

Abstract
Objective
Despite findings from numerous cross‐sectional studies suggesting a substantial association between loneliness and different types of disordered eating, much remains unknown about the impact of confounding, the order of cause and effect, and gender differences in the relationship. Thus, this study followed a large, population‐based, mixed‐gender sample through adolescence and young adulthood, applying a random intercept cross‐lagged panel model (RI‐CLPM) approach to examine the bidirectional prospective associations between loneliness and disordered eating while ruling out the effect of unmeasured time‐invariant confounders.
Method
A Norwegian sample of N = 2933 adolescents (54.2% female) was examined across four time points (T1, M age = 15.44, grades 7–12; T2, M age = 16.93; T3, M age = 21.84; and T4, M age = 28.33) from 1992 to 2005 using RI‐CLPMs for overall disordered eating and specific forms for disordered eating (dieting and bulimic symptoms). Multigroup structural equation models were used to assess gender differences.
Results
For male participants, high levels of loneliness at T1 predicted more overall disordered eating and more dieting at T2. Meanwhile, among female participants, disordered eating and bulimic symptoms at T2 predicted more loneliness at T3, whereas loneliness at T3 predicted more disordered eating and bulimic symptoms at T4, and vice versa.
Discussion
The findings suggest a pattern of bidirectional associations between loneliness and disordered eating that varies by time points, gender, and type of eating problem. Preventive interventions and treatment should consider social factors involved in the onset and maintenance of eating problems in male adolescents and young adult women.
Public Significance
This study contributes to the existing knowledge by examining for the first time the dynamic nature of the association between loneliness and disordered eating while accounting for all time‐invariant confounding. Our findings reveal a pattern of bidirectional associations between loneliness and disordered eating that appears to vary by developmental period, gender, and type of eating problem. Our findings suggest that social factors have to be taken into account when designing prevention strategies aimed at disordered eating.
Keywords: adolescence, bidirectional association, disordered eating, gender, loneliness, random intercept cross‐lagged panel model, young adulthood
1. INTRODUCTION
Disordered eating or subsyndromal forms of eating disorders (EDs), such as fasting, vomiting, and laxative use for weight loss are commonly experienced during adolescence and early adulthood (e.g., Keel, 2018; Slane et al., 2014), and such behavior presents significant health hazards beyond increasing the risk for later EDs (Ackard et al., 2011; Stice et al., 2009). Identifying risk factors for the emergence and maintenance of disordered eating is crucial because it can inform interventions to reduce disordered eating and its consequences.
In this regard, increasing attention has fastened upon loneliness (i.e., feeling socially disconnected from others; Cacioppo & Patrick, 2008) as a potential source of mental health problems, including disordered eating (Beutel et al., 2017; Levine, 2012). However, even though research has revealed a robust association between loneliness and disordered eating (e.g., Levine, 2012), we know little about the longitudinal nature of this association. This study aimed to provide novel knowledge on this issue by means of state‐of‐the‐art longitudinal modeling across adolescence and young adulthood. We cover these developmental periods because adolescence and young adulthood represent not only a crucial stage for the onset of disordered eating (Keel, 2018; Slane et al., 2014) but also show elevated levels of loneliness (von Soest et al., 2020).
To date, cross‐sectional studies have supported an association between loneliness and different forms of disordered eating. For instance, Rotenberg and Flood (1999) reported that feelings of loneliness were associated with dietary restraint as well as higher food consumption. Likewise, scholars have found perceived loneliness to be related to emotional eating (Raspopow et al., 2013)—which is a precursor of binge eating (Stice et al., 2000)—and excessive calorie consumption (Henriksen et al., 2014; Mason, 2020). In a study focusing on college students, Wright and Pritchard (2009) showed that loneliness was positively related to disordered eating. In the same vein, perceived social problems and low levels of attachment with peers have been linked to more disordered eating in adolescents and young adults (Pritchard & Yalch, 2009; Schutz & Paxton, 2007).
The association between loneliness and disordered eating may be understood in several ways. It has been suggested that loneliness may be a source of disordered eating. For example, in accordance with the Interpersonal Model of EDs (Burke et al., 2018; Wilfley et al., 2000), individuals experiencing loneliness may resort to bulimic behavior and binge eating as a way to distract themselves from negative affect while also attempting to fill the emotional and social needs they may be encountering (Grant, 2008; Levine, 2012). Lonely people may also engage in restrictive eating or dieting as a way to numb their emotions and recreate a sense of control over their lives (Cain et al., 2008; Faber et al., 2018). Conversely, disordered eating may give rise to social isolation and feelings of loneliness (Levine, 2012; Treasure et al., 2011). Specifically, individuals with disordered eating may tend to avoid contact with peers and family in order to hide unhealthy eating behaviors (Levine, 2012). For instance, research has shown that bulimic symptoms are often associated with intense feelings of shame and guilt (Stice et al., 2000), which may lead individuals who engage in binge eating and purging to socially withdraw themselves (Basile, 2004; Rotenberg et al., 2013). Moreover, individuals who engage in restrictive dieting may avoid social gatherings since socializing often revolves around the consumption of food (Levine, 2012; Woolley et al., 2020). Lastly, the association between loneliness and disordered eating may be explained by the effects of potential time‐invariant confounders, such as common genetics (Day et al., 2018; Wade & Bulik, 2018), personality and temperamental factors (Buecker et al., 2020; Cassin & von Ranson, 2005), and response‐style biases (Decaluwé & Braet, 2004). Therefore, the association between loneliness and disordered eating may conceivably diminish once such potentially confounding factors are accounted for.
Accordingly, longitudinal studies designed to disentangle the temporal dynamics of the associations are needed to provide information about the nature of the loneliness–disordered eating association. However, to the best of our knowledge, only two studies to date have examined the prospective association between loneliness and disordered eating. Through participants' self‐report daily diaries, Mason et al. (2016) found that perceived social isolation was predictive of greater binge eating among college women who completed measures nightly each day for 14 days. Similarly, in a study that featured a large population‐based sample of youth, Abebe et al. (2014) identified loneliness as a prospective risk factor for disordered eating during adolescence and young adulthood. However, neither study examined reverse temporal associations whereby disordered eating may function as risk factor of loneliness. Also, the two studies did not rule out important potential time‐invariant confounders.
The hypothesized effects of loneliness on disordered eating or vice versa are stipulated to take place at the within‐person level, whereby a person's feeling of loneliness at a given time is expected to predict changes in that same person's disordered eating (or vice versa). However, until recently, cross‐lagged panel models (CLPMs) have been primarily used to disentangle potential reciprocal longitudinal associations between psychopathology and potential risk factors (Selig & Little, 2012), even though they do not separate between‐person variation from within‐person variation in longitudinal data (Hamaker et al., 2015). As a result, parameter estimates derived from traditional CLPM approaches are difficult to interpret meaningfully when examining individual processes across time (Berry & Willoughby, 2017). We are the first to address this limitation by applying the recently developed random intercept CLPM (RI‐CLPM) to effectively disaggregate longitudinal data into its between‐ and within‐person sources of variance (Hamaker et al., 2015; Mulder & Hamaker, 2020) when examining the association between loneliness and disordered eating. This modeling framework allows the estimation of cross‐lagged effects that are not confounded by any potential time‐invariant confounders.
