

Abstract
Backgrounds
This study aimed to determine whether the Mayo adhesive probability score (MAP), which evaluated adherent perinephric fat (APF), is useful in evaluating the difficulty of retroperitoneal laparoscopic adrenalectomy (RLA), and to analyse the correlation between MAP and perioperative parameters.
Methods
Clinical data of 104 patients with adrenal adenoma who underwent RLA were collected for retrospective analysis. According to the CT images obtained before surgery, patients were divided into two groups: High MAP group (2–5 points) and Low MAP group (0–1 points). Comparison of the general clinical characteristics and the perioperative data between the two groups was made.
Results
There were more male patients (73.7% versus 34.3%), more patients with a smoking history (24.3% versus 7.5%), higher BMI (25.7 versus 23.2, kg/m2), and bigger (23.8 versus 18.5, mm) neoplasm in the high MAP group (P < 0.05). Significant difference was observed in operative time (128.8 versus 102.3, min), estimated blood loss (47.2 versus 25.2, ml) and drainage tube removal time (4.0 versus 3.2, d) between the two groups (P < 0.05). A high MAP score (P < 0.001) and the size of tumour (P = 0.024) were independent risk factors for extended operative time. A higher BMI (OR = 1.525, P < 0.001) and larger tumour size (OR = 2.862, P = 0.004) were independent risk factors for a high MAP score.
Conclusions
MAP score was associated with the perioperative outcomes of RLA. BMI and tumour size were better indicators of MAP score, which can influence the difficulty of RLA.
Keywords: adherent perinephric fat, Mayo adhesive probability score, perioperative outcomes, retroperitoneal laparoscopic adrenalectomy
MAP score was associated with the perioperative outcomes of RLA. BMI and tumour size were better indicators of MAP score, which can influence the difficulty of RLA.
Introduction
Retroperitoneal laparoscopic adrenalectomy (RLA) has gradually become a standard procedure in the treatment of small benign adrenal neoplasms in China. 1 , 2 Owing to the advantages of little interference to the abdominal organs, low risk of intraoperative injury, and rapid postoperative recovery, it is favoured by urologists. Surgical difficulties associated with RLA include localization of the adrenal glands, avoidance of peritoneal injury and separation and exposure of the central adrenal vein. However, this approach is more complicated in some obese patients. Some factors related to obesity, including body mass index (BMI) and the perinephric fat content, contribute to the difficulty of surgery. 3 , 4 , 5 It has been reported that not only the volume but also the features of perinephric fat increase the difficulty of dissecting and exposing tumours. 3 Nonetheless, no studies have examined the effects of adherent perinephric fat (APF) on RLA. It is necessary to evaluate the difficulty of the operation and choose the appropriate surgical method before the operation.
Currently, there is lack of scoring systems for adrenal surgery. Davidiuk et al. established the Mayo adhesive probability (MAP) scoring system to anticipate the occurrence of APF in nephron sparing surgery based on the surrounding environment in 2014. 6 Increasing evidence indicates that MAP scores can be a credible and accurate APF indicator. 7 , 8 , 9 , 10 RLA also passes through the space around the kidney, and surgeons must contend with perinephric fat to reach the adrenal gland. It would be beneficial if APF could be predicted before RLA. Therefore, we speculate that the MAP scoring system is also suitable for adrenal surgery. To explore the clinical significance of the MAP score in the preoperative evaluation of RLA, retrospective analysis of 104 patients with adrenal adenoma who underwent RLA was conducted in this study. The remainder of this paper is organized as follows.
Methods
Patients
Our study retrospectively collected data from patients with functional or non‐functional adrenal adenoma(diagnosed by pathology), who had complete clinical records and underwent RLA from September 2015 to October 2020 at our hospital. Preoperatively, all patients underwent computed tomography and endocrine laboratory examinations at our hospital. Patients with nonsurgical treatment, other pathologic types except adenoma, and incomplete medical records were excluded. All patients signed informed consent. The surgeries were performed by urologists with years of experience in our department using the same technique. 1 The collected clinical variables were patients' age, sex, BMI, history of hypertension, diabetes, and smoking, size and side of the tumour, and functional neoplasm, including hypercortisolism and primary aldosteronism. Surgical outcomes collected from medical records were operative time, drainage tube removal time, estimated blood loss, duration of postoperative hospital stay, complications, and pathological results. This study was approved by the Ethics Committee of our hospital.
