

Abstract
Objectives
There is limited information on how a change in patients' expectations over time results in symptom change in psychotherapy. This study aimed to investigate the changes in patients' expectations and symptoms during treatment and across follow‐up as well as to determine the within‐ and between‐patient relationships between two types of patient expectations, that is, self‐efficacy and outcome expectation, and symptom change.
Methods
Participants (80 participants × 6 repeated measures; 480 observations) with generalized anxiety disorder were treated using cognitive behavioral therapy and the within‐ and between‐patient scores of self‐efficacy and outcome expectation were evaluated in multilevel models as predictors of symptom change.
Results
Patients' self‐efficacy and outcome expectation increased, whereas severity of their symptoms reduced during and after treatment. At the within‐patient (WP) level, an increase in self‐efficacy was associated with a decrease in worry and depressive symptoms, and an increase in outcome expectation was associated with a decrease in depressive symptoms. The between‐patient (BP) effect, however, was contrary to the WP effect, that is, self‐efficacy was positively correlated with worry and outcome expectation was positively correlated with depressive symptoms
Conclusion
These results highlight the importance of disaggregating the WP variability from BP variability in psychotherapy process–outcome research as they exhibit different associations at the within‐ and between‐patient levels. Clinical Trial Registration: ClinicalTrial.gov (NCT03079336).
Keywords: between‐patient association, generalized anxiety disorder, outcome expectation, self‐efficacy, symptom reduction, within‐patient association
1. INTRODUCTION
Patient expectations have long been known to play a key role in successful psychotherapy (Goldfried, 1980; Wampold & Flückiger, 2022). Frank and Frank (1991) argued that for any therapy to be effective, the patient must have mobilization of the belief in the ability to improve. From this perspective, one of the main areas of focus of psychotherapy is to encourage and develop patients' adaptive expectations and to revise their maladaptive expectations (Constantino & Westra, 2012; Greenberg et al., 2006; Kirsch, 1990). Outcome expectation (OE) and self‐efficacy (SE) are two types of such adaptive expectations. OE reflects a patient's belief that engaging in a particular treatment will improve the outcome (i.e., alleviate symptoms and improve functioning; Constantino et al., 2018), whereas generalized SE refers to an individual's belief in their capacity to behave as necessary to achieve specific performance goals in everyday life, for example, handle difficult life situations (Bandura, 1977; Scholz et al., 2002).
SE is a robust predictor of better treatment outcomes in eating disorders, depression, and anxiety (Clarke et al., 2014; Keshen et al., 2017; Pinto et al., 2008). In a comprehensive meta‐analysis, patient‐rated treatment OE before or during early treatment was associated with better posttreatment outcome across varied therapies and diagnoses (weighted r = 0.18; 95% CI: [0.14−0.22]; Constantino et al., 2018). However, despite the extensive research on the initial OE and SE levels, there is limited knowledge of how OE changes over the treatment course (Brown et al., 2014; Meyerhoff & Rohan, 2016; Newman & Fisher, 2010; Thiruchselvam et al., 2019; Vîslă et al., 2019; Vîslă & Constantino, 2021), and only few studies have examined changes in patient SE during psychotherapy (Brown et al., 2014; Keshen et al., 2017). Moreover, even less information is available on how a change in these constructs is associated with improvement in symptoms (Brown et al., 2014; Newman & Fisher, 2010).
For instance, in patients with generalized anxiety disorder (GAD), Newman and Fisher (2010) found that the rate of change in OE across multiple therapy sessions can predict the reduction in GAD severity after cognitive behavioral therapy (CBT). Pre‐ to posttreatment changes in SE precede symptom reduction (Bouchard et al., 2007) and predict symptom improvement after treatment (Bandura & Adams, 1977; Black et al., 2012). In a study that examined both OE and SE in terms of psychotherapy outcomes, Brown et al. (2014) revealed that OE and SE increase over the treatment course, and such increase significantly predicts symptom reduction and functioning improvement. However, despite OE and SE being related constructs (Bandura, 1977), Brown et al. (2014) did not simultaneously study OE and SE as predictors of outcome improvement. This allows testing for the unique associations between the two expectation types and symptom reductions. Therefore, investigating the degree to which the increase in OE and SE during CBT simultaneously predicts symptom reductions will provide a better understanding of the impact of patients' cognition on their symptoms. Furthermore, the study by Brown et al. (2014) comprised patients with various anxiety diagnoses, and it is unclear whether these relations would be the same when studying other homogeneous groups, such as patients with specific anxiety disorders (e.g., GAD). A recent meta‐analysis (Constantino et al., 2018) found no significant moderation effect of diagnosis on the association between OE and outcome; therefore, one could argue that the effects should also be similar within anxiety disorders. However, more disorder‐specific studies are required to draw such a conclusion.
Previous research (Bauer & Curran, 2011; Wang & Maxwell, 2015) and particularly psychotherapy research (Falkenström et al., 2013; Rubel et al., 2017, 2019) have indicated the importance of disentangling within‐individuals and between‐individuals variance components. Between‐patient (BP) associations focus on comparisons between patients, whereas within‐patient (WP) effects focus on comparisons between measurements obtained from the same patient at different time points, for example, WP variation in a construct that occurs over time (Bolger & Laurenceau, 2013). Simply focusing on the associations at the BP level does not necessarily account for the association WP. Analyzing the BP associations will increase our knowledge of important variables that distinguish patients from each other, whereas analyzing the WP associations will provide insights into the dynamic associations between variables and their dependence on situational circumstances and life contexts (Bolger & Laurenceau, 2013). Examining associations at the WP level allows us to better understand how the changes and variations in expectations are manifested in everyday life among patients and how they are associated with symptom improvement.
Regarding the constructs of interest in the current study, one study conducted on patients with GAD disentangled the WP from BP levels when investigating OE‐outcome association (Constantino & Aviram, 2020). In this study, testing the indirect effect of OE on outcome (i.e., worry) through therapeutic alliance, higher OE was related with worry reduction at the WP level, while at the BP level the association between OE and worry reduction was not significant. Moreover, to the best of our knowledge, there has been no prior research disentangling the WP from BP effects in the SE‐outcome association during psychotherapy. However, despite the lack of research distinguishing the two analysis levels in the case of SE, we provided a few theoretical assumptions in this study. At the WP level, the relations could be similar with the results on OE found in the study of Constantino and Aviram (2020) and with the relations evidenced when WP effects are not distinguished from BP effects but are usually interpreted as they were WP effects (see studies included in the meta‐analyses of Clarke et al., 2014; Constantino et al., 2018). Specifically, OE or hope for improvement increase at some point during therapy could be associated with symptom reduction. This negative relation between treatment OE and symptoms might be explained by the therapeutic alliance quality (Constantino & Aviram, 2020, Constantino & Coyne, 2020; Vîslă et al., 2018) and patient involvement with the therapeutic techniques, such as cognitive restructuring and behavior activation (Webb et al., 2013). Similarly, an increase in the belief in one's ability to handle difficult life situations (i.e., generalized SE) could be associated with symptom reduction. Similar to OE, SE is hypothesized to enhance the motivation to get involved in a task, the degree of effort invested in that specific task, and persistence despite aversive experiences (Bandura, 1982, 2018; Eccles & Wigfield, 2002; Maddux et al., 1982; Scholz et al., 2002).
Although the only study disentangling WP from BP effects when investigating the OE‐outcome association found a nonsignificant BP effect of OE on outcome (Constantino & Aviram, 2020), considering that in the current study the simultaneous predictive effect of OE and SE on outcome is investigated, at least three different associations might emerge. First, similar to the relations hypothesized at the WP level (when not disaggregating the WP from BP effects), patients with high SE and OE show less symptom severity on average. Second, an increased tendency to worry might be positively correlated with a general belief in one's ability to handle difficult daily situations (i.e., generalized SE). According to the Contrast avoidance model (Llera & Newman, 2014; Newman & Llera, 2011), patients with GAD tend to worry to maintain a constant level of negative emotions (and controllability over emotional experiences; Vîslă & Zinbarg, 2021), thereby avoiding emotional contrasts (in preparation for future dangers). To avoid negative contrasts, patients with GAD might have realized that if they are prepared enough (i.e., constantly worrying), they could handle any difficult problem that they might encounter (e.g., “No matter what comes my way, I'm usually able to handle it”). Based on the same rationale, on average, patients with GAD with high OE over the treatment course might show more depressive symptoms because the anticipation of something positive might be against their usual thinking pattern (i.e., worrying that something “bad” could happen just to be prepared for possible future dangers and avoid emotional contrast; Llera & Newman, 2014). Third, at the BP level, expectations and symptom improvement are unrelated. A nonsignificant relationship between OE and outcome was identified in several studies that did not separate the WP effects from the BP ones (Borkovec et al., 2002; Steketee et al., 2011). Moreover, the only study disentangling WP from BP effects when investigating the OE‐outcome association found a nonsignificant BP effect of OE on outcome (Constantino & Aviram, 2020). In summary, several studies have found increases in OE and SE to be associated with symptom reduction (Brown et al., 2014; Newman & Fisher, 2010). However, as none of these studies disaggregated the WP from BP effects (at least for SE; for OE, see Constantino & Aviram, 2020), it is unclear whether these results apply to the clinically relevant WP level.