A further limitation of the existing research is the scarcity of studies examining both male and female samples. In one such study, Rotenberg and Flood (1999) argued that, particularly in women, loneliness might be one of the motives responsible for dietary restraint. Similarly, Masheb and Grilo (2006) reported that, among patients with binge‐ED, women were more likely than men to report overeating in response to loneliness. In contrast, Pritchard and Yalch (2009) found that loneliness was related to disordered eating in men but not in women. In the same vein, Abebe et al. (2014) found that loneliness was a male‐specific predictor of disordered eating. Thus, more research is necessary to better elucidate whether the association between loneliness and disordered eating differs across genders during the transition from adolescence to young adulthood.
The present study aimed to examine for the first time the bidirectional associations between loneliness and different forms of disordered eating from adolescence to young adulthood while ruling out all time‐invariant confounding by means of state‐of‐the‐art longitudinal modeling techniques. We also tested whether such longitudinal associations and their timing would differ by gender. Generating such knowledge is a fundamental step in designing prevention strategies for both problems.
2. METHOD
2.1. Participants and procedure
Data for the present research come from the Young in Norway Study conducted in 1992 (T1; early‐middle adolescence), 1994 (T2; late adolescence), 1999 (T3; emerging adulthood), and 2005 (T4; adulthood). The initial sample at the first data collection included 12,655 students in grades 7 through 12 (M age = 15.44, SD = 1.66). Participants were recruited from 67 representative junior and senior high schools in the country, with a response rate of 97%. At the first follow‐up 2 years later (late adolescence, M age = 16.93, SD = 1.75), approximately half of the students had completed the 3‐year track at the junior or senior high school and had left the school they had been attending at the first data collection. Only students who had completed the questionnaires at school at the second data collection (n = 3844) were followed up in emerging adulthood (M age = 21.84, SD = 1.76) and adulthood (M age = 28.33, SD = 1.73). The response rates among students eligible for participation were 92%, 84%, and 82% in late adolescence, emerging adulthood, and adulthood, respectively. The overall participation rate, based on all eligible students at T1 who still were at their original school at T2, was 68% at T3 and 67% at T4. The study was approved by the Norwegian Regional Committee for Medical Research Ethics (reference S‐05030). All participants consented prior to study participation.
In this study, after excluding participants over 18 years of age at the first data collection, we used data from 2933 students (54.2% female) who participated at least at 1 time point in emerging adulthood and adulthood. At the first data collection, the parents' educational level (measured as the highest educational level attained by either parent) was as follows: 20.5% junior high school or less, 36.9% senior high school, 22.1% college education (not more than 3 years) and 20.5% university education. Moreover, 12.6% of the respondents reported parental occupational level (based on the highest occupational attainment by either parent) to be higher administrative position/leaders, 40.8% professional higher level, 13.0% professional lower level, 6.4% farmer/fisherman, and 27.3% manual workers. Of all respondents, 1.8% had both parents with immigration background (i.e., both parents were not born in Norway). Most of them were born in countries in Asia (56.6%), followed by those born in Western countries (22.6%), in South America (15.1%), and in Africa (5.6%).
Multiple logistic regression analyses showed that being female increased the likelihood of participating in the study in late adolescence (OR = 1.58, 95% CI [1.43, 1.75]), emerging adulthood (OR = 1.41, 95% CI [1.28, 1.56]), and adulthood (OR = 1.41, 95% CI [1.28, 1.56]). In addition, being younger significantly predicted participating in late adolescence (OR = .85, 95% CI [.83, .87]), emerging adulthood (OR = .73, 95% CI [.71, .76]), and adulthood (OR = .74, 95% CI [.73, .77]). Regarding disordered eating, lower scores in early‐middle adolescence predicted participating in the study during late adolescence (OR = .80, 95% CI [.71, .92]). Finally, lower levels in loneliness in early‐middle adolescence increased the likelihood of participating in emerging adulthood (OR = .88, 95% CI [.81, .96]) and adulthood (OR = .87, 95% CI [.80, .95]).
2.2. Measures
2.2.1. Disordered eating
Disordered eating was measured using the 12‐item version of the Eating Attitude Test‐26 (EAT‐26; Garner et al., 1982), developed by Lavik et al. (1991). A 4‐point scale ranging from never (1) to always (4) was used. Mean scores were calculated, with high scores reflecting high levels of disordered eating. The EAT‐12 yields three factors: dieting, bulimia‐food preoccupation, and oral control. Each factor comprises four items. α coefficients for the whole scale ranged from .71 to .75 across data collection waves. Moreover, α coefficients ranged from .80 to .84 for the dieting subscale, and from .61 to .76 for the bulimia‐food preoccupation subscale. The somewhat large variation in internal consistency for the bulimia‐food preoccupation subscale was due to lower α coefficients at the earlier waves. The oral control subscale has been shown to be psychometrically weak (Fekken et al., 1988; Garner et al., 1982), and results based on this subscale are therefore not presented. The construct validity of the overall EAT‐12 has been supported in validation studies (Wichstrøm, 1995).
2.2.2. Loneliness
Feelings of loneliness were assessed using a 4‐item short version of the UCLA Loneliness Scale developed by Russell et al. (1980). The short version of this scale has been reported to be reliable and to correlate highly with the full version (Russell et al., 1980). In addition, a fifth item, “I feel lonely,” was added to measure loneliness directly. This measure has been shown to have good face and predictive validity (von Soest et al., 2020). Response options ranged from 1 = never to 4 = often. This study's 5‐item scale has been used previously (e.g., Abebe et al., 2014) and α coefficients ranged from .65 to .78 in the present study, with lower coefficients at earlier data collection waves.
2.3. Statistical analysis
Statistical analyses were performed using Mplus (Version 8.5). RI‐CLPM models that account for time‐invariant stability by the inclusion of random intercepts (Hamaker et al., 2015; Mulder & Hamaker, 2020) were used to test whether loneliness predicted changes in disordered eating over time and, conversely, whether disordered eating predicted loneliness. For this purpose, autoregressive, CLPMs were estimated in the structural equation modeling framework, including loneliness and disordered eating at all four time points. In addition, random intercepts for both loneliness and disordered eating were included in the models; see Figure 1 for a graphical display of the model. We used the Satorra–Bentler χ2‐difference test (Satorra, 2000) to assess gender differences by means of multiple group analyses. A robust maximum‐likelihood estimator was applied, and full information maximum likelihood was used to handle missing data.
FIGURE 1.
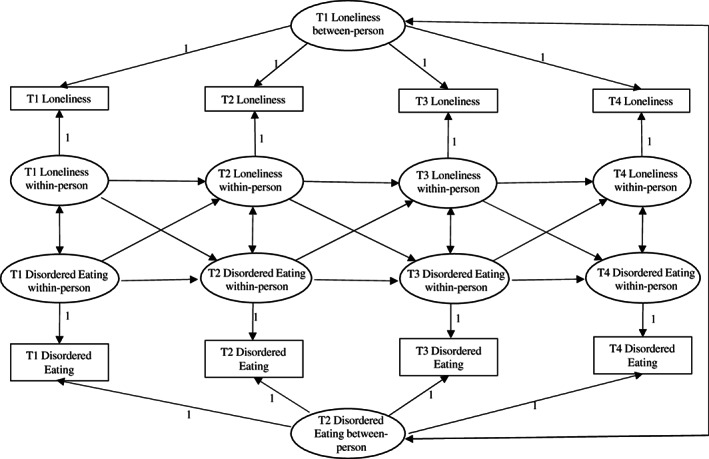
Four waves random intercept cross‐lagged panel model disentangling between‐person and within‐person effects of loneliness and disordered eating
3. RESULTS
3.1. Descriptive statistics
Table 1 shows that female participants had higher scores for disordered eating and loneliness than their male counterparts across all time points. In addition, loneliness was positively correlated to disordered eating (total score and both subscales) at all time points for both women and men.
