

Abstract
Background and Aims
The dengue virus is widespread throughout Bangladesh and significantly contributes to morbidity and mortality. One effective method for preventing further dengue epidemics is to reduce mosquito breeding at the most opportune period each year. This study aims to determine dengue prevalence in 2022 by comparing previous years' data and estimating the period of this disease's most significant incidence.
Methods
From the beginning of 2008–December 15, 2022, we looked at the monthly reports of cases made to the Bangladesh Institute of Epidemiology, Disease Control, and Research.
Results
According to our findings, there were 61089 confirmed dengue cases in 2022, with 269 fatalities ‐ the highest annual death toll for this disease since 2000. Almost one‐third (32.14%) of all dengue deaths in Bangladesh occurred in 2022 (1 January–15 December), highlighting the severity of the threat posed by this disease in the coming year. Furthermore, we observe that the months in the second half of any year in Bangladesh are the most at risk for dengue transmission. In 2022, Dhaka city and Chittagong are hit the hardest (incidence: 63.07% vs. 14.42%; morality: 63.34% vs. 24.16%), showing the relevance of population density in spreading this fatal disease.
Conclusion
Statistics show an increase in dengue cases every day, and the year 2022 will be marked as the peak of the disease's death prevalence. Both the individuals and the government of Bangladesh need to take action to reduce the dissemination of this epidemic. If not, the country will soon be in great peril.
Keywords: Bangladesh, DENV 1‐4, dengue, epidemic, outbreaks
1. INTRODUCTION
Dengue fever is an infectious disease spread by the bite of an infected Aedes mosquito and is caused by one of four antigenically different serotypes of the dengue virus (DENV 1‐4). 1 It can be found in both urban and semi‐urban settings across the tropics and sub‐tropics, and more than half of the world's population is in danger of dengue fever. Moreover, there are over 400 million documented cases and 22000 deaths of dengue virus infection every year. 2 , 3 , 4 , 5 Dengue can cause anything from a slight fever to the life‐threatening dengue hemorrhagic fever (DHF) or dengue shock syndrome (DSS), characterized by a decrease in platelets, white blood cells, and an increase in vascular permeability. 5 Both endemic and epidemic cycles of dengue transmission have established their global presence, even though the virus is frequently asymptomatic in humans. 2
Dengue fever outbreak management is challenging in tropical regions, where year‐round warm temperatures make it possible for mosquitoes to reproduce and the virus to replicate. In addition, large‐scale dengue outbreak control is resource‐intensive, necessitating the deployment of insecticides to reduce mosquito populations and substantial medical personnel to care for those who become ill. 6 Because of its proximity to the equator and its subtropical/tropical climate, Bangladesh, like other Southeast Asian (SE) countries, has become an ideal environment for the dengue vector and the subsequent increase in dengue transmission. 7 According to the findings of the Bangladesh National Health Accounts (BNHA‐V) study, the dengue situation in Bangladesh is causing an economic burden in our health sector, just as it is in other lower and middle‐income countries. 8 Between 2012 and 2019, the largest dengue cases were reported in Dhaka, the capital and most populous city in Bangladesh, with a population of almost 16 million. 9 , 10
According to several studies, recovery from DENV infection is associated with permanent immunity against that serotype, whereas infection with different serotypes results in only transitory and partial protection, increasing the risk of severe dengue. 11 Indicators of dengue fever are similar to those of the common cold and influenza; that is why people get confused with the treatment of dengue. It can damage the liver by increasing the liver enzymes. 12 Evidence suggests that severe dengue patients experience systolic and diastolic cardiac impairment due to damage to the septum and right ventricular wall. 13 Studies suggest that dengue fever adversely affects the kidney, 14 eyes, 15 blood, 16 brain, 17 pancreas, 18 and endothelial cells. 19
A distinctive feature of dengue is that the likelihood of a severe and potentially fatal disease increases with each subsequent infection with a new serotype. 20 Little is known about how the virus communicates with the immune system or how specific forms of pre‐existing immunity can amplify illness. To prevent making a person extremely vulnerable to dengue fever, a safe and effective dengue vaccine must be tetravalent and concurrently elicit substantial and long‐lived protection against all four serotypes. 21 Moreover, illness awareness in a population and health‐related behavior are essential in disease prevention. 22 However, due to a lack of awareness, the people of Bangladesh are unaware of this potentially fatal illness. Given the growing number of dengue cases in Bangladesh and the recent spike in dengue‐related mortality in the country's most populous metropolis, Dhaka, it is crucial to regularly evaluate the level of education, awareness, and prevention efforts among locals.