Calculation of MAP score and grouping
MAP score was assessed using preoperative enhanced computed tomography by two urologists who were blinded to patients' information. MAP score was calculated by adding the following two parameters (0–5 points). The thickness of posterior perinephric fat was measured at the renal vein level (<1.0 cm, 0 points; 1.0–2.0 cm, 1 point; ≥2.0 cm, 2 points) (Figure S1). The evaluation of perinephric fat stranding was: no, 0 points; mild, 2 points; severe, 3 points. 6 According to the score, all patients were divided into two groups (Low MAP group, ≤1 points, High MAP group, ≥2 points) (Figure S2).
Statistical analysis
Data are shown as mean (± standard deviation). Two‐group comparisons were performed by the Student's t‐test for continuous variables and the Fisher's exact test or Chi‐square test for categorical data. Multiple linear or logistic regression analysis was used to evaluate the factors which were significant in the univariate analysis (P < 0.05). All analyses were performed using GraphPad Prism 9. A P‐value <0.05 was considered significant. Postoperative complications were classified by Clavien–Dindo grading system.
Results
Patients' characteristics
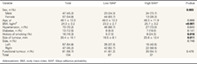
A total of 104 patients were enrolled, the clinical characteristics of them are shown in Table 1. There were 67 patients in Low MAP group and 37 patients in High MAP group, respectively. There were more men (73.7% versus 34.3%, p = 0.003) and smoker (24.3% versus 7.5%, p = 0.016) in the High MAP group. High MAP patients had higher BMI values (25.7 versus 23.2, kg/m2, P < 0.001) and larger tumours (23.8 versus 18.5, mm, P = 0.011). Functional adrenal adenomas occurred in 11 patients with hypercortisolism and 50 patients with primary aldosteronism, but no statistical difference was found between the two groups.
Table 1.
Patients (n = 104) clinical characteristics in different MAP score group
| Variable | Total | Low MAP | High MAP | P‐value |
|---|---|---|---|---|
| Sex, n (%) | 0.003 | |||
| Male | 47 (45.2) | 23 (34.3) | 24 (73.7) | |
| Female | 57 (54.8) | 44 (65.7) | 13 (26.3) | |
| Age, yr | 48.1 ± 12.0 | 48.0 ± 12.2 | 48.3 ± 11.9 | 0.888 |
| BMI, kg/m2 | 24.3 ± 3.2 | 23.2 ± 2.7 | 25.7 ± 3.2 | <0.001 |
| Hypertension, n (%) | 73 (70.2) | 46 (68.7) | 27 (73.0) | 0.645 |
| Diabetes, n (%) | 13 (12.5) | 6 (9.0) | 7 (19.0) | 0.141 |
| History of smoking (%) | 16 (16.3) | 5 (7.5) | 9 (24.3) | 0.016 |
| Size of tumour, mm | 20.4 ± 10.1 | 18.5 ± 8.1 | 23.8 ± 12.4 | 0.011 |
| Side, n (%) | 0.746 | |||
| Left | 57 (54.8) | 25 (37.3) | 15 (40.5) | |
| Right | 47 (45.2) | 42 (62.7) | 22 (59.5) | |
| Functional tumour, n (%) | 61 (58.7) | 41 (61.2) | 20 (54.1) | 0.479 |
| Total | 104 | 67 | 37 |
Abbreviations: BMI, body mass index; MAP, Mayo adhesive probability. P < 0.05 was considered significant.
Impact of MAP on RLA outcomes
The impact of MAP on the RLA outcomes is shown in Table 2. Operative time (128.8 versus 102.3, min, P < 0.001) was longer in the High MAP group. High MAP was related to higher estimated blood loss (EBL) (47.2 versus 25.2, ml, P < 0.001) during the operation and prolonged drainage tube removal time (4.0 versus 3.2, d, P = 0.001) after the operation, but it did not significantly influence the postoperative hospital stays of patients (4.5 versus 4.2, d, P = 0.464). No conversion to open operation was occurred. The incidence of post‐operative complications (Clavien grade ≤ 2) was higher in the High MAP group, but there was no significant difference (11.4% versus 6%). There were no 3 or greater grade complications occurred in either groups. In the multivariate linear regression model, high MAP score (P < 0.001), and tumour size (P = 0.024) were considered independent risk factors for extended operative time (Table S1).