TABLE 1.
Descriptive statistics and bivariate correlations for men and women from early‐middle adolescence (T1) to adulthood (T4)
| Variables | Men (n = 1343) | Women (n = 1590) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||||||||||||||||
| 1. Loneliness T1 | 1.83 (.53) | 1.90 (.55) | .53 | .32 | .31 | .27 | .25 | .15 | .15 | .15 | .14 | .06 | .04 | .22 | .19 | .15 | .14 | |
| 2. Loneliness T2 | 1.79 (.56) | 1.86 (.57) | .59 | .44 | .41 | .19 | .28 | .20 | .18 | .12 | .14 | .10 | .07 | .16 | .22 | .19 | .17 | |
| 3. Loneliness T3 | 1.78 (.53) | 1.83 (.48) | .41 | .50 | .55 | .16 | .16 | .28 | .18 | .04 | .07 | .13 | .05 | .11 | .12 | .21 | .14 | |
| 4. Loneliness T4 | 1.76 (.51) | 1.79 (.49) | .37 | .44 | .54 | .12 | .15 | .22 | .26 | .04 | .04 | .08 | .08 | .09 | .10 | .19 | .25 | |
| 5. Disordered Eating T1 | 1.49 (.33) | 1.71 (.38) | .18 | .12 | .13 | .11 | .53 | .32 | .29 | .72 | .44 | .27 | .20 | .74 | .36 | .20 | .24 | |
| 6. Disordered Eating T2 | 1.43 (.31) | 1.74 (.39) | .09 | .12 | .14 | .08 | .59 | .39 | .32 | .42 | .72 | .34 | .24 | .42 | .74 | .26 | .24 | |
| 7. Disordered Eating T3 | 1.44 (.29) | 1.71 (.39) | .07 | .10 | .20 | .15 | .34 | .44 | .53 | .29 | .35 | .75 | .44 | .19 | .26 | .66 | .38 | |
| 8. Disordered Eating T4 | 1.48 (.35) | 1.62 (.39) | .10 | .15 | .18 | .26 | .28 | .32 | .50 | .27 | .31 | .46 | .80 | .21 | .22 | .38 | .74 | |
| 9. Dieting T1 | 1.52 (.56) | 2.02 (.71) | .08 | .05 | .07 | .05 | .78 | .55 | .33 | .28 | .62 | .41 | .32 | .33 | .20 | .15 | .19 | |
| 1. Dieting T2 | 1.44 (.52) | 2.08 (.72) | .04 | .05 | .06 | .02 | .50 | .80 | .38 | .29 | .69 | .50 | .37 | .25 | .34 | .17 | .20 | |
| 11. Dieting T3 | 1.59 (.58) | 2.17 (.67) | .05 | .07 | .13 | .08 | .31 | .40 | .81 | .44 | .43 | .51 | .59 | .14 | .20 | .31 | .29 | |
| 12. Dieting T4 | 1.80 (.70) | 2.17 (.73) | .04 | .09 | .10 | .15 | .25 | .28 | .41 | .84 | .34 | .37 | .52 | .13 | .16 | .25 | .42 | |
| 13. Bulimia T1 | 1.39 (.41) | 1.49 (.47) | .16 | .12 | .12 | .09 | .75 | .41 | .26 | .20 | .42 | .30 | .21 | .16 | .47 | .22 | .25 | |
| 14. Bulimia T2 | 1.35 (.40) | 1.54 (.49) | .08 | .12 | .13 | .07 | .47 | .77 | .36 | .25 | .38 | .48 | .29 | .19 | .50 | .30 | .25 | |
| 15. Bulimia T3 | 1.20 (.31) | 1.40 (.50) | .00 | .06 | .18 | .13 | .29 | .38 | .82 | .41 | .26 | .30 | .56 | .30 | .30 | .42 | .43 | |
| 16. Bulimia T4 | 1.23 (.36) | 1.32 (.46) | .06 | .10 | .17 | .23 | .25 | .28 | .43 | .78 | .25 | .25 | .35 | .52 | .24 | .29 | .48 |
Note: Pearson correlations for women under the diagonal. Pearson correlations for men above the diagonal. Intercorrelations of r = |.06| or above are statistically significantly different from zero at p < .001.
For loneliness, the intra‐class correlation (ICC) was .78, indicating that 78% of the variance in loneliness was due to variation between persons, whereas 22% was due to variation in loneliness within persons across time points. The ICC for disordered eating was .77 whereas examination of the subscales of the EAT‐12 yielded ICC values of .82 and .69 for dieting and bulimia and food preoccupation, respectively.
3.2. Prospective associations between loneliness and disordered eating
We used the mean scores of the EAT‐12 scale to estimate a multigroup RI‐CLPM for the associations between loneliness and disordered eating for both females and males. The model fit of the model was good (see Table 2). Results from the RI‐CLPM multigroup analyses can be found in Figure 2. At the between level, the correlation between the intercepts was significant for both males (r = .47, p < .001) and females (r = .27, p < .001), suggesting that individuals who had more disordered eating across the four measurement points reported in general more loneliness as well. At the within level, for boys, loneliness in early‐middle adolescence predicted more disordered eating in late adolescence, thereby indicating that within‐person deviations in loneliness predicted within‐person changes in disordered eating from early‐middle to late adolescence. In contrast, for girls, disordered eating in late adolescence predicted more loneliness in emerging adulthood on the within‐person level. Testing gender‐specific associations for one parameter at a time showed that the cross‐lagged association from loneliness in early‐middle adolescence to disordered eating in late adolescence differed significantly across gender (∆χ2 (1) = 6.82, p = .009), being significantly stronger in boys than in girls.
TABLE 2.
Model fit indices of multigroup random intercept cross‐lagged panel models (RI‐CLPM) examining the longitudinal associations between loneliness and three types of eating symptomatology
| χ2 | df | RMSEA (90% CI) | SRMR | CFI | TLI | |
|---|---|---|---|---|---|---|
| Model 1: Disordered eating | 29.23 | 18 | .021 (.003, .034) | .018 | .997 | .992 |
| Model 2: Dieting | 28.26 | 18 | .020 (.000, .033) | .016 | .998 | .994 |
| Model 3: Bulimia‐food preoccupation | 35.69 | 18 | .026 (.013, .038) | .019 | .995 | .986 |
Abbreviations: 90% CI, 90% confidence interval of RMSEA; CFI, comparative fit index; df, degrees of freedom; RMSEA, root‐mean‐square error of approximation; SRMR, standardized root‐mean‐square residual; TLI, Tucker–Lewis index.