Since dengue fever has spread to the point that it occurs every year during the monsoon in Bangladesh, a more precise accounting of the disease's incidence and mortality rate during the past two decades may aid in the diagnosis and control of future outbreaks. Therefore, this study aimed to examine the prevalence of dengue and the death rate associated with this disease to provide a complete picture of the dengue epidemic in Bangladesh.
2. METHODS
2.1. Setting, subjects, and contributors to the study
Data was compiled from two national databases, both of which had released the confirmed dengue cases and related death through a government press release from the Directorate General of Health Services (DGHS), Ministry of Health and Family Welfare, Bangladesh, and Institute of Epidemiology, Disease Control and Research (IEDCR), Bangladesh. https://old.dghs.gov.bd/index.php/bd/ and https://iedcr.gov.bd/surveillances/ were the two portals from which we collected all the released data.
All of the data are for the Bangladeshi population from January 1, 2000 to December 15, 2022. Curves were plotted with Microsoft Excel 2021.
3. RESULTS
From January 2008 to December 15, 2022, the monthly dengue case counts are shown in Table 1. Almost one‐third (31.87%) of all dengue fever cases during this period occurred in August. In 2022 though, things were different, as October saw more than one‐third (35.90%) of the year's dengue cases and November at the second position (31.65%). Due to the COVID‐19 pandemic, dengue fever in Bangladesh dropped dramatically in 2020 after 2019s unprecedented spike in dengue cases (which surpassed 100,000). In 2021, there were 28,429 cases of dengue fever, but from January to December 15, 2022, the disease had spread to almost 61,089 people. Since 2008, a total of 220,572 cases of dengue fever have been documented in Bangladesh; with new cases being reported every day, this disease poses a serious risk to the country. Moreover, the months of August, September, and October are the most vulnerable to a dengue outbreak in Bangladesh, as seen in Table 1. Nonetheless, the frequency of dengue fever cases in November 2022 suggests that this month is also a high‐risk month for the disease.
Table 1.
Monthly prevalence of cases from 2008–2022.
| Month | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | Cases | % Cases |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| January | 0 | 0 | 0 | 0 | 0 | 6 | 15 | 0 | 13 | 92 | 26 | 38 | 199 | 32 | 126 | 547 | 0.25 |
| February | 0 | 0 | 0 | 0 | 0 | 7 | 7 | 0 | 3 | 58 | 7 | 18 | 45 | 9 | 20 | 174 | 0.08 |
| March | 0 | 0 | 0 | 0 | 0 | 3 | 2 | 2 | 17 | 36 | 19 | 17 | 27 | 13 | 20 | 156 | 0.07 |
| April | 0 | 0 | 0 | 0 | 0 | 3 | 0 | 6 | 38 | 73 | 29 | 58 | 25 | 3 | 23 | 258 | 0.12 |
| May | 0 | 1 | 0 | 0 | 0 | 12 | 8 | 10 | 70 | 134 | 52 | 193 | 10 | 43 | 163 | 696 | 0.32 |
| June | 0 | 0 | 0 | 61 | 10 | 50 | 9 | 28 | 254 | 267 | 295 | 1884 | 20 | 272 | 737 | 3887 | 1.76 |
| July | 160 | 4 | 61 | 255 | 129 | 172 | 82 | 171 | 926 | 286 | 946 | 16,253 | 23 | 2286 | 1571 | 23,325 | 10.57 |