Table 2.
Impact of MAP on perioperative outcomes
| Variable | Low MAP | High MAP | P‐value |
|---|---|---|---|
| Operative time, min | 102.3 ± 25.4 | 128.8 ± 35.4 | <0.001 |
| Estimated blood loss, ml | 25.2 ± 12.9 | 47.2 ± 34.1 | <0.001 |
| Drainage tube removal time, d | 3.2 ± 1.2 | 4.0 ± 1.4 | 0.001 |
| Postoperative hospital stays, d | 4.2 ± 1.6 | 4.5 ± 2.0 | 0.464 |
| Clavien grade of Complications, n (%) | 0.441 | ||
| ≤2 | 4(6.0) | 4(11.4) | |
| ≥3 | 0 | 0 | |
| Total | 67 | 37 |
P < 0.05 was considered significant.
Risk factors of MAP
In order to estimate the cut‐off value of BMI (AUC = 0.773, P < 0.001) and tumour size (AUC = 0.655, P = 0.009) associated with a high MAP score, the ROC curve was used. The results showed that patients with BMI>25.6 kg/m2 or tumour size>21.5 mm will probably represent APF during the operation. The results of the multivariate logistic analyses are listed in Tables 3. In the univariate analysis, male sex (OR = 3.532, P = 0.003), BMI>25.6 kg/m2 (OR = 1.478, P < 0.001), history of smoking (OR = 4.593, P = 0.010), and tumour size>21.5 mm (OR = 2.972, P = 0.011) were all associated with a high MAP score. In the multivariate analysis, BMI>25.6 kg/m2 (OR = 5.933, P < 0.001) and tumour size>21.5 mm (OR = 3.064, P = 0.032) remained independent risk factors for a high MAP score.
Table 3.
Examining the risk factors associated with high MAP score in a multivariate logistic regression model
| Variable | OR | Univariate 95%CI | P‐value | OR | Multivariate 95%CI | P‐value |
|---|---|---|---|---|---|---|
| Age | 1.002 | 0.969–1.037 | 0.886 | |||
| Sex (Male) | 3.532 | 1.544–8.397 | 0.003 | 2.385 | 0.780–7.495 | 0.128 |
| BMI (>25.6 kg/m2) | 9.399 | 3.801–24.89 | <0.001 | 5.933 | 2.236–16.83 | <0.001 |
| HBP (Yes) | 1.233 | 0.514–3.090 | 0.645 | |||
| Diabetes (Yes) | 2.372 | 0.728–7.971 | 0.149 | |||
| Smoker(Yes) | 4.593 | 1.486–15.95 | 0.010 | 1.859 | 0.433–8.522 | 0.408 |
| Size (>21.5 mm) | 2.972 | 1.298–6.967 | 0.011 | 3.064 | 1.116–8.879 | 0.032 |
| Side(Right) | 0.873 | 0.384–2.004 | 0.746 | |||
| Functional(Yes) | 0.746 | 0.330–1.687 | 0.707 |
Abbreviations: CI, confidence interval; OR, odds ratios. P < 0.05 was considered significant.