1.1. The current study
The first aim of the current study was to describe the changes in SE, OE, worry, and depressive symptoms in patients receiving CBT for GAD. While the changes in OE were examined during treatment, the changes in SE and symptoms were examined during treatment and across follow‐up. Based on previous studies (Brown et al., 2014; Newman & Fisher, 2010; Vîslă et al., 2019), we hypothesized that patients would exhibit improvements in SE, OE, and symptoms over time. In the current study, we focused on worry and depressive symptoms as worry is the main diagnostic criterion for GAD, and GAD is often associated with an increased risk of developing major depressive disorder (Kessler et al., 1999). Specifically, meta‐analytic evidence shows that anxiety disorders, including GAD, are a risk factor for developing later depression, and vice versa (Jacobson & Newman, 2017). Moreover, there is an overlap in core symptoms between GAD and major depressive disorder (e.g., difficulty concentrating, feeling keyed up, or on edge; Zbozinek et al., 2012).
Furthermore, considering that patient adaptive expectations, such as SE and OE, are actively targeted during mental health interventions (Constantino & Westra, 2012; Greenberg et al., 2006; Kirsch, 1990) and that patient symptoms do not seem to substantially improve after an intervention had ended (in general, Flückiger et al., 2014, 2015; Podina et al., 2019; and particularly in GAD—Flückiger et al., 2022), we expected the change in investigated variables to differ depending on the study phase, that is, a more pronounced change during the intervention than after intervention. 1
The second and main aim of the current study was to investigate whether changes in SE and OE are uniquely associated with changes in worry and depressive symptoms. Thus, we tested the simultaneous predictive effect of SE and OE changes on worry and depressive symptom changes, disentangling WP effects from BP effects in these correlated changes. Based on the assumption that positive expectations stimulate the effort toward achieving desired goals by enhancing the motivation to get involved and persist in a task (Bandura, 1982, 2018; Eccles & Wigfield, 2002; Greenberg et al., 2006), we expected that WP, improvements in SE and OE would be associated with improvements in worry and depressive symptoms. However, the question of whether these associations would be significant (and in what direction) at the BP level was exploratory. However, three potential outcomes may emerge. First, a similar correlation pattern with the one at the WP level could be established, that is, an average improvement in SE and OE over the study course would be associated with few overall symptoms (Clarke et al., 2014; Constantino et al., 2018). Second, based on the assumptions of the Contrast avoidance model of GAD (Newman & Llera, 2011), an increased tendency to worry might be associated with a general belief in one's ability to handle difficult daily situations (i.e., generalized SE; e.g., “No matter what comes my way, I'm usually able to handle it”). Based on the same rationale, patients with GAD with high treatment OE over the treatment course might show more depressive symptoms on average (as expecting something positive to happen might be against their thinking pattern of expecting the worst, which prepares them for possible future dangers; Llera & Newman, 2014). Third, expectations and outcomes might be unrelated at the BP level, considering similar results obtained when there was no disaggregation (Borkovec et al., 2002; Steketee et al., 2011) or when the BP association between OE and outcome was disaggregated from the WP association (Constantino & Aviram, 2020).
2. MATERIALS AND METHODS
2.1. Setting
This novel study reanalyses the data from a randomized controlled trial comparing a prolonged focus on change (PFC) condition versus state of the art (SOTA) condition in GAD (Flückiger et al., 2021; ClinicalTrials.gov Identifier: NCT03079336). Both conditions were based on the Mastery of your Anxiety and Worry package (MAW‐package; Craske & Barlow, 2006; Zinbarg et al., 2006), a widely used CBT approach. The MAW package for GAD typically comprises psychoeducation, relaxation training and/or mindfulness exercises, cognitive restructuring, and imagery and in vivo situational exposure. In both conditions, treatment included 16 sessions plus 3 booster sessions within 12 months, with the only difference being that the focus on changes in the check‐in phase of each session was prolonged in the PFC condition. Results from the original analyses revealed that the PFC condition showed faster symptom reduction in terms of worry during therapy and until the 12‐month follow‐up than the SOTA implementation (Flückiger et al., 2021). Given the focus of the current study, analyses were performed for the overall samples while we adjusted for the implementation condition.
2.2. Participants
2.2.1. Patients
Of the 343 patients initially screened for trial eligibility, 80 were included for treatment at Psychotherapy Outpatient Clinic of the University of Zurich's Department of Psychology (for more details about the selection procedure, see Flückiger et al., 2021). Patients who (a) fulfilled the diagnostic criteria for GAD based on the structured interview for Diagnostic and Statistical Manual (DSM‐5; Black & Grant, 2014), (b) were aged ≥18 years, (c) had sufficient knowledge of the German language, and (d) provided informed consent were included in the study. Patients who (a) had a score of ≥2 on the suicide item of the Beck Depression Inventory–Second Edition (BDI‐II; Beck et al., 1996) and/or had active suicidal thoughts during the diagnostic screening interview, (b) were currently receiving medication for psychotic or bipolar disorder treatment, or (c) were currently receiving treatment from a professional psychotherapist were excluded from the study. Patients receiving prescribed medications for anxiety or depressive disorders were not excluded from the study provided the dosage of their medication remained constant for at least 1 month. The mean sample (N = 80) age was 31.4 years (standard deviation [SD] = 11.0 years). Women represented 75% of the participants, whereas men represented 25%. The majority of the participants were generally well‐educated (57.5% with a Bachelor's degree), belonged to the middle class (mean of $81,000 annual household income), and indicated a high comorbidity rate with other psychological disorders (58%). All participants were Caucasian and 39% had a foreign background (for the complete patients' characteristics at intake see Flückiger et al., 2021).
2.2.2. Therapists
A total of 20 graduate‐level psychologists were recruited from local postgraduate CBT training centers. Therapists and supervisors were trained according to the most recent version of the MAW package in an initial 16 h workshop presented by one of the MAW‐package co‐authors (Craske & Barlow, 2006; Zinbarg et al., 2006). Additionally, therapists participated in a 2 h study supervision in small groups on a biweekly basis. Most therapists attended additional individualized CBT supervision as part of their postgraduate training protocol (200 h supervision and 600 h practice‐based workshop are required to obtain a psychotherapy license in Switzerland). Therapists were crossed over the two treatment conditions, and each therapist treated four patients, two under the PFC condition and two under the SOTA condition (ABAB design) 2 . The mean age of the therapists was 30.9 years (SD = 6.9 years). Of those, 90% identified as women and 10% identified as men; all were Caucasian. For the complete baseline characteristics of patients and therapists, see Flückiger et al. (2021).
2.3. Measures
2.3.1. Generalized SE
The Generalized Self‐Efficacy Scale (GSE; Schwarzer & Jerusalem, 1995) was used to measure generalized SE. GSE comprises 10 items rated from 1 (“not at all true”) to 4 (“exactly true”), yielding a total score between 10 and 40. Similar to the situation‐specific SE investigated by Bandura (1977), GSE measures the belief in one's ability to respond to novel or difficult situations and deal with any associated obstacles (Schwarzer & Jerusalem, 1995). Examples of items are presented as following: “Thanks to my resourcefulness, I know how to handle unforeseen situations” (item 5), “When I am confronted with a problem, I can usually find several solutions” (item 8), and “No matter what comes my way, I'm usually able to handle it” (item 10). GSE scale, originally developed in German and then translated to multiple languages, has shown good psychometric properties in various countries (Luszczynska et al., 2005; Scholz et al., 2002). In line with the literature (Scholz et al., 2002), Cronbach's α for the current sample was α > 0.78.