FIGURE 2.
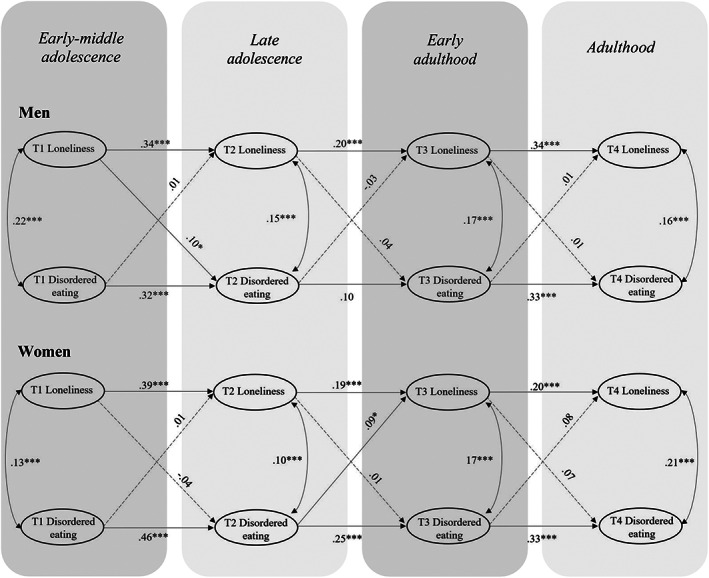
Multigroup random intercept cross‐lagged panel model (RI‐CLPM) examining the association between loneliness and disordered eating for men and women. Only within‐person effects are depicted
3.3. Prospective associations between loneliness and dieting
Next, we conducted RI‐CLPM analyses with the dieting subscale. The overall model fit for the two‐group model was good (see Table 2). Figure 3 displays the results from gender‐specific analysis. At the between level, no significant associations were observed between the two intercepts of loneliness and dieting. At the within the level, the analysis revealed a significant cross‐lagged association from loneliness in early‐middle adolescence to dieting symptoms in late adolescence for boys only, indicating loneliness on the within‐person level to be associated with within‐person changes in dieting during this period. The results of testing gender‐specific associations showed that the cross‐lagged associations from loneliness in early‐middle adolescence to dieting in late adolescence were significantly stronger for boys than for girls, ∆χ2 (1) = 4.84, p = .027.
FIGURE 3.
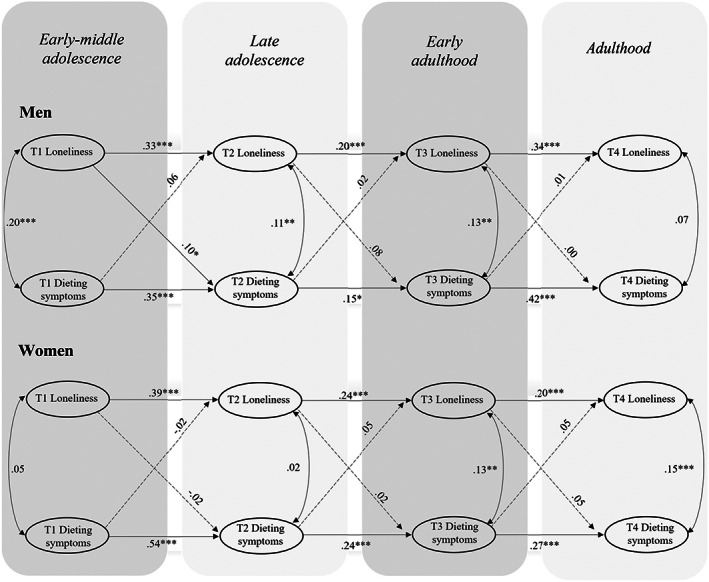
Multigroup random intercept cross‐lagged panel model (RI‐CLPM) examining the association between loneliness and dieting for men and women. Only within‐person effects are depicted
3.4. Prospective associations between loneliness and bulimic symptoms
Regarding multigroup RI‐CLPM results for loneliness and bulimic symptoms, the model fit for the two groups was also good (see Table 2). Figure 4 presents the results. At the between level, the associations between the intercepts were significant for both males (r = .43, p < .001) and females (r = .19, p = .010). At the within the level, significant cross‐lagged paths were found only among females, where bulimic symptoms in late adolescence predicted more loneliness in emerging adulthood, loneliness in emerging adulthood predicted more bulimic symptoms in adulthood, and bulimic symptoms in emerging adulthood predicted more loneliness in adulthood. Constraining one parameter at a time revealed a significantly stronger cross‐lagged association from loneliness in emerging adulthood to bulimic symptoms in adulthood for women than for men, ∆χ2 (1) = 5.28, p = .025.
FIGURE 4.
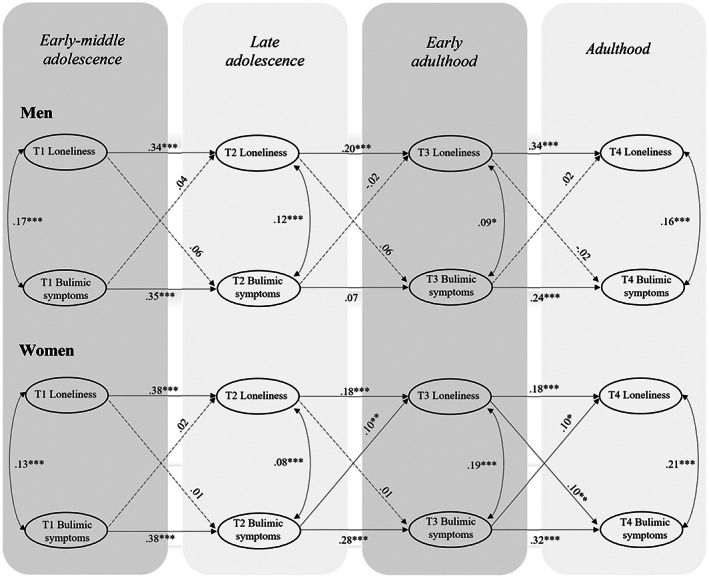
Multigroup random intercept cross‐lagged panel model (RI‐CLPM) examining the association between loneliness and bulimic symptoms for men and women. Only within‐person effects are depicted
4. DISCUSSION
Following a large population‐based sample throughout 13 years covering adolescence and young adulthood, this study used RI‐CLPM to examine, for the first time, the longitudinal, within‐person associations between loneliness and disordered eating among males and females. Within‐person, cross‐lagged estimates showed that the associations varied by gender and developmental period. Among boys, loneliness in early‐middle adolescence was prospectively related to more disordered eating and dieting 2 years later. Among women, we identified bidirectional prospective associations from early adulthood to adulthood between loneliness and bulimic symptoms. Moreover, among women, late adolescent disordered eating and bulimic symptoms were related to higher levels of loneliness in early adulthood, whereas no significant associations were observed earlier in adolescence for any type of disordered eating.