Discussion
As surgical techniques become more mature, it is increasingly important to preoperatively assess the surgical difficulty and risk, and how to systematically evaluate surgical complexity and select the appropriate approach has been the focus of surgeons' attention. In the past 10 years, the surgical evaluation system for the renal aspect has gradually improved, but that for the adrenal is still lacking. Most renal scoring systems in the past ignored the ‘environment’, such as the APF, where the tumour was located. APF increases the difficulty of stripping perirenal fat from the kidney, resulting in unclear exposure of the surgical field, and makes it hard to distinguish fat from normal tissue, making it difficult to separate the tumour. It is also easy to cause damage to the peritoneal membrane, blood vessels, and even the kidney, which increases the difficulty of surgical operation. 11 Many studies have shown that APF negatively impacts surgical outcomes. 12 The MAP scoring system, which consist of posterior perinephric fat thickness and perinephric fat stranding, can predict the occurrence of APF. There is increasing evidence that the MAP score can be used as a reliable and accurate indicator of APF, 8 , 10 as well as for the prediction of longer operative times, longer dissection time, and greater estimated blood loss. 9 , 13 , 14
Generally speaking, adrenal glands are located above the kidneys, surrounded by the perirenal fat in all populations, regardless of obesity. Considering that RLA also needs to pass through the surrounding renal environment and separate part of the perinephric fat, APF should also affect RLA. The MAP score should also be applied to preliminarily judge the difficulty of RLA owing to the features of APF, including thickness and stickiness. Because APF is too subjective and the MAP score can reflect surgical difficulty by predicting the presence of APF, we directly investigated the association of MAP score with indicators of RLA to explore the potential application value of the MAP score in RLA. Previous research demonstrated that a MAP score > 0 was associated with a prolonged operative time in laparoscopic adrenalectomy. 15 However, it only involved in the patients who underwent the transabdominal approach operation with functional tumours, including hypercortisolism and primary aldosteronism. Additionally, the proportion of APF increased as the MAP score increased. The present study compared the patient characteristics and perioperative parameters in patients whose MAP score was ≥2 with those in patients whose MAP score was ≤1, and more indicators were analysed. Our results showed that an increased MAP score was associated with prolonged operative time, drainage tube removal time, and increased EBL. We also found that there were more male patients, more patients with smoking history, higher BMI, and larger tumours in the high MAP group (P < 0.05). Multivariate analysis demonstrated that BMI and size of tumour were independent predictors of MAP score.
It is revealed that men are more prone to possessing APF than women. 7 , 8 , 16 These differences were due to the body fat distribution in the different sexes. Although women were thought to have more subcutaneous fat, men had more visceral fat. 17 , 18 In this study, a high MAP score was more common in men than in women, which is similar to previous studies. A history of smoking, mostly among males, was another risk factor for a high MAP score. Unfortunately, neither factor was meaningful in the multivariate analysis.
In our study, tumour size was one of the independent risk factors for MAP and operative time. The size of adrenal mass is an important factor in determining surgical protocols. In the past, the vast majority of urologists believed that RLA was only applied to small adrenal tumours, and whether RLA could be used for tumours with a max diameter greater than 6 cm was controversial. With improvements in experience and technological advancement, the successful excision of large adrenal tumours (>6 cm) using RLA in recent years has been increasingly reported. 19 , 20 , 21 In general, as the adrenal tumour is larger in diameter, it is more likely to adheres to the surrounding tissues, making separation and removal more difficult. The operative time may also be prolonged, and the complication rate may increase. According to our research, tumour size is associated with MAP score, increasing the difficulty of surgery.
Although BMI may indicate the composition of body fat, the distribution of perirenal fat may differ in patients with the same BMI. It was proved that High BMI was related to APF, 12 , 13 but it is controversial whether BMI can indirectly reflect perirenal fat status by predicting MAP score. Our results showed that BMI was correlated with the MAP score, and higher BMI was an independent predictor of a high MAP score, which indicated a high probability of APF. This is the same as Davidiuk's research. 6 Further analysis revealed that BMI > 25.6 kg/m2 was a predictor of high MAP score. Although RLA is safe and effective even for patients with BMI > 40 kg/m2, 22 , 23 most studies suggested the transperitoneal approach for obese patients (BMI > 30 kg/m2). 24 Based on the above two independent parameters, transperitoneal laparoscopic adrenalectomy or open operation should be considered instead of RLA when obese patients have large adrenal tumours.
As a preliminary study, this study has limitations. For example, there were more MAP scores of 0, and a few MAP scores of 5, which may attribute to lack of sample volume or the error of individual interpretation of imaging data. We only enrolled patients that used the retroperitoneal approach and excluded those used the transperitoneal approach. Furthermore, we did not include patients with other pathological type, such as adrenal cyst, myelolipoma, pheochromocytomas, and so on. Therefore, the results of this study need to be verified further using expanded data and more cases.
Conclusion
The MAP score was associated with the perioperative outcomes of RLA, and it was correlated with BMI, sex, history of smoking, and tumour size. BMI and tumour size were independent risk factors of MAP score, which may influence the difficulty of RLA.
