

Abstract
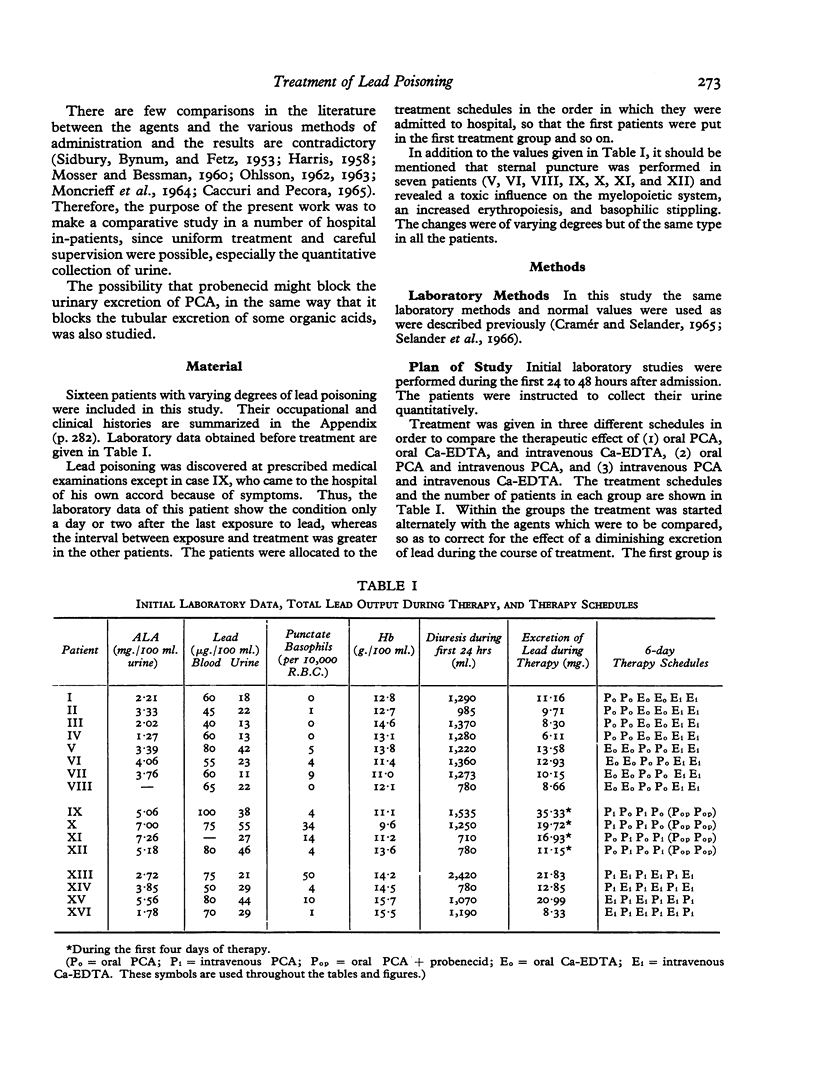
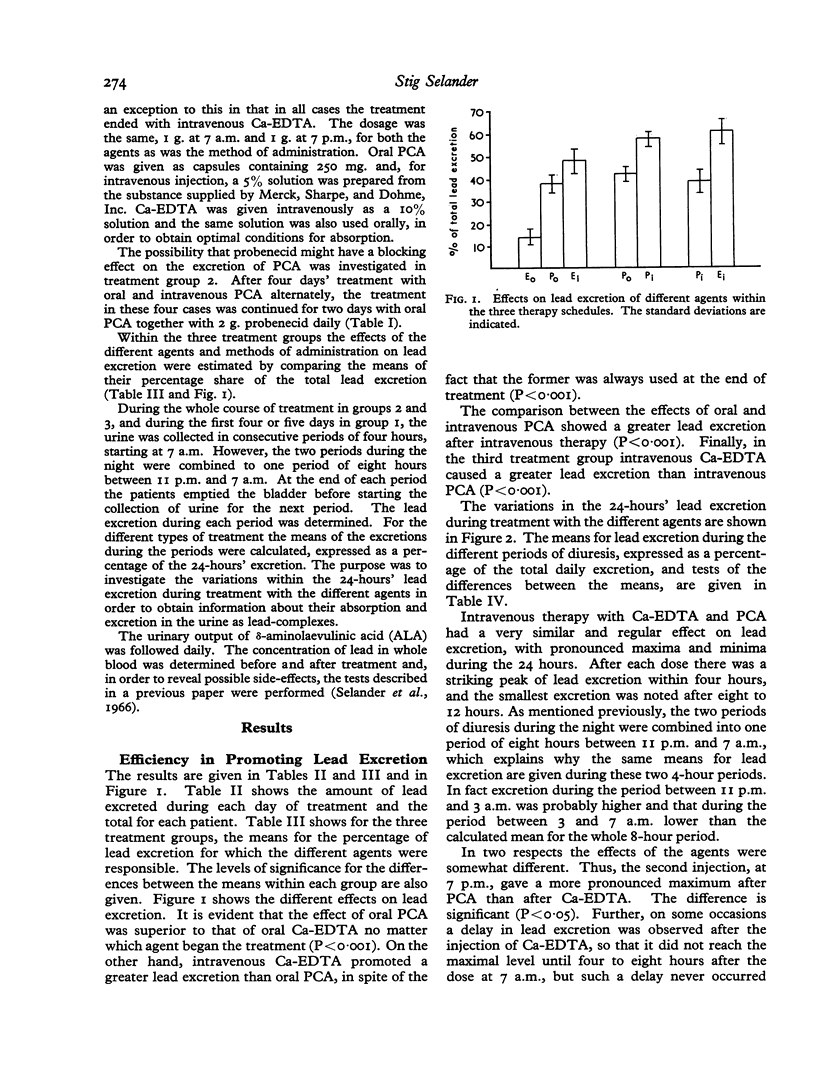
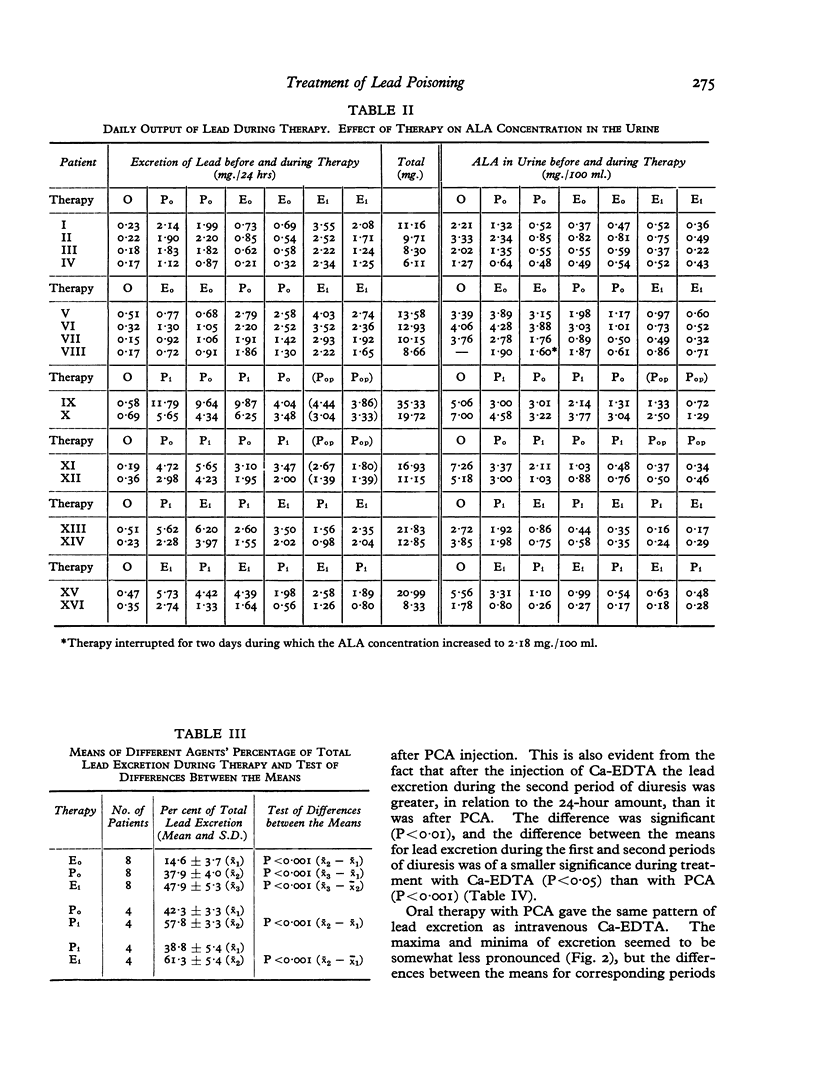
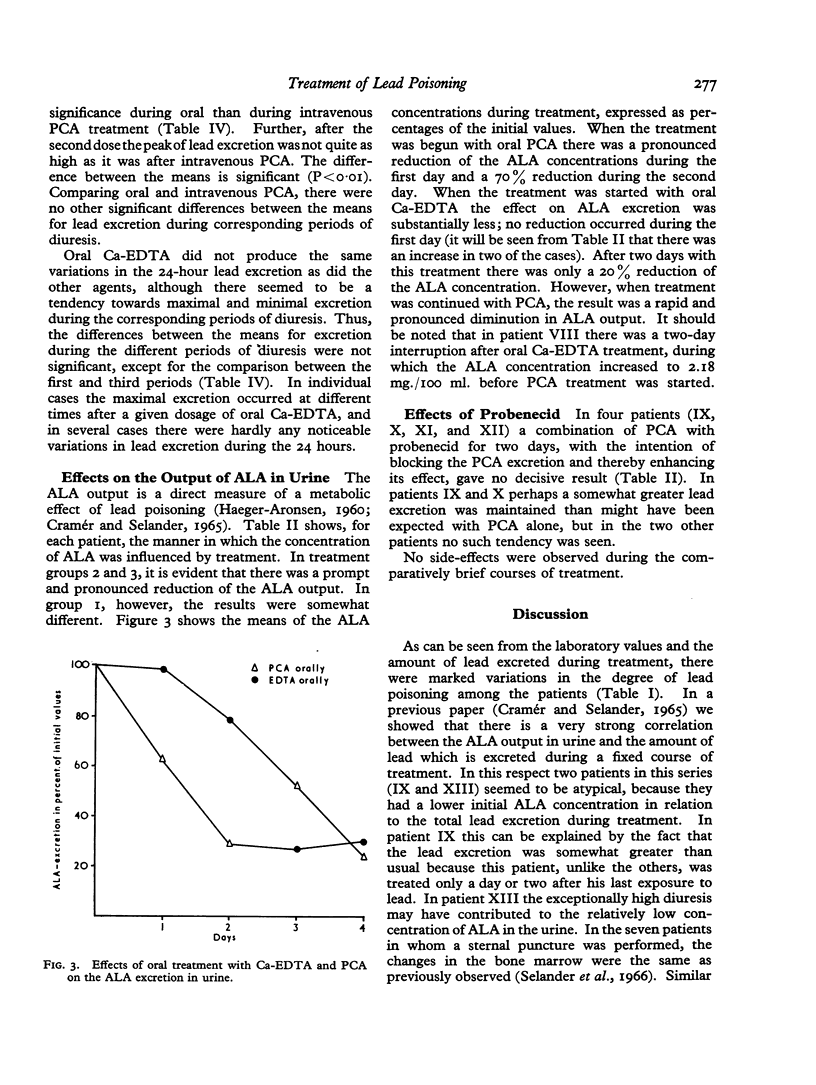
In 16 workers with lead poisoning of varying degrees, a comparison was made between the therapeutic efficacy of sodium calciumedetate (Ca-EDTA) and penicillamine (PCA), administered intravenously and orally. The question of comparable dosages of ligands, forming metal complexes in different ways, is discussed. With the dosages given, intravenous Ca-EDTA promoted the greatest output of lead in the urine, followed by intravenous and oral PCA. These three agents also had a very satisfactory effect on the output δ-aminolaevulinic acid (ALA) in urine. Oral Ca-EDTA was found to be greatly inferior in both these respects.