The significant within‐person associations between loneliness in early‐middle adolescence and disordered eating in late adolescence among boys indicate that feelings of loneliness may render boys vulnerable to developing disordered eating during adolescence, even when adjusting for all time‐invariant confounding. Of note, the significant association with male dieting in adolescence indicates that the relationship between loneliness and the overall disordered eating score is mainly driven by dieting behavior. Early and middle adolescence entails profound physical, cognitive, and affective developmental changes and is therefore a period characterized by heightened vulnerability to problems in regulation of emotions and behaviors, particularly among boys (Steinberg, 2005). At this age, adolescents are also more susceptible to peer influence and the need to belong to a social group becomes increasingly important (Pattiselanno et al., 2015). Feelings of loneliness may therefore be of particular importance for guiding emotions and behavior, including eating symptomatology, in this developmental period. In addition, boys increasingly focus on their own bodies in terms of body performance and muscularity as they navigate through adolescence (Eisenberg et al., 2012; Ricciardelli, 2012). Thus, lonely boys may attempt to become more integrated within their peer group by engaging in intense physical exercise and unhealthy eating behaviors to build muscle mass (McCabe & Ricciardelli, 2003) or reduce weight (Ricciardelli, 2012; Vincent & McCabe, 2000), which may explain the within‐person longitudinal association between loneliness and dieting in adolescence.
In contrast, no significant associations between loneliness and any form of disordered eating were found among girls in early‐middle and late adolescence. A potential explanation of this finding is that the pervasive norm for female thinness (Wertheim & Paxton, 2012) may be the main driving factor for disordered eating for many adolescent girls, independent of whether they feel socially isolated or not. Moreover, some aspects of social integration may even promote disordered eating. For example, research has revealed that adolescent girls frequently use “fat talk” when socializing (Shannon & Mills, 2015; Sharpe et al., 2013). Such negative remarks about one's own or another's appearance may, in turn, lead to more disordered eating symptoms, counterbalancing the potential negative effects of loneliness. Research has also shown that, during early‐mid adolescence, boys and girls differ in terms of stage of pubertal maturation (Tanner, 1971), whereby girls, in general, go through puberty earlier than boys (Hayward, 2003), and such differences may explain gender differences in the association between loneliness and disordered eating in adolescence. However, such potential explanations are speculative and further research examining gender differences is needed.
When examining female disordered eating later in life, we found that disordered eating prospectively predicted increased levels of loneliness, which supports our hypothesis that eating problems may indeed promote social withdrawal and loneliness among women (Fairburn & Harrison, 2003; Levine, 2012). Bulimic symptoms may be of particular importance for the development of loneliness, as indicated by the significant association between the bulimia‐food preoccupation subscale and loneliness among women. The results are in line with the notion that disordered eating in general, and bulimic symptoms in particular, are often accompanied by feelings of shame and guilt (Stice et al., 2000). Such feelings may, in turn, lead to social isolation and loneliness, especially in the late teens through the mid‐20s, a developmental period where new social relationships are formed and where people typically lack the daily companionship of either their family of origin or their family to be (Arnett, 2000). Women in this age group with disordered eating may, therefore, be particularly prone to isolate themselves from the normalizing influence of their peers and family, allowing their unhealthy eating behaviors, such as bulimic symptoms, to persist unchallenged (Levine, 2012).
Nevertheless, we also found reverse associations in that loneliness predicted increased bulimic symptoms among women. Again, the particular situation of young adulthood may increase lonely people's risk of developing bulimic symptoms: In this age group, many of those who experience loneliness may live alone; thus, they may not be exposed to the type of “social control” from family members that would make it difficult for them to maintain symptoms such as binging and purging (von Soest & Wichstrøm, 2006). Moreover, it is possible that women who isolate themselves and feel lonely to a larger degree than men struggle with bulimic symptoms, such as purging and binging, as a way to distract themselves and numb the negative emotions that result from feelings of failing in the interpersonal domain (Fairburn et al., 2003; Murphy et al., 2012).
Our results thus indicate that loneliness and bulimic symptoms are interconnected in a reciprocal fashion among women, where loneliness and bulimic symptoms exacerbate each other in a maladaptive cycle (Esplen et al., 2000; Levine, 2012). Consequently, our findings indicate that loneliness and bulimic symptoms may foster each other through a reciprocal process among women during young adulthood.
4.1. Limitations
Our results should be interpreted within the context of several limitations. Because participants were Norwegian, generalizing the present results to other countries and cultures should be approached with care. The study also relied solely on self‐reports from one source. However, as the rater did not change over time, common method bias is accounted for by adjusting for the random intercepts in the model. As another factor to consider, we studied disordered eating symptoms, but no information about ED diagnoses was included in the data. Therefore, it cannot be ruled out that prospective associations would differ if EDs were examined. Moreover, there have been critics questioning the validity of the EAT short version questioning its validity for measuring disordered eating among non‐clinical samples (Engelsen & Hagtvet, 1999) and especially among men (Murray et al., 2017; Sangha et al., 2019). Our study also shows that the internal consistency of the bulimia‐food preoccupation subscale and the loneliness measure was lower at earlier data collection waves than later ones. Even though this finding is consistent with previous research showing that individual difference instruments obtain lower reliability for younger than older participants (McFarland & Sparks, 1985), the heterogeneity in internal consistency may indicate that these measures are perceived somewhat differently at different ages.
Another limitation concerns the partial overlap of different developmental periods across the first and second data collections, where early‐middle adolescence could not precisely be separated from late adolescence, as the age of the participants partly overlapped at these two data collections. Moreover, although time‐invariant factors were accounted for by our modeling approach, the potential effect of time‐varying factors (e.g., negative life events such as the death of a family member) were not addressed. In particular, negative affect was not considered as a time‐varying confounder or mediator in the association between loneliness and disordered eating.
Some researchers have recently argued that the RI‐CLPM does not allow for a perfect distinction between within‐person and between‐person variance (Orth et al., 2021). Nevertheless, based on the current state of knowledge, RI‐CLPMs are the preferred state‐of‐the‐art models when examining within‐person developmental processes (Orth et al., 2021).
As with most longitudinal research, we observed attrition bias, as key variables in this study (i.e., loneliness, disordered eating, gender) were related to drop‐out, and therefore our findings should be interpreted with caution. However, simulation studies have shown that—even though nonrandom attrition affecting the results cannot be completely ruled out—associations between variables are only to a small degree affected by systematic attrition (Gustavson et al., 2012). Moreover, we applied a full information maximum likelihood procedure, which produces less biased estimates than complete case analysis (Enders & Bandalos, 2001). Finally, the effect sizes reported were small to moderate. However, large‐sized associations may not be expected, given the rather long time span involved and the rigorous control for all time‐invariant confounding in our analyses.
4.2. Implications for practice and research
Our findings underscore that the longitudinal associations of loneliness with disordered eating vary by timing and gender in the transition from adolescence to young adulthood. In line with the Interpersonal Model of EDs (Wilfley et al., 1997; Burke et al., 2018), the study highlights the importance of considering the social factors that may be involved in the onset of disordered eating when designing preventive and intervention efforts, particularly in adolescent boys and women in young adulthood. Nevertheless, further research exploring the intersection of other relevant time‐varying constructs, such as negative affect and negative life events, with loneliness and disordered eating is needed to better inform prevention and early intervention strategies.
