6 months. However, the last national survey in 2018–19, which used retrospectively collected maternal reports, showed a more rapid decline in exclusive breastfeeding after 4 months of age. 8
5. CONCLUSION
During 2010–2018, the prevalence of any and exclusive breastfeeding in the Norwegian municipality of Bergen was stable at 6 weeks, and that of any breastfeeding also at 6 months. Exclusive breastfeeding declined halfway through the study period, to a stable, but low, prevalence. This drop occurred even though national programmes were in place to promote exclusive breastfeeding. This decline in exclusive breastfeeding in Norway has not been observed in most high‐income countries and further studies are needed to clarify this unexpected discrepancy.
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare.
Supporting information
Fig S1
ACKNOWLEDGEMENTS
We would like to thank the healthcare nurses who registered the data in the HealthProfile 0‐20 application.
Revheim I, Balthasar MR, Akerkar RR, et al. Trends in the prevalence of breastfeeding up to 6 months of age using structured data from routine child healthcare visits. Acta Paediatr. 2023;112:100–105. doi: 10.1111/apa.16367
Funding information
This study did not have any external funding.
REFERENCES
- 1. Chowdhury R, Sinha B, Sankar MJ, et al. Breastfeeding and maternal health outcomes: a systematic review and meta‐analysis. Acta Paediatr. 2015;104(467):96‐113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Mosca F, Giannì ML. Human milk: composition and health benefits. Pediatr Med Chir. 2017;39(2):155. [DOI] [PubMed] [Google Scholar]
- 3. World Health Organization . The optimal duration of exclusive breastfeeding: Report of an expert consultation. World Health Organization; 2001. https://apps.who.int/iris/bitstream/handle/10665/67219/WHO_NHD_01.09.pdf?ua=1. Accessed November 12, 2021. [Google Scholar]
- 4. The Norwegian Direcorate of Health . The National Guidelines – Infant feeding practices. The Ministry of Health and Care Services; First published October 11, 2016. https://www.helsedirektoratet.no/retningslinjer/spedbarnsernaering. Accessed November 11, 2021. [Google Scholar]
- 5. World Health Organization . Indicators for Assessing Infant and Young Child Feeding Practices: Conclusions of a Consensus Meeting held 6‐8 November 2007 in Washington DC, USA. World Health Organization; 2008. https://apps.who.int/iris/bitstream/handle/10665/43895/9789241596664_eng.pdf?sequence=1&isAllowed=y. Accessed November 12, 2021. [Google Scholar]
- 6. The Ministry of Health and Care Services . Norwegian Action Plan for a Healthier Diet – an outline. The Ministry of Health and Care Services. The Ministry of Health and Care Services of Norway; 2017. https://www.regjeringen.no/contentassets/fab53cd681b247bfa8c03a3767c75e66/norwegian_national_action_plan_for_a_healthier_diet_an_outline.pdf. Accessed November 12, 2021. [Google Scholar]
- 7. Øverby NC, Kristiansen AL, Andersen LF, Lande B. Spedkost – 6 måneder: Landsomfattende kostholdsundersøkelse blant 6 måneder gamle barn [Spedkost – 6 months: Nationwide dietary survey among infants aged 6 months]. The Norwegian Directorate of Health, the Nirwegian Food Safety Authority and the Univeristy of Olso; 2008. [Google Scholar]
- 8. Myhre JB, Andersen LF, Kristiansen AL. Spedkost 3. Landsomfattende undersøkelse av kostholdet blant spedbarn i Norge, 6 måneder [Spedkost 3. Nationwide dietary survey among infants in Norway, age 6 months]. The National Institute of Public Health of Norway and The University of Oslo; 2020. https://www.fhi.no/globalassets/dokumenterfiler/rapporter/2020/kostholdsundersokelser/spedkost‐3‐‐‐barn‐6‐mnd‐alder.pdf. Accessed November 12, 2021. [Google Scholar]
- 9. Henderson M, Page L. Appraising the evidence: what is selection bias? Evid Based Ment Health. 2007;10(3):67‐68. [DOI] [PubMed] [Google Scholar]
- 10. Halvorsen MK, Langeland E, Almenning G, et al. Breastfeeding surveyed using routine data. Tidsskr nor Legeforen. 2015;135(3):236‐241. [DOI] [PubMed] [Google Scholar]
- 11. The Norwegian Directorate of Health . Norwegian National Guidelines – Public Child Health Centers and School health care. The Ministry of Health and Services of Norway. https://www.helsedirektoratet.no/retningslinjer/helsestasjons‐og‐skolehelsetjenesten/. Accessed November 12, 2021. [Google Scholar]
- 12. World Health Organization, UNICEF . Protecting, promoting, and supporting breastfeeding in facilities providing maternity and newborn services: the revised Baby‐friendly Hospital Initiativ 2018 ‐ Implementation guidance. World Health Organization / UNICEF; 2018. https://apps.who.int/iris/bitstream/handle/10665/272943/9789241513807‐eng.pdf?sequence=19&isAllowed=y. Accessed November 12, 2021. [Google Scholar]
- 13. Ammehjelpen. www.ammehjelpen.no. Accessed November 12, 2021.
- 14. Bærug A, Langsrud Ø, Løland BG, Tufte E, Tylleskär T, Fretheim A. Effectiviness of baby‐friendly community health services on exclusive breastfeeding and maternal satisfaction: a pragmatic trial. Matern Child Nutr. 2016;12(3):428‐439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Du Toit G, Fong R‐X, Lack G. Prevention of food allergy – early dietary interventions. Allergol Int. 2016;65(4):370‐377. [DOI] [PubMed] [Google Scholar]
- 16. Størdal K, Lundeby KM, Brantsæter AL, et al. Breast‐feeding and infant hospitalization for infections: large cohort and sibling analysis. J Pediatr Gastroentrol Nutr. 2017;65(2):225‐231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Torsvik IK, Ueland PM, Markestad T, Midttun Ø, Bjørke Monsen AL. Motor development related to duration of exclusive breastfeeding, B vitamin status and B12 supplementation in infants with a birth weight between 2000–3000 g, results from a randomized intervention trial. BMC Pediatr. 2015;15:218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Mulrine HM, Skeaff SA, Ferguson EL, Gray AR, Valeix P. Breast‐milk iodine concentration declines over the first 6 mo postpartum in iodine‐deficient women. Am J Clin Nutr. 2010;92(4):849‐856. [DOI] [PubMed] [Google Scholar]
- 19. Vaz JS, Maia MFS, Neves PAR, Santos TM, Vidaletti LP, Victora C. Monitoring breastfeeding indicators in high‐income countries: levels, trends and challenges. Matern Child Nutr. 2021;17(3):e13137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Li R, Scanlon KS, Serdula MK. The validity and reliability of maternal recall of breastfeeding practice. Nutr Rev. 2005;63(4):103‐110. [DOI] [PubMed] [Google Scholar]
- 21. Natland ST, Andersen LF, Nilsen TI, Forsmo S, Jacobsen GW. Maternal recall of breastfeeding duration twenty years after delivery. BMC Med Res Methodol. 2012;12:179. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Fig S1