2.3.2. OE
The Hope of Improvement subscale of Therapy Expectation and Evaluation scale (PATHEVH; Schulte, 2005) was used to measure treatment OE. This subscale comprises four items rated from 1 (absolutely wrong) to 5 (absolutely right), for example, “I'm afraid I can't even be helped by psychotherapy” (item 1), “I believe my problems can finally be solved” (item 4), “Even with therapy, my problems will not change very much” (item 5), and “Actually, I'm rather skeptical about whether treatment can help me” (item 9). Items 1, 5, and 9 are reversed‐scored before summing all items. The possible score range for this subscale is from 4 to 20, with higher scores reflecting more positive OE or hope for improvement. PATHEVH demonstrates satisfactory reliability in patients with depression and anxiety (Schulte, 2005; 2008; Vîslă et al., 2019; Vîslă et al., 2021). The internal consistency for the current sample was α > 0.76.
2.3.3. Worry
The Penn State Worry Questionnaire (PSWQ; Meyer et al., 1990) was used to evaluate worry frequency and intensity. PSWQ is a 16‐item self‐reporting measure in which items are rated on a scale from 1 to 5, with higher scores indicating greater worry (range: 16−80). PSWQ showed good psychometric properties (Meyer et al., 1990) with an internal consistency of α > 0.86 for the current sample.
2.3.4. Depression
The German version of BDI‐II (Beck et al., 1996), which is a widely used 21‐item measure, was used to assess depressive symptoms. The item scores range from 0 to 3, with higher scores reflecting more depression (range: 0−63). German BDI‐II has previously shown satisfactory internal consistency (α = 0.89 and 0.93) and test−retest reliability (r tt = 0.78), good convergent and discriminant validity, and good sensitivity to change (Kühner et al., 2007). The internal consistency for the current sample was α > 0.89.
2.3.5. Control variables
In all our models, we adjusted for several variables, including patient intake symptoms (i.e., worry and depressive symptoms), the presence of comorbidity (yes/no), and treatment conditions (SOTA vs. PFC).
2.4. Procedure
All participants, regardless of the intervention condition, were asked to complete the assessments six times during the study. The baseline assessment was conducted before treatment, two assessments were conducted during the treatment phase (at session 5 and session 10), one assessment was conducted at the end of the intervention (at session 16), and two assessments after the intervention had ended (at 6 months after treatment completion [follow‐up 1] and at 12 months after treatment completion [follow‐up 2]). We converted months to weeks to maintain a consistent unit of time. Therefore, baseline assessment was coded as T0, the two assessments during the intervention were coded as T5 and T10, the assessment at the end of the intervention was coded as T16, and the two assessments after the intervention had ended were coded as T40 and T64.
2.5. Analytic strategy
2.5.1. Power analysis
The present study focused on WP effects using 480 observations (80 participants × 6 repeated measures). We conducted a power analysis assuming a traditional analysis of variance with repeated measures to assure adequate power, within factors with an estimated effect size of d = 0.20, 80% power at p = 0.05, and six repeated measures. This power analysis suggested a sample size of at least 64 participants. Thus, the sample size of the present study provided enough power to detect the WP effects.
2.5.2. Data analytic strategy
We used longitudinal multilevel models (Bolger & Laurenceau, 2013) and the lme4 package (Bates et al., 2015) in R software (R Core Team, 2021) to test our two study aims, given that the data structure included repeated assessments of SE, OE, and symptoms (level 1) nested within patients (level 2), which were nested within their therapists (level 3). Compared with the more traditional analyses, these models account for multiple dependencies in repeated measures from the same patients and therapists (Raudenbush & Bryk, 2002). We investigated the hierarchical data structure by computing intraclass correlation coefficients and analyzed the total variation proportion that was accounted for by BP and WP variation. During the intervention phase, we found that 70% of total SE variance, 58% of total OE variance, 27% of total worry variance, and 44% of total depressive symptoms variance was BP. At postintervention phase, it was found that 67% of total SE variance, 71% of total worry variance, and 70% of total depressive symptoms variance was BP. In each phase, the remaining variance in the respective variables was WP. Moreover, there were also differences among therapists in the investigated variables (see Supporting Information: Table S1 Online Supplemental Material). A graphical illustration of each patient's SE over time and an overall SE growth trajectory is presented in Supporting Information: Figure S1.
The three‐level multilevel models were estimated with random intercepts and time slopes. Model comparison testing the inclusion or exclusion of random effects for certain variables was conducted using Akaike Information Criterium (Akaike, 1973) and log‐likelihood ratio test. When contrasting different models, the model allowing patients to randomly vary in terms of intercept (i.e., random‐intercepts‐fixed‐slopes model) fitted the data better than a model fixing the intercept as constant across patients (these results were consistent across different variables; see Supporting Information: Table S3, Online Supplemental Material). We then determined whether there was significant time variation among patients by estimating a model with a random slope for time (i.e., random‐intercepts‐random‐slopes model). The model with random slopes fitted the data better than the model without the random slopes (Supporting Information: Table S3).
We added a dummy coded variable for study phase (0 = intervention; 1 = postintervention) to the multilevel models to examine the effect of the study phase (intervention phase [time 0, 5, 10, 16] vs. postintervention phase [time 16, 40, 64]) and to describe the change in our variables over time (study aim 1). Additionally, a time by phase interaction term was added to the models on changes in SE, worry, and depressive symptoms to examine whether the change in these variables differed between the two study phases. Time was coded linearly (in weeks) across the study period from 0 = first measurement occasion (i.e., before treatment start) to 64 = last measurement occasion (i.e., 12‐months follow‐up). Further, we tested quadratic models to examine possible nonlinear trajectories of change. When comparing the fit indices of the linear and quadratic change over time, the linear slopes showed the best fit for both the intervention and postintervention phases. Therefore, we used linear models.
We tested the simultaneous predictive effect of changes in OE and SE on change in symptoms using multilevel models to determine whether changes in both patients' OE and SE predicted the change in symptoms (study aim 2). We decomposed these predictors into BP and WP parts (Bolger & Laurenceau, 2013) to account for both inter‐ and intraindividual variation in patients' OE and SE. The BP part refers to the aggregated mean of all observations within a patient and how much this differs from the sample mean. The WP part refers to the raw value obtained at each measurement occasion and how much these differ from the patient mean. This decomposition was applied to explore the variability in the fluctuations of the investigated variables from assessment occasion to assessment occasion by simultaneously controlling for BP differences (i.e., mean value). The BP OE and SE were centered on the grand mean (i.e., patients' scores above or below the sample mean), and the WP variables were centered on the patient‐mean (i.e., above or below the patient's time‐specific score; Bolger & Laurenceau, 2013). All four components (WP SE, BP SE, WP OE, BP OE) were simultaneously included as predictors in a single model. Therefore, two models were conducted to answer study aim 2, one predicting worry and the other one predicting depression.
In all models (testing study aims 1 and 2), we ajusted for symptoms at baseline/intake (i.e., worry and depression), the presence of comorbidities (no/yes), and intervention condition (SOTA vs. PFC). The control variables were included in all models as level‐2 predictors of the intercepts.
3. RESULTS
3.1. How fast do changes in SE, OE, worry, and depressive symptoms occur? (study aim 1)
Supporting Information: Table S2 shows the descriptive statistics of all investigated variables at different assessment points during the study. Table 1 presents the results of the linear multilevel model of changes in SE, OE, worry, and depressive symptoms over time. The fixed effects in Table 1 can be thought of as the effects for a typical patient. The results indicate that SE and OE significantly increased over time, whereas worry and depressive symptoms significantly decreased over time. The time by phase interaction term indicates that the amount and direction of change differed between the intervention and postintervention phases. In particular, the increase in SE and the decrease in worry and depression were more pronounced during the intervention than at postintervention (note that OE was measured only during the intervention).
Table 1.