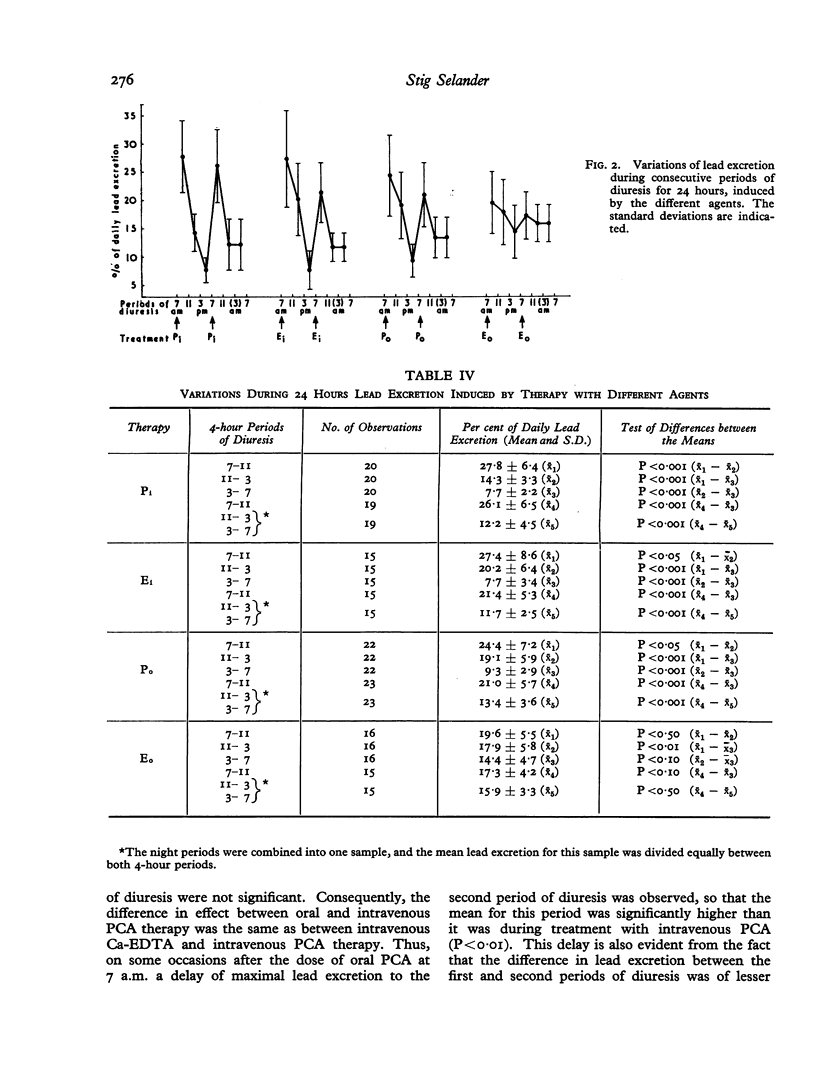
In order to study the absorption of the agents and the renal excretion of the formed lead complexes, the urine was collected quantitatively and fractionated in consecutive 4-hour periods, after which the lead excretion during each period was determined. It was found that the oral absorption of PCA was rapid and quantitatively great, whereas the oral absorption of Ca-EDTA was very slow and quantitatively small. The possible resorption of ligand-lead complexes is discussed and indications were found of resorption of the Ca-EDTA-lead complex but not of the PCA-lead complex. The renal excretion of the different ligand-lead complexes was very effective and reached its maximal level within four hours. However, in some subjects excretion of the Ca-EDTA-lead complex showed some delay. An investigation, in four subjects, of a blocking effect of probenecid on the renal excretion of PCA and/or PCA-lead complexes gave no conclusive results. It is concluded that oral PCA is satisfactory in most cases of lead poisoning. However, in more severe cases intravenous treatment is preferable. Which agent should be chosen, Ca-EDTA or PCA, appears to be unimportant as both are quite satisfactory from the point of view of treatment, but it seems that Ca-EDTA may cause more serious side-effects. Oral Ca-EDTA is quite unsatisfactory and there is good evidence to indicate that the agent causes a resorption of Ca-EDTA-lead complexes from the gastro-intestinal tract.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BELL R. F., GILLILAND J. C., BOLAND J. R., SULLIVAN B. R. Effect of oral edathamil calcium-disodium on urinary and fecal lead excretion; comparative excretory studies with intravenous therapy. AMA Arch Ind Health. 1956 Apr;13(4):366–371. [PubMed] [Google Scholar]
- BESSMAN S. P., RIED H., RUBIN M. Treatment of lead encephalopathy with calcium disodium versenate; report of a case. Med Ann Dist Columbia. 1952 Jun;21(6):312–315. [PubMed] [Google Scholar]
- BYERS R. K. Lead poisoning; review of the literature and report on 45 cases. Pediatrics. 1959 Mar;23(3):585–603. [PubMed] [Google Scholar]
- Caccuri S., Pecora L. La terapia del saturnismo professionale mediante penicillamina. Minerva Med. 1965 Dec 26;56(103):4543–4554. [PubMed] [Google Scholar]
- DAVID A. [The bone marrow in occupational lead poisoning]. Arch Gewerbepathol Gewerbehyg. 1959;17:329–338. [PubMed] [Google Scholar]
- HARRIS C. E. A comparison of intravenous calcium disodium versenate and oral penicillamine in promoting elimination of lead. Can Med Assoc J. 1958 Oct 15;79(8):664–666. [PMC free article] [PubMed] [Google Scholar]