Author contributions
Yeqing Yuan: Conceptualization; funding acquisition; investigation; methodology; project administration; software; validation; writing – original draft; writing – review and editing. Huiquan Feng: Data curation; formal analysis; writing – original draft. Zheng Kang: Data curation; resources; validation. Yunhai Xie: Formal analysis; methodology; resources. Xueqi Zhang: Data curation; methodology; validation. Yixiang Zhang: Conceptualization; funding acquisition; methodology; project administration; resources; supervision; validation.
Conflicts of interest
None declared.
Supporting information
Table S1. Examining the risk factors associated with Operative time in a multivariate linear regression model
Figure S1. Method of determining perinephric fat measurements at the level of the renal vein. P = posterior, RV = renal vein.
{kind=link}
Figure S2. Grading of perinephric fat stranding. (a) No stranding: 0 points. (b) Mild stranding: 2 points. The fat around the kidney presents slight stranding. (c) Severe stranding: 3 points. There are thick image‐dense bars around the kidney.
{kind=link}
Acknowledgement
This study was supported by Shenzhen Commission of Science and Innovation programs (JCYJ20190806155007197).
Y. Yuan PhD; H. Feng MM; Z. Kang MBBS; Y. Xie MBBS; X. Zhang MM; Y. Zhang MD.
Yeqing Yuan and Huiquan Feng have contributed equally to this work.
References
- 1. Zhang X, Fu B, Lang B et al. Technique of anatomical retroperitoneoscopic adrenalectomy with report of 800 cases. J. Urol. 2007; 177: 1254–7. [DOI] [PubMed] [Google Scholar]
- 2. Lang B, Fu B, OuYang JZ et al. Retrospective comparison of retroperitoneoscopic versus open adrenalectomy for pheochromocytoma. J. Urol. 2008; 179: 57–60. [DOI] [PubMed] [Google Scholar]
- 3. Pearlstein SS, Kuo JH, Chabot JA, Lee JA. Periadrenal volume is a better predictor of prolonged operative time in laparoscopic retroperitoneal Adrenalectomy than BMI. World J. Surg. 2020; 44: 578–84. [DOI] [PubMed] [Google Scholar]
- 4. Ersoz F, Erbil Y, Sari S et al. Predictive value of retroperitoneal fat area measurement for detecting metabolic syndrome in patients undergoing adrenalectomy. World J. Surg. 2011; 35: 986–94. [DOI] [PubMed] [Google Scholar]
- 5. Kazaure HS, Roman SA, Sosa JA. Obesity is a predictor of morbidity in 1,629 patients who underwent adrenalectomy. World J. Surg. 2011; 35: 1287–95. [DOI] [PubMed] [Google Scholar]
- 6. Davidiuk AJ, Parker AS, Thomas CS et al. Mayo adhesive probability score: an accurate image‐based scoring system to predict adherent perinephric fat in partial nephrectomy. Eur. Urol. 2014; 66: 1165–71. [DOI] [PubMed] [Google Scholar]
- 7. Kawamura N, Saito K, Inoue M et al. Adherent perinephric fat in Asian patients: predictors and impact on perioperative outcomes of partial nephrectomy. Urol. Int. 2018; 101: 437–42. [DOI] [PubMed] [Google Scholar]
- 8. Kocher NJ, Kunchala S, Reynolds C, Lehman E, Nie S, Raman JD. Adherent perinephric fat at minimally invasive partial nephrectomy is associated with adverse peri‐operative outcomes and malignant renal histology. BJU Int. 2016; 117: 636–41. [DOI] [PubMed] [Google Scholar]
- 9. Yao Y, Xu Y, Gu L et al. The Mayo adhesive probability score predicts longer dissection time during laparoscopic partial nephrectomy. J. Endourol. 2020; 34: 594–9. [DOI] [PubMed] [Google Scholar]
- 10. Dariane C, Le Guilchet T, Hurel S et al. Prospective assessment and histological analysis of adherent perinephric fat in partial nephrectomies. Urol. Oncol. 2017; 35: 39 e39–17. [DOI] [PubMed] [Google Scholar]