| August | 473 | 125 | 183 | 691 | 122 | 339 | 80 | 765 | 1451 | 346 | 1796 | 52,636 | 68 | 7698 | 3521 | 70,294 | 31.87 |
| September | 334 | 188 | 120 | 193 | 246 | 385 | 76 | 965 | 1544 | 430 | 3087 | 16,856 | 47 | 7841 | 9911 | 42,223 | 19.14 |
| October | 184 | 154 | 45 | 114 | 107 | 501 | 63 | 869 | 1077 | 512 | 2406 | 8143 | 164 | 5458 | 21,932 | 41,729 | 18.92 |
| November | 0 | 0 | 0 | 36 | 27 | 218 | 22 | 271 | 522 | 409 | 1192 | 4011 | 546 | 3567 | 19,334 | 30,155 | 13.67 |
| December | 0 | 0 | 0 | 9 | 0 | 53 | 11 | 75 | 145 | 126 | 293 | 1247 | 231 | 1207 | 3731 | 7128 | 3.23 |
| Total | 1151 | 472 | 409 | 1359 | 641 | 1749 | 375 | 3162 | 6060 | 2769 | 10,148 | 101,354 | 1405 | 28,429 | 61,089 | 220,572 | 100 |
Table 2 describes the prevalence of dengue fever and the death rate from 2000 to December 15, 2022. Based on the data in the table, Bangladesh recorded 2,42,919 cases of dengue disease from the year 2000. It is clear that 2022 had the highest annual mortality rate (0.44%, 32.14% of total death from 2000 to 2022) of any year in the 21st century, and the number of patients who perished from dengue fever continues to rise. Eight hundred thirty‐seven people lost their lives to dengue fever between 2000 and 2022, with almost half of those fatalities occurring in 2019 and 2022 alone (51.74%). These findings suggest that dengue fever is a severe problem in Bangladesh. In 2022, the number of confirmed dengue patients was 61,089 and the death was 269 till 15 December which is 32.14% of total death (837) from 2000. In 2003, approximately 2% of all diagnosed patients died (10 of 486); this was the highest annual mortality rate in the period spanning from 2000 to 2022, based on the diagnosed patients. While 466, 1151, 472, 409, and 375 people were respectively diagnosed with dengue in 2007, 2008, 2009, 2010, and 2014, no deaths were reported from the disease in any of those years (Table 3).
Table 2.
Year‐wise cases and deaths from 2000‐2022.
| Year | Cases | Death | Yearly Mortality rate (%) based on the confirmed cases | % of Yearly Death based on the total deaths (837) |
|---|---|---|---|---|
| 2000 | 5551 | 93 | 1.68 | 11.11 |
| 2001 | 2430 | 44 | 1.81 | 5.26 |
| 2002 | 6232 | 58 | 0.93 | 6.93 |
| 2003 | 486 | 10 | 2.06 | 1.19 |
| 2004 | 3934 | 13 | 0.33 | 1.55 |
| 2005 | 1048 | 4 | 0.38 | 0.48 |
| 2006 | 2200 | 11 | 0.50 | 1.31 |
| 2007 | 466 | 0 | 0.00 | 0.00 |
| 2008 | 1151 | 0 | 0.00 | 0.00 |
| 2009 | 472 | 0 | 0.00 | 0.00 |
| 2010 | 409 | 0 | 0.00 | 0.00 |
| 2011 | 1359 | 6 | 0.44 | 0.72 |
| 2012 | 641 | 1 | 0.16 | 0.12 |
| 2013 | 1749 | 2 | 0.11 | 0.24 |
| 2014 | 375 | 0 | 0.00 | 0.00 |
| 2015 | 3162 | 6 | 0.19 | 0.72 |
| 2016 | 6060 | 14 | 0.23 | 1.67 |
| 2017 | 2769 | 8 | 0.29 | 0.96 |
| 2018 | 10148 | 26 | 0.26 | 3.11 |
| 2019 | 101354 | 164 | 0.16 | 19.60 |
| 2020 | 1405 | 3 | 0.21 | 0.36 |
| 2021 | 28429 | 105 | 0.37 | 12.54 |
| 2022 | 61089 | 269 | 0.44 | 32.14 |
| Total | 242919 | 837 | 10.55 | 100.00 |
Table 3.