- KEHOE R. A. Misuse of edathamil calciumdisodium for prophylaxis of lead poisoning. J Am Med Assoc. 1955 Jan 22;157(4):341–342. [PubMed] [Google Scholar]
- MANVILLE I. A., MOSER R. Recent developments in the care of workers exposed to lead; the effect of the calcium chelate of disodium ethylenediamine-tetraacetic acid on lead in the blood and urine of battery workers. AMA Arch Ind Health. 1955 Nov;12(5):528–538. [PubMed] [Google Scholar]
- MONCRIEFF A. A., KOUMIDES O. P., CLAYTON B. E., PATRICK A. D., RENWICK A. G., ROBERTS G. E. LEAD POISONING IN CHILDREN. Arch Dis Child. 1964 Feb;39:1–13. doi: 10.1136/adc.39.203.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MOSSER R. S., BESSMAN S. P. Lead excretion following oral dlpenicillamine with a method for comparing the relative effectiveness of chelating agents on the excretion of lead. Bull Sch Med Univ Md. 1960 Jul;45:47–49. [PubMed] [Google Scholar]
- PEROL R., GRAVELEAU J., POTTER M., MORIN M. [Therapeutic effects of D-penicillamine in 3 cases of lead poisoning]. Sem Hop. 1962 Oct 26;38:3342–3347. [PubMed] [Google Scholar]
- RIEDERS F., DUNNINGTON W. G., BREIGER H. The efficacy of edathamil calcium disodium in the treatment of occupational lead poisoning. Ind Med Surg. 1955 May;24(5):195–202. [PubMed] [Google Scholar]
- SHIELS D. O., THOMAS D. L., KEARLEY E. Treatment of lead poisoning by edathamil calcium-disodium. AMA Arch Ind Health. 1956 May;13(5):489–498. [PubMed] [Google Scholar]
- SIDBURY J. B., Jr, BYNUM J. C., FETZ L. L. Effect of chelating agent on urinary lead excretion; comparison of oral and intravenous administration. Proc Soc Exp Biol Med. 1953 Feb;82(2):226–228. doi: 10.3181/00379727-82-20073. [DOI] [PubMed] [Google Scholar]
- SRBOVA J., TEISINGER J. Uber die Resorption des Calciumdinatriumsalzes der Athylendiamintetraessigsäure bei der peroralen Verabreichung zur Therapie der Bleivergiftung. Arch Gewerbepathol Gewerbehyg. 1957;15(6):572–580. [PubMed] [Google Scholar]
- Selander S., Cramér K., Hallberg L. Studies in lead poisoning. Oral therapy with penicillamine: relationship between lead in blood and other laboratory tests. Br J Ind Med. 1966 Oct;23(4):282–291. doi: 10.1136/oem.23.4.282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- TISHKOFF G. H., GRANVILLE N. B., ROSEN R., DAMESHEK W. Excretion of delta-aminolevulinic acid in lead intoxication. Acta Haematol. 1958 Jun;19(6):321–326. doi: 10.1159/000205451. [DOI] [PubMed] [Google Scholar]