Fixed effects parameter estimates of change in SE, OE, worry, and depressive symptoms over time
| Fixed effects | GSE | PATHEVH | PSWQ | BDI‐II |
|---|---|---|---|---|
| Intercept | ||||
| γ (SE) | 29.87 (3.22) | 12.34 (2.05) | 25.45 (4.62) | 15.72 (4.32) |
| t | 9.29*** | 6.02*** | 5.51*** | 3.64*** |
| Linear time | ||||
| γ (SE) | 0.23 (0.04) | 0.07 (0.02) | −1.06 (0.10) | −0.75 (0.08) |
| t | 6.10*** | 3.09** | −10.99*** | −9.66*** |
| Phase | ||||
| γ (SE) | 2.31 (0.45) | ‐ | −13.83 (1.13) | −8.51 (0.91) |
| t | 5.08*** | 12.20*** | −9.32*** | |
| Time x Phase | ||||
| γ (SE) | −0.19 (0.04) | ‐ | 1.02 (0.10) | 0.73 (0.08) |
| t | −5.02*** | 10.32*** | 9.21*** | |
| Baseline PSWQ | ||||
| γ (SE) | −0.04 (0.05) | 0.07 (0.03) | 0.54 (0.07) | −0.12 (0.07) |
| t | −0.77 | 1.98 | 7.17*** | −1.67 |
| Baseline BDI‐II | ||||
| γ (SE) | −0.11 (0.05) | −0.08 (0.03) | 0.02 (0.07) | 0.45 (0.07) |
| t | −2.12* | −2.35* | 0.28 | 6.69*** |
| Comorbidity | ||||
| γ (SE) | −1.99 (0.82) | −0.08 (0.53) | 2.90 (1.19) | 2.74 (1.10) |
| t | −2.42* | −0.16 | 2.27* | 2.48* |
| Condition | ||||
| γ (SE) | 1.10 (0.75) | 0.18 (0.51) | 1.61 (1.16) | −1.07 (1.00) |
| t | 1.47 | 0.36 | 1.39 | −1.08 |
Abbreviations: BDI‐II, Beck Depression Inventory—Second Edition; GSE, General Self‐Efficacy Scale; OE, outcome expectation; PATHEVH, Therapy Expectation and Evaluation scale, Hope of Improvement subscale; PSWQ, Penn State Worry Questionnaire; SE, self‐efficacy.
p < 0.05;
p < 0.01;
p < 0.001.
For example, a typical patient showed an initial level (intercept) of 29.89 from a total possible total score of 40 in SE. The significant fixed effect of time demonstrates that a typical patient showed an increase of 0.23 in SE at each time period across the study. Moreover, the significant fixed effect of phase shows that the two study phases differed significantly, that is, the intercept of the postintervention phase was 2.31 times higher than the intercept of the intervention phase. Further, the fixed effect of time by phase indicates that a typical patient demonstrated a larger SE increase during the intervention phase than during the postintervention phase. Regarding the control variables, baseline depression severity and the presence of comorbidity showed significant effects (whereas baseline worry and treatment condition had no significant impact on how SE changed over time). In particular, high depression severity at baseline was associated with less SE at pretreatment (intercept). The presence of comorbidity was also associated with a low SE intercept.
3.2. Do changes in SE and OE account for changes in symptoms and do these correlated changes differ at between‐ and within‐patient levels? (study aim 2)
Table 2 presents the results of the multilevel models linking the changes in SE and OE with the changes in worry and depressive symptoms. At the WP level, changes in SE over time were negatively associated with changes in worry and depressive symptoms; particularly, at a certain measurement occasion, high levels of SE were associated with low levels of worry and depressive symptoms. Moreover, an increase in OE was associated with a decrease in depressive symptoms (but not in worry). However, the BP effect was contrary to the WP‐effect, that is, SE was positively associated with worry (but not with depressive symptoms). This result indicates that across the entire study, the high levels of SE were associated with the high levels of worry. Moreover, OE was positively associated with depressive symptoms (but not with worry) at the BP level. 3
Table 2.
Linking change in SE and OE to change in worry and depressive symptoms
| Fixed effects | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Intercept | Linear time | WP SE | BP SE | WP OE | BP OE | Baseline PSWQ | Baseline BDI‐II | Comorbidity | Condition | |
| PSWQ | ||||||||||
| γ (SE) | 28.80 (5.78) | −0.80 (0.07) | −0.46 (0.17) | 0.32 (0.16) | −0.35 (0.23) | 0.18 (0.25) | 0.56 (0.07) | −0.02 (0.07) | 1.55 (1.15) | 1.38 (1.11) |
| t | 4.97*** | −10.65*** | −2.74** | 1.99* | −1.50 | 0.77 | 7.57*** | −0.28 | 1.35 | 1.24 |
| BDI‐II | ||||||||||
| γ (SE) | 16.64 (5.61) | −0.45 (0.07) | −0.55 (0.13) | 0.26 (0.16) | −0.49 (0.19) | 0.52 (0.24) | −0.07 (0.07) | 0.38 (0.07) | 2.33 (1.15) | −0.95 (1.04) |
| t | 2.97** | −6.84*** | −4.06*** | 1.69 | −2.64** | 2.14* | −0.98 | 5.29*** | 2.02* | −0.91 |
Abbreviations: BDI‐II, Beck Depression Inventory—Second Edition; BP, between‐patient; GSE, General Self‐Efficacy Scale; OE, Outcome expectation; PATHEVH, Therapy Expectation and Evaluation scale, Hope of Improvement subscale; PSWQ, Penn State Worry Questionnaire; SE, self‐efficacy; WP, within‐patient.
p < 0.05;
p < 0.01;
p < 0.001.
For example, as shown in Table 2, a typical patient showed an initial level (intercept) of 28.80 from a total possible score of 80 in worry (as measured using PSWQ). The significant fixed effect of time indicates that a typical patient showed a decrease of −0.80 in worry at each time point across the study. Moreover, the significant fixed effect of within SE indicates that at a certain measurement occasion, high levels of worry were associated with a −0.46 unit lower level of SE, and the significant fixed effect of between SE indicates that a high level of worry was associated with a 0.32 unit higher level of SE on average. We plotted the results of these models predicting worry (Figure 1) and depressive symptoms (Figure 2) to illustrate these findings.
Figure 1.
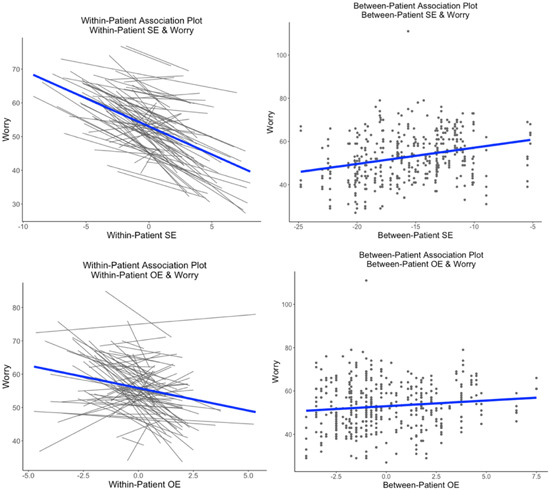
Model predicting worry using between‐ and within‐patient level predictors of self‐efficacy (SE) and outcome expectation (OE), adjusting for baseline worry, depression, presence of comorbidity, and treatment condition. Note that the plot is not actually using the model output—so it is just an approximation of the exact model (using geom_smooth embedded within ggplot)
Figure 2.
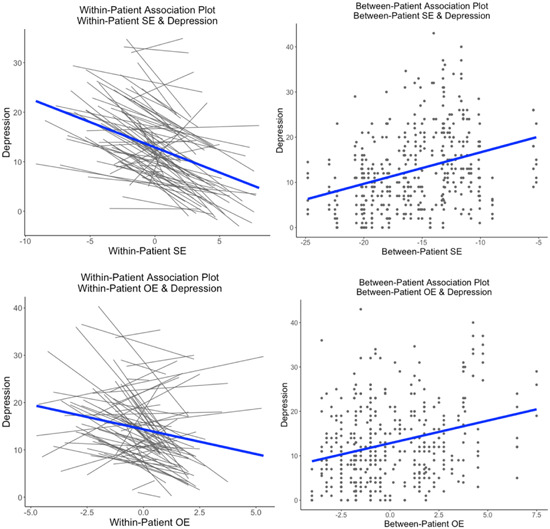
Model predicting depression using between‐ and within‐patient level predictors of self‐efficacy (SE) and outcome expectation (OE), adjusting for baseline worry, depression, presence of comorbidity, and treatment condition. Note that these plots are not actually using the model output—so it is just an approximation of the exact model (using geom_smooth embedded within ggplot)
4. DISCUSSION
The current study aimed to describe the changes in SE, OE, worry, and depressive symptoms in patients with GAD during CBT treatment and across follow‐up (OE was measured only during treatment). Further, this study aimed to investigate whether the simultaneous SE and OE changes are associated with worry and depressive symptom changes by disentangling WP effects from BP effects in these correlated changes. As expected, patients showed improvement in SE, OE, worry, and depressive symptoms over time and showed greater improvement in these during treatment than across follow‐up. Moreover, at the WP level, improvements in SE and OE over time were associated with improvements in symptoms. However, at the BP level, high SE and more positive OE across the entire study were associated with high symptom levels. These results clearly underscore the significance of examining the associations at both WP and BP levels. We have discussed these results in more detail below.