Year‐wise comparison of cases and deaths.
| Year | Cases | Death | p value |
|---|---|---|---|
| January 1, 2000–December 15, 2022 | 10,561.7 ± 5084.21 | 36.39 ± 14.02 | <0.05* |
| 2022 (January–December 15) | 5090.75 ± 2255.34 | 22.42 ± 10.91 | <0.05* |
| 2021 (January–December) | 2369.08 ± 881.90 | 8.75 ± 3.36 | 0.007** |
| 2019 (January–December) | 8446.17 ± 4395.53 | 13.67 ± 7.10 | 0.063 |
Figure 1 represents the cases of dengue fever and related deaths in Bangladesh by year (1 January 2000–December 15, 2022), and the monthly incidence and fatality rates for the year 2022 are shown in Figure 2. Two hundred sixty‐nine deaths were recorded in 2022, making it the deadliest year in the 22‐year span from 2000 to 2022, and new instances continue to be found every day, highlighting the epidemic's pervasiveness. In 2019, there were 164 fatalities, making it the second deadliest year on record; in that year, there were 1,01,354 confirmed cases of dengue fever. Figure 2 shows that October has the highest concentration of dengue illnesses, with 86 reported deaths attributable to this fetal disease, pointing to the fact that it poses a danger to Bangladesh. There were 19,334 confirmed dengue cases in November, and 113 died from this devastating, life‐threatening disease, making it the highest of any month in 2022. In the first half of December, there were 3731 patients affected with this disease, and 15 people died by it, pointing out that dengue severity may decrease due to the winter season.
Figure 1.
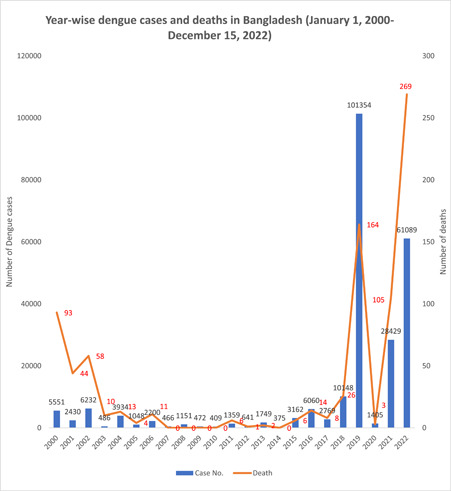
Year‐wise dengue cases and deaths in Bangladesh (January 1, 2000–December 15, 2022).
Figure 2.
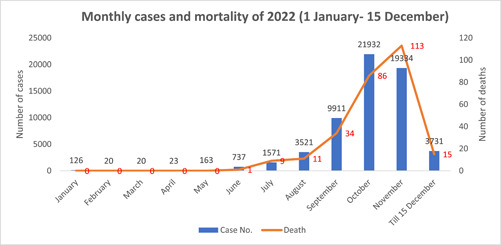
Monthly cases and mortality of 2022 (January 1–December 15).
Figures 3 and 4 show a distinct picture of dengue fever in 2021 and 2019, respectively; there were only 372 instances in the first half of 2021, which is approximately a third of the number of cases in the first half of 2022. The difference between the second half of these 2 years (July–December 2021 and July–18 November 2022) is 22,456 patients, indicating that dengue fever is more common in Bangladesh now than in 2021. In 2019, 101,354 cases of dengue fever were confirmed, with nearly 98% of cases occurring between July and December. The highest number of dengue cases and deaths occurred between July and December in 2019, 2021, and 2022, suggesting that the end of the year is a particularly vulnerable time for the spread of the disease.
Figure 3.