- 11. Macleod LC, Hsi RS, Gore JL, Wright JL, Harper JD. Perinephric fat thickness is an independent predictor of operative complexity during robot‐assisted partial nephrectomy. J. Endourol. 2014; 28: 587–91. [DOI] [PubMed] [Google Scholar]
- 12. Khene ZE, Peyronnet B, Mathieu R, Fardoun T, Verhoest G, Bensalah K. Analysis of the impact of adherent perirenal fat on peri‐operative outcomes of robotic partial nephrectomy. World J. Urol. 2015; 33: 1801–6. [DOI] [PubMed] [Google Scholar]
- 13. Yanishi M, Kinoshita H, Koito Y et al. Adherent perinephric fat is a surgical risk factor in laparoscopic single‐site donor nephrectomy: analysis using Mayo adhesive probability score. Transplant. Proc. 2020; 52: 84–8. [DOI] [PubMed] [Google Scholar]
- 14. Ozcelik U, Eren E, Urut DU, Talih T, Tokac M, Dinckan A. Correlation between the Mayo adhesive probability score and the operative time in laparoscopic donor nephrectomy. Transplant. Proc. 2021; 53: 793–8. [DOI] [PubMed] [Google Scholar]
- 15. Kira S, Sawada N, Nakagomi H et al. Mayo adhesive probability score is associated with the operative time in laparoscopic adrenalectomy. J. Laparoendosc. Adv. Surg. Tech. A 2021; 32: 595–9. [DOI] [PubMed] [Google Scholar]
- 16. Zheng Y, Espiritu P, Hakky T, Jutras K, Spiess PE. Predicting ease of perinephric fat dissection at time of open partial nephrectomy using preoperative fat density characteristics. BJU Int. 2014; 114: 872–80. [DOI] [PubMed] [Google Scholar]
- 17. Anderson KM, Lindler TU, Lamberton GR, Baron PW, Ojogho OK, Baldwin DD. Laparoscopic donor nephrectomy: effect of perirenal fat upon donor operative time. J. Endourol. 2008; 22: 2269–74. [DOI] [PubMed] [Google Scholar]
- 18. Eisner BH, Zargooshi J, Berger AD et al. Gender differences in subcutaneous and perirenal fat distribution. Surg. Radiol. Anat. 2010; 32: 879–82. [DOI] [PubMed] [Google Scholar]
- 19. Chen W, Liang Y, Lin W, Fu GQ, Ma ZW. Surgical management of large adrenal tumors: impact of different laparoscopic approaches and resection methods on perioperative and long‐term outcomes. BMC Urol. 2018; 18: 31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Agha A, Iesalnieks I, Hornung M et al. Laparoscopic trans‐ and retroperitoneal adrenal surgery for large tumors. J. Minim. Access Surg. 2014; 10: 57–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Hwang I, Jung SI, Yu SH et al. Is larger tumor size a contraindication to retroperitoneal laparoscopic adrenalectomy? World J. Urol. 2014; 32: 723–8. [DOI] [PubMed] [Google Scholar]
- 22. Zonca P, Buzga M, Ihnat P, Martinek L. Retroperitoneoscopic adrenalectomy in obese patients: is it suitable? Obes. Surg. 2015; 25: 1203–8. [DOI] [PubMed] [Google Scholar]
- 23. Ottlakan A, Paszt A, Simonka Z et al. Laparoscopic transperitoneal and retroperitoneal adrenalectomy: a 20‐year, single‐institution experience with an analysis of the learning curve and tumor size [lap transper and retroper adrenalectomy]. Surg. Endosc. 2020; 34: 5421–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Lee CR, Walz MK, Park S et al. A comparative study of the transperitoneal and posterior retroperitoneal approaches for laparoscopic adrenalectomy for adrenal tumors. Ann. Surg. Oncol. 2012; 19: 2629–34. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Examining the risk factors associated with Operative time in a multivariate linear regression model
Figure S1. Method of determining perinephric fat measurements at the level of the renal vein. P = posterior, RV = renal vein.
Figure S2. Grading of perinephric fat stranding. (a) No stranding: 0 points. (b) Mild stranding: 2 points. The fat around the kidney presents slight stranding. (c) Severe stranding: 3 points. There are thick image‐dense bars around the kidney.