Although extensive research investigating patients' initial SE (Clarke et al., 2014; Keshen et al., 2017; Pinto et al., 2008) and OE (Constantino et al., 2018) levels exists, there is limited information on how these patients' cognition change during treatment, especially the change in SE (for a discussion on change in OE in the current sample, see Vîslă et al., 2021). In the present study, we found that SE improved during CBT treatment for GAD, which is consistent with the results of two other studies that investigated SE change during treatment (Brown et al., 2014; Keshen et al., 2017). However, unlike the present study, the study by Brown et al. (2014) included patients with various anxiety disorders. Moreover, in the study by Keshen et al. (2017), group treatment incorporating different therapy models (i.e., CBT, acceptance and commitment therapy, and dialectical behavior therapy) was used to treat patients with eating disorders. Previous research also investigated pre‐ to posttreatment increase in SE in socially anxious heavy drinkers (Black et al., 2012) and patients with panic attacks (Bouchard et al., 2007). Our findings show that CBT treatment for patients with GAD may increase their belief in their ability to face difficult situations in daily life. Moreover, our study adds to the limited literature demonstrating that different treatment approaches/formats influence growth in patients' SE across various clinical diagnoses. Notably, our study investigated SE in handling difficult and challenging situations in everyday patient life (i.e., generalized SE; Schwarzer & Jerusalem, 1995), which is more similar to the type of SE assessed by Keshen et al. (2017) (i.e., SE in employing specific coping strategies when facing life challenges) compared with other studies that mostly assessed SE change in handling symptoms (e.g., drink refusal SE, SE in handling panic attacks, SE regarding anxiety treatment; Bouchard et al., 2007; Brown et al., 2014. Black et al., 2012). Most importantly, the consistent results across these studies, including the current one, indicate that psychotherapy can increase patients' belief in their ability to handle their own symptoms and difficult and challenging situations in everyday life.
However, it should be noted that linear change in SE is the average estimated pattern in the current sample, and there is variability around the pattern, as with any change pattern across a sample. As presented in Supporting Information: Figure S1, some patients' belief in their ability to handle difficult and challenging situations in their life showed a lower increase compared to the overall SE growth trajectory, did not increase at all, or even decreased during therapy. These patients with low or decreasing SE during treatment might particularly benefit from strategies designed to improve SE. Examples of such strategies include actively praising small and intermediate successes, eliminating barriers through problem‐solving training, and reframing perceived failures, all of which are motivational interviewing and strength‐based techniques (Chou et al., 2009; Flückiger et al., 2010). Bandura suggested that the most powerful strategy for improving SE is approaching and coping with previously avoided situations (i.e., performance accomplishment; Bandura, 1997), which is accomplished using CBT, for example, through exposure techniques. Moreover, strategies that can decrease emotional tension, such as relaxation training, may improve SE (Bandura, 1997).
A strength of the current study is that the change in SE and symptoms was investigated both during treatment and across follow‐up. Interestingly, SE continued to increase after the end of the treatment (although the increase was less steep compared with that during treatment). To the best of our knowledge, this is the first study that examined the lasting psychotherapy effect on patients' generalized SE or belief in their own ability to deal with difficult situations in everyday life. This result indicates that psychotherapy for patients with GAD might have a long‐lasting influence on their belief in their ability to handle difficult or challenging situations in daily life (e.g., through relaxation training, exposure, and reframing perceived negative situations). However, before reaching any definite conclusions, future studies are needed to replicate the current results in other GAD samples as this is, to the best of our knowledge, the first study investigating the change in SE in a GAD sample. Moreover, worry and depressive symptoms continued to decrease across follow‐up, although the decrease was less pronounced than that during treatment. This is consistent with several meta‐analyses on long‐term psychotherapy efficacy (Flückiger et al., 2014, 2015, 2022; Podina et al., 2019). Future studies with larger sample size would provide the opportunity to use statistical analyses such as Piecewise Growth Curve Models (Bollen & Curran, 2006) to separate time into discrete phases of change to explain observed rates of change within each phase (Hoffman, 2015).
Notably, the WP and BP effects of expectations on symptoms not only differed from each other but also changed in opposite directions. The WP effects demonstrated that increasing patient SE might improve worrying and depressive symptoms, whereas fostering OE might be particularly beneficial in decreasing depressive symptoms. One possible reason for the significant association of OE with depression (and not with worry) in the current study could be that depression centrally involves a general feeling of hopelessness and negative expectation for change (DeVellis & Blalock, 1992). Therefore, the restoration of hope and positive expectations for improvement might decrease depressive feelings (rather than diminish worrying).
At the BP level, our results indicate that patients with firmer beliefs in their ability to handle difficult situations demonstrate high worry levels on average. This result might be explained by the tendency of patients with GAD to control how they might react to future danger by worrying to maintain a negative emotional state (by this approach, they avoid negative emotional contrasts; Newman & Llera, 2011). Therefore, in patients with GAD, SE might be a mechanism through which worry maintains negative mood (e.g., “No matter what comes my way, I'm usually able to handle it”). However, this assumption should be tested in future studies. Moreover, in patients with GAD, expecting something positive to happen might be against their usual thinking pattern (i.e., expecting the worst so as to be prepared in case something bad happens; Llera & Newman, 2014), which might explain the positive relation between OE and depressive symptoms that we found at the BP level. These results are contrary to the those of Constantino & Aviram (2020) that found no significant relation between OE and outcome at the BP level. A possible explanation for the contrary results might be that in the current study we investigated the predictive effect of both OE and SE simultaneously, types of expectations that might influence each other. However, some studies conducted outside psychotherapy suggest opposite directions at the within‐ versus between‐person level when investigating SE impact on performance (Bandura, 1982; Vancouver et al., 2002).
Our results exemplify the potential relevance of disentangling the WP from BP variability, that is, drawing conclusions at the WP level based on the findings obtained at the BP level could result in false recommendations for practitioners (Falkenström et al., 2013; Rubel et al., 2017; Zilcha‐Mano, 2021). From the positive BP associations between expectations and symptoms, if a therapist concludes that decreasing patient SE and positive OE would be a good strategy, our results indicate that this could have negative rather than positive effects on their patients' symptoms. The negative WP effect suggests that expectations (i.e., SE and OE) are important active ingredients of successful therapies, which therapists should try to increase rather than decrease. As a side note, although there was much less WP than BP variations in SE, we found that the WP SE increase was significantly associated with worry and depressive symptom reduction.
In particular, the WP associations can be translated to clinical recommendations for practitioners. Clinically, this result could indicate that even small variations in patients' belief in their ability to handle difficult situations during and after therapy could have an influence on patients' change in symptoms. Therefore, therapists should be attentive to patients' SE and OE changes (even though such changes may be small), as this might have an influence on symptom reduction. As previously assumed, increasing patient adaptive expectations, such as SE and OE, could stimulate patient's efforts toward achieving desired goals by enhancing motivation to get involved in psychotherapy and attend it despite the challenges (Bandura, 1982; Eccles & Wigfield, 2002; Greenberg et al., 2006). In clinical practice, it would be optimal to have both an increase in patient SE as well as OE relative to patient own average. However, if this patient overall level gets too high (which might be an indicator of unrealistic patient expectations), then this benefit could become a risk factor for poorer outcome. Therefore, clinicians should try to foster an increase in their patients SE and OE over time and at the same time be attentive to high overall SE and OE patients' levels and rework their unrealistic nature, when needed.”