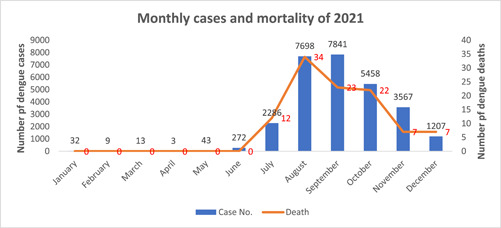
Monthly cases and mortality of 2021.
Figure 4.
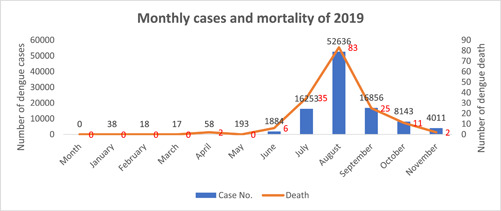
Monthly cases and mortality of 2019.
Figure 5 indicates the annual and monthly dengue virus reports from 2012 to December 15, 2022. The majority of confirmed dengue fever cases occurred in the latter half of the year, as depicted by the graph. In August 2019, 52,636 confirmed cases of dengue fever were the highest monthly total on record. The subsequent highest dengue confirmation was in October 2022, with 21,932 patients. With 16,856 and 16,253 instances, respectively, September and July of 2019 tied for third and fourth place.
Figure 5.
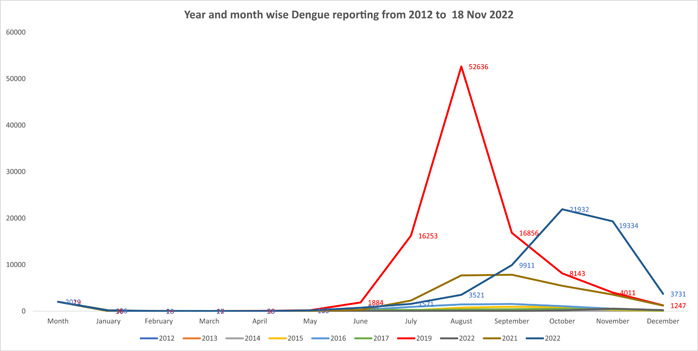
Year and month‐wise dengue reporting from 2012 to December 15, 2022.
Using data from October 1, 2022 to December 15, 2022, Figure 6 depicts the number of people who have been affected by dengue in the previous 76 days. On October 23rd, there was a record‐breaking cluster of dengue fever cases, with 1034 confirmed cases. There were some fluctuations from day to day, but the total number of dengue cases continued to rise, reaching 1094 on November 2, 2022. For the last 76 days, the number of confirmed dengue cases was lowest on Fridays. This is likely due to the fact that most hospitals and community clinics, especially diagnostic labs, were closed on Fridays in Bangladesh. Except for Fridays and 23 November, the dengue cases are more than 500 till November 24. Then the dengue confirms cases are declining with some fluctuations. On December 14 and 15, for the first time, dengue‐confirmed cases reached below 200 after a severe pandemic in the middle half of the year.
Figure 6.
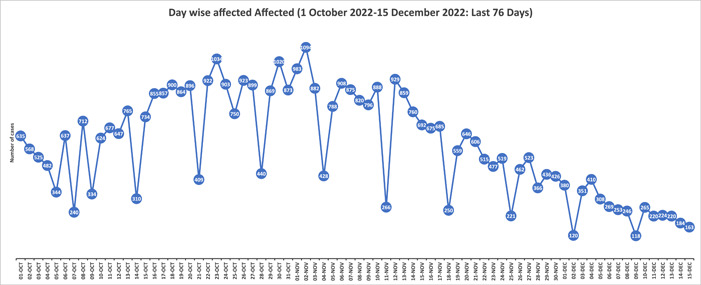
Day‐wise affected (October 1, 2022–December 15, 2022): Last 76 days.
