

Abstract
This paper presents a study of renal function in 102 patients with lead poisoning admitted to the Occupational Diseases Clinic in Bucharest during the past 10 years; nearly half the patients had no history of lead colic. Every possible cause of renal damage, other than lead, was excluded by a careful differential diagnosis.
Renal function was investigated by repeated determinations of blood urea, creatinine and uric acid, urea clearance, and endogenous creatinine clearance tests.
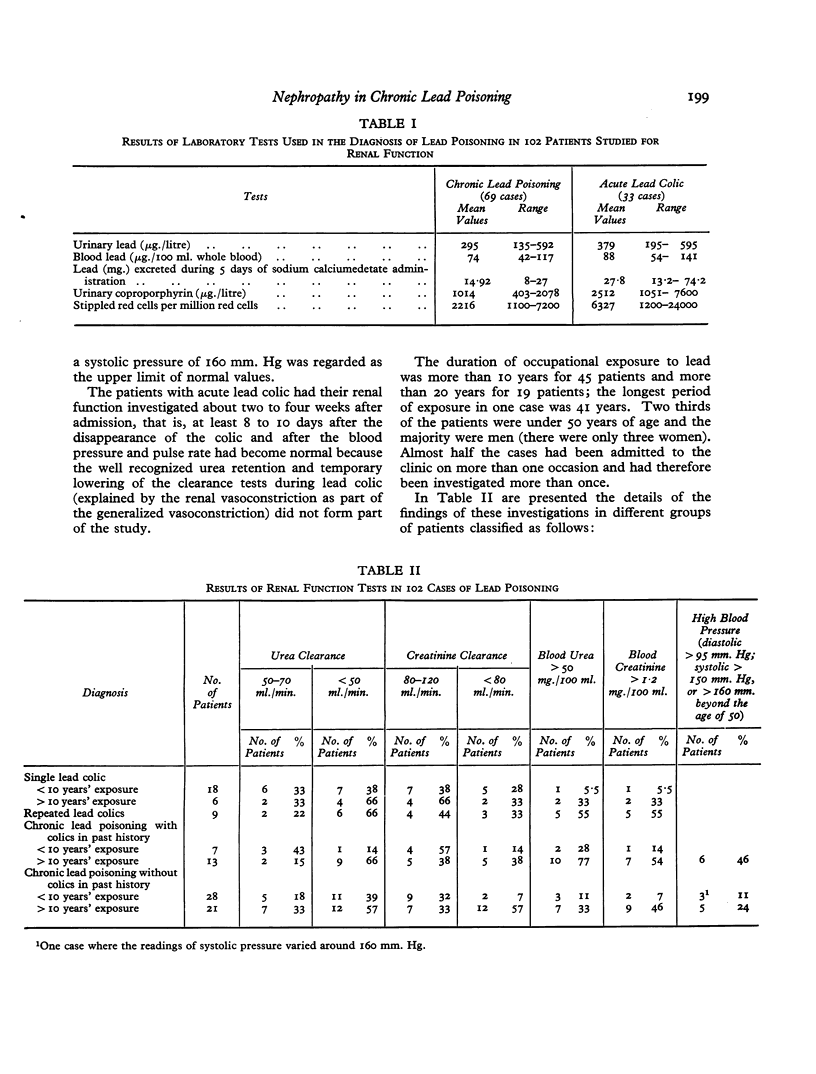
Significant decreases of the clearance values (less than 50 ml./min. urea clearance and less than 80 ml./min. creatinine clearance), persistent high blood urea (more than 50 mg./100 ml.), and high blood creatinine (more than 1·2 mg./100 ml.) were found in a significant number of cases. These signs of impaired renal function were more frequent in the group of patients with chronic lead poisoning who had had several episodes of colic and an occupational exposure of more than 10 years. A high blood pressure was also found more frequently in this group of patients.