Although speculative (as the focus of the current sample was not on investigating mediators of the SE/OE‐outcome association), a possible reason why SE and OE predict improvement in symptoms can be a good patient–therapist relationship. Research has shown that the relation between both SE and OE and outcome is mediated by the therapeutic alliance quality (Ilgen et al., 2006; Maisto et al., 2015; Vîslă et al., 2018). This indirect therapeutic alliance effect is consistent with goal theory (Eccles & Wigfield, 2002), which suggests that people will devote more resources to achieve a goal if they believe that they have a chance of attaining it. Accordingly, when a patient shows high SE levels and positive OE, this will be associated with a more collaborative working alliance with their therapist than when the patient shows low SE levels and more pessimistic OE (reported to patients' own SE and OE average), which, in turn, can improve the symptoms of that particular patient (Constantino et al., 2021; Wampold & Flückiger, 2022). Moreover, other mechanisms through which OE exerts its ameliorative influence on symptoms have been investigated, such as behavioral and cognitive skill usage (Webb et al., 2013) and greater patient homework compliance (Westra et al., 2007). However, most of these mechanisms have been investigated at the BP level. Future studies should consider investigating WP mediators of the relationship between expectations and symptoms.
The present study has several limitations. First, consistent with epidemiology research on the higher GAD prevalence in women than men (Vesga‐López et al., 2008), this study sample included more women (75%), and only Caucasian participants. Therefore, these patterns of results might be particularly relevant to Caucasian females. Second, the included sample was relatively young, and the investigated relations in this study might be different in an older GAD sample (Vîslă et al., 2022). Third, more measurement repetitions (even in the form of single items) and shorter measurement intervals are required to better understand the dynamic interplay between expectations and symptoms. Despite these limitations, the current study highlights the importance of disaggregating the WP from BP variability in psychotherapy process–outcome research and suggests that clinicians should try to foster an increase in patients SE and OE over time at the same time with being attentive to high overall SE and OE patients' levels which might become a risk factor for poor outcome.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
ETHICS STATEMENT
The study was approved by the Ethics Committee of the Canton of Zurich (BASEC. 2016–00773). All patients included in this study gave their approved consent to participate in the study.
PEER REVIEW
The peer review history for this article is available at https://publons.com/publon/10.1002/jclp.23407
Supporting information
Supporting information.
ACKNOWLEDGMENT
This study was supported by the Swiss National Science Foundation (Grant PP00P1_163702; PP00P1_190083, recipient: Christoph Flückiger). Open access funding provided by Universitat Zurich.
Vîslă, A. , Allemand, M. , & Flückiger, C. (2023). Within‐ and between‐patients associations between self‐efficacy, outcome expectation, and symptom change in cognitive behavioral therapy for generalized anxiety disorder. Journal of Clinical Psychology, 79, 86–104. 10.1002/jclp.23407
ENDNOTES
For the overall trial design and treatment outcomes see Flückiger et al. (2021). Furthermore, secondary analyses of predictors of OE change were investigated in Vîslă et al. (2021).
Due to personal reasons, one therapist only provided two therapies and the remaining two therapies were conducted by another therapist with six therapies. These two therapists were still crossed over conditions, meaning that both of them treated patients in both conditions. The analyses in the current paper were computed on the actual collected data where the within‐therapist factor was treated as two therapies by one therapist and six therapies by the other therapist.
As change in the investigated variables differed between the two study phases (i.e., intervention and postintervention), we rerun all the models presented in Table 2 separately for the two phases (at postintervention only with SE as predictor, as OE was assessed during the intervention only). The WP and BP results of the models looking at intervention versus postintervention did not differ from the results examining the two phases together.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Akaike, H. (1973). Information theory and an extension of the maximum likelihood principle. In Petrov B. N., & Csaki F. (Eds.), Second international symposium on information theory (p. 267e281). Academiai Kiado. [Google Scholar]
- Bandura, A. (1977). Social learning theory. Prentice‐Hall. [Google Scholar]
- Bandura, A. (1982). Self‐efficacy mechanism in human agency. American Psychologist, 37(2), 122–147. 10.1037/0003-066X.37.2.122 [DOI] [Google Scholar]
- Bandura, A. (1997). Self‐efficacy, the exercise of control. W. H. Freeman and Company. [Google Scholar]
- Bandura, A. (2018). Toward a psychology of human agency: Pathways and reflections. Perspectives on Psychological Science, 13(2), 130–136. 10.1177/1745691617699280 [DOI] [PubMed] [Google Scholar]
- Bandura, A. , & Adams, N. E. (1977). Analysis of self‐efficacy theory of behavioral change. Cognitive Therapy and Research, 1(4), 287–310. [Google Scholar]
- Bates, D. , Maechler, M. , Bolker, B. , & Walker, S. (2015). Fitting linear mixed‐effects models using lme4. Journal of Statistical Software, 67, 1–48. 10.18637/jss.v067.i01 [DOI] [Google Scholar]
- Bauer, D. J. , & Curran, P. J. (2011). Introduction to multilevel modeling. Curran‐Bauer Analytics. [Google Scholar]
- Beck, A. T. , Brown, G. , & Steer, R. A. (1996). Beck depression inventory–II manual. The Psychological Corporation. [Google Scholar]
- Black, D. W. , & Grant, J. E. (2014). DSM‐5™ guidebook: The essential companion to the diagnostic and statistical manual of mental disorders (5th ed). American Psychiatric Publishing, Inc. [Google Scholar]
- Black, J. J. , Tran, G. Q. , Goldsmith, A. A. , Thompson, R. D. , Smith, J. P. , & Welge, J. A. (2012). Alcohol expectancies and social self‐efficacy as mediators of differential intervention outcomes for college hazardous drinkers with social anxiety. Addictive Behaviors, 37(3), 248–255. 10.1016/j.addbeh.2011.10.004 [DOI] [PubMed] [Google Scholar]
- Bolger, N. , & Laurenceau, J. P. (2013). Intensive longitudinal methods. Guilford Press. [Google Scholar]
- Bollen, K. A. , & Curran, P. J. (2006). Latent curve models: A structural equation perspective. Wiley. [Google Scholar]
- Borkovec, T. D. , Newman, M. G. , Pincus, A. L. , & Lytle, R. (2002). A component analysis of cognitive‐behavioral therapy for generalized anxiety disorder and the role of interpersonal problems. Journal of Consulting and Clinical Psychology, 70(2), 288–298. 10.1037/0022-006X.70.2.288 [DOI] [PubMed] [Google Scholar]
- Bouchard, S. , Gauthier, J. , Nouwen, A. , Ivers, H. , Vallières, A. , Simard, S. , & Fournier, T. (2007). Temporal relationship between dysfunctional beliefs, self‐efficacy and panic apprehension in the treatment of panic disorder with agoraphobia. Journal of Behavior Therapy and Experimental Psychiatry, 38(3), 275–292. 10.1016/j.jbtep.2006.08.002 [DOI] [PubMed] [Google Scholar]
- Brown, L. A. , Wiley, J. F. , Wolitzky‐Taylor, K. , Roy‐Byrne, P. , Sherbourne, C. , Stein, M. B. , Sullivan, G. , Rose, R. D. , Bystritsky, A. , & Craske, M. G. (2014). Changes in self‐efficacy and outcome expectancy as predictors of anxiety outcomes from the CALM study. Depression and Anxiety, 31(8), 678–689. 10.1002/da.22256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chou, C. C. , Ditchman, N. , Pruett, S. R. , Chan, F. , & Hunter, C. (2009). Applications of social cognitive theory in psychosocial interventions. Springer. [Google Scholar]