Future studies should expand our research to different populations, such as clinical samples and participants from diverse locations and ethnic backgrounds. Furthermore, it would be interesting to examine whether the present findings hold when using different measures for disordered eating, such as clinical interviews, and other self‐report measures more suitable for boys, such as the Eating Disorder Assessment for Men (Stanford & Lemberg, 2012). It should also be acknowledged that loneliness could be a non‐specific/transdiagnostic risk factor for other mental health problems (Beutel et al., 2017) and therefore not specific to ED symptoms. We therefore encourage future studies to explore the nature of the prospective association between loneliness and other forms of psychopathology on a within‐person level. Finally, further work examining the temporal association between loneliness and disordered eating should consider shorter‐interval longitudinal monitoring across specific developmental periods in adolescence (i.e., early, middle, and late adolescence). Such studies could identify potential gender differences in associations at specific stages of maturation on these associations and thereby inform age‐specific prevention programs in adolescence.
5. CONCLUSION
This study contributes to the existing knowledge by examining the prospective associations between loneliness and disordered eating, which seems to be driven by dieting for boys and bulimic behavior for women while accounting for all time‐invariant confounding. In adolescence, more loneliness appeared to predict more disordered eating and dieting among boys. In contrast, in the transition to young adulthood, both disordered eating and bulimic symptoms predicted more loneliness among women. In addition, reciprocal associations between loneliness and bulimic symptoms appeared among women, indicating that both foster each other. Our findings highlight the complex interrelationship between loneliness and disordered eating and suggest that social factors have to be taken into account when designing prevention strategies aimed at disordered eating.
AUTHOR CONTRIBUTIONS
Laura Cortés‐García: Conceptualization; data curation; formal analysis; methodology; visualization; writing – original draft; writing – review and editing. Rubén Rodríguez Cano: Data curation; formal analysis; writing – review and editing. Tilmann von Soest: Conceptualization; data curation; funding acquisition; methodology; writing – review and editing.
FUNDING INFORMATION
This research was supported by two grants from the Research Council of Norway, Grant Numbers: 288083 and 301010.
CONFLICT OF INTEREST
All authors declare that they have no conflict of interest to disclose.
Cortés‐García, L. , Rodríguez‐Cano, R. , & von Soest, T. (2022). Prospective associations between loneliness and disordered eating from early adolescence to adulthood. International Journal of Eating Disorders, 55(12), 1678–1689. 10.1002/eat.23793
Action Editor: Anja Hilbert
Funding information Norges Forskningsråd, Grant/Award Numbers: 288083, 301010
Contributor Information
Laura Cortés‐García, Email: l.c.garcia@psykologi.uio.no.
Tilmann von Soest, Email: t.v.soest@psykologi.uio.no.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy and ethical restrictions.
REFERENCES
- Abebe, D. S. , Torgersen, L. , Lien, L. , Hafstad, G. S. , & von Soest, T. (2014). Predictors of disordered eating in adolescence and young adulthood: A population‐based, longitudinal study of females and males in Norway. International Journal of Behavioral Development, 38(2), 128–138. 10.1177/0165025413514871 [DOI] [Google Scholar]
- Ackard, D. M. , Fulkerson, J. A. , & Neumark‐Sztainer, D. (2011). Psychological and behavioral risk profiles as they relate to eating disorder diagnoses and symptomatology among a school‐based sample of youth. International Journal of Eating Disorders, 44(5), 440–446. 10.1002/eat.20846 [DOI] [PubMed] [Google Scholar]
- Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American Psychologist, 55(5), 469–480. 10.1037/0003-066X.55.5.469 [DOI] [PubMed] [Google Scholar]
- Basile, B. (2004). Self‐disclosure in eating disorders. Eating and Weight Disorders ‐ Studies on Anorexia, Bulimia and Obesity, 9(3), 217–223. 10.1007/BF03325070 [DOI] [PubMed] [Google Scholar]
- Berry, D. , & Willoughby, M. T. (2017). On the practical interpretability of cross‐lagged panel models: Rethinking a developmental workhorse. Child Development, 88(4), 1186–1206. 10.1111/cdev.12660 [DOI] [PubMed] [Google Scholar]
- Beutel, M. E. , Klein, E. M. , Brähler, E. , Reiner, I. , Jünger, C. , Michal, M. , Wiltink, J. , Wild, P. S. , Münzel, T. , Lackner, K. J. , & Tibubos, A. N. (2017). Loneliness in the general population: Prevalence, determinants and relations to mental health. BMC Psychiatry, 17(1), 97. 10.1186/s12888-017-1262-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buecker, S. , Maes, M. , Denissen, J. J. A. , & Luhmann, M. (2020). Loneliness and the big five personality traits: A meta‐analysis. European Journal of Personality, 34(1), 8–28. 10.1002/per.2229 [DOI] [Google Scholar]
- Burke, N. L. , Karam, A. M. , Tanofsky‐Kraff, M. , & Wilfley, D. E. (2018). Interpersonal psychotherapy for the treatment of eating disorders. In Agras W. S. & Robinson A. (Eds.), The Oxford handbook of eating disorders (pp. 287–318). Oxford University Press. [Google Scholar]
- Cacioppo, J. T. , & Patrick, W. (2008). Loneliness: Human nature and the need for social connection (pp. xiv, 317). W W Norton & Company. [Google Scholar]
- Cain, A. S. , Bardone‐Cone, A. M. , Abramson, L. Y. , Vohs, K. D. , & Joiner, T. E. (2008). Refining the relationships of perfectionism, self‐efficacy, and stress to dieting and binge eating: Examining the appearance, interpersonal, and academic domains. International Journal of Eating Disorders, 41(8), 713–721. 10.1002/eat.20563 [DOI] [PubMed] [Google Scholar]
- Cassin, S. E. , & von Ranson, K. M. (2005). Personality and eating disorders: A decade in review. Clinical Psychology Review, 25(7), 895–916. 10.1016/j.cpr.2005.04.012 [DOI] [PubMed] [Google Scholar]
- Day, F. , Ong, K. O. , & Perry, J. R. B. (2018). Elucidating the genetic basis of social interaction and isolation. Nature Communications, 9(1), 2457. 10.1038/s41467-018-04930-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Decaluwé, V. , & Braet, C. (2004). Assessment of eating disorder psychopathology in obese children and adolescents: Interview versus self‐report questionnaire. Behaviour Research and Therapy, 42(7), 799–811. 10.1016/j.brat.2003.07.008 [DOI] [PubMed] [Google Scholar]