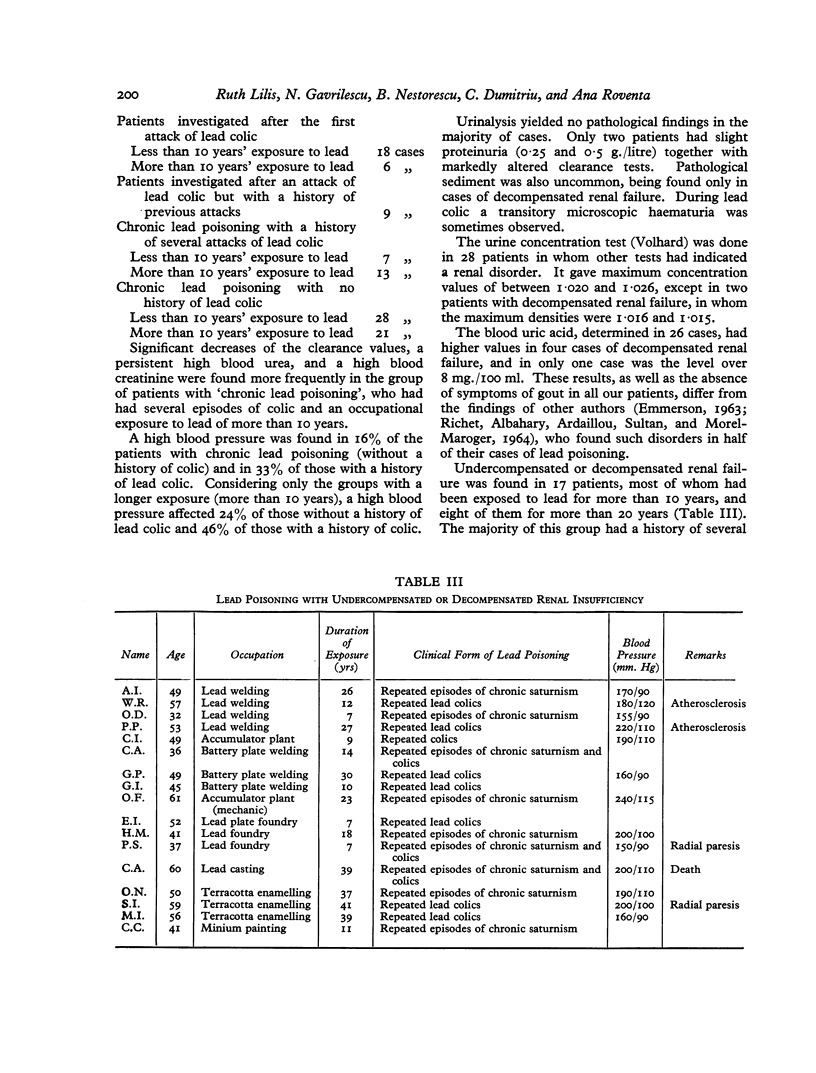
Undercompensated and decompensated renal failure was found in 17 patients, most of whom had been exposed to lead for more than 10 years and had a history of several attacks of colic. Arterial hypertension accompanied the chronic renal failure in 13 patients, the renal impairment generally preceding the rise in blood pressure by several years.
The duration of occupational lead exposure, the high absorption in the past, and the long period of observation of these patients, most of whom were repeatedly hospitalized, may explain the relatively high incidence (17 cases) of nephropathy with chronic renal failure in the present group.
Impairment of urea clearance seems to be the earliest sign, at a time when the creatinine clearance is still normal. As the duration of exposure lengthens and the patient is subjected to active episodes of poisoning the creatinine clearance also deteriorates. Persistent urea retention and high creatininaemia may follow in time, accompanied rather frequently by arterial hypertension. A study of some of the cases followed for several years demonstrated this progressive evolution of lead nephropathy.
A functional and transitory impairment of renal function is very probably caused by an impairment of intrarenal circulation, resulting from marked vasoconstriction of the renal vessels, forming part of the generalized vasoconstriction of lead poisoning. Prolonged exposure and frequently recurring episodes of acute poisoning may lead to progressive impairment of renal function and to the development of organic lesions.
Special attention should be paid to renal function tests in all cases with prolonged exposure to lead in order to prevent the development of severe lead nephropathy.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ANGEVINE J. M., KAPPAS A., DEGOWIN R. L., SPARGO B. H. Renal tubular nuclear inclusions of lead poisoning. A clinical and experimental study. Arch Pathol. 1962 Jun;73:486–494. [PubMed] [Google Scholar]
- BAADER E. W. L'aspect clinique de i'intoxication saturnine professionnelle. Maroc Med. 1958 Apr;37(395):409–415. [PubMed] [Google Scholar]
- BALDI G., SBERTOLI C. Evoluzione delle alterazioni renali che possono condurre al rene grinzo saturnino: un caso dimostrativo. Med Lav. 1957 Oct;48(10):533–538. [PubMed] [Google Scholar]
- BESSMAN S. P., LAYNE E. C., Jr A rapid procedure for the determination of lead in blood or urine in the presence of organic chelating agents. J Lab Clin Med. 1955 Jan;45(1):159–166. [PubMed] [Google Scholar]
- CRUTCHER J. C. CLINICAL MANIFESTATIONS AND THERAPY OF ACUTE LEAD INTOXICATION DUE TO THE INGESTION OF ILLICITLY DISTILLED ALCOHOL. Ann Intern Med. 1963 Nov;59:707–715. doi: 10.7326/0003-4819-59-5-707. [DOI] [PubMed] [Google Scholar]
- HENDERSON D. A. Chronic nephritis in Queensland. Australas Ann Med. 1955 Aug;4(3):163–177. doi: 10.1111/imj.1955.4.3.163. [DOI] [PubMed] [Google Scholar]
- LANDING B. H., NAKAI H. Histochemical properties of renal lead-inclusions and their demonstration in urinary sediment. Am J Clin Pathol. 1959 Jun;31(6):499–503. doi: 10.1093/ajcp/31.6.499. [DOI] [PubMed] [Google Scholar]