- Clarke, J. , Proudfoot, J. , Birch, M. R. , Whitton, A. E. , Parker, G. , Manicavasagar, V. , & Hadzi‐Pavlovic, D. (2014). Effects of mental health self‐efficacy on outcomes of a mobile phone and web intervention for mild‐to‐moderate depression, anxiety and stress: Secondary analysis of a randomised controlled trial. BMC Psychiatry, 14(1), 1–10. 10.1186/s12888-014-0272-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Constantino, M. J. , Aviram, A. , Coyne, A. E. , Newkirk, K. , Greenberg, R. P. , Westra, H. A. , & Antony, M. M. (2020). Dyadic, longitudinal associations among outcome expectation and alliance, and their indirect effects on patient outcome. Journal of Counseling Psychology, 67(1), 40–50. 10.1037/cou0000364 [DOI] [PubMed] [Google Scholar]
- Constantino, M. J. , Coyne, A. E. , Goodwin, B. J. , Vîslă, A. , Flückiger, C. , Muir, H. J. , & Gaines, A. N. (2020). Indirect effect of patient outcome expectation on improvement through alliance quality: A meta‐analysis. Psychotherapy Research , 1–15. 10.1080/10503307.2020.1851058 [DOI] [PubMed]
- Constantino, M. J. , Vîslă, A. , Coyne, A. E. , & Boswell, J. F. (2018). A meta‐analysis of the association between patients' early‐treatment outcome expectation and their posttreatment outcomes. Psychotherapy, 55, 473–485. 10.1037/pst0000169 [DOI] [PubMed] [Google Scholar]
- Constantino, M. J. , & Westra, H. A. (2012). An expectancy‐based approach to facilitating corrective experiences in psychotherapy. In Castonguay L. G., & Hill C. E. (Eds.), Transformation in psychotherapy: Corrective experiences across cognitive, behavioral, humanistic, and psychodynamic approaches (pp. 121–139). American Psychological Association. [Google Scholar]
- Craske, M. G. , & Barlow, D. H. (2006). Mastery of your anxiety and worry. Workbook. Oxford University Press. [Google Scholar]
- DeVellis, B. M. , & Blalock, S. J. (1992). Illness attributions and hopelessness depression: The role of hopelessness expectancy. Journal of Abnormal Psychology, 101(2), 257–264. 10.1037/0021-843X.101.2.257 [DOI] [PubMed] [Google Scholar]
- Eccles, J. S. , & Wigfield, A. (2002). Motivational beliefs, values, and goals. Annual Review of Psychology, 53(1), 109–132. 10.1146/annurev.psych.53.100901.135153 [DOI] [PubMed] [Google Scholar]
- Falkenström, F. , Granström, F. , & Holmqvist, R. (2013). Therapeutic alliance predicts symptomatic improvement session by session. Journal of Counseling Psychology, 60(3), 317–328. 10.1037/a0032258 [DOI] [PubMed] [Google Scholar]
- Flückiger, C. , Cameratta, K. , Del Re, A. C. , Probst, G. , Vîslă, A. , Gómez‐Penedo, J.‐M. , & Wampold, B. E. (2022). The relative efficacy of bona fide cognitive behavioral therapy and applied relaxation for generalized anxiety disorder at follow‐up: A longitudinal meta‐analysis. Journal of Consulting and Clinical Psychology, 90, 339–352. [DOI] [PubMed] [Google Scholar]
- Flückiger, C. , Del Re, A. C. , Munder, T. , Heer, S. , & Wampold, B. E. (2014). Enduring effects of evidence‐based psychotherapies in acute depression and anxiety disorders versus treatment as usual at follow‐up—A longitudinal meta‐analysis. Clinical Psychology Review, 34(5), 367–375. 10.1016/j.cpr.2014.05.001 [DOI] [PubMed] [Google Scholar]
- Flückiger, C. , Del Re, A. C. , & Wampold, B. E. (2015). The sleeper effect: Artifact or phenomenon—A brief comment on Bell et al. (2013). Journal of Consulting and Clinical Psychology, 83(2), 438–442. 10.1037/2Fa0037220 [DOI] [PubMed] [Google Scholar]
- Flückiger, C. , Vîslă, A. , Wolfer, C. , Hilpert, P. , Zinbarg, R. E. , Lutz, W. , grosse Holtforth, M. , & Allemand, M. (2021). Exploring change in cognitive‐behavioral therapy for generalized anxiety disorder—A two‐arms ABAB crossed‐therapist randomized clinical implementation trial. Journal of Consulting and Clinical Psychology, 89(5), 454–468. 10.1037/ccp0000639 [DOI] [PubMed] [Google Scholar]
- Flückiger, C. , Wüsten, G. , Zinbarg, R. E. , & Wampold, B. E. (2010). Resource activatio—Nusing clients' own strengths for psychotherapy and counseling. Hogrefe. [Google Scholar]
- Frank, J. D. , & Frank, J. B. (1991). Persuasion and healing: A comparative study of psychotherapy (3rd ed.). The Johns Hopkins Press. [Google Scholar]
- Goldfried, M. R. (1980). Toward the delineation of therapeutic change principles. American Psychologist, 35, 991–999. 10.1037/0003-066X.35.11.991 [DOI] [PubMed] [Google Scholar]
- Greenberg, R. P. , Constantino, M. J. , & Bruce, N. (2006). Are expectations still relevant for psychotherapy process and outcome? Clinical Psychology Review, 26, 657–678. 10.1016/j.cpr.2005.03.002 [DOI] [PubMed] [Google Scholar]
- Hoffman, L. (2015). Longitudinal analysis: Modeling within‐person fluctuation and change. Routledge. [Google Scholar]
- Ilgen, M. , Tiet, Q. , Finney, J. , & Moos, R. H. (2006). Self‐efficacy, therapeutic alliance, and alcohol‐use disorder treatment outcomes. Journal of Studies on Alcohol and Drugs, 67(3), 465–472. 10.15288/jsa.2006.67.465 [DOI] [PubMed] [Google Scholar]
- Jacobson, N. C. , & Newman, M. G. (2017). Anxiety and depression as bidirectional risk factors for one another: A meta‐analysis of longitudinal studies. Psychological Bulletin, 143(11), 1155–1200. 10.1037/bul0000111 [DOI] [PubMed] [Google Scholar]
- Keshen, A. , Helson, T. , Town, J. , & Warren, K. (2017). Self‐efficacy as a predictor of treatment outcome in an outpatient eating disorder program. Eating Disorders, 25(5), 406–419. 10.1080/10640266.2017.1324073 [DOI] [PubMed] [Google Scholar]
- Kessler, R. C. , DuPont, R. L. , Berglund, P. , & Wittchen, H. U. (1999). Impairment in pure and comorbid generalized anxiety disorder and major depression at 12 months in two national surveys. American Journal of Psychiatry, 156(12), 1915–1923. [DOI] [PubMed] [Google Scholar]
- Kirsch, I. (1990). Changing expectations: A key to effective psychotherapy. Brooks/Cole. [Google Scholar]
- Kühner, C. , Bürger, C. , Keller, F. , & Hautzinger, M. (2007). Reliabilität und validität des revidierten beck‐depressionsinventars (BDI‐II) [reliability and validity of the revised beck depression inventory (BDI‐II): findings from German‐language samples]. Der Nervenarzt, 78(6), 651–656. 10.1007/s00115-006-2098-7 [DOI] [PubMed] [Google Scholar]
- Llera, S. J. , & Newman, M. G. (2014). Rethinking the role of worry in generalized anxiety disorder: Evidence supporting a model of emotional contrast avoidance. Behavior Therapy, 45, 283–299. 10.1016/j.beth.2013.12.011 [DOI] [PubMed] [Google Scholar]
- Luszczynska, A. , Scholz, U. , & Schwarzer, R. (2005). The general self‐efficacy scale: Multicultural validation studies. The Journal of Psychology, 139(5), 439–457. 10.3200/JRLP.139.5.439-457 [DOI] [PubMed] [Google Scholar]
- Maddux, J. E. , Sherer, M. , & Rogers, R. W. (1982). Self‐efficacy expectancy and outcome expectancy: Their relationship and their effects on behavioral intentions. Cognitive Therapy and Research, 6(2), 207–211. [Google Scholar]
- Maisto, S. A. , Roos, C. R. , O'Sickey, A. J. , Kirouac, M. , Connors, G. J. , Tonigan, J. S. , & Witkiewitz, K. (2015). The indirect effect of the therapeutic alliance and alcohol abstinence self‐efficacy on alcohol use and alcohol‐related problems in project MATCH. Alcoholism: Clinical and Experimental Research, 39(3), 504–513. 10.1111/acer.12649 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer, T. J. , Miller, M. L. , Metzger, R. L. , & Borkovec, T. D. (1990). Development and validation of the Penn State worry questionnaire. Behaviour Research and Therapy, 28(6), 487–495. 10.1016/0005-7967(90)90135-6 [DOI] [PubMed] [Google Scholar]