- Eisenberg, M. E. , Wall, M. , & Neumark‐Sztainer, D. (2012). Muscle‐enhancing behaviors among adolescent girls and boys. Pediatrics, 130(6), 1019–1026. 10.1542/peds.2012-0095 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enders, C. K. , & Bandalos, D. L. (2001). The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Structural Equation Modeling: A Multidisciplinary Journal, 8(3), 430–457. 10.1207/S15328007SEM0803_5 [DOI] [Google Scholar]
- Engelsen, B. K. , & Hagtvet, K. A. (1999). The dimensionality of the 12‐item version of the eating attitudes test. Confirmatory factor analyses. Scandinavian Journal of Psychology, 40(4), 293–300. 10.1111/1467-9450.404129 [DOI] [PubMed] [Google Scholar]
- Esplen, M. J., Garfinkel, P., & Gallop, R. (2000). Relationship between self‐soothing, aloneness, and evocative memory in bulimia nervosa. International Journal of Eating Disorders, 27(1), 96–100. https://doi.org/10.1002/(sici)1098‐108x(200001)27:1<96::aid‐eat11>3.0.co;2‐s [DOI] [PubMed] [Google Scholar]
- Faber, A. , Dubé, L. , & Knäuper, B. (2018). Attachment and eating: A meta‐analytic review of the relevance of attachment for unhealthy and healthy eating behaviors in the general population. Appetite, 123, 410–438. 10.1016/j.appet.2017.10.043 [DOI] [PubMed] [Google Scholar]
- Fairburn, C. G. , Cooper, Z. , & Shafran, R. (2003). Cognitive behaviour therapy for eating disorders: A “transdiagnostic” theory and treatment. Behaviour Research and Therapy, 41(5), 509–528. 10.1016/s0005-7967(02)00088-8 [DOI] [PubMed] [Google Scholar]
- Fairburn, C. G. , & Harrison, P. J. (2003). Eating disorders. Lancet, 361(9355), 407–416. 10.1016/S0140-6736(03)12378-1 [DOI] [PubMed] [Google Scholar]
- Fekken, G. C. , Boland, F. J. , & Vanderheyden, D. A. (1988). Critical variables associated with bingeing and bulimia in a university population: A factor analytic study. International Journal of Eating Disorders, 7(3), 321–329. [DOI] [Google Scholar]
- Garner, D. M. , Olmsted, M. P. , Bohr, Y. , & Garfinkel, P. E. (1982). The eating attitudes test: Psychometric features and clinical correlates. Psychological Medicine, 12(4), 871–878. 10.1017/s0033291700049163 [DOI] [PubMed] [Google Scholar]
- Grant, P. G. (2008). Food for the soul: Social and emotional origins of comfort eating in the morbidly obese. In Psychological responses to eating disorders and obesity (pp. 121–137). John Wiley & Sons. 10.1002/9780470773253.ch7 [DOI] [Google Scholar]
- Gustavson, K. , von Soest, T. , Karevold, E. , & Røysamb, E. (2012). Attrition and generalizability in longitudinal studies: Findings from a 15‐year population‐based study and a Monte Carlo simulation study. BMC Public Health, 12, 918. 10.1186/1471-2458-12-918 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamaker, E. L. , Kuiper, R. M. , & Grasman, R. P. P. P. (2015). A critique of the cross‐lagged panel model. Psychological Methods, 20(1), 102–116. 10.1037/a0038889 [DOI] [PubMed] [Google Scholar]
- Hayward, C. (2003). Gender differences at puberty. Cambridge University Press. 10.1017/CBO9780511489716 [DOI] [Google Scholar]
- Henriksen, R. E. , Torsheim, T. , & Thuen, F. (2014). Loneliness, social integration and consumption of sugar‐containing beverages: Testing the social baseline theory. PLoS One, 9(8), e104421. 10.1371/journal.pone.0104421 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keel, P. (2018). Epidemiology and course of eating disorders. In Agras W. S. & Robinson A. (Eds.), The Oxford handbook of eating disorders (pp. 34–43). Oxford University Press. 10.1093/oxfordhb/9780190620998.013.3 [DOI] [Google Scholar]
- Lavik, N. J. , Clausen, S. E. , & Pedersen, W. (1991). Eating behaviour, drug use, psychopathology and parental bonding in adolescents in Norway. Acta Psychiatrica Scandinavica, 84(4), 387–390. 10.1111/j.1600-0447.1991.tb03164.x [DOI] [PubMed] [Google Scholar]
- Levine, M. P. (2012). Loneliness and eating disorders. Journal of Psychology, 146(1–2), 243–257. 10.1080/00223980.2011.606435 [DOI] [PubMed] [Google Scholar]
- Masheb, R. M. , & Grilo, C. M. (2006). Emotional overeating and its associations with eating disorder psychopathology among overweight patients with binge eating disorder. International Journal of Eating Disorders, 39(2), 141–146. 10.1002/eat.20221 [DOI] [PubMed] [Google Scholar]
- Mason, T. B. (2020). Loneliness, eating, and body mass index in parent–adolescent dyads from the family life, activity, sun, health, and eating study. Personal Relationships, 27(2), 420–432. 10.1111/pere.12321 [DOI] [Google Scholar]
- Mason, T. B. , Heron, K. E. , Braitman, A. L. , & Lewis, R. J. (2016). A daily diary study of perceived social isolation, dietary restraint, and negative affect in binge eating. Appetite, 97, 94–100. 10.1016/j.appet.2015.11.027 [DOI] [PubMed] [Google Scholar]
- McCabe, M. P. , & Ricciardelli, L. A. (2003). Sociocultural influences on body image and body changes among adolescent boys and girls. Journal of Social Psychology, 143(1), 5–26. 10.1080/00224540309598428 [DOI] [PubMed] [Google Scholar]
- McFarland, S. G. , & Sparks, C. M. (1985). Age, education, and the internal consistency of personality scales. Journal of Personality and Social Psychology, 49(6), 1692–1702. 10.1037/0022-3514.49.6.1692 [DOI] [Google Scholar]
- Mulder, J. D. , & Hamaker, E. L. (2020). Three extensions of the random intercept cross‐lagged panel model. Structural Equation Modeling: A Multidisciplinary Journal, 28(4), 638–648. 10.1080/10705511.2020.1784738 [DOI] [Google Scholar]
- Murphy, R. , Straebler, S. , Basden, S. , Cooper, Z. , & Fairburn, C. G. (2012). Interpersonal psychotherapy for eating disorders. Clinical Psychology & Psychotherapy, 19(2), 150–158. 10.1002/cpp.1780 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murray, S. B. , Nagata, J. M. , Griffiths, S. , Calzo, J. P. , Brown, T. A. , Mitchison, D. , Blashill, A. J. , & Mond, J. M. (2017). The enigma of male eating disorders: A critical review and synthesis. Clinical Psychology Review, 57, 1–11. 10.1016/j.cpr.2017.08.001 [DOI] [PubMed] [Google Scholar]
- Orth, U. , Clark, D. A. , Donnellan, M. B. , & Robins, R. W. (2021). Testing prospective effects in longitudinal research: Comparing seven competing cross‐lagged models. Journal of Personality and Social Psychology, 120(4), 1013–1034. 10.1037/pspp0000358 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pattiselanno, K. , Dijkstra, J. K. , Steglich, C. , Vollebergh, W. , & Veenstra, R. (2015). Structure matters: The role of clique hierarchy in the relationship between adolescent social status and aggression and Prosociality. Journal of Youth and Adolescence, 44(12), 2257–2274. 10.1007/s10964-015-0310-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pritchard, M. E. , & Yalch, K. L. (2009). Relationships among loneliness, interpersonal dependency, and disordered eating in young adults. Personality and Individual Differences, 46(3), 341–346. 10.1016/j.paid.2008.10.027 [DOI] [Google Scholar]
- Raspopow, K. , Matheson, K. , Abizaid, A. , & Anisman, H. (2013). Unsupportive social interactions influence emotional eating behaviors. The role of coping styles as mediators. Appetite, 62, 143–149. 10.1016/j.appet.2012.11.031 [DOI] [PubMed] [Google Scholar]
- Ricciardelli, L. (2012). Body image development – Adolescent boys. In Cash T. F. (Ed.), Encyclopedia of body image and human appearance (pp. 180–186). Elsevier. [Google Scholar]
- Rotenberg, K. J. , Bharathi, C. , Davies, H. , & Finch, T. (2013). Bulimic symptoms and the social withdrawal syndrome. Eating Behaviors, 14(3), 281–284. 10.1016/j.eatbeh.2013.05.003 [DOI] [PubMed] [Google Scholar]
- Rotenberg, K. J. , & Flood, D. (1999). Loneliness, dysphoria, dietary restraint, and eating behavior. International Journal of Eating Disorders, 25(1), 55–64. [DOI] [PubMed] [Google Scholar]
- Russell, D. , Peplau, L. A. , & Cutrona, C. E. (1980). The revised UCLA loneliness scale: Concurrent and discriminant validity evidence. Journal of Personality and Social Psychology, 39(3), 472–480. 10.1037/0022-3514.39.3.472 [DOI] [PubMed] [Google Scholar]
- Sangha, S. , Oliffe, J. L. , Kelly, M. T. , & McCuaig, F. (2019). Eating disorders in males: How primary care providers can improve recognition, diagnosis, and treatment. American Journal of Men's Health, 13(3), 1557988319857424. 10.1177/1557988319857424 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Satorra, A. (2000). Scaled and adjusted restricted tests in multi‐sample analysis of moment structures. In Heijmans R. D. H., Pollock D. S. G., & Satorra A. (Eds.), Innovations in multivariate statistical analysis. A Festschrift for Heinz Neudecker (pp. 233–247). Kluwer Academic. [Google Scholar]
- Schutz, H. K. , & Paxton, S. J. (2007). Friendship quality, body dissatisfaction, dieting and disordered eating in adolescent girls. British Journal of Clinical Psychology, 46(1), 67–83. 10.1348/014466506x115993 [DOI] [PubMed] [Google Scholar]
- Selig, J. P. , & Little, T. D. (2012). Autoregressive and cross‐lagged panel analysis for longitudinal data. In Laursen B., Little T. D., & Card N. A. (Eds.), Handbook of developmental research methods (pp. 265–278). The Guilford Press. [Google Scholar]
- Shannon, A. , & Mills, J. S. (2015). Correlates, causes, and consequences of fat talk: A review. Body Image, 15, 158–172. 10.1016/j.bodyim.2015.09.003 [DOI] [PubMed] [Google Scholar]
- Sharpe, H. , Naumann, U. , Treasure, J. , & Schmidt, U. (2013). Is fat talking a causal risk factor for body dissatisfaction? A systematic review and meta‐analysis. International Journal of Eating Disorders, 46(7), 643–652. 10.1002/eat.22151 [DOI] [PubMed] [Google Scholar]
- Slane, J. D. , Klump, K. L. , McGue, M. , & Iacono, W. G. (2014). Developmental trajectories of disordered eating from early adolescence to young adulthood: A longitudinal study. International Journal of Eating Disorders, 47(7), 793–801. 10.1002/eat.22329 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanford, S. C., & Lemberg, R. (2012). Measuring eating disorders in men: Development of the eating disorder assessment for men (EDAM). Eating Disorders, 20(5), 427–436. 10.1080/10640266.2012.715522 [DOI] [PubMed] [Google Scholar]
- Steinberg, L. (2005). Cognitive and affective development in adolescence. Trends in Cognitive Sciences, 9(2), 69–74. 10.1016/j.tics.2004.12.005 [DOI] [PubMed] [Google Scholar]
- Stice, E. , Hayward, C. , Cameron, R. P. , Killen, J. D. , & Taylor, C. B. (2000). Body‐image and eating disturbances predict onset of depression among female adolescents: A longitudinal study. Journal of Abnormal Psychology, 109(3), 438–444. 10.1037/0021-843X.109.3.438 [DOI] [PubMed] [Google Scholar]
- Stice, E. , Marti, C. N. , Shaw, H. , & Jaconis, M. (2009). An 8‐year longitudinal study of the natural history of threshold, subthreshold, and partial eating disorders from a community sample of adolescents. Journal of Abnormal Psychology, 118(3), 587–597. 10.1037/a0016481 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanner, J. M. (1971). Sequence, tempo, and individual variation in the growth and development of boys and girls aged twelve to sixteen. Daedalus, 100(4), 907–930. [Google Scholar]
- Treasure, J. , Crane, A. , McKnight, R. , Buchanan, E. , & Wolfe, M. (2011). First do no harm: Iatrogenic maintaining factors in anorexia nervosa. European Eating Disorders Review, 19(4), 296–302. 10.1002/erv.1056 [DOI] [PubMed] [Google Scholar]
- Vincent, M. A. , & McCabe, M. P. (2000). Gender differences among adolescents in family, and peer influences on body dissatisfaction, weight loss, and binge eating behaviors. Journal of Youth and Adolescence, 29(2), 205–221. 10.1023/A:1005156616173 [DOI] [Google Scholar]
- von Soest, T. , Luhmann, M. , & Gerstorf, D. (2020). The development of loneliness through adolescence and young adulthood: Its nature, correlates, and midlife outcomes. Developmental Psychology, 56(10), 1919–1934. 10.1037/dev0001102 [DOI] [PubMed] [Google Scholar]
- von Soest, T. , & Wichstrøm, L. (2006). Cohabitation reduces bulimic symptoms in young women. International Journal of Eating Disorders, 39(6), 484–491. 10.1002/eat.20273 [DOI] [PubMed] [Google Scholar]
- Wade, T. D., & Bulik, C. M. (2018). Genetic influences on eating disorders. In W. S. Agras & A. Robinson (Eds.), The Oxford handbook of eating disorders (pp. 80–105). Oxford University Press. [Google Scholar]
- Wertheim, E. H. , & Paxton, S. J. (2012). Body image development—Adolescent girls. In Cash T. (Ed.), Encyclopedia of body image and human appearance (pp. 187–193). Academic Press. 10.1016/B978-0-12-384925-0.00029-8 [DOI] [Google Scholar]
- Wichstrøm, L. (1995). Social, psychological and physical correlates of eating problems: A study of the general adolescent population in Norway. Psychological Medicine, 25(3), 567–579. 10.1017/S0033291700033481 [DOI] [PubMed] [Google Scholar]
- Wilfley, D. E. , Mackenzie, K. , Welch, R. R. , Ayres, V. E. , & Weissman, M. M. (2000). Interpersonal psychotherapy for group. Basic Books. [Google Scholar]
- Wilfley, D. E., Pike, K. M., & Striegel‐Moore, R. H. (1997). Toward an integrated model of risk for binge eating disorder. Journal of Gender, Culture, and Health, 2, 1–3. [Google Scholar]
- Woolley, K. , Fishbach, A. , & Wang, R. M. (2020). Food restriction and the experience of social isolation. Journal of Personality and Social Psychology, 119(3), 657–671. 10.1037/pspi0000223 [DOI] [PubMed] [Google Scholar]
- Wright, A. , & Pritchard, M. E. (2009). An examination of the relation of gender, mass media influence, and loneliness to disordered eating among college students. Eating and Weight Disorders, 14(2–3), e144–e147. 10.1007/BF03327813 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy and ethical restrictions.