Cases and fatalities from dengue fever in 2022 are shown by the geographical region depicted in Figure 7. Dhaka, the capital of Bangladesh, is the hardest hit by the dengue epidemic, which may be a result of the city's dense population. Dengue fever has devastated the inhabitants of the Dhaka metropolitan area, with 38,526 confirmed cases in the city alone. This accounts for around two‐thirds (63.07%) of the country's total dengue incidents. Dhaka city likewise has a high mortality rate, with 165 deaths (61.34%) out of 269 for the entire country. There were 8,809 cases (14.42%) of dengue in Chittagong, and 65 patients died (24.16%) from the disease there. Dengue fever is less common in Rangpur and Sylhet, with 172 and 124 confirmed cases. But there were no dengue deaths in these two Bangladeshi divisions.
Figure 7.
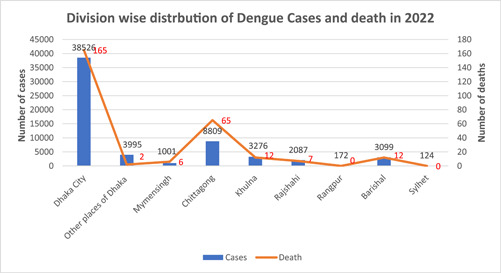
Division‐wise distribution of Dengue Cases and death in 2022.
4. DISCUSSION
Over half of the world's population in more than 100 countries now resides in DENV‐endemic regions, as the disease's incidence has increased by a factor of 30 in the last 50 years. 23 Dengue virus, like other members of the Flaviviridae family, is an enveloped virus that uses positive‐sense single‐stranded RNA as its genetic material. Researchers looking into this virus's life cycle uncovered potential host targets vital to the virus's reproduction process. 24 The spread of dengue fever is speeding up as a result of global factors like warming temperatures and increased human population density. 25 Dengue fever has spread around the world due to the proliferation of Aedes mosquitoes. 26 Because of its rapid spread in low‐ and middle‐income countries, this illness is a global concern currently.
In Asia, children under the age of 15 who are infected with DENV are at a higher risk of getting the severe disease than adults. 27 In contrast, moderate disease is more common in the adult population in the Americas. However, a rising trend of cases advancing toward DHF/DSS has also been seen in adults in the Americas. 27
Dengue fever is still a significant problem in Bangladesh's public health despite the efforts that have been made over the last decade to manage vectors. These efforts have focused on eliminating mosquitoes and the habitats in which they reproduce. 6 There have been only isolated outbreaks of dengue in Dhaka and other regions of the country before the year 2000. An unexpected dengue epidemic in 2000 led to 5551 cases and 93 fatalities, which posed a substantial threat to public health. 28 The climate in Bangladesh is ideal for the year‐round spread of diseases carried by Aedes mosquitoes. However, the months of May through August coincide with the monsoon season and its accompanying mosquitoes. 29 To combat Culex mosquitoes, the Bangladeshi government uses larvicide (Temephos) sprayed into drainage systems and fogging adulticides throughout the vector season.
According to the data we compiled, dengue incidence rises faster in early July and ends in December. Previous research has shown that August and September account for the vast majority (over 90%) of dengue fever cases. 29 Coronavirus disease caused dengue fever to decline after a significant increase in 2019. That may be due to a lot of overlap in symptoms between the two viral infections, making it difficult for doctors to tell them apart. 30 However, following COVID‐19, it blossoms, and dengue is already the leading cause of death in Bangladesh. Dengue fever was identified in 46,846 people in 2022; of those, 192 victims died from the illness due to its severity. From 2000 to the present, dengue has claimed the lives of 788 people, 492 of whom—more than 62.44%—died from 2019 to 2022. This statistic highlights how devastating the condition is. Moreover, Dhaka city is the most susceptible region for dengue in terms of prevalence and fatality. This problem is likely due in large part to the ever‐increasing population density.
5. CONCLUSION
During the monsoon season, Dengue fever spreads rapidly in Bangladesh. In 2022, however, after COVID‐19, its virulence poses a severe danger to national economies around the country. Raising public consciousness is crucial in reducing the risk of this fatal disease. The government of Bangladesh is also responsible for educating the public, running campaigns, and taking appropriate measures to mitigate the impact of the disease.
AUTHOR CONTRIBUTIONS
Khokon Kanti Bhowmik: Data curation; formal analysis; methodology; validation; writing—original draft. Jannatul Ferdous: Data curation; formal analysis; validation; writing—original draft. Prodip Kumar Baral: Methodology; validation; visualization; writing—original draft. Mohammad Safiqul Islam: Conceptualization; data curation; resources; software; supervision; writing—review & editing.
CONFLICT OF INTEREST STATEMENT
The corresponding author Mohammad Safiqul Islam is an editorial board member and will not be involved in decision‐making regarding this manuscript. The researchers have no other conflicts of interest.
TRANSPARENCY STATEMENT
The lead author Mohammad Safiqul Islam affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Bhowmik KK, Ferdous J, Baral PK, Islam MS. Recent outbreak of dengue in Bangladesh: a threat to public health. Health Sci Rep. 2023;6:e1210. 10.1002/hsr2.1210
DATA AVAILABILITY STATEMENT
All the raw data were collected from the public database (https://old.dghs.gov.bd/index.php/bd/home/5200-daily-dengue-status-report) and will also be available from the corresponding authors on request.
REFERENCES
- 1. Guzman MG, Harris E. Dengue. The Lancet. 2015;385(9966):453‐465. 10.1016/S0140-6736(14)60572-9 [DOI] [PubMed] [Google Scholar]
- 2. Bhatt S, Gething PW, Brady OJ, et al. The global distribution and burden of dengue. Nature. 2013;496(7446):504‐507. 10.1038/nature12060 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Shepard DS, Undurraga EA, Halasa YA, Stanaway JD. The global economic burden of dengue: a systematic analysis. Lancet Infect Dis. 2016;16(8):935‐941. 10.1016/s1473-3099(16)00146-8 [DOI] [PubMed] [Google Scholar]
- 4. Li Z, Dong J. Big geospatial data and data‐driven methods for urban dengue risk forecasting: a review. Remote Sens. 2022;14(19):5052. [Google Scholar]
- 5. Roy SK, Bhattacharjee S. Dengue virus: epidemiology, biology, and disease aetiology. Can J Microbiol. 2021;67(10):687‐702. 10.1139/cjm-2020-0572 [DOI] [PubMed] [Google Scholar]
- 6. Haider N, Chang Y‐M, Rahman M, Zumla A, Kock RA. Dengue outbreaks in Bangladesh: historic epidemic patterns suggest earlier mosquito control intervention in the transmission season could reduce the monthly growth factor and extent of epidemics. Curr Res Parasitol Vector‐Borne Dis. 2021;1:100063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Mutsuddy P, Tahmina Jhora S, Shamsuzzaman AKM, Kaisar SMG, Khan MNA. Dengue situation in Bangladesh: an epidemiological shift in terms of morbidity and mortality. Can J Infect Dis Med Microbiol. 2019;2019:1‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Mustafa A, Rahman A, Hossain N, Begum T Bangladesh National Health Accounts 1997‐2015 (BNHA‐V). 2018.
- 9. Banu S, Hu W, Hurst C, Guo Y, Islam MZ, Tong S. Space‐time clusters of dengue fever in Bangladesh. Trop Med Int Health. 2012;17(9):1086‐1091. 10.1111/j.1365-3156.2012.03038.x [DOI] [PubMed] [Google Scholar]
- 10. Sharmin S, Glass K, Viennet E, Harley D. Geostatistical mapping of the seasonal spread of under‐reported dengue cases in Bangladesh. PLoS Neglected Trop Dis. 2018;12(11):e0006947. 10.1371/journal.pntd.0006947 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Ali F, Chorsiya A, Anjum V, Khasimbi S, Ali A. A systematic review on phytochemicals for the treatment of dengue. Phytother Res. 2021;35(4):1782‐1816. 10.1002/ptr.6917 [DOI] [PubMed] [Google Scholar]
- 12. Jagadishkumar K, Jain P, Manjunath VG, Umesh L. Hepatic involvement in dengue fever in children. Iran J Ped. 2012;22(2):231‐236. [PMC free article] [PubMed] [Google Scholar]
- 13. Yacoub S, Griffiths A, Hong Chau TT, et al. Cardiac function in Vietnamese patients with different dengue severity grades. Crit Care Med. 2012;40(2):477‐483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Goonasekera CDA, Thenuwara BG, Kumarasiri RPV. Peritoneal dialysis in dengue shock syndrome may be detrimental. J Trop Med. 2012;2012:1‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Lim W, Mathur R, Koh A, Yeoh R, Chee S. Ocular manifestations of dengue fever. Ophthalmology. 2004;111(11):2057‐2064. [DOI] [PubMed] [Google Scholar]
- 16. Mairuhu A, Mac Gillavry M, Setiati T, et al. Is clinical outcome of dengue‐virus infections influenced by coagulation and fibrinolysis? A critical review of the evidence. Lancet Infect Dis. 2003;3(1):33‐41. [DOI] [PubMed] [Google Scholar]
- 17. Gubler DJ. Dengue and dengue hemorrhagic fever: its history and resurgence as a global public health problem. Clin Microbiol Rev. 1998;11(3):480‐496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Simadibrata M. Acute pancreatitis in dengue hemorrhagic fever. Acta Med Indones. 2012;44(1):57‐61. [PubMed] [Google Scholar]
- 19. Dalrymple NA, Mackow ER. Roles for endothelial cells in dengue virus infection. Adv Virol. 2012;2012:1‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Gibbons RV. Dengue: an escalating problem. BMJ. 2002;324(7353):1563‐1566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Robert Putnak J, Coller B‐A, Voss G, et al. An evaluation of dengue type‐2 inactivated, recombinant subunit, and live‐attenuated vaccine candidates in the rhesus macaque model. Vaccine. 2005;23(35):4442‐4452. [DOI] [PubMed] [Google Scholar]
- 22. Alyousefi TAA, Abdul‐Ghani R, Mahdy MAK, et al. A household‐based survey of knowledge, attitudes and practices towards dengue fever among local urban communities in Taiz governorate, Yemen. BMC Infect Dis. 2016;16(1):543. 10.1186/s12879-016-1895-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Harapan H, Michie A, Sasmono RT, Imrie A. Dengue: a minireview. Viruses. 2020;12(8):829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Nanaware N, Banerjee A, Mullick Bagchi S, Bagchi P, Mukherjee A. Dengue virus infection: a tale of viral exploitations and host responses. Viruses. 2021;13(10):1967. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Messina JP, Brady OJ, Golding N, et al. The current and future global distribution and population at risk of dengue. Nat Microbiol. 2019;4(9):1508‐1515. 10.1038/s41564-019-0476-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Stanaway JD, Shepard DS, Undurraga EA, et al. The global burden of dengue: an analysis from the global burden of disease study 2013. Lancet Infect Dis. 2016;16(6):712‐723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Martina BEE, Koraka P, Osterhaus ADME. Dengue virus pathogenesis: an integrated view. Clin Microbiol Rev. 2009;22(4):564‐581. 10.1128/CMR.00035-09 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Amin M, Hussain A, Nahar K, Chowdhury I, Murshed M, Chowdhury S. Searo‐diagnosis of dengue infections in four metropolitan cities of Bangladesh. WHO Regional Office for South‐East Asia; 2000. [Google Scholar]
- 29. Ahsan A, Haider N, Kock R, Benfield C. Possible drivers of the 2019 dengue outbreak in Bangladesh: the need for a robust community‐level surveillance system. J Med Entomol. 2021;58(1):37‐39. [DOI] [PubMed] [Google Scholar]
- 30. Rahman FI, Ether SA, Islam MR. Upsurge of dengue prevalence during the third wave of COVID‐19 pandemic in Bangladesh: pouring gasoline to fire. Clin Pathol. 2022;15:2632010X2210760. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All the raw data were collected from the public database (https://old.dghs.gov.bd/index.php/bd/home/5200-daily-dengue-status-report) and will also be available from the corresponding authors on request.