- Meyerhoff, J. , & Rohan, K. J. (2016). Treatment expectations for cognitive‐behavioral therapy and light therapy for seasonal affective disorder: Change across treatment and relation to outcome. Journal of Consulting and Clinical Psychology, 84(10), 898–906. 10.1037/ccp0000121 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Newman, M. G. , & Fisher, A. J. (2010). Expectancy/credibility change as a mediator of cognitive behavioral therapy for generalized anxiety disorder: Mechanism of action or proxy for symptom change. International Journal of Cognitive Therapy, 3, 245–261. 10.1521/ijct.2010.3.3.245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Newman, M. G. , & Llera, S. J. (2011). A novel theory of experiential avoidance in generalized anxiety disorder: A review and synthesis of research supporting a contrast avoidance model of worry. Clinical Psychology Review, 31, 371–382. 10.1016/j.cpr.2011.01.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pinto, A. M. , Heinberg, L. J. , Coughlin, J. W. , Fava, J. L. , & Guarda, A. S. (2008). The eating disorder recovery self‐efficacy questionnaire (EDRSQ): Change with treatment and prediction of outcome. Eating Behaviors, 9(2), 143–153. 10.1016/j.eatbeh.2007.07.001 [DOI] [PubMed] [Google Scholar]
- Podina, I. R. , Vîslă, A. , Fodor, L. A. , & Flückiger, C. (2019). Is there a sleeper effect of exposure‐based vs. cognitive‐only intervention for anxiety disorders? A longitudinal multilevel meta‐analysis. Clinical Psychology Review, 73, 101774. 10.1016/j.cpr.2019.101774 [DOI] [PubMed] [Google Scholar]
- Raudenbush, S. W. , & Bryk, A. S. (2002). Hierarchical linear models: Applications and data analysis methods (2nd ed.). Sage Publications. [Google Scholar]
- R Core Team (2021). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/ [Google Scholar]
- Rubel, J. A. , Hilpert, P. , Wolfer, C. , Held, J. , Vîslă, A. , & Flückiger, C. (2019). The working alliance in manualized CBT for generalized anxiety disorder: Does it lead to change and does the effect vary depending on manual implementation flexibility? Journal of Consulting and Clinical Psychology, 87, 989–1002. 10.1037/ccp0000433 [DOI] [PubMed] [Google Scholar]
- Rubel, J. A. , Rosenbaum, D. , & Lutz, W. (2017). Patients' in‐session experiences and symptom change: Session‐to‐session effects on a within‐and between‐patient level. Behaviour Research and Therapy, 90, 58–66. 10.1016/j.brat.2016.12.007 [DOI] [PubMed] [Google Scholar]
- Scholz, U. , Doña, B. G. , Sud, S. , & Schwarzer, R. (2002). Is general self‐efficacy a universal construct? Psychometric findings from 25 countries. European Journal of Psychological Assessment, 18(3), 242–251. 10.1027/1015-5759.18.3.242 [DOI] [Google Scholar]
- Schulte, D. (2005). Messung der Therapieerwartung und Therapieevaluation von Patienten (PATHEV) [assessment of treatment expectancy and treatment evaluation]. Zeitschrift für klinische Psychologie und Psychotherapie, 34(3), 176–187. [Google Scholar]
- Schwarzer, R. , & Jerusalem, M. (1995). Generalized self‐efficacy scale. In Weinman J., Wright S., & Johnston M. (Eds.), Measures in health psychology: A user's portfolio. Causal and control beliefs (pp. 35–37). NFER‐NELSON. [Google Scholar]
- Steketee, G. , Siev, J. , Fama, J. M. , Keshaviah, A. , Chosak, A. , & Wilhelm, S. (2011). Predictors of treatment outcome in modular cognitive therapy for obsessive—Compulsive disorder. Depression and Anxiety, 28(4), 333–341. 10.1002/da.20785 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thiruchselvam, T. , Dozois, D. J. , Bagby, R. M. , Lobo, D. S. , Ravindran, L. N. , & Quilty, L. C. (2019). The role of outcome expectancy in therapeutic change across psychotherapy versus pharmacotherapy for depression. Journal of Affective Disorders, 251, 121–129. 10.1016/j.jad.2019.01.046 [DOI] [PubMed] [Google Scholar]
- Vancouver, J. B. , Thompson, C. M. , Tischner, E. C. , & Putka, D. J. (2002). Two studies examining the negative effect of self‐efficacy on performance. Journal of Applied Psychology, 87(3), 506–516. 10.1037/0021-9010.87.3.506 [DOI] [PubMed] [Google Scholar]
- Vesga‐López, O. , Schneier, F. , Wang, S. , Heimberg, R. , Liu, S. M. , Hasin, D. S. , & Blanco, C. (2008). Gender differences in generalized anxiety disorder: Results from the National Epidemiologic Survey on alcohol and related conditions (NESARC). The Journal of Clinical Psychiatry, 69(10), 1606–16016. [PMC free article] [PubMed] [Google Scholar]
- Vîslă, A. , Constantino, M. , & Flückiger, C. (2021). Predictors of change in patient treatment outcome expectation during cognitive‐behavioral psychotherapy for generalized anxiety disorder. Psychotherapy, 58(2), 219–229. 10.1037/pst0000371 [DOI] [PubMed] [Google Scholar]
- Vîslă, A. , Constantino, M. J. , Newkirk, K. , Ogrodniczuk, J. S. , & Söchting, I. (2018). The relation between outcome expectation, therapeutic alliance, and outcome among depressed patients in group cognitive‐behavioral therapy. Psychotherapy Research, 28(3), 446–456. 10.1080/10503307.2016.1218089 [DOI] [PubMed] [Google Scholar]
- Vîslă, A. , Flückiger, C. , Constantino, M. J. , Krieger, T. , & Grosse Holtforth, M. (2019). Patient characteristics and the therapist as predictors of depressed patients' outcome expectation over time: A multilevel analysis. Psychotherapy Research, 29(6), 709–722. 10.1080/10503307.2018.1428379 [DOI] [PubMed] [Google Scholar]
- Visla, A. , Stadelmann, C. , Watkins, E. , Zinbarg, R. , & Flückiger, C. (2022). The relation between worry and mental health in nonclinical population and individuals with anxiety and depressive disorders: A meta‐analysis. Cognitive Therapy and Research . 10.1007/s10608-021-10288-4 [DOI]
- Vîslă, A. , Zinbarg, R. , Hilpert, P. , Allemand, M. , & Flückiger, C. (2021). Worry and positive episodes in the daily lives of individuals with generalized anxiety disorder: An ecological momentary assessment study. Frontiers in Psychology, 12, 722881. 10.3389/fpsyg.2021.722881 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wampold, B. E. , & Flückiger, C. (2022). The alliance in mental health care: Conceptualization, evidence and clinical applications. World psychiatry: Official journal of the World Psychiatric Association (WPA) . [DOI] [PMC free article] [PubMed]
- Wang, L. P. , & Maxwell, S. E. (2015). On disaggregating between‐person and within‐person effects with longitudinal data using multilevel models. Psychological Methods, 20(1), 63–83. 10.1037/met0000030 [DOI] [PubMed] [Google Scholar]
- Webb, C. A. , Kertz, S. J. , Bigda‐Peyton, J. S. , & Björgvinsson, T. (2013). The role of pretreatment outcome expectancies and cognitive‐behavioral skills in symptom improvement in an acute psychiatric setting. Journal of Affective Disorders, 149, 375–382. 10.1016/j.jad.2013.02.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Westra, H. A. , Dozois, D. J. , & Marcus, M. (2007). Expectancy, homework compliance, and initial change in cognitive‐behavioral therapy for anxiety. Journal of Consulting and Clinical Psychology, 75, 363–373. 10.1037/0022-006X.75.3.363 [DOI] [PubMed] [Google Scholar]
- Zbozinek, T. D. , Rose, R. D. , Wolitzky‐Taylor, K. B. , Sherbourne, C. , Sullivan, G. , Stein, M. B. , & Craske, M. G. (2012). Diagnostic overlap of generalized anxiety disorder and major depressive disorder in a primary care sample. Depression and Anxiety, 29(12), 1065–1071. 10.1002/da.22026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zilcha‐Mano, S. (2021). Toward personalized psychotherapy: The importance of the trait‐like/state‐like distinction for understanding therapeutic change. American Psychologist, 76(3), 516–528. 10.1037/amp0000629 [DOI] [PubMed] [Google Scholar]
- Zinbarg, R. E. , Craske, M. G. , & Barlow, D. H. (2006). Mastery of your anxiety and worry. Therapist guide . Oxford University Press. [Google Scholar]
- Schulte, D. (2008). Patients’ outcome expectancies and their impression of suitability as predictors of treatment outcome. Psychotherapy Research, 18(4), 481–494. 10.1080/10503300